Advances in cancer immunotherapy and future directions in personalized medicine

Abstract
Cancer immunotherapy has revolutionized oncologic treatment by harnessing and reprogramming the immune system to target malignant cells. This review provides a comprehensive picture of modern approaches to immunotherapy-based treatment strategies, such as immune checkpoint inhibitors (ICIs), chimeric antigen receptor T cells, mRNA vaccines, and biomaterials-based platforms, with a focus on their translational value and application to precision medicine. Emerging insights into the tumor microenvironment, immune resistance mechanisms, and T-cell subpopulation dynamics (e.g., γδ T cells, exhausted CD8⁺ T cells) are analyzed to elucidate immunotherapy response variability. Biomaterials such as injectable scaffolds, nanogels, and artificial antigen-presenting cells enable localized and sustained immune modulation, improving delivery precision and therapeutic efficacy. Personalized approaches, including neoantigen vaccine development and artificial intelligence (AI)-assisted biomarker prediction, are rapidly advancing individualized treatment regimens. Clinical trials illustrate how combination strategies with ICIs, chemotherapy, and nanomedicine enhance patient survival. Despite challenges including immune-related adverse events, manufacturing complexity, and global access disparities, integration of AI and multi-omics platforms promises to optimize patient stratification and therapeutic outcomes. This evolving paradigm positions personalized immunotherapy at the forefront of future oncologic care.
Graphical abstract

1 Introduction
Immunotherapy is a type of cancer treatment that uses the body’s immune system to detect, attack, and eliminate cancer cells. Unlike chemotherapy or radiation, which directly attacks cancer cells, immunotherapy works by boosting the body’s natural immune system to fight the cancer. Cancer immunotherapy (CIT) includes various strategies such as monoclonal antibodies, immune checkpoint inhibitors (ICIs), cancer vaccines, and adoptive cell therapies like chimeric antigen receptor (CAR) T cells, all aimed at counteracting the tumor’s ability to evade immune detection [1,2,3]. The immune system is vital for health because it identifies and destroys defective cells within the body. However, various strategies employed by cancer cells for escape include giving out signals that suppress the immune system or building an environment that suppresses the immune system. Immunotherapy seeks to overcome these drawbacks and, therefore, is a revolutionary treatment method in oncology [4].
One of the most successful immunotherapeutic strategies involves checkpoint inhibition. Molecules like programmed death-1 (PD-1) and cytotoxic T lymphocyte-associated antigen 4 (CTLA-4) normally act as brakes to prevent overactivation of the immune system [5,6]. These inhibitors have proved useful in the treatment of metastatic melanoma, lung cancer, and other cancers. As an example, pembrolizumab and nivolumab have manifested higher survival in patients with previously incurable cancers [7]. CIT is mainly designed to boost the activity of cytotoxic T cells (HLA class I), rather than helper T cells (HLA class II). However, recent studies show that CD4+ helper T cells also play a crucial role in fighting tumors [8]. It has functional versatility, which makes these cells develop into subgroups, including Th1, Th2, Th17, and regulatory T cells (Tregs) [9]. On the level of Th1, it stimulates cytotoxic activity and secretion of interferon-gamma to improve anti-tumor effects [10], while Tregs may diminish immune response and form an immunosuppressive environment within the tumor [11]. This bivalency situates CD4+ T cells as an attractive therapeutic avenue in next-generation immunotherapies [12].
Another strength of immunotherapy lies in its selectivity – it typically targets cancerous cells while sparing healthy tissues. Targeted therapies include endocrine therapy, molecular targeted therapy, and monoclonal antibodies like trastuzumab for human epidermal growth factor receptor 2 (HER2) positive breast cancer [13,14]. Likewise, bispecific antibodies bind to cancer cells and immune effector cells, enhancing immunosuppressive activity against tumor [15,16,17]. Another factor that makes immunotherapy a potential therapy for cancer and other diseases is its synergistic potential with other therapies. The use of immunotherapy in combination with either chemotherapy [18,19] or radiation boosts the general effectiveness as cancer is treated through multiple approaches. For instance, the integration of radiation therapy with immunotherapy enhances the destruction of tumor cells and diminishes the immune system’s ability to shield the tumor from destruction [20,21]. Furthermore, research has surveyed approaches for improving the concordance of these pairs in order to boost the efficacy of the interventions [22,23]. These combination strategies have been found to prevent the failure of single-agent therapies and enhance the survival of patients with recalcitrant cancers [24].
Among emerging modalities, CAR T-cell therapy involves genetically engineering a patient’s T cells to target specific cancer antigens and has shown remarkable efficacy in hematologic malignancies like leukemia and lymphoma [25,26]. In the same way, oncolytic anti-tumor selective viruses are being genetically developed to destroy cancer cells and trigger immunity [27,28,29]. New investigations also point to the synergism of CAR T therapy and oncolytic virotherapy to enhance efficient treatment strategies [30,31].
To improve efficacy and reduce systemic toxicity, localized delivery of immunotherapies is gaining attention. Interventional radiology allows the local administration of immunomodulators to malignant neoplasms. They have given encouraging outcomes in early trials and are expected in carcinomas that are unresponsive to systemic treatments [32,33,34]. Advancements like hydrogel delivery systems and implantable scaffolds supplement the idea of localized immunotherapy by providing long-term release and action [35,36]. These techniques are growing progressively to overcome impediments resulting from resistant tumors, offering new avenues to curing the disease [37,38].
Immunotherapy, on the other hand, has been more successful in recent years despite certain difficulties. Challenges like immune-related side effects, drug resistance, as well as high costs are still major [39,40]. Also, deciding on the optimal dose and searching for biomarkers that would indicate patient response are two areas of interest for the treatment method. Nevertheless, all those complications make the future of immunotherapy look rather bright. Due to the continuous scientific activities, new ways and techniques will be developed, such as personalized immunotherapy and other new cellular therapies, and global patients’ prognosis will be better and have an increased number of treatments. The change that immunotherapy has brought means that this type of treatment will be central to cancer treatment in the future.
Given the rapid evolution of immunotherapy and its transformative impact on cancer treatment, there is a need to consolidate current knowledge and identify future directions. This review presents both established and emerging immunotherapy strategies – including ICIs, CAR T-cells, and mRNA-based cancer vaccines – while also addressing delivery platforms, artificial intelligence (AI)-assisted modeling, and resistance in the tumor microenvironment (TME). Emphasis is placed on clinical translation and predictive approaches to ensure immunotherapy remains central to modern oncology.
2 Overview of the TME
2.1 Immune cycle and its four stages in tumor immunity
Immunotherapy is a therapeutic approach to intervene in the body’s immune system with the help of modulators or drugs, which mainly stimulate the body’s immune response to kill cancer cells during the treatment process [41]. The immune cycle in tumor immunity can be broadly divided into four interconnected stages: pre-phase (early stage), mid-phase, mid-late phase, and late phase. These stages collectively describe the process by which the immune system identifies, targets, and eliminates cancer cells. Each phase has distinct events that contribute to the overall anti-tumor immune response, forming the basis for many modern immunotherapies.
During the pre-phase (early phase), tumor antigens are shed off by cancer cells due to either apoptosis or necrosis. These antigen presenting cells (APCs), namely, the dendritic cells (DCs), which then digest them and present them by the Major Histocompatibility Complex (MHC) on the surface of the naive T cells, despite the fact that a T-cell receptor (TCR) with an antigen-MHC, special signals are needed for the activation of the T-cells. This is the foundational step targeted by cancer vaccines and ICIs to enhance T-cell priming and antigen recognition [42]. The mid-phase involves the trafficking of activated T cells toward the TME. This is facilitated under the direction of chemokine gradients, for instance, in CXCL9 and CXCL10. When in the TME, T cells lodge in the endothelium and bind to the cancer cell and recognize tumor antigens presented on the latter through MHC molecules. The engagement of TCRs on T cells with neoantigenic complexes guarantees the selective destruction of cancerous cells. Cytotoxic T cells then induce the apoptosis of cancer cells through such actions as granzyme and perforin-mediated activities. This stage emphasizes the need to traffic T-cells into the tumor; this aspect is helped by some immunotherapies such as ICIs (anti-PD-1, anti-CTLA-4), engineered CAR T cell therapies expressing CXCR3, VEGF inhibitors that normalize tumor vasculature, and chemokine-modulating therapies like nanomaterials enhancing CXCL9 expression. These approaches have been shown to improve T-cell infiltration and enhance anti-tumor immunity [43,44].
During the mid-late phase, the cycle becomes endogenous; that is, the elements that constitute the cycle become continuous and independent. Immune mediated death of tumor cells releases more tumor antigens into the TME as a result of the anti-tumor immune response. Again, these antigens are picked up by the APCs, which boost the immune response by attracting more and more effector T cells. However, this phase is also accompanied by immunosuppressive mechanisms, including the use of Tregs and myeloid derived suppressor cells (MDSCs). In the last period, the immune response against cancer cells is initiated and continued vigorously. Memory T cells generated in earlier stages play a pivotal role in maintaining long-term immune surveillance. These cells maintain the specificity of the primary immune response and are quickly responsive in case of tumor recurrence. Sustained tumor antigen release and continued effector T cell activation result in persistent anti-tumor immunity. Figure 1 displays this cancer immunity cycle and essential steps through which T cells mediate anti-tumor responses.
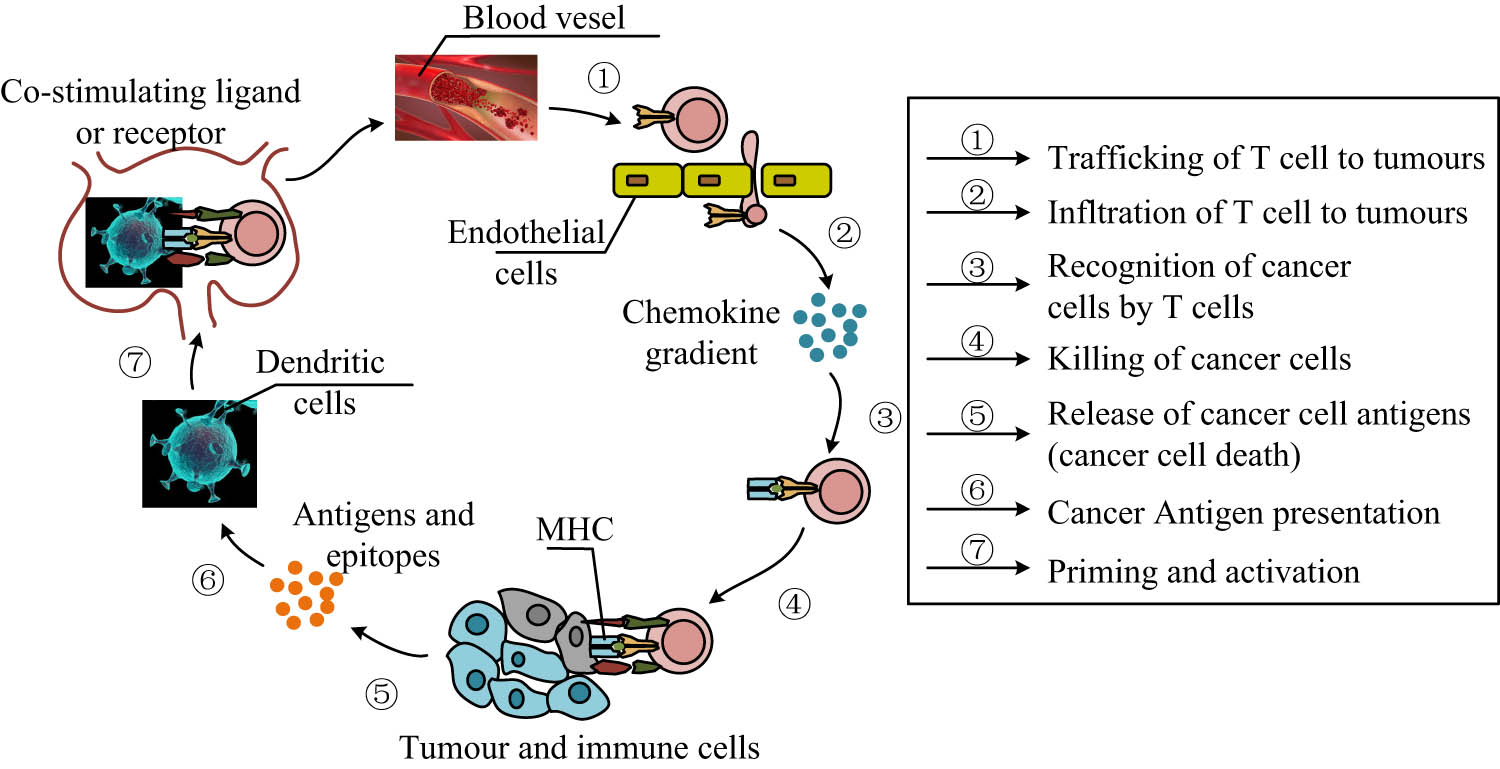
Cancer-immunity cycle depicting the essential steps through which T cells mediate anti-tumor responses. The process begins with the trafficking of T cells to tumor sites via the bloodstream (Step 1), guided by chemokine gradients that facilitate their infiltration into the TME (Step 2). Upon arrival, T cells recognize tumor cells through specific interactions with antigen-MHC complexes (Step 3), leading to the targeted killing of cancer cells (Step 4). This cytotoxic activity results in the release of tumor-associated antigens (Step 5), which are subsequently captured and processed by DCs (Step 6). These APCs prime and activate naive T cells by presenting tumor antigens via MHC molecules and delivering co-stimulatory signals (Step 7), thus initiating a new cycle of immune activation.
2.2 Molecular mechanisms of immune therapy resistance
Immunotherapy has revolutionized cancer care by attacking tumors using both cellular and molecular immune responses, and the TME has emerged as an important target of therapeutic response [45]. However, resistance mechanisms, both intrinsic and extrinsic, remain a significant challenge [46]. Tumors can release suppressor cytokines or metabolites and recruit immunosuppressive cells like Tregs and N2 neutrophils. Consequently, treatments such as ICIs also affect cytokine signaling, which can be overcome by tumor-related immune escape [47]. Some of the key resistance mechanisms, as demonstrated in Figure 2, include the MDSC influence on the release of factors such as reactive nitroxide intermediates, ARG1, and interleukin 10, an action which inhibits T-cell activation and prevents the tumor cells from immune mediated cell death [48]. Similarly, Tregs and signaling molecules like TGF-β enhance immune suppression by modulating signaling pathways, including the Programmed death-ligand 1 (PD-L1) pathway, contributing to a highly immunosuppressive TME [49].

Illustration of the immunosuppressive mechanisms within the TME that contribute to immune evasion and resistance to immunotherapy. MDSCs release a variety of suppressive molecules – including reactive nitroxide intermediates, arginase-1 (ARG1), IL-10, PRG2, TGF-α, and TGF-β – that inhibit T cell function and protect tumor cells from TNF-α-induced cell death. Simultaneously, N1 neutrophils, under the influence of TGF-β and associated signaling pathways, contribute to immune response inhibition. Regulatory T cells (Tregs) further suppress cytotoxic T cell activity by engaging immune checkpoints and altering signaling pathways such as PD-L1, which is often overexpressed on tumor cells to evade immune destruction.
Research by Leko and Rosenberg identified different types of tumor antigen recognition mediated by T lymphocytes and explored their clinical safety and efficacy in targeted immunotherapy [50]. Their results imply that enhancing access to antigenic therapy may increase the therapeutic capacity of immunotherapy in cancer patients. Additionally, Zhao et al. demonstrated that activating ferritin decarboxylase could reduce drug resistance in conventional cancer therapy by regulating metabolic pathways and signaling involving iron desiccation [51].
Despite these advancements, resistance remains a significant limitation. For instance, intratumoral heterogeneity and poor immunogenicity in cancers like glioblastoma hinder the success of immunotherapeutic strategies. Murciano-Goroff et al. proposed that overcoming resistance requires both direct tumor modifications and alterations to the TME [52]. Insufficient tumor antigen recognition, ICI modulation, and signaling pathway alterations also play critical roles, as discussed by Bashash et al. [53].
2.3 Immunotherapeutic strategies under different treatments
2.3.1 Biomaterials based immunotherapy
Biomaterials based immunotherapy entails the association of fabricated materials aimed at boosting the immune system of the body against diseases, especially cancer. This approach is expected to enhance the effectiveness, selectivity, and safety of immunotherapies by employing biomaterials to deliver and release immunotherapy cargoes and to regulate immune responses [54,55,56].
2.3.2 Implantable and injectable scaffolds for immunotherapy
Implantable and injectable biomaterial scaffolds provide favorable environment on a micro scale for the activation and proliferation of immune cells [57]. For instance, implantable scaffolds have been used to introduce DC-activating agents, making it possible to activate immune reactions in situ [58]. Furthermore, these scaffolds may be used for the controlled release of immunomodulatory agents per se that engage and stimulate immune cells onsite inside tumors. These implantable biomaterials also have specific release characteristics or kinetic profiles in order to sustain the therapeutic impact. New developments have investigated the incorporation of 3D printing and biotic materials in order to improve the structural and functional properties of such support structures [59].
Injectable scaffolds provide a more minimally invasive method of delivering immunotherapy. These can be prepared as hydrogels or microparticles and can be directly implanted into the desired site for drug delivery, where the system, upon implantation, undergoes self-assembly or gelation to form a reservoir for the drug. In particular, injectable biomaterials have been proven to be practical for metastatic cancers and for regions that are difficult to operate on. In this way, they can secrete cytokines or ICIs to remodulate the immune context of tumors [60]. However, the injectable scaffolds can be administered with any concentration and can easily accommodate combination therapy. Research has shown their potential in the delivery of multiple agents, including tumor antigens and adjuvants to boost immunity [56].
Both implantable and injectable scaffolds have a similar benefit of targeted delivery, therefore reducing toxicity associated with systemic exposure. It is possible to design such systems to only respond to certain biological signals, thus enabling the delivery of therapeutic agents to occur based on changes within the microenvironment. Combined application of these scaffolds with other treatment strategies, including ICIs or CAR T cell therapy, is a relatively new trend that has the potential to provide enhanced and individualized immunotherapies [37].
2.3.3 Nanoparticle-based delivery systems
Immunotherapeutic agents are delivered through nanoparticles to target specific immune cells or tumor sites. Liposomes and polymersomes as synthetic nanoparticles can be designed and coated with tumor antigens or immune modulating agents to give high immune response signals. Also, the use of biologically derived nanocarriers such as extracellular vesicles has been considered owing to their inherent biocompatibility and immune-associated functions [61]. Nanoparticles act to encapsulate immunotherapeutic agents, including antigens, adjuvants, or immune modulators, in order to enhance their stability and have slow-release properties. For example, nanoparticulate based vaccination offers more efficient antigen deposition and presentation, with resultant improvement in immune response in cancer immunotherapies [62]. In addition, lipid based nanoparticles, gold nanorods, and mesoporous silica nanoparticles have also been used for enhancing the DC uptake, which is crucial for the activation of the immune system [63].
Furthermore, in recent years, nanocarrier-based biomedicine has made significant progress in cancer therapy. Ma et al. analyzed the research progress of nanogels applied to immunotherapy, including gel-mediated immunomodulatory drugs, antibodies, vaccines, and CAR T cell therapy [64]. This study concluded that nanogels had better application potential for immunotherapy. As a three-dimensional crosslinked aqueous material, nanogels are structurally stable, have a large specific surface area, and can better target particular immune cell subpopulations or immunological organs, which boosts the drug’s bioavailability. Additionally, fewer adverse events are produced by its slower release impact. Zhang and Pu proposed to combine fusion nanomedicines with immunotherapy and discussed tumor immunotherapy under molecular and nanoengineering approaches [65]. This study concluded that activatable nano-formulations could produce immunotherapeutic effects on TME under internal and external stimuli and reduce the incidence of immune-related adverse events. Xu et al. prepared a personalized nano vaccine based on a cationic fluoropolymer and achieved control of melanoma with the help of a Toll-like receptor 4 mediated signaling pathway [66]. The results showed that this method could better inhibit tumor recurrence and metastasis after surgery.
Another notable application involves using nanoparticles to overcome resistance in the TME. As an example, nanomedicines that target tumor-associated macrophages or other immune-suppressive cells have demonstrated efficacy in augmenting therapeutic efficacy in drug-resistant tumors [67]. Moreover, the controlled and local delivery of immune-stimulating agents can be achieved using polymer-derived nano and microparticle carriers [68]. The adaptability of nanoparticle-based systems allows for the integration of multiple therapeutic functionalities. They can administer drugs and immune stimulants either simultaneously or sequentially so as to capitalize on the synergies. As an example, paclitaxel combined with engineered nanoparticles has been utilized as carriers that may also alter immune response as a cancer therapy strategy [69].
