Hyperosmolar hyperglycemic state with severe hypernatremia coexisting with central diabetes insipidus: A case report and literature review
-
Congcong Yao


Abstract
Diabetes insipidus is characterized by polyuria and polydipsia, often resulting from central or nephrogenic causes. In diabetic emergencies, hyperosmolar hyperglycemic state (HHS), severe hypernatremia, and ventricular fibrillation are life-threatening conditions that require prompt intervention. This report describes a 47-year-old male with poorly controlled diabetes mellitus, who developed coma, excessive thirst, polyuria, hyperglycemia (47.29 mmol/L), hypernatremia (195.6 mmol/L), and plasma hyperosmolality (385 mOsm/kg). Despite fluid resuscitation and insulin therapy, refractory hypernatremia persisted, leading to a diagnosis of central diabetes insipidus (CDI). The patient also developed ventricular fibrillation, which was managed with defibrillation. Concurrently, desmopressin and blood purification were administered to address CDI and severe hypernatremia. This case emphasizes the importance of considering CDI when polyuria persists despite glucose control. The occurrence of ventricular fibrillation underscores the necessity of continuous cardiac monitoring in the context of hypovolemia and severe electrolyte imbalance. We propose that diabetes mellitus-related vascular injury impairs blood flow in the hypothalamus–pituitary tract, disrupting arginine vasopressin synthesis and secretion, contributing to CDI in poorly controlled diabetes mellitus.
Graphical abstract

1 Introduction
Polyuria, defined as a daily urine output exceeding 3 L, is a common clinical manifestation observed in conditions such as diabetes mellitus, diabetes insipidus (DI), acute renal failure, and electrolyte imbalances [1]. In diabetic patients with well-controlled blood glucose levels who continue to experience persistent polyuria and polydipsia, the possibility of coexisting DI should be considered. DI, a component of the polyuria–polydipsia syndrome, is characterized by the excretion of large volumes of dilute urine accompanied by extreme thirst and polydipsia [2]. The differential diagnosis of polyuria involves distinguishing primary DI from secondary causes [3]. Central diabetes insipidus (CDI) results from reduced synthesis and secretion of arginine vasopressin (AVP) due to various etiologies, leading to markedly decreased plasma AVP levels [4]. Treatment with exogenous AVP is typically effective. Additionally, the measurement of copeptin – a stable surrogate marker for AVP secretion – serves as an important adjunctive tool in diagnosing CDI [5]. A markedly reduced plasma copeptin level indicates impaired synthesis or secretion of AVP by the hypothalamus or pituitary gland, thereby providing further confirmation of CDI [6]. CDI can be classified into primary and secondary forms [7]. Approximately 30% of cases are primary, often idiopathic or of unknown cause, while the remaining cases are secondary, arising from identifiable pathological processes: around 25% are associated with tumors in the hypothalamic–pituitary region, 16% follow traumatic brain injury, and approximately 20% occur as a complication of intracranial surgery [8].
Hyperosmolar hyperglycemic syndrome (HHS) is a severe and common acute complication of type 2 diabetes mellitus, with a reported mortality rate of up to 20% [9]. Due to its high lethality, HHS demands prompt recognition, accurate diagnosis, and aggressive management. Its onset is typically marked by classic diabetic symptoms, including excessive thirst, polydipsia, polyuria, and fatigue, which may be newly developed or exacerbated [10]. The hallmark clinical features of HHS include severe hyperglycemia, markedly elevated plasma osmolality, profound dehydration, and varying degrees of impaired consciousness [11,12]. The underlying pathophysiological mechanism is primarily attributed to a relative deficiency of insulin, which leads to excessive hyperglycemia. This, in turn, induces osmotic diuresis and significant fluid loss, ultimately culminating in a hyperosmolar state [13].
This case report describes a rare and clinically significant presentation of a 47-year-old male who initially manifested with coma, polyuria, and dehydration, the laboratory confirmed severe hypernatremia (180 mmol/L), followed by ventricular fibrillation. He was diagnosed with CDI in the setting of a hyperosmolar hyperglycemic coma – a complex and rarely documented clinical scenario. It is hypothesized that diabetes mellitus-related microvascular injury may impair the blood supply to the hypothalamic–pituitary axis, thereby disrupting the synthesis and secretion of AVP. This case exemplifies the complex interplay between metabolic dysregulation and neuroendocrine dysfunction, suggesting that chronic diabetes mellitus may serve as a precipitating factor for CDI – a diagnosis that is frequently overlooked.
2 Case presentation
2.1 Initial presentation and symptom onset
A 47-year-old male presented with a 19-day history of polydipsia and polyuria, followed by the onset of coma 1 day prior to admission. He has a 4-year history of unclassified diabetes, usually treated with oral Chinese medicine, with a maximum recorded blood glucose level of 47 mmol/L but had not been compliant with medication. Additionally, he had a 4-year history of hypertension, with a peak systolic blood pressure of 180 mmHg, also without regular treatment or monitoring. Nineteen days before presentation, the patient developed increased thirst, excessive fluid intake (approximately 5,000 mL/day), frequent urination including nocturia, and experienced a weight loss of 2.5 kg. He reported no fever, chills, nausea, vomiting, abdominal pain, diarrhea, visual disturbances, or altered mental status during this period, and did not seek medical care.
-
Informed consent: Informed consent has been obtained from all individuals included in this study.
-
Ethical approval: The research related to human use has been complied with all the relevant national regulations, institutional policies and in accordance with the tenets of the Helsinki Declaration, and has been approved by the Medical Ethics Committee of Tianjin Medical University General Hospital.
2.2 Initial emergency management at local hospital
One day before admission, he experienced a sudden loss of consciousness, became unresponsive, and developed respiratory difficulty. He was brought to Ninghe District Hospital in Tianjin, where arterial blood gas analysis revealed: pH 7.354, PO₂ 85.3 mmHg, PCO2 21.9 mmHg, sodium 180 mmol/L, potassium 2.7 mmol/L, calcium 1.03 mmol/L, and lactate 1.5 mmol/L. A complete blood count showed: white blood cell count 25.17 × 109/L, red blood cell count 6.12 × 10¹²/L, hemoglobin 179.0 g/L, and platelet count 288 × 109/L. Biochemical tests revealed uric acid 1,255 μmol/L, glucose 47.29 mmol/L, creatinine 202 μmol/L, and urea 17.86 mmol/L.
2.3 Transfer and hospital admission
Despite treatment with 0.45% saline infusion, glucose-lowering therapy, and supportive care, the patient’s condition did not improve, prompting transfer to the Emergency Department of our hospital. Repeat blood gas analysis showed: pH 7.390, PCO₂ 45.5 mmHg, sodium 195.6 mmol/L, potassium 3.49 mmol/L, calcium 1.160 mmol/L, glucose 24.2 mmol/L, lactate 3.1 mmol/L, and plasma osmolality 385.0 mOsm/kg. Subsequent laboratory results indicated a white blood cell count of 14.14 × 10⁹/L, uric acid 938 μmol/L, creatine kinase 8,464 U/L, creatinine 118 μmol/L, and urea 8.0 mmol/L. Urinalysis revealed strongly positive glucose (++++), specific gravity of 1.014, negative ketones, and strongly positive hematuria (+++). Electrocardiography showed sinus rhythm. Additional test results are summarized in Table 1.
Laboratory results of the patients
| Laboratory test | Result | Reference value |
|---|---|---|
| Cortisol (μg/dL) | 23.90 | 5.00–25.00 |
| Adrenocorticotropic hormone (pg/mL) | 20.80 | 0.00–46.00 |
| Free triiodothyronine (pmol/L) | 1.96 | 2.43–6.01 |
| Free thyroxine (pmol/L) | 7.12 | 9.01–19.05 |
| Sensitive thyrotropin (μIU/mL) | 0.640 | 0.350–4.940 |
| Total cholesterol (mmol/L) | 4.22 | 3.59–5.17 |
| Triglycerides (mmol/L) | 1.08 | 0.57–1.71 |
| High-density lipoprotein cholesterol (mmol/L) | 0.98 | 0.80–2.20 |
| Low-density lipoprotein cholesterol (mmol/L) | 2.41 | 1.33–3.36 |
| Glycated hemoglobin (%) | 16.40 | 4.00–6.00 |
| Plasma aldosterone (ng/dL) | 3.4 | 3.0–23.6 |
| Plasma renin (μIU/mL) | 11.6 | 2.8–39.9 |
| Follicle-stimulating hormone (IU/L) | 4.0 | 0.95–11.95 |
| Luteinizing hormone (IU/L) | 0.40 | 0.57–12.07 |
| Prolactin (ng/mL) | 4.36 | 3.46–19.40 |
| Growth hormone (ng/mL) | 5.67 | 0.06–4.940 |
| Brain natriuretic peptide (pg/mL) | 115 | 0.0–100.0 |
| Troponin I (ng/mL) | <0.05 | 0.00–0.40 |
| Myoglobin (ng/mL) | >500 | 0.0–107.0 |
| Creatine kinase-MB isoenzyme (ng/mL) | 14.0 | 0.0–4.3 |
2.4 Hospital admission and initial management
Within the first 24 h of admission, the patient underwent a comprehensive diagnostic evaluation, including measurements of plasma and urine osmolality, 24 h urinary electrolytes, urinary protein and glucose levels, as well as assessments of pituitary function (Table 1).
Treatment was initiated with a low-dose insulin infusion at a rate of 0.04 IU/kg/min for glycemic control, along with hypotonic fluid replacement using 0.45% saline. Additional supportive measures included acid suppression therapy, gastric mucosal protection, and correction of electrolyte imbalances. Over the 24 h period, a total of 5,375 mL of intravenous fluid was administered, while the recorded urine output was 5,620 mL.
2.5 Treatment adjustments
Following initial treatment, the patient’s blood glucose levels exhibited a downward trend; however, he remained comatose, hypernatremia persisted, and urine output did not significantly improve (Figure 1a–c). Urine specific gravity declined, and serum creatinine levels showed a decreasing trend. Serial measurements revealed urine specific gravity fluctuating between 1.014 and 1.005 (Figure 1d). The patient was diagnosed with HHS accompanied by hypernatremia upon admission. Patients with HHS typically present with a marked reduction in effective circulating blood volume, increased urine output due to osmotic diuresis, and elevated urine osmolality. However, in this case, despite glycemic control, the patient’s urine output did not significantly decrease and was accompanied by a decline in urine osmolality. Based on these findings, a deficiency in antidiuretic hormone was suspected, prompting the initiation of desmopressin therapy. Considering the possibility of CDI, the patient was treated with oral desmopressin acetate at a dose of 0.1 mg, three times daily.
