Using of endoscopic polypectomy in patients with diagnosed malignant colorectal polyp – The cross-sectional clinical study
-
Vladislava Stojic
 ,
Tamara Nikolic-Turnic
,
Tamara Nikolic-Turnic

Abstract
The aim of this study was to evaluate the efficacy of endoscopic polypectomy as a therapeutic treatment for malignant alteration of colorectal polyps. In a 5-year research, 89 patients were included, who were tested and treated at the University Clinical Center Kragujevac, Kragujevac, Serbia, with the confirmed presence of malignant alteration polyps of the colon by colonoscopy, which were removed using the method of endoscopic polypectomy and confirmed by the histopathological examination of the entire polyp. After that, the same group of patients was monitored endoscopically within a certain period, controlling polypectomy locations and the occurrence of a possible remnant of the polyp, in the period of up to 2 years of polypectomy. We observed that, with an increasing size of polyps, there is also an increase in the percentage of the complexity of endoscopic resection and the appearance of remnant with histological characteristics of the invasive cancer. The highest percentage of incomplete endoscopic resection and the appearance of remnant with histological characteristics of the invasive cancer were shown at malignant altered polyps in the field of tubulovillous adenoma. Eighteen patients in total underwent the surgical intervention. In conclusion, our data support the high efficacy of endoscopic polypectomy for the removal of the altered malignant polyp.
1 Introduction
The removal of the malignant colon polyps during endoscopy raises a number of concerns, including the risk of the procedure and the possibility of inadequate polypectomy, ptsince these polyps have an increased risk of harboring the invasive carcinoma [1]. Colorectal cancer is most often caused by a malignant alteration in the adenoma (adenoma-carcinoma sequence) which was not promptly detected and removed (Morson theory) [2]. All adenomas have a dysplastic epithelium, which does not always take the polypoid shape and therefore the term adenoma–carcinoma sequence is replaced by the term dysplasia–carcinoma sequence [3]. In a minority of patients, colorectal cancer develops from de novo lesions, which grow from the mucosa [4].
The malignant potential of colorectal adenomas depends on their size, histological type, and degree of dysplasia [5]. Because of the specificity of the colorectal mucosa, unlike malignant tumors in other localizations, the malignant polyp includes intraepithelial and intramucosal carcinoma, as well as tumors, with the penetration of malignant cells into the mucosa muscularis, but not beyond [6]. The malignant polyps, respectively, represent the middle stage of the final one in the process of colorectal carcinogenesis, and the frequency of the malignant polyps is considered to be 9.5% [7]. A high-grade dysplasia (carcinoma in situ) and intramucosal carcinoma which contains intracryptal cell proliferation are considered to be the non-invasive cancer that has the metastatic potential. When the neoplastic tissue lesions exceed this limit, it is referred to as the invasive carcinoma [8,9].
Colorectal cancer screening and endoscopic polyp resection can reduce mortality from colorectal cancer and are now recommended by many national guidelines. Endoscopic polypectomy and endoscopic mucosal resection are the standard treatment options for colorectal neoplasia. Endoscopic submucosal dissection has great potential for the en bloc resection of larger flat or sessile lesions. However, it is technically demanding and time consuming and should be reserved for histologically advanced lesions. Endoscopic full-thickness resection is a welcome addition of endoscopic resection techniques and is very useful for the treatment of smaller difficult-to-resect lesions. The colonoscopic polypectomy technique was first described by Wolff and Shinya [10,11]. The diagnosis is made after the histological examination of entirely removed polyps [12,13,14,15]. The endoscopic polypectomy is much simpler, less expensive, and more comfortable than the surgical one; however, the final decision on the selection of the therapy depends on the shape, size, and histopathologic features of the polyp [8]. Special therapeutic problems are the malignant polyps, because of the increased possibility for the development of residual or metastatic carcinoma, especially if polypectomy was inadequate [16]. If the adenoma with the noninvasive carcinoma is completely removed with the endoscopic method, this procedure is considered curative.
There are two issues after electro-resections of colorectal polyps: whether that is the appropriate therapy for the malignant polyps, and if not, which types of polyps can lead to residues or relapse after electro-resections. That influences the decision concerning the laparotomy and resection of the intestine as a complement to adenoma electro-resections [16]. To avoid the possibility of residual or metastatic carcinoma after the endoscopic polypectomy, the subsequent endoscopy, and biopsy are required to detect possible carcinoma infiltration to the resection border area, the presence of carcinoma, and malignant affection of the lymph and blood vessels. If the malignant tissue infiltrates the border intestinal resection plates, polypectomy is considered inappropriate and the surgical resection should be performed [17].
Minimally invasive surgical techniques have proven to be superior to conventional open techniques in colorectal surgery for short-term outcomes, such as improved postoperative recovery and a reduced postoperative systemic immune response. There are various minimally invasive local excision treatments for malignant polyps, such as trans-anal resection, trans-anal endoscopic microsurgery, and laparoscopic-assisted colectomy as another minimally invasive alternative to open colorectal surgery. However, there are lack of studies that have compared the outcome of transanal minimally invasive surgery (TAMIS) and endoscopic mucosal resection.
Different complication rates between minimally invasive colorectal surgery and endoscopic polypectomy are compared in one of the studies through surgical-related outcomes and postoperative complications. Surgical-related outcomes were operating time (9.49 vs 15.28 min), blood loss (no significant differences), and lesion fragmentation rate (22.6 vs 0%), compared between the endoscopic mucosal resection and TAMIS groups. The establishment of pneumorectum and placement of a single-hole laparoscope prolong the operation time in TAMIS. The secondary outcomes were complications such as hemorrhage (higher rate in the endoscopic mucosal resection group), urinary retention (13.6% in TAMIS vs 1.9% in other groups), and postoperative infection (no significant differences) [18].
Other studies also have shown that endoscopic mucosal resection is simpler, has less morbidity and mortality, is more suitable for the treatment of rectal polyps with a longer distance from the anus, can be performed by a single person with a shorter operating time, and is cost-effective than surgery. It also should be considered the first line of treatment for patients with polyps (≥20 mm) lesions [19,20]. A meta-analysis of 50 studies, including patients with colorectal polyps treated with endoscopic mucosal resection, showed an initial success rate of 92% for endoscopic resection and 8% of patients underwent surgery due to non-curative endoscopic resection. Complications such as endoscopic recurrence, perforation, and bleeding occur in 13.8, 1.5, and 6.5% [21]. Bleeding (in 0.7–24% of the cases) and perforation (risk of 1–2%) are two main complications associated with endoscopic mucosal resection procedure [22]. Other complications include such as non-specific postprocedural pain and post-polypectomy syndrome (1%) [23].
2 Materials and methods
2.1 Ethics approval and consent to participate
The study was conducted at the Clinic of Gastroenterology and Hepatology, the University Clinical Center Kragujevac, Kragujevac, Serbia. All of the patients gave their written and informed consent to participate and the research project was approved by the Ethics Committee of the University Clinical Center Kragujevac and the Faculty of Medical Sciences, the University of Kragujevac, Serbia (n. 01/1627 and 01-311/6, date: March 8, 2010, and January 20, 2010). Additionally, adherence to the Principle of Good Clinical Practice and the Helsinki Declaration were valued throughout the process.
2.2 Consent for publication
All of the patients gave their consent for the publication of their data.
2.3 Design of study and study population
In this cross-sectional study, we investigated the total of 89 patients with the malignant altered polyp (60 male and 29 female patients; 30–89 years of age) who were, during that period of time, tested and treated at the Clinic of Gastroenterology and Hepatology, the University Clinical Center Kragujevac, Kragujevac, Serbia, and in whom colonoscopy confirmed the incidence of malignant alteration of polyps in the colon that was removed by polypectomy including endoscopic mucosal resection and confirmed by the histopathological examination of the entire polyp. The same group of patients was then followed by the endoscopic defined protocol within 2 years after the polypectomy. The study did not include the patients with initially verified existence of the invasive carcinoma through the histopathological examination of endoscopic polypectomy of the entire polyp. Neither did the study include patients diagnosed with the invasive carcinoma, after the initial polypectomy of the malignant polyps in the line of resection. Instead, these patients were sent to the surgeon. The study included patients who, besides the malignant polyps had had synchronous carcinoma at other locations that were surgically removed, and then, the malignant polyp was removed endoscopically.
2.4 Criteria for diagnosing the malignant altered polyp
In this study, the following described criteria were used for the diagnosis of malignant altered polyp, and histologic features that had to be included in the pathology report were emphasized.
Architectural alterations and cytologic abnormalities, principally cellular and nuclear pleomorphism, hyperchromatic cells with multilayered irregular nuclei and loss of mucin, high nuclear/cytoplasmic ratio, marked nuclear atypia with prominent nuclei, and focal cribriform patterns are considered in high-grade dysplasia. Not all these features are necessarily present to the same degree [24].
For the diagnosis of a carcinoma “in situ,” high dysplasia, intramucosal carcinoma or intraepithelial carcinoma, by definition, the main step is identifying changes with the above-mentioned characteristics in the stage at which they are solely confined to the epithelium, lamina propria, or muscularis mucosa and no extending into the submucosa. It is classified as pTis in the AJCC staging system and the National Comprehensive Cancer Network guidelines [25]. These terms were defined as non-invasive high-grade neoplasia in the Vienna classification [26]. Carcinoma in situ or severe dysplasia or intraepithelial carcinoma corresponds to a carcinoma that is restricted to the epithelial layer without invasion into the lamina propria. Intramucosal carcinoma is a carcinoma characterized by the invasion into the lamina propria. When the carcinoma spreads to the submucosa, the polyp is considered to have become malignant, being able to spread to the lymph nodes or distant sites. It is believed that the endoscopic therapy is sufficient for the malignant altered polyps that meet the following criteria (Practice Parameters Committee of the American College of Gastroenterology) [17]: the excision of the entire polyp; a regular finding of mucosa that is more than or equal to 1 mm from the edge of the polyp; well or moderately well-differentiated histology of carcinoma without lymph nodes’ invasion, without invasion of blood vessels, and a negative follow-up colonoscopy 3 months after the polypectomy.
2.5 Endoscopic polypectomy
Colonoscopy and endoscopic polypectomy with endoscopic mucosal resection were performed in the endoscopic cabinet of the Clinic of Gastroenterology and Hepatology, the University Clinical Center Kragujevac, Kragujevac, Serbia, using a colonoscopy device of the brand Olympus EXERA II, while the endoscopic polypectomy was performed with the electrosurgical unit of ERBE brand. The malignant polyps were removed entirely, using the standard method “in a single act” (en bloc resection) or “piece by piece.” The polyps from the colon were drawn along the top of the endoscope with biopic forceps or a polypectomy belt loop.