2.3.4 Modulation of the TME
Implanted biomaterials can be bioengineered in a way to modulate the TME and encourage immune cell infiltration and effectiveness. For instance, biomaterials that let out oxygen counter tumor hypoxia, which tends to dampen the immune response. Other strategies include delivering agents that are capable of breaking down the surrounding matrix and thus increasing immunological access [70]. Based on their findings, Martin et al. asserted that TME acts as a barrier to the release of drugs and thus negatively affects the effectiveness of nanomedicine and immunotherapy, which may lead to increased drug toxicity and adverse events in malignant tumors [71].
2.3.5 Artificial antigen presenting cells (aAPCs)
aAPCs are artificial systems designed to resemble the natural APCs to activate T cells ex vivo or in vivo. The construction of aAPCs includes the use of biodegradable materials or nanoparticles, which are functionalized with signals that are critical in the activation of T cells. These include the display of ligands both in MHCs and co-stimulatory molecules that make sure that there is a firm T-cell activation. For example, the use of nanoellipsoidal aAPCs demonstrated much potential for antigen specific T-cell activation due to a large surface area for contact [72]. The effectiveness of aAPCs can also depend on how they have been designed. Some investigations gave evidence that the shape of the particle and its material affect the activation of T-cells at supra-physiological levels. For example, ellipsoidal nanoparticles and lipid based aAPCs hold the biological model of natural APCs to provide signals [73]. Another example is structured cell-sized lipid vesicles with protein coupled bilayer layers showing antigen-specific T-cell stimulation [74].
Furthermore, aAPCs possess antigen presentation versatility for multiple immunotherapeutic uses, such as adoptive cell transfer. By altering these design parameters, including the antigen density and co-stimulatory molecules, they can improve T-cell proliferation and activation prior to the therapeutic delivery. These systems have a particular potential to avoid the drawbacks inherent to natural APCs, such as interferences with immune reactions and scarcity of supply. The possibilities of aAPC are not only limited to identifying the immune targets in CIT but also to overcoming immune issues. Particle-based aAPCs have been developed to overcome the immunosuppressive TME by activating tumor reactive T-cells [75].
2.3.6 Bioinstructive materials
Bioconductive materials are designed for specific cellular responses such as differentiation, proliferation, and migration. For instance, synthetic materials that were produced to specify certain pore sizes were used in works that illustrated that mesenchymal stem cell differentiation is affected by the structure of materials [76]. Likewise, electrospun nanofibers function as scaffolds that can control differentiation through Mechanotransduction pathways in musculoskeletal, vascular, as well as immune systems [77]. Bioinstructive materials also require the ability to influence the immune system response. For example, immune-instructive biomaterials are under development for improving the foreign body response and tissue integration and functioning of implants, maintaining immunological tolerance [78]. These materials apply chemical and physical features to modulate the activities of immune cells so as to initiate or inhibit immune response.
Recent advancements in technology, for instance, High-Throughput Screening technology, help scientists find efficient bioinstructive materials for particular usage. Screening techniques based on gradient profiling have been especially successful in the context of cell-biomaterial interactions and specific control of cell behavior, including proliferation and differentiation [79]. Bioinstructive scaffolds have been applied to develop an environment for therapeutic cell production in situ. For instance, implantable scaffolds have been developed to synthesize and deliver CAR T-cells within the body, thereby synchronizing immunity across different types of complex cell therapy techniques [80]. These innovations emphasize the possibilities of bioinstructive materials in improving the outcome of act T therapies. This field is already transitioning to dual-mode applications where implants provide both structural support and deliver bioactive cues in conjunction with other forms of treatment, including drug delivery and gene modification. For example, bioinstructive hydrogels have been designed to create pronto environments for implantation as well as enhanced tissue healing [81]. Table 1 summarizes current innovations in biomaterial-based platforms such as injectable scaffolds and hydrogels, highlighting their composition, mechanism of action, and tumor-specific applications.
Innovative biomaterial platforms for CIT
| Category | Biomaterial type | Example | Tumor type/application | References |
|---|---|---|---|---|
| Injectable scaffolds | Nano-vaccine in hydrogel (NvIH) | NvIH hydrogel with ICB antibodies and polymeric nanoparticles activating TLR7/8/9 and STING | Glioblastoma and poorly immunogenic tumors | [82] |
| Injectable scaffolds | L-Norvaline-based hydrogel | Hydrogel blocking ARG1 pathway for T-cell reactivation and combination immunotherapy | Primary tumors, abscopal tumors, pulmonary metastasis | [83] |
| Injectable scaffolds | PEI-based immunotherapeutic hydrogel (PEIGel) | PEIGel hydrogel with polyvinyl alcohol, polyethylenimine, and magnesium ions to upregulate PD-L1 and M1 macrophages | Breast cancer, tumor relapse prevention | [84] |
| Injectable scaffolds | Sodium alginate-based | Injectable sodium alginate hydrogel for deep tumor penetration and personalized vaccines | Colorectal cancer | [85] |
| Injectable scaffolds | Supramolecular hydrogel for in situ CAR T reprogramming | Hydrogel loaded with plasmid CAR (pCAR) with CD2 promoter for enhanced CAR T therapy | Solid tumors (Humanized mice models) | [86] |
| Injectable scaffolds | Silk fibroin (SF) microsphere-based vaccine | Macroporous SF microsphere loaded with antigens and adjuvants for single-dose cancer vaccination | General solid tumors | [87] |
| Injectable scaffolds | Super-soft DNA hydrogel depot | Injectable DNA hydrogel with ATP aptamers for sequential doxorubicin, CpG ODN, and aPDL1 release | General solid tumors | [88] |
| Cancer vaccine hydrogels | Nucleic acid-based hydrogel vaccine | Three-in-One hydrogel with CpG, SN38, and PD-L1 siRNA for immune activation | Melanoma (Murine model) | [89] |
| Cancer vaccine nanocomposites | Oxidized bacterial cellulose/thrombin/gold nanocomposites (AuNCs) | Nanocomposite with αPD-1@AuNCs for pyroptosis-inducing photothermal and ICI therapy | Postoperative head and neck squamous cell carcinoma (HNSCC) | [90] |
| Cancer vaccine hydrogels | Bio-responsive cargo-catchable gel depot | Pullulan/chitosan hydrogel for doxorubicin and aPDL1 co-delivery to prevent tumor recurrence | Post-surgical breast cancer (4T1 Mouse model) | [91] |
2.4 Immunotherapy in cancer management
Immunotherapies ranging from ICI blockade to cellular therapeutic vaccines have changed the paradigm of tumor treatment. Among them, T-cell antigen specificity has been shown to have a link to tumor phenotype. The utilization of T-cell subsets is discussed to be important for elucidating the anti-tumor cellular mechanisms of immunotherapy and guiding treatment regimens [92]. T-cell serves as the most potent effector cells in the anti-tumor immune response. In current CIT, T-cells are mainly used to achieve interventions from both ICIs and overt cell therapy. Chow et al. analyzed the immunobiology of T-cell exhaustion and noted its correlation with tumor control. They emphasized that targeting exhaustion pathways could significantly enhance immunotherapy efficacy [93]. T-cell-based immunotherapy has become an effective therapeutic strategy for anti-tumor therapy in addition to surgery, chemotherapy, and radiotherapy. Based on the differences in cell receptor expression, T-cells can be classified into two subpopulations, αβ T and γδ T. Mensurado et al. concluded that current αβ T-C are more dependent on MHC-mediated and neoantigen expression, which limits their applicability. In contrast, γδ T-C were less dependent on neoantigen loading and MHC antigens due to their unique tissue orientation, allowing them to have better anti-tumor activity. The study of γδ T-cell subsets could provide a reference value for cancer prognostic intervention and therapeutic strategy development [94]. Figure 3 shows the regulatory mechanism of tumor-promoting γδ T-C.

Regulatory mechanism of tumor promoting gamma delta T-C. IL-17 production, driven by ITCH and NOS2 signaling, promotes inflammation and tumor growth. Amphiregulin and IL-4 further enhance cancer cell survival. Conversely, ROS from DCs and galectin signaling can inhibit IL-17 production.
Natural Killer (NK) cells resemble a significant part of the innate immune system and can recognize and kill tumor cells. Recent literature has isolated certain NK cell subsets, including RAC1 high NK cells, which exhibit augmented tumor killing abilities in hepatocellular carcinoma (HCC) via regulating the STAT3-NKG2D axis [95]. Single-cell sequencing has advanced the understanding of the tumor immune microenvironment (TiME), revealing distinct immune subpopulations. As an example, T-cell, B-cell, and myeloid secondary clustering have been used to make predictions regarding the responsiveness of melanoma to immunotherapy [96]. These insights enable the development of therapies targeting immune subpopulations critical to anti-tumor immunity. In colorectal cancer, subpopulations of high immune infiltration defined by the peroxisome pathway and TIM3 expression are associated with better immunotherapies. This illustrates the role of understanding individual immune parameters in informing patient-specific therapeutic approaches [97]. Terminally exhausted T-cells, marked by TOX and PD-1 expression, present challenges in solid tumors. Blocking PD-1 and TIGIT in a co-blockade approach has been demonstrated to renew these exhausted cells, increasing their anti-tumor capacity in bladder cancer [98]. DCs are pivotal for initiating adaptive immunity. The heterogeneity of monocyte-derived and type-2 conventional DCs has been shown in single-cell analysis, underscoring their value in custom applications in immunotherapy [99]. Subpopulation-based approaches also address limitations in CAR T-cell therapy. Using omics technologies to analyze the tumor immune microenvironment, scientists are finding ways to boost the effectiveness of CAR T-cells in non-T-cell-inflamed tumors [100]. In glioblastoma, stromal subpopulations, such as perivascular fibroblasts, have been identified as predictors of immunotherapy resistance. It is noteworthy that this observation highlights the significance of addressing both immune cells and stromal subpopulations to maximize treatment effects [101].
A discussion of CAR T-cells vs bispecific antibodies presents varying efficacy, toxicity, and cost profiles (Table 2). CAR T has shown maximum efficiency in hematological malignancies but is fraught with cytokine release syndrome (CRS) and neurotoxicity, excessive costs, and production delays. Moreover, unlike monoclonal antibodies, bispecific antibodies like blinatumomab are enabled in the form of an off-the-shelf product, at lower cost and higher access, especially through a community-based model. However, they generally have lower persistence and moderate efficacy compared to CAR T [102].
Comparative evaluation of CAR T-cells and bispecific antibodies
| Parameter | CAR T-cell therapy | Bispecific antibodies (BsAbs) | References |
|---|---|---|---|
| Efficacy | High response rates in relapsed/refractory hematologic malignancies; durable remissions in Large B-Cell Lymphoma and Multiple Myeloma; Overall Response Rate (ORR) >50% in many trials | Rapid response onset; effective in hematologic cancers; responses less durable compared to CAR-T | [103,104] |
| Toxicity | High: CRS, neurotoxicity; requires inpatient care and close monitoring | Lower: lower-grade CRS and neurotoxicity; more manageable in outpatient settings | [105,106] |
| Cost (per patient) | Estimated ∼$375,000–$475,000 (not including hospitalization, supportive care); highest upfront cost | Estimated ∼$180,000–$250,000; generally lower than CAR T but cumulative costs increase with long-term use | [107,108] |
| Turnaround time | 2–3 weeks for cell engineering; logistical complexity due to autologous manufacturing | Off-the-shelf, immediate availability | [109,110] |
| Ideal use case | Curative intent in fit, relapsed/refractory patients; aggressive or resistant cancers | Bridge to CAR T or alternative for less fit patients, outpatient settings | [106,111] |
2.5 Immune checkpoint-based immunotherapy
Approved in 2011, the first generation of ICIs targets tumor cells by interfering with the inhibitory signals that the tumor cells send to immune effector cells. Its immunostimulatory properties may lead to the occurrence of associated adverse reactions and damage to organ systems. Chhabra and Kennedy concluded that there was a need for greater multidisciplinary coordination in responding to the management of adverse reactions to achieve individualized protocol development for the patient’s therapeutic goals [112]. Figure 4 shows the structure of PD-1 and PD-L1.

Mechanism of immune checkpoint inhibition targeting the PD-1/PD-L1 axis in CIT. On the left, tumor cells express PD-L1, which binds to PD-1 receptors on activated T cells, leading to suppression of T cell-mediated immune responses and allowing tumor cells to evade immune destruction. On the right, the administration of anti-PD-1 or anti-PD-L1 monoclonal antibodies blocks this interaction, thereby restoring T cell activity. This blockade enables T cells to recognize tumor antigens through the T cell receptor (TCR) and induce tumor cell apoptosis.
ICIs like PD-1/PD-L1 and CTLA-4 inhibitors have been particularly effective in improving survival outcomes in several cancers, including HCC, melanoma, and non-small cell lung cancer (NSCLC) [113,114,115]. In HCC, antibody-based ICIs enhance T-cell responses within TME, contributing to improved therapeutic efficacy. Figure 5 shows the role of trimethylation in regulating immune responses within the HCC TME.

Regulatory mechanism of trimethylation on the HCC TME. The EZH2-EED complex facilitates CXCL10 repression through histone trimethylation, suppressing NK cell migration. Upon treatment with an EZH2/EED inhibitor, CXCL10 expression is restored, leading to increased NK cell migration. However, HDAC12 can induce CXCL10 re-repression, maintaining a suppressive TME.
In cancer therapy, anti-tumor immune (anti-TI) effects can be enhanced through neoadjuvant ICI blockade methods. Topalian et al. suggested that research on checkpoint blockade responses and drug resistance markers holds potential for further development [116]. Koerner et al. discovered that double-stranded (ds) RNA adjuvants effectively activate DCs and increase tumor-specific CD8+ T-cell responses [117]. ICI blockade reactivates cytotoxic T lymphocyte (CTL) responses, and its combination with biodegradable polylactic acid-co-glycolic acid (PLGA) particles significantly improves immunotherapeutic efficacy.
Targeting emerging pathways like the IGSF8–NK receptor axis also offers promise. Disrupting these interactions, alone or with PD-1 antibodies, enhances cytotoxic function and T-cell signaling [118]. Despite their effectiveness, ICIs are associated with irAEs such as inflammation and organ toxicity. This is due to their multifaceted modulation of immune pathways [119]. Sharma et al. noted that resistance to ICIs is often tumor-type dependent, highlighting the importance of identifying predictive biomarkers to guide personalized treatment [120]. In gliomas, O6-methylguanine-DNA methyltransferase (MGMT) status has been associated with ICI resistance. Kinslow et al. reported a negative association between MGMT staining and primary brain tumor risk scores, suggesting its potential as a biomarker for ICI responsiveness in glioma [121]. Monoclonal ICIs prevent T-cell inactivation by blocking ICIs, effectively enhancing antigen recognition and cytotoxicity [122]. However, phenomena like hyperprogression and irAEs remain major barriers to broader application [123]. These therapies do this by rewriting the antigens of the immune system so that they can recognize the tumor.
Originally developed for oncology, ICIs are now being explored for other immune-regulated diseases like autoimmune disorders and atherosclerosis, where checkpoint modulation may regulate inflammation and plaque formation [124]. Recent research is also expanding ICI use beyond T-cells – investigating NK cells and single-cell transcriptomic profiling to reveal how checkpoint pathways affect diverse immune subsets [125,126]. This has helped inform combination therapies with small molecule inhibitors or radiotherapy that may enhance treatment efficacy while minimizing toxicity [127].
2.6 Combination immunotherapy
Combination immunotherapy represents a versatile and increasingly prominent strategy in cancer treatment, aiming to overcome limitations associated with single-agent therapies (Table 3). While many nanomedicines are in development, challenges persist – including over-activation of immune responses, increased immunogenicity, and drug resistance [128]. TME modulation strategies are particularly critical for enhancing immunotherapy outcomes. Traditional immunotherapeutic drugs often have a short retention time during administration, limiting their effectiveness. Yang et al. concluded that nanoparticle-based drug delivery systems can effectively penetrate the TME and release drugs with precision. These systems could also be combined with other therapeutic approaches, although careful control of TME changes at different stages remains key to designing personalized nano-application platforms in the future [129].
Summary of some combination immunotherapy strategies
| Strategy | Description | Examples | Benefits | Challenges | References |
|---|---|---|---|---|---|
| ICIs in combination | Combining ICIs targeting PD-1/PD-L1 and CTLA-4 pathways for synergistic effects | Nivolumab + Ipilimumab in metastatic melanoma | Enhanced tumor clearance and survival | Increased risk of immune-related adverse events (irAEs) | [130,131] |
| ICIs and targeted therapy | Combining ICIs with tyrosine kinase inhibitors to modulate the TME | PD-1 inhibitors with VEGF inhibitors in NSCLC | Synergistic immune activation | Managing complex dosing and cumulative toxicities | [132] |
| ICIs and adoptive cell therapies (ACTs) | Combining checkpoint blockade with CAR T-cells or TCR-engineered T cells | Anti-PD-1 + CAR T-cells for solid tumors | Prevents T cell exhaustion | Complexity of therapy design and delivery | [133] |
| Dual immune modulators | Targeting multiple immune pathways to enhance anti-tumor responses | IL-2 agonists with ICIs | Activates diverse immune populations | Increased systemic immune activation risks | [134] |
| ICIs and oncolytic viruses | Using viruses that selectively infect and kill cancer cells, combined with ICIs | T-VEC (Talimogene laherparepvec) with anti-PD-1 therapy | Increases tumor immunogenicity | Optimizing virus delivery and immune responses | [135] |
| ICIs and chemotherapy | Enhancing antigen presentation and immune activation through combined mechanisms | Anti-PD-L1 + platinum-based chemotherapy in lung cancer | Broader efficacy across cancers | Higher rates of irAEs and systemic toxicity | [136] |
PD-1 inhibitors such as pembrolizumab or atezolizumab, when combined with chemotherapy, have emerged as significant therapeutic strategies for non-immunogenic malignancies. This combination has demonstrated better clinical activity and increased the median progression-free survival of patients. However, uncertainties in the pathways activated by immunotherapy in breast cancer complicate its application in advanced triple-negative breast cancer, HER2+ breast cancer, and estrogen receptor-positive breast cancer [137]. Torres and Emens suggested that immunomodulation strategies, including checkpoint inhibition, bispecific antibodies, and drug eurythmy, could activate immune responses more effectively [138].
Single-agent anti-PD-1 ICIs have shown efficacy in early HCC treatment. Later-stage studies incorporated atezolizumab in combination with bevacizumab, which was approved as a first-line treatment modality. This combination significantly improved response and survival rates. Enhancing the combined use of ICIs or combining them with targeted therapies remains an important focus of future clinical research [139]. In advanced or metastatic gastric cancer, ICIs combined with chemotherapy and HER2-targeted treatments have shown promise. For instance, patients with PD-1 positivity exhibited higher overall survival rates when injectable olaparib (nivolumab) was combined with chemotherapy [140].
To overcome challenges associated with CAR T-cell therapy in hematologic malignancies, especially related to antigen heterogeneity and TME induction that limit the cytotoxic effects and the payload, Rezaei et al. suggested a synergistic strategy of a combination of lysosomal viral therapy and immunotherapy. This targeting approach selectively localizes therapeutic agents within the tumor milieu and can be used as a prototype in the treatment of solid malignancies [25]. The clinical advancement and identification of ICIs against CTLA-4, PD-1, and PD-L1 have transformed cancer treatments. Further discussing the modulation of T-cell functions, Kraehenbuehl et al. summarized co-stimulatory and co-inhibitory TCRs. They highlighted that a better optimization of co-inhibitor strategies should focus on tumor- and patient-specific properties. The use of targeted immunotherapy employing poorly co-stimulated receptors, cell subtype-specific targeting, and manipulating tumor cell metabolism may enable personalized treatment regimens [141].
2.7 Advancements in personalized CIT
Personalized medicine supports better treatment decisions through analysis of individual patients’ genetic information and tumor abnormalities, and biomarkers to identify optimal therapy options. The main barrier in personalized medicine practice emerges from uniting information from biological data with clinical choices to enhance cancer treatment efficiency [142]. The main advancement in personalized medicine involves targeted therapies and immunotherapies that exclusively target cancer cells yet protect healthy tissue. The use of HER2 inhibitors in breast cancer treatment, alongside EGFR inhibitors in lung cancer treatment, has proven more effective than traditional chemotherapy methods [143].
Unlike conventional “one-size-fits-all” approaches, personalized medicine tailors treatments based on individual patient characteristics, including tumor heterogeneity. Table 4 shows varied comparisons of traditional and personalized cancer treatments with differences in treatment approach, efficacy, and patient specificity highlighted. Research shows that traditional chemotherapy and radiation treatments succeed in specific cancers, but various treatment response rates exist among patients diagnosed with the same cancer type because of tumor heterogeneity [144]. The integration of personalized medicine techniques with conventional cancer treatments aims to maximize therapy results rather than substitute existing treatments. Genomic profiling enables doctors to identify patients who will benefit from chemotherapy, thus helping them avoid giving worthless treatments. A combination of precision medicines together with standard cancer treatments has resulted in promising outcomes. Targeted agents used together with radiation therapy generate stronger tumor control and minimize radiation resistance [145].
