Oral nifedipine and phytosterol, intravenous nicardipine, and oral nifedipine only: Three-arm, retrospective, cohort study for management of severe preeclampsia
-
Shanduo Ma
 ,
Limei Zhu
,
Tiantian Zhou
,
Ting Qi
und
Weijun Wang
,
Limei Zhu
,
Tiantian Zhou
,
Ting Qi
und
Weijun Wang


Abstract
The treatment of preeclampsia is delivering women and extracting the placenta, but the Chinese Society of Obstetrics and Gynecology guidelines do not recommend the delivery of babies without severe features. The objectives of the study were to compare the effectiveness and safety of nifedipine and phytosterol in combination with nicardipine for the management of severe preeclampsia. Women (19–32 years; gestation age ≥ 30 weeks) with the complication of severe preeclampsia have received 10 mg of oral nifedipine (pregnant women received 10 mg of oralnifedipine, n = 112) or 1 mg/h intravenous nicardipine (pregnant women received 1 mg/h intravenous nicardipine (ND cohort), n = 115) or oral 10 mg nifedipine and 500 mg phytosterol (pregnant women received oral 10 mg nifedipine and 500 mg phytosterol (np cohort), n = 111) until 150/100 mmHg blood pressure was achieved. The time required to achieve the desired blood pressure control was 13 minutes shorter in the NP cohort compared to the NF (p < 0.0001, t = 11.605), and 3 minutes shorter compared to the ND (p < 0.0001, t = 2.79) cohorts. Stillbirths were reported in 14 (13%), 28 (24%), and 10 (9%) infants, and 13 (12%), 26 (23%), and 10 (9%) infants died from the NF, ND, and NP cohorts, respectively. The undesirable tocolytic effect was reported in 17 (15%) women of the ND cohort. Phytosterol with nifedipine has a synergistic or additive effect on the management of preeclampsia with fewer adverse outcomes.
1 Introduction
Preeclampsia is the leading cause of maternal morbidity and mortality [1] due to complications that have arisen from severe hypertension in pregnant women [2]. Therefore, in pregnant women with severe hypertension, blood pressure is required to be controlled [3]. Preeclampsia is reported in pregnancy after 20 weeks of gestation and is characterized by high blood pressure (systolic blood pressure >160 mmHg/diastolic blood pressure >110 mmHg) and proteinuria (≥300 mg/24 h) [2]. Preeclampsia leads to the development of eclampsia [4]. The prevalence of eclampsia in China is 0.2% [5].
The treatment of preeclampsia is delivering the patient and extracting the placenta [6] but when the blood pressure of a pregnant woman is higher (>160/110 mmHg), antihypertensive agents are administered to stabilize the patient [2]. However, these recommendations are not uniform with many recommended guidelines for a lower threshold (the National Institute for Health and Care Guidelines, World Health Organization [7] HYPERTENSION Canada, the International Society for the Study of Hypertension in Pregnancy, and the International Federation of Gynecology and Obstetrics guidelines [4]). Chinese guidelines of the Chinese Society of Obstetrics and Gynecology [8] have different diagnostic criteria for preeclampsia than the other international guidelines and are not recommending the delivery of babies in pregnant women with preeclampsia without severe features. Women should not give birth until 37 weeks gestation, which leads to delayed delivery in women with preeclampsia. In severe preeclampsia, termination of pregnancy is recommended at 34 weeks or even earlier depending on the maternal–fetal state. Also, there is a lack of a detailed management plan for preeclampsia in the guidelines of the Chinese Society of Obstetrics and Gynecology [8].
The American College of Obstetricians and Gynecologists 2013 [9] and the National Institute for Health and Care Guidelines [10], are recommending oral nifedipine (a calcium channel blocker), and intravenous labetalol (a combined α- and β-adrenergic blocker), but do not recommend intravenous nicardipine (a calcium channel blocker) in severe preeclampsia. Intravenous labetalol provides comparatively faster management of blood pressure and is successful in delaying further hypertensive crises after its administration in pregnant women with severe preeclampsia. However, it is expensive and has a higher chance of neonatal death [2,6,11]. While, oral nifedipine is comparatively less expensive and safe for neonates, and convenient for women [12]. It achieves slower management of high blood pressure [2,6,11]. Also, oral nifedipine is not successful in delaying further hypertensive crises after its administration in women with severe preeclampsia [13]. Therefore, the total dose for preeclampsia management is comparatively higher. The placebo-controlled, randomized trial reported the safety and superior efficacy of the combination of oral nifedipine and phytosterol (a natural compound) than nifedipine alone for the management of preeclampsia [14]. However, the mechanism of action responsible for the antihypertensive effect of phytosterol is unknown. For fast and adequate management of preeclampsia, intravenous nicardipine is used [15]. However, there are no adequate studies on intravenous nicardipine in pregnant females. It is used for the management of preeclampsia but animal studies have reported the secretion of nicardipine in breast milk [16]. Also, intravenous nicardipine interferes with the spontaneous induction of labor (undesirable tocolytic effect) before 34 weeks of gestation [17] and is only used when no other suitable option is available for preeclampsia and is not used in multiple pregnancies [18].
The objectives of the retrospective study were to compare the time and the amount of calcium channel blocker required to control the blood pressure to less than 150/100 mmHg, the time required for further hypertensive crisis after intervention(s), and the safety of the mother and fetus for oral nifedipine and phytosterol combination and oral nifedipine only with intravenous nicardipine in Chinese pregnant women with severe preeclampsia.
2 Materials and methods
2.1 Ethics approval and consent to participate
The designed protocol (TJMC220120 dated October 2, 2020) of the established study was approved by the First People’s Hospital of Lianyungang review board and the Chinese Society of Obstetrics and Gynecology. The study reporting adheres to the law of China and the V2008 the World Medical Association Declaration of Helsinki. Informed written consent was obtained from all subjects and/or their legal guardian(s) (routine protocol of the institute) before admission to hospitals regarding intervention(s), pathology, and participation in the study.
-
Informed consent: Informed consent has been obtained from all individuals included in this study.
-
Ethical approval: The research related to human use has been complied with all the relevant national regulations, institutional policies, and in accordance with the tenets of the Helsinki Declaration, and has been approved by the authors’ institutional review board or equivalent committee.
2.2 Inclusion criteria
Women (age >18 years) with the complication of severe preeclampsia diagnosed according to the report of the American College of Obstetricians and Gynecologists Task Force on Hypertension in Pregnancy [9] (gestation age >20 weeks, blood pressure >160/110 mmHg, and higher proteinuria ≥ 300 mg/24 h) and who had needed to receive treatment for the management of high blood pressure during their pregnancy were included in the analysis after getting written approval from the authorities.
2.3 Exclusion criteria
Women who had HELLP syndrome (Hemolysis, elevated liver enzymes, and low platelet count), diabetes, and a history of heart disease(s) were excluded from the analysis. Women who had a history of using other relevant drug therapies were excluded from the analysis.
2.4 Sample size calculation
The sample size (OpenEpi, Version 3, 01, Open-Source Epidemiologic Statistics for Public Health, USA) was calculated based on the assumption that 80 ± 13% of women achieved less than 150/100 mmHg blood pressure after intervention(s), 80% power (β = 0.2), and two-sided 5% type-I error (α = 0.05), and 95% confidence interval. This is a retrospective study of all eligible cases between January 2017 and December 2019. A “power analysis” i.e., what differences are achievable was preferred for sample size calculation.
2.5 Cohort
The oral nifedipine (NF) cohort consisted of 112 women who received immediate-release 10 mg tablet of oral nifedipine (Procardia, Pfizer, New York, NY, USA) at 15 min time intervals until 150/100 mmHg blood pressure was achieved or a maximum of up to five doses [2]. The nicardipine infusion (ND) cohort consisted of 115 women who received a continuous infusion of 1 mg/h of nicardipine (Cardene, PDL BioPharma, Inc., Redwood City, CA, USA) and the dose was increased by 0.5 mg at every hour (maximum 4 mg/h) until 150/100 mmHg blood pressure was achieved [16]. The oral nifedipine and phytosterol (NP) cohort consisted of 111 women who received immediate-release 10 mg of oral nifedipine tablet and oral 500 mg phytosterol powder (Shanghai Fudan Fuhua Pharmaceutical Co., Ltd, Shanghai, China; each 500 mg phytosterol powder contains 450 mg β-sitosterol) at 15 min time interval until 150/100 mmHg blood pressure was achieved or maximum up to five doses [14]. The different treatments for the management of severe preeclampsia were decided as per the preference of the concerned obstetrician(s). The very structured dosing schedule is an institutional protocol (not published yet). None of the women received magnesium sulfate. Once control was achieved, a maintenance dose (10 mg of oral nifedipine/8 h) was initiated in all women of all cohorts.
2.6 Demographical and clinical parameters
Data regarding socioeconomic status, height, weight, and blood pressure at the time of admission to the hospital were retrospectively collected from institutional records of women. Blood pressure was measured using the Sphygmomanometer (MDF® Calibra®, MDF Instruments Direct, Inc., Rincon, PR, USA) during treatment and at the time of admission.
2.7 Outcome measures
Time and amount of the calcium channel blocker required to control blood pressure to less than 150/100 mmHg and time required for further hypertensive crisis (blood pressure >160/110 mmHg, and higher proteinuria ≥300 mg/24 h) after intervention(s) were retrospectively collected from the institutional records of women (the primary outcomes). All women have graphs that report differences in blood pressure per minute. Also, adverse effects and the infant dose of medication were retrospectively collected from the institutional records of women (the secondary outcomes). Proteinuria was measured in terms of mg/24 h from the urine sample.
2.8 Adverse effects
Treatment-emergent adverse effects for women and their infants were retrospectively collected from the institutional records of women and infants.
2.9 Relative infant dose of calcium channel blocker
Data on the concentration of calcium channel blockers in breast milk was collected from institutional records of women. The relative infant dose of calcium channel blocker was calculated as per equation (1). It was estimated that the maximum milk consumed by the infant was 150 ± 10 mL/day. Less than 10% of the relative infant dose of calcium channels was considered safe [16]. The milk samples were taken as soon as they started secreting from the breast of the women.
2.10 Statistical analysis
InStat® 3.01, GraphPad Software, San Diego, CA, USA was used for statistical analysis purposes. Categorical variables are presented as frequency (percentages) and continuous variables are presented as mean value ± standard deviation (SD). Histograms and plots of normality were used to check for a normal distribution of the data. One-way analysis of variance (ANOVA) was performed for continuous variables and the Chi-square test for independence (χ 2 -test) was performed for categorical data. The Bonferroni multiple comparisons test was used for post hoc analysis (if the value of t is greater than 2.4, then the p-value is less than 0.050). Univariate followed by multivariate analyses were performed between the demographical and clinical conditions of women and treatment received by women for adverse infant outcomes [19]. All results were considered significant if the p-value was reported as less than 0.050.
3 Results
3.1 Study population
From 15 January 2017 to 19 December 2019, a total of 394 pregnant women (age >18 years) were diagnosed with the complication of severe preeclampsia and needed to receive treatment for the management of high blood pressure at the Department of Obstetrics and Gynecology of the First People’s Hospital of Lianyungang, Lianyungang, Jiangsu, China, and the referring hospital. Among 394 pregnant women, one woman had a history of heart failure, 13 women had HELLP syndrome, and 42 women had diabetes. Therefore, data of these women (n = 56) were excluded from the analysis.
Data of the demographical and clinical parameters of women at the time of admission, the time and amount of the calcium channel blocker required to control blood pressure to less than 150/100 mmHg, the time required for further hypertensive crisis after admiration of drug(s), and treatment-emergent adverse effects for women and their infants for a total of 338 women and their infants were collected from the institutional records of women and infants and were analyzed.