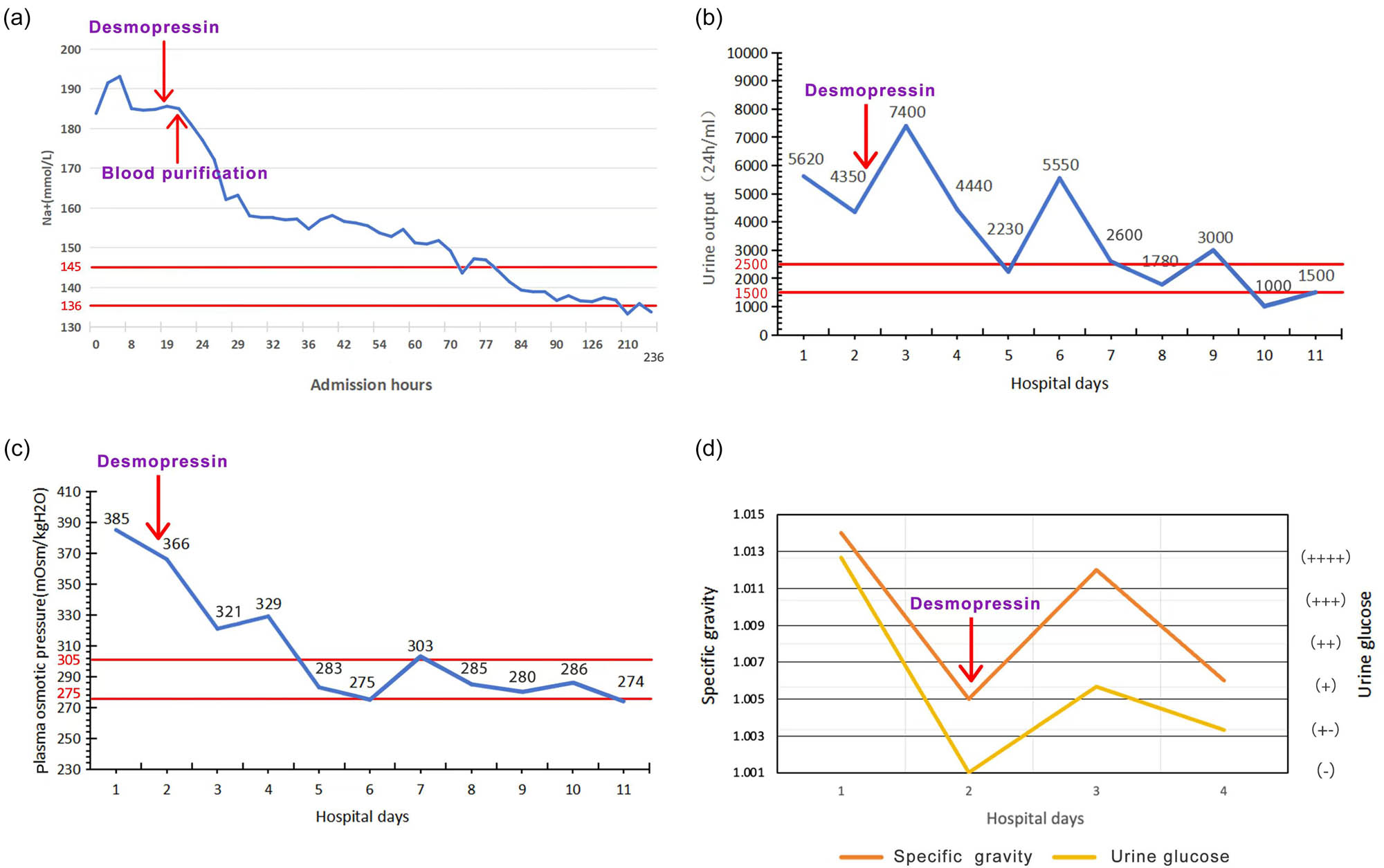
A graphical representation of changes in patients’ laboratory parameters. (a) Change trend of serum sodium after admission. (b) Change trend of urine specific gravity and urine glucose after admission. (c) Change trend of urine volume after admission. (d) Change trend of plasma osmolality after admission. Between the two red lines is the normal range. Specific gravity reference value: 1.005–1.030. Urine glucose reference value: (−). Vertical arrow indicates timing of initial desmopressin administration; maintenance therapy continued throughout hospitalization.
During treatment, the patient suddenly developed ventricular tachycardia, which progressed to ventricular fibrillation, accompanied by a precipitous drop in blood pressure to 50/25 mmHg. Immediate cardiopulmonary resuscitation and defibrillation were performed. Arterial blood gas analysis at that time showed: pH 7.466, PCO₂ 42.8 mmHg, sodium 181.2 mmol/L, potassium 4.13 mmol/L, calcium 0.957 mmol/L, glucose 13.8 mmol/L, lactate 2.4 mmol/L, and plasma osmolality 365.00 mOsm/kg. The initial electrocardiographic indicated sinus rhythm. The episode of ventricular fibrillation was considered secondary to hypovolemia induced by severe hypernatremia. Desmopressin therapy was continued in combination with fluid resuscitation, glucose management, and intravenous lidocaine for antiarrhythmic treatment. The patient was intubated, placed on mechanical ventilation, and underwent bedside continuous blood purification to maintain internal homeostasis. The sodium concentration in the replacement fluid was adjusted to 128–133 mmol/L to gradually lower serum sodium levels.
Subsequently, the patient’s level of consciousness improved, accompanied by a downward trend in both serum sodium and urine output. After 38.5 h of continuous blood purification, serum sodium decreased to 151.8 mmol/L. Blood purification was then discontinued, while desmopressin therapy was maintained (oral desmopressin acetate at a dose of 0.1 mg, three times daily). Sodium levels normalized, urine output decreased to 750–2,500 mL/day, and symptoms of thirst, polydipsia, and dehydration resolved. Plasma osmolality decreased, and urine osmolality increased (Table 2). Oral glucose tolerance test (OGTT) and insulin release test were performed, along with pituitary magnetic resonance imaging (MRI). OGTT and insulin release test revealed the following results: plasma glucose levels were 12.10 mmol/L at 0 min, 14.70 mmol/L at 30 min, 16.88 mmol/L at 60 min, 24.73 mmol/L at 120 min, and 28.79 mmol/L at 180 min. Corresponding insulin levels were 1.00, 1.60, 2.00, 2.40, and 3.50 mIU/L, respectively. C-peptide levels were 0.61, 0.68, 0.72, 0.93, and 1.28 ng/mL, respectively. The patient was diagnosed with type 1 diabetes mellitus. Pituitary MRI demonstrated mildly heterogeneous signal intensity within the pituitary gland. The pituitary stalk was midline and of normal thickness. No evidence of a mass lesion, hemorrhage, or infarction was observed (Figure S1). Following the initiation of desmopressin, the patient’s urine output declined, and clinical symptoms improved, confirming the diagnosis of CDI in the context of HHS. Maintenance therapy included oral desmopressin (0.1 mg, three times daily) with daily urine output monitoring. Insulin therapy was also implemented: 12 IU of rapid-acting insulin (Rui Xiu Lin) before meals and 16 IU of long-acting insulin (Sanofi) at bedtime. The patient remained clinically stable, with postprandial blood glucose levels ranging from 7.5 to 9.0 mmol/L and urine output between 1,000 and 1,500 mL/day. He was discharged on hospital Day 19 and reported no discomfort at a 1-month follow-up. At the 3- and 6-month follow-ups, oral desmopressin acetate (0.1 mg, three times daily) was found to effectively control the symptoms of DI.
Laboratory results before desmopressin (24 h post-admission) and after treatment (72 h post-desmopressin initiation)
| Laboratory test | Before treatment | After treatment | Reference value |
|---|---|---|---|
| White blood cells (*109/L) | 14.14 | 6.69 | 3.50–9.50 |
| Red blood cells (*1012/L) | 4.89 | 3.56 | 4.30–5.80 |
| Hemoglobin (g/L) | 144 | 104 | 130–175 |
| Platelets (*109/L) | 105 | 286 | 125–350 |
| Prothrombin time (s) | 12.2 | 12.2 | 9.5–15.0 |
| Activated partial thromboplastin time (s) | 26.8 | 30.0 | 20.0–40.0 |
| Thrombin time (s) | 25.5 | 15.2 | 13.0–25.0 |
| Fibrinogen (g/L) | 3.1 | 4.427 | 1.80–4.00 |
| d-dimer (ng/mL) | 377 | 950 | 0.00–500.0 |
| Serum creatinine (μmol/L) | 118 | 57 | 62–133 |
| Uric acid (μmol/L) | 938 | 192 | 140–414 |
| Blood urea nitrogen (mmol/L) | 8.0 | 4.2 | 2.5–7.1 |
| Total protein (g/L) | 51 | 54 | 65–85 |
| Albumin (g/L) | 27 | 27 | 40–55 |
| Alanine aminotransferase (U/L) | 37 | 23 | 9–50 |
| Aspartate aminotransferase (U/L) | 118 | 14 | 15–40 |
| Total bilirubin (μmol/L) | 9.1 | 8.3 | ≤26 |
| pH | 7.452 | 7.475 | 7.350–7.450 |
| Na+ (mmol/L) | 195.6 | 133.8 | 136.0–145.0 |
| K+ (mmol/L) | 2.93 | 3.93 | 3.50–5.10 |
| PO2 (mmHg) | 92.65 | 163.82 | 83.0–108.0 |
| PCO2 (mmHg) | 38.4 | 36.5 | 32.0–48.0 |
| Glucose (mmol/L) | 47.29 | 7.1 | 3.5–5.3 |
| Lac (mmol/L) | 2.4 | 1.0 | 0.6–1.4 |
| Plasma osmotic pressure (mOsm/kgH2O) | 385 | 303 | 275–305 |
| Urine glucose | (++++) | (−) | (−) |
| Urine occult blood | (+++) | (−) | (−) |
| Urine pH | 5.0 | 5.0 | 5.50–8.00 |
| Urinary albumin | (+−) | (−) | (−) |
| Urine leukocyte esterase | (+++) | (−) | (−) |
3 Discussion
The diagnosis of CDI in this case was established based on three key clinical criteria: (1) persistent hypotonic polyuria, as evidenced by a urine specific gravity of 1.005–1.014, despite severe hyperosmolality; (2) a marked reduction in urine output and an increase in urine osmolality following desmopressin administration (Table 2); and (3) absence of the posterior pituitary bright spot on MRI, a characteristic radiological indicator of CDI. We acknowledge that copeptin and AVP levels were not measured due to resource limitations and the patient’s critical condition. Additionally, the water deprivation test was contraindicated due to severe hypernatremia and unstable hemodynamic status. As such, the diagnosis of CDI was made based on clinical presentation (persistent polyuria, hypernatremia, low urine osmolality) and a positive clinical response to desmopressin, which rapidly reduced urine output and serum sodium levels. Nephrogenic diabetes insipidus (NDI) was excluded based on the observed response to desmopressin, as NDI typically shows resistance to vasopressin analogs.
This case highlights three critical principles in the management of complex metabolic emergencies: (1) Vigilance for dual pathology: in patients with HHS who present with persistent polyuria and refractory hypernatremia, CDI should be considered – particularly when polyuria persists despite normalization of blood glucose levels. Early administration of desmopressin reversed hypotonic polyuria and confirmed the diagnosis [14]. (2) Balanced electrolyte correction: rapid correction of hypernatremia (exceeding 0.5 mmol/L/h) increases the risk of cerebral edema, whereas delayed correction may exacerbate myocardial ischemia. In this case, bedside continuous renal replacement therapy using sodium-adjusted replacement fluid (128–133 mmol/L) enabled controlled serum sodium reduction while avoiding neurological complications. (3) Prevention of cardiac events: severe hypovolemia due to fluid loss from both HHS and CDI can compromise coronary perfusion. Concurrent electrolyte disturbances further reduce the threshold for life-threatening arrhythmias such as ventricular fibrillation. Continuous electrocardiographic monitoring and hemodynamic support are essential, with immediate defibrillation critical in the event of ventricular fibrillation.
Among the key insights, maintaining vigilance for dual pathology is particularly critical. In this case, the coexistence of HHS and CDI created a vicious cycle that significantly worsened the patient’s clinical condition. HHS, characterized by profound hyperglycemia, triggered osmotic diuresis, leading to severe dehydration and hypernatremia [11]. Concurrently, CDI – resulting from AVP deficiency – impaired renal water reabsorption, further exacerbating polyuria and hyperosmolality. The synergistic effect of HHS-induced osmotic diuresis and CDI-induced hypotonic polyuria caused profound volume depletion and hypernatremia, culminating in hypovolemic shock. This, in turn, compromised coronary perfusion and increased the risk of ventricular fibrillation, which ultimately occurred. Moreover, in patients with long-standing or poorly controlled diabetes mellitus, chronic hyperglycemia may cause microvascular lesions in the pituitary stalk, thereby impairing blood flow to AVP-producing neurons. This disruption can inhibit AVP synthesis and secretion, increasing susceptibility to CDI. Although rare, Wolfram syndrome – a genetic disorder characterized by the coexistence of DI, type 1 diabetes mellitus, optic atrophy, and deafness – should also be considered in such presentations [14,15]. However, the absence of visual or auditory abnormalities in this patient ruled out Wolfram syndrome. In conclusion, microvascular injury resulting from chronic hyperglycemia represents a plausible etiology for CDI in this case, although other possibilities, such as subclinical autoimmune hypophysitis, warrant consideration. While pituitary MRI revealed no structural abnormalities, diabetic microangiopathy could have caused pituitary stalk ischemia, impairing AVP axonal transport.