Differences between traditional and personalized cancer treatments
| Aspect | Traditional cancer treatment | Personalized cancer therapy |
|---|---|---|
| Approach | Standardized for all patients | Tailored to individual molecular profiles |
| Targeting | Non-specific (affects cancerous and healthy cells) | Tumor-specific antigens and molecular pathways |
| Side effects | Higher toxicity, off-target effects | Reduced toxicity due to precision targeting |
| Effectiveness | Variable response across patients | Higher efficacy in selected patient populations |
| Examples | Chemotherapy, radiation, surgery | CAR T-cell therapy, checkpoint inhibitors, neoantigen vaccines |
2.7.1 Neoantigen-based cancer vaccines
Personalized cancer vaccines employ tumor-specific mutant proteins known as neoantigens to induce immune responses that are tailored to each patient. In laboratory studies, neoantigen-based vaccines have proven to enhance T-cell activation and their specificity, leading to better destruction of tumors by immune responses [146]. Recent studies have shown an immense potential of personalized cancer vaccines in clinical practice of treating melanoma and other solid tumors [146]. Studies indicate that there are a maximum of 20 predicted cancer-specific neoantigens in every patient, which makes personalized vaccines a promising method within the framework of targeted immune response [147]. The feasibility of such vaccines and the resulting robust immune response was confirmed through multiple clinical trials, which made them effective tools in precision immunotherapy [148].
2.7.2 Precision oncology and immunotherapy integration
Cancer treatment through precision medicine combined with immunotherapy has become revolutionary, specifically in colorectal cancer management. The identification of biomarkers, together with molecular profiling advances, allows healthcare providers to create personalized treatment plans that increase treatment effectiveness [149]. The future of ICI’s development focuses on both enhancing resistance-breaking abilities and attaining superior therapeutic outcomes [150]. Recent evolutions in CAR T-cell therapy focus on developing multiple tumor antigen recognition systems to prevent tumors from escaping immune responses. Tisagenlecleucel and Axicabtagene-ciloleucel represent the first approved CAR T therapeutic agents that enable research into enhanced cellular immunological treatments [151].
2.7.3 Next-generation biomarkers
Biomarker detection serves as the fundamental basis for enhancing precision medicine applications in CIT. Biomarker-based stratification continues to enhance treatment selection through which clinicians can anticipate patient reactions to ICIs, as well as CAR T therapy and cancer vaccines [152]. Research teams have developed circulating tumor DNA (ctDNA)-based biomarkers to monitor tumors directly through the detection of real-time evolution and therapy response, as well as resistance mechanisms. Researchers have developed technological updates that will give clinicians access to adaptable treatment plans for the future [144].
2.7.4 Novel immunotherapeutic approaches
Scientists are developing engineered synthetic high-density lipoproteins (sHDL) for personalized immunotherapy applications that act as nanoparticle-based immune stimulators to regulate tumor-associated macrophages and DCs [153]. Immune-engineered biomaterials represent a major advancement through their function as artificial lymph nodes for better T-cell activation, along with enhanced antigen presentation. The bioengineered implants offer extended immune activation against tumors, so they improve how well immunotherapy works over long periods of time [154]. Tumor-infiltrating lymphocyte therapy represents a new development as medical professionals expand T-cells derived from patients to reintroduce them into the body. Scientific studies have demonstrated that this therapy produces significant anti-tumor outcomes among patients whose solid tumors resist treatment [155].
2.8 Clinical translation: From preclinical models to clinical trials
Several therapies have translational issues despite promising findings in preclinical discussion of nanocarrier-based delivery and immune-enhancing biomaterials. The encouraging evidence of human efficacy is provided by recent clinical trial programs, e.g., KEYNOTE-942, that showed an improvement in survival in melanoma using mRNA-based neoantigen vaccines. In this Phase II trial, combination therapy with personalized vaccines and pembrolizumab showed a significant increase in recurrence-free survival over monotherapy, indicating how early leadership in preclinical understanding is starting to translate into clinical gains [156]. Other trials, mentioned in Table 5 have also moved beyond early-phase safety studies, suggesting a maturing field ripe for broader clinical adoption.
Summary of clinical trials evaluating immunotherapeutic strategies
| Study type | Cancer type | Immunotherapy agent | Immunotherapy strategy | Patient population | Key findings | References |
|---|---|---|---|---|---|---|
| Phase III (CheckMate 141 - TBP Subanalysis) | HNSCC | Nivolumab (PD-1) | Treatment Beyond Progression (TBP) | Post-platinum, RECIST-progressed patients allowed TBP with stable performance | 25% had stable tumor burden; 25% had tumor reduction; overall survival (OS) = 12.7 months; no new safety signals | [157] |
| Phase III (OAK Trial - TBP subanalysis) | NSCLC | Atezolizumab (PD-L1) | TBP allowed post-progression | Patients continuing atezolizumab after radiographic progression | Post-progression OS = 12.7 months (vs 2.2 months no further tx); 49% stable lesions; no increased toxicity | [158] |
| Phase II study | NSCLC (Stage I–IV, post-surgery) | Autologous CIK cells | Adoptive cell therapy + chemotherapy | 87 matched patients per arm (chemo vs chemo + CIK) | Advanced-stage OS = 24 vs 10 months (p < 0.001); early-stage 3-year OS = 82 vs 66%; progression free survival (PFS) and OS improved with more CIK cycles | [159] |
| Phase I/II | Prostate cancer | Peptide-pulsed DCs (PSM-P1, PSM-P2) | Vaccine-based adoptive therapy | Immunocompetent patients assessed for cytokine response | Response correlated with skin antigen reactivity and T-cell cytokine production; potential biomarker for inclusion | [160] |
| Pooled, retrospective analysis from Phase III trials (CheckMate 066 & 067) | Advanced Melanoma | Nivolumab (PD-1) | TBP | Treatment-naive patients from CheckMate 066 and 067; 85 patients received nivolumab >6 weeks after RECIST-defined progression | 28% of TBP group had >30% tumor reduction after progression; 76% still alive at analysis; grade 3–4 adverse events similar to non-TBP group | [161] |
| Phase II, open-label, single-arm (KEYNOTE-427, Cohort A) | Advanced clear cell renal cell carcinoma (ccRCC) | Pembrolizumab (PD-1) | Monotherapy, first-line | 110 treatment-naive patients with advanced ccRCC | ORR = 36.4% (3.6% CR, 32.7% PR); 58.2% disease control rate; median progression-free survival (PFS) = 7.1 months; 12- and 24-month OS = 88.2 and 70.8%; durable responses in all risk groups; 30% experienced grade 3–5 adverse events (colitis, diarrhea most common) | [162] |
| Phase I/IIa, dose-escalation | NSCLC | CV9201 (RNActive® mRNA vaccine) | Multi-antigen mRNA vaccine targeting 5 NSCLC-associated antigens | 46 patients with locally advanced (n = 7) or metastatic (n = 39) NSCLC post–first-line therapy, all with ≥ stable disease | Well-tolerated at all doses; 63% had antigen-specific immune responses; 60% had ≥ 2× increase in activated IgD⁺CD38hi B cells; median PFS = 5.0 month, OS = 10.8 month; 2- and 3-year survival = 26.7 and 20.7%; no related grade 4/5 adverse events (AEs) | [163] |
| Phase Ib | Stage IV NSCLC | BI1361849 (CV9202) | mRNA vaccine (6 antigens) + local radiation ± maintenance therapy | 26 patients (stratified by histology and EGFR mutation status) with PR/SD after first-line therapy | 84% showed increased antigen-specific immune responses; 80% had higher antibody levels, 40% functional T-cell increases; SD in 46.2%, PR in 1 pt; vaccine well tolerated with mostly mild/moderate flu-like symptoms; supports further combination studies | [164] |
| Phase I (KEYNOTE-603) | Resected NSCLC (Part A) and Resected Melanoma (Part D) | mRNA-4157 (V940) ± Pembrolizumab | Individualized neoantigen mRNA vaccine, with/without checkpoint inhibitor | 4 NSCLC patients (mRNA-4157 alone), 12 melanoma patients (mRNA-4157 + pembrolizumab) | Well tolerated; no grade 4/5 AEs; mRNA-4157 induced robust de novo and boosted preexisting T-cell responses; combination with pembrolizumab expanded cytotoxic CD4⁺ and CD8⁺ T cells | [165] |
| Phase I/II (First-in-human, open-label) | Multiple solid tumors (melanoma, NSCLC, bladder, HNSCC, MSS-CRC, BCC, TNBC) | mRNA-4359 ± Pembrolizumab | Lipid nanoparticle mRNA vaccine encoding PD-L1 and IDO1 peptides; monotherapy and combo with PD-1 inhibitor | Dose escalation (Arm 1a): refractory advanced/metastatic tumors; Combo (Arm 1b/Arm 2): ICI-refractory or ICI-naive melanoma and NSCLC | Designed to activate PD-L1/IDO1-specific T-cells to reverse immunosuppression; aims to kill both tumor and regulatory immune cells | [166] |
2.9 AI in immunotherapy
The future of personalized medicine in immunotherapy emphasizes biomarker-driven approaches, innovative modalities, and AI integration to enhance cancer treatment outcomes (Table 6). As part of CIT strategies, AI has progressively become a key component, potentially providing transformational methods of enhancing treatment precision, outcome prediction, and personalized treatment. AI algorithms, notably machine learning, have been applied to define biomarkers that show treatment effectiveness, such as PD-L1 expression levels and Tumor Mutation Burden. These biomarkers assist in determining the chances of a patient’s response towards immunotherapy. Works referring to Xie et al. reveal how imaging omics can be used to investigate tumor heterogeneity with regard to immunotherapy response and biomarker expression [167]. AI plays an important role in differentiating patients about their responsiveness to immunotherapy using large datasets such as genomics and imaging data. This improves the outcomes of treatment and minimizes the patient’s exposure to the wrong treatment plan [168]. It has been anticipated that neoantigens play a vital role in devising a cancer vaccine because of recognizing tumor-specific antigens. AI helps in the construction of these vaccines because it can predict the neoantigen presentation and immunogenicity [169]. By contrast, AI tools adapt tool strategies based on the response of the patient to interventions using longitudinal data. Integrated imaging biomarkers improve upon conventional evaluations, as described by Ghaffari Laleh et al., by providing ongoing feedback [170]. AI facilitates personalizing immunotherapy intervention based on multi-omics analysis tailored to the individual tumor. AI’s cooperation with omics technologies increases the speed of finding therapeutic targets [171].
Future directions in personalized medicine
| Focus area | Description | Examples/insights | Challenges | Future impact | Technologies involved | References |
|---|---|---|---|---|---|---|
| Biomarker development | Identification of predictive biomarkers for therapy optimization | Genomic technologies, AI to discover robust biomarkers for immunotherapies | Variability in patient genetic profiles, high costs of validation | Improved treatment precision and reduced adverse effects | Genomic sequencing, AI algorithms | [172,173] |
| New immunotherapy modalities | Emerging treatments targeting specific antigens or immune pathways | Neoantigen-based vaccines, bispecific antibodies, engineered TCR therapies | Limited efficacy in heterogeneous tumors, logistical complexities | Expanded therapeutic arsenal, tackling resistant cancers | Synthetic biology, CRISPR, mRNA technology | [174] |
| AI & big data integration | Use of AI to analyze complex datasets for therapy customization | AI predicts treatment responses, tumor evolution, and optimal therapy combinations | Data privacy concerns, integration with clinical workflows | Accelerated discovery of treatment pathways and improved patient stratification | Machine learning, Natural Language Processing (NLP) | [175] |
| Combination therapy | Integration of immunotherapy with other treatments | Synergistic effects with targeted therapy, chemotherapy, or radiation | Complex clinical trial designs, managing cumulative side effects | Enhanced efficacy and reduced therapeutic resistance | Multimodal therapy platforms, computational biology | [176,177] |
| TME | Modulating the tumor’s immune environment to improve therapy outcomes | Targeting suppressive immune cells and reprogramming the immune landscape | Incomplete understanding of microenvironment dynamics | Boosted immune system response and minimized immune evasion by tumors | Cellular therapy, immune modulators, high-resolution imaging | [178] |
| Focus on hard-to-treat cancers | Novel approaches for cancers resistant to current treatments | DCs vaccines, personalized peptide vaccines | High costs, lack of universal efficacy, and limited clinical data | Targeted treatment options for previously untreatable cancers | Vaccine development, peptide synthesis, proteomics | [179] |
| Accessibility and equity | Ensuring global access to personalized immunotherapy treatments | Reduced costs, simplified diagnostics, and equitable therapies | High cost of therapies, and lack of infrastructure in low-income regions | Wider adoption of personalized treatments, reduced global health disparities | Point-of-care diagnostics, low-cost platforms.IR | [180] |
AI-powered platforms such as DeepNeo, pVACtools, and NetMHCpan are revolutionizing neoantigen prediction and vaccine design by integrating multi-omics data for epitope identification (Table 7). However, clinical adoption is challenged by issues like algorithm transparency, regulatory validation, and a lack of interpretability in real-time decision-making [181].
Summary of some neoantigen prediction tools
| Tool | Methodology | Interpretability | Clinical integration | Key challenges | References |
|---|---|---|---|---|---|
| DeepNeo/DeepNeo-v2 | Deep learning–based peptide–MHC binding and immunogenicity predictor | Moderate – black-box models; enhanced in v2 via improved rank metrics | Web server available; widely used for preclinical vaccine design | Limited transparency; needs clinical validation | [182] |
| DeepNeo-AGNet | Graph attention network + CNN for capturing neoantigen patterns | Moderate – architecture complexity limits user explainability | Early-stage; research-focused | Deep model complexity and reproducibility | [183] |
| ImmuScope | Self-iterative multiple-instance learning for CD4⁺ T-cell epitope prediction | High – allows feature attribution and region activation analysis | Integrates with antigen presentation prediction; benchmarked against DeepNeo | Still under validation; heavy computational demand | [184] |
| HLAIImaster | Adaptive deep learning for HLA class II binding prediction | High – trained on domain-informed architectures | Focus on class II neoepitopes; useful for vaccine design | Limited support for rare HLA alleles | [185] |
| FusionHLAII | BiGRU + Transformer using physicochemical encoding | High – captures temporal and global interactions; interpretable attention | Open-source; early research stage | Requires benchmark validation and wider testing | [186] |
| THLANet | ESM-2 + Transformer-Encoder for TCR–neoantigen–HLA class I prediction | High – 3D binding site visualization and alanine scanning enhance explainability | Validated across cancer datasets; outperforms PanPep and pMTnet | TCR–pHLA binding is data-limited; early in clinical uptake | [187] |
The development of personalized medicine and immunotherapy has greatly impacted the approaches to treating cancer by specifically targeting genetic and molecular markers. Colorectal cancer treatment has embraced precision medicine together with immunotherapy, involving genomic knowledge for targeted treatment [188]. Research stresses immunotherapy as a viable approach to ovarian cancer, especially for its inclusion in the future treatment plan of personalized medicine [189]. A new horizon for immunotherapy has emerged with gene editing and RNA interference technology in the treatment of patients.
2.10 Challenges in CIT
The clinical uptake of next-generation immunotherapies faces several systemic barriers. One of the most pressing barriers is the manufacturing complexity, particularly for personalized therapies like CAR T-cells and individualized neoantigen vaccines. CAR T therapy involves ex vivo genetic modification of a patient’s own T-cells, a process that takes 2–3 weeks and requires highly controlled good manufacturing practice environments. This time lag is problematic in aggressive cancers where rapid progression outpaces therapy preparation. Conversely, neoantigen vaccines, such as mRNA-4157 and CV9202, continue to mandate labor-intensive antigen identification, peptide synthesis, and formulations with turnaround times extending to more than 1 month, and thus are non-viable in clinical settings [182]. AI tools themselves, as computation pipeline technologies accelerate prediction, even though the framework requires timely tumor exome sequencing and HLA typings that are not equally accessible in healthcare environments. Workflows are also often delayed by data bottlenecks and inconsistency of sample quality, which do not allow their timely integration with the therapeutic decision-making [190].
Regulatory pathways remain unclear for many neoantigen-based therapies. Whereas ICIs and CAR T-cells have made it through regulatory approval with standardized clinical measures (e.g., ORR, PFS), neoantigen vaccines and AI-predicted epitope treatments have no normalized surrogate measures and population-wide clinical trial design. In principle, phase III designs are not easily affected by personalized vaccine trials owing to the lack of sample size and standardization. Regulatory agencies like the U.S. Food and drug administration and the European Medicines Agency require both regulation and scalability, which are both overstretched in high-personalized mutanome and immune profiling-driven therapies. Moreover, there is also the problem of interpretability of AI-based tools, which establishes a bottleneck for clinical validation. These models often operate as “black boxes,” challenging traditional regulatory frameworks that require explainable outputs, especially when integrated into diagnostics or companion decision tools [191]. The economic burden of immunotherapy remains one of the most well-documented obstacles to widespread use.
Global disparities in immunotherapy access remain stark. Access to CAR T and ICIs is mostly available in high-income markets, whereas limited infrastructure and funding exist in low- and middle-income countries to conduct clinical trials and provide delivery systems. Furthermore, racial and ethnic minorities are not well-represented in clinical trials, distorting efficacy and toxicity data. To bridge this gap, strategies such as global licensing, public-private manufacturing partnerships, and regional regulatory harmonization are essential.
3 Conclusion
Advances in personalized medicine, particularly in the realm of CIT, signify a transformative era in oncology. Immunotherapy has brought innovative strategies for cancer treatment by stimulating the human immune system to resist tumors. While it demonstrates promising application effects, it is not without certain defects and limitations. This study analyzed recent advances and the current status of immunotherapy research, emphasizing emerging tools such as nanomedicine formulations that provide targeted cancer therapies. The use of T-cell subsets, novel antigen expression methods, and the development of interventions targeting the TME hold significant potential. Neoadjuvant ICI blockades and combined immunotherapeutic approaches further enhance anti-tumor efficacy. Additionally, the integration of AI into CIT marks a critical leap forward. Innovations in deep learning, NLP, and federated learning are expected to expand the scope of biomarker discovery and predictive modeling. AI’s role in clinical workflows will likely accelerate personalized therapeutic decisions while reducing the time and costs associated with drug development and clinical trials.
Future research must prioritize individualized detection and management, the rapid development of new technologies and vaccines targeting novel antigens, the reduction of side effects, and the mitigation of immunotherapy-associated drug resistance. Looking ahead, the convergence of personalized medicine, immunotherapy, and AI offers a transformative potential to revolutionize cancer treatment. Through continued innovation and efforts to address existing challenges, this multidisciplinary approach promises not only improved patient outcomes but also a future where cancer care is highly efficient, targeted, and accessible for all.
-
Funding information: Author states no funding involved.
-
Author contribution: Author confirms the sole responsibility for the conception of the study, presented results, and manuscript preparation.
-
Conflict of interest: Author states no conflict of interest.
-
Data availability statement: Data sharing is not applicable to this article as no datasets were generated or analyzed during the current study.