2.6 Histological analysis of samples
The electro-resected material was distributed and treated at the Department of Pathology of the University Clinical Center Kragujevac, Kragujevac, Serbia. The fixation was carried out in 10% formalin, the tissue was routinely processed, embedded in paraffin, and the classic method of staining with hematoxylin-eosin was applied. The histopathological examination was carried out on the entire polyps/lesions up to 3 cm in size. As for the bigger polyps, they were examined through numerous samples, to the deepest layers and the basal part of the polyp (with pedicle or without it), which corresponds to the insertion location of the polyp. The classical protocol of histopathological reports for polyps and precursor lesions contains the following information: (1) the verification and description of the received material and how representative it is; (2) the histological diagnosis and/or (sub) type of the lesion; (3) the presence and extent of neoplasia (adenoma and/or carcinoma) in samples; (4) the presence of the highest grade dysplasia or grade of histological malignancy; (5) the level of carcinoma invasion, which includes the depth and position of carcinoma; (6) the presence of vascular (lymphoid, venular) invasion; and (7) the residual status of the polypectomy: complete-radical excision of polyps (R 0 category), involvement of the resection margins of a base or a pedicle (R 1 category), indistinct involvement of resection margins (fragmented parts of the polyp), or estimation is not possible for other reasons (R x category) [27].
2.7 Statistical analysis
All statistical analyses were conducted using the software package IBM SPSS Statistics version 22.0 (SPSS, Chicago, IL, USA). Categorical variables were presented in frequencies and percentages. The results were analyzed using Student’s t-test or a Mann–Whitney test on the dependence of normal distribution determined by a Kolmogorov–Smirnov test. For determining the correlation between the categorical variables, the chi-square test was used. The data were expressed as the mean ± standard error. All statistical analyses in this article were conducted with a confidence interval of 95%. The values of p < 0.05 were considered statistically significant.
3 Results
3.1 Socio-epidemiological data
Eighty-nine patients with the malignant polyp, 60 (67.4%) males and 29 (32.6%) females with the mean age of 62.5 ± 10.4 years, were studied. Two-thirds of the patients were male. The age of patients of both sexes was in the variation interval 30–89 years old. The highest frequency of patients for the whole group was in the age group 50–69 with 60.6% of the patients, and the lowest frequency was in the age group 30–49, with 13.5% of the patients. The male patients had the identical age structure as the whole group, while in the female patients, the representation was equal in the age intervals 30–49 and 70–89 years. Malignant polyps affect persons of all ages above 30, with the age frequency that increases and reaches the peak in the age group of 50–69 years. In support of this statement are χ² test values, with frequency schedule 30 (p < 0.05).
3.2 Characteristics of polyps and endoscopic polypectomy
All the patients had one malignant polyp each. The clinicopathological characteristics of the polyps are presented in Table 1. The dominant localization of the malignant polyps is in the sigmoid area, where the tumor was diagnosed in 77.6% of the patients. In the distal colon and rectum, 94.4% of the malignant polyps are localized, and in the right colon 5.6%. The malignant polyps were from 5 mm to over 30 mm in endoscopic size, an average of 19.2 ± 6.46. The most frequent are malignant polyps 10–19 and 20–29 mm in size that were diagnosed in 77.5% of patients – a much higher percentage in relation to the malignant polyps 1–9 and over 30 mm in size. The sigma malignant polyps are, on average, significantly bigger than the malignant polyps of other localizations. The pedunculated altered malignant polyps were 3.4 times more frequent than the polyps of the extensive base. The malignant polyps in the tubulovillous adenoma are statistically significantly more represented in relation to the malignant polyps in the tubular and villous colon adenoma (p < 0.05). Intramucosal depth of invasion of the malignant polyps is 2.3 times more frequent than the intraepithelial depth of invasion (p < 0.05).
Epidemiological data, polyps’ characteristics, and endoscopic polypectomy
| Number of patients | 89 |
|---|---|
| Age (years), mean (s.d.) | 62.5 ± 10.4 |
| Gender, n (%) | |
| Women | 29 (32.6%) |
| Men | 60 (67.4%) |
| Location, n (%) | |
| Rectum | 13 (14.6%) |
| Sigmoid colon | 69 (77.6%) |
| Descending colon | 2 (2.2%) |
| Transverse colon | 2 (2.2%) |
| Ascending colon | 2 (2.2%) |
| Cecum | 1 (1.1%) |
| Size, n (%) | |
| 1–9 mm | 8 (8.9%) |
| 10–19 mm | 38 (42.7%) |
| 20–29 mm | 31 (34.8%) |
| >30 mm | 12 (13.5%) |
| Configurations, n (%) | |
| Pedunculated | 65 (73.1%) |
| Sessile | 22 (24.7%) |
| Flat | 2 (2.2%) |
| Histological characteristics, n (%) | |
| Tubular adenomas | 23 (25.8%) |
| Villous adenomas | 18 (20.2%) |
| Tubulovillous adenomas | 48 (53.9%) |
| Polypectomy, n (%) | |
| Complete resection | 62 (69.7%) |
| Incomplete resection | 27 (30.3%) |
| Technique of polypectomy, n (%) | |
| In one act | 71 (79.8%) |
| Piece by piece | 18 (20.2%) |
| Depth of invasion, n (%) | |
| Intraepithelial | 27 (30.3%) |
| Intramucous | 62 (69.7%) |
| Line of resection, n (%) | |
| Not available | 20 (22.5%) |
| Without dysplasia | 47 (52.7%) |
| Dysplasia grade I | 2 (2.3%) |
| Dysplasia grade II | 3 (3.4%) |
| Dysplasia grade III | 8 (9.0%) |
| Carcinoma in situ | 9 (10.1%) |
| Residual status, n (%) | |
| Radical excision of polyps | 47 (52.8%) |
| Vague involvement of resection margins | 37 (41.6%) |
| Involvement of resection margins | 5 (5.5%) |
At localities of the malignant polyps, polypectomy in 69.7% of patients who had endoscopic controls at prescribed intervals within 2 years, the control colonoscopy did not verify the residual adenomatous tissue, recurrence of polyps, nor nodular growth. In 30.3% of patients, polypectomy was incomplete. In 79.8% of total study patients, polypectomy was performed in one act, and in 52.7% of patients, after polypectomy, the line of resection with no signs of dysplasia and invasion was verified. Radical excision of polyp was diagnosed in 52.8% of patients.
3.3 Histopathological characteristics of the polypectomy localization
In the group of patients with incomplete resection, 11 patients were diagnosed with benign remnant histopathological characteristics, and in 16 patients, the remnant was with malignant histological characteristics. All 11 patients with benign remnant histopathologic features had the endoscopic treatment and had a regular finding at the location of previous polypectomy in endoscopic examinations within 2 years of the follow-up period (Table 2).
Histological characteristics of the polypectomy localization
| Histological characteristics | Percentage (%) | Number |
|---|---|---|
| Tubular adenomas | 22.2 | 6 |
| Villous adenomas | 7.4 | 2 |
| Tubulovillous ademonas | 11.1 | 3 |
| Invasive carcinoma | 29.7 | 8 |
| Carcinoma in situ | 29.6 | 8 |
The lowest percentage of incomplete resection was identified in the malignant polyps 1–9 mm in size. With an increased size of polyps, there is also an increase in percentage of the incomplete resection, so that it is 3.2 times more frequent in a group of the malignant polyps bigger than 30 mm (p < 0.05) (Figure 1a).

Incomplete resection and referral to the surgeon according to the size and configuration of the polyp. (a) With an increase in the size of polyps, there grows also the percentage of the incomplete resection. (b) The highest percentage of referral to the surgeon is in the category of polyps size over 30 mm. (c) Higher percentage of incomplete resection in the sessile configuration of the malignant polyps. (d) Patients with sessile configuration of malignant-altered polyps were referred to the surgeon.
The examination of the number of patients who were referred to the surgeon and those who were not, for each size category of polyps, revealed that the group of polyps larger than 30 mm had the highest percentage of referrals to the surgeon (χ² = 0.036, p < 0.05) (Figure 1b).
A higher percentage of incomplete resection was verified in a sessile configuration of the malignant polyps (p < 0.05) compared to other macro-types (Figure 1c). The patients with sessile configuration of the malignant polyps were 2.8 times more referred to the surgeon, compared to the patients with a peduncle configuration (χ² = 0.008, p < 0.05) (Figure 1d).
In patients with incomplete resection of the malignant polyps, it was 66.7% who had polypectomy in one act and 33.3% who had polypectomy performed in a technique piece by piece. A higher percentage of incomplete resection is seen in a polypectomy technique piece by piece (p < 0.05) (Figure 2a).