This pathophysiological hypothesis requires further validation in future studies. Clinically, the focus should remain on recognizing the pathological interplay between HHS and CDI in the context of uncontrolled type 1 diabetes mellitus.
DI is characterized by impaired renal water reabsorption, either due to a deficiency of AVP or renal resistance to its action, resulting in hypotonic polyuria and polydipsia [16]. It is a rare disorder, with an estimated prevalence of approximately 1 in 25,000 individuals, affecting all age groups and occurring equally across genders [17,18]. The pathophysiology of DI involves disruptions in the synthesis or transport of AVP by the supraoptic and paraventricular nuclei of the hypothalamus. This results in an inability of the kidneys to reabsorb water in the collecting ducts, leading to the excretion of large volumes of dilute urine, increased plasma osmolality, and stimulation of the hypothalamic thirst center, thereby causing excessive thirst and fluid intake [19]. CDI arises from AVP deficiency due to dysfunction of the hypothalamic–pituitary axis. Etiologies of CDI can be either acquired or hereditary [20]. Acquired CDI is more common and typically occurs when more than 80% of AVP-secreting neurons are destroyed, while hereditary CDI accounts for approximately 1% of cases [21,22]. The primary pathogenesis involves impaired AVP synthesis or insufficient release from the posterior pituitary in response to osmotic stimuli [23].
Patients with CDI can be treated with vasopressin replacement therapy, which is effective in restoring water balance. In contrast, NDI, characterized by renal insensitivity to AVP, does not respond to exogenous hormone administration and currently lacks a definitive, targeted treatment [24]. Although the water deprivation test remains a key diagnostic tool for differentiating CDI from NDI, it was contraindicated in this patient due to the presence of severe hypernatremia, hyperosmolarity, and altered mental status. Plasma AVP measurement would have further aided the diagnosis, but it was unavailable at our facility. Given these limitations, the diagnosis of CDI relied on indirect clinical indicators. Notably, the patient’s urine specific gravity and clinical response to desmopressin therapy were pivotal. A reduction in urine specific gravity during treatment, in conjunction with symptomatic improvement following desmopressin administration, strongly supported the diagnosis of CDI [25]. Following treatment, the patient underwent pituitary MRI, which revealed a slightly heterogeneous pituitary signal with preserved size and morphology. No evidence of mass lesions, hemorrhage, or infarction was observed [26]. This imaging finding was critical in ruling out structural causes of acquired CDI. The typical MRI manifestation of CDI is the absence of the normal posterior pituitary “bright spot” on T1-weighted imaging, reflecting the depletion or dysfunction of AVP and its neurosecretory granules in the neurohypophysis [25]. However, in this case, a temporal or individual discrepancy may exist between the MRI findings and the patient’s hormonal functional status. Previous studies have shown that the visibility of the posterior pituitary high signal is not entirely equivalent to intact AVP function [27]. In certain CDI patients – particularly in the early stages of disease, with mild involvement, or in cases with obscure etiology (such as idiopathic or autoimmune CDI) – the structural integrity of the neurohypophysis may be partially preserved, and obvious radiologic abnormalities may not yet be apparent [28].
Based on these findings, it is proposed that the patient’s CDI may have resulted from diabetes mellitus-associated microvascular injury, which likely compromised blood supply to the hypothalamic–pituitary axis, thereby disrupting the synthesis and secretion of AVP. Furthermore, chronic systemic inflammation, a well-recognized feature of diabetes mellitus, may contribute to the development of complications such as hypernatremia and CDI [29]. Elevated inflammatory markers, including white blood cell count, C-reactive protein, and the neutrophil-to-lymphocyte ratio, are frequently observed in patients with type 2 diabetes mellitus and are associated with poor glycemic control and endothelial dysfunction. Emerging evidence suggests that inflammation may also impair AVP secretion and action, further disrupting water homeostasis and contributing to the pathogenesis of CDI [30]. Additionally, the uric acid to high-density lipoprotein cholesterol ratio, a composite marker of metabolic and inflammatory stress, has been linked to poorly controlled diabetes mellitus and its complications, suggesting a potential connection between metabolic inflammation and CDI [31]. Inflammatory responses may directly influence kidney function and AVP activity, playing a central role in the development of both hypernatremia and CDI in diabetic patients. These findings underscore the importance of comprehensive management strategies that target not only glycemic control but also systemic inflammation to prevent and mitigate complex complications such as CDI [32,33].
Severe hypernatremia, defined as a serum sodium concentration exceeding 160 mmol/L, and extreme hypernatremia (>190 mmol/L), are associated with significant morbidity and mortality rates exceeding 60% [34,35]. Hyperosmolarity causes cellular dehydration, particularly in neural tissues, leading to neurological dysfunction, coma, and death [36,37]. Extreme hypernatremia is rare, and reports describing electrocardiographic changes at such high sodium levels are limited [38]. Sodium, the principal extracellular cation, is critical for cellular depolarization and action potential generation. Hypernatremia-related electrocardiographic abnormalities, including QT prolongation and reduced P and QRS amplitudes, have been documented. Guidelines for chronic hypernatremia recommend a correction rate of 10–12 mmol/L/24 h to prevent cerebral edema [39]. However, recent studies suggest that slower correction rates in hospitalized patients with severe hypernatremia may be associated with increased mortality [40]. Although evidence on extreme hypernatremia is scarce, several case reports have demonstrated successful rapid correction under close monitoring without neurological complications [41]. Both overly rapid and excessively delayed correction carry significant risks [42]. Rapid correction may result in cerebral edema and myocardial ischemia, while insufficient correction can lead to persistent hypernatremia and its complications [43]. In the present case, a combination of fluid resuscitation and sodium-regulated continuous blood purification enabled safe normalization of serum sodium levels and reduction of urine output. The serum sodium decreased from 195.6 to 144.3 mmol/L over 79 h, corresponding to a correction rate of approximately 0.64 mmol/L/h. This rate was below the maximum recommended 2 mmol/L/h for acute hypernatremia to prevent cerebral edema but exceeded the conventional 10–12 mmol/L24 h target for chronic hypernatremia. Given the critical presentation, the accelerated correction was justified and achieved without neurological complications under continuous monitoring [44,45]. This case underscores the importance of carefully balancing the rate of sodium correction to prevent potentially fatal complications while ensuring effective management of hypernatremia.
4 Conclusions
In conclusion, this case demonstrates the complex interplay between CDI and HHS in a patient with poorly controlled type 1 diabetes mellitus. The occurrence of severe hypernatremia and ventricular fibrillation due to combined hypovolemia and electrolyte imbalance is exceptionally rare. This includes careful correction of electrolyte abnormalities, strict glycemic control, and hemodynamic stabilization. The case further emphasizes the importance of considering CDI in patients presenting with persistent polyuria and refractory hypernatremia, even after partial normalization of blood glucose levels. Additionally, it highlights the critical necessity of continuous cardiac monitoring during severe electrolyte disturbances.
Acknowledgments
The authors thank Department of Emergency Medicine, Tianjin Medical University General Hospital for providing the experimental place used in this study.
-
Funding information: This research was funded by Tianjin Municipal Science and Technology Bureau (grant number: 24ZYCGSN01310).
-
Author contributions: All authors have contributed to this manuscript and have agreed to its submission to the journal. Congcong Yao and Yan Zhang attended the patient. Congcong Yao and Lishuang Zhu wrote the manuscript. Heng Jin and Songtao Shou reviewed the literature. All authors read and approved the final manuscript.
-
Conflict of interest: Authors state no conflict of interest.
-
Data availability statement: The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
References
[1] Jakes AD, Bhandari S. Investigating polyuria. BMJ. 2013;347:f6772.10.1136/bmj.f6772Suche in Google Scholar PubMed
[2] Refardt J. Diagnosis and differential diagnosis of diabetes insipidus: update. Best Pract Res Clin Endocrinol Metab. 2020;34(5):101398.10.1016/j.beem.2020.101398Suche in Google Scholar PubMed
[3] Tomkins M, Lawless S, Martin-Grace J, Sherlock M, Thompson CJ. Diagnosis and management of central diabetes insipidus in adults. J Clin Endocrinol Metab. 2022;107(10):2701–15.10.1210/clinem/dgac381Suche in Google Scholar PubMed PubMed Central