3.2 Demographical and clinical parameters
The age range of the included women was 19–32 years. All the included women had a gestation age of 30 weeks or more, a singleton pregnancy, higher blood pressure (>160/110 mmHg), and higher proteinuria (≥300 mg/24 h) at the time of hospital admission. A total of 19 (17%), 16 (14%), and 28 (25%) women in the pregnant women received 10 mg of oral nifedipine (NF cohort), pregnant women received 1 mg/h intravenous nicardipine (ND cohort), and pregnant women received oral 10 mg nifedipine and 500 mg phytosterol (NP cohort), respectively, had gestation age <32 weeks at the time of hospital admission. A total of 48 (43%), 49 (43%), and 55 (50%) women in the NF cohort, ND cohort, and NP cohort, respectively, had gestation age <34 weeks at the time of hospital admission. There were no significant differences in the demographical and clinical parameters of women (p > 0.050 for all, χ 2 -test, or ANOVA) at the time of hospital admission. None of these women had aspirin prophylaxis before hospital admission. The details of the demographical and clinical parameters of women at the time of hospital admission are presented in Table 1.
Demographical, clinical, and socioeconomic parameters of women at the time of admission to the hospital
| Parameters | Cohorts | ||||||
|---|---|---|---|---|---|---|---|
| NF | ND | NP | |||||
| Number of women included in the analysis | 112 | 115 | 111 | Comparisons | |||
| Treatment(s) for the management of high blood pressure | Oral nifedipine | Intravenous nicardipine | Oral nifedipine + oral phytosterol | p-value | F-value | Df | |
| Maternal age (years) | Minimum | 20 | 19 | 20 | 0.064 (ANOVA) | 2.77 | N/A |
| Maximum | 31 | 30 | 32 | ||||
| Mean value ± SD | 25.71 ± 3.56 | 24.71 ± 3.44 | 25.65 ± 3.72 | ||||
| Gestation age (weeks) | Minimum | 30 | 30 | 30 | 0.429 (ANOVA) | 0.85 | N/A |
| Maximum | 38 | 39 | 38 | ||||
| Mean value ± SD | 34.18 ± 2.51 | 34.31 ± 2.48 | 33.88 ± 2.62 | ||||
| <32 weeks | 19 (17%) | 16 (14%) | 28 (25%) | 0.079 (χ 2 -test) | N/A | 1 | |
| <34 weeks | 48 (43%) | 49 (43%) | 55 (50%) | 0.496 (χ 2 -test) | N/A | 1 | |
| Systolic blood pressure (mmHg) | 169.88 ± 4.74 | 170.50 ± 4.32 | 169.23 ± 4.74 | 0.118 (ANOVA) | 2.15 | N/A | |
| Diastolic blood pressure (mmHg) | 118.96 ± 3.72 | 119.44 ± 3.73 | 118.95 ± 3.67 | 0.524 (ANOVA) | 0.65 | N/A | |
| Heart rate (beats/min) | 81.79 ± 4.22 | 81.67 ± 4.40 | 81.42 ± 4.29 | 0.807 (ANOVA) | 0.21 | N/A | |
| Body mass index (kg/m2) | 25.12 ± 3.15 | 24.89 ± 3.67 | 25.41 ± 4.01 | 0.559 (ANOVA) | 0.54 | N/A | |
| Proteinuria (mg/24 h) | 310.48 ± 6.28 | 311.84 ± 4.53 | 311.97 ± 5.37 | 0.078 (ANOVA) | 0.23 | N/A | |
| Socioeconomic status | Poor | 31 (28%) | 41 (36%) | 42 (38%) | 0.334 (χ 2 -test) | N/A | 4 |
| Middle | 49 (44%) | 39 (34%) | 35 (32%) | ||||
| High | 32 (28%) | 35 (30%) | 34 (30%) | ||||
Categorical variables are presented as frequency (percentages) and continuous variables are presented as mean value ± SD.
One-way ANOVA was performed for continuous variables and the Chi-square test for independence was performed for categorical data.
p-value < 0.05 was considered as significant.
χ 2 -test: The Chi-square test for independence, N/A: Not applicable, Df: Degree of freedom.
3.3 Outcome measures
3.3.1 Time required to control blood pressure to less than 150/100 mmHg
All women had responded to the treatment. The time required to control blood pressure to less than 150/100 mmHg for women of the NP cohort was shorter than those of the NF (47.42 ± 6.99 min/woman vs 60.83 ± 9.07 min/woman, p < 0.0001, t = 11.6, ANOVA/Bonferroni test) and the ND (47.42 ± 6.99 min/woman vs 50.63 ± 9.56 min/woman, p < 0.0001, t = 2.8, ANOVA/Bonferroni test) cohorts. Also, the time required to control blood pressure to less than 150/100 mmHg for women of the ND cohort was shorter than those of the NF cohort (p < 0.0001, t = 8.9, ANOVA/Bonferroni test; Figure 1).
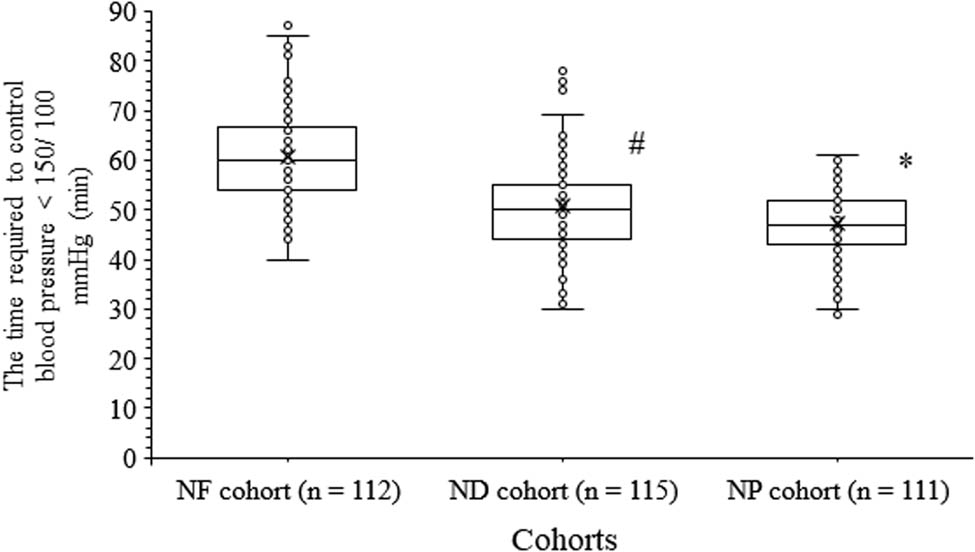
The time required to control blood pressure to less than 150/100 mmHg. * indicates shorter values than those of the NF and the ND cohorts. # indicates shorter values than those of the NF cohort. Box represents mean value.
3.3.2 Amount of calcium channel blocker required to control blood pressure to less than 150/100 mmHg
The amount of calcium channel blocker required to control blood pressure to less than 150/100 mmHg was fewer for women of the NP cohort than those of the NF (22.52 ± 8.36 mg/woman vs 26.16 ± 10.68 mg/woman, p < 0.0001, t = 2.7, ANOVA/Bonferroni test) and the ND (22.52 ± 8.36 mg/woman vs 51.05 ± 10.75 mg/woman, p < 0.0001, t = 21.4, ANOVA/Bonferroni test) cohorts. The amount of calcium channel blocker required to control blood pressure to less than 150/100 mmHg was fewer for women of the NF cohort than those of the ND cohort (p < 0.0001, t = 18.7, ANOVA/Bonferroni test, Figure 2).

The amount of calcium channel blocker required to control blood pressure to less than 150/100 mmHg. * indicates shorter values than those of the NF and the ND cohorts. # indicates shorter values than those of the ND cohort. Box represents mean value.
3.3.3 Time required for further hypertensive crisis
The time required for further hypertensive crisis (the time until the next hypertensive crisis) in women after administration of the drug(s) was longer for the NP cohort than those of the NF (8.90 ± 2.07 h/woman vs 6.13 ± 0.87 h/woman, p < 0.0001, t = 13.8, ANOVA/Bonferroni test) and ND (8.90 ± 2.07 h/woman vs 7.03 ± 1.30 h/woman, p < 0.0001, t = 4.6, ANOVA/Bonferroni test) cohorts. Also, the time required for the further hypertensive crisis in women after administration of drug(s) was longer for the ND cohort than those of the NF cohort (p < 0.0001, q = 9.4, ANOVA/Bonferroni test, Figure 3).

The time required for further hypertensive crisis after administration of the drug(s). * indicates longer values than those of the NF and the ND cohorts. # indicates longer values than those of the NF cohort. Box represents mean value.
3.4 Adverse effects
There were no significant differences in results of maternal vomiting, tachycardia, headache, dizziness, shortness of breath, and frequencies of intensive care unit admission for the infants among cohorts (p > 0.050 for all, ANOVA/Bonferroni test or χ 2 -test). The undesirable tocolytic effect was reported in 2 (2%), 17 (15%), and 1 (1%) women of the NF, ND, and NP cohorts, respectively. Induction of labor was attempted in all women who had faced the tocolytic effect. Stillbirths were reported in 14 (13%), 28 (24%), and 10 (9%) infants of the NF, ND, and NP cohorts, respectively. Death was reported in 13 (12%), 26 (23%), and 10 (9%) infants of the NF, ND, and NP cohorts, respectively (Table 2).
Short-term effects of treatments on maternal and infants’ outcomes
| Effects | Cohorts | Comparison | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| NF | ND | NP | ||||||||
| Numbers of women included in the analysis | 112 | 115 | 111 | p-value | F-value | Df | t-value | |||
| Treatment(s) for the management of high blood pressure | Oral nifedipine | Intravenous nicardipine | Oral nifedipine + oral phytosterol | NF vs ND | NF vs NP | ND vs NP | ||||
| Maternal nausea | 8 (7%) | 6 (5%) | 5 (5%) | 0.677 (ANOVA) | 0.39 | N/A | N/C | N/C | N/C | |
| Maternal vomiting | 4 (4%) | 4 (3%) | 2 (2%) | 0.715 (ANOVA) | 0.34 | N/A | N/C | N/C | N/C | |
| Maternal tachycardia | 2 (2%) | 7 (6%) | 2 (2%) | 0.109 (ANOVA) | 2.23 | N/A | N/C | N/C | N/C | |
| Maternal headache | 6 (5%) | 4 (4%) | 2 (2%) | 0.359 (ANOVA) | 1.03 | N/A | N/C | N/C | N/C | |
| Maternal dizziness | 4 (4%) | 5(4%) | 2 (2%) | 0.547 (ANOVA) | 0.60 | N/A | N/C | N/C | N/C | |
| Maternal shortness of breath | 1 (1%) | 1 (1%) | 1 (1%) | 0.999 (ANOVA) | 0.01 | N/A | N/C | N/C | N/C | |
| Undesirable tocolytic effect | 2 (2%) | 17 (15%)* | 1 (1%) | <0.0001 (ANOVA) | 13.19 | N/A | 4.3 | 0.3 | 4.6 | |
| Infants’ birth weight (kg) | 3.08 ± 0.41 | 2.99 ± 0.42 | 3.08 ± 0.11 | 0.078 (ANOVA) | 1.07 | N/A | N/A | N/A | N/A | |
| Apgar score | 4–6 | 25 (22%) | 20 (17%) | 20 (18%) | 0.593 (χ 2 -test) | N/A | 2 | N/C | N/C | N/C |
| >6 | 87 (78%) | 95 (82%) | 91 (82%) | |||||||
| NICU admission | 34 (30%) | 27 (23%) | 22 (20%) | 0.097 (ANOVA) | 2.35 | N/A | N/C | N/C | N/C | |
| Stillbirths | 14 (13%) | 28 (24%)* | 10 (9%) | 0.003 (ANOVA) | 5.78 | N/A | 2.5 | 0.7 | 3.2 | |
| Infants’ death | 13 (12%) | 26 (23%)* | 10 (9%) | 0.008 (ANOVA) | 4.87 | N/A | 2.4 | 0.6 | 2.9 | |
NICU: Neonatal intensive care unit.
Categorical variables are presented as frequency (percentages) and continuous variables are presented as mean value ± SD.
One-way ANOVA or χ 2 -test was performed for statistical analysis.