References
[1] Morrissey KM, Yuraszeck TM, Li CC, Zhang Y, Kasichayanula S. Immunotherapy and novel combinations in oncology: current landscape, challenges, and opportunities. Clin Transl Sci. 2016;9:89–104.10.1111/cts.12391Search in Google Scholar PubMed PubMed Central
[2] Eno J. Immunotherapy through the years. J Adv Pract Oncol. 2017;8:747–53.10.6004/jadpro.2017.8.7.8Search in Google Scholar
[3] Knuth A, Jäger D, Jäger E. Cancer immunotherapy in clinical oncology. Cancer Chemother Pharmacol. 2000;46:S46–51.10.1007/PL00014050Search in Google Scholar
[4] Barbari C, Fontaine T, Parajuli P, Lamichhane N, Jakubski S, Lamichhane P, et al. Immunotherapies and combination strategies for immuno-oncology. Int J Mol Sci. 2020;21:1–28.10.3390/ijms21145009Search in Google Scholar PubMed PubMed Central
[5] Aggarwal C, Ben-Shachar R, Gao Y, Hyun SW, Rivers Z, Epstein C, et al. Assessment of tumor mutational burden and outcomes in patients with diverse advanced cancers treated with immunotherapy. JAMA Netw Open. 2023;6:e2311181.10.1001/jamanetworkopen.2023.11181Search in Google Scholar PubMed PubMed Central
[6] Abdo J, Cornell DL, Mittal SK, Agrawal DK. Immunotherapy plus cryotherapy: potential augmented abscopal effect for advanced cancers. Front Oncol. 2018;8:85. 10.3389/fonc.2018.00085.Search in Google Scholar PubMed PubMed Central
[7] Freshwater T, Kondic A, Ahamadi M, Li CH, de Greef R, de Alwis D, et al. Evaluation of dosing strategy for pembrolizumab for oncology indications. J Immunother Cancer. 2017;5:43.10.1186/s40425-017-0242-5Search in Google Scholar PubMed PubMed Central
[8] Tay RE, Richardson EK, Toh HC. Revisiting the role of CD4+ T cells in cancer immunotherapy – new insights into old paradigms. Cancer Gene Ther. 2021;28:5–17.10.1038/s41417-020-0183-xSearch in Google Scholar PubMed PubMed Central
[9] Borst J, Ahrends T, Bąbała N, Melief C, Kastenmüller W. CD4+ T cell help in cancer immunology and immunotherapy. Nat Rev Immunol. 2018;18:635–47.10.1038/s41577-018-0044-0Search in Google Scholar PubMed
[10] Speiser DE, Chijioke O, Schaeuble K, Münz C. CD4+ T cells in cancer. Nat Cancer. 2023;4:317–29.10.1038/s43018-023-00521-2Search in Google Scholar PubMed
[11] Nishikawa H, Sakaguchi S. Regulatory T cells in cancer immunotherapy. Curr Opin Immunol. 2014;27:1–7.10.1016/j.coi.2013.12.005Search in Google Scholar PubMed
[12] Ben Khelil M, Godet Y, Abdeljaoued S, Borg C, Adotévi O, Loyon R. Harnessing antitumor cD4+ T cells for cancer immunotherapy. Cancers (Basel). 2022;14:260.10.3390/cancers14010260Search in Google Scholar PubMed PubMed Central
[13] Kimiz-Gebologlu I, Gulce-Iz S, Biray-Avci C. Monoclonal antibodies in cancer immunotherapy. Mol Biol Rep. 2018;45:2935–40.10.1007/s11033-018-4427-xSearch in Google Scholar PubMed
[14] Weiner LM, Dhodapkar MV, Ferrone S. Monoclonal antibodies for cancer immunotherapy. Lancet. 2009;373:1033–40.10.1016/S0140-6736(09)60251-8Search in Google Scholar PubMed PubMed Central
[15] Zhou Y, Penny HL, Kroenke MA, Bautista B, Hainline K, Chea LS, et al. Immunogenicity assessment of bispecific antibody-based immunotherapy in oncology. J Immunother Cancer. 2022;10:e004225.10.1136/jitc-2021-004225Search in Google Scholar PubMed PubMed Central
[16] Krishnamurthy A, Jimeno A. Bispecific antibodies for cancer therapy: A review. Pharmacol Ther. 2018;185:122–34.10.1016/j.pharmthera.2017.12.002Search in Google Scholar PubMed
[17] Dahlén E, Veitonmäki N, Norlén P. Bispecific antibodies in cancer immunotherapy. Ther Adv Vaccines Immunother. 2018;6:3–17.10.1177/2515135518763280Search in Google Scholar PubMed PubMed Central
[18] Wargo JA, Reuben A, Cooper ZA, Oh KS, Sullivan RJ. Immune effects of chemotherapy, radiation, and targeted therapy and opportunities for combination with immunotherapy. Semin Oncol. 2015;42:601–16.10.1053/j.seminoncol.2015.05.007Search in Google Scholar PubMed PubMed Central
[19] Yu W-D, Sun G, Li J, Xu J, Wang X. Mechanisms and therapeutic potentials of cancer immunotherapy in combination with radiotherapy and/or chemotherapy. Cancer Lett. 2019;452:66–70.10.1016/j.canlet.2019.02.048Search in Google Scholar PubMed
[20] Drake CG. Combination immunotherapy approaches. Ann Oncol. 2012;23:viii41–6.10.1093/annonc/mds262Search in Google Scholar PubMed PubMed Central
[21] Kalbasi A, June CH, Haas N, Vapiwala N. Radiation and immunotherapy: a synergistic combination. J Clin Invest. 2013;123:2756–63.10.1172/JCI69219Search in Google Scholar PubMed PubMed Central
[22] Vatner RE, Cooper BT, Vanpouille-Box C, Demaria S, Formenti SC. Combinations of immunotherapy and radiation in cancer therapy. Front Oncol. 2014;4:325. 10.3389/fonc.2014.00325.Search in Google Scholar PubMed PubMed Central
[23] Jagodinsky JC, Harari PM, Morris ZS. The promise of combining radiation therapy with immunotherapy. Int J Radiat Oncol. 2020;108:6–16.10.1016/j.ijrobp.2020.04.023Search in Google Scholar PubMed PubMed Central
[24] Pan C, Liu H, Robins E, Song W, Liu D, Li Z, et al. Next-generation immuno-oncology agents: current momentum shifts in cancer immunotherapy. J Hematol Oncol. 2020;13:29.10.1186/s13045-020-00862-wSearch in Google Scholar PubMed PubMed Central
[25] Rezaei R, Esmaeili Gouvarchin Ghaleh H, Farzanehpour M, Dorostkar R, Ranjbar R, Bolandian M, et al. Combination therapy with CAR T cells and oncolytic viruses: a new era in cancer immunotherapy. Cancer Gene Ther. 2022;29:647–60.10.1038/s41417-021-00359-9Search in Google Scholar PubMed
[26] Guedan S, Alemany R. CAR-T cells and oncolytic viruses: joining forces to overcome the solid tumor challenge. Front Immunol. 2018;9:2460. 10.3389/fimmu.2018.02460 Search in Google Scholar PubMed PubMed Central
[27] Ajina A, Maher J. Prospects for combined use of oncolytic viruses and CAR T-cells. J Immunother Cancer. 2017;5:90.10.1186/s40425-017-0294-6Search in Google Scholar PubMed PubMed Central
[28] Shi T, Song X, Wang Y, Liu F, Wei J. Combining oncolytic viruses with cancer immunotherapy: establishing a new generation of cancer treatment. Front Immunol. 2020;11:683. 10.3389/fimmu.2020.00683.Search in Google Scholar PubMed PubMed Central
[29] Raja J, Ludwig JM, Gettinger SN, Schalper KA, Kim HS. Oncolytic virus immunotherapy: future prospects for oncology. J Immunother Cancer. 2018;6:140.10.1186/s40425-018-0458-zSearch in Google Scholar PubMed PubMed Central
[30] Zarezadeh Mehrabadi A, Roozbahani F, Ranjbar R, Farzanehpour M, Shahriary A, Dorostkar R, et al. Overview of the pre-clinical and clinical studies about the use of CAR-T cell therapy of cancer combined with oncolytic viruses. World J Surg Oncol. 2022;20:16.10.1186/s12957-021-02486-xSearch in Google Scholar PubMed PubMed Central
[31] Evgin L, Huff AL, Wongthida P, Thompson J, Kottke T, Tonne J, et al. Oncolytic virus-derived type I interferon restricts CAR T cell therapy. Nat Commun. 2020;11:3187.10.1038/s41467-020-17011-zSearch in Google Scholar PubMed PubMed Central
[32] Tselikas L, Champiat S, Sheth RA, Yevich S, Ammari S, Deschamps F, et al. Interventional radiology for local immunotherapy in oncology. Clin Cancer Res. 2021;27:2698–705.10.1158/1078-0432.CCR-19-4073Search in Google Scholar PubMed
[33] Aznar MA, Tinari N, Rullán AJ, Sánchez-Paulete AR, Rodriguez-Ruiz ME, Melero I. Intratumoral delivery of immunotherapy – act locally, think globally. J Immunol. 2017;198:31–9.10.4049/jimmunol.1601145Search in Google Scholar PubMed
[34] Mikhail AS, Morhard R, Mauda-Havakuk M, Kassin M, Arrichiello A, Wood BJ. Hydrogel drug delivery systems for minimally invasive local immunotherapy of cancer. Adv Drug Deliv Rev. 2023;202:115083.10.1016/j.addr.2023.115083Search in Google Scholar PubMed PubMed Central
[35] Shang Q, Dong Y, Su Y, Leslie F, Sun M, Wang F. Local scaffold-assisted delivery of immunotherapeutic agents for improved cancer immunotherapy. Adv Drug Deliv Rev. 2022;185:114308.10.1016/j.addr.2022.114308Search in Google Scholar PubMed
[36] Nguyen KG, Vrabel MR, Mantooth SM, Hopkins JJ, Wagner ES, Gabaldon TA, et al. Localized interleukin-12 for cancer immunotherapy. Front Immunol. 2020;11:575597. 10.3389/fimmu.2020.575597.Search in Google Scholar PubMed PubMed Central
[37] Minaei E, Ranson M, Aghmesheh M, Sluyter R, Vine KL. Enhancing pancreatic cancer immunotherapy: Leveraging localized delivery strategies through the use of implantable devices and scaffolds. J Control Rel. 2024;373:145–60.10.1016/j.jconrel.2024.07.023Search in Google Scholar PubMed
[38] Li X, Pan J, Li Y, Xu F, Hou J, Yang G, et al. Development of a localized drug delivery system with a step-by-step cell internalization capacity for cancer immunotherapy. ACS Nano. 2022;16:5778–94.10.1021/acsnano.1c10892Search in Google Scholar PubMed
[39] Muranski P, Restifo NP. Adoptive immunotherapy of cancer using CD4+ T cells. Curr Opin Immunol. 2009;21:200–8.10.1016/j.coi.2009.02.004Search in Google Scholar PubMed PubMed Central
[40] Brightman SE, Naradikian MS, Miller AM, Schoenberger SP. Harnessing neoantigen specific CD4 T cells for cancer immunotherapy. J Leukoc Biol. 2020;107:625–33.10.1002/JLB.5RI0220-603RRSearch in Google Scholar PubMed PubMed Central
[41] Dougan M, Luoma AM, Dougan SK, Wucherpfennig KW. Understanding and treating the inflammatory adverse events of cancer immunotherapy. Cell. 2021;184:1575–88.10.1016/j.cell.2021.02.011Search in Google Scholar PubMed PubMed Central
[42] Luo J, Jiang B, Li C, Jia X, Shi D. CYC27 synthetic derivative of bromophenol from Red Alga Rhodomela confervoides: Anti-diabetic effects of sensitizing insulin signaling pathways and modulating RNA splicing-associated RBPs. Mar Drugs. 2019;17:49.10.3390/md17010049Search in Google Scholar PubMed PubMed Central
[43] Donnadieu E, Dupré L, Pinho LG, Cotta-de-Almeida V. Surmounting the obstacles that impede effective CAR T cell trafficking to solid tumors. J Leukoc Biol. 2020;108:1067–79.10.1002/JLB.1MR0520-746RSearch in Google Scholar PubMed PubMed Central
[44] Anandappa AJ, Wu CJ, Ott PA. Directing traffic: How to effectively drive T cells into tumors. Cancer Discov. 2020;10:185–97.10.1158/2159-8290.CD-19-0790Search in Google Scholar PubMed PubMed Central
[45] Wu P, Gao W, Su M, Nice EC, Zhang W, Lin J, et al. Adaptive mechanisms of tumor therapy resistance driven by tumor microenvironment. Front Cell Dev Biol. 2021;9:641469. 10.3389/fcell.2021.641469.Search in Google Scholar PubMed PubMed Central
[46] Sun Y. Tumor microenvironment and cancer therapy resistance. Cancer Lett. 2016;380:205–15.10.1016/j.canlet.2015.07.044Search in Google Scholar PubMed
[47] Gajewski TF. Identifying and overcoming immune resistance mechanisms in the melanoma tumor microenvironment. Clin Cancer Res. 2006;12:2326s–30s.10.1158/1078-0432.CCR-05-2517Search in Google Scholar PubMed
[48] Son B, Lee S, Youn H, Kim E, Kim W, Youn B. The role of tumor microenvironment in therapeutic resistance. Oncotarget. 2017;8:3933–45.10.18632/oncotarget.13907Search in Google Scholar PubMed PubMed Central
[49] Khalaf K, Hana D, Chou JT, Singh C, Mackiewicz A, Kaczmarek M. Aspects of the tumor microenvironment involved in immune resistance and drug resistance. Front Immunol. 2021;12:656364. 10.3389/fimmu.2021.656364.Search in Google Scholar PubMed PubMed Central
[50] Leko V, Rosenberg SA. Identifying and targeting human tumor antigens for T cell-based immunotherapy of solid tumors. Cancer Cell. 2020;38:454–72.10.1016/j.ccell.2020.07.013Search in Google Scholar PubMed PubMed Central
[51] Zhao L, Zhou X, Xie F, Zhang L, Yan H, Huang J, et al. Ferroptosis in cancer and cancer immunotherapy. Cancer Commun. 2022;42:88–116.10.1002/cac2.12250Search in Google Scholar PubMed PubMed Central
[52] Murciano-Goroff YR, Warner AB, Wolchok JD. The future of cancer immunotherapy: microenvironment-targeting combinations. Cell Res. 2020;30:507–19.10.1038/s41422-020-0337-2Search in Google Scholar PubMed PubMed Central
[53] Bashash D, Zandi Z, Kashani B, Pourbagheri-Sigaroodi A, Salari S, Ghaffari SH. Resistance to immunotherapy in human malignancies: Mechanisms, research progresses, challenges, and opportunities. J Cell Physiol. 2022;237:346–72.10.1002/jcp.30575Search in Google Scholar PubMed
[54] Adu-Berchie K, Mooney DJ. Biomaterials as local niches for immunomodulation. Acc Chem Res. 2020;53:1749–60.10.1021/acs.accounts.0c00341Search in Google Scholar PubMed
[55] Wang H, Najibi AJ, Sobral MC, Seo BR, Lee JY, Wu D, et al. Biomaterial-based scaffold for in situ chemo-immunotherapy to treat poorly immunogenic tumors. Nat Commun. 2020;11:5696.10.1038/s41467-020-19540-zSearch in Google Scholar PubMed PubMed Central
[56] Han S, Wu J. Three-dimensional (3D) scaffolds as powerful weapons for tumor immunotherapy. Bioact Mater. 2022;17:300–19.10.1016/j.bioactmat.2022.01.020Search in Google Scholar PubMed PubMed Central
[57] Li J, Luo Y, Li B, Xia Y, Wang H, Fu C. Implantable and injectable biomaterial scaffolds for cancer immunotherapy. Front Bioeng Biotechnol. 2020;8:612950. 10.3389/fbioe.2020.612950.Search in Google Scholar PubMed PubMed Central
[58] Leach DG, Young S, Hartgerink JD. Advances in immunotherapy delivery from implantable and injectable biomaterials. Acta Biomater. 2019;88:15–31.10.1016/j.actbio.2019.02.016Search in Google Scholar PubMed PubMed Central
[59] Yang C, Blum NT, Lin J, Qu J, Huang P. Biomaterial scaffold-based local drug delivery systems for cancer immunotherapy. Sci Bull. 2020;65:1489–504.10.1016/j.scib.2020.04.012Search in Google Scholar PubMed
[60] Pechnikova NA, Aggeli A, Latypova AA, Iaremenko AV, Domvri K, Zubarev IV, et al. Implantable biomaterials for cancer immunotherapies. Adv Funct Mater. 2024;35:2416813. 10.1002/adfm.202416813.Search in Google Scholar
[61] Oliveira I, Rodrigues-Santos P, Ferreira L, Pires das Neves R. Synthetic and biological nanoparticles for cancer immunotherapy. Biomater Sci. 2024;12:5933–60.10.1039/D4BM00995ASearch in Google Scholar
[62] Park Y-M, Lee SJ, Kim YS, Lee MH, Cha GS, Jung ID, et al. Nanoparticle-based vaccine delivery for cancer immunotherapy. Immune Netw. 2013;13:177–83.10.4110/in.2013.13.5.177Search in Google Scholar PubMed PubMed Central
[63] Liu J, Zhang R, Xu ZP. Nanoparticle‐based nanomedicines to promote cancer immunotherapy: Recent advances and future directions. Small. 2019;15:1900262. 10.1002/smll.201900262.Search in Google Scholar PubMed
[64] Ma X, Li S-J, Liu Y, Zhang T, Xue P, Kang Y, et al. Bioengineered nanogels for cancer immunotherapy. Chem Soc Rev. 2022;51:5136–74.10.1039/D2CS00247GSearch in Google Scholar
[65] Zhang C, Pu K. Molecular and nanoengineering approaches towards activatable cancer immunotherapy. Chem Soc Rev. 2020;49:4234–53.10.1039/C9CS00773CSearch in Google Scholar PubMed
[66] Xu J, Lv J, Zhuang Q, Yang Z, Cao Z, Xu L, et al. A general strategy towards personalized nanovaccines based on fluoropolymers for post-surgical cancer immunotherapy. Nat Nanotechnol. 2020;15:1043–52.10.1038/s41565-020-00781-4Search in Google Scholar PubMed
[67] Wu P, Han J, Gong Y, Liu C, Yu H, Xie N. Nanoparticle-based drug delivery systems targeting tumor microenvironment for cancer immunotherapy resistance: current advances and applications. Pharmaceutics. 2022;14:1990.10.3390/pharmaceutics14101990Search in Google Scholar PubMed PubMed Central
[68] Leleux J, Roy K. Micro and nanoparticle‐based delivery systems for vaccine immunotherapy: an immunological and materials perspective. Adv Healthc Mater. 2013;2:72–94.10.1002/adhm.201200268Search in Google Scholar PubMed
[69] Gupta B, Kim JO. Recent progress in cancer immunotherapy approaches based on nanoparticle delivery devices. J Pharm Investig. 2021;51:399–412.10.1007/s40005-021-00527-xSearch in Google Scholar
[70] Feng Y, Tang Q, Wang B, Yang Q, Zhang Y, Lei L, et al. Targeting the tumor microenvironment with biomaterials for enhanced immunotherapeutic efficacy. J Nanobiotechnol. 2024;22:737.10.1186/s12951-024-03005-2Search in Google Scholar PubMed PubMed Central
[71] Martin JD, Cabral H, Stylianopoulos T, Jain RK. Improving cancer immunotherapy using nanomedicines: progress, opportunities and challenges. Nat Rev Clin Oncol. 2020;17:251–66.10.1038/s41571-019-0308-zSearch in Google Scholar PubMed PubMed Central
[72] Meyer RA, Sunshine JC, Perica K, Kosmides AK, Aje K, Schneck JP, et al. Biodegradable nanoellipsoidal artificial antigen presenting cells for antigen specific T‐cell activation. Small. 2015;11:1519–25.10.1002/smll.201402369Search in Google Scholar PubMed PubMed Central
[73] Sunshine JC, Perica K, Schneck JP, Green JJ. Particle shape dependence of CD8+ T cell activation by artificial antigen presenting cells. Biomaterials. 2014;35:269–77.10.1016/j.biomaterials.2013.09.050Search in Google Scholar PubMed PubMed Central
[74] Chen JY, Agrawal S, Yi HP, Vallejo D, Agrawal A, Lee AP. Cell‐sized lipid vesicles as artificial antigen‐presenting cells for antigen‐specific T cell activation. Adv Healthc Mater. 2023;12:2203163. 10.1002/adhm.202203163.Search in Google Scholar PubMed PubMed Central
[75] Latouche J-B, Sadelain M. Induction of human cytotoxic T lymphocytes by artificial antigen-presenting cells. Nat Biotechnol. 2000;18:405–9.10.1038/74455Search in Google Scholar PubMed
[76] Gonzalez-Fernandez T, Sikorski P, Leach JK. Bio-instructive materials for musculoskeletal regeneration. Acta Biomater. 2019;96:20–34.10.1016/j.actbio.2019.07.014Search in Google Scholar PubMed PubMed Central
[77] Bowers DT, Brown JL. Nanofibers as bioinstructive scaffolds capable of modulating differentiation through mechanosensitive pathways for regenerative engineering. Regen Eng Transl Med. 2019;5:22–9.10.1007/s40883-018-0076-9Search in Google Scholar PubMed PubMed Central
[78] Kämmerling L, Fisher LE, Antmen E, Simsek GM, Rostam HM, Vrana NE, et al. Mitigating the foreign body response through ‘immune-instructive’ biomaterials. J Immunol Regen Med. 2021;12:100040.10.1016/j.regen.2021.100040Search in Google Scholar
[79] van der Boon T. On the verge of bio-instructive medical implant surfaces. Groningen: University of Groningen; 2024. 10.33612/diss.979326658.Search in Google Scholar
[80] Agarwalla P, Ogunnaike EA, Ahn S, Froehlich KA, Jansson A, Ligler FS, et al. Bioinstructive implantable scaffolds for rapid in vivo manufacture and release of CAR-T cells. Nat Biotechnol. 2022;40:1250–8.10.1038/s41587-022-01245-xSearch in Google Scholar PubMed PubMed Central
[81] He Y, Wang W, Lin S, Yang Y, Song L, Jing Y, et al. Fabrication of a bio-instructive scaffold conferred with a favorable microenvironment allowing for superior implant osseointegration and accelerated in situ vascularized bone regeneration via type H vessel formation. Bioact Mater. 2022;9:491–507.10.1016/j.bioactmat.2021.07.030Search in Google Scholar PubMed PubMed Central