[4] Mutter CM, Smith T, Menze O, Zakharia M, Nguyen H. Diabetes insipidus: pathogenesis, diagnosis, and clinical management. Cureus. 2021;13(2):e13523.10.7759/cureus.13523Suche in Google Scholar PubMed PubMed Central
[5] Moodley N. Copeptin analysis in endocrine disorders. Front Endocrinol (Lausanne). 2023;14:1230045.10.3389/fendo.2023.1230045Suche in Google Scholar PubMed PubMed Central
[6] Jalleh R, Torpy DJ. The emerging role of copeptin. Clin Biochem Rev. 2021;42(1):17–25.10.33176/AACB-20-00001Suche in Google Scholar PubMed PubMed Central
[7] Patti G, Ibba A, Morana G, Napoli F, Fava D, di Iorgi N, et al. Central diabetes insipidus in children: diagnosis and management. Best Pract Res Clin Endocrinol Metab. 2020;34(5):101440.10.1016/j.beem.2020.101440Suche in Google Scholar PubMed
[8] Christ-Crain M, Winzeler B, Refardt J. Diagnosis and management of diabetes insipidus for the internist: an update. J Intern Med. 2021;290(1):73–87.10.1111/joim.13261Suche in Google Scholar PubMed
[9] Adeyinka A, Kondamudi NP. Hyperosmolar hyperglycemic syndrome. Treasure Island (FL): StatPearls; 2024.Suche in Google Scholar
[10] Adeyinka A, Kondamudi NP. Hyperosmolar hyperglycemic syndrome. Treasure Island (FL): StatPearls; 2025.Suche in Google Scholar
[11] Orłowska D, Kapłan W, Ostański J, Zalewa K, Bartoszek L, Świdziński R, et al. Hyperosmolar hyperglycemic syndrome: a comprehensive review of clinical presentation, diagnosis, and treatment strategies in hyperglycemic crises. J Educ Health Sport. 2024;55:217–30.10.12775/JEHS.2024.55.014Suche in Google Scholar
[12] Mustafa OG, Haq M, Dashora U, Castro E, Dhatariya KK. Management of hyperosmolar hyperglycaemic state (HHS) in adults: an updated guideline from the Joint British Diabetes Societies (JBDS) for Inpatient Care group. Diabet Med. 2022;40(3):e15005. 10.1111/dme.15005.Suche in Google Scholar PubMed PubMed Central
[13] Umpierrez GE, Davis GM, ElSayed NA, Fadini GP, Galindo RJ, Hirsch IB, et al. Hyperglycaemic crises in adults with diabetes: a consensus report. Diabetologia. 2024;67(8):1455–79.10.1007/s00125-024-06183-8Suche in Google Scholar PubMed PubMed Central
[14] Spiess M, Beuret N, Rutishauser J. Genetic forms of neurohypophyseal diabetes insipidus. Best Pract Res Clin Endocrinol Metab. 2020;34(5):101432.10.1016/j.beem.2020.101432Suche in Google Scholar PubMed
[15] Waschbisch A, Volbers B, Struffert T, Hoyer J, Schwab S, Bardutzky J. Primary diagnosis of Wolfram syndrome in an adult patient – case report and description of a novel pathogenic mutation. J Neurol Sci. 2011;300(1–2):191–3.10.1016/j.jns.2010.08.044Suche in Google Scholar PubMed
[16] Refardt J, Winzeler B, Christ-Crain M. Diabetes insipidus: an update. Endocrinol Metab Clin North Am. 2020;49(3):517–31.10.1016/j.ecl.2020.05.012Suche in Google Scholar PubMed
[17] Kalra S, Zargar AH, Jain SM, Sethi B, Chowdhury S, Singh AK, et al. Diabetes insipidus: the other diabetes. Indian J Endocrinol Metab. 2016;20(1):9–21.10.4103/2230-8210.172273Suche in Google Scholar PubMed PubMed Central
[18] Christ-Crain M, Bichet DG, Fenske WK, Goldman MB, Rittig S, Verbalis JG, et al. Diabetes insipidus. Nat Rev Dis Primers. 2019;5(1):54.10.1038/s41572-019-0103-2Suche in Google Scholar PubMed
[19] Fabre L, Silva VCD. Idiopathic partial central diabetes insipidus. Einstein (Sao Paulo). 2023;21:eRC0124.10.31744/einstein_journal/2023RC0124Suche in Google Scholar PubMed PubMed Central
[20] Angelousi A, Alexandraki KI, Mytareli C, Grossman AB, Kaltsas G. New developments and concepts in the diagnosis and management of diabetes insipidus (AVP-deficiency and resistance). J Neuroendocrinol. 2023;35(1):e13233.10.1111/jne.13233Suche in Google Scholar PubMed
[21] Priya G, Kalra S, Dasgupta A, Grewal E. Diabetes insipidus: a pragmatic approach to management. Cureus. 2021;13(1):e12498.10.7759/cureus.12498Suche in Google Scholar PubMed PubMed Central
[22] Adams NC, Farrell TP, O’Shea A, O’Hare A, Thornton J, Power S, et al. Neuroimaging of central diabetes insipidus-when, how and findings. Neuroradiology. 2018;60(10):995–1012.10.1007/s00234-018-2072-7Suche in Google Scholar PubMed
[23] Di Iorgi N, Napoli F, Allegri AE, Olivieri I, Bertelli E, Gallizia A, et al. Diabetes insipidus – diagnosis and management. Horm Res Paediatr. 2012;77(2):69–84.10.1159/000336333Suche in Google Scholar PubMed
[24] Cerbone M, Visser J, Bulwer C, Ederies A, Vallabhaneni K, Ball S, et al. Management of children and young people with idiopathic pituitary stalk thickening, central diabetes insipidus, or both: a national clinical practice consensus guideline. Lancet Child Adolesc Health. 2021;5(9):662–76.10.1016/S2352-4642(21)00088-2Suche in Google Scholar PubMed
[25] Christ-Crain M, Gaisl O. Diabetes insipidus. Presse Med. 2021;50(4):104093.10.1016/j.lpm.2021.104093Suche in Google Scholar PubMed
[26] Farrell TP, Adams NC, Looby S. Neuroimaging of central diabetes insipidus. Handb Clin Neurol. 2021;181:207–37.10.1016/B978-0-12-820683-6.00016-6Suche in Google Scholar PubMed
[27] Manaka K, Sato J, Makita N. Neuroendocrine manifestations of Erdheim-Chester disease. Handb Clin Neurol. 2021;181:137–47.10.1016/B978-0-12-820683-6.00010-5Suche in Google Scholar PubMed
[28] Palumbo C, Nicolaci N, La Manna AA, Branek N, Pissano MN. Association between central diabetes insipidus and type 2 diabetes mellitus. Medicina (B Aires). 2018;78(2):127–30.Suche in Google Scholar
[29] Liu S, Chen W, Zhao Y, Ma S, Shi B, Guo H. SGLT2 inhibitor in a type 2 diabetes mellitus patient coexisted with central diabetes insipidus following hyperosmolar hyperglycemic state. BMC Endocr Disord. 2025;25(1):112.10.1186/s12902-025-01924-1Suche in Google Scholar PubMed PubMed Central
[30] Wang J, Wang G, Cheng L, Zhu H, Wang J, Ding X, et al. Preoperative peripheral inflammatory markers are predictors of postoperative central diabetes insipidus in craniopharyngioma patients: a retrospective study. BMC Cancer. 2024;24(1):572. 10.1186/s12885-024-12324-4.Suche in Google Scholar PubMed PubMed Central
[31] Aktas G, Kocak MZ, Bilgin S, Atak BM, Duman TT, Kurtkulagi O. Uric acid to HDL cholesterol ratio is a strong predictor of diabetic control in men with type 2 diabetes mellitus. Aging Male. 2019;23(5):1098–102.10.1080/13685538.2019.1678126Suche in Google Scholar PubMed
[32] Aktas G. Association between the prognostic nutritional index and chronic microvascular complications in patients with type 2 diabetes mellitus. J Clin Med. 2023;12(18):5952. 10.3390/jcm12185952.Suche in Google Scholar PubMed PubMed Central
[33] Tuladhar A, Shaver JC, McGee WA, Yu K, Dorn J, Horne JL, et al. Prkd1 regulates the formation and repair of plasma membrane disruptions (PMD) in osteocytes. Bone. 2024;186:117147.10.1016/j.bone.2024.117147Suche in Google Scholar PubMed PubMed Central
[34] Braun MM, Barstow CH, Pyzocha NJ. Diagnosis and management of sodium disorders: hyponatremia and hypernatremia. Am Fam Physician. 2015;91(5):299–307.Suche in Google Scholar
[35] Arzhan S, Roumelioti M-E, Litvinovich I, Bologa CG, Unruh ML. Outcomes of hospital-acquired hypernatremia. Clin J Am Soc Nephrol. 2023;18(11):1396–407.10.2215/CJN.0000000000000250Suche in Google Scholar PubMed PubMed Central
[36] Sterns RH. Disorders of plasma sodium – causes, consequences, and correction. N Engl J Med. 2015;372(1):55–65.10.1056/NEJMra1404489Suche in Google Scholar PubMed
[37] Ravioli S, Rohn V, Lindner G. Hypernatremia at presentation to the emergency department: a case series. Intern Emerg Med. 2022;17(8):2323–8.10.1007/s11739-022-03097-4Suche in Google Scholar PubMed PubMed Central
[38] Arambewela MH, Somasundaram NP, Garusinghe C. Extreme hypernatremia as a probable cause of fatal arrhythmia: a case report. J Med Case Rep. 2016;10(1):272.10.1186/s13256-016-1062-9Suche in Google Scholar PubMed PubMed Central
[39] Al-Absi A, Gosmanova EO, Wall BM. A clinical approach to the treatment of chronic hypernatremia. Am J Kidney Dis. 2012;60(6):1032–8.10.1053/j.ajkd.2012.06.025Suche in Google Scholar PubMed
[40] Alshayeb HM, Showkat A, Babar F, Mangold T, Wall BM. Severe hypernatremia correction rate and mortality in hospitalized patients. Am J Med Sci. 2011;341(5):356–60.10.1097/MAJ.0b013e31820a3a90Suche in Google Scholar PubMed
[41] Yang TY, Chang JW, Tseng MH, Wang HH, Niu DM, Yang LY. Extreme hypernatremia combined with rhabdomyolysis and acute renal failure. J Chin Med Assoc. 2009;72(10):555–8.10.1016/S1726-4901(09)70428-9Suche in Google Scholar PubMed
[42] Chand R, Chand R, Goldfarb DS. Hypernatremia in the intensive care unit. Curr Opin Nephrol Hypertens. 2022;31(2):199–204.10.1097/MNH.0000000000000773Suche in Google Scholar PubMed
[43] Ilardi A. Diagnostic and therapeutic approach to hypernatremia. Diagnosis (Berl). 2022;9(4):403–10.10.1515/dx-2022-0034Suche in Google Scholar PubMed
[44] Chauhan K, Pattharanitima P, Patel N, Duffy A, Saha A, Chaudhary K, et al. Rate of correction of hypernatremia and health outcomes in critically ill patients. Clin J Am Soc Nephrol. 2019;14(5):656–63.10.2215/CJN.10640918Suche in Google Scholar PubMed PubMed Central
[45] Liamis G, Filippatos TD, Elisaf MS. Evaluation and treatment of hypernatremia: a practical guide for physicians. Postgrad Med. 2016;128(3):299–306.10.1080/00325481.2016.1147322Suche in Google Scholar PubMed
© 2025 the author(s), published by De Gruyter
This work is licensed under the Creative Commons Attribution 4.0 International License.