The Bonferroni test was used for post hoc analysis.
p-value < 0.05 and t > 2.406 were considered as significant.
*Intravenous nicardipine-emergent adverse effects.
The effect was considered as “1” and the absence of effect was considered as “0” for statistical analysis.
χ 2 -test: The Chi-square test for independence, N/A: not applicable, Df: degree of freedom, N/C: not calculated.
3.5 Risk of adverse infant outcomes
A dosage amount of total of 50 mg/woman or more of intravenous nicardipine required to control the blood pressure to less than 150/100 mmHg (p = 0.045, multivariate analysis) and 40 mg/woman or more of oral nifedipine required to control the blood pressure to less than 150/100 mmHg (p = 0.048, multivariate analysis) in women with less than 32 weeks of gestation age (p = 0.021, multivariate analysis) was associated with adverse infants’ outcomes. While this dosage amount in women with less than 34 weeks of gestation age was not associated with adverse infant outcomes (p = 0.502, multivariate analysis).
3.6 Relative infant dose of calcium channel blocker
The relative infant dose of calcium channel blocker in infants born to women in the NF cohort was 5.95 ± 1.74%, in the ND cohort was 10.07 ± 2.04%, and in the NP cohort was 4.64 ± 2.25%.
4 Discussion
This is a retrospective study comparing three cohorts of preeclamptic mothers treated with nifedipine alone, nifedipine plus phytosterol, and nicardipine infusion. Phytosterol was found to have a synergistic effect on the action of nifedipine in the time and amount of calcium channel blocker required to control blood pressure to less than 150/100 mmHg, the time until a further hypertensive crisis, and maternal and infants’ treatment-emergent adverse effects compared to oral nifedipine alone or intravenous nicardipine. The results of the preeclampsia management of the current study agreed with those of randomized clinical trials [13,14]. Oral nifedipine and intravenous nicardipine are common drugs used for the management of preeclampsia [3]. Phytosterol has a plant origin and it is proven to be safe during pregnancy [20]. Also, the additive or synergistic effect can delay further hypertensive crisis after the control of hypertension [21]. Phytosterol has been evaluated in a meta-analysis and was shown to reduce both systolic and diastolic blood pressure by an average of 1.55 and 0.84 mmHg, respectively, in data pooled from 19 randomized clinical trials [21]. It has been supported as a food supplement to reduce cardiovascular risks by organizations such as the United States Food and Drug Administration. This is still insufficient to recommend it to pregnant women since its safety profile has not been thoroughly investigated. Oral phytosterol with nifedipine provides a synergistic effect to control hypertension for the management of severe preeclampsia and advantages of a delay crisis in preeclampsia women.
The time required to control blood pressure to less than 150/100 mmHg for women suffering from preeclampsia was shorter and the time until a further hypertensive crisis occurred was longer in the case of intravenous nicardipine than oral nifedipine. Nifedipine is a very short-acting drug so the efficiency of lowering the blood pressure within a few minutes of administration relative to nicardipine is not very important, but once the blood pressure is down, the drug is so short-acting that keeping the blood pressure down will require other medications with a longer duration of action.
The amount of calcium channel blocker required to control blood pressure to less than 150/100 mmHg was less in the case of oral nifedipine than intravenous nicardipine. Moreover, controlled intravenous nicardipine was associated with undesirable tocolytic effects, stillbirths, and infant death. Women with severe preeclampsia have a higher risk of adverse pregnancy outcomes than women with chronic/gestational hypertension [22]. Severe intrauterine growth restriction and placental abruption are responsible for stillbirths and infant death [6]. The antihypertensive agent can reduce uteroplacental blood flow in women with less than 32 weeks of gestation age, which can in turn result in severe intrauterine growth restriction and placental abruption [23]. The reason for different outcome results for oral nifedipine and intravenous nicardipine is that different mechanisms of action for reduction in blood pressure i.e., oral nifedipine gradually decreases blood pressure while intravenous nicardipine reduces blood pressure by rapid onset of action [16]. Neonatal outcomes are better with oral nifedipine in the management of preeclampsia [22]. It is well known that a fast reduction in increased blood pressure may be associated with cardiotocographic signs of fetal distress. Intravenous nicardipine is superiorly effective compared to oral nifedipine in the management of preeclampsia but this treatment has associated risk for infants’ health, especially in women with less than 32 weeks of gestation age, and undesirable tocolytic effect.
The study reported that oral nifedipine, oral phytosterol, and intravenous nicardipine did not significantly affect maternal health. These results indicated that oral nifedipine, intravenous nicardipine, and oral phytosterol are safe for women suffering from severe preeclampsia. In the context of perinatal mortality, the other infants’ outcomes are also required to be considered to reach this conclusion.
The time required to control blood pressure for NP was the shortest among the three cohorts. The use of oral medications in severe preeclampsia is potentially problematic as some women may have altered sensorium or nausea/vomiting and be unable to safely swallow pills; also, oral medications such as short-acting nifedipine cause unpredictable reductions in blood pressure which at times can be very precipitous. Oral nifedipine plus phytosterol gradually and precipitously lower blood pressure than nicardipine and other medications that are recommended for use in severe preeclampsia such as hydralazine and labetalol. Further research is required to find out the paradoxical results of the current study with expected outcomes.
Relative infant dose of calcium channel blockers of infants of women who received intravenous nicardipine was reported higher than 10%. A total of 10% or more of the relative infant dose of any drug is not recommended because of the lower drug clearance capacity of infants [16]. The intravenous administration of nicardipine is the likely explanation for the higher relative infant dose. Nicardipine clearance in the placenta cannot be ruled out.
The absolute incidence of 9–24% stillbirth is very high. The ND cohort presented a very-high frequency of stillbirths and neonatal deaths (summing both, almost half of the women who received this medication lost their babies). The neonatal death rate was also so high among all women. This was not near zero. Although fetal monitoring is a normal policy in China, the setting has no fetal monitoring (this is a resource issue locally). This is an unacceptable fetal and infant death rate. It raises questions on possible unsafe management of pregnant women with preeclampsia especially in the average gestational age of 33–34 weeks. Intravenous nicardipine should not be a standard choice for the management of severe preeclampsia in pregnant women. Also, clear Chinese guidelines are required from the Chinese Society of Obstetrics and Gynecology for severe preeclampsia management.
None of the women received magnesium sulfate. Administration of magnesium sulfate is a clear recommendation, especially for severe preeclampsia before 32 weeks of gestation (the current study had 63 pregnant women with gestation less than 32 weeks) because its neuroprotective role for the newborn and anticonvulsant for pregnant women have been scientifically proven. This is a wrong approach, both ethically and methodologically. The worse perceptions and experiences of healthcare providers related to the administration of magnesium sulfate to the parent and the referring institutes restrict the use of magnesium sulfate for severe preeclampsia. Clear Chinese guidelines are required from the Chinese Society of Obstetrics and Gynecology for the use of magnesium sulfate for severe preeclampsia.
The starting dose of nicardipine used in the available research [16] cited by the current study was 0.5 mg/h, not 1 mg/h as described in the methods section of the current study. However, the time required to achieve blood pressure less than 150/100 mmHg for women of the ND cohort was 50.63 ± 9.56 min/woman. Previous studies demonstrated that nicardipine has a fast onset of action (within 10 min) and a short elimination half-life (2–5 min), resulting in a fast and controllable antihypertensive effect. Sufficient reduction in blood pressure occurs most of the time within 20 min if the initial infusion rate is set at 2–3 mg/h of nicardipine with increments of 0.5–1 mg/h. A relatively low initial dose (continuous infusion of 1 mg/h) may be the potential reason for the same. However, the dosage of nicardipine used (1 mg/h) in the current study differed from the majority of previous studies for the fast action of nicardipine due to severe preeclampsia.
The use of phytosterols with calcium channel blockers is an interesting idea and is worthy of investigation. However, the study was a retrospective study. The other limitations of the study, for example, the underlying mechanism for the synergistic effect of oral phytosterol with nifedipine is still not clear. It is hypothesized that oral phytosterol can decrease the production of matrix metalloproteinase-3 and matrix metalloproteinase-13 [24], which are responsible for preeclampsia [25]. A placebo-controlled trial is required to elucidate the mechanism of action responsible for the synergistic effect of oral phytosterol with nifedipine to control hypertension for the management of preeclampsia. The long-term effects of treatments on maternal and infant outcomes were not evaluated. The perinatal mortality rate for a cohort with a mean gestational age of 34 weeks (3.0 kg) seems high. The conditions of fetal surveillance, the utilization of c-sections, and the infants’ nursery capacity for respiratory support were not discussed. With data on phytosterol alone, it is inaccurate to state that the effects of nifedipine and phytosterol are truly synergistic as suggested or merely additive. Neither the dose of nifedipine or nicardipine was increased nor other drugs were added to avoid hypertensive crises. The possible justification is that the dose of the drug and intervention(s) were kept less to avoid any fetal effect. Importantly, in 2020, The American College of Obstetrics and Gynecology [26] published evidence-based clinical guidelines for the diagnosis and management of gestational hypertension and preeclampsia and recommended prophylactic aspirin between 12 and 28 weeks of gestation age. However, the current study data were from before the publication of these guidelines.
5 Conclusion
Intravenous nicardipine is superiorly effective to oral nifedipine for the management of preeclampsia but is associated with stillbirth, infant death, especially with less than 32 weeks of gestation age, and undesirable tocolytic effect. Oral nifedipine is generally used by physicians for the management of high blood pressure in severe preeclampsia but it has slower management of high blood pressure and risk of further hypertensive crisis after the control of hypertension. Also, oral nifedipine has the risk of adverse infant outcomes if 40 mg or more amount is used to control blood pressure to less than 150/100 mmHg. The current study provides evidence that oral phytosterol with nifedipine combination has a synergistic or additive effect to control hypertension for the management of preeclampsia with fewer risks of maternal and infant adverse outcomes, especially with less than 32 weeks of gestation age. Also, oral phytosterol appears safe for women and infants. The current study recommended clear Chinese guidelines to the Chinese Society of Obstetrics and Gynecology for severe preeclampsia management. The study is recommending a diet other than the mother’s milk to the infants if delivery is done under intravenous nicardipine to rule out nicardipine clearance in the placenta. There is already evidence of the effects of various antihypertensive medications on preeclampsia. Most of the available evidence is limited by the lack of controlled randomized trials, but over recent years some large series have been published that illustrate the advantages and disadvantages of the main available drugs concerning the main phenotypes of preeclampsia (i.e., early vs late forms). The current study contains information of interest but the retrospective design and the relatively small numbers limit the interpretations of the results. However, it adds substantially novel information to what is already known on the subject.
Acknowledgments
The authors are thankful to the Obstetrics, Gynecology, medical, and non-medical staff of the First People’s Hospital of Lianyungang, Lianyungang, Jiangsu, China.
-
Funding information: Authors state no funding involved.
-
Authors contributions: The authors have read and approved the manuscript for publication. S.M. was the project administrator and contributed to the supervision, literature review, resources, and methodology of the study. L.Z. contributed to the literature review, resources, methodology, investigation, and software of the study. T.Z. contributed to the conceptualization, methodology, resources, literature review, and formal analysis of the study. T.Q. contributed to the formal analysis, data curation, validation, methodology, and literature review of the study. W.W. contributed to the methodology, literature review, and resources of the study and drafted, reviewed, and edited the manuscript for intellectual content. The authors agree to be accountable for all aspects of the work, ensuring integrity and accuracy.
-
Conflict of interest: Authors state no conflict of interest.