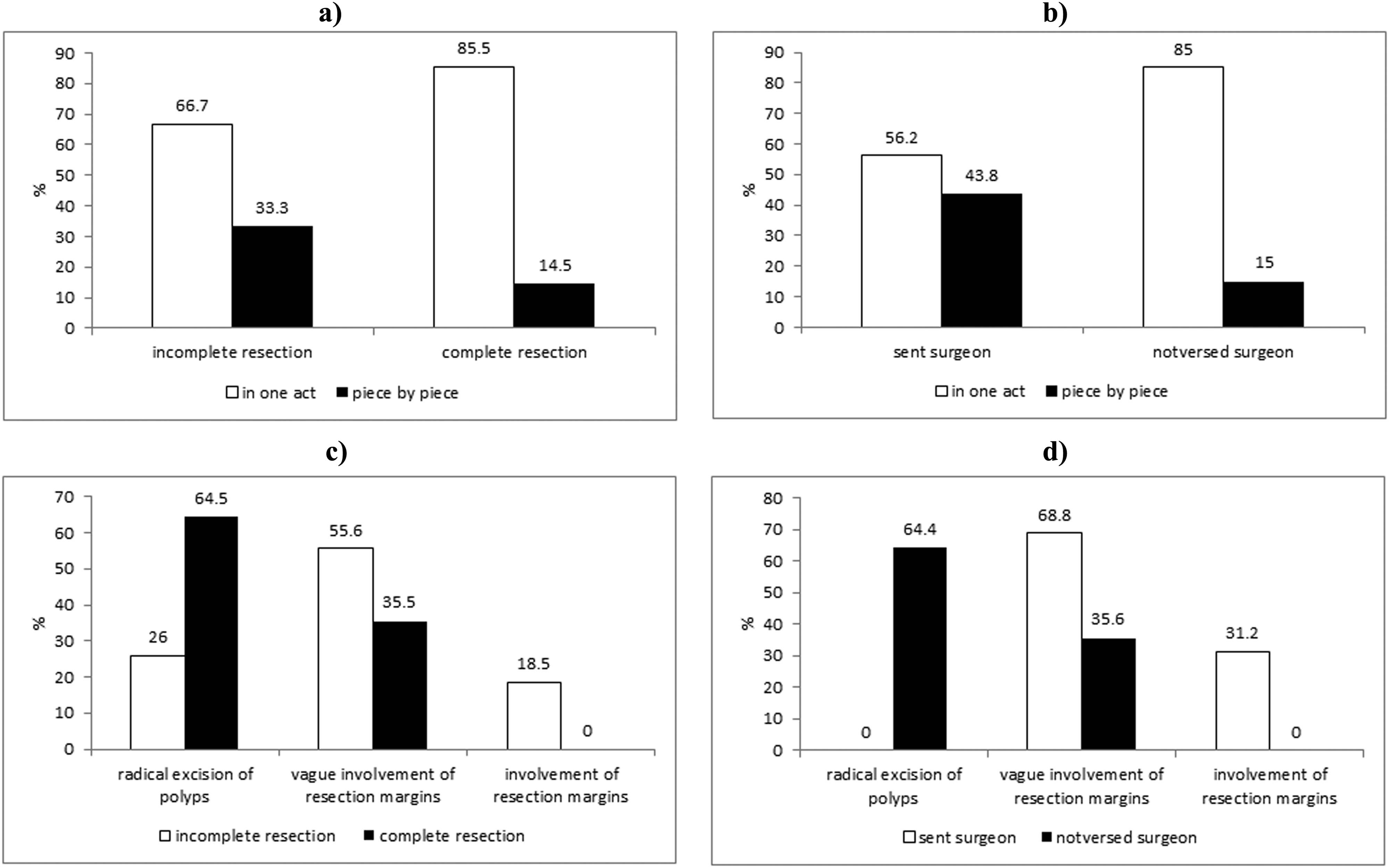
Incomplete resection and referral to the surgeon according to the type of polypectomy and residual polypectomy status. (a) Higher percentage of incomplete resection is in polypectomy technique piece by piece. (b) The percentage of referral to the surgeon is greater in those patients with the malignant polyps, in which resection was performed using technique piece by piece. (c) Verified incomplete polypectomy in 7 patients with the radical excision of polyps, and in 5 patients including involvement of resection margins. (d) Surgeon is not addressed to a single patient with a residual status that showed the radical excision of polyp.
In the group of 16 patients who were referred to the surgeon, 56.2% polypectomy was performed the “in one act” technique and 43.8% the “piece by piece” technique. The percentage of referral to the surgeon is greater in those patients with malignant-altered polyps, in which resection was performed using the “piece by piece” technique (χ² = 0.016, p < 0.05) (Figure 2b).
3.4 Distribution of polypectomy localizations in relation to the histopathological alterations
Analyzing the polypectomy localizations, depending on the histopathological characteristics of the malignant polyps, we got the results that in the group of patients with incomplete resection, most of the malignant polyps were in the area of tubulovillous adenoma, however, without statistical significance (Figure 3a). The surgeon has referred 15 patients with malignant changed tubulovillous adenoma. No patient with malignant changed villous adenoma was identified (χ² = 0.043, p < 0.05) (Figure 3b).
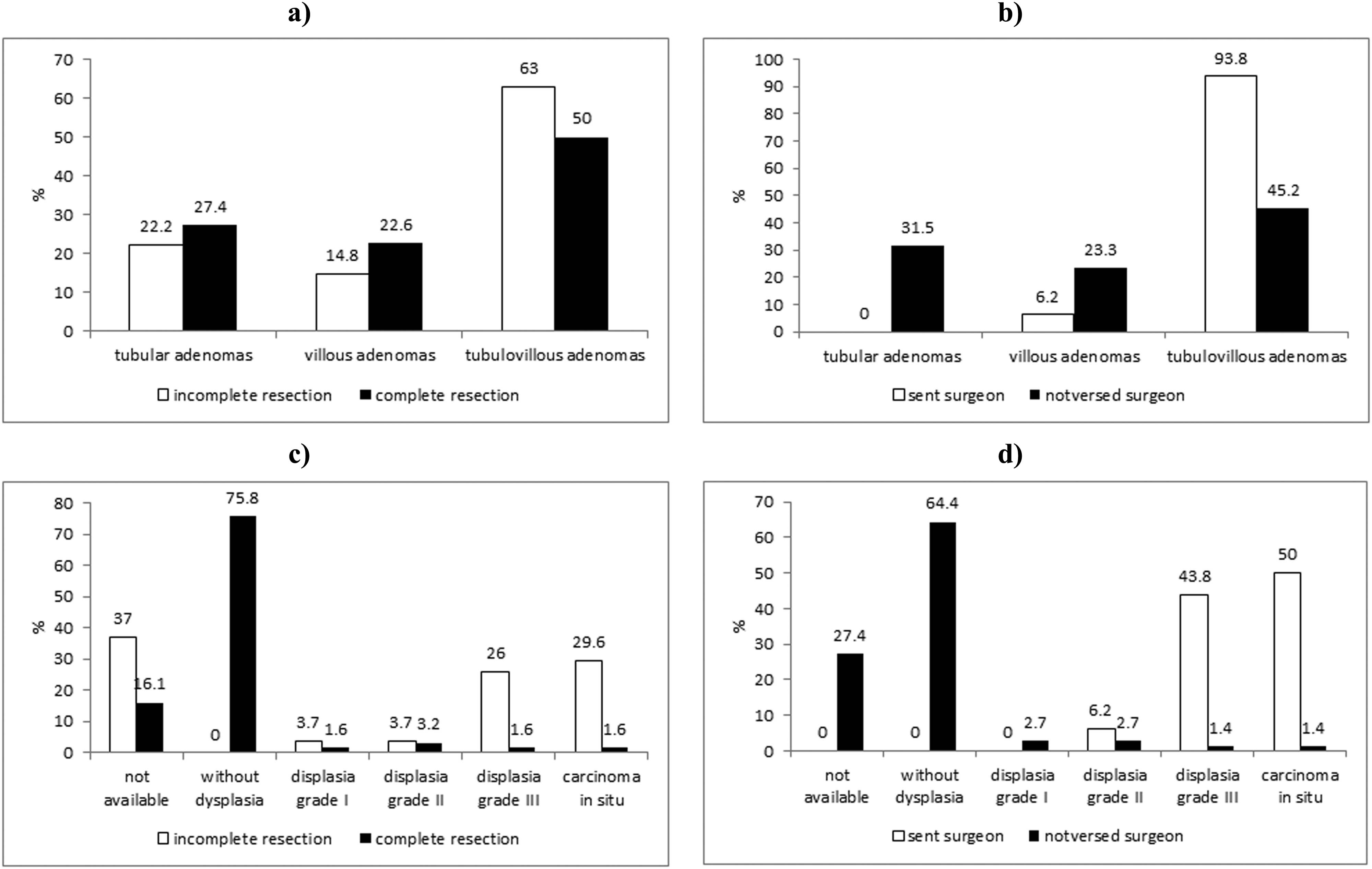
Incomplete resection and referral to the surgeon according to the histopathological characteristics and resection line. (a) Incomplete resection is more common in the tubulovillous malignant polyps. (b) The highest percentage of patients with the malignant-altered tubulovillous polyp was referred to the surgeon. (c) A high percentage of incomplete resection has been verified in resected polyp dysplasia grade III and a focus of carcinoma in situ at the line of resection. (d) With the gradation lines, resection increases the percentage of patients referred to the surgeon.
Incomplete resection was verified at 22.2% of malignant-altered polyps with intraepithelial depth of invasion, and 77.8% with intramucosal depth of invasion. The completeness of resection is independent of the depth of invasion of the malignant-altered polyp which is removed by polypectomy (p > 0.05). The patients referred to the surgeon scaled as 31.3% of patients with intraepithelial depth of invasion of the malignant polyps and 68.7% with intramucosal depth of invasion of the malignant polyps. The percentage of patients referred to the surgeon does not depend on the depth of invasion of malignant-altered polyps (χ² = 0.754, p > 0.05).
3.5 Distribution of malignant polyps with/without resection
All malignant polyps with a resection line with no signs of dysplasia and invasion were fully resected. A high percentage of incomplete resection was verified in resected polyp dysplasia grade III with a focus of carcinoma in situ at the line of resection (Figure 3c). The completeness of resection is dependent on the line of resection (χ² = 0.039, p < 0.05), and odds ratio is 4.928 (each gradation line of resection of increased risk for restoration to about 2 times). With the gradation of the line of resection, the percentage of patients referred to the surgeon increases, so that no patient was referred to the surgeon with the line of resection without signs of dysplasia and the invasion, nor with dysplasia grade I. One patient who was sent to the surgeon had the line of resection of a dysplasia grade II and 7 patients referred to the surgeon had the line of resection grade III dysplasia. Eight patients referred to the surgeon had on the line of resection with the focus of carcinoma in situ (Figure 3d).
The frequency of referring to the surgeon depends on the line of resection (χ² = 0.009, p < 0.05), and the odds ratio is 3.441 (each gradation of the line of resection increases the risk of referring to the surgeon about 3.5×). Incomplete polypectomy was verified in 7 patients with a radical excision of polyps, and in 5 patients including involvement of resection margins (p < 0.05) (Figure 2c). 68.8% of patients with an unclear margin were sent to the surgeon as well as 31.2% of patients with a clear one including involvement of resection (χ² = 0.000, p < 0.05) (Figure 2d). No patient with a residual status showing the radical excision of polyp (χ² = 0.000, p < 0.05) was referred to the surgeon.
3.6 Histopathological features of polypectomy in situ referred to the surgeon
The clinicopathological features of in situ polypectomy referred to the surgeon are presented in Table 3. Eight out of 16 patients who went to the surgeon’s check-up after the endoscopic examination had carcinoma in situ at the polypectomy location, 7 invasive carcinomas, and one of them, dysplasia grade III. The highest percentage of patients with the remnant of invasive cancer had the sigmoid localization of malignant-altered polyps (p = 0.001), over 30 mm in size (p = 0.001), of the sessile configurations (χ² = 0.024, p = 0.001, odds ratio 4.957) at the area of tubulovillous adenoma (p = 0.001). With each gradation of the line of resection, the risk of malignant remnant characteristics increases by 5 times (χ² = 0.010, p < 0.001, odds ratio 5.041). There was no remnant with a malignant histological status, after the radical excision of the malignant-altered polyp; in 45.5% of the patients with unclear invasion of the resection margins, there was rest and histological characteristics of the invasive carcinoma and the same percentage is obtained in the group where invasion of the resection margins was confirmed (χ² = 0.001, p < 0.001).