Artikel in diesem Heft
- Safety assessment and modulation of hepatic CYP3A4 and UGT enzymes by Glycyrrhiza glabra aqueous extract in female Sprague–Dawley rats
- Adult-onset Still’s disease with hemophagocytic lymphohistiocytosis and minimal change disease
- Role of DZ2002 in reducing corneal graft rejection in rats by influencing Th17 activation via inhibition of the PI3K/AKT pathway and downregulation of TRAF1
- Biomedical Sciences
- Mechanism of triptolide regulating proliferation and apoptosis of hepatoma cells by inhibiting JAK/STAT pathway
- Maslinic acid improves mitochondrial function and inhibits oxidative stress and autophagy in human gastric smooth muscle cells
- Comparative analysis of inflammatory biomarkers for the diagnosis of neonatal sepsis: IL-6, IL-8, SAA, CRP, and PCT
- Post-pandemic insights on COVID-19 and premature ovarian insufficiency
- Proteome differences of dental stem cells between permanent and deciduous teeth by data-independent acquisition proteomics
- Optimizing a modified cetyltrimethylammonium bromide protocol for fungal DNA extraction: Insights from multilocus gene amplification
- Preliminary analysis of the role of small hepatitis B surface proteins mutations in the pathogenesis of occult hepatitis B infection via the endoplasmic reticulum stress-induced UPR-ERAD pathway
- Efficacy of alginate-coated gold nanoparticles against antibiotics-resistant Staphylococcus and Streptococcus pathogens of acne origins
- Battling COVID-19 leveraging nanobiotechnology: Gold and silver nanoparticle–B-escin conjugates as SARS-CoV-2 inhibitors
- Neurodegenerative diseases and neuroinflammation-induced apoptosis
- Impact of fracture fixation surgery on cognitive function and the gut microbiota in mice with a history of stroke
- COLEC10: A potential tumor suppressor and prognostic biomarker in hepatocellular carcinoma through modulation of EMT and PI3K-AKT pathways
- High-temperature requirement serine protease A2 inhibitor UCF-101 ameliorates damaged neurons in traumatic brain-injured rats by the AMPK/NF-κB pathway
- SIK1 inhibits IL-1β-stimulated cartilage apoptosis and inflammation in vitro through the CRTC2/CREB1 signaling
- Rutin–chitooligosaccharide complex: Comprehensive evaluation of its anti-inflammatory and analgesic properties in vitro and in vivo
- Knockdown of Aurora kinase B alleviates high glucose-triggered trophoblast cells damage and inflammation during gestational diabetes
- Calcium-sensing receptors promoted Homer1 expression and osteogenic differentiation in bone marrow mesenchymal stem cells
- ABI3BP can inhibit the proliferation, invasion, and epithelial–mesenchymal transition of non-small-cell lung cancer cells
- Changes in blood glucose and metabolism in hyperuricemia mice
- Rapid detection of the GJB2 c.235delC mutation based on CRISPR-Cas13a combined with lateral flow dipstick
- IL-11 promotes Ang II-induced autophagy inhibition and mitochondrial dysfunction in atrial fibroblasts
- Short-chain fatty acid attenuates intestinal inflammation by regulation of gut microbial composition in antibiotic-associated diarrhea
- Application of metagenomic next-generation sequencing in the diagnosis of pathogens in patients with diabetes complicated by community-acquired pneumonia
- NAT10 promotes radiotherapy resistance in non-small cell lung cancer by regulating KPNB1-mediated PD-L1 nuclear translocation
- Phytol-mixed micelles alleviate dexamethasone-induced osteoporosis in zebrafish: Activation of the MMP3–OPN–MAPK pathway-mediating bone remodeling
- Association between TGF-β1 and β-catenin expression in the vaginal wall of patients with pelvic organ prolapse
- Primary pleomorphic liposarcoma involving bilateral ovaries: Case report and literature review
- Effects of de novo donor-specific Class I and II antibodies on graft outcomes after liver transplantation: A pilot cohort study
- Sleep architecture in Alzheimer’s disease continuum: The deep sleep question
- Ephedra fragilis plant extract: A groundbreaking corrosion inhibitor for mild steel in acidic environments – electrochemical, EDX, DFT, and Monte Carlo studies
- Langerhans cell histiocytosis in an adult patient with upper jaw and pulmonary involvement: A case report
- Inhibition of mast cell activation by Jaranol-targeted Pirin ameliorates allergic responses in mouse allergic rhinitis
- Aeromonas veronii-induced septic arthritis of the hip in a child with acute lymphoblastic leukemia
- Clusterin activates the heat shock response via the PI3K/Akt pathway to protect cardiomyocytes from high-temperature-induced apoptosis
- Research progress on fecal microbiota transplantation in tumor prevention and treatment
- Low-pressure exposure influences the development of HAPE
- Stigmasterol alleviates endplate chondrocyte degeneration through inducing mitophagy by enhancing PINK1 mRNA acetylation via the ESR1/NAT10 axis
- AKAP12, mediated by transcription factor 21, inhibits cell proliferation, metastasis, and glycolysis in lung squamous cell carcinoma
- Association between PAX9 or MSX1 gene polymorphism and tooth agenesis risk: A meta-analysis
- A case of bloodstream infection caused by Neisseria gonorrhoeae
- Case of nasopharyngeal tuberculosis complicated with cervical lymph node and pulmonary tuberculosis
- p-Cymene inhibits pro-fibrotic and inflammatory mediators to prevent hepatic dysfunction
- GFPT2 promotes paclitaxel resistance in epithelial ovarian cancer cells via activating NF-κB signaling pathway
- Transfer RNA-derived fragment tRF-36 modulates varicose vein progression via human vascular smooth muscle cell Notch signaling
- RTA-408 attenuates the hepatic ischemia reperfusion injury in mice possibly by activating the Nrf2/HO-1 signaling pathway
- Decreased serum TIMP4 levels in patients with rheumatoid arthritis
- Sirt1 protects lupus nephritis by inhibiting the NLRP3 signaling pathway in human glomerular mesangial cells
- Sodium butyrate aids brain injury repair in neonatal rats
- Interaction of MTHFR polymorphism with PAX1 methylation in cervical cancer
- Convallatoxin inhibits proliferation and angiogenesis of glioma cells via regulating JAK/STAT3 pathway
- The effect of the PKR inhibitor, 2-aminopurine, on the replication of influenza A virus, and segment 8 mRNA splicing
- Effects of Ire1 gene on virulence and pathogenicity of Candida albicans
- Small cell lung cancer with small intestinal metastasis: Case report and literature review
- GRB14: A prognostic biomarker driving tumor progression in gastric cancer through the PI3K/AKT signaling pathway by interacting with COBLL1
- 15-Lipoxygenase-2 deficiency induces foam cell formation that can be restored by salidroside through the inhibition of arachidonic acid effects
- FTO alleviated the diabetic nephropathy progression by regulating the N6-methyladenosine levels of DACT1
- Clinical relevance of inflammatory markers in the evaluation of severity of ulcerative colitis: A retrospective study
- Zinc valproic acid complex promotes osteoblast differentiation and exhibits anti-osteoporotic potential
- Primary pulmonary synovial sarcoma in the bronchial cavity: A case report
- Metagenomic next-generation sequencing of alveolar lavage fluid improves the detection of pulmonary infection
- Uterine tumor resembling ovarian sex cord tumor with extensive rhabdoid differentiation: A case report
- Genomic analysis of a novel ST11(PR34365) Clostridioides difficile strain isolated from the human fecal of a CDI patient in Guizhou, China
- Effects of tiered cardiac rehabilitation on CRP, TNF-α, and physical endurance in older adults with coronary heart disease
- Changes in T-lymphocyte subpopulations in patients with colorectal cancer before and after acupoint catgut embedding acupuncture observation
- Modulating the tumor microenvironment: The role of traditional Chinese medicine in improving lung cancer treatment
- Alterations of metabolites related to microbiota–gut–brain axis in plasma of colon cancer, esophageal cancer, stomach cancer, and lung cancer patients
- Research on individualized drug sensitivity detection technology based on bio-3D printing technology for precision treatment of gastrointestinal stromal tumors
- CEBPB promotes ulcerative colitis-associated colorectal cancer by stimulating tumor growth and activating the NF-κB/STAT3 signaling pathway
- Oncolytic bacteria: A revolutionary approach to cancer therapy
- A de novo meningioma with rapid growth: A possible malignancy imposter?
- Diagnosis of secondary tuberculosis infection in an asymptomatic elderly with cancer using next-generation sequencing: Case report
- Hesperidin and its zinc(ii) complex enhance osteoblast differentiation and bone formation: In vitro and in vivo evaluations
- Research progress on the regulation of autophagy in cardiovascular diseases by chemokines
- Anti-arthritic, immunomodulatory, and inflammatory regulation by the benzimidazole derivative BMZ-AD: Insights from an FCA-induced rat model
- Immunoassay for pyruvate kinase M1/2 as an Alzheimer’s biomarker in CSF
- The role of HDAC11 in age-related hearing loss: Mechanisms and therapeutic implications
- Evaluation and application analysis of animal models of PIPNP based on data mining
- Therapeutic approaches for liver fibrosis/cirrhosis by targeting pyroptosis
- Fabrication of zinc oxide nanoparticles using Ruellia tuberosa leaf extract induces apoptosis through P53 and STAT3 signalling pathways in prostate cancer cells
- Haplo-hematopoietic stem cell transplantation and immunoradiotherapy for severe aplastic anemia complicated with nasopharyngeal carcinoma: A case report
- Modulation of the KEAP1-NRF2 pathway by Erianin: A novel approach to reduce psoriasiform inflammation and inflammatory signaling
- The expression of epidermal growth factor receptor 2 and its relationship with tumor-infiltrating lymphocytes and clinical pathological features in breast cancer patients
- Innovations in MALDI-TOF Mass Spectrometry: Bridging modern diagnostics and historical insights
- BAP1 complexes with YY1 and RBBP7 and its downstream targets in ccRCC cells
- Hypereosinophilic syndrome with elevated IgG4 and T-cell clonality: A report of two cases
- Electroacupuncture alleviates sciatic nerve injury in sciatica rats by regulating BDNF and NGF levels, myelin sheath degradation, and autophagy
- Polydatin prevents cholesterol gallstone formation by regulating cholesterol metabolism via PPAR-γ signaling
- RNF144A and RNF144B: Important molecules for health
- Analysis of the detection rate and related factors of thyroid nodules in the healthy population
- Artesunate inhibits hepatocellular carcinoma cell migration and invasion through OGA-mediated O-GlcNAcylation of ZEB1
- Endovascular management of post-pancreatectomy hemorrhage caused by a hepatic artery pseudoaneurysm: Case report and review of the literature
- Efficacy and safety of anti-PD-1/PD-L1 antibodies in patients with relapsed refractory diffuse large B-cell lymphoma: A meta-analysis
- SATB2 promotes humeral fracture healing in rats by activating the PI3K/AKT pathway
- Overexpression of the ferroptosis-related gene, NFS1, corresponds to gastric cancer growth and tumor immune infiltration
- Understanding risk factors and prognosis in diabetic foot ulcers
- Atractylenolide I alleviates the experimental allergic response in mice by suppressing TLR4/NF-kB/NLRP3 signalling
- FBXO31 inhibits the stemness characteristics of CD147 (+) melanoma stem cells
- Immune molecule diagnostics in colorectal cancer: CCL2 and CXCL11
- Inhibiting CXCR6 promotes senescence of activated hepatic stellate cells with limited proinflammatory SASP to attenuate hepatic fibrosis
- Cadmium toxicity, health risk and its remediation using low-cost biochar adsorbents
- Pulmonary cryptococcosis with headache as the first presentation: A case report
- Solitary pulmonary metastasis with cystic airspaces in colon cancer: A rare case report
- RUNX1 promotes denervation-induced muscle atrophy by activating the JUNB/NF-κB pathway and driving M1 macrophage polarization
- Morphometric analysis and immunobiological investigation of Indigofera oblongifolia on the infected lung with Plasmodium chabaudi
- The NuA4/TIP60 histone-modifying complex and Hr78 modulate the Lobe2 mutant eye phenotype
- Experimental study on salmon demineralized bone matrix loaded with recombinant human bone morphogenetic protein-2: In vitro and in vivo study
- A case of IgA nephropathy treated with a combination of telitacicept and half-dose glucocorticoids
- Analgesic and toxicological evaluation of cannabidiol-rich Moroccan Cannabis sativa L. (Khardala variety) extract: Evidence from an in vivo and in silico study
- Wound healing and signaling pathways
- Combination of immunotherapy and whole-brain radiotherapy on prognosis of patients with multiple brain metastases: A retrospective cohort study
- To explore the relationship between endometrial hyperemia and polycystic ovary syndrome
- Research progress on the impact of curcumin on immune responses in breast cancer
- Biogenic Cu/Ni nanotherapeutics from Descurainia sophia (L.) Webb ex Prantl seeds for the treatment of lung cancer