-
Data availability statement: The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
References
[1] Bijvank SW, Visser W, Duvekot JJ, Steegers EA, Edens MA, Roofthooft DW, et al. Ketanserin versus dihydralazine for the treatment of severe hypertension in early-onset preeclampsia: A double-blind randomized controlled trial. Eur J Obstet Gynecol Reprod Biol. 2015;189:106–11.10.1016/j.ejogrb.2015.02.002Suche in Google Scholar PubMed
[2] Shi DD, Yang FZ, Zhou L, Wang N. Oral nifedipine vs intravenous labetalol for treatment of pregnancy-induced severe preeclampsia. J Clin Pharm Ther. 2016;41:657–61.10.1111/jcpt.12439Suche in Google Scholar PubMed
[3] Abalos E, Duley L, Steyn DW, Gialdini C. Antihypertensive drug therapy for mild to moderate hypertension during pregnancy. Cochrane Database Syst Rev. 2018;10:CD002252.10.1002/14651858.CD002252.pub4Suche in Google Scholar PubMed PubMed Central
[4] Poon LC, Shennan A, Hyett JA, Kapur A, Hadar E, Divakar H, et al. The International Federation of Gynecology and Obstetrics (FIGO) initiative on preeclampsia: A pragmatic guide for first-trimester screening and prevention. Int J Gynaecol Obstet. 2019;145:1–33.10.1002/ijgo.12892Suche in Google Scholar PubMed
[5] Cao W, Wang X, Chen T, Qin M, Wang Z, Wang Q, et al. Successful rescue of antepartum eclampsia in a Chinese patient: Case report. Medicine. 2019;98:1–4.10.1097/MD.0000000000014301Suche in Google Scholar PubMed PubMed Central
[6] Wasim T, Agha S, Saeed K, Riaz A. Oral nifidepine versus IV labetalol in severe preeclampsia: A randomized control trial. Pak J Med Sci. 2020;36:1147–52.10.12669/pjms.36.6.2591Suche in Google Scholar PubMed PubMed Central
[7] WHO Recommendations for Prevention and Treatment of Preeclampsia and Eclampsia. Geneva: World Health Organization; 2011. Summary of recommendations. https://www.ncbi.nlm.nih.gov/books/NBK140555/.Suche in Google Scholar
[8] Hypertensive Disorders in Pregnancy Subgroup, Chinese Society of Obstetrics and Gynecology, Chinese Medical Association; Hypertensive Disorders in Pregnancy Subgroup Chinese Society of Obstetrics and Gynecology Chinese Medical Association. Diagnosis and treatment guideline of hypertensive disorders in pregnancy. Chin J Obstet Gynecol. 2015;50:721–8 [Article in Chinese].Suche in Google Scholar
[9] American College of Obstetricians and Gynecologists; Task Force on Hypertension in Pregnancy. Hypertension in pregnancy. Report of the American College of Obstetricians and Gynecologists’ Task Force on Hypertension in Pregnancy. Obstet Gynecol. 2013;122:1122–31.Suche in Google Scholar
[10] National Institute for Health and Care Guidelines. Hypertension in pregnancy: Diagnosis and management. https://www.nice.org.uk/guidance/ng133/resources/hypertension-in-pregnancy-diagnosis-and-management-pdf-66141717671365 [Accessed on October 2, 2020].Suche in Google Scholar
[11] Raheem IA, Saaid R, Omar SZ, Tan PC. Oral nifedipine versus intravenous labetalol for acute blood pressure control in hypertensive emergencies of pregnancy: A randomised trial. BLOG. 2012;119:78–85.10.1111/j.1471-0528.2011.03151.xSuche in Google Scholar PubMed
[12] Bellos I, Pergialiotis V, Papapanagiotou A, Loutradis D, Daskalakis G. Comparative efficacy and safety of oral antihypertensive agents in pregnant women with chronic hypertension: A network meta-analysis. Am J Obstet Gynecol. 2020;223:525–37.10.1016/j.ajog.2020.03.016Suche in Google Scholar PubMed
[13] Xiao S, Zhang M, Liang Y, Wang D. Celastrol synergizes with oral nifedipine to attenuate hypertension in preeclampsia: A randomized, placebo-controlled, and double blinded trial. J Am Soc Hypertens. 2017;11:598–603.10.1016/j.jash.2017.07.004Suche in Google Scholar PubMed
[14] Zhang M, Feng H. Phytosterol enhances oral nifedipine treatment in pregnancy-induced preeclampsia: A placebo-controlled, double-blinded, randomized clinical trial. Exp Biol Med. 2019;244:1120–4.10.1177/1535370219861574Suche in Google Scholar PubMed PubMed Central
[15] Trang HN, Tuyet HD. Intravenous perfusor of nicardipine to treat severe pre-esclampsia at Vietnam. J Gynecol Women’s Health. 2019;15(2):555906.10.19080/JGWH.2019.15.555906Suche in Google Scholar
[16] Matsumura H, Takagi K, Seki H, Ono Y, Ichinose S, Masuko H, et al. Placental transfer of intravenous nicardipine and disposition into breast milk during the control of hypertension in women with preeclampsia. Hypertens Pregnancy. 2014;33:93–101.10.3109/10641955.2013.846367Suche in Google Scholar PubMed
[17] Lee HL, Lu KC, Foo J, Huang IT, Fan YC, Tsai PS, et al. Different impacts of various tocolytic agents on increased risk of postoperative hemorrhage in preterm labor women undergoing cesarean delivery: A population-based cohort study. Medicine. 2020;99:1–7.10.1097/MD.0000000000023651Suche in Google Scholar PubMed PubMed Central
[18] Serena C, Begot E, Cros J, Hodler C, Fedou AL, Nathan-Denizot N, et al. Nicardipine-induced acute pulmonary edema: A rare but severe complication of tocolysis. Case Rep Crit Care. 2014;2014:242703.10.1155/2014/242703Suche in Google Scholar PubMed PubMed Central
[19] Heida KY, Zeeman GG, Van Veen TR, Hulzebos CV. Neonatal side effects of maternal labetalol treatment in severe preeclampsia. Early Hum Dev. 2012;88:503–7.10.1016/j.earlhumdev.2011.12.012Suche in Google Scholar PubMed
[20] Correani A, Visentin S, Cosmi E, Ponchia E, D’Aronco S, Simonato M, et al. The maternal-fetal gradient of free and esterified phytosterols at the time of delivery in humans. Clin Nutr. 2018;37:2107–12.10.1016/j.clnu.2017.10.004Suche in Google Scholar PubMed
[21] Ghaedi E, Foshati S, Ziaei R, Beigrezaei S, Kord-Varkaneh H, Ghavami A, et al. Effects of phytosterols supplementation on blood pressure: A systematic review and meta-analysis. Clin Nutr. 2020;39(9):2702–10.10.1016/j.clnu.2019.12.020Suche in Google Scholar PubMed
[22] Dassah ET, Kusi-Mensah E, Morhe ES, Odoi AT. Maternal and perinatal outcomes among women with hypertensive disorders in pregnancy in Kumasi, Ghana. PLoS One. 2019;14:1–13.10.1371/journal.pone.0223478Suche in Google Scholar PubMed PubMed Central
[23] Barton JR, Sibai BM. Controversies regarding diagnosis and treatment of severe hypertension in pregnancy. Clin Obstet Gynecol. 2017;60:198–205.10.1097/GRF.0000000000000254Suche in Google Scholar PubMed
[24] Gabay O, Sanchez C, Salvat C, Chevy F, Breton M, Nourissat G, et al. Stigmasterol: A phytosterol with potential anti-osteoarthritic properties. Osteoarthr Cartil. 2010;18:106–16.10.1016/j.joca.2009.08.019Suche in Google Scholar PubMed
[25] Laskowska M. Altered maternal serum matrix metalloproteinases MMP-2, MMP-3, MMP-9, and MMP-13 in severe early- and late-onset preeclampsia. Biomed Res Int. 2017;2017:6432426.10.1155/2017/6432426Suche in Google Scholar PubMed PubMed Central
[26] The American College of Obstetrics and Gynecology. Gestational Hypertension and Preeclampsia: ACOG Practice Bulletin, Number 222. Obstet Gynecol. 2020;135(6):e237–60.10.1097/AOG.0000000000003891Suche in Google Scholar PubMed
© 2023 the author(s), published by De Gruyter
This work is licensed under the Creative Commons Attribution 4.0 International License.
Artikel in diesem Heft
- Biomedical Sciences
- Systemic investigation of inetetamab in combination with small molecules to treat HER2-overexpressing breast and gastric cancers
- Immunosuppressive treatment for idiopathic membranous nephropathy: An updated network meta-analysis
- Identifying two pathogenic variants in a patient with pigmented paravenous retinochoroidal atrophy
- Effects of phytoestrogens combined with cold stress on sperm parameters and testicular proteomics in rats
- A case of pulmonary embolism with bad warfarin anticoagulant effects caused by E. coli infection
- Neutrophilia with subclinical Cushing’s disease: A case report and literature review
- Isoimperatorin alleviates lipopolysaccharide-induced periodontitis by downregulating ERK1/2 and NF-κB pathways
- Immunoregulation of synovial macrophages for the treatment of osteoarthritis
- Novel CPLANE1 c.8948dupT (p.P2984Tfs*7) variant in a child patient with Joubert syndrome
- Antiphospholipid antibodies and the risk of thrombosis in myeloproliferative neoplasms
- Immunological responses of septic rats to combination therapy with thymosin α1 and vitamin C
- High glucose and high lipid induced mitochondrial dysfunction in JEG-3 cells through oxidative stress
- Pharmacological inhibition of the ubiquitin-specific protease 8 effectively suppresses glioblastoma cell growth
- Levocarnitine regulates the growth of angiotensin II-induced myocardial fibrosis cells via TIMP-1
- Age-related changes in peripheral T-cell subpopulations in elderly individuals: An observational study
- Single-cell transcription analysis reveals the tumor origin and heterogeneity of human bilateral renal clear cell carcinoma
- Identification of iron metabolism-related genes as diagnostic signatures in sepsis by blood transcriptomic analysis
- Long noncoding RNA ACART knockdown decreases 3T3-L1 preadipocyte proliferation and differentiation
- Surgery, adjuvant immunotherapy plus chemotherapy and radiotherapy for primary malignant melanoma of the parotid gland (PGMM): A case report
- Dosimetry comparison with helical tomotherapy, volumetric modulated arc therapy, and intensity-modulated radiotherapy for grade II gliomas: A single‑institution case series
- Soy isoflavone reduces LPS-induced acute lung injury via increasing aquaporin 1 and aquaporin 5 in rats
- Refractory hypokalemia with sexual dysplasia and infertility caused by 17α-hydroxylase deficiency and triple X syndrome: A case report
- Meta-analysis of cancer risk among end stage renal disease undergoing maintenance dialysis
- 6-Phosphogluconate dehydrogenase inhibition arrests growth and induces apoptosis in gastric cancer via AMPK activation and oxidative stress
- Experimental study on the optimization of ANM33 release in foam cells
- Primary retroperitoneal angiosarcoma: A case report
- Metabolomic analysis-identified 2-hydroxybutyric acid might be a key metabolite of severe preeclampsia
- Malignant pleural effusion diagnosis and therapy
- Effect of spaceflight on the phenotype and proteome of Escherichia coli
- Comparison of immunotherapy combined with stereotactic radiotherapy and targeted therapy for patients with brain metastases: A systemic review and meta-analysis
- Activation of hypermethylated P2RY1 mitigates gastric cancer by promoting apoptosis and inhibiting proliferation
- Association between the VEGFR-2 -604T/C polymorphism (rs2071559) and type 2 diabetic retinopathy
- The role of IL-31 and IL-34 in the diagnosis and treatment of chronic periodontitis
- Triple-negative mouse breast cancer initiating cells show high expression of beta1 integrin and increased malignant features
- mNGS facilitates the accurate diagnosis and antibiotic treatment of suspicious critical CNS infection in real practice: A retrospective study
- The apatinib and pemetrexed combination has antitumor and antiangiogenic effects against NSCLC
- Radiotherapy for primary thyroid adenoid cystic carcinoma
- Design and functional preliminary investigation of recombinant antigen EgG1Y162–EgG1Y162 against Echinococcus granulosus
- Effects of losartan in patients with NAFLD: A meta-analysis of randomized controlled trial
- Bibliometric analysis of METTL3: Current perspectives, highlights, and trending topics
- Performance comparison of three scaling algorithms in NMR-based metabolomics analysis
- PI3K/AKT/mTOR pathway and its related molecules participate in PROK1 silence-induced anti-tumor effects on pancreatic cancer
- The altered expression of cytoskeletal and synaptic remodeling proteins during epilepsy
- Effects of pegylated recombinant human granulocyte colony-stimulating factor on lymphocytes and white blood cells of patients with malignant tumor
- Prostatitis as initial manifestation of Chlamydia psittaci pneumonia diagnosed by metagenome next-generation sequencing: A case report
- NUDT21 relieves sevoflurane-induced neurological damage in rats by down-regulating LIMK2
- Association of interleukin-10 rs1800896, rs1800872, and interleukin-6 rs1800795 polymorphisms with squamous cell carcinoma risk: A meta-analysis
- Exosomal HBV-DNA for diagnosis and treatment monitoring of chronic hepatitis B
- Shear stress leads to the dysfunction of endothelial cells through the Cav-1-mediated KLF2/eNOS/ERK signaling pathway under physiological conditions
- Interaction between the PI3K/AKT pathway and mitochondrial autophagy in macrophages and the leukocyte count in rats with LPS-induced pulmonary infection
- Meta-analysis of the rs231775 locus polymorphism in the CTLA-4 gene and the susceptibility to Graves’ disease in children