[82] Cheng F, Su T, Zhou S, Liu X, Yang S, Lin S, et al. Single-dose injectable nanovaccine-in-hydrogel for robust immunotherapy of large tumors with abscopal effect. Sci Adv. 2023;9:6257. 10.1126/sciadv.ade6257.Search in Google Scholar PubMed PubMed Central
[83] Ren X, Wang N, Zhou Y, Song A, Jin G, Li Z, et al. An injectable hydrogel using an immunomodulating gelator for amplified tumor immunotherapy by blocking the arginase pathway. Acta Biomater. 2021;124:179–90.10.1016/j.actbio.2021.01.041Search in Google Scholar PubMed
[84] Xiao Z, Wang D, Wang C, Chen Z, Huang C, Yang Y, et al. PEIGel: A biocompatible and injectable scaffold with innate immune adjuvanticity for synergized local immunotherapy. Mater Today Bio. 2022;15:100297.10.1016/j.mtbio.2022.100297Search in Google Scholar PubMed PubMed Central
[85] Yang X, Huang C, Wang H, Yang K, Huang M, Zhang W, et al. Multifunctional nanoparticle-loaded injectable alginate hydrogels with deep tumor penetration for enhanced chemo-immunotherapy of cancer. ACS Nano. 2024;18:18604–21.10.1021/acsnano.4c04766Search in Google Scholar PubMed
[86] Zhu C, Ke L, Ao X, Chen Y, Cheng H, Xin H, et al. Injectable supramolecular hydrogels for in situ programming of CAR‐T cells toward solid tumor immunotherapy. Adv Mater. 2024;36:2310078. 10.1002/adma.202310078.Search in Google Scholar PubMed
[87] Lei F, Cai J, Lyu R, Shen H, Xu Y, Wang J, et al. Efficient tumor immunotherapy through a single injection of injectable antigen/adjuvant-loaded macroporous silk fibroin microspheres. ACS Appl Mater Interfaces. 2022;14:42950–62.10.1021/acsami.2c11286Search in Google Scholar PubMed
[88] Fan Y, Zhan M, Liang J, Yang X, Zhang B, Shi X, et al. Programming injectable DNA hydrogels yields tumor microenvironment‐activatable and immune‐instructive depots for augmented chemo‐immunotherapy. Adv Sci. 2023;10:2302119. 10.1002/advs.202302119.Search in Google Scholar PubMed PubMed Central
[89] Wang F, Xie M, Huang Y, Liu Y, Liu X, Zhu L, et al. In situ vaccination with an injectable nucleic acid hydrogel for synergistic cancer immunotherapy. Angew Chem Int Ed. 2024;63:202315282. 10.1002/anie.202315282.Search in Google Scholar PubMed
[90] Zhou J-J, Li X-H, He P-Y, Qi FY, Ullah MW, Li SJ, et al. Implantable versatile oxidized bacterial cellulose membrane for postoperative HNSCC treatment via photothermal-boosted immunotherapy. Nano Res. 2023;16:951–63.10.1007/s12274-022-4811-7Search in Google Scholar
[91] Chen Q, Zhou S, Ding Y, Chen D, Dahiru NS, Tang H, et al. A bio-responsive, cargo-catchable gel for postsurgical tumor treatment via ICD-based immunotherapy. J Control Rel. 2022;346:212–25.10.1016/j.jconrel.2022.04.015Search in Google Scholar PubMed
[92] Oliveira G, Wu CJ. Dynamics and specificities of T cells in cancer immunotherapy. Nat Rev Cancer. 2023;23:295–316.10.1038/s41568-023-00560-ySearch in Google Scholar PubMed PubMed Central
[93] Chow A, Perica K, Klebanoff CA, Wolchok JD. Clinical implications of T cell exhaustion for cancer immunotherapy. Nat Rev Clin Oncol. 2022;19:775–90.10.1038/s41571-022-00689-zSearch in Google Scholar PubMed PubMed Central
[94] Mensurado S, Blanco-Domínguez R, Silva-Santos B. The emerging roles of γδ T cells in cancer immunotherapy. Nat Rev Clin Oncol. 2023;20:178–91.10.1038/s41571-022-00722-1Search in Google Scholar PubMed
[95] Shi X, Chen W, Yin Y, Cao H, Wang X, Jiang W, et al. RAC1high NK cell-based immunotherapy in hepatocellular carcinoma via STAT3-NKG2D axis. Cancer Lett. 2024;592:216909.10.1016/j.canlet.2024.216909Search in Google Scholar PubMed
[96] Dong Y, Chen Z, Yang F, Wei J, Huang J, Long X. Prediction of immunotherapy responsiveness in melanoma through single-cell sequencing-based characterization of the tumor immune microenvironment. Transl Oncol. 2024;43:101910.10.1016/j.tranon.2024.101910Search in Google Scholar PubMed PubMed Central
[97] Yin J, Wang H, Hong Y, Ren A, Wang H, Liu L, et al. Identification of an at-risk subpopulation with high immune infiltration based on the peroxisome pathway and TIM3 in colorectal cancer. BMC Cancer. 2022;22:44.10.1186/s12885-021-09085-9Search in Google Scholar PubMed PubMed Central
[98] Han HS, Jeong S, Kim H, Kim HD, Kim AR, Kwon M, et al. TOX-expressing terminally exhausted tumor-infiltrating CD8+ T cells are reinvigorated by co-blockade of PD-1 and TIGIT in bladder cancer. Cancer Lett. 2021;499:137–47.10.1016/j.canlet.2020.11.035Search in Google Scholar PubMed
[99] Gao Y, Li H, Li Z, Xie L, Liu X, Huang Z, et al. Single-cell analysis reveals the heterogeneity of monocyte-derived and peripheral type-2 conventional dendritic cells. J Immunol. 2021;207:837–48.10.4049/jimmunol.2100094Search in Google Scholar PubMed
[100] Zhou Z, Wang J, Wang J, Yang S, Wang R, Zhang G, et al. Deciphering the tumor immune microenvironment from a multidimensional omics perspective: insight into next-generation CAR-T cell immunotherapy and beyond. Mol Cancer. 2024;23:131.10.1186/s12943-024-02047-2Search in Google Scholar PubMed PubMed Central
[101] Zarodniuk M, Steele A, Lu X, Li J, Datta M. CNS tumor stroma transcriptomics identify perivascular fibroblasts as predictors of immunotherapy resistance in glioblastoma patients. npj Genomic Med. 2023;8:35.10.1038/s41525-023-00381-wSearch in Google Scholar PubMed PubMed Central
[102] Dhar S. Advances in clinical immunology. Prem J Immunol. 2025;2:100004. 10.70389/PJI.100004.Search in Google Scholar
[103] Kim J, Cho J, Lee MH, Yoon SE, Kim WS, Kim SJ. CAR T cells vs bispecific antibody as third- or later-line large B-cell lymphoma therapy: a meta-analysis. Blood. 2024;144:629–38.10.1182/blood.2023023419Search in Google Scholar PubMed
[104] Morabito F, Martino EA, Nizzoli ME, Talami A, Pozzi S, Martino M, et al. Comparative analysis of bispecific antibodies and CAR T‐cell therapy in Follicular lymphoma. Eur J Haematol. 2025;114:4–16.10.1111/ejh.14335Search in Google Scholar PubMed PubMed Central
[105] Hay AE, Cheung MC. CAR T-cells: costs, comparisons, and commentary. J Med Econ. 2019;22:613–5.10.1080/13696998.2019.1582059Search in Google Scholar PubMed
[106] Bangolo A, Amoozgar B, Mansour C, Zhang L, Gill S, Ip A, et al. Comprehensive review of early and late toxicities in CAR T-cell therapy and bispecific antibody treatments for hematologic malignancies. Cancers (Basel). 2025;17:282.10.3390/cancers17020282Search in Google Scholar PubMed PubMed Central
[107] Chacim S, Monjardino T, Cunha JL, Medeiros P, Redondo P, Bento MJ, et al. Costs, effectiveness, and safety associated with Chimeric Antigen Receptor (CAR) T-cell therapy: Results from a comprehensive cancer center. PLoS One. 2022;17:e0278950.10.1371/journal.pone.0278950Search in Google Scholar PubMed PubMed Central
[108] Kapinos KA, Hu E, Trivedi J, Geethakumari PR, Kansagra A. Cost-effectiveness analysis of CAR T-cell therapies vs antibody drug conjugates for patients with advanced multiple myeloma. Cancer Control. 2023;30:10732748221142945. 10.1177/10732748221142945.Search in Google Scholar PubMed PubMed Central
[109] Strohl WR, Naso M. Bispecific T-cell redirection versus chimeric antigen receptor (CAR)-T cells as approaches to kill cancer cells. Antibodies. 2019;8:41.10.3390/antib8030041Search in Google Scholar PubMed PubMed Central
[110] Trabolsi A, Arumov A, Schatz JH. Bispecific antibodies and CAR-T cells: dueling immunotherapies for large B-cell lymphomas. Blood Cancer J. 2024;14:27.10.1038/s41408-024-00997-wSearch in Google Scholar PubMed PubMed Central
[111] Keesari PR, Samuels D, Vegivinti CTR, Pulakurthi YS, Kudithi R, Dhar M, et al. Navigating the economic burden of Multiple Myeloma: Insights into cost-effectiveness of CAR-T and bispecific antibody therapies. Curr Hematol Malig Rep. 2025;20:3.10.1007/s11899-024-00748-5Search in Google Scholar PubMed PubMed Central
[112] Chhabra N, Kennedy J. A review of cancer immunotherapy toxicity: Immune checkpoint inhibitors. J Med Toxicol. 2021;17:411–24.10.1007/s13181-021-00833-8Search in Google Scholar PubMed PubMed Central
[113] Carlino MS, Larkin J, Long GV. Immune checkpoint inhibitors in melanoma. Lancet. 2021;398:1002–14.10.1016/S0140-6736(21)01206-XSearch in Google Scholar PubMed
[114] Yoneda K, Imanishi N, Ichiki Y, Tanaka F. Immune checkpoint inhibitors (ICIs) in non-small cell lung cancer (NSCLC). J UOEH. 2018;40:173–89.10.7888/juoeh.40.173Search in Google Scholar PubMed
[115] Dave S, Yang K, Schnickel GT, Kono Y, Delebecque F, Arellano D, et al. The impact of treatment of hepatocellular carcinoma with immune checkpoint inhibitors on pre- and post-liver transplant outcomes. Transplantation. 2022;106:e308–9.10.1097/TP.0000000000004108Search in Google Scholar PubMed PubMed Central
[116] Topalian SL, Forde PM, Emens LA, Yarchoan M, Smith KN, Pardoll DM. Neoadjuvant immune checkpoint blockade: A window of opportunity to advance cancer immunotherapy. Cancer Cell. 2023;41:1551–66.10.1016/j.ccell.2023.07.011Search in Google Scholar PubMed PubMed Central
[117] Koerner J, Horvath D, Herrmann VL, MacKerracher A, Gander B, Yagita H, et al. PLGA-particle vaccine carrying TLR3/RIG-I ligand Riboxxim synergizes with immune checkpoint blockade for effective anti-cancer immunotherapy. Nat Commun. 2021;12:2935.10.1038/s41467-021-23244-3Search in Google Scholar PubMed PubMed Central
[118] Li Y, Wu X, Sheng C, Liu H, Liu H, Tang Y, et al. IGSF8 is an innate immune checkpoint and cancer immunotherapy target. Cell. 2024;187:2703–16.e23.10.1016/j.cell.2024.03.039Search in Google Scholar PubMed
[119] Bai J, Liang P, Li Q, Feng R, Liu J. Cancer immunotherapy - immune checkpoint inhibitors in hepatocellular carcinoma. Recent Pat Anticancer Drug Discov. 2021;16:239–48.10.2174/1574892816666210212145107Search in Google Scholar PubMed
[120] Sharma P, Goswami S, Raychaudhuri D, Siddiqui BA, Singh P, Nagarajan A, et al. Immune checkpoint therapy – current perspectives and future directions. Cell. 2023;186:1652–69.10.1016/j.cell.2023.03.006Search in Google Scholar PubMed
[121] Kinslow CJ, Rae AI, Taparra K, Kumar P, Siegelin MD, Grinband J, et al. MGMT promoter methylation predicts overall survival after chemotherapy for 1p/19q-codeleted gliomas. Clin Cancer Res. 2023;29:4399–407.10.1158/1078-0432.CCR-23-1295Search in Google Scholar PubMed PubMed Central
[122] Kocikowski M, Dziubek K, Parys M. Hyperprogression under immune checkpoint-based immunotherapy – current understanding, the role of pd-1/pd-l1 tumour-intrinsic signalling, future directions and a potential large animal model. Cancers (Basel). 2020;12:1–19.10.3390/cancers12040804Search in Google Scholar PubMed PubMed Central
[123] Wei Z, Zhang Y. Immune cells in hyperprogressive disease under immune checkpoint-based immunotherapy. Cells. 2022;11:1–19.10.3390/cells11111758Search in Google Scholar PubMed PubMed Central
[124] Lutgens E, Mulder WJM, CHECKPOINT ATHERO c. CHECKPOINT ATHERO: developing immune checkpoint-based therapeutics for atherosclerosis. Eur Heart J. 2023;44:1010–2.10.1093/eurheartj/ehac793Search in Google Scholar PubMed
[125] Khan M, Arooj S, Wang H. NK cell-based immune checkpoint inhibition. Front Immunol. 2020;11:167. 10.3389/fimmu.2020.00167.Search in Google Scholar PubMed PubMed Central
[126] Wu Q, Qian W, Sun X, Jiang S. Small-molecule inhibitors, immune checkpoint inhibitors, and more: FDA-approved novel therapeutic drugs for solid tumors from 1991 to 2021. J Hematol Oncol. 2022;15:143.10.1186/s13045-022-01362-9Search in Google Scholar PubMed PubMed Central
[127] Huang Y, Liang D, Liu J, Zeng J, Zeng Y. The breakthroughs in cancer immune checkpoint based therapy: a review of development in immune checkpoint study and its application. Comb Chem High Throughput Screen. 2017;20:430–9. 10.2174/1386207320666170315121728.Search in Google Scholar PubMed
[128] Akkın S, Varan G, Bilensoy E. A review on cancer immunotherapy and applications of nanotechnology to chemoimmunotherapy of different cancers. Molecules. 2021;26:3382.10.3390/molecules26113382Search in Google Scholar PubMed PubMed Central
[129] Yang M, Li J, Gu P, Fan X. The application of nanoparticles in cancer immunotherapy: Targeting tumor microenvironment. Bioact Mater. 2021;6:1973–87.10.1016/j.bioactmat.2020.12.010Search in Google Scholar PubMed PubMed Central
[130] Tawbi HA, Forsyth PA, Algazi A, Hamid O, Hodi FS, Moschos SJ, et al. Combined nivolumab and ipilimumab in melanoma metastatic to the brain. N Engl J Med. 2018;379:722–30.10.1056/NEJMoa1805453Search in Google Scholar PubMed PubMed Central
[131] Hodi FS, Chiarion-Sileni V, Gonzalez R, Grob JJ, Rutkowski P, Cowey CL, et al. Nivolumab plus ipilimumab or nivolumab alone versus ipilimumab alone in advanced melanoma (CheckMate 067): 4-year outcomes of a multicentre, randomised, phase 3 trial. Lancet Oncol. 2018;19:1480–92.10.1016/S1470-2045(18)30700-9Search in Google Scholar PubMed
[132] Zhao Y, Chen G, Chen J, Zhuang L, Du Y, Yu Q, et al. AK112, a novel PD-1/VEGF bispecific antibody, in combination with chemotherapy in patients with advanced non-small cell lung cancer (NSCLC): an open-label, multicenter, phase II trial. eClinicalMedicine. 2023;62:102106.10.1016/j.eclinm.2023.102106Search in Google Scholar PubMed PubMed Central
[133] Kato D, Yaguchi T, Iwata T, Katoh Y, Morii K, Tsubota K, et al. GPC1 specific CAR-T cells eradicate established solid tumor without adverse effects and synergize with anti-PD-1 Ab. Elife. 2020;9:e49392. 10.7554/eLife.49392.Search in Google Scholar PubMed PubMed Central
[134] Wu W, Chia T, Lu J, Li X, Guan J, Li Y, et al. IL-2Rα-biased agonist enhances antitumor immunity by invigorating tumor-infiltrating CD25 + CD8 + T cells. Nat Cancer. 2023;4:1309–25.10.1038/s43018-023-00612-0Search in Google Scholar PubMed
[135] Sun L, Funchain P, Song JM, Rayman P, Tannenbaum C, Ko J, et al. Talimogene Laherparepvec combined with anti-PD-1 based immunotherapy for unresectable stage III-IV melanoma: a case series. J Immunother Cancer. 2018;6:36.10.1186/s40425-018-0337-7Search in Google Scholar PubMed PubMed Central
[136] Shin J, Chung J-H, Kim SH, Lee KS, Suh KJ, Lee JY, et al. Effect of platinum-based chemotherapy on PD-L1 expression on tumor cells in non-small cell lung cancer. Cancer Res Treat. 2019;51:1086–97.10.4143/crt.2018.537Search in Google Scholar PubMed PubMed Central
[137] MaruYama T, Chen W, Shibata H. TGF-β and cancer immunotherapy. Biol Pharm Bull. 2022;45:155–61.10.1248/bpb.b21-00966Search in Google Scholar PubMed
[138] Torres ETR, Emens LA. Emerging combination immunotherapy strategies for breast cancer: dual immune checkpoint modulation, antibody–drug conjugates and bispecific antibodies. Breast Cancer Res Treat. 2022;191:291–302.10.1007/s10549-021-06423-0Search in Google Scholar PubMed
[139] Sperandio RC, Pestana RC, Miyamura BV, Kaseb AO. Hepatocellular Carcinoma Immunotherapy. Annu Rev Med. 2022;73:267–78.10.1146/annurev-med-042220-021121Search in Google Scholar PubMed
[140] Högner A, Moehler M. Immunotherapy in gastric cancer. Curr Oncol. 2022;29:1559–74.10.3390/curroncol29030131Search in Google Scholar PubMed PubMed Central
[141] Kraehenbuehl L, Weng C-H, Eghbali S, Wolchok JD, Merghoub T. Enhancing immunotherapy in cancer by targeting emerging immunomodulatory pathways. Nat Rev Clin Oncol. 2022;19:37–50.10.1038/s41571-021-00552-7Search in Google Scholar PubMed
[142] Krzyszczyk P, Acevedo A, Davidoff EJ, Timmins LM, Marrero-Berrios I, Patel M, et al. The growing role of precision and personalized medicine for cancer treatment. Technology. 2018;6:79–100.10.1142/S2339547818300020Search in Google Scholar PubMed PubMed Central
[143] Shin SH, Bode AM, Dong Z. Precision medicine: the foundation of future cancer therapeutics. npj Precis Oncol. 2017;1:12.10.1038/s41698-017-0016-zSearch in Google Scholar PubMed PubMed Central
[144] Dey A, Mitra A, Pathak S, Prasad S, Zhang AS, Zhang H, et al. Recent advancements, limitations, and future perspectives of the use of personalized medicine in treatment of colon cancer. Technol Cancer Res Treat. 2023;22:15330338231178403. 10.1177/15330338231178403.Search in Google Scholar PubMed PubMed Central
[145] Verma M. Personalized medicine and cancer. J Pers Med. 2012;2:1–14.10.3390/jpm2010001Search in Google Scholar PubMed PubMed Central
[146] Faghfuri E. Recent advances in personalized cancer immunotherapy with immune checkpoint inhibitors, T cells and vaccines. Per Med. 2024;21:45–57.10.2217/pme-2023-0054Search in Google Scholar PubMed
[147] Wang Y, Wang M, Wu HX, Xu RH. Advancing to the era of cancer immunotherapy. Cancer Commun. 2021;41:803–29.10.1002/cac2.12178Search in Google Scholar PubMed PubMed Central
[148] Sahin U, Türeci Ö. Personalized vaccines for cancer immunotherapy. Science. 2018;359:1355–60.10.1126/science.aar7112Search in Google Scholar PubMed
[149] Shuford RA, Cairns AL, Moaven O. Precision approaches in the management of colorectal cancer: current evidence and latest advancements towards individualizing the treatment. Cancers (Basel). 2020;12:3481.10.3390/cancers12113481Search in Google Scholar PubMed PubMed Central
[150] Garg P, Pareek S, Kulkarni P, Horne D, Salgia R, Singhal SS. Next-generation immunotherapy: advancing clinical applications in cancer treatment. J Clin Med. 2024;13:6537.10.3390/jcm13216537Search in Google Scholar PubMed PubMed Central
[151] Kruger S, Ilmer M, Kobold S, Cadilha BL, Endres S, Ormanns S, et al. Advances in cancer immunotherapy 2019 – latest trends. J Exp Clin Cancer Res. 2019;38:268.10.1186/s13046-019-1266-0Search in Google Scholar PubMed PubMed Central
[152] Passaro A, Al Bakir M, Hamilton EG, Diehn M, André F, Roy-Chowdhuri S, et al. Cancer biomarkers: Emerging trends and clinical implications for personalized treatment. Cell. 2024;187:1617–35.10.1016/j.cell.2024.02.041Search in Google Scholar PubMed PubMed Central
[153] Wang C, Ye Y, Hu Q, Bellotti A, Gu Z. Tailoring biomaterials for cancer immunotherapy: emerging trends and future outlook. Adv Mater. 2017;29:1606036. 10.1002/adma.201606036.Search in Google Scholar PubMed
[154] Yuan J, Hegde PS, Clynes R, Foukas PG, Harari A, Kleen TO, et al. Novel technologies and emerging biomarkers for personalized cancer immunotherapy. J Immunother Cancer. 2016;4:3.10.1186/s40425-016-0107-3Search in Google Scholar PubMed PubMed Central
[155] Nakajima H, Nakatsura T. Towards the era of immune checkpoint inhibitors and personalized cancer immunotherapy. Immunol Med. 2021;44:10–5.10.1080/25785826.2020.1785654Search in Google Scholar PubMed