- Dapagliflozin attenuates atrial fibrosis via the HMGB1/RAGE pathway in atrial fibrillation rats
- Glycitein alleviates inflammation and apoptosis in keratinocytes via ROS-associated PI3K–Akt signalling pathway
- ADH5 inhibits proliferation but promotes EMT in non-small cell lung cancer cell through activating Smad2/Smad3
- Apoptotic efficacies of AgNPs formulated by Syzygium aromaticum leaf extract on 32D-FLT3-ITD human leukemia cell line with PI3K/AKT/mTOR signaling pathway
- Novel cuproptosis-related genes C1QBP and PFKP identified as prognostic and therapeutic targets in lung adenocarcinoma
- Bee venom promotes exosome secretion and alters miRNA cargo in T cells
- Treatment of pure red cell aplasia in a chronic kidney disease patient with roxadustat: A case report
- Comparative bioinformatics analysis of the Wnt pathway in breast cancer: Selection of novel biomarker panels associated with ER status
- Kynurenine facilitates renal cell carcinoma progression by suppressing M2 macrophage pyroptosis through inhibition of CASP1 cleavage
- RFX5 promotes the growth, motility, and inhibits apoptosis of gastric adenocarcinoma cells through the SIRT1/AMPK axis
- ALKBH5 exacerbates early cardiac damage after radiotherapy for breast cancer via m6A demethylation of TLR4
- Phytochemicals of Roman chamomile: Antioxidant, anti-aging, and whitening activities of distillation residues
- Circadian gene Cry1 inhibits the tumorigenicity of hepatocellular carcinoma by the BAX/BCL2-mediated apoptosis pathway
- The TNFR-RIPK1/RIPK3 signalling pathway mediates the effect of lanthanum on necroptosis of nerve cells
- Longitudinal monitoring of autoantibody dynamics in patients with early-stage non-small-cell lung cancer undergoing surgery
- The potential role of rutin, a flavonoid, in the management of cancer through modulation of cell signaling pathways
- Construction of pectinase gene engineering microbe and its application in tobacco sheets
- Construction of a microbial abundance prognostic scoring model based on intratumoral microbial data for predicting the prognosis of lung squamous cell carcinoma
- Sepsis complicated by haemophagocytic lymphohistiocytosis triggered by methicillin-resistant Staphylococcus aureus and human herpesvirus 8 in an immunocompromised elderly patient: A case report
- Sarcopenia in liver transplantation: A comprehensive bibliometric study of current research trends and future directions
- Advances in cancer immunotherapy and future directions in personalized medicine
- Can coronavirus disease 2019 affect male fertility or cause spontaneous abortion? A two-sample Mendelian randomization analysis
- Heat stroke associated with novel leukaemia inhibitory factor receptor gene variant in a Chinese infant
- PSME2 exacerbates ulcerative colitis by disrupting intestinal barrier function and promoting autophagy-dependent inflammation
- Hyperosmolar hyperglycemic state with severe hypernatremia coexisting with central diabetes insipidus: A case report and literature review
- Efficacy and mechanism of escin in improving the tissue microenvironment of blood vessel walls via anti-inflammatory and anticoagulant effects: Implications for clinical practice
- Merkel cell carcinoma: Clinicopathological analysis of three patients and literature review
- Genetic variants in VWF exon 26 and their implications for type 1 Von Willebrand disease in a Saudi Arabian population
- Lipoxin A4 improves myocardial ischemia/reperfusion injury through the Notch1-Nrf2 signaling pathway
- High levels of EPHB2 expression predict a poor prognosis and promote tumor progression in endometrial cancer
- Knockdown of SHP-2 delays renal tubular epithelial cell injury in diabetic nephropathy by inhibiting NLRP3 inflammasome-mediated pyroptosis
- Exploring the toxicity mechanisms and detoxification methods of Rhizoma Paridis
- Concomitant gastric carcinoma and primary hepatic angiosarcoma in a patient: A case report
- YAP1 inhibition protects retinal vascular endothelial cells under high glucose by inhibiting autophagy
- Identification of secretory protein related biomarkers for primary biliary cholangitis based on machine learning and experimental validation
- Integrated genomic and clinical modeling for prognostic assessment of radiotherapy response in rectal neoplasms
- Stem cell-based approaches for glaucoma treatment: a mini review
- Bacteriophage titering by optical density means: KOTE assays
- Neutrophil-related signature characterizes immune landscape and predicts prognosis of esophageal squamous cell carcinoma
- Integrated bioinformatic analysis and machine learning strategies to identify new potential immune biomarkers for Alzheimer’s disease and their targeting prediction with geniposide
- TRIM21 accelerates ferroptosis in intervertebral disc degeneration by promoting SLC7A11 ubiquitination and degradation
- TRIM21 accelerates ferroptosis in intervertebral disc degeneration by promoting SLC7A11 ubiquitination and degradation
- Histone modification and non-coding RNAs in skin aging: emerging therapeutic avenues
- A multiplicative behavioral model of DNA replication initiation in cells
- Biogenic gold nanoparticles synthesized from Pergularia daemia leaves: a novel approach for nasopharyngeal carcinoma therapy
- Creutzfeldt-Jakob disease mimicking Hashimoto’s encephalopathy: steroid response followed by decline
- Impact of semaphorin, Sema3F, on the gene transcription and protein expression of CREB and its binding protein CREBBP in primary hippocampal neurons of rats
- Iron overloaded M0 macrophages regulate hematopoietic stem cell proliferation and senescence via the Nrf2/Keap1/HO-1 pathway
- Revisiting the link between NADPH oxidase p22phox C242T polymorphism and ischemic stroke risk: an updated meta-analysis
- Exercise training preferentially modulates α1D-adrenergic receptor expression in peripheral arteries of hypertensive rats
- Overexpression of HE4/WFDC2 gene in mice leads to keratitis and corneal opacity
- Tumoral calcinosis complicating CKD-MBD in hemodialysis: a case report
- Mechanism of KLF4 Inhibition of epithelial-mesenchymal transition in gastric cancer cells
- Dissecting the molecular mechanisms of T cell infiltration in psoriatic lesions via cell-cell communication and regulatory network analysis
- Circadian rhythm-based prognostic features predict immune infiltration and tumor microenvironment in molecular subtypes of hepatocellular carcinoma
- Ecology and Environmental Science
- Optimization and comparative study of Bacillus consortia for cellulolytic potential and cellulase enzyme activity
- The complete mitochondrial genome analysis of Haemaphysalis hystricis Supino, 1897 (Ixodida: Ixodidae) and its phylogenetic implications
- Epidemiological characteristics and risk factors analysis of multidrug-resistant tuberculosis among tuberculosis population in Huzhou City, Eastern China
- Indices of human impacts on landscapes: How do they reflect the proportions of natural habitats?
- Genetic analysis of the Siberian flying squirrel population in the northern Changbai Mountains, Northeast China: Insights into population status and conservation
- Diversity and environmental drivers of Suillus communities in Pinus sylvestris var. mongolica forests of Inner Mongolia
- Global assessment of the fate of nitrogen deposition in forest ecosystems: Insights from 15N tracer studies
- Fungal and bacterial pathogenic co-infections mainly lead to the assembly of microbial community in tobacco stems
- Influencing of coal industry related airborne particulate matter on ocular surface tear film injury and inflammatory factor expression in Sprague-Dawley rats
- Temperature-dependent development, predation, and life table of Sphaerophoria macrogaster (Thomson) (Diptera: Syrphidae) feeding on Myzus persicae (Sulzer) (Homoptera: Aphididae)
- Eleonora’s falcon trophic interactions with insects within its breeding range: A systematic review
- Agriculture
- Integrated analysis of transcriptome, sRNAome, and degradome involved in the drought-response of maize Zhengdan958
- Variation in flower frost tolerance among seven apple cultivars and transcriptome response patterns in two contrastingly frost-tolerant selected cultivars
- Heritability of durable resistance to stripe rust in bread wheat (Triticum aestivum L.)
- Molecular mechanism of follicular development in laying hens based on the regulation of water metabolism
- Molecular identification and control studies on Coridius sp. (Hemiptera: Dinidoridae) in Al-Khamra, south of Jeddah, Saudi Arabia
- 10.1515/biol-2025-1218
- Animal Science
- Effect of sex ratio on the life history traits of an important invasive species, Spodoptera frugiperda
- Plant Sciences
- Hairpin in a haystack: In silico identification and characterization of plant-conserved microRNA in Rafflesiaceae
- Widely targeted metabolomics of different tissues in Rubus corchorifolius
- The complete chloroplast genome of Gerbera piloselloides (L.) Cass., 1820 (Carduoideae, Asteraceae) and its phylogenetic analysis
- Field trial to correlate mineral solubilization activity of Pseudomonas aeruginosa and biochemical content of groundnut plants
- Correlation analysis between semen routine parameters and sperm DNA fragmentation index in patients with semen non-liquefaction: A retrospective study
- Plasticity of the anatomical traits of Rhododendron L. (Ericaceae) leaves and its implications in adaptation to the plateau environment
- Effects of Piriformospora indica and arbuscular mycorrhizal fungus on growth and physiology of Moringa oleifera under low-temperature stress
- Effects of different sources of potassium fertiliser on yield, fruit quality and nutrient absorption in “Harward” kiwifruit (Actinidia deliciosa)
- Comparative efficiency and residue levels of spraying programs against powdery mildew in grape varieties
- The DREB7 transcription factor enhances salt tolerance in soybean plants under salt stress
- Using plant electrical signals of water hyacinth (Eichhornia crassipes) for water pollution monitoring
- Response of hybrid grapes (Vitis spp.) to two biotic stress factors and their seedlessness status
- Metabolomic profiling reveals systemic metabolic reprogramming in Alternaria alternata under salt stress
- Effects of mixed salinity and alkali stress on photosynthetic characteristics and PEPC gene expression of vegetable soybean seedlings
- Food Science
- Phytochemical analysis of Stachys iva: Discovering the optimal extract conditions and its bioactive compounds
- Review on role of honey in disease prevention and treatment through modulation of biological activities
- Computational analysis of polymorphic residues in maltose and maltotriose transporters of a wild Saccharomyces cerevisiae strain
- Optimization of phenolic compound extraction from Tunisian squash by-products: A sustainable approach for antioxidant and antibacterial applications
- Liupao tea aqueous extract alleviates dextran sulfate sodium-induced ulcerative colitis in rats by modulating the gut microbiota
- Toxicological qualities and detoxification trends of fruit by-products for valorization: A review
- Polyphenolic spectrum of cornelian cherry fruits and their health-promoting effect
- Optimizing the encapsulation of the refined extract of squash peels for functional food applications: A sustainable approach to reduce food waste
- Advancements in curcuminoid formulations: An update on bioavailability enhancement strategies curcuminoid bioavailability and formulations
- Impact of saline sprouting on antioxidant properties and bioactive compounds in chia seeds
- The dilemma of food genetics and improvement
- Causal effects of trace elements on congenital foot deformities and their subtypes: a Mendelian randomization study with gut microbiota mediation
- Honey meets acidity: a novel biopreservative approach against foodborne pathogens
- Bioengineering and Biotechnology
- Impact of hyaluronic acid-modified hafnium metalorganic frameworks containing rhynchophylline on Alzheimer’s disease
- Emerging patterns in nanoparticle-based therapeutic approaches for rheumatoid arthritis: A comprehensive bibliometric and visual analysis spanning two decades
- Application of CRISPR/Cas gene editing for infectious disease control in poultry
- Preparation of hafnium nitride-coated titanium implants by magnetron sputtering technology and evaluation of their antibacterial properties and biocompatibility
- Preparation and characterization of lemongrass oil nanoemulsion: Antimicrobial, antibiofilm, antioxidant, and anticancer activities
- Fluorescent detection of sialic acid–binding lectins using functionalized quantum dots in ELISA format
- Smart tectorigenin-loaded ZnO hydrogel nanocomposites for targeted wound healing: synthesis, characterization, and biological evaluation
- Corrigendum
- Corrigendum to “Utilization of convolutional neural networks to analyze microscopic images for high-throughput screening of mesenchymal stem cells”
- Corrigendum to “Effects of Ire1 gene on virulence and pathogenicity of Candida albicans”
- Retraction
- Retraction of “Down-regulation of miR-539 indicates poor prognosis in patients with pancreatic cancer”