- Cloning, subcellular localization and expression of phosphate transporter gene HvPT6 of hulless barley
- Coptisine mitigates diabetic nephropathy via repressing the NRLP3 inflammasome
- Significant elevated CXCL14 and decreased IL-39 levels in patients with tuberculosis
- Whole-exome sequencing applications in prenatal diagnosis of fetal bowel dilatation
- Gemella morbillorum infective endocarditis: A case report and literature review
- An unusual ectopic thymoma clonal evolution analysis: A case report
- Severe cumulative skin toxicity during toripalimab combined with vemurafenib following toripalimab alone
- Detection of V. vulnificus septic shock with ARDS using mNGS
- Novel rare genetic variants of familial and sporadic pulmonary atresia identified by whole-exome sequencing
- The influence and mechanistic action of sperm DNA fragmentation index on the outcomes of assisted reproduction technology
- Novel compound heterozygous mutations in TELO2 in an infant with You-Hoover-Fong syndrome: A case report and literature review
- ctDNA as a prognostic biomarker in resectable CLM: Systematic review and meta-analysis
- Diagnosis of primary amoebic meningoencephalitis by metagenomic next-generation sequencing: A case report
- Phylogenetic analysis of promoter regions of human Dolichol kinase (DOLK) and orthologous genes using bioinformatics tools
- Collagen changes in rabbit conjunctiva after conjunctival crosslinking
- Effects of NM23 transfection of human gastric carcinoma cells in mice
- Oral nifedipine and phytosterol, intravenous nicardipine, and oral nifedipine only: Three-arm, retrospective, cohort study for management of severe preeclampsia
- Case report of hepatic retiform hemangioendothelioma: A rare tumor treated with ultrasound-guided microwave ablation
- Curcumin induces apoptosis in human hepatocellular carcinoma cells by decreasing the expression of STAT3/VEGF/HIF-1α signaling
- Rare presentation of double-clonal Waldenström macroglobulinemia with pulmonary embolism: A case report
- Giant duplication of the transverse colon in an adult: A case report and literature review
- Ectopic thyroid tissue in the breast: A case report
- SDR16C5 promotes proliferation and migration and inhibits apoptosis in pancreatic cancer
- Vaginal metastasis from breast cancer: A case report
- Screening of the best time window for MSC transplantation to treat acute myocardial infarction with SDF-1α antibody-loaded targeted ultrasonic microbubbles: An in vivo study in miniswine
- Inhibition of TAZ impairs the migration ability of melanoma cells
- Molecular complexity analysis of the diagnosis of Gitelman syndrome in China
- Effects of maternal calcium and protein intake on the development and bone metabolism of offspring mice
- Identification of winter wheat pests and diseases based on improved convolutional neural network
- Ultra-multiplex PCR technique to guide treatment of Aspergillus-infected aortic valve prostheses
- Virtual high-throughput screening: Potential inhibitors targeting aminopeptidase N (CD13) and PIKfyve for SARS-CoV-2
- Immune checkpoint inhibitors in cancer patients with COVID-19
- Utility of methylene blue mixed with autologous blood in preoperative localization of pulmonary nodules and masses
- Integrated analysis of the microbiome and transcriptome in stomach adenocarcinoma
- Berberine suppressed sarcopenia insulin resistance through SIRT1-mediated mitophagy
- DUSP2 inhibits the progression of lupus nephritis in mice by regulating the STAT3 pathway
- Lung abscess by Fusobacterium nucleatum and Streptococcus spp. co-infection by mNGS: A case series
- Genetic alterations of KRAS and TP53 in intrahepatic cholangiocarcinoma associated with poor prognosis
- Granulomatous polyangiitis involving the fourth ventricle: Report of a rare case and a literature review
- Studying infant mortality: A demographic analysis based on data mining models
- Metaplastic breast carcinoma with osseous differentiation: A report of a rare case and literature review
- Protein Z modulates the metastasis of lung adenocarcinoma cells
- Inhibition of pyroptosis and apoptosis by capsaicin protects against LPS-induced acute kidney injury through TRPV1/UCP2 axis in vitro
- TAK-242, a toll-like receptor 4 antagonist, against brain injury by alleviates autophagy and inflammation in rats
- Primary mediastinum Ewing’s sarcoma with pleural effusion: A case report and literature review
- Association of ADRB2 gene polymorphisms and intestinal microbiota in Chinese Han adolescents
- Tanshinone IIA alleviates chondrocyte apoptosis and extracellular matrix degeneration by inhibiting ferroptosis
- Study on the cytokines related to SARS-Cov-2 in testicular cells and the interaction network between cells based on scRNA-seq data
- Effect of periostin on bone metabolic and autophagy factors during tooth eruption in mice
- HP1 induces ferroptosis of renal tubular epithelial cells through NRF2 pathway in diabetic nephropathy
- Intravaginal estrogen management in postmenopausal patients with vaginal squamous intraepithelial lesions along with CO2 laser ablation: A retrospective study
- Hepatocellular carcinoma cell differentiation trajectory predicts immunotherapy, potential therapeutic drugs, and prognosis of patients
- Effects of physical exercise on biomarkers of oxidative stress in healthy subjects: A meta-analysis of randomized controlled trials
- Identification of lysosome-related genes in connection with prognosis and immune cell infiltration for drug candidates in head and neck cancer
- Development of an instrument-free and low-cost ELISA dot-blot test to detect antibodies against SARS-CoV-2
- Research progress on gas signal molecular therapy for Parkinson’s disease
- Adiponectin inhibits TGF-β1-induced skin fibroblast proliferation and phenotype transformation via the p38 MAPK signaling pathway
- The G protein-coupled receptor-related gene signatures for predicting prognosis and immunotherapy response in bladder urothelial carcinoma
- α-Fetoprotein contributes to the malignant biological properties of AFP-producing gastric cancer
- CXCL12/CXCR4/CXCR7 axis in placenta tissues of patients with placenta previa
- Association between thyroid stimulating hormone levels and papillary thyroid cancer risk: A meta-analysis
- Significance of sTREM-1 and sST2 combined diagnosis for sepsis detection and prognosis prediction
- Diagnostic value of serum neuroactive substances in the acute exacerbation of chronic obstructive pulmonary disease complicated with depression
- Research progress of AMP-activated protein kinase and cardiac aging
- TRIM29 knockdown prevented the colon cancer progression through decreasing the ubiquitination levels of KRT5
- Cross-talk between gut microbiota and liver steatosis: Complications and therapeutic target
- Metastasis from small cell lung cancer to ovary: A case report
- The early diagnosis and pathogenic mechanisms of sepsis-related acute kidney injury
- The effect of NK cell therapy on sepsis secondary to lung cancer: A case report
- Erianin alleviates collagen-induced arthritis in mice by inhibiting Th17 cell differentiation
- Loss of ACOX1 in clear cell renal cell carcinoma and its correlation with clinical features
- Signalling pathways in the osteogenic differentiation of periodontal ligament stem cells
- Crosstalk between lactic acid and immune regulation and its value in the diagnosis and treatment of liver failure
- Clinicopathological features and differential diagnosis of gastric pleomorphic giant cell carcinoma
- Traumatic brain injury and rTMS-ERPs: Case report and literature review
- Extracellular fibrin promotes non-small cell lung cancer progression through integrin β1/PTEN/AKT signaling
- Knockdown of DLK4 inhibits non-small cell lung cancer tumor growth by downregulating CKS2
- The co-expression pattern of VEGFR-2 with indicators related to proliferation, apoptosis, and differentiation of anagen hair follicles
- Inflammation-related signaling pathways in tendinopathy
- CD4+ T cell count in HIV/TB co-infection and co-occurrence with HL: Case report and literature review
- Clinical analysis of severe Chlamydia psittaci pneumonia: Case series study
- Bioinformatics analysis to identify potential biomarkers for the pulmonary artery hypertension associated with the basement membrane
- Influence of MTHFR polymorphism, alone or in combination with smoking and alcohol consumption, on cancer susceptibility
- Catharanthus roseus (L.) G. Don counteracts the ampicillin resistance in multiple antibiotic-resistant Staphylococcus aureus by downregulation of PBP2a synthesis
- Combination of a bronchogenic cyst in the thoracic spinal canal with chronic myelocytic leukemia
- Bacterial lipoprotein plays an important role in the macrophage autophagy and apoptosis induced by Salmonella typhimurium and Staphylococcus aureus
- TCL1A+ B cells predict prognosis in triple-negative breast cancer through integrative analysis of single-cell and bulk transcriptomic data
- Ezrin promotes esophageal squamous cell carcinoma progression via the Hippo signaling pathway
- Ferroptosis: A potential target of macrophages in plaque vulnerability
- Predicting pediatric Crohn's disease based on six mRNA-constructed risk signature using comprehensive bioinformatic approaches
- Applications of genetic code expansion and photosensitive UAAs in studying membrane proteins
- HK2 contributes to the proliferation, migration, and invasion of diffuse large B-cell lymphoma cells by enhancing the ERK1/2 signaling pathway
- IL-17 in osteoarthritis: A narrative review
- Circadian cycle and neuroinflammation
- Probiotic management and inflammatory factors as a novel treatment in cirrhosis: A systematic review and meta-analysis
- Hemorrhagic meningioma with pulmonary metastasis: Case report and literature review
- SPOP regulates the expression profiles and alternative splicing events in human hepatocytes
- Knockdown of SETD5 inhibited glycolysis and tumor growth in gastric cancer cells by down-regulating Akt signaling pathway
- PTX3 promotes IVIG resistance-induced endothelial injury in Kawasaki disease by regulating the NF-κB pathway
- Pancreatic ectopic thyroid tissue: A case report and analysis of literature
- The prognostic impact of body mass index on female breast cancer patients in underdeveloped regions of northern China differs by menopause status and tumor molecular subtype
- Report on a case of liver-originating malignant melanoma of unknown primary
- Case report: Herbal treatment of neutropenic enterocolitis after chemotherapy for breast cancer
- The fibroblast growth factor–Klotho axis at molecular level
- Characterization of amiodarone action on currents in hERG-T618 gain-of-function mutations
- A case report of diagnosis and dynamic monitoring of Listeria monocytogenes meningitis with NGS
- Effect of autologous platelet-rich plasma on new bone formation and viability of a Marburg bone graft
- Small breast epithelial mucin as a useful prognostic marker for breast cancer patients
- Continuous non-adherent culture promotes transdifferentiation of human adipose-derived stem cells into retinal lineage
- Nrf3 alleviates oxidative stress and promotes the survival of colon cancer cells by activating AKT/BCL-2 signal pathway
- Favorable response to surufatinib in a patient with necrolytic migratory erythema: A case report
- Case report of atypical undernutrition of hypoproteinemia type
- Down-regulation of COL1A1 inhibits tumor-associated fibroblast activation and mediates matrix remodeling in the tumor microenvironment of breast cancer
- Sarcoma protein kinase inhibition alleviates liver fibrosis by promoting hepatic stellate cells ferroptosis
- Research progress of serum eosinophil in chronic obstructive pulmonary disease and asthma
- Clinicopathological characteristics of co-existing or mixed colorectal cancer and neuroendocrine tumor: Report of five cases
- Role of menopausal hormone therapy in the prevention of postmenopausal osteoporosis
- Precisional detection of lymph node metastasis using tFCM in colorectal cancer
- Advances in diagnosis and treatment of perimenopausal syndrome
- A study of forensic genetics: ITO index distribution and kinship judgment between two individuals
- Acute lupus pneumonitis resembling miliary tuberculosis: A case-based review
- Plasma levels of CD36 and glutathione as biomarkers for ruptured intracranial aneurysm
- Fractalkine modulates pulmonary angiogenesis and tube formation by modulating CX3CR1 and growth factors in PVECs
- Novel risk prediction models for deep vein thrombosis after thoracotomy and thoracoscopic lung cancer resections, involving coagulation and immune function
- Exploring the diagnostic markers of essential tremor: A study based on machine learning algorithms