[156] Islam N, Budvytyte L, Khera N, Hilal T. Disparities in clinical trial enrollment–focus on CAR-T and bispecific antibody therapies. Curr Hematol Malig Rep. 2025;20:1.10.1007/s11899-024-00747-6Search in Google Scholar PubMed PubMed Central
[157] Haddad R, Concha-Benavente F, Blumenschein G Jr, Fayette J, Guigay J, Colevas AD, et al. Nivolumab treatment beyond RECIST‐defined progression in recurrent or metastatic squamous cell carcinoma of the head and neck in CheckMate 141: A subgroup analysis of a randomized phase 3 clinical trial. Cancer. 2019;125:3208–18.10.1002/cncr.32190Search in Google Scholar PubMed PubMed Central
[158] Gandara DR, von Pawel J, Mazieres J, Sullivan R, Helland Å, Han JY, et al. Atezolizumab treatment beyond progression in advanced NSCLC: Results from the randomized, phase III OAK study. J Thorac Oncol. 2018;13:1906–18.10.1016/j.jtho.2018.08.2027Search in Google Scholar PubMed
[159] Li R, Wang C, Liu L, Du C, Cao S, Yu J, et al. Autologous cytokine-induced killer cell immunotherapy in lung cancer: a phase II clinical study. Cancer Immunol Immunother. 2012;61:2125–33.10.1007/s00262-012-1260-2Search in Google Scholar PubMed PubMed Central
[160] Lodge PA, Jones LA, Bader RA, Murphy GP, Salgaller ML. Dendritic cell-based immunotherapy of prostate cancer: Immune monitoring of a phase II clinical trial. Cancer Res. 2000;60:829–33.Search in Google Scholar
[161] Long GV, Weber JS, Larkin J, Atkinson V, Grob JJ, Schadendorf D, et al. Nivolumab for patients with advanced melanoma treated beyond progression. JAMA Oncol. 2017;3:1511–9.10.1001/jamaoncol.2017.1588Search in Google Scholar PubMed PubMed Central
[162] McDermott DF, Lee J-L, Bjarnason GA, Larkin J, Gafanov RA, Kochenderfer MD, et al. Open-label, single-arm phase II study of pembrolizumab monotherapy as first-line therapy in patients with advanced clear cell renal cell carcinoma. J Clin Oncol. 2021;39:1020–8.10.1200/JCO.20.02363Search in Google Scholar PubMed PubMed Central
[163] Sebastian M, Schröder A, Scheel B, Hong HS, Muth A, von Boehmer L, et al. A phase I/IIa study of the mRNA-based cancer immunotherapy CV9201 in patients with stage IIIB/IV non-small cell lung cancer. Cancer Immunol Immunother. 2019;68:799–812.10.1007/s00262-019-02315-xSearch in Google Scholar PubMed PubMed Central
[164] Papachristofilou A, Hipp MM, Klinkhardt U, Früh M, Sebastian M, Weiss C, et al. Phase Ib evaluation of a self-adjuvanted protamine formulated mRNA-based active cancer immunotherapy, BI1361849 (CV9202), combined with local radiation treatment in patients with stage IV non-small cell lung cancer. J Immunother Cancer. 2019;7:38.10.1186/s40425-019-0520-5Search in Google Scholar PubMed PubMed Central
[165] Gainor JF, Patel MR, Weber JS, Gutierrez M, Bauman JE, Clarke JM, et al. T-cell responses to individualized neoantigen therapy mRNA-4157 (V940) alone or in combination with pembrolizumab in the phase 1 KEYNOTE-603 study. Cancer Discov. 2024;14:2209–23.10.1158/2159-8290.CD-24-0158Search in Google Scholar PubMed
[166] Brahmer JR, Drake CG, Wollner I, Powderly JD, Picus J, Sharfman WH, et al. Phase 1/2 study of mRNA-4359 administered alone and in combination with immune checkpoint blockade in adult participants with advanced solid tumors. J Clin Oncol. 2023;41:TPS2676–723.10.1200/JCO.2023.41.16_suppl.TPS2676Search in Google Scholar
[167] Xie J, Luo X, Deng X, Tang Y, Tian W, Cheng H, et al. Advances in artificial intelligence to predict cancer immunotherapy efficacy. Front Immunol. 2023;13:1076883. 10.3389/fimmu.2022.1076883.Search in Google Scholar PubMed PubMed Central
[168] Li T, Li Y, Zhu X, He Y, Wu Y, Ying T, et al. Artificial intelligence in cancer immunotherapy: Applications in neoantigen recognition, antibody design and immunotherapy response prediction. Semin Cancer Biol. 2023;91:50–69.10.1016/j.semcancer.2023.02.007Search in Google Scholar PubMed
[169] Zhou X, Qu M, Tebon P, Jiang X, Wang C, Xue Y, et al. Screening cancer immunotherapy: when engineering approaches meet artificial intelligence. Adv Sci. 2020;7:2001447. 10.1002/advs.202001447.Search in Google Scholar PubMed PubMed Central
[170] Ghaffari Laleh N, Ligero M, Perez-Lopez R, Kather JN. Facts and hopes on the use of artificial intelligence for predictive immunotherapy biomarkers in cancer. Clin Cancer Res. 2023;29:316–23.10.1158/1078-0432.CCR-22-0390Search in Google Scholar PubMed
[171] Xiang W, Yu L, Chen X, Herold MJ. Artificial intelligence in cancer immunotherapy: Navigating challenges and unlocking opportunities. Engineering. 2024;44:12–6. 10.1016/j.eng.2024.12.014.Search in Google Scholar
[172] Jiang J, Ding Y, Wu M, Chen Y, Lyu X, Lu J, et al. Integrated genomic analysis identifies a genetic mutation model predicting response to immune checkpoint inhibitors in melanoma. Cancer Med. 2020;9:8498–518.10.1002/cam4.3481Search in Google Scholar PubMed PubMed Central
[173] He Y, Wang X. Identifying biomarkers associated with immunotherapy response in melanoma by multi-omics analysis. Comput Biol Med. 2023;167:107591.10.1016/j.compbiomed.2023.107591Search in Google Scholar PubMed
[174] Li J, Xiao Z, Wang D, Jia L, Nie S, Zeng X, et al. The screening, identification, design and clinical application of tumor-specific neoantigens for TCR-T cells. Mol Cancer. 2023;22:141.10.1186/s12943-023-01844-5Search in Google Scholar PubMed PubMed Central
[175] Mei T, Wang T, Zhou Q. Multi-omics and artificial intelligence predict clinical outcomes of immunotherapy in non-small cell lung cancer patients. Clin Exp Med. 2024;24:60.10.1007/s10238-024-01324-0Search in Google Scholar PubMed PubMed Central
[176] Ni K, Lan G, Chan C, Quigley B, Lu K, Aung T, et al. Nanoscale metal-organic frameworks enhance radiotherapy to potentiate checkpoint blockade immunotherapy. Nat Commun. 2018;9:2351.10.1038/s41467-018-04703-wSearch in Google Scholar PubMed PubMed Central
[177] Tang S, Li S, Tang B, Wang X, Xiao Y, Cheke RA. Hormetic and synergistic effects of cancer treatments revealed by modelling combinations of radio - or chemotherapy with immunotherapy. BMC Cancer. 2023;23:1040.10.1186/s12885-023-11542-6Search in Google Scholar PubMed PubMed Central
[178] Renaude E, Kroemer M, Borg C, Peixoto P, Hervouet E, Loyon R, et al. Epigenetic reprogramming of CD4+ helper T cells as a strategy to improve anticancer immunotherapy. Front Immunol. 2021;12:669992. 10.3389/fimmu.2021.669992.Search in Google Scholar PubMed PubMed Central
[179] Sarivalasis A, Boudousquié C, Balint K, Stevenson BJ, Gannon PO, Iancu EM, et al. A phase I/II trial comparing autologous dendritic cell vaccine pulsed either with personalized peptides (PEP-DC) or with tumor lysate (OC-DC) in patients with advanced high-grade ovarian serous carcinoma. J Transl Med. 2019;17:391.10.1186/s12967-019-02133-wSearch in Google Scholar PubMed PubMed Central
[180] Shaker M, Greenhawt M. Estimation of health and economic benefits of commercial peanut immunotherapy products. JAMA Netw Open. 2019;2:e193242.10.1001/jamanetworkopen.2019.3242Search in Google Scholar PubMed PubMed Central
[181] Shahzadi M, Rafique H, Waheed A, Naz H, Waheed A, Zokirova FR, et al. Artificial intelligence for chimeric antigen receptor-based therapies: a comprehensive review of current applications and future perspectives. Ther Adv Vaccines Immunother. 2024;12:25151355241305856. 10.1177/25151355241305856.Search in Google Scholar PubMed PubMed Central
[182] Kim JY, Bang H, Noh S-J, Choi JK. DeepNeo: a webserver for predicting immunogenic neoantigens. Nucleic Acids Res. 2023;51:W134–40.10.1093/nar/gkad275Search in Google Scholar PubMed PubMed Central
[183] Liu X-X, Wei Y, Xu M, Song Q, Fong S. Deepneoagnet: Enhancing cancer immunotherapy with deep learning for precise neoantigen prediction and immunogenicity assessment. 2024. 10.2139/ssrn.4984357.Search in Google Scholar
[184] Shen L-C, Zhang Y, Wang Z, Littler DR, Liu Y, Tang J, et al. Self-iterative multiple-instance learning enables the prediction of CD4+ T cell immunogenic epitopes. Nat Mach Intell. 2025;7:1250–65. 10.1038/s42256-025-01073-z.Search in Google Scholar
[185] Yang Q, Xu L, Dong W, Li X, Wang K, Dong S, et al. HLAIImaster: a deep learning method with adaptive domain knowledge predicts HLA II neoepitope immunogenic responses. Brief Bioinform. 2024;25:bbae302. 10.1093/bib/bbae302.Search in Google Scholar PubMed PubMed Central
[186] Wang Z, Lin W, Chen Y. FusionHLAII: A hierarchical model for predicting HLA II–peptide interactions. In 2025 4th International Symposium on Computer Applications and Information Technology (ISCAIT). IEEE; p. 1208–16.10.1109/ISCAIT64916.2025.11010642Search in Google Scholar
[187] Long X, Yang Q, Dong W, Li X, Wang K, Dong S, et al. THLANet: A deep learning framework for predicting TCR-pHLA binding in immunotherapy applications. PLOS Comput Biol. 2025;21(9):e1013050. 10.1101/2025.04.14.648678.Search in Google Scholar
[188] Jayawickrama SM, Ranaweera PM, Pradeep RGGR, Jayasinghe YA, Senevirathna K, Hilmi AJ, et al. Developments and future prospects of personalized medicine in head and neck squamous cell carcinoma diagnoses and treatments. Cancer Rep. 2024;7:2045. 10.1002/cnr2.2045.Search in Google Scholar PubMed PubMed Central
[189] Morand S, Devanaboyina M, Staats H, Stanbery L, Nemunaitis J. Ovarian cancer immunotherapy and personalized medicine. Int J Mol Sci. 2021;22:6532.10.3390/ijms22126532Search in Google Scholar PubMed PubMed Central
[190] Zhang Y, Chen T-T, Li X, Lan AL, Ji PF, Zhu YJ, et al. Advances and challenges in neoantigen prediction for cancer immunotherapy. Front Immunol. 2025;16:1617654. 10.3389/fimmu.2025.1617654.Search in Google Scholar PubMed PubMed Central
[191] Bulashevska A, Nacsa Z, Lang F, Braun M, Machyna M, Diken M, et al. Artificial intelligence and neoantigens: paving the path for precision cancer immunotherapy. Front Immunol. 2024;15:1394003. 10.3389/fimmu.2024.1394003.Search in Google Scholar PubMed PubMed Central
© 2025 the author(s), published by De Gruyter
This work is licensed under the Creative Commons Attribution 4.0 International License.
Articles in the same Issue
- Safety assessment and modulation of hepatic CYP3A4 and UGT enzymes by Glycyrrhiza glabra aqueous extract in female Sprague–Dawley rats
- Adult-onset Still’s disease with hemophagocytic lymphohistiocytosis and minimal change disease
- Role of DZ2002 in reducing corneal graft rejection in rats by influencing Th17 activation via inhibition of the PI3K/AKT pathway and downregulation of TRAF1
- Biomedical Sciences
- Mechanism of triptolide regulating proliferation and apoptosis of hepatoma cells by inhibiting JAK/STAT pathway
- Maslinic acid improves mitochondrial function and inhibits oxidative stress and autophagy in human gastric smooth muscle cells
- Comparative analysis of inflammatory biomarkers for the diagnosis of neonatal sepsis: IL-6, IL-8, SAA, CRP, and PCT
- Post-pandemic insights on COVID-19 and premature ovarian insufficiency
- Proteome differences of dental stem cells between permanent and deciduous teeth by data-independent acquisition proteomics
- Optimizing a modified cetyltrimethylammonium bromide protocol for fungal DNA extraction: Insights from multilocus gene amplification
- Preliminary analysis of the role of small hepatitis B surface proteins mutations in the pathogenesis of occult hepatitis B infection via the endoplasmic reticulum stress-induced UPR-ERAD pathway
- Efficacy of alginate-coated gold nanoparticles against antibiotics-resistant Staphylococcus and Streptococcus pathogens of acne origins
- Battling COVID-19 leveraging nanobiotechnology: Gold and silver nanoparticle–B-escin conjugates as SARS-CoV-2 inhibitors
- Neurodegenerative diseases and neuroinflammation-induced apoptosis
- Impact of fracture fixation surgery on cognitive function and the gut microbiota in mice with a history of stroke
- COLEC10: A potential tumor suppressor and prognostic biomarker in hepatocellular carcinoma through modulation of EMT and PI3K-AKT pathways
- High-temperature requirement serine protease A2 inhibitor UCF-101 ameliorates damaged neurons in traumatic brain-injured rats by the AMPK/NF-κB pathway
- SIK1 inhibits IL-1β-stimulated cartilage apoptosis and inflammation in vitro through the CRTC2/CREB1 signaling
- Rutin–chitooligosaccharide complex: Comprehensive evaluation of its anti-inflammatory and analgesic properties in vitro and in vivo
- Knockdown of Aurora kinase B alleviates high glucose-triggered trophoblast cells damage and inflammation during gestational diabetes
- Calcium-sensing receptors promoted Homer1 expression and osteogenic differentiation in bone marrow mesenchymal stem cells
- ABI3BP can inhibit the proliferation, invasion, and epithelial–mesenchymal transition of non-small-cell lung cancer cells
- Changes in blood glucose and metabolism in hyperuricemia mice
- Rapid detection of the GJB2 c.235delC mutation based on CRISPR-Cas13a combined with lateral flow dipstick
- IL-11 promotes Ang II-induced autophagy inhibition and mitochondrial dysfunction in atrial fibroblasts
- Short-chain fatty acid attenuates intestinal inflammation by regulation of gut microbial composition in antibiotic-associated diarrhea
- Application of metagenomic next-generation sequencing in the diagnosis of pathogens in patients with diabetes complicated by community-acquired pneumonia
- NAT10 promotes radiotherapy resistance in non-small cell lung cancer by regulating KPNB1-mediated PD-L1 nuclear translocation
- Phytol-mixed micelles alleviate dexamethasone-induced osteoporosis in zebrafish: Activation of the MMP3–OPN–MAPK pathway-mediating bone remodeling
- Association between TGF-β1 and β-catenin expression in the vaginal wall of patients with pelvic organ prolapse
- Primary pleomorphic liposarcoma involving bilateral ovaries: Case report and literature review
- Effects of de novo donor-specific Class I and II antibodies on graft outcomes after liver transplantation: A pilot cohort study
- Sleep architecture in Alzheimer’s disease continuum: The deep sleep question
- Ephedra fragilis plant extract: A groundbreaking corrosion inhibitor for mild steel in acidic environments – electrochemical, EDX, DFT, and Monte Carlo studies
- Langerhans cell histiocytosis in an adult patient with upper jaw and pulmonary involvement: A case report
- Inhibition of mast cell activation by Jaranol-targeted Pirin ameliorates allergic responses in mouse allergic rhinitis
- Aeromonas veronii-induced septic arthritis of the hip in a child with acute lymphoblastic leukemia
- Clusterin activates the heat shock response via the PI3K/Akt pathway to protect cardiomyocytes from high-temperature-induced apoptosis
- Research progress on fecal microbiota transplantation in tumor prevention and treatment
- Low-pressure exposure influences the development of HAPE
- Stigmasterol alleviates endplate chondrocyte degeneration through inducing mitophagy by enhancing PINK1 mRNA acetylation via the ESR1/NAT10 axis
- AKAP12, mediated by transcription factor 21, inhibits cell proliferation, metastasis, and glycolysis in lung squamous cell carcinoma
- Association between PAX9 or MSX1 gene polymorphism and tooth agenesis risk: A meta-analysis
- A case of bloodstream infection caused by Neisseria gonorrhoeae
- Case of nasopharyngeal tuberculosis complicated with cervical lymph node and pulmonary tuberculosis
- p-Cymene inhibits pro-fibrotic and inflammatory mediators to prevent hepatic dysfunction
- GFPT2 promotes paclitaxel resistance in epithelial ovarian cancer cells via activating NF-κB signaling pathway
- Transfer RNA-derived fragment tRF-36 modulates varicose vein progression via human vascular smooth muscle cell Notch signaling
- RTA-408 attenuates the hepatic ischemia reperfusion injury in mice possibly by activating the Nrf2/HO-1 signaling pathway
- Decreased serum TIMP4 levels in patients with rheumatoid arthritis
- Sirt1 protects lupus nephritis by inhibiting the NLRP3 signaling pathway in human glomerular mesangial cells
- Sodium butyrate aids brain injury repair in neonatal rats
- Interaction of MTHFR polymorphism with PAX1 methylation in cervical cancer
- Convallatoxin inhibits proliferation and angiogenesis of glioma cells via regulating JAK/STAT3 pathway
- The effect of the PKR inhibitor, 2-aminopurine, on the replication of influenza A virus, and segment 8 mRNA splicing
- Effects of Ire1 gene on virulence and pathogenicity of Candida albicans
- Small cell lung cancer with small intestinal metastasis: Case report and literature review
- GRB14: A prognostic biomarker driving tumor progression in gastric cancer through the PI3K/AKT signaling pathway by interacting with COBLL1
- 15-Lipoxygenase-2 deficiency induces foam cell formation that can be restored by salidroside through the inhibition of arachidonic acid effects
- FTO alleviated the diabetic nephropathy progression by regulating the N6-methyladenosine levels of DACT1
- Clinical relevance of inflammatory markers in the evaluation of severity of ulcerative colitis: A retrospective study
- Zinc valproic acid complex promotes osteoblast differentiation and exhibits anti-osteoporotic potential
- Primary pulmonary synovial sarcoma in the bronchial cavity: A case report
- Metagenomic next-generation sequencing of alveolar lavage fluid improves the detection of pulmonary infection
- Uterine tumor resembling ovarian sex cord tumor with extensive rhabdoid differentiation: A case report
- Genomic analysis of a novel ST11(PR34365) Clostridioides difficile strain isolated from the human fecal of a CDI patient in Guizhou, China
- Effects of tiered cardiac rehabilitation on CRP, TNF-α, and physical endurance in older adults with coronary heart disease
- Changes in T-lymphocyte subpopulations in patients with colorectal cancer before and after acupoint catgut embedding acupuncture observation
- Modulating the tumor microenvironment: The role of traditional Chinese medicine in improving lung cancer treatment
- Alterations of metabolites related to microbiota–gut–brain axis in plasma of colon cancer, esophageal cancer, stomach cancer, and lung cancer patients
- Research on individualized drug sensitivity detection technology based on bio-3D printing technology for precision treatment of gastrointestinal stromal tumors
- CEBPB promotes ulcerative colitis-associated colorectal cancer by stimulating tumor growth and activating the NF-κB/STAT3 signaling pathway
- Oncolytic bacteria: A revolutionary approach to cancer therapy
- A de novo meningioma with rapid growth: A possible malignancy imposter?