Artikel in diesem Heft
- Safety assessment and modulation of hepatic CYP3A4 and UGT enzymes by Glycyrrhiza glabra aqueous extract in female Sprague–Dawley rats
- Adult-onset Still’s disease with hemophagocytic lymphohistiocytosis and minimal change disease
- Role of DZ2002 in reducing corneal graft rejection in rats by influencing Th17 activation via inhibition of the PI3K/AKT pathway and downregulation of TRAF1
- Biomedical Sciences
- Mechanism of triptolide regulating proliferation and apoptosis of hepatoma cells by inhibiting JAK/STAT pathway
- Maslinic acid improves mitochondrial function and inhibits oxidative stress and autophagy in human gastric smooth muscle cells
- Comparative analysis of inflammatory biomarkers for the diagnosis of neonatal sepsis: IL-6, IL-8, SAA, CRP, and PCT
- Post-pandemic insights on COVID-19 and premature ovarian insufficiency
- Proteome differences of dental stem cells between permanent and deciduous teeth by data-independent acquisition proteomics
- Optimizing a modified cetyltrimethylammonium bromide protocol for fungal DNA extraction: Insights from multilocus gene amplification
- Preliminary analysis of the role of small hepatitis B surface proteins mutations in the pathogenesis of occult hepatitis B infection via the endoplasmic reticulum stress-induced UPR-ERAD pathway
- Efficacy of alginate-coated gold nanoparticles against antibiotics-resistant Staphylococcus and Streptococcus pathogens of acne origins
- Battling COVID-19 leveraging nanobiotechnology: Gold and silver nanoparticle–B-escin conjugates as SARS-CoV-2 inhibitors
- Neurodegenerative diseases and neuroinflammation-induced apoptosis
- Impact of fracture fixation surgery on cognitive function and the gut microbiota in mice with a history of stroke
- COLEC10: A potential tumor suppressor and prognostic biomarker in hepatocellular carcinoma through modulation of EMT and PI3K-AKT pathways
- High-temperature requirement serine protease A2 inhibitor UCF-101 ameliorates damaged neurons in traumatic brain-injured rats by the AMPK/NF-κB pathway
- SIK1 inhibits IL-1β-stimulated cartilage apoptosis and inflammation in vitro through the CRTC2/CREB1 signaling
- Rutin–chitooligosaccharide complex: Comprehensive evaluation of its anti-inflammatory and analgesic properties in vitro and in vivo
- Knockdown of Aurora kinase B alleviates high glucose-triggered trophoblast cells damage and inflammation during gestational diabetes
- Calcium-sensing receptors promoted Homer1 expression and osteogenic differentiation in bone marrow mesenchymal stem cells
- ABI3BP can inhibit the proliferation, invasion, and epithelial–mesenchymal transition of non-small-cell lung cancer cells
- Changes in blood glucose and metabolism in hyperuricemia mice
- Rapid detection of the GJB2 c.235delC mutation based on CRISPR-Cas13a combined with lateral flow dipstick
- IL-11 promotes Ang II-induced autophagy inhibition and mitochondrial dysfunction in atrial fibroblasts
- Short-chain fatty acid attenuates intestinal inflammation by regulation of gut microbial composition in antibiotic-associated diarrhea
- Application of metagenomic next-generation sequencing in the diagnosis of pathogens in patients with diabetes complicated by community-acquired pneumonia
- NAT10 promotes radiotherapy resistance in non-small cell lung cancer by regulating KPNB1-mediated PD-L1 nuclear translocation
- Phytol-mixed micelles alleviate dexamethasone-induced osteoporosis in zebrafish: Activation of the MMP3–OPN–MAPK pathway-mediating bone remodeling
- Association between TGF-β1 and β-catenin expression in the vaginal wall of patients with pelvic organ prolapse
- Primary pleomorphic liposarcoma involving bilateral ovaries: Case report and literature review
- Effects of de novo donor-specific Class I and II antibodies on graft outcomes after liver transplantation: A pilot cohort study
- Sleep architecture in Alzheimer’s disease continuum: The deep sleep question
- Ephedra fragilis plant extract: A groundbreaking corrosion inhibitor for mild steel in acidic environments – electrochemical, EDX, DFT, and Monte Carlo studies
- Langerhans cell histiocytosis in an adult patient with upper jaw and pulmonary involvement: A case report
- Inhibition of mast cell activation by Jaranol-targeted Pirin ameliorates allergic responses in mouse allergic rhinitis
- Aeromonas veronii-induced septic arthritis of the hip in a child with acute lymphoblastic leukemia
- Clusterin activates the heat shock response via the PI3K/Akt pathway to protect cardiomyocytes from high-temperature-induced apoptosis
- Research progress on fecal microbiota transplantation in tumor prevention and treatment
- Low-pressure exposure influences the development of HAPE
- Stigmasterol alleviates endplate chondrocyte degeneration through inducing mitophagy by enhancing PINK1 mRNA acetylation via the ESR1/NAT10 axis
- AKAP12, mediated by transcription factor 21, inhibits cell proliferation, metastasis, and glycolysis in lung squamous cell carcinoma
- Association between PAX9 or MSX1 gene polymorphism and tooth agenesis risk: A meta-analysis
- A case of bloodstream infection caused by Neisseria gonorrhoeae
- Case of nasopharyngeal tuberculosis complicated with cervical lymph node and pulmonary tuberculosis
- p-Cymene inhibits pro-fibrotic and inflammatory mediators to prevent hepatic dysfunction
- GFPT2 promotes paclitaxel resistance in epithelial ovarian cancer cells via activating NF-κB signaling pathway
- Transfer RNA-derived fragment tRF-36 modulates varicose vein progression via human vascular smooth muscle cell Notch signaling
- RTA-408 attenuates the hepatic ischemia reperfusion injury in mice possibly by activating the Nrf2/HO-1 signaling pathway
- Decreased serum TIMP4 levels in patients with rheumatoid arthritis
- Sirt1 protects lupus nephritis by inhibiting the NLRP3 signaling pathway in human glomerular mesangial cells
- Sodium butyrate aids brain injury repair in neonatal rats
- Interaction of MTHFR polymorphism with PAX1 methylation in cervical cancer
- Convallatoxin inhibits proliferation and angiogenesis of glioma cells via regulating JAK/STAT3 pathway
- The effect of the PKR inhibitor, 2-aminopurine, on the replication of influenza A virus, and segment 8 mRNA splicing
- Effects of Ire1 gene on virulence and pathogenicity of Candida albicans
- Small cell lung cancer with small intestinal metastasis: Case report and literature review
- GRB14: A prognostic biomarker driving tumor progression in gastric cancer through the PI3K/AKT signaling pathway by interacting with COBLL1
- 15-Lipoxygenase-2 deficiency induces foam cell formation that can be restored by salidroside through the inhibition of arachidonic acid effects
- FTO alleviated the diabetic nephropathy progression by regulating the N6-methyladenosine levels of DACT1
- Clinical relevance of inflammatory markers in the evaluation of severity of ulcerative colitis: A retrospective study
- Zinc valproic acid complex promotes osteoblast differentiation and exhibits anti-osteoporotic potential
- Primary pulmonary synovial sarcoma in the bronchial cavity: A case report
- Metagenomic next-generation sequencing of alveolar lavage fluid improves the detection of pulmonary infection
- Uterine tumor resembling ovarian sex cord tumor with extensive rhabdoid differentiation: A case report
- Genomic analysis of a novel ST11(PR34365) Clostridioides difficile strain isolated from the human fecal of a CDI patient in Guizhou, China
- Effects of tiered cardiac rehabilitation on CRP, TNF-α, and physical endurance in older adults with coronary heart disease
- Changes in T-lymphocyte subpopulations in patients with colorectal cancer before and after acupoint catgut embedding acupuncture observation
- Modulating the tumor microenvironment: The role of traditional Chinese medicine in improving lung cancer treatment
- Alterations of metabolites related to microbiota–gut–brain axis in plasma of colon cancer, esophageal cancer, stomach cancer, and lung cancer patients
- Research on individualized drug sensitivity detection technology based on bio-3D printing technology for precision treatment of gastrointestinal stromal tumors
- CEBPB promotes ulcerative colitis-associated colorectal cancer by stimulating tumor growth and activating the NF-κB/STAT3 signaling pathway
- Oncolytic bacteria: A revolutionary approach to cancer therapy
- A de novo meningioma with rapid growth: A possible malignancy imposter?
- Diagnosis of secondary tuberculosis infection in an asymptomatic elderly with cancer using next-generation sequencing: Case report
- Hesperidin and its zinc(ii) complex enhance osteoblast differentiation and bone formation: In vitro and in vivo evaluations
- Research progress on the regulation of autophagy in cardiovascular diseases by chemokines
- Anti-arthritic, immunomodulatory, and inflammatory regulation by the benzimidazole derivative BMZ-AD: Insights from an FCA-induced rat model
- Immunoassay for pyruvate kinase M1/2 as an Alzheimer’s biomarker in CSF
- The role of HDAC11 in age-related hearing loss: Mechanisms and therapeutic implications
- Evaluation and application analysis of animal models of PIPNP based on data mining
- Therapeutic approaches for liver fibrosis/cirrhosis by targeting pyroptosis
- Fabrication of zinc oxide nanoparticles using Ruellia tuberosa leaf extract induces apoptosis through P53 and STAT3 signalling pathways in prostate cancer cells
- Haplo-hematopoietic stem cell transplantation and immunoradiotherapy for severe aplastic anemia complicated with nasopharyngeal carcinoma: A case report
- Modulation of the KEAP1-NRF2 pathway by Erianin: A novel approach to reduce psoriasiform inflammation and inflammatory signaling
- The expression of epidermal growth factor receptor 2 and its relationship with tumor-infiltrating lymphocytes and clinical pathological features in breast cancer patients
- Innovations in MALDI-TOF Mass Spectrometry: Bridging modern diagnostics and historical insights
- BAP1 complexes with YY1 and RBBP7 and its downstream targets in ccRCC cells
- Hypereosinophilic syndrome with elevated IgG4 and T-cell clonality: A report of two cases
- Electroacupuncture alleviates sciatic nerve injury in sciatica rats by regulating BDNF and NGF levels, myelin sheath degradation, and autophagy
- Polydatin prevents cholesterol gallstone formation by regulating cholesterol metabolism via PPAR-γ signaling
- RNF144A and RNF144B: Important molecules for health
- Analysis of the detection rate and related factors of thyroid nodules in the healthy population
- Artesunate inhibits hepatocellular carcinoma cell migration and invasion through OGA-mediated O-GlcNAcylation of ZEB1
- Endovascular management of post-pancreatectomy hemorrhage caused by a hepatic artery pseudoaneurysm: Case report and review of the literature
- Efficacy and safety of anti-PD-1/PD-L1 antibodies in patients with relapsed refractory diffuse large B-cell lymphoma: A meta-analysis
- SATB2 promotes humeral fracture healing in rats by activating the PI3K/AKT pathway
- Overexpression of the ferroptosis-related gene, NFS1, corresponds to gastric cancer growth and tumor immune infiltration
- Understanding risk factors and prognosis in diabetic foot ulcers
- Atractylenolide I alleviates the experimental allergic response in mice by suppressing TLR4/NF-kB/NLRP3 signalling
- FBXO31 inhibits the stemness characteristics of CD147 (+) melanoma stem cells
- Immune molecule diagnostics in colorectal cancer: CCL2 and CXCL11
- Inhibiting CXCR6 promotes senescence of activated hepatic stellate cells with limited proinflammatory SASP to attenuate hepatic fibrosis
- Cadmium toxicity, health risk and its remediation using low-cost biochar adsorbents
- Pulmonary cryptococcosis with headache as the first presentation: A case report
- Solitary pulmonary metastasis with cystic airspaces in colon cancer: A rare case report
- RUNX1 promotes denervation-induced muscle atrophy by activating the JUNB/NF-κB pathway and driving M1 macrophage polarization
- Morphometric analysis and immunobiological investigation of Indigofera oblongifolia on the infected lung with Plasmodium chabaudi
- The NuA4/TIP60 histone-modifying complex and Hr78 modulate the Lobe2 mutant eye phenotype
- Experimental study on salmon demineralized bone matrix loaded with recombinant human bone morphogenetic protein-2: In vitro and in vivo study
- A case of IgA nephropathy treated with a combination of telitacicept and half-dose glucocorticoids
- Analgesic and toxicological evaluation of cannabidiol-rich Moroccan Cannabis sativa L. (Khardala variety) extract: Evidence from an in vivo and in silico study
- Wound healing and signaling pathways
- Combination of immunotherapy and whole-brain radiotherapy on prognosis of patients with multiple brain metastases: A retrospective cohort study
- To explore the relationship between endometrial hyperemia and polycystic ovary syndrome
- Research progress on the impact of curcumin on immune responses in breast cancer
- Biogenic Cu/Ni nanotherapeutics from Descurainia sophia (L.) Webb ex Prantl seeds for the treatment of lung cancer
- Dapagliflozin attenuates atrial fibrosis via the HMGB1/RAGE pathway in atrial fibrillation rats
- Glycitein alleviates inflammation and apoptosis in keratinocytes via ROS-associated PI3K–Akt signalling pathway
- ADH5 inhibits proliferation but promotes EMT in non-small cell lung cancer cell through activating Smad2/Smad3
- Apoptotic efficacies of AgNPs formulated by Syzygium aromaticum leaf extract on 32D-FLT3-ITD human leukemia cell line with PI3K/AKT/mTOR signaling pathway
- Novel cuproptosis-related genes C1QBP and PFKP identified as prognostic and therapeutic targets in lung adenocarcinoma
- Bee venom promotes exosome secretion and alters miRNA cargo in T cells
- Treatment of pure red cell aplasia in a chronic kidney disease patient with roxadustat: A case report
- Comparative bioinformatics analysis of the Wnt pathway in breast cancer: Selection of novel biomarker panels associated with ER status
- Kynurenine facilitates renal cell carcinoma progression by suppressing M2 macrophage pyroptosis through inhibition of CASP1 cleavage
- RFX5 promotes the growth, motility, and inhibits apoptosis of gastric adenocarcinoma cells through the SIRT1/AMPK axis
- ALKBH5 exacerbates early cardiac damage after radiotherapy for breast cancer via m6A demethylation of TLR4
- Phytochemicals of Roman chamomile: Antioxidant, anti-aging, and whitening activities of distillation residues
- Circadian gene Cry1 inhibits the tumorigenicity of hepatocellular carcinoma by the BAX/BCL2-mediated apoptosis pathway
- The TNFR-RIPK1/RIPK3 signalling pathway mediates the effect of lanthanum on necroptosis of nerve cells
- Longitudinal monitoring of autoantibody dynamics in patients with early-stage non-small-cell lung cancer undergoing surgery
- The potential role of rutin, a flavonoid, in the management of cancer through modulation of cell signaling pathways
- Construction of pectinase gene engineering microbe and its application in tobacco sheets
- Construction of a microbial abundance prognostic scoring model based on intratumoral microbial data for predicting the prognosis of lung squamous cell carcinoma
- Sepsis complicated by haemophagocytic lymphohistiocytosis triggered by methicillin-resistant Staphylococcus aureus and human herpesvirus 8 in an immunocompromised elderly patient: A case report
- Sarcopenia in liver transplantation: A comprehensive bibliometric study of current research trends and future directions
- Advances in cancer immunotherapy and future directions in personalized medicine
- Can coronavirus disease 2019 affect male fertility or cause spontaneous abortion? A two-sample Mendelian randomization analysis
- Heat stroke associated with novel leukaemia inhibitory factor receptor gene variant in a Chinese infant
- PSME2 exacerbates ulcerative colitis by disrupting intestinal barrier function and promoting autophagy-dependent inflammation
- Hyperosmolar hyperglycemic state with severe hypernatremia coexisting with central diabetes insipidus: A case report and literature review
- Efficacy and mechanism of escin in improving the tissue microenvironment of blood vessel walls via anti-inflammatory and anticoagulant effects: Implications for clinical practice
- Merkel cell carcinoma: Clinicopathological analysis of three patients and literature review
- Genetic variants in VWF exon 26 and their implications for type 1 Von Willebrand disease in a Saudi Arabian population
- Lipoxin A4 improves myocardial ischemia/reperfusion injury through the Notch1-Nrf2 signaling pathway
- High levels of EPHB2 expression predict a poor prognosis and promote tumor progression in endometrial cancer
- Knockdown of SHP-2 delays renal tubular epithelial cell injury in diabetic nephropathy by inhibiting NLRP3 inflammasome-mediated pyroptosis
- Exploring the toxicity mechanisms and detoxification methods of Rhizoma Paridis
- Concomitant gastric carcinoma and primary hepatic angiosarcoma in a patient: A case report
- YAP1 inhibition protects retinal vascular endothelial cells under high glucose by inhibiting autophagy
- Identification of secretory protein related biomarkers for primary biliary cholangitis based on machine learning and experimental validation
- Integrated genomic and clinical modeling for prognostic assessment of radiotherapy response in rectal neoplasms
- Stem cell-based approaches for glaucoma treatment: a mini review
- Bacteriophage titering by optical density means: KOTE assays
- Neutrophil-related signature characterizes immune landscape and predicts prognosis of esophageal squamous cell carcinoma
- Integrated bioinformatic analysis and machine learning strategies to identify new potential immune biomarkers for Alzheimer’s disease and their targeting prediction with geniposide
- TRIM21 accelerates ferroptosis in intervertebral disc degeneration by promoting SLC7A11 ubiquitination and degradation
- TRIM21 accelerates ferroptosis in intervertebral disc degeneration by promoting SLC7A11 ubiquitination and degradation
- Histone modification and non-coding RNAs in skin aging: emerging therapeutic avenues
- A multiplicative behavioral model of DNA replication initiation in cells
- Biogenic gold nanoparticles synthesized from Pergularia daemia leaves: a novel approach for nasopharyngeal carcinoma therapy
- Creutzfeldt-Jakob disease mimicking Hashimoto’s encephalopathy: steroid response followed by decline
- Impact of semaphorin, Sema3F, on the gene transcription and protein expression of CREB and its binding protein CREBBP in primary hippocampal neurons of rats
- Iron overloaded M0 macrophages regulate hematopoietic stem cell proliferation and senescence via the Nrf2/Keap1/HO-1 pathway
- Revisiting the link between NADPH oxidase p22phox C242T polymorphism and ischemic stroke risk: an updated meta-analysis
- Exercise training preferentially modulates α1D-adrenergic receptor expression in peripheral arteries of hypertensive rats
- Overexpression of HE4/WFDC2 gene in mice leads to keratitis and corneal opacity
- Tumoral calcinosis complicating CKD-MBD in hemodialysis: a case report
- Mechanism of KLF4 Inhibition of epithelial-mesenchymal transition in gastric cancer cells
- Dissecting the molecular mechanisms of T cell infiltration in psoriatic lesions via cell-cell communication and regulatory network analysis
- Circadian rhythm-based prognostic features predict immune infiltration and tumor microenvironment in molecular subtypes of hepatocellular carcinoma
- Ecology and Environmental Science
- Optimization and comparative study of Bacillus consortia for cellulolytic potential and cellulase enzyme activity
- The complete mitochondrial genome analysis of Haemaphysalis hystricis Supino, 1897 (Ixodida: Ixodidae) and its phylogenetic implications
- Epidemiological characteristics and risk factors analysis of multidrug-resistant tuberculosis among tuberculosis population in Huzhou City, Eastern China
- Indices of human impacts on landscapes: How do they reflect the proportions of natural habitats?
- Genetic analysis of the Siberian flying squirrel population in the northern Changbai Mountains, Northeast China: Insights into population status and conservation
- Diversity and environmental drivers of Suillus communities in Pinus sylvestris var. mongolica forests of Inner Mongolia
- Global assessment of the fate of nitrogen deposition in forest ecosystems: Insights from 15N tracer studies
- Fungal and bacterial pathogenic co-infections mainly lead to the assembly of microbial community in tobacco stems
- Influencing of coal industry related airborne particulate matter on ocular surface tear film injury and inflammatory factor expression in Sprague-Dawley rats
- Temperature-dependent development, predation, and life table of Sphaerophoria macrogaster (Thomson) (Diptera: Syrphidae) feeding on Myzus persicae (Sulzer) (Homoptera: Aphididae)
- Eleonora’s falcon trophic interactions with insects within its breeding range: A systematic review
- Agriculture
- Integrated analysis of transcriptome, sRNAome, and degradome involved in the drought-response of maize Zhengdan958
- Variation in flower frost tolerance among seven apple cultivars and transcriptome response patterns in two contrastingly frost-tolerant selected cultivars
- Heritability of durable resistance to stripe rust in bread wheat (Triticum aestivum L.)
- Molecular mechanism of follicular development in laying hens based on the regulation of water metabolism
- Molecular identification and control studies on Coridius sp. (Hemiptera: Dinidoridae) in Al-Khamra, south of Jeddah, Saudi Arabia
- 10.1515/biol-2025-1218
- Animal Science
- Effect of sex ratio on the life history traits of an important invasive species, Spodoptera frugiperda
- Plant Sciences
- Hairpin in a haystack: In silico identification and characterization of plant-conserved microRNA in Rafflesiaceae
- Widely targeted metabolomics of different tissues in Rubus corchorifolius
- The complete chloroplast genome of Gerbera piloselloides (L.) Cass., 1820 (Carduoideae, Asteraceae) and its phylogenetic analysis
- Field trial to correlate mineral solubilization activity of Pseudomonas aeruginosa and biochemical content of groundnut plants
- Correlation analysis between semen routine parameters and sperm DNA fragmentation index in patients with semen non-liquefaction: A retrospective study
- Plasticity of the anatomical traits of Rhododendron L. (Ericaceae) leaves and its implications in adaptation to the plateau environment
- Effects of Piriformospora indica and arbuscular mycorrhizal fungus on growth and physiology of Moringa oleifera under low-temperature stress
- Effects of different sources of potassium fertiliser on yield, fruit quality and nutrient absorption in “Harward” kiwifruit (Actinidia deliciosa)
- Comparative efficiency and residue levels of spraying programs against powdery mildew in grape varieties
- The DREB7 transcription factor enhances salt tolerance in soybean plants under salt stress
- Using plant electrical signals of water hyacinth (Eichhornia crassipes) for water pollution monitoring
- Response of hybrid grapes (Vitis spp.) to two biotic stress factors and their seedlessness status
- Metabolomic profiling reveals systemic metabolic reprogramming in Alternaria alternata under salt stress
- Effects of mixed salinity and alkali stress on photosynthetic characteristics and PEPC gene expression of vegetable soybean seedlings
- Food Science
- Phytochemical analysis of Stachys iva: Discovering the optimal extract conditions and its bioactive compounds
- Review on role of honey in disease prevention and treatment through modulation of biological activities
- Computational analysis of polymorphic residues in maltose and maltotriose transporters of a wild Saccharomyces cerevisiae strain
- Optimization of phenolic compound extraction from Tunisian squash by-products: A sustainable approach for antioxidant and antibacterial applications
- Liupao tea aqueous extract alleviates dextran sulfate sodium-induced ulcerative colitis in rats by modulating the gut microbiota
- Toxicological qualities and detoxification trends of fruit by-products for valorization: A review
- Polyphenolic spectrum of cornelian cherry fruits and their health-promoting effect
- Optimizing the encapsulation of the refined extract of squash peels for functional food applications: A sustainable approach to reduce food waste
- Advancements in curcuminoid formulations: An update on bioavailability enhancement strategies curcuminoid bioavailability and formulations
- Impact of saline sprouting on antioxidant properties and bioactive compounds in chia seeds
- The dilemma of food genetics and improvement
- Causal effects of trace elements on congenital foot deformities and their subtypes: a Mendelian randomization study with gut microbiota mediation
- Honey meets acidity: a novel biopreservative approach against foodborne pathogens
- Bioengineering and Biotechnology
- Impact of hyaluronic acid-modified hafnium metalorganic frameworks containing rhynchophylline on Alzheimer’s disease
- Emerging patterns in nanoparticle-based therapeutic approaches for rheumatoid arthritis: A comprehensive bibliometric and visual analysis spanning two decades
- Application of CRISPR/Cas gene editing for infectious disease control in poultry
- Preparation of hafnium nitride-coated titanium implants by magnetron sputtering technology and evaluation of their antibacterial properties and biocompatibility
- Preparation and characterization of lemongrass oil nanoemulsion: Antimicrobial, antibiofilm, antioxidant, and anticancer activities
- Fluorescent detection of sialic acid–binding lectins using functionalized quantum dots in ELISA format
- Smart tectorigenin-loaded ZnO hydrogel nanocomposites for targeted wound healing: synthesis, characterization, and biological evaluation
- Corrigendum
- Corrigendum to “Utilization of convolutional neural networks to analyze microscopic images for high-throughput screening of mesenchymal stem cells”
- Corrigendum to “Effects of Ire1 gene on virulence and pathogenicity of Candida albicans”
- Retraction
- Retraction of “Down-regulation of miR-539 indicates poor prognosis in patients with pancreatic cancer”