- Evaluation of effects of small-incision approach treatment on proximal tibia fracture by deep learning algorithm-based magnetic resonance imaging
- An online diagnosis method for cancer lesions based on intelligent imaging analysis
- Medical imaging in rheumatoid arthritis: A review on deep learning approach
- Predictive analytics in smart healthcare for child mortality prediction using a machine learning approach
- Utility of neutrophil–lymphocyte ratio and platelet–lymphocyte ratio in predicting acute-on-chronic liver failure survival
- A biomedical decision support system for meta-analysis of bilateral upper-limb training in stroke patients with hemiplegia
- TNF-α and IL-8 levels are positively correlated with hypobaric hypoxic pulmonary hypertension and pulmonary vascular remodeling in rats
- Stochastic gradient descent optimisation for convolutional neural network for medical image segmentation
- Comparison of the prognostic value of four different critical illness scores in patients with sepsis-induced coagulopathy
- Application and teaching of computer molecular simulation embedded technology and artificial intelligence in drug research and development
- Hepatobiliary surgery based on intelligent image segmentation technology
- Value of brain injury-related indicators based on neural network in the diagnosis of neonatal hypoxic-ischemic encephalopathy
- Analysis of early diagnosis methods for asymmetric dementia in brain MR images based on genetic medical technology
- Early diagnosis for the onset of peri-implantitis based on artificial neural network
- Clinical significance of the detection of serum IgG4 and IgG4/IgG ratio in patients with thyroid-associated ophthalmopathy
- Forecast of pain degree of lumbar disc herniation based on back propagation neural network
- SPA-UNet: A liver tumor segmentation network based on fused multi-scale features
- Systematic evaluation of clinical efficacy of CYP1B1 gene polymorphism in EGFR mutant non-small cell lung cancer observed by medical image
- Rehabilitation effect of intelligent rehabilitation training system on hemiplegic limb spasms after stroke
- A novel approach for minimising anti-aliasing effects in EEG data acquisition
- ErbB4 promotes M2 activation of macrophages in idiopathic pulmonary fibrosis
- Clinical role of CYP1B1 gene polymorphism in prediction of postoperative chemotherapy efficacy in NSCLC based on individualized health model
- Lung nodule segmentation via semi-residual multi-resolution neural networks
- Evaluation of brain nerve function in ICU patients with Delirium by deep learning algorithm-based resting state MRI
- A data mining technique for detecting malignant mesothelioma cancer using multiple regression analysis
- Markov model combined with MR diffusion tensor imaging for predicting the onset of Alzheimer’s disease
- Effectiveness of the treatment of depression associated with cancer and neuroimaging changes in depression-related brain regions in patients treated with the mediator-deuterium acupuncture method
- Molecular mechanism of colorectal cancer and screening of molecular markers based on bioinformatics analysis
- Monitoring and evaluation of anesthesia depth status data based on neuroscience
- Exploring the conformational dynamics and thermodynamics of EGFR S768I and G719X + S768I mutations in non-small cell lung cancer: An in silico approaches
- Optimised feature selection-driven convolutional neural network using gray level co-occurrence matrix for detection of cervical cancer
- Incidence of different pressure patterns of spinal cerebellar ataxia and analysis of imaging and genetic diagnosis
- Pathogenic bacteria and treatment resistance in older cardiovascular disease patients with lung infection and risk prediction model
- Adoption value of support vector machine algorithm-based computed tomography imaging in the diagnosis of secondary pulmonary fungal infections in patients with malignant hematological disorders
- From slides to insights: Harnessing deep learning for prognostic survival prediction in human colorectal cancer histology
- Ecology and Environmental Science
- Monitoring of hourly carbon dioxide concentration under different land use types in arid ecosystem
- Comparing the differences of prokaryotic microbial community between pit walls and bottom from Chinese liquor revealed by 16S rRNA gene sequencing
- Effects of cadmium stress on fruits germination and growth of two herbage species
- Bamboo charcoal affects soil properties and bacterial community in tea plantations
- Optimization of biogas potential using kinetic models, response surface methodology, and instrumental evidence for biodegradation of tannery fleshings during anaerobic digestion
- Understory vegetation diversity patterns of Platycladus orientalis and Pinus elliottii communities in Central and Southern China
- Studies on macrofungi diversity and discovery of new species of Abortiporus from Baotianman World Biosphere Reserve
- Food Science
- Effect of berrycactus fruit (Myrtillocactus geometrizans) on glutamate, glutamine, and GABA levels in the frontal cortex of rats fed with a high-fat diet
- Guesstimate of thymoquinone diversity in Nigella sativa L. genotypes and elite varieties collected from Indian states using HPTLC technique
- Analysis of bacterial community structure of Fuzhuan tea with different processing techniques
- Untargeted metabolomics reveals sour jujube kernel benefiting the nutritional value and flavor of Morchella esculenta
- Mycobiota in Slovak wine grapes: A case study from the small Carpathians wine region
- Elemental analysis of Fadogia ancylantha leaves used as a nutraceutical in Mashonaland West Province, Zimbabwe
- Microbiological transglutaminase: Biotechnological application in the food industry
- Influence of solvent-free extraction of fish oil from catfish (Clarias magur) heads using a Taguchi orthogonal array design: A qualitative and quantitative approach
- Chromatographic analysis of the chemical composition and anticancer activities of Curcuma longa extract cultivated in Palestine
- The potential for the use of leghemoglobin and plant ferritin as sources of iron
- Investigating the association between dietary patterns and glycemic control among children and adolescents with T1DM
- Bioengineering and Biotechnology
- Biocompatibility and osteointegration capability of β-TCP manufactured by stereolithography 3D printing: In vitro study
- Clinical characteristics and the prognosis of diabetic foot in Tibet: A single center, retrospective study
- Agriculture
- Biofertilizer and NPSB fertilizer application effects on nodulation and productivity of common bean (Phaseolus vulgaris L.) at Sodo Zuria, Southern Ethiopia
- On correlation between canopy vegetation and growth indexes of maize varieties with different nitrogen efficiencies
- Exopolysaccharides from Pseudomonas tolaasii inhibit the growth of Pleurotus ostreatus mycelia
- A transcriptomic evaluation of the mechanism of programmed cell death of the replaceable bud in Chinese chestnut
- Melatonin enhances salt tolerance in sorghum by modulating photosynthetic performance, osmoregulation, antioxidant defense, and ion homeostasis
- Effects of plant density on alfalfa (Medicago sativa L.) seed yield in western Heilongjiang areas
- Identification of rice leaf diseases and deficiency disorders using a novel DeepBatch technique
- Artificial intelligence and internet of things oriented sustainable precision farming: Towards modern agriculture
- Animal Sciences
- Effect of ketogenic diet on exercise tolerance and transcriptome of gastrocnemius in mice
- Combined analysis of mRNA–miRNA from testis tissue in Tibetan sheep with different FecB genotypes
- Isolation, identification, and drug resistance of a partially isolated bacterium from the gill of Siniperca chuatsi
- Tracking behavioral changes of confined sows from the first mating to the third parity
- The sequencing of the key genes and end products in the TLR4 signaling pathway from the kidney of Rana dybowskii exposed to Aeromonas hydrophila
- Development of a new candidate vaccine against piglet diarrhea caused by Escherichia coli
- Plant Sciences
- Crown and diameter structure of pure Pinus massoniana Lamb. forest in Hunan province, China
- Genetic evaluation and germplasm identification analysis on ITS2, trnL-F, and psbA-trnH of alfalfa varieties germplasm resources
- Tissue culture and rapid propagation technology for Gentiana rhodantha
- Effects of cadmium on the synthesis of active ingredients in Salvia miltiorrhiza
- Cloning and expression analysis of VrNAC13 gene in mung bean
- Chlorate-induced molecular floral transition revealed by transcriptomes
- Effects of warming and drought on growth and development of soybean in Hailun region
- Effects of different light conditions on transient expression and biomass in Nicotiana benthamiana leaves
- Comparative analysis of the rhizosphere microbiome and medicinally active ingredients of Atractylodes lancea from different geographical origins
- Distinguish Dianthus species or varieties based on chloroplast genomes
- Comparative transcriptomes reveal molecular mechanisms of apple blossoms of different tolerance genotypes to chilling injury
- Study on fresh processing key technology and quality influence of Cut Ophiopogonis Radix based on multi-index evaluation
- An advanced approach for fig leaf disease detection and classification: Leveraging image processing and enhanced support vector machine methodology
- Erratum
- Erratum to “Protein Z modulates the metastasis of lung adenocarcinoma cells”
- Erratum to “BRCA1 subcellular localization regulated by PI3K signaling pathway in triple-negative breast cancer MDA-MB-231 cells and hormone-sensitive T47D cells”
- Retraction
- Retraction to “Protocatechuic acid attenuates cerebral aneurysm formation and progression by inhibiting TNF-alpha/Nrf-2/NF-kB-mediated inflammatory mechanisms in experimental rats”
Artikel in diesem Heft
- Biomedical Sciences
- Systemic investigation of inetetamab in combination with small molecules to treat HER2-overexpressing breast and gastric cancers
- Immunosuppressive treatment for idiopathic membranous nephropathy: An updated network meta-analysis
- Identifying two pathogenic variants in a patient with pigmented paravenous retinochoroidal atrophy
- Effects of phytoestrogens combined with cold stress on sperm parameters and testicular proteomics in rats
- A case of pulmonary embolism with bad warfarin anticoagulant effects caused by E. coli infection
- Neutrophilia with subclinical Cushing’s disease: A case report and literature review
- Isoimperatorin alleviates lipopolysaccharide-induced periodontitis by downregulating ERK1/2 and NF-κB pathways
- Immunoregulation of synovial macrophages for the treatment of osteoarthritis
- Novel CPLANE1 c.8948dupT (p.P2984Tfs*7) variant in a child patient with Joubert syndrome
- Antiphospholipid antibodies and the risk of thrombosis in myeloproliferative neoplasms
- Immunological responses of septic rats to combination therapy with thymosin α1 and vitamin C
- High glucose and high lipid induced mitochondrial dysfunction in JEG-3 cells through oxidative stress
- Pharmacological inhibition of the ubiquitin-specific protease 8 effectively suppresses glioblastoma cell growth
- Levocarnitine regulates the growth of angiotensin II-induced myocardial fibrosis cells via TIMP-1
- Age-related changes in peripheral T-cell subpopulations in elderly individuals: An observational study
- Single-cell transcription analysis reveals the tumor origin and heterogeneity of human bilateral renal clear cell carcinoma
- Identification of iron metabolism-related genes as diagnostic signatures in sepsis by blood transcriptomic analysis
- Long noncoding RNA ACART knockdown decreases 3T3-L1 preadipocyte proliferation and differentiation
- Surgery, adjuvant immunotherapy plus chemotherapy and radiotherapy for primary malignant melanoma of the parotid gland (PGMM): A case report
- Dosimetry comparison with helical tomotherapy, volumetric modulated arc therapy, and intensity-modulated radiotherapy for grade II gliomas: A single‑institution case series
- Soy isoflavone reduces LPS-induced acute lung injury via increasing aquaporin 1 and aquaporin 5 in rats
- Refractory hypokalemia with sexual dysplasia and infertility caused by 17α-hydroxylase deficiency and triple X syndrome: A case report
- Meta-analysis of cancer risk among end stage renal disease undergoing maintenance dialysis
- 6-Phosphogluconate dehydrogenase inhibition arrests growth and induces apoptosis in gastric cancer via AMPK activation and oxidative stress
- Experimental study on the optimization of ANM33 release in foam cells
- Primary retroperitoneal angiosarcoma: A case report