- Diagnosis of secondary tuberculosis infection in an asymptomatic elderly with cancer using next-generation sequencing: Case report
- Hesperidin and its zinc(ii) complex enhance osteoblast differentiation and bone formation: In vitro and in vivo evaluations
- Research progress on the regulation of autophagy in cardiovascular diseases by chemokines
- Anti-arthritic, immunomodulatory, and inflammatory regulation by the benzimidazole derivative BMZ-AD: Insights from an FCA-induced rat model
- Immunoassay for pyruvate kinase M1/2 as an Alzheimer’s biomarker in CSF
- The role of HDAC11 in age-related hearing loss: Mechanisms and therapeutic implications
- Evaluation and application analysis of animal models of PIPNP based on data mining
- Therapeutic approaches for liver fibrosis/cirrhosis by targeting pyroptosis
- Fabrication of zinc oxide nanoparticles using Ruellia tuberosa leaf extract induces apoptosis through P53 and STAT3 signalling pathways in prostate cancer cells
- Haplo-hematopoietic stem cell transplantation and immunoradiotherapy for severe aplastic anemia complicated with nasopharyngeal carcinoma: A case report
- Modulation of the KEAP1-NRF2 pathway by Erianin: A novel approach to reduce psoriasiform inflammation and inflammatory signaling
- The expression of epidermal growth factor receptor 2 and its relationship with tumor-infiltrating lymphocytes and clinical pathological features in breast cancer patients
- Innovations in MALDI-TOF Mass Spectrometry: Bridging modern diagnostics and historical insights
- BAP1 complexes with YY1 and RBBP7 and its downstream targets in ccRCC cells
- Hypereosinophilic syndrome with elevated IgG4 and T-cell clonality: A report of two cases
- Electroacupuncture alleviates sciatic nerve injury in sciatica rats by regulating BDNF and NGF levels, myelin sheath degradation, and autophagy
- Polydatin prevents cholesterol gallstone formation by regulating cholesterol metabolism via PPAR-γ signaling
- RNF144A and RNF144B: Important molecules for health
- Analysis of the detection rate and related factors of thyroid nodules in the healthy population
- Artesunate inhibits hepatocellular carcinoma cell migration and invasion through OGA-mediated O-GlcNAcylation of ZEB1
- Endovascular management of post-pancreatectomy hemorrhage caused by a hepatic artery pseudoaneurysm: Case report and review of the literature
- Efficacy and safety of anti-PD-1/PD-L1 antibodies in patients with relapsed refractory diffuse large B-cell lymphoma: A meta-analysis
- SATB2 promotes humeral fracture healing in rats by activating the PI3K/AKT pathway
- Overexpression of the ferroptosis-related gene, NFS1, corresponds to gastric cancer growth and tumor immune infiltration
- Understanding risk factors and prognosis in diabetic foot ulcers
- Atractylenolide I alleviates the experimental allergic response in mice by suppressing TLR4/NF-kB/NLRP3 signalling
- FBXO31 inhibits the stemness characteristics of CD147 (+) melanoma stem cells
- Immune molecule diagnostics in colorectal cancer: CCL2 and CXCL11
- Inhibiting CXCR6 promotes senescence of activated hepatic stellate cells with limited proinflammatory SASP to attenuate hepatic fibrosis
- Cadmium toxicity, health risk and its remediation using low-cost biochar adsorbents
- Pulmonary cryptococcosis with headache as the first presentation: A case report
- Solitary pulmonary metastasis with cystic airspaces in colon cancer: A rare case report
- RUNX1 promotes denervation-induced muscle atrophy by activating the JUNB/NF-κB pathway and driving M1 macrophage polarization
- Morphometric analysis and immunobiological investigation of Indigofera oblongifolia on the infected lung with Plasmodium chabaudi
- The NuA4/TIP60 histone-modifying complex and Hr78 modulate the Lobe2 mutant eye phenotype
- Experimental study on salmon demineralized bone matrix loaded with recombinant human bone morphogenetic protein-2: In vitro and in vivo study
- A case of IgA nephropathy treated with a combination of telitacicept and half-dose glucocorticoids
- Analgesic and toxicological evaluation of cannabidiol-rich Moroccan Cannabis sativa L. (Khardala variety) extract: Evidence from an in vivo and in silico study
- Wound healing and signaling pathways
- Combination of immunotherapy and whole-brain radiotherapy on prognosis of patients with multiple brain metastases: A retrospective cohort study
- To explore the relationship between endometrial hyperemia and polycystic ovary syndrome
- Research progress on the impact of curcumin on immune responses in breast cancer
- Biogenic Cu/Ni nanotherapeutics from Descurainia sophia (L.) Webb ex Prantl seeds for the treatment of lung cancer
- Dapagliflozin attenuates atrial fibrosis via the HMGB1/RAGE pathway in atrial fibrillation rats
- Glycitein alleviates inflammation and apoptosis in keratinocytes via ROS-associated PI3K–Akt signalling pathway
- ADH5 inhibits proliferation but promotes EMT in non-small cell lung cancer cell through activating Smad2/Smad3
- Apoptotic efficacies of AgNPs formulated by Syzygium aromaticum leaf extract on 32D-FLT3-ITD human leukemia cell line with PI3K/AKT/mTOR signaling pathway
- Novel cuproptosis-related genes C1QBP and PFKP identified as prognostic and therapeutic targets in lung adenocarcinoma
- Bee venom promotes exosome secretion and alters miRNA cargo in T cells
- Treatment of pure red cell aplasia in a chronic kidney disease patient with roxadustat: A case report
- Comparative bioinformatics analysis of the Wnt pathway in breast cancer: Selection of novel biomarker panels associated with ER status
- Kynurenine facilitates renal cell carcinoma progression by suppressing M2 macrophage pyroptosis through inhibition of CASP1 cleavage
- RFX5 promotes the growth, motility, and inhibits apoptosis of gastric adenocarcinoma cells through the SIRT1/AMPK axis
- ALKBH5 exacerbates early cardiac damage after radiotherapy for breast cancer via m6A demethylation of TLR4
- Phytochemicals of Roman chamomile: Antioxidant, anti-aging, and whitening activities of distillation residues
- Circadian gene Cry1 inhibits the tumorigenicity of hepatocellular carcinoma by the BAX/BCL2-mediated apoptosis pathway
- The TNFR-RIPK1/RIPK3 signalling pathway mediates the effect of lanthanum on necroptosis of nerve cells
- Longitudinal monitoring of autoantibody dynamics in patients with early-stage non-small-cell lung cancer undergoing surgery
- The potential role of rutin, a flavonoid, in the management of cancer through modulation of cell signaling pathways
- Construction of pectinase gene engineering microbe and its application in tobacco sheets
- Construction of a microbial abundance prognostic scoring model based on intratumoral microbial data for predicting the prognosis of lung squamous cell carcinoma
- Sepsis complicated by haemophagocytic lymphohistiocytosis triggered by methicillin-resistant Staphylococcus aureus and human herpesvirus 8 in an immunocompromised elderly patient: A case report
- Sarcopenia in liver transplantation: A comprehensive bibliometric study of current research trends and future directions
- Advances in cancer immunotherapy and future directions in personalized medicine
- Can coronavirus disease 2019 affect male fertility or cause spontaneous abortion? A two-sample Mendelian randomization analysis
- Heat stroke associated with novel leukaemia inhibitory factor receptor gene variant in a Chinese infant
- PSME2 exacerbates ulcerative colitis by disrupting intestinal barrier function and promoting autophagy-dependent inflammation
- Hyperosmolar hyperglycemic state with severe hypernatremia coexisting with central diabetes insipidus: A case report and literature review
- Efficacy and mechanism of escin in improving the tissue microenvironment of blood vessel walls via anti-inflammatory and anticoagulant effects: Implications for clinical practice
- Merkel cell carcinoma: Clinicopathological analysis of three patients and literature review
- Genetic variants in VWF exon 26 and their implications for type 1 Von Willebrand disease in a Saudi Arabian population
- Lipoxin A4 improves myocardial ischemia/reperfusion injury through the Notch1-Nrf2 signaling pathway
- High levels of EPHB2 expression predict a poor prognosis and promote tumor progression in endometrial cancer
- Knockdown of SHP-2 delays renal tubular epithelial cell injury in diabetic nephropathy by inhibiting NLRP3 inflammasome-mediated pyroptosis
- Exploring the toxicity mechanisms and detoxification methods of Rhizoma Paridis
- Concomitant gastric carcinoma and primary hepatic angiosarcoma in a patient: A case report
- YAP1 inhibition protects retinal vascular endothelial cells under high glucose by inhibiting autophagy
- Identification of secretory protein related biomarkers for primary biliary cholangitis based on machine learning and experimental validation
- Integrated genomic and clinical modeling for prognostic assessment of radiotherapy response in rectal neoplasms
- Stem cell-based approaches for glaucoma treatment: a mini review
- Bacteriophage titering by optical density means: KOTE assays
- Neutrophil-related signature characterizes immune landscape and predicts prognosis of esophageal squamous cell carcinoma
- Integrated bioinformatic analysis and machine learning strategies to identify new potential immune biomarkers for Alzheimer’s disease and their targeting prediction with geniposide
- TRIM21 accelerates ferroptosis in intervertebral disc degeneration by promoting SLC7A11 ubiquitination and degradation
- TRIM21 accelerates ferroptosis in intervertebral disc degeneration by promoting SLC7A11 ubiquitination and degradation
- Histone modification and non-coding RNAs in skin aging: emerging therapeutic avenues
- A multiplicative behavioral model of DNA replication initiation in cells
- Biogenic gold nanoparticles synthesized from Pergularia daemia leaves: a novel approach for nasopharyngeal carcinoma therapy
- Creutzfeldt-Jakob disease mimicking Hashimoto’s encephalopathy: steroid response followed by decline
- Impact of semaphorin, Sema3F, on the gene transcription and protein expression of CREB and its binding protein CREBBP in primary hippocampal neurons of rats
- Iron overloaded M0 macrophages regulate hematopoietic stem cell proliferation and senescence via the Nrf2/Keap1/HO-1 pathway
- Revisiting the link between NADPH oxidase p22phox C242T polymorphism and ischemic stroke risk: an updated meta-analysis
- Exercise training preferentially modulates α1D-adrenergic receptor expression in peripheral arteries of hypertensive rats
- Overexpression of HE4/WFDC2 gene in mice leads to keratitis and corneal opacity
- Tumoral calcinosis complicating CKD-MBD in hemodialysis: a case report
- Mechanism of KLF4 Inhibition of epithelial-mesenchymal transition in gastric cancer cells
- Dissecting the molecular mechanisms of T cell infiltration in psoriatic lesions via cell-cell communication and regulatory network analysis
- Circadian rhythm-based prognostic features predict immune infiltration and tumor microenvironment in molecular subtypes of hepatocellular carcinoma
- Ecology and Environmental Science
- Optimization and comparative study of Bacillus consortia for cellulolytic potential and cellulase enzyme activity
- The complete mitochondrial genome analysis of Haemaphysalis hystricis Supino, 1897 (Ixodida: Ixodidae) and its phylogenetic implications
- Epidemiological characteristics and risk factors analysis of multidrug-resistant tuberculosis among tuberculosis population in Huzhou City, Eastern China
- Indices of human impacts on landscapes: How do they reflect the proportions of natural habitats?
- Genetic analysis of the Siberian flying squirrel population in the northern Changbai Mountains, Northeast China: Insights into population status and conservation
- Diversity and environmental drivers of Suillus communities in Pinus sylvestris var. mongolica forests of Inner Mongolia
- Global assessment of the fate of nitrogen deposition in forest ecosystems: Insights from 15N tracer studies
- Fungal and bacterial pathogenic co-infections mainly lead to the assembly of microbial community in tobacco stems
- Influencing of coal industry related airborne particulate matter on ocular surface tear film injury and inflammatory factor expression in Sprague-Dawley rats
- Temperature-dependent development, predation, and life table of Sphaerophoria macrogaster (Thomson) (Diptera: Syrphidae) feeding on Myzus persicae (Sulzer) (Homoptera: Aphididae)
- Eleonora’s falcon trophic interactions with insects within its breeding range: A systematic review
- Agriculture
- Integrated analysis of transcriptome, sRNAome, and degradome involved in the drought-response of maize Zhengdan958
- Variation in flower frost tolerance among seven apple cultivars and transcriptome response patterns in two contrastingly frost-tolerant selected cultivars
- Heritability of durable resistance to stripe rust in bread wheat (Triticum aestivum L.)
- Molecular mechanism of follicular development in laying hens based on the regulation of water metabolism
- Molecular identification and control studies on Coridius sp. (Hemiptera: Dinidoridae) in Al-Khamra, south of Jeddah, Saudi Arabia
- 10.1515/biol-2025-1218
- Animal Science
- Effect of sex ratio on the life history traits of an important invasive species, Spodoptera frugiperda
- Plant Sciences
- Hairpin in a haystack: In silico identification and characterization of plant-conserved microRNA in Rafflesiaceae
- Widely targeted metabolomics of different tissues in Rubus corchorifolius
- The complete chloroplast genome of Gerbera piloselloides (L.) Cass., 1820 (Carduoideae, Asteraceae) and its phylogenetic analysis
- Field trial to correlate mineral solubilization activity of Pseudomonas aeruginosa and biochemical content of groundnut plants
- Correlation analysis between semen routine parameters and sperm DNA fragmentation index in patients with semen non-liquefaction: A retrospective study
- Plasticity of the anatomical traits of Rhododendron L. (Ericaceae) leaves and its implications in adaptation to the plateau environment
- Effects of Piriformospora indica and arbuscular mycorrhizal fungus on growth and physiology of Moringa oleifera under low-temperature stress
- Effects of different sources of potassium fertiliser on yield, fruit quality and nutrient absorption in “Harward” kiwifruit (Actinidia deliciosa)
- Comparative efficiency and residue levels of spraying programs against powdery mildew in grape varieties
- The DREB7 transcription factor enhances salt tolerance in soybean plants under salt stress
- Using plant electrical signals of water hyacinth (Eichhornia crassipes) for water pollution monitoring
- Response of hybrid grapes (Vitis spp.) to two biotic stress factors and their seedlessness status
- Metabolomic profiling reveals systemic metabolic reprogramming in Alternaria alternata under salt stress
- Effects of mixed salinity and alkali stress on photosynthetic characteristics and PEPC gene expression of vegetable soybean seedlings
- Food Science
- Phytochemical analysis of Stachys iva: Discovering the optimal extract conditions and its bioactive compounds
- Review on role of honey in disease prevention and treatment through modulation of biological activities
- Computational analysis of polymorphic residues in maltose and maltotriose transporters of a wild Saccharomyces cerevisiae strain
- Optimization of phenolic compound extraction from Tunisian squash by-products: A sustainable approach for antioxidant and antibacterial applications
- Liupao tea aqueous extract alleviates dextran sulfate sodium-induced ulcerative colitis in rats by modulating the gut microbiota
- Toxicological qualities and detoxification trends of fruit by-products for valorization: A review
- Polyphenolic spectrum of cornelian cherry fruits and their health-promoting effect
- Optimizing the encapsulation of the refined extract of squash peels for functional food applications: A sustainable approach to reduce food waste
- Advancements in curcuminoid formulations: An update on bioavailability enhancement strategies curcuminoid bioavailability and formulations
- Impact of saline sprouting on antioxidant properties and bioactive compounds in chia seeds
- The dilemma of food genetics and improvement
- Causal effects of trace elements on congenital foot deformities and their subtypes: a Mendelian randomization study with gut microbiota mediation
- Honey meets acidity: a novel biopreservative approach against foodborne pathogens
- Bioengineering and Biotechnology
- Impact of hyaluronic acid-modified hafnium metalorganic frameworks containing rhynchophylline on Alzheimer’s disease
- Emerging patterns in nanoparticle-based therapeutic approaches for rheumatoid arthritis: A comprehensive bibliometric and visual analysis spanning two decades
- Application of CRISPR/Cas gene editing for infectious disease control in poultry
- Preparation of hafnium nitride-coated titanium implants by magnetron sputtering technology and evaluation of their antibacterial properties and biocompatibility
- Preparation and characterization of lemongrass oil nanoemulsion: Antimicrobial, antibiofilm, antioxidant, and anticancer activities
- Fluorescent detection of sialic acid–binding lectins using functionalized quantum dots in ELISA format
- Smart tectorigenin-loaded ZnO hydrogel nanocomposites for targeted wound healing: synthesis, characterization, and biological evaluation
- Corrigendum
- Corrigendum to “Utilization of convolutional neural networks to analyze microscopic images for high-throughput screening of mesenchymal stem cells”
- Corrigendum to “Effects of Ire1 gene on virulence and pathogenicity of Candida albicans”
- Retraction
- Retraction of “Down-regulation of miR-539 indicates poor prognosis in patients with pancreatic cancer”
Articles in the same Issue
- Safety assessment and modulation of hepatic CYP3A4 and UGT enzymes by Glycyrrhiza glabra aqueous extract in female Sprague–Dawley rats
- Adult-onset Still’s disease with hemophagocytic lymphohistiocytosis and minimal change disease
- Role of DZ2002 in reducing corneal graft rejection in rats by influencing Th17 activation via inhibition of the PI3K/AKT pathway and downregulation of TRAF1
- Biomedical Sciences
- Mechanism of triptolide regulating proliferation and apoptosis of hepatoma cells by inhibiting JAK/STAT pathway
- Maslinic acid improves mitochondrial function and inhibits oxidative stress and autophagy in human gastric smooth muscle cells
- Comparative analysis of inflammatory biomarkers for the diagnosis of neonatal sepsis: IL-6, IL-8, SAA, CRP, and PCT
- Post-pandemic insights on COVID-19 and premature ovarian insufficiency
- Proteome differences of dental stem cells between permanent and deciduous teeth by data-independent acquisition proteomics
- Optimizing a modified cetyltrimethylammonium bromide protocol for fungal DNA extraction: Insights from multilocus gene amplification
- Preliminary analysis of the role of small hepatitis B surface proteins mutations in the pathogenesis of occult hepatitis B infection via the endoplasmic reticulum stress-induced UPR-ERAD pathway
- Efficacy of alginate-coated gold nanoparticles against antibiotics-resistant Staphylococcus and Streptococcus pathogens of acne origins
- Battling COVID-19 leveraging nanobiotechnology: Gold and silver nanoparticle–B-escin conjugates as SARS-CoV-2 inhibitors
- Neurodegenerative diseases and neuroinflammation-induced apoptosis
- Impact of fracture fixation surgery on cognitive function and the gut microbiota in mice with a history of stroke
- COLEC10: A potential tumor suppressor and prognostic biomarker in hepatocellular carcinoma through modulation of EMT and PI3K-AKT pathways
- High-temperature requirement serine protease A2 inhibitor UCF-101 ameliorates damaged neurons in traumatic brain-injured rats by the AMPK/NF-κB pathway
- SIK1 inhibits IL-1β-stimulated cartilage apoptosis and inflammation in vitro through the CRTC2/CREB1 signaling
- Rutin–chitooligosaccharide complex: Comprehensive evaluation of its anti-inflammatory and analgesic properties in vitro and in vivo
- Knockdown of Aurora kinase B alleviates high glucose-triggered trophoblast cells damage and inflammation during gestational diabetes
- Calcium-sensing receptors promoted Homer1 expression and osteogenic differentiation in bone marrow mesenchymal stem cells
- ABI3BP can inhibit the proliferation, invasion, and epithelial–mesenchymal transition of non-small-cell lung cancer cells
- Changes in blood glucose and metabolism in hyperuricemia mice
- Rapid detection of the GJB2 c.235delC mutation based on CRISPR-Cas13a combined with lateral flow dipstick
- IL-11 promotes Ang II-induced autophagy inhibition and mitochondrial dysfunction in atrial fibroblasts
- Short-chain fatty acid attenuates intestinal inflammation by regulation of gut microbial composition in antibiotic-associated diarrhea
- Application of metagenomic next-generation sequencing in the diagnosis of pathogens in patients with diabetes complicated by community-acquired pneumonia
- NAT10 promotes radiotherapy resistance in non-small cell lung cancer by regulating KPNB1-mediated PD-L1 nuclear translocation
- Phytol-mixed micelles alleviate dexamethasone-induced osteoporosis in zebrafish: Activation of the MMP3–OPN–MAPK pathway-mediating bone remodeling
- Association between TGF-β1 and β-catenin expression in the vaginal wall of patients with pelvic organ prolapse
- Primary pleomorphic liposarcoma involving bilateral ovaries: Case report and literature review
- Effects of de novo donor-specific Class I and II antibodies on graft outcomes after liver transplantation: A pilot cohort study
- Sleep architecture in Alzheimer’s disease continuum: The deep sleep question
- Ephedra fragilis plant extract: A groundbreaking corrosion inhibitor for mild steel in acidic environments – electrochemical, EDX, DFT, and Monte Carlo studies
- Langerhans cell histiocytosis in an adult patient with upper jaw and pulmonary involvement: A case report
- Inhibition of mast cell activation by Jaranol-targeted Pirin ameliorates allergic responses in mouse allergic rhinitis
- Aeromonas veronii-induced septic arthritis of the hip in a child with acute lymphoblastic leukemia
- Clusterin activates the heat shock response via the PI3K/Akt pathway to protect cardiomyocytes from high-temperature-induced apoptosis
- Research progress on fecal microbiota transplantation in tumor prevention and treatment
- Low-pressure exposure influences the development of HAPE
- Stigmasterol alleviates endplate chondrocyte degeneration through inducing mitophagy by enhancing PINK1 mRNA acetylation via the ESR1/NAT10 axis
- AKAP12, mediated by transcription factor 21, inhibits cell proliferation, metastasis, and glycolysis in lung squamous cell carcinoma
- Association between PAX9 or MSX1 gene polymorphism and tooth agenesis risk: A meta-analysis
- A case of bloodstream infection caused by Neisseria gonorrhoeae
- Case of nasopharyngeal tuberculosis complicated with cervical lymph node and pulmonary tuberculosis
- p-Cymene inhibits pro-fibrotic and inflammatory mediators to prevent hepatic dysfunction
- GFPT2 promotes paclitaxel resistance in epithelial ovarian cancer cells via activating NF-κB signaling pathway
- Transfer RNA-derived fragment tRF-36 modulates varicose vein progression via human vascular smooth muscle cell Notch signaling
- RTA-408 attenuates the hepatic ischemia reperfusion injury in mice possibly by activating the Nrf2/HO-1 signaling pathway
- Decreased serum TIMP4 levels in patients with rheumatoid arthritis
- Sirt1 protects lupus nephritis by inhibiting the NLRP3 signaling pathway in human glomerular mesangial cells
- Sodium butyrate aids brain injury repair in neonatal rats
- Interaction of MTHFR polymorphism with PAX1 methylation in cervical cancer
- Convallatoxin inhibits proliferation and angiogenesis of glioma cells via regulating JAK/STAT3 pathway
- The effect of the PKR inhibitor, 2-aminopurine, on the replication of influenza A virus, and segment 8 mRNA splicing
- Effects of Ire1 gene on virulence and pathogenicity of Candida albicans
- Small cell lung cancer with small intestinal metastasis: Case report and literature review
- GRB14: A prognostic biomarker driving tumor progression in gastric cancer through the PI3K/AKT signaling pathway by interacting with COBLL1
- 15-Lipoxygenase-2 deficiency induces foam cell formation that can be restored by salidroside through the inhibition of arachidonic acid effects
- FTO alleviated the diabetic nephropathy progression by regulating the N6-methyladenosine levels of DACT1
- Clinical relevance of inflammatory markers in the evaluation of severity of ulcerative colitis: A retrospective study
- Zinc valproic acid complex promotes osteoblast differentiation and exhibits anti-osteoporotic potential
- Primary pulmonary synovial sarcoma in the bronchial cavity: A case report
- Metagenomic next-generation sequencing of alveolar lavage fluid improves the detection of pulmonary infection
- Uterine tumor resembling ovarian sex cord tumor with extensive rhabdoid differentiation: A case report
- Genomic analysis of a novel ST11(PR34365) Clostridioides difficile strain isolated from the human fecal of a CDI patient in Guizhou, China
- Effects of tiered cardiac rehabilitation on CRP, TNF-α, and physical endurance in older adults with coronary heart disease
- Changes in T-lymphocyte subpopulations in patients with colorectal cancer before and after acupoint catgut embedding acupuncture observation
- Modulating the tumor microenvironment: The role of traditional Chinese medicine in improving lung cancer treatment
- Alterations of metabolites related to microbiota–gut–brain axis in plasma of colon cancer, esophageal cancer, stomach cancer, and lung cancer patients
- Research on individualized drug sensitivity detection technology based on bio-3D printing technology for precision treatment of gastrointestinal stromal tumors
- CEBPB promotes ulcerative colitis-associated colorectal cancer by stimulating tumor growth and activating the NF-κB/STAT3 signaling pathway
- Oncolytic bacteria: A revolutionary approach to cancer therapy
- A de novo meningioma with rapid growth: A possible malignancy imposter?