Clinicopathological features of the polypectomy localization addresed surgeon
| Dysplasia grade III | Carcinoma in situ | Invasive carcinoma | p value | |
|---|---|---|---|---|
| Location, n (%) | ||||
| Rectum | 0 (0.0%) | 3 (75.0%) | 1 (25%) | |
| Sigmoid colon | 1 (9.0%) | 3 (27.2%) | 7 (63.6%) | p = 0.001 |
| Descending colon | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | |
| Transverse colon | 0 (0.0%) | 1 (100.0%) | 0 (0.0%) | |
| Ascending colon | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | |
| Cecum | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | |
| Size, n (%) | ||||
| 1–9 mm | 0 (0.0%) | 1(100.0%) | 0 (0.0%) | |
| 10–19 mm | 1 (16.6%) | 3 (50.0%) | 2 (33.3%) | |
| 20–29 mm | 0 (0.0%) | 3 (75.0%) | 1 (25.0%) | |
| >30 mm | 0 (0.0%) | 1 (20.0%) | 4 (80.0%) | p = 0.005 |
| Configurations, n (%) | ||||
| Pedunculated | 0 (0.0%) | 3 (57.1%) | 3 (42.9%) | |
| Sessile | 1 (12.5%) | 3 (37.5%) | 4 (50.0%) | p = 0.042 |
| Flat | 0 (0.0%) | 1 (100.0%) | 0 (0.0%) | |
| Histological characteristics, n (%) | ||||
| Tubular adenomas | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | |
| Villous adenomas | 1 (100.0%) | 0 (0.0%) | 0 (0.0%) | |
| Tubulovillous adenomas | 0 (0.0%) | 8 (53.3%) | 7 (46.7%) | p = 0.003 |
| Technique of polypectomy, n (%) | ||||
| In one act | 1 (11.1%) | 7 (77.8%) | 1 (11.1%) | |
| Piece by piece | 0 (0.0%) | 1 (14.3%) | 6 (85.7%) | p = 0.023 |
| Depth of invasion, n (%) | ||||
| Intraepithelial | 1 (20.0%) | 3 (60.0%) | 1 (20.0%) | |
| Intramucous | 0 (0.0%) | 5 (45.5%) | 6 (54.5%) | |
| Line of resection, n (%) | ||||
| Not available | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | |
| Dysplasia grade I | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | |
| Dysplasia grade II | 0 (0.0%) | 1 (100.0%) | 0 (0.0%) | |
| Dysplasia grade III | 1 (14.3%) | 2 (28.6%) | 4 (56.1%) | |
| Carcinoma in situ | 0 (0.0%) | 5 (62.5%) | 3 (37.3%) | p = 0.001 |
| Residual status, n (%) | ||||
| Radical excision of polyps | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | |
| Vague involvement of resection margins | 1 (9.1%) | 5 (45.4%) | 5 (45.4%) | |
| Involvement of resection margins | 0 (0.0%) | 3 (60.0%) | 2 (40.0%) | p = 0.003 |
4 Discussion
The progress of the visual techniques [28,29,30] and techniques of polypectomy, which allow detection and removal of polypoid transformations, have resulted in a decrease in the incidence of colorectal carcinoma [31,32,33], which is consistent with the theory of adenoma-carcinoma sequence [34,35]. The precursor lesions for developing the colorectal cancer have been defined, as well as the aberrant crypt focuses [36,37,38]; the genes responsible for colorectal apoptosis have been discovered [39,40,41], as well as the genes responsible for the incidence of familial adenomatous polyposis [42], and hereditary un-polypoid colorectal cancer [43,44,45,46]. Flat adenomas [47,48,49,50] and a flat colorectal carcinoma [30,51], adenomas showing a depressed surface, colorectal carcinoma [52,53] as well as de novo colorectal carcinoma [54] have been described in the literature so far.
However, in spite of those important discoveries and satisfactory doctrine of primary and secondary preventions of colorectal carcinomas, the incidence is increasing. Good prevention of colorectal carcinomas implies timely diagnosis and removal of adenomas. It is necessary to make clinical, endoscopic, histologic, and histochemical analyses to define the optimal plan for further treatment. The removal of the malignant polyps directly prevents cancer development and reduces the incidence of colorectal cancer to 90.0% [55].
Based on the number of colonoscopy examinations, the number of patients who had polypectomy, and the total number of endoscopically removed polyps in our study, the malignant polyps were diagnosed in 12.5% of patients who had polypectomy and represent 8.7% of all polyps removed endoscopically. The literature data show that the malignant polyps are diagnosed in 0.2–9.0% of endoscopically removed adenomatous polyps, and 9.0–11.0% of the surgically treated polyps [51]. The diagnosis of malignant alteration of the adenoma is exclusively histological. Friability, hardness, ulceration, the shape of “Christmas tree,” the asymmetry [52], and to a lesser extent, lobular surface adenoma are macroscopic criteria indicating malignancy. Theoretically, the endoscopic polypectomy is curative; however, in practice, there are some restrictions [53]. Recommendations of some authors have clearly defined that adenomas with carcinoma in situ should be treated only by polypectomy [51,52,53].
In our study, at polypectomy localizations of the malignant polyps in 69.7% of patients, who were endoscopically controlled at prescribed intervals up to 2 years, the control colonoscopy did not verify the residual adenomatous tissue, recurrence of polyps, nor nodular growth. In 30.3% of patients, the control colonoscopy verified relapse. In the group of patients with incomplete resection, 11 patients were diagnosed with residual adenomatous tissue benign pathohistological characteristics and 16 patients had malignant histological characteristics. All 11 patients with benign pathohistological characteristics were resolved endoscopically and they had neat polypectomy sites at control endoscopic examinations in follow-up 2 years later. A high percentage of success of the polypectomy of the malignant polyps with normal endoscopy findings at control colonoscopy examinations is described also by other authors [34,35,36,37,38,39,40].
Also, in our study, the highest frequency of patients for the group as a whole is at the age group 50–69 years. The prevalence of malignant polyps was in a decline after the age of 70, which is explained by the fact that the small number of patients of this age had been examined, due to intolerance to the examination or reduced possibilities of patients of that age to be correctly prepared for colonoscopy. According to Morson and associates [53] the malignant polyps most frequently occur at the age of 60–79 years. The slightly higher average age of the patients was verified in studies by Seitz and associates [55]. The older age is a risk factor, because during aging, there is an accumulation of genetic changes and mutations in the cells. Hakama et al. noted the risk for developing colorectal cancer considering the age and displayed the rate of incidence of 19.2/100,000 in patients older than 65 and 37.1/100,000 in patients older than 65 [54].
We have shown sexual predilection, i.e., a dominant representation of the malignant polyps in male patients. Song et al. [53] showed some higher prevalence of the malignant polyps in females. In some reports, there is an equal representation of both sexes [55]. The explanation for the evident difference between the sexes can be found in the results of controlled experiments. It has been proven that men and women differ in terms of the intestinal transit time, volume of feces, and production of short-chain fatty acids and bile acids [48,51,53].
The malignant polyps in the colon can be found in all of its segments. The dominant localization of the malignant polyp is in the sigmoid area. There is an evident trend of decreasing the prevalence of malignant polyps from distal toward proximal segments. The higher appearance of the malignant polyps distally located is confirmed by other authors [34,41,52,54]. The observed higher incidence of distal parts, verified in our and other studies, explains the earlier manifestation of symptoms in the distal colon compared to the proximal. There are studies, in which the results indicate a trend of increase in the incidence of colorectal carcinoma in the proximal segment of the large intestine, instead of a decrease in the distal parts [41].
There are suggested different genetic mechanisms of cancer appearance in the right and left colon and rectum. It is believed that the increase in the incidence of colorectal carcinoma in the right column is a result of the routine use of colonoscopy [36]. The most common localization of the malignant polyps at the distal part of the colon is in accordance with the predominant prevalence of colorectal cancer in precisely this part of the colon, which is one of the significant confirmations of the theory of adenoma-carcinoma sequence. The altered malignant polyps, regardless of the histological structure, were most rarely represented in the caecoascedent part of the colon. Since malignant polyps may be found in all segments of the colon, colonoscopy is the method of choice for the optimal endoscopic analysis of such tumors.
The most common are malignant polyps 10–29 mm in size. It has been observed that the increasing size of the malignant polyp is followed by the trend of malignant polyp localization in the distal segments of the colon. Many studies [53,55] have revealed an increasing incidence of the malignant polyp size >20 mm. The increase in the size of the adenoma increased the risk for malignancy [31,37,53,56]. Some studies have shown that a K-ras mutation is more frequently represented in larger adenomas [38].
The macroscopic tumor type is an important factor in determining the recurrence and metastatic potential of tumor cells [30]. By analyzing the configuration of the polyp, we have shown the dominance of the peduncular polyps, which are 3.4 times stronger than the polyp of the extensive base. Similar results have been shown in studies by other authors [56,57,58,59].
Significantly more frequent incomplete resection of the polyp was at those sessile configurations and patients with sessile configurations of malignant-altered polyps were 2.8 times more often referred to the surgeon. Similar results were shown by other authors [52]. The sessile macro-morphological configuration of the adenoma facilitates the development of residual and metastatic cancer. In all these cases, surgical intervention is necessary [27]. A polyp with a non-invasive carcinoma becomes an invasive polyp in a time [42] which can be interrupted by a polypectomy [37].
Endoscopic polypectomy and endoscopic mucosal resection were the endoscopic techniques available in our study for the removal of colon polyp. Considering endoscopic mucosal resection as a lower risk of adverse events, relatively simple to perform, and endoscopic submucosal dissection as a more complex, high-risk procedure performed by endoscopists associated with a higher perforation rate.
The most common complication after the endoscopic mucosal resection is bleeding, reported in 0.7–24% of the cases. Intraprocedural bleeding has been reported in 11–22% of cases [60].
The risk factor for intraprocedural bleeding includes large polyps, tubulovillous or villous lesion, and minimally elevated sessile polyps. Previously published articles showed that postprocedural bleeding occurs in 2–11% of cases, however, the rate of clinically significant bleeding is present in only 6% of cases and occurs hours to days after the procedure [61]. The bleeding rate after submucosal endoscopic resection has been reported in 0–11.9% for up to 15 days post-procedure [61]. Meta-analysis of 104 studies showed the rate of immediate and delayed major bleeding after submucosal endoscopic resection for colorectal lesions of 0.75 and 2.1% [62]. Risk factors for delayed bleeding include the lesion’s size, sessile type, the occurrence of intraprocedural bleeding, use of prior anti-thrombotic agents, and lesions in the cecum and rectum with a higher incidence [63].
Perforation is also a potential complication after endoscopic mucosal and submucosal resections. The perforation rate after endoscopic mucosal resection is low, reported as 1–2%.
Perforation is more common following colorectal endoscopic submucosal resection, with reported rate 3.3–10% [64]. Risk factors include using larger diameter snares (≥20 mm), proximal location, bulky lesions, and cutting current. Meta-analysis of 66 studies comparing these two endoscopic procedures for colorectal lesions found higher perforation rate with submucosal compared to mucosal resection [65]. Risk factors for perforations during submucosal resection, besides tumor size and location, include submucosal fibrosis and perforations are more in the ascending colon and cecum due to its thin wall. With reference to 2022 European Society of Gastrointestinal Endoscopy (ESGE) guidelines, submucosal endoscopic resection should be considered for en bloc resection of colorectal (but particularly rectal) lesions with suspicion of limited submucosal invasion (demarcated depressed area with irregular surface pattern or a large protruding or bulky component, particularly if the lesions are larger than 20 mm) or for lesions that otherwise cannot be completely removed by snare-based techniques [66]. Submucosal endoscopic resection showed benefits in the technical, histological, and oncological outcomes as it provides curative treatment without the need for surgery for lesions with a significant likelihood of submucosal invasion. ESD showed benefits in the technical, histological, and oncological outcomes as it provides curative treatment, associated with higher rate of en bloc and complete resection and lower recurrence compared to mucosal resection but, at the cost of increased procedural time, needs for additional surgical operations and perforation risk. [67].
Most of the malignant polyps are removed by polypectomy in one act; however, a higher percentage of incomplete resections was verified using the technique piece by piece. The results of other studies also show a slightly higher percentage of polypectomy technique in one act [43,44,45,46,47,52].
Most of the malignant polyps, as well as the highest percentage of remnant polyps, were in the area of tubulovillous adenoma type. The reports of other studies have shown the highest percentage of the polyp in the field of tubular adenoma, and the highest percentage of malignant alteration is in the field of villous adenoma, wherein the percentage of malignant tubulovillous adenomas is closer to the villous type instead of the tubular adenoma types [52,53,54,55,56,57]. The data from these and other studies are confirmation that the villous adenomas are the rarest histologic type of adenomas of the colon, but with the greatest malignant potential. Despite numerous tests, it cannot be claimed with certainty that the histological structure of villous adenoma is only directly responsible for the increased level of their malignant alteration.
The line of resection on the site of malignant-altered polyps which were removed by polypectomy in patients with complete resection was, in the highest percentage, without dysplasia and invasion. The radical excision of the polyp existed in 52.8% of patients and none of the patients from this group were sent to the surgeon. Five patients were diagnosed with the clear resection margin involvement, and all five patients on the control endoscopy had histological characteristics of remnant carcinoma in situ and invasive carcinoma and all were sent to the surgeon. The recurrent potential of adenoma or adenoma with carcinoma depends on the residual status, hereditary load, age, anatomical location, and histopathological features [56,58].
The group of patients who were referred to the surgeon for further treatment had shown malignant polyps over 30 mm in size and sessile configurations in the field of tubulovillous adenoma with a clear and ambiguous invasion of resection margins. The efficiency of a polypectomy and the rest of sessile polyps are dependent on several factors: the size of the polyp, the resection technique, endoscopist experiences, and histological type [54].
It should be noted that all adenomas grow over time and can change their size and the level of their appeared components. The process of malignant transformation is a lengthy multistep process that, depending on the characteristics of the adenoma, can last for years. In terms of the residual status, it is shown that for R 0 status, there is a high risk of recurrence or alterations and it requires an intensive monitoring within 3, 6, and 12 months. R x and R 1 are the status of a very high risk of recurrence or alteration with an intense monitoring or surgical resection [16]. The presence of neoplasia/cancer in adenoma always gives a long-term risk of adenoma recurrence (20.0–60.0% in the first 2 years) or the occurrence of carcinoma in the colon (5.0% in the next 15 years). The metastatic risk of the malignant polyps is dependent on the existence of submucosal invasion, presence of lymphatic-vascular invasion in 9.7–44.0% of neoplastic lesions, venular invasion in 3.5% malignant polyps, residual tumors at the resection margins, and poor histological differentiation of carcinoma [31,58,59].
Witold and colleagues have tried to define the histopathological criteria that were used to decide the therapeutic treatment of the malignant polyps [59]. The distance of the tumor from the resection margin, which is less than 1 mm of resection and/or grade III and/or lymphatic invasion and/or venous invasion, has been defined as unfavorable histological criteria [59]. The post-polypectomy follow-up period confirmed that the malignant polyp size over 3 cm with the incomplete resection, vascular space invasion, and poor histological differentiation requires the surgical resection [58].
5 Conclusions
Our data support the high efficacy of endoscopic polypectomy for the removal of the malignant polyp. Histology of the varied polyps and polypectomy were an adequate treatment except in cases with an invasive cancer. Most polyps were located in the left colon. The endoscopic polypectomy is effective in the removal of the malignant polyp and, thus, it reduces the risk of developing cancer, as supported by the literature. A regular follow-up program for these patients is mandatory.
Acknowledgments
Not applicable.
-
Funding information: The research was funded by the Faculty of Medical Sciences University of Kragujevac (Junior Project No. 09/10 “Expression of p16, p53, and VEGF, and cytokine profile in malignomas of the colorectal region”).
-
Author contributions: VS, NZ2, and JD performed the statistical analyses of all data, NZ1, JZ, TNT, AM, KJ, and SM designed the study and collected all data. All authors approved the final version of the article.
-
Conflict of interest: The authors declare that there is no conflict of interest regarding the publication of this article.
-
Data availability statement: The datasets generated and/or analyzed during the current study are available at the Department of Internal Medicine, the Faculty of Medical Sciences the University of Kragujevac, Serbia.
References
[1] Moss A, Williams SJ, Hourigan LF, Brown G, Tam W, Singh R, et al. Long-term adenoma recurrence following wide-field endoscopic mucosal resection (WF-EMR) for advanced colonic mucosal neoplasia is infrequent: results and risk factors in 1000 cases from the Australian Colonic EMR (ACE) study. Gut. 2015;64(1):57–65.10.1136/gutjnl-2013-305516Suche in Google Scholar PubMed
[2] Bond JH. Colon polyps and cancer. Endoscopy. 2003;35(1):27–35.10.1055/s-2003-36410Suche in Google Scholar PubMed
[3] Katabathina VS, Menias CO, Khanna L, Murphy L, Dasyam AK, Lubner MG, et al. Hereditary gastrointestinal cancer syndromes: role of imaging in screening, diagnosis, and management. Radiographics. 2019;39(5):1280–301.10.1148/rg.2019180185Suche in Google Scholar PubMed
[4] Papagiorgis PC, Zizi AE, Tseleni S, Oikonomakis IN, Nikiteas NI. Clinicopathological differences of colorectal cancers according to tumor origin: Identification of possibly de novo lesions. Biomed Rep. 2013;1(1):97–104.10.3892/br.2012.17Suche in Google Scholar PubMed PubMed Central
[5] Mandic O, Jovanovic I, Cvetkovic M, Maksimovic J, Radonjic T, Popovic M, et al. Factors Predicting Malignant Occurrence and Polyp Recurrence after the Endoscopic Resection of Large Colorectal Polyps: A Single Center Experience. Medicina. 2022;58(10):1440.10.3390/medicina58101440Suche in Google Scholar PubMed PubMed Central
[6] Comton CC. Colon and rectum. Protocols applies to all carcinomas of the colon and rectum. Carcinoid tumors, lymphomas, sarcomas and tumors of the vermiform appendix are exluded. Arch Path Lab Med. 2000;124:1016–25.10.5858/2000-124-1016-UPFTEOSuche in Google Scholar PubMed
[7] Papadopoulos V, Michalopoulos A, Basdanis G, Papapolychroniadis K, Paramythiotis D, Fotiadis P, et al. Synchronous and metachronous colorectal carcinoma. Tech Coloproctol. 2004;8:97–100.10.1007/s10151-004-0124-ySuche in Google Scholar PubMed
[8] Vucelić B, Hrstić I. Gastroenterologija i hepatologija. Medicinska naklada. 2002;31:872–94.Suche in Google Scholar
[9] Siskova A, Cervena K, Kral J, Hucl T, Vodicka P, Vymetalkova V. Colorectal adenomas—genetics and searching for new molecular screening biomarkers. Int J Mol Sci. 2020;21(9):3260.10.3390/ijms21093260Suche in Google Scholar PubMed PubMed Central
[10] Winawer SJ, Zauber AG. Colonoscopic polypectomy and the incidence of colorectal cancer. Gut. 2001;48(6):753–4.10.1136/gut.48.6.753Suche in Google Scholar PubMed PubMed Central
[11] Ferlitsch M, Moss A, Hassan C, Bhandari P, Dumonceau JM, Paspatis G. Colorectal polypectomy and endoscopic mucosal resection (EMR): European Society of Gastrointestinal Endoscopy (ESGE) clinical guideline. Endoscopy. 2017;49(3):270–97.10.1055/s-0043-102569Suche in Google Scholar PubMed
[12] Trakarnsanga A, Akaraviputh T. Endoscopic tattooing of colorectal lesions: is it a risk-free procedure? World J Gastrointest Endosc. 2011;3(12):256.10.4253/wjge.v3.i12.256Suche in Google Scholar PubMed PubMed Central
[13] Pohl J. Endoscopic tattooing. Video J Encycl GI Endosc. 2013;1(2):355–6.10.1016/S2212-0971(13)70155-9Suche in Google Scholar
[14] Rex DK. The appropriate use and techniques of tattooing in the colon. Gastroenterol Hepatol. 2018;14(5):314.Suche in Google Scholar
[15] Bang CS, Kim YS, Baik GH, Han SH. Colonic abscess induced by India ink tattooing. Korean J Gastroenterol. 2014;64(1):45–8.10.4166/kjg.2014.64.1.45Suche in Google Scholar PubMed
[16] Haumaier F, Sterlacci W, Vieth M. Histological and molecular classification of gastrointestinal polyps. Best Pract Res Clin Gastroenterol. 2017;31(4):369–79.10.1016/j.bpg.2017.06.005Suche in Google Scholar PubMed
[17] Kornbluth A, Sachar DB. Ulcerative colitis practice guidelines in adults (Update), american college of gastroenterology, practice parameters committee. Am J Gastroenterol. 2004;99:1371–85.10.1111/j.1572-0241.2004.40036.xSuche in Google Scholar PubMed
[18] Shen JM, Zhao JY, Ye T, Gong LF, Wang HP, Chen WJ, et al. Transanal minimally invasive surgery vs endoscopic mucosal resection for rectal benign tumors and rectal carcinoids: A retrospective analysis. World J Clin Cases. 2020;8:4311–9.10.12998/wjcc.v8.i19.4311Suche in Google Scholar PubMed PubMed Central
[19] Jayanna M, Burgess NG, Singh R, Hourigan LF, Brown GJ, Zanati SA, et al. Cost analysis of endoscopic mucosal resection vs surgery for large laterally spreading colorectal lesions. Clin Gastroenterol Hepatol. 2016;14:271–8.10.1016/j.cgh.2015.08.037Suche in Google Scholar PubMed
[20] Ahlenstiel G, Hourigan LF, Brown G, Zanati S, Williams SJ, Singh R, et al. Actual endoscopic versus predicted surgical mortality for treatment of advanced mucosal neoplasia of the colon. Gastrointest Endosc. 2014;80:668–76.10.1016/j.gie.2014.04.015Suche in Google Scholar PubMed
[21] Hassan C, Repici A, Sharma P, Correale L, Zullo A, Bretthauer M, et al. Efficacy and safety of endoscopic resection of large colorectal polyps: a systematic review and meta-analysis. Gut. 2016;65:806–20.10.1136/gutjnl-2014-308481Suche in Google Scholar PubMed
[22] Burgess NG, Metz AJ, Williams SJ, Singh R, Tam W, Hourigan LF, et al. Risk factors for intraprocedural and clinically significant delayed bleeding after wide-field endoscopic mucosal resection of large colonic lesions. Clin Gastroenterol Hepatol. 2014;12:651–61.10.1016/j.cgh.2013.09.049Suche in Google Scholar PubMed
[23] Hirasawa K, Sato C, Makazu M, Kaneko H, Kobayashi R, Kokawa A, et al. Coagulation syndrome: delayed perforation after colorectal endoscopic treatments. World J Gastrointest Endosc. 2015;7:1055–61.10.4253/wjge.v7.i12.1055Suche in Google Scholar PubMed PubMed Central
[24] Appelman HD. High-grade dysplasia and villous features should not be part of the routine diagnosis of colorectal adenomas. Am J Gastroenterol. 2008;103:1329–31.10.1111/j.1572-0241.2008.02005_3.xSuche in Google Scholar PubMed
[25] Amin MB, Greene FL, Edge SB, Compton CC, Gershenwald JE, Brookland RK. The Eighth Edition AJCC Cancer Staging Manual: dontinuing to build a bridge from a population-based to a more “personalized” approach to cancer staging. CA Cancer J Clin. 2017;67:93–9.10.3322/caac.21388Suche in Google Scholar PubMed
[26] Shaukat A, Kaltenbach T, Dominitz JA, Robertson DJ, Anderson JC, Cruise M, et al. Endoscopic Recognition and Management Strategies for Malignant Colorectal Polyps: Recommendations of the US Multi-Society Task Force on Colorectal Cancer. Am J Gastroenterol. 2020;115:1751–67.10.14309/ajg.0000000000001013Suche in Google Scholar PubMed
[27] Burt RW. Colon cancer Screening. Gastroenterology. 2000;119:837–53.10.1053/gast.2000.16508Suche in Google Scholar PubMed
[28] Høydahl Ø, Edna TH, Xanthoulis A, Lydersen S, Endreseth BH. Long-term trends in colorectal cancer: incidence, localization, and presentation. BMC Cancer. 2020;20(1):1–3.10.1186/s12885-020-07582-xSuche in Google Scholar PubMed PubMed Central
[29] Wood BJ, Razavi P. Virtual endoscopy: a promising new technology. Am Fam Physician. 2002;66(1):107.Suche in Google Scholar
[30] Zauber AG, Winawer SJ, O’Brien MJ, Lansdorp-Vogelaar I, van Ballegooijen M, Hankey BF, et al. Colonoscopic polypectomy and long-term prevention of colorectal-cancer deaths. N Engl J Med. 2012;366:687–96.10.1056/NEJMoa1100370Suche in Google Scholar PubMed PubMed Central
[31] García-Alfonso P, García-Carbonero R, García-Foncillas J, et al. Update of the recommendations for the determination of biomarkers in colorectal carcinoma: National Consensus of the Spanish Society of Medical Oncology and the Spanish Society of Pathology. Clin Transl Oncol. 2020;1976–91.10.1007/s12094-020-02357-zSuche in Google Scholar PubMed PubMed Central
[32] Lin OS, Kozarek RA, Cha JM. Impact of sigmoidoscopy and colonoscopy on colorectal cancer incidence and mortality: an evidence-based review of published prospective and retrospective studies. Intest Res. 2014;12(4):268.10.5217/ir.2014.12.4.268Suche in Google Scholar PubMed PubMed Central
[33] Deschner BW, Vander Walde NA, Grothey A, Shibata D. Evolution and current status of the multidisciplinary management of locally advanced rectal cancer. J Oncol Pract. 2021;17(7):383–402.10.1200/OP.20.00885Suche in Google Scholar PubMed
[34] Perše M, Cerar A. The role, significance and applicability of aberrant crypt foci in clinical practice. Colorectal cancer-surgery, diagnostics and treatment. InTech; 2014. p. 467–8310.5772/57474Suche in Google Scholar
[35] Clapper ML, Chang WC, Cooper HS. Dysplastic aberrant crypt foci: biomarkers of early colorectal neoplasia and response to preventive intervention. Cancer Prev Res. 2020;13(3):229–40.10.1158/1940-6207.CAPR-19-0316Suche in Google Scholar PubMed PubMed Central
[36] Alrawi SJ, Schiff M, Carroll RE, Dayton M, Gibbs JF, Kulavlat M, et al. Aberrant crypt foci. Anticancer Res. 2006;26(1):107–19.Suche in Google Scholar
[37] Gala M, Sun R, Yang VW. Inhibition of cell transformation by sulindac sulfide is confined to specific oncogenic pathways. Cancer Lett. 2002;175(1):89–94.10.1016/S0304-3835(01)00716-9Suche in Google Scholar PubMed PubMed Central
[38] Watson AJ. Apoptosis and colorectal cancer. Gut. 2004;53(11):1701–9.10.1136/gut.2004.052704Suche in Google Scholar PubMed PubMed Central
[39] Ockner RK. Apoptosis and liver diseases: Recent concepts of mechanism and significance 1. J Gastroenterol Hepatol. 2001;16(3):248–60.10.1046/j.1440-1746.2001.02426.xSuche in Google Scholar PubMed
[40] Plawski A, Banasiewicz T, Borun P, Kubaszewski L, Krokowicz P, Skrzypczak-Zielinska M, et al. Familial adenomatous polyposis of the colon. Hered Cancer ClinPract. 2013;11(1):1–9.10.1186/1897-4287-11-15Suche in Google Scholar PubMed PubMed Central
[41] Trojan J, Zeuzem S, Randolph A, Hemmerle C, Brieger A, Raedle J, et al. Functional analysis of hMLH1 variants and HNPCC-related mutations using a human expression system. Gastroenterology. 2002;122(1):211–9.10.1053/gast.2002.30296Suche in Google Scholar PubMed
[42] Müller A, Fishel R. Mismatch repair and the hereditary non-polyposis colorectal cancer syndrome (HNPCC). Cancer Investig J. 2002;20(1):102–9.10.1081/CNV-120000371Suche in Google Scholar
[43] Scharf F, Silva RM, Morak M, Hastie A, Pickl JM, Sendelbach K, et al. Constitutional chromothripsis of the APC locus as a cause of genetic predisposition to colon cancer. J Med Genet. 2022;59(10):976–83.10.1136/jmedgenet-2021-108147Suche in Google Scholar PubMed PubMed Central
[44] Giraldo A, Gómez A, Salguero G, García H, Aristizábal F, Gutiérrez Ó, et al. MLH1 and MSH2 mutations in Colombian families with hereditary nonpolyposis colorectal cancer (Lynch syndrome)–description of four novel mutations. Fam Cancer. 2005;4(4):285–90.10.1007/s10689-005-4523-7Suche in Google Scholar PubMed
[45] Adachi M, Okinaga K, Muto T. Flat adenoma of the large bowel. Dis Colon Rectum. 2000;43(6):782–7.10.1007/BF02238014Suche in Google Scholar PubMed
[46] Choi WT. Non-conventional dysplastic subtypes in inflammatory bowel disease: a review of their diagnostic characteristics and potential clinical implications. J Pathol Transl Med. 2021;55(2):83–93.10.4132/jptm.2021.02.17Suche in Google Scholar PubMed PubMed Central
[47] Lau PC, Sung JJ. Flat adenoma in colon: two decades of debate. J Dig Dis. 2010;11(4):201–7.10.1111/j.1751-2980.2010.00439.xSuche in Google Scholar PubMed
[48] Saitoh Y, Waxman I, West AB, Popnikolov NK, Gatalica Z, Watari J, et al. Prevalence and distinctive biologic features of flat colorectal adenomas in a North American population. Gastroenterology. 2001;120(7):1657–65.10.1053/gast.2001.24886Suche in Google Scholar PubMed
[49] Rembacken BJ, Fujii T, Cairns A, Dixon MF, Yoshida S, Chalmers DM, et al. Flat and depressed colonic neoplasms, a prospective study of 1000 colonoscopies in the UK. Lancet. 2000;355:1211–4.10.1016/S0140-6736(00)02086-9Suche in Google Scholar
[50] Choi HH, Bae SH, Jang EC, Kim SY, Yeom JO, Lee SY, et al. Intramucosal colon cancer developing in an inverted hyperplastic polyp. Gut and Liver. 2013;7(1):126.10.5009/gnl.2013.7.1.126Suche in Google Scholar PubMed PubMed Central
[51] Ribeiro MS, Wallace MB. Endoscopic treatment of early cancer of the colon. Gastroenterology Hepatology. 2015;11(7):445.Suche in Google Scholar
[52] Lu D, Wang M, Ke X, Wang Q, Wang J, Li D, et al. Association between H. pylori infection and colorectal polyps: A meta-analysis of observational studies. Front Med. 2022;8:2968.10.3389/fmed.2021.706036Suche in Google Scholar PubMed PubMed Central
[53] Song EM, Park B, Ha CA, Hwang SW, Park SH, Yang DH, et al. Endoscopic diagnosis and treatment planning for colorectal polyps using a deep-learning model. Sci Rep. 2020;10(1):30.10.1038/s41598-019-56697-0Suche in Google Scholar PubMed PubMed Central
[54] Hakama M, Hoff G, Kronborg O, Påhlman L. Screening for colorectal cancer. Acta Oncol. 2005;44(5):425–39.10.1080/02841860510029969Suche in Google Scholar PubMed
[55] Seitz U, Bohnacker S, Seewald S, Thonke F, Brand B, Braiutiqam T, et al. Is endoscopic polypectomy an adequate therapy for malignant colorectal adenomas? Presentation of 114 patients and review of the literature. Dis Colon Rectum. 2004;47:1789–96.10.1007/s10350-004-0680-2Suche in Google Scholar PubMed
[56] Fleming M, Ravula S, Tatishchev SF, Wang HL. Colorectal carcinoma: Pathologic aspects. J Gastrointest Oncol. 2012;3(3):153.Suche in Google Scholar
[57] Lonhert MS, Wittmer A, Doniec JM. Endoscopic removal of large colorectal polyps. Zentralbl Chir. 2004;4:291–5.10.1055/s-2004-822832Suche in Google Scholar PubMed
[58] Roldan P, Carro G, Huidobro L, Garcia V, Fernandez S, Esteban DP, et al. Endoscopicresection of largecolorectalpolyps. Rev Esp Enferm Dig. 2004;96:36–47.10.4321/S1130-01082004000100006Suche in Google Scholar PubMed
[59] Witold K, Anna K, Maciej T, Jakub J. Adenomas–Genetic factors in colorectal cancer prevention. Rep Pract Oncol. 2018;23(2):75–83.10.1016/j.rpor.2017.12.003Suche in Google Scholar PubMed PubMed Central
[60] Hwang JH, Konda V, Abu Dayyeh BK, Chauhan SS, Enestvedt BK, Fujii-Lau LL, et al. Endoscopic mucosal resection. Gastrointest Endosc. 2015;82:215–26.10.1016/j.gie.2015.05.001Suche in Google Scholar PubMed
[61] Klein A, Bourke MJ. Advanced polypectomy and resection techniques. Gastrointest Endosc Clin N Am. 2015;25:303–33.10.1016/j.giec.2014.11.005Suche in Google Scholar PubMed
[62] Yamamoto K, Michida T, Nishida T, Hayashi S, Naito M, Ito T. Colorectal endoscopic submucosal dissection: recent technical advances for safe and successful procedures. World J Gastrointest Endosc. 2015;7:1114–28.10.4253/wjge.v7.i14.1114Suche in Google Scholar PubMed PubMed Central
[63] Akintoye E, Kumar N, Aihara H, Nas H, Thompson CC. Colorectal endoscopic submucosal dissection: a systematic review and meta-analysis. Endosc Int Open. 2016;4:1030–44.10.1055/s-0042-114774Suche in Google Scholar PubMed PubMed Central
[64] Okamoto K, Watanabe T, Komeda Y, Kono T, Takashima K, Okamoto A, et al. Risk factors for postoperative bleeding in endoscopic submucosal dissection of colorectal tumors. Oncology. 2017;93(1):35–42.10.1159/000481228Suche in Google Scholar PubMed
[65] Draganov PV, Aihara H, Karasik MS, Ngamruengphong S, Aadam AA, Othman MO, et al. Endoscopic submucosal dissection In North America: a large prospective multicenter study. Gastroenterology. 2021;160:2317–27.10.1053/j.gastro.2021.02.036Suche in Google Scholar PubMed PubMed Central
[66] Fuccio L, Hassan C, Ponchon T, Mandolesi D, Farioli A, Cucchetti A, et al. Clinical outcomes after endoscopic submucosal dissection for colorectal neoplasia: a systematic review and meta-analysis. Gastrointest Endosc. 2017;86:74–86.10.1016/j.gie.2017.02.024Suche in Google Scholar PubMed
[67] Pimentel-Nunes P, Libânio D, Bastiaansen BAJ, Bhandari P, Bisschops R, Bourke JM, et al. Endoscopic submucosal dissection for superficial gastrointestinal lesions: European Society of Gastrointestinal Endoscopy (ESGE) Guideline - Update 2022. Endoscopy. 2022;54(6):591–622.10.1055/a-1811-7025Suche in Google Scholar PubMed
© 2023 the author(s), published by De Gruyter
This work is licensed under the Creative Commons Attribution 4.0 International License.
Artikel in diesem Heft
- Research Articles
- Exosomes derived from mesenchymal stem cells overexpressing miR-210 inhibits neuronal inflammation and contribute to neurite outgrowth through modulating microglia polarization
- Current situation of acute ST-segment elevation myocardial infarction in a county hospital chest pain center during an epidemic of novel coronavirus pneumonia
- circ-IARS depletion inhibits the progression of non-small-cell lung cancer by circ-IARS/miR-1252-5p/HDGF ceRNA pathway
- circRNA ITGA7 restrains growth and enhances radiosensitivity by up-regulating SMAD4 in colorectal carcinoma
- WDR79 promotes aerobic glycolysis of pancreatic ductal adenocarcinoma (PDAC) by the suppression of SIRT4
- Up-regulation of collagen type V alpha 2 (COL5A2) promotes malignant phenotypes in gastric cancer cell via inducing epithelial–mesenchymal transition (EMT)
- Inhibition of TERC inhibits neural apoptosis and inflammation in spinal cord injury through Akt activation and p-38 inhibition via the miR-34a-5p/XBP-1 axis
- 3D-printed polyether-ether-ketone/n-TiO2 composite enhances the cytocompatibility and osteogenic differentiation of MC3T3-E1 cells by downregulating miR-154-5p
- Propofol-mediated circ_0000735 downregulation restrains tumor growth by decreasing integrin-β1 expression in non-small cell lung cancer
- PVT1/miR-16/CCND1 axis regulates gastric cancer progression
- Silencing of circ_002136 sensitizes gastric cancer to paclitaxel by targeting the miR-16-5p/HMGA1 axis
- Short-term outcomes after simultaneous gastrectomy plus cholecystectomy in gastric cancer: A pooling up analysis
- SCARA5 inhibits oral squamous cell carcinoma via inactivating the STAT3 and PI3K/AKT signaling pathways
- Molecular mechanism by which the Notch signaling pathway regulates autophagy in a rat model of pulmonary fibrosis in pigeon breeder’s lung
- lncRNA TPT1-AS1 promotes cell migration and invasion in esophageal squamous-cell carcinomas by regulating the miR-26a/HMGA1 axis
- SIRT1/APE1 promotes the viability of gastric cancer cells by inhibiting p53 to suppress ferroptosis
- Glycoprotein non-metastatic melanoma B interacts with epidermal growth factor receptor to regulate neural stem cell survival and differentiation
- Treatments for brain metastases from EGFR/ALK-negative/unselected NSCLC: A network meta-analysis
- Association of osteoporosis and skeletal muscle loss with serum type I collagen carboxyl-terminal peptide β glypeptide: A cross-sectional study in elder Chinese population
- circ_0000376 knockdown suppresses non-small cell lung cancer cell tumor properties by the miR-545-3p/PDPK1 pathway
- Delivery in a vertical birth chair supported by freedom of movement during labor: A randomized control trial
- UBE2J1 knockdown promotes cell apoptosis in endometrial cancer via regulating PI3K/AKT and MDM2/p53 signaling
- Metabolic resuscitation therapy in critically ill patients with sepsis and septic shock: A pilot prospective randomized controlled trial
- Lycopene ameliorates locomotor activity and urinary frequency induced by pelvic venous congestion in rats
- UHRF1-induced connexin26 methylation is involved in hearing damage triggered by intermittent hypoxia in neonatal rats
- LINC00511 promotes melanoma progression by targeting miR-610/NUCB2
- Ultra-high-performance liquid chromatography-tandem mass spectrometry analysis of serum metabolomic characteristics in people with different vitamin D levels
- Role of Jumonji domain-containing protein D3 and its inhibitor GSK-J4 in Hashimoto’s thyroiditis
- circ_0014736 induces GPR4 to regulate the biological behaviors of human placental trophoblast cells through miR-942-5p in preeclampsia
- Monitoring of sirolimus in the whole blood samples from pediatric patients with lymphatic anomalies
- Effects of osteogenic growth peptide C-terminal pentapeptide and its analogue on bone remodeling in an osteoporosis rat model
- A novel autophagy-related long non-coding RNAs signature predicting progression-free interval and I-131 therapy benefits in papillary thyroid carcinoma
- WGCNA-based identification of potential targets and pathways in response to treatment in locally advanced breast cancer patients
- Radiomics model using preoperative computed tomography angiography images to differentiate new from old emboli of acute lower limb arterial embolism
- Dysregulated lncRNAs are involved in the progress of myocardial infarction by constructing regulatory networks
- Single-arm trial to evaluate the efficacy and safety of baclofen in treatment of intractable hiccup caused by malignant tumor chemotherapy
- Genetic polymorphisms of MRPS30-DT and NINJ2 may influence lung cancer risk
- Efficacy of immune checkpoint inhibitors in patients with KRAS-mutant advanced non-small cell lung cancer: A retrospective analysis
- Pyroptosis-based risk score predicts prognosis and drug sensitivity in lung adenocarcinoma
- Upregulation of lncRNA LANCL1-AS1 inhibits the progression of non-small-cell lung cancer via the miR-3680-3p/GMFG axis
- CircRANBP17 modulated KDM1A to regulate neuroblastoma progression by sponging miR-27b-3p
- Exosomal miR-93-5p regulated the progression of osteoarthritis by targeting ADAMTS9
- Downregulation of RBM17 enhances cisplatin sensitivity and inhibits cell invasion in human hypopharyngeal cancer cells
- HDAC5-mediated PRAME regulates the proliferation, migration, invasion, and EMT of laryngeal squamous cell carcinoma via the PI3K/AKT/mTOR signaling pathway
- The association between sleep duration, quality, and nonalcoholic fatty liver disease: A cross-sectional study
- Myostatin silencing inhibits podocyte apoptosis in membranous nephropathy through Smad3/PKA/NOX4 signaling pathway
- A novel long noncoding RNA AC125257.1 facilitates colorectal cancer progression by targeting miR-133a-3p/CASC5 axis
- Impact of omicron wave and associated control measures in Shanghai on health management and psychosocial well-being of patients with chronic conditions
- Clinicopathological characteristics and prognosis of young patients aged ≤45 years old with non-small cell lung cancer
- TMT-based comprehensive proteomic profiling identifies serum prognostic signatures of acute myeloid leukemia
- The dose limits of teeth protection for patients with nasopharyngeal carcinoma undergoing radiotherapy based on the early oral health-related quality of life
- miR-30b-5p targeting GRIN2A inhibits hippocampal damage in epilepsy
- Long non-coding RNA AL137789.1 promoted malignant biological behaviors and immune escape of pancreatic carcinoma cells
- IRF6 and FGF1 polymorphisms in non-syndromic cleft lip with or without cleft palate in the Polish population
- Comprehensive analysis of the role of SFXN family in breast cancer
- Efficacy of bronchoscopic intratumoral injection of endostar and cisplatin in lung squamous cell carcinoma patients underwent conventional chemoradiotherapy
- Silencing of long noncoding RNA MIAT inhibits the viability and proliferation of breast cancer cells by promoting miR-378a-5p expression
- AG1024, an IGF-1 receptor inhibitor, ameliorates renal injury in rats with diabetic nephropathy via the SOCS/JAK2/STAT pathway
- Downregulation of KIAA1199 alleviated the activation, proliferation, and migration of hepatic stellate cells by the inhibition of epithelial–mesenchymal transition
- Exendin-4 regulates the MAPK and WNT signaling pathways to alleviate the osteogenic inhibition of periodontal ligament stem cells in a high glucose environment
- Inhibition of glycolysis represses the growth and alleviates the endoplasmic reticulum stress of breast cancer cells by regulating TMTC3
- The function of lncRNA EMX2OS/miR-653-5p and its regulatory mechanism in lung adenocarcinoma
- Tectorigenin alleviates the apoptosis and inflammation in spinal cord injury cell model through inhibiting insulin-like growth factor-binding protein 6
- Ultrasound examination supporting CT or MRI in the evaluation of cervical lymphadenopathy in patients with irradiation-treated head and neck cancer
- F-box and WD repeat domain containing 7 inhibits the activation of hepatic stellate cells by degrading delta-like ligand 1 to block Notch signaling pathway
- Knockdown of circ_0005615 enhances the radiosensitivity of colorectal cancer by regulating the miR-665/NOTCH1 axis
- Long noncoding RNA Mhrt alleviates angiotensin II-induced cardiac hypertrophy phenotypes by mediating the miR-765/Wnt family member 7B pathway
- Effect of miR-499-5p/SOX6 axis on atrial fibrosis in rats with atrial fibrillation
- Cholesterol induces inflammation and reduces glucose utilization
- circ_0004904 regulates the trophoblast cell in preeclampsia via miR-19b-3p/ARRDC3 axis
- NECAB3 promotes the migration and invasion of liver cancer cells through HIF-1α/RIT1 signaling pathway
- The poor performance of cardiovascular risk scores in identifying patients with idiopathic inflammatory myopathies at high cardiovascular risk
- miR-2053 inhibits the growth of ovarian cancer cells by downregulating SOX4
- Nucleophosmin 1 associating with engulfment and cell motility protein 1 regulates hepatocellular carcinoma cell chemotaxis and metastasis
- α-Hederin regulates macrophage polarization to relieve sepsis-induced lung and liver injuries in mice
- Changes of microbiota level in urinary tract infections: A meta-analysis
- Identification of key enzalutamide-resistance-related genes in castration-resistant prostate cancer and verification of RAD51 functions
- Falls during oxaliplatin-based chemotherapy for gastrointestinal malignancies – (lessons learned from) a prospective study
- Outcomes of low-risk birth care during the Covid-19 pandemic: A cohort study from a tertiary care center in Lithuania
- Vitamin D protects intestines from liver cirrhosis-induced inflammation and oxidative stress by inhibiting the TLR4/MyD88/NF-κB signaling pathway
- Integrated transcriptome analysis identifies APPL1/RPS6KB2/GALK1 as immune-related metastasis factors in breast cancer
- Genomic analysis of immunogenic cell death-related subtypes for predicting prognosis and immunotherapy outcomes in glioblastoma multiforme
- Circular RNA Circ_0038467 promotes the maturation of miRNA-203 to increase lipopolysaccharide-induced apoptosis of chondrocytes
- An economic evaluation of fine-needle cytology as the primary diagnostic tool in the diagnosis of lymphadenopathy
- Midazolam impedes lung carcinoma cell proliferation and migration via EGFR/MEK/ERK signaling pathway
- Network pharmacology combined with molecular docking and experimental validation to reveal the pharmacological mechanism of naringin against renal fibrosis
- PTPN12 down-regulated by miR-146b-3p gene affects the malignant progression of laryngeal squamous cell carcinoma
- miR-141-3p accelerates ovarian cancer progression and promotes M2-like macrophage polarization by targeting the Keap1-Nrf2 pathway
- lncRNA OIP5-AS1 attenuates the osteoarthritis progression in IL-1β-stimulated chondrocytes
- Overexpression of LINC00607 inhibits cell growth and aggressiveness by regulating the miR-1289/EFNA5 axis in non-small-cell lung cancer
- Subjective well-being in informal caregivers during the COVID-19 pandemic
- Nrf2 protects against myocardial ischemia-reperfusion injury in diabetic rats by inhibiting Drp1-mediated mitochondrial fission
- Unfolded protein response inhibits KAT2B/MLKL-mediated necroptosis of hepatocytes by promoting BMI1 level to ubiquitinate KAT2B
- Bladder cancer screening: The new selection and prediction model
- circNFATC3 facilitated the progression of oral squamous cell carcinoma via the miR-520h/LDHA axis
- Prone position effect in intensive care patients with SARS-COV-2 pneumonia
- Clinical observation on the efficacy of Tongdu Tuina manipulation in the treatment of primary enuresis in children
- Dihydroartemisinin ameliorates cerebral I/R injury in rats via regulating VWF and autophagy-mediated SIRT1/FOXO1 pathway
- Knockdown of circ_0113656 assuages oxidized low-density lipoprotein-induced vascular smooth muscle cell injury through the miR-188-3p/IGF2 pathway
- Low Ang-(1–7) and high des-Arg9 bradykinin serum levels are correlated with cardiovascular risk factors in patients with COVID-19
- Effect of maternal age and body mass index on induction of labor with oral misoprostol for premature rupture of membrane at term: A retrospective cross-sectional study
- Potential protective effects of Huanglian Jiedu Decoction against COVID-19-associated acute kidney injury: A network-based pharmacological and molecular docking study
- Clinical significance of serum MBD3 detection in girls with central precocious puberty
- Clinical features of varicella-zoster virus caused neurological diseases detected by metagenomic next-generation sequencing
- Collagen treatment of complex anorectal fistula: 3 years follow-up
- LncRNA CASC15 inhibition relieves renal fibrosis in diabetic nephropathy through down-regulating SP-A by sponging to miR-424
- Efficacy analysis of empirical bismuth quadruple therapy, high-dose dual therapy, and resistance gene-based triple therapy as a first-line Helicobacter pylori eradication regimen – An open-label, randomized trial
- SMOC2 plays a role in heart failure via regulating TGF-β1/Smad3 pathway-mediated autophagy
- A prospective cohort study of the impact of chronic disease on fall injuries in middle-aged and older adults
- circRNA THBS1 silencing inhibits the malignant biological behavior of cervical cancer cells via the regulation of miR-543/HMGB2 axis
- hsa_circ_0000285 sponging miR-582-3p promotes neuroblastoma progression by regulating the Wnt/β-catenin signaling pathway
- Long non-coding RNA GNAS-AS1 knockdown inhibits proliferation and epithelial–mesenchymal transition of lung adenocarcinoma cells via the microRNA-433-3p/Rab3A axis
- lncRNA UCA1 regulates miR-132/Lrrfip1 axis to promote vascular smooth muscle cell proliferation
- Twenty-four-color full spectrum flow cytometry panel for minimal residual disease detection in acute myeloid leukemia
- Hsa-miR-223-3p participates in the process of anthracycline-induced cardiomyocyte damage by regulating NFIA gene
- Anti-inflammatory effect of ApoE23 on Salmonella typhimurium-induced sepsis in mice
- Analysis of somatic mutations and key driving factors of cervical cancer progression
- Hsa_circ_0028007 regulates the progression of nasopharyngeal carcinoma through the miR-1179/SQLE axis
- Variations in sexual function after laparoendoscopic single-site hysterectomy in women with benign gynecologic diseases
- Effects of pharmacological delay with roxadustat on multi-territory perforator flap survival in rats
- Analysis of heroin effects on calcium channels in rat cardiomyocytes based on transcriptomics and metabolomics
- Risk factors of recurrent bacterial vaginosis among women of reproductive age: A cross-sectional study
- Alkbh5 plays indispensable roles in maintaining self-renewal of hematopoietic stem cells
- Study to compare the effect of casirivimab and imdevimab, remdesivir, and favipiravir on progression and multi-organ function of hospitalized COVID-19 patients
- Correlation between microvessel maturity and ISUP grades assessed using contrast-enhanced transrectal ultrasonography in prostate cancer
- The protective effect of caffeic acid phenethyl ester in the nephrotoxicity induced by α-cypermethrin
- Norepinephrine alleviates cyclosporin A-induced nephrotoxicity by enhancing the expression of SFRP1
- Effect of RUNX1/FOXP3 axis on apoptosis of T and B lymphocytes and immunosuppression in sepsis
- The function of Foxp1 represses β-adrenergic receptor transcription in the occurrence and development of bladder cancer through STAT3 activity
- Risk model and validation of carbapenem-resistant Klebsiella pneumoniae infection in patients with cerebrovascular disease in the ICU
- Calycosin protects against chronic prostatitis in rats via inhibition of the p38MAPK/NF-κB pathway
- Pan-cancer analysis of the PDE4DIP gene with potential prognostic and immunotherapeutic values in multiple cancers including acute myeloid leukemia
- The safety and immunogenicity to inactivated COVID-19 vaccine in patients with hyperlipemia
- Circ-UBR4 regulates the proliferation, migration, inflammation, and apoptosis in ox-LDL-induced vascular smooth muscle cells via miR-515-5p/IGF2 axis
- Clinical characteristics of current COVID-19 rehabilitation outpatients in China
- Luteolin alleviates ulcerative colitis in rats via regulating immune response, oxidative stress, and metabolic profiling
- miR-199a-5p inhibits aortic valve calcification by targeting ATF6 and GRP78 in valve interstitial cells
- The application of iliac fascia space block combined with esketamine intravenous general anesthesia in PFNA surgery of the elderly: A prospective, single-center, controlled trial
- Elevated blood acetoacetate levels reduce major adverse cardiac and cerebrovascular events risk in acute myocardial infarction
- The effects of progesterone on the healing of obstetric anal sphincter damage in female rats
- Identification of cuproptosis-related genes for predicting the development of prostate cancer
- Lumican silencing ameliorates β-glycerophosphate-mediated vascular smooth muscle cell calcification by attenuating the inhibition of APOB on KIF2C activity
- Targeting PTBP1