- Metabolomic analysis-identified 2-hydroxybutyric acid might be a key metabolite of severe preeclampsia
- Malignant pleural effusion diagnosis and therapy
- Effect of spaceflight on the phenotype and proteome of Escherichia coli
- Comparison of immunotherapy combined with stereotactic radiotherapy and targeted therapy for patients with brain metastases: A systemic review and meta-analysis
- Activation of hypermethylated P2RY1 mitigates gastric cancer by promoting apoptosis and inhibiting proliferation
- Association between the VEGFR-2 -604T/C polymorphism (rs2071559) and type 2 diabetic retinopathy
- The role of IL-31 and IL-34 in the diagnosis and treatment of chronic periodontitis
- Triple-negative mouse breast cancer initiating cells show high expression of beta1 integrin and increased malignant features
- mNGS facilitates the accurate diagnosis and antibiotic treatment of suspicious critical CNS infection in real practice: A retrospective study
- The apatinib and pemetrexed combination has antitumor and antiangiogenic effects against NSCLC
- Radiotherapy for primary thyroid adenoid cystic carcinoma
- Design and functional preliminary investigation of recombinant antigen EgG1Y162–EgG1Y162 against Echinococcus granulosus
- Effects of losartan in patients with NAFLD: A meta-analysis of randomized controlled trial
- Bibliometric analysis of METTL3: Current perspectives, highlights, and trending topics
- Performance comparison of three scaling algorithms in NMR-based metabolomics analysis
- PI3K/AKT/mTOR pathway and its related molecules participate in PROK1 silence-induced anti-tumor effects on pancreatic cancer
- The altered expression of cytoskeletal and synaptic remodeling proteins during epilepsy
- Effects of pegylated recombinant human granulocyte colony-stimulating factor on lymphocytes and white blood cells of patients with malignant tumor
- Prostatitis as initial manifestation of Chlamydia psittaci pneumonia diagnosed by metagenome next-generation sequencing: A case report
- NUDT21 relieves sevoflurane-induced neurological damage in rats by down-regulating LIMK2
- Association of interleukin-10 rs1800896, rs1800872, and interleukin-6 rs1800795 polymorphisms with squamous cell carcinoma risk: A meta-analysis
- Exosomal HBV-DNA for diagnosis and treatment monitoring of chronic hepatitis B
- Shear stress leads to the dysfunction of endothelial cells through the Cav-1-mediated KLF2/eNOS/ERK signaling pathway under physiological conditions
- Interaction between the PI3K/AKT pathway and mitochondrial autophagy in macrophages and the leukocyte count in rats with LPS-induced pulmonary infection
- Meta-analysis of the rs231775 locus polymorphism in the CTLA-4 gene and the susceptibility to Graves’ disease in children
- Cloning, subcellular localization and expression of phosphate transporter gene HvPT6 of hulless barley
- Coptisine mitigates diabetic nephropathy via repressing the NRLP3 inflammasome
- Significant elevated CXCL14 and decreased IL-39 levels in patients with tuberculosis
- Whole-exome sequencing applications in prenatal diagnosis of fetal bowel dilatation
- Gemella morbillorum infective endocarditis: A case report and literature review
- An unusual ectopic thymoma clonal evolution analysis: A case report
- Severe cumulative skin toxicity during toripalimab combined with vemurafenib following toripalimab alone
- Detection of V. vulnificus septic shock with ARDS using mNGS
- Novel rare genetic variants of familial and sporadic pulmonary atresia identified by whole-exome sequencing
- The influence and mechanistic action of sperm DNA fragmentation index on the outcomes of assisted reproduction technology
- Novel compound heterozygous mutations in TELO2 in an infant with You-Hoover-Fong syndrome: A case report and literature review
- ctDNA as a prognostic biomarker in resectable CLM: Systematic review and meta-analysis
- Diagnosis of primary amoebic meningoencephalitis by metagenomic next-generation sequencing: A case report
- Phylogenetic analysis of promoter regions of human Dolichol kinase (DOLK) and orthologous genes using bioinformatics tools
- Collagen changes in rabbit conjunctiva after conjunctival crosslinking
- Effects of NM23 transfection of human gastric carcinoma cells in mice
- Oral nifedipine and phytosterol, intravenous nicardipine, and oral nifedipine only: Three-arm, retrospective, cohort study for management of severe preeclampsia
- Case report of hepatic retiform hemangioendothelioma: A rare tumor treated with ultrasound-guided microwave ablation
- Curcumin induces apoptosis in human hepatocellular carcinoma cells by decreasing the expression of STAT3/VEGF/HIF-1α signaling
- Rare presentation of double-clonal Waldenström macroglobulinemia with pulmonary embolism: A case report
- Giant duplication of the transverse colon in an adult: A case report and literature review
- Ectopic thyroid tissue in the breast: A case report
- SDR16C5 promotes proliferation and migration and inhibits apoptosis in pancreatic cancer
- Vaginal metastasis from breast cancer: A case report
- Screening of the best time window for MSC transplantation to treat acute myocardial infarction with SDF-1α antibody-loaded targeted ultrasonic microbubbles: An in vivo study in miniswine
- Inhibition of TAZ impairs the migration ability of melanoma cells
- Molecular complexity analysis of the diagnosis of Gitelman syndrome in China
- Effects of maternal calcium and protein intake on the development and bone metabolism of offspring mice
- Identification of winter wheat pests and diseases based on improved convolutional neural network
- Ultra-multiplex PCR technique to guide treatment of Aspergillus-infected aortic valve prostheses
- Virtual high-throughput screening: Potential inhibitors targeting aminopeptidase N (CD13) and PIKfyve for SARS-CoV-2
- Immune checkpoint inhibitors in cancer patients with COVID-19
- Utility of methylene blue mixed with autologous blood in preoperative localization of pulmonary nodules and masses
- Integrated analysis of the microbiome and transcriptome in stomach adenocarcinoma
- Berberine suppressed sarcopenia insulin resistance through SIRT1-mediated mitophagy
- DUSP2 inhibits the progression of lupus nephritis in mice by regulating the STAT3 pathway
- Lung abscess by Fusobacterium nucleatum and Streptococcus spp. co-infection by mNGS: A case series
- Genetic alterations of KRAS and TP53 in intrahepatic cholangiocarcinoma associated with poor prognosis
- Granulomatous polyangiitis involving the fourth ventricle: Report of a rare case and a literature review
- Studying infant mortality: A demographic analysis based on data mining models
- Metaplastic breast carcinoma with osseous differentiation: A report of a rare case and literature review
- Protein Z modulates the metastasis of lung adenocarcinoma cells
- Inhibition of pyroptosis and apoptosis by capsaicin protects against LPS-induced acute kidney injury through TRPV1/UCP2 axis in vitro
- TAK-242, a toll-like receptor 4 antagonist, against brain injury by alleviates autophagy and inflammation in rats
- Primary mediastinum Ewing’s sarcoma with pleural effusion: A case report and literature review
- Association of ADRB2 gene polymorphisms and intestinal microbiota in Chinese Han adolescents
- Tanshinone IIA alleviates chondrocyte apoptosis and extracellular matrix degeneration by inhibiting ferroptosis
- Study on the cytokines related to SARS-Cov-2 in testicular cells and the interaction network between cells based on scRNA-seq data
- Effect of periostin on bone metabolic and autophagy factors during tooth eruption in mice
- HP1 induces ferroptosis of renal tubular epithelial cells through NRF2 pathway in diabetic nephropathy
- Intravaginal estrogen management in postmenopausal patients with vaginal squamous intraepithelial lesions along with CO2 laser ablation: A retrospective study
- Hepatocellular carcinoma cell differentiation trajectory predicts immunotherapy, potential therapeutic drugs, and prognosis of patients
- Effects of physical exercise on biomarkers of oxidative stress in healthy subjects: A meta-analysis of randomized controlled trials
- Identification of lysosome-related genes in connection with prognosis and immune cell infiltration for drug candidates in head and neck cancer
- Development of an instrument-free and low-cost ELISA dot-blot test to detect antibodies against SARS-CoV-2
- Research progress on gas signal molecular therapy for Parkinson’s disease
- Adiponectin inhibits TGF-β1-induced skin fibroblast proliferation and phenotype transformation via the p38 MAPK signaling pathway
- The G protein-coupled receptor-related gene signatures for predicting prognosis and immunotherapy response in bladder urothelial carcinoma
- α-Fetoprotein contributes to the malignant biological properties of AFP-producing gastric cancer
- CXCL12/CXCR4/CXCR7 axis in placenta tissues of patients with placenta previa
- Association between thyroid stimulating hormone levels and papillary thyroid cancer risk: A meta-analysis
- Significance of sTREM-1 and sST2 combined diagnosis for sepsis detection and prognosis prediction
- Diagnostic value of serum neuroactive substances in the acute exacerbation of chronic obstructive pulmonary disease complicated with depression
- Research progress of AMP-activated protein kinase and cardiac aging
- TRIM29 knockdown prevented the colon cancer progression through decreasing the ubiquitination levels of KRT5
- Cross-talk between gut microbiota and liver steatosis: Complications and therapeutic target
- Metastasis from small cell lung cancer to ovary: A case report
- The early diagnosis and pathogenic mechanisms of sepsis-related acute kidney injury
- The effect of NK cell therapy on sepsis secondary to lung cancer: A case report
- Erianin alleviates collagen-induced arthritis in mice by inhibiting Th17 cell differentiation
- Loss of ACOX1 in clear cell renal cell carcinoma and its correlation with clinical features
- Signalling pathways in the osteogenic differentiation of periodontal ligament stem cells
- Crosstalk between lactic acid and immune regulation and its value in the diagnosis and treatment of liver failure
- Clinicopathological features and differential diagnosis of gastric pleomorphic giant cell carcinoma
- Traumatic brain injury and rTMS-ERPs: Case report and literature review
- Extracellular fibrin promotes non-small cell lung cancer progression through integrin β1/PTEN/AKT signaling
- Knockdown of DLK4 inhibits non-small cell lung cancer tumor growth by downregulating CKS2
- The co-expression pattern of VEGFR-2 with indicators related to proliferation, apoptosis, and differentiation of anagen hair follicles
- Inflammation-related signaling pathways in tendinopathy
- CD4+ T cell count in HIV/TB co-infection and co-occurrence with HL: Case report and literature review
- Clinical analysis of severe Chlamydia psittaci pneumonia: Case series study
- Bioinformatics analysis to identify potential biomarkers for the pulmonary artery hypertension associated with the basement membrane
- Influence of MTHFR polymorphism, alone or in combination with smoking and alcohol consumption, on cancer susceptibility
- Catharanthus roseus (L.) G. Don counteracts the ampicillin resistance in multiple antibiotic-resistant Staphylococcus aureus by downregulation of PBP2a synthesis
- Combination of a bronchogenic cyst in the thoracic spinal canal with chronic myelocytic leukemia
- Bacterial lipoprotein plays an important role in the macrophage autophagy and apoptosis induced by Salmonella typhimurium and Staphylococcus aureus
- TCL1A+ B cells predict prognosis in triple-negative breast cancer through integrative analysis of single-cell and bulk transcriptomic data
- Ezrin promotes esophageal squamous cell carcinoma progression via the Hippo signaling pathway
- Ferroptosis: A potential target of macrophages in plaque vulnerability
- Predicting pediatric Crohn's disease based on six mRNA-constructed risk signature using comprehensive bioinformatic approaches
- Applications of genetic code expansion and photosensitive UAAs in studying membrane proteins
- HK2 contributes to the proliferation, migration, and invasion of diffuse large B-cell lymphoma cells by enhancing the ERK1/2 signaling pathway
- IL-17 in osteoarthritis: A narrative review
- Circadian cycle and neuroinflammation
- Probiotic management and inflammatory factors as a novel treatment in cirrhosis: A systematic review and meta-analysis
- Hemorrhagic meningioma with pulmonary metastasis: Case report and literature review
- SPOP regulates the expression profiles and alternative splicing events in human hepatocytes
- Knockdown of SETD5 inhibited glycolysis and tumor growth in gastric cancer cells by down-regulating Akt signaling pathway