- Diagnosis of secondary tuberculosis infection in an asymptomatic elderly with cancer using next-generation sequencing: Case report
- Hesperidin and its zinc(ii) complex enhance osteoblast differentiation and bone formation: In vitro and in vivo evaluations
- Research progress on the regulation of autophagy in cardiovascular diseases by chemokines
- Anti-arthritic, immunomodulatory, and inflammatory regulation by the benzimidazole derivative BMZ-AD: Insights from an FCA-induced rat model
- Immunoassay for pyruvate kinase M1/2 as an Alzheimer’s biomarker in CSF
- The role of HDAC11 in age-related hearing loss: Mechanisms and therapeutic implications
- Evaluation and application analysis of animal models of PIPNP based on data mining
- Therapeutic approaches for liver fibrosis/cirrhosis by targeting pyroptosis
- Fabrication of zinc oxide nanoparticles using Ruellia tuberosa leaf extract induces apoptosis through P53 and STAT3 signalling pathways in prostate cancer cells
- Haplo-hematopoietic stem cell transplantation and immunoradiotherapy for severe aplastic anemia complicated with nasopharyngeal carcinoma: A case report
- Modulation of the KEAP1-NRF2 pathway by Erianin: A novel approach to reduce psoriasiform inflammation and inflammatory signaling
- The expression of epidermal growth factor receptor 2 and its relationship with tumor-infiltrating lymphocytes and clinical pathological features in breast cancer patients
- Innovations in MALDI-TOF Mass Spectrometry: Bridging modern diagnostics and historical insights
- BAP1 complexes with YY1 and RBBP7 and its downstream targets in ccRCC cells
- Hypereosinophilic syndrome with elevated IgG4 and T-cell clonality: A report of two cases
- Electroacupuncture alleviates sciatic nerve injury in sciatica rats by regulating BDNF and NGF levels, myelin sheath degradation, and autophagy
- Polydatin prevents cholesterol gallstone formation by regulating cholesterol metabolism via PPAR-γ signaling
- RNF144A and RNF144B: Important molecules for health
- Analysis of the detection rate and related factors of thyroid nodules in the healthy population
- Artesunate inhibits hepatocellular carcinoma cell migration and invasion through OGA-mediated O-GlcNAcylation of ZEB1
- Endovascular management of post-pancreatectomy hemorrhage caused by a hepatic artery pseudoaneurysm: Case report and review of the literature
- Efficacy and safety of anti-PD-1/PD-L1 antibodies in patients with relapsed refractory diffuse large B-cell lymphoma: A meta-analysis
- SATB2 promotes humeral fracture healing in rats by activating the PI3K/AKT pathway
- Overexpression of the ferroptosis-related gene, NFS1, corresponds to gastric cancer growth and tumor immune infiltration
- Understanding risk factors and prognosis in diabetic foot ulcers
- Atractylenolide I alleviates the experimental allergic response in mice by suppressing TLR4/NF-kB/NLRP3 signalling
- FBXO31 inhibits the stemness characteristics of CD147 (+) melanoma stem cells
- Immune molecule diagnostics in colorectal cancer: CCL2 and CXCL11
- Inhibiting CXCR6 promotes senescence of activated hepatic stellate cells with limited proinflammatory SASP to attenuate hepatic fibrosis
- Cadmium toxicity, health risk and its remediation using low-cost biochar adsorbents
- Pulmonary cryptococcosis with headache as the first presentation: A case report
- Solitary pulmonary metastasis with cystic airspaces in colon cancer: A rare case report
- RUNX1 promotes denervation-induced muscle atrophy by activating the JUNB/NF-κB pathway and driving M1 macrophage polarization
- Morphometric analysis and immunobiological investigation of Indigofera oblongifolia on the infected lung with Plasmodium chabaudi
- The NuA4/TIP60 histone-modifying complex and Hr78 modulate the Lobe2 mutant eye phenotype
- Experimental study on salmon demineralized bone matrix loaded with recombinant human bone morphogenetic protein-2: In vitro and in vivo study
- A case of IgA nephropathy treated with a combination of telitacicept and half-dose glucocorticoids
- Analgesic and toxicological evaluation of cannabidiol-rich Moroccan Cannabis sativa L. (Khardala variety) extract: Evidence from an in vivo and in silico study
- Wound healing and signaling pathways
- Combination of immunotherapy and whole-brain radiotherapy on prognosis of patients with multiple brain metastases: A retrospective cohort study
- To explore the relationship between endometrial hyperemia and polycystic ovary syndrome
- Research progress on the impact of curcumin on immune responses in breast cancer
- Biogenic Cu/Ni nanotherapeutics from Descurainia sophia (L.) Webb ex Prantl seeds for the treatment of lung cancer
- Dapagliflozin attenuates atrial fibrosis via the HMGB1/RAGE pathway in atrial fibrillation rats
- Glycitein alleviates inflammation and apoptosis in keratinocytes via ROS-associated PI3K–Akt signalling pathway
- ADH5 inhibits proliferation but promotes EMT in non-small cell lung cancer cell through activating Smad2/Smad3
- Apoptotic efficacies of AgNPs formulated by Syzygium aromaticum leaf extract on 32D-FLT3-ITD human leukemia cell line with PI3K/AKT/mTOR signaling pathway
- Novel cuproptosis-related genes C1QBP and PFKP identified as prognostic and therapeutic targets in lung adenocarcinoma
- Bee venom promotes exosome secretion and alters miRNA cargo in T cells
- Treatment of pure red cell aplasia in a chronic kidney disease patient with roxadustat: A case report
- Comparative bioinformatics analysis of the Wnt pathway in breast cancer: Selection of novel biomarker panels associated with ER status
- Kynurenine facilitates renal cell carcinoma progression by suppressing M2 macrophage pyroptosis through inhibition of CASP1 cleavage
- RFX5 promotes the growth, motility, and inhibits apoptosis of gastric adenocarcinoma cells through the SIRT1/AMPK axis
- ALKBH5 exacerbates early cardiac damage after radiotherapy for breast cancer via m6A demethylation of TLR4
- Phytochemicals of Roman chamomile: Antioxidant, anti-aging, and whitening activities of distillation residues
- Circadian gene Cry1 inhibits the tumorigenicity of hepatocellular carcinoma by the BAX/BCL2-mediated apoptosis pathway
- The TNFR-RIPK1/RIPK3 signalling pathway mediates the effect of lanthanum on necroptosis of nerve cells
- Longitudinal monitoring of autoantibody dynamics in patients with early-stage non-small-cell lung cancer undergoing surgery
- The potential role of rutin, a flavonoid, in the management of cancer through modulation of cell signaling pathways
- Construction of pectinase gene engineering microbe and its application in tobacco sheets
- Construction of a microbial abundance prognostic scoring model based on intratumoral microbial data for predicting the prognosis of lung squamous cell carcinoma
- Sepsis complicated by haemophagocytic lymphohistiocytosis triggered by methicillin-resistant Staphylococcus aureus and human herpesvirus 8 in an immunocompromised elderly patient: A case report
- Sarcopenia in liver transplantation: A comprehensive bibliometric study of current research trends and future directions
- Advances in cancer immunotherapy and future directions in personalized medicine
- Can coronavirus disease 2019 affect male fertility or cause spontaneous abortion? A two-sample Mendelian randomization analysis
- Heat stroke associated with novel leukaemia inhibitory factor receptor gene variant in a Chinese infant
- PSME2 exacerbates ulcerative colitis by disrupting intestinal barrier function and promoting autophagy-dependent inflammation
- Hyperosmolar hyperglycemic state with severe hypernatremia coexisting with central diabetes insipidus: A case report and literature review
- Efficacy and mechanism of escin in improving the tissue microenvironment of blood vessel walls via anti-inflammatory and anticoagulant effects: Implications for clinical practice
- Merkel cell carcinoma: Clinicopathological analysis of three patients and literature review
- Genetic variants in VWF exon 26 and their implications for type 1 Von Willebrand disease in a Saudi Arabian population
- Lipoxin A4 improves myocardial ischemia/reperfusion injury through the Notch1-Nrf2 signaling pathway
- High levels of EPHB2 expression predict a poor prognosis and promote tumor progression in endometrial cancer
- Knockdown of SHP-2 delays renal tubular epithelial cell injury in diabetic nephropathy by inhibiting NLRP3 inflammasome-mediated pyroptosis
- Exploring the toxicity mechanisms and detoxification methods of Rhizoma Paridis
- Concomitant gastric carcinoma and primary hepatic angiosarcoma in a patient: A case report
- YAP1 inhibition protects retinal vascular endothelial cells under high glucose by inhibiting autophagy
- Identification of secretory protein related biomarkers for primary biliary cholangitis based on machine learning and experimental validation
- Integrated genomic and clinical modeling for prognostic assessment of radiotherapy response in rectal neoplasms
- Stem cell-based approaches for glaucoma treatment: a mini review
- Bacteriophage titering by optical density means: KOTE assays
- Neutrophil-related signature characterizes immune landscape and predicts prognosis of esophageal squamous cell carcinoma
- Integrated bioinformatic analysis and machine learning strategies to identify new potential immune biomarkers for Alzheimer’s disease and their targeting prediction with geniposide
- TRIM21 accelerates ferroptosis in intervertebral disc degeneration by promoting SLC7A11 ubiquitination and degradation
- TRIM21 accelerates ferroptosis in intervertebral disc degeneration by promoting SLC7A11 ubiquitination and degradation
- Histone modification and non-coding RNAs in skin aging: emerging therapeutic avenues
- A multiplicative behavioral model of DNA replication initiation in cells
- Biogenic gold nanoparticles synthesized from Pergularia daemia leaves: a novel approach for nasopharyngeal carcinoma therapy
- Creutzfeldt-Jakob disease mimicking Hashimoto’s encephalopathy: steroid response followed by decline
- Impact of semaphorin, Sema3F, on the gene transcription and protein expression of CREB and its binding protein CREBBP in primary hippocampal neurons of rats
- Iron overloaded M0 macrophages regulate hematopoietic stem cell proliferation and senescence via the Nrf2/Keap1/HO-1 pathway
- Revisiting the link between NADPH oxidase p22phox C242T polymorphism and ischemic stroke risk: an updated meta-analysis
- Exercise training preferentially modulates α1D-adrenergic receptor expression in peripheral arteries of hypertensive rats
- Overexpression of HE4/WFDC2 gene in mice leads to keratitis and corneal opacity
- Tumoral calcinosis complicating CKD-MBD in hemodialysis: a case report
- Mechanism of KLF4 Inhibition of epithelial-mesenchymal transition in gastric cancer cells
- Dissecting the molecular mechanisms of T cell infiltration in psoriatic lesions via cell-cell communication and regulatory network analysis
- Circadian rhythm-based prognostic features predict immune infiltration and tumor microenvironment in molecular subtypes of hepatocellular carcinoma
- Ecology and Environmental Science
- Optimization and comparative study of Bacillus consortia for cellulolytic potential and cellulase enzyme activity
- The complete mitochondrial genome analysis of Haemaphysalis hystricis Supino, 1897 (Ixodida: Ixodidae) and its phylogenetic implications
- Epidemiological characteristics and risk factors analysis of multidrug-resistant tuberculosis among tuberculosis population in Huzhou City, Eastern China
- Indices of human impacts on landscapes: How do they reflect the proportions of natural habitats?
- Genetic analysis of the Siberian flying squirrel population in the northern Changbai Mountains, Northeast China: Insights into population status and conservation
- Diversity and environmental drivers of Suillus communities in Pinus sylvestris var. mongolica forests of Inner Mongolia
- Global assessment of the fate of nitrogen deposition in forest ecosystems: Insights from 15N tracer studies
- Fungal and bacterial pathogenic co-infections mainly lead to the assembly of microbial community in tobacco stems
- Influencing of coal industry related airborne particulate matter on ocular surface tear film injury and inflammatory factor expression in Sprague-Dawley rats
- Temperature-dependent development, predation, and life table of Sphaerophoria macrogaster (Thomson) (Diptera: Syrphidae) feeding on Myzus persicae (Sulzer) (Homoptera: Aphididae)
- Eleonora’s falcon trophic interactions with insects within its breeding range: A systematic review
- Agriculture
- Integrated analysis of transcriptome, sRNAome, and degradome involved in the drought-response of maize Zhengdan958
- Variation in flower frost tolerance among seven apple cultivars and transcriptome response patterns in two contrastingly frost-tolerant selected cultivars
- Heritability of durable resistance to stripe rust in bread wheat (Triticum aestivum L.)
- Molecular mechanism of follicular development in laying hens based on the regulation of water metabolism
- Molecular identification and control studies on Coridius sp. (Hemiptera: Dinidoridae) in Al-Khamra, south of Jeddah, Saudi Arabia
- 10.1515/biol-2025-1218
- Animal Science
- Effect of sex ratio on the life history traits of an important invasive species, Spodoptera frugiperda
- Plant Sciences
- Hairpin in a haystack: In silico identification and characterization of plant-conserved microRNA in Rafflesiaceae
- Widely targeted metabolomics of different tissues in Rubus corchorifolius
- The complete chloroplast genome of Gerbera piloselloides (L.) Cass., 1820 (Carduoideae, Asteraceae) and its phylogenetic analysis
- Field trial to correlate mineral solubilization activity of Pseudomonas aeruginosa and biochemical content of groundnut plants
- Correlation analysis between semen routine parameters and sperm DNA fragmentation index in patients with semen non-liquefaction: A retrospective study
- Plasticity of the anatomical traits of Rhododendron L. (Ericaceae) leaves and its implications in adaptation to the plateau environment
- Effects of Piriformospora indica and arbuscular mycorrhizal fungus on growth and physiology of Moringa oleifera under low-temperature stress
- Effects of different sources of potassium fertiliser on yield, fruit quality and nutrient absorption in “Harward” kiwifruit (Actinidia deliciosa)
- Comparative efficiency and residue levels of spraying programs against powdery mildew in grape varieties
- The DREB7 transcription factor enhances salt tolerance in soybean plants under salt stress
- Using plant electrical signals of water hyacinth (Eichhornia crassipes) for water pollution monitoring
- Response of hybrid grapes (Vitis spp.) to two biotic stress factors and their seedlessness status
- Metabolomic profiling reveals systemic metabolic reprogramming in Alternaria alternata under salt stress
- Effects of mixed salinity and alkali stress on photosynthetic characteristics and PEPC gene expression of vegetable soybean seedlings
- Food Science
- Phytochemical analysis of Stachys iva: Discovering the optimal extract conditions and its bioactive compounds
- Review on role of honey in disease prevention and treatment through modulation of biological activities
- Computational analysis of polymorphic residues in maltose and maltotriose transporters of a wild Saccharomyces cerevisiae strain
- Optimization of phenolic compound extraction from Tunisian squash by-products: A sustainable approach for antioxidant and antibacterial applications
- Liupao tea aqueous extract alleviates dextran sulfate sodium-induced ulcerative colitis in rats by modulating the gut microbiota
- Toxicological qualities and detoxification trends of fruit by-products for valorization: A review
- Polyphenolic spectrum of cornelian cherry fruits and their health-promoting effect
- Optimizing the encapsulation of the refined extract of squash peels for functional food applications: A sustainable approach to reduce food waste
- Advancements in curcuminoid formulations: An update on bioavailability enhancement strategies curcuminoid bioavailability and formulations
- Impact of saline sprouting on antioxidant properties and bioactive compounds in chia seeds
- The dilemma of food genetics and improvement
- Causal effects of trace elements on congenital foot deformities and their subtypes: a Mendelian randomization study with gut microbiota mediation
- Honey meets acidity: a novel biopreservative approach against foodborne pathogens
- Bioengineering and Biotechnology
- Impact of hyaluronic acid-modified hafnium metalorganic frameworks containing rhynchophylline on Alzheimer’s disease
- Emerging patterns in nanoparticle-based therapeutic approaches for rheumatoid arthritis: A comprehensive bibliometric and visual analysis spanning two decades
- Application of CRISPR/Cas gene editing for infectious disease control in poultry
- Preparation of hafnium nitride-coated titanium implants by magnetron sputtering technology and evaluation of their antibacterial properties and biocompatibility
- Preparation and characterization of lemongrass oil nanoemulsion: Antimicrobial, antibiofilm, antioxidant, and anticancer activities
- Fluorescent detection of sialic acid–binding lectins using functionalized quantum dots in ELISA format
- Smart tectorigenin-loaded ZnO hydrogel nanocomposites for targeted wound healing: synthesis, characterization, and biological evaluation
- Corrigendum
- Corrigendum to “Utilization of convolutional neural networks to analyze microscopic images for high-throughput screening of mesenchymal stem cells”
- Corrigendum to “Effects of Ire1 gene on virulence and pathogenicity of Candida albicans”
- Retraction
- Retraction of “Down-regulation of miR-539 indicates poor prognosis in patients with pancreatic cancer”