- PTX3 promotes IVIG resistance-induced endothelial injury in Kawasaki disease by regulating the NF-κB pathway
- Pancreatic ectopic thyroid tissue: A case report and analysis of literature
- The prognostic impact of body mass index on female breast cancer patients in underdeveloped regions of northern China differs by menopause status and tumor molecular subtype
- Report on a case of liver-originating malignant melanoma of unknown primary
- Case report: Herbal treatment of neutropenic enterocolitis after chemotherapy for breast cancer
- The fibroblast growth factor–Klotho axis at molecular level
- Characterization of amiodarone action on currents in hERG-T618 gain-of-function mutations
- A case report of diagnosis and dynamic monitoring of Listeria monocytogenes meningitis with NGS
- Effect of autologous platelet-rich plasma on new bone formation and viability of a Marburg bone graft
- Small breast epithelial mucin as a useful prognostic marker for breast cancer patients
- Continuous non-adherent culture promotes transdifferentiation of human adipose-derived stem cells into retinal lineage
- Nrf3 alleviates oxidative stress and promotes the survival of colon cancer cells by activating AKT/BCL-2 signal pathway
- Favorable response to surufatinib in a patient with necrolytic migratory erythema: A case report
- Case report of atypical undernutrition of hypoproteinemia type
- Down-regulation of COL1A1 inhibits tumor-associated fibroblast activation and mediates matrix remodeling in the tumor microenvironment of breast cancer
- Sarcoma protein kinase inhibition alleviates liver fibrosis by promoting hepatic stellate cells ferroptosis
- Research progress of serum eosinophil in chronic obstructive pulmonary disease and asthma
- Clinicopathological characteristics of co-existing or mixed colorectal cancer and neuroendocrine tumor: Report of five cases
- Role of menopausal hormone therapy in the prevention of postmenopausal osteoporosis
- Precisional detection of lymph node metastasis using tFCM in colorectal cancer
- Advances in diagnosis and treatment of perimenopausal syndrome
- A study of forensic genetics: ITO index distribution and kinship judgment between two individuals
- Acute lupus pneumonitis resembling miliary tuberculosis: A case-based review
- Plasma levels of CD36 and glutathione as biomarkers for ruptured intracranial aneurysm
- Fractalkine modulates pulmonary angiogenesis and tube formation by modulating CX3CR1 and growth factors in PVECs
- Novel risk prediction models for deep vein thrombosis after thoracotomy and thoracoscopic lung cancer resections, involving coagulation and immune function
- Exploring the diagnostic markers of essential tremor: A study based on machine learning algorithms
- Evaluation of effects of small-incision approach treatment on proximal tibia fracture by deep learning algorithm-based magnetic resonance imaging
- An online diagnosis method for cancer lesions based on intelligent imaging analysis
- Medical imaging in rheumatoid arthritis: A review on deep learning approach
- Predictive analytics in smart healthcare for child mortality prediction using a machine learning approach
- Utility of neutrophil–lymphocyte ratio and platelet–lymphocyte ratio in predicting acute-on-chronic liver failure survival
- A biomedical decision support system for meta-analysis of bilateral upper-limb training in stroke patients with hemiplegia
- TNF-α and IL-8 levels are positively correlated with hypobaric hypoxic pulmonary hypertension and pulmonary vascular remodeling in rats
- Stochastic gradient descent optimisation for convolutional neural network for medical image segmentation
- Comparison of the prognostic value of four different critical illness scores in patients with sepsis-induced coagulopathy
- Application and teaching of computer molecular simulation embedded technology and artificial intelligence in drug research and development
- Hepatobiliary surgery based on intelligent image segmentation technology
- Value of brain injury-related indicators based on neural network in the diagnosis of neonatal hypoxic-ischemic encephalopathy
- Analysis of early diagnosis methods for asymmetric dementia in brain MR images based on genetic medical technology
- Early diagnosis for the onset of peri-implantitis based on artificial neural network
- Clinical significance of the detection of serum IgG4 and IgG4/IgG ratio in patients with thyroid-associated ophthalmopathy
- Forecast of pain degree of lumbar disc herniation based on back propagation neural network
- SPA-UNet: A liver tumor segmentation network based on fused multi-scale features
- Systematic evaluation of clinical efficacy of CYP1B1 gene polymorphism in EGFR mutant non-small cell lung cancer observed by medical image
- Rehabilitation effect of intelligent rehabilitation training system on hemiplegic limb spasms after stroke
- A novel approach for minimising anti-aliasing effects in EEG data acquisition
- ErbB4 promotes M2 activation of macrophages in idiopathic pulmonary fibrosis
- Clinical role of CYP1B1 gene polymorphism in prediction of postoperative chemotherapy efficacy in NSCLC based on individualized health model
- Lung nodule segmentation via semi-residual multi-resolution neural networks
- Evaluation of brain nerve function in ICU patients with Delirium by deep learning algorithm-based resting state MRI
- A data mining technique for detecting malignant mesothelioma cancer using multiple regression analysis
- Markov model combined with MR diffusion tensor imaging for predicting the onset of Alzheimer’s disease
- Effectiveness of the treatment of depression associated with cancer and neuroimaging changes in depression-related brain regions in patients treated with the mediator-deuterium acupuncture method
- Molecular mechanism of colorectal cancer and screening of molecular markers based on bioinformatics analysis
- Monitoring and evaluation of anesthesia depth status data based on neuroscience
- Exploring the conformational dynamics and thermodynamics of EGFR S768I and G719X + S768I mutations in non-small cell lung cancer: An in silico approaches
- Optimised feature selection-driven convolutional neural network using gray level co-occurrence matrix for detection of cervical cancer
- Incidence of different pressure patterns of spinal cerebellar ataxia and analysis of imaging and genetic diagnosis
- Pathogenic bacteria and treatment resistance in older cardiovascular disease patients with lung infection and risk prediction model
- Adoption value of support vector machine algorithm-based computed tomography imaging in the diagnosis of secondary pulmonary fungal infections in patients with malignant hematological disorders
- From slides to insights: Harnessing deep learning for prognostic survival prediction in human colorectal cancer histology
- Ecology and Environmental Science
- Monitoring of hourly carbon dioxide concentration under different land use types in arid ecosystem
- Comparing the differences of prokaryotic microbial community between pit walls and bottom from Chinese liquor revealed by 16S rRNA gene sequencing
- Effects of cadmium stress on fruits germination and growth of two herbage species
- Bamboo charcoal affects soil properties and bacterial community in tea plantations
- Optimization of biogas potential using kinetic models, response surface methodology, and instrumental evidence for biodegradation of tannery fleshings during anaerobic digestion
- Understory vegetation diversity patterns of Platycladus orientalis and Pinus elliottii communities in Central and Southern China
- Studies on macrofungi diversity and discovery of new species of Abortiporus from Baotianman World Biosphere Reserve
- Food Science
- Effect of berrycactus fruit (Myrtillocactus geometrizans) on glutamate, glutamine, and GABA levels in the frontal cortex of rats fed with a high-fat diet
- Guesstimate of thymoquinone diversity in Nigella sativa L. genotypes and elite varieties collected from Indian states using HPTLC technique
- Analysis of bacterial community structure of Fuzhuan tea with different processing techniques
- Untargeted metabolomics reveals sour jujube kernel benefiting the nutritional value and flavor of Morchella esculenta
- Mycobiota in Slovak wine grapes: A case study from the small Carpathians wine region
- Elemental analysis of Fadogia ancylantha leaves used as a nutraceutical in Mashonaland West Province, Zimbabwe
- Microbiological transglutaminase: Biotechnological application in the food industry
- Influence of solvent-free extraction of fish oil from catfish (Clarias magur) heads using a Taguchi orthogonal array design: A qualitative and quantitative approach
- Chromatographic analysis of the chemical composition and anticancer activities of Curcuma longa extract cultivated in Palestine
- The potential for the use of leghemoglobin and plant ferritin as sources of iron
- Investigating the association between dietary patterns and glycemic control among children and adolescents with T1DM
- Bioengineering and Biotechnology
- Biocompatibility and osteointegration capability of β-TCP manufactured by stereolithography 3D printing: In vitro study
- Clinical characteristics and the prognosis of diabetic foot in Tibet: A single center, retrospective study
- Agriculture
- Biofertilizer and NPSB fertilizer application effects on nodulation and productivity of common bean (Phaseolus vulgaris L.) at Sodo Zuria, Southern Ethiopia
- On correlation between canopy vegetation and growth indexes of maize varieties with different nitrogen efficiencies
- Exopolysaccharides from Pseudomonas tolaasii inhibit the growth of Pleurotus ostreatus mycelia
- A transcriptomic evaluation of the mechanism of programmed cell death of the replaceable bud in Chinese chestnut
- Melatonin enhances salt tolerance in sorghum by modulating photosynthetic performance, osmoregulation, antioxidant defense, and ion homeostasis
- Effects of plant density on alfalfa (Medicago sativa L.) seed yield in western Heilongjiang areas
- Identification of rice leaf diseases and deficiency disorders using a novel DeepBatch technique
- Artificial intelligence and internet of things oriented sustainable precision farming: Towards modern agriculture
- Animal Sciences
- Effect of ketogenic diet on exercise tolerance and transcriptome of gastrocnemius in mice
- Combined analysis of mRNA–miRNA from testis tissue in Tibetan sheep with different FecB genotypes
- Isolation, identification, and drug resistance of a partially isolated bacterium from the gill of Siniperca chuatsi
- Tracking behavioral changes of confined sows from the first mating to the third parity
- The sequencing of the key genes and end products in the TLR4 signaling pathway from the kidney of Rana dybowskii exposed to Aeromonas hydrophila
- Development of a new candidate vaccine against piglet diarrhea caused by Escherichia coli
- Plant Sciences
- Crown and diameter structure of pure Pinus massoniana Lamb. forest in Hunan province, China
- Genetic evaluation and germplasm identification analysis on ITS2, trnL-F, and psbA-trnH of alfalfa varieties germplasm resources
- Tissue culture and rapid propagation technology for Gentiana rhodantha
- Effects of cadmium on the synthesis of active ingredients in Salvia miltiorrhiza
- Cloning and expression analysis of VrNAC13 gene in mung bean
- Chlorate-induced molecular floral transition revealed by transcriptomes
- Effects of warming and drought on growth and development of soybean in Hailun region
- Effects of different light conditions on transient expression and biomass in Nicotiana benthamiana leaves
- Comparative analysis of the rhizosphere microbiome and medicinally active ingredients of Atractylodes lancea from different geographical origins
- Distinguish Dianthus species or varieties based on chloroplast genomes
- Comparative transcriptomes reveal molecular mechanisms of apple blossoms of different tolerance genotypes to chilling injury
- Study on fresh processing key technology and quality influence of Cut Ophiopogonis Radix based on multi-index evaluation
- An advanced approach for fig leaf disease detection and classification: Leveraging image processing and enhanced support vector machine methodology
- Erratum
- Erratum to “Protein Z modulates the metastasis of lung adenocarcinoma cells”
- Erratum to “BRCA1 subcellular localization regulated by PI3K signaling pathway in triple-negative breast cancer MDA-MB-231 cells and hormone-sensitive T47D cells”
- Retraction
- Retraction to “Protocatechuic acid attenuates cerebral aneurysm formation and progression by inhibiting TNF-alpha/Nrf-2/NF-kB-mediated inflammatory mechanisms in experimental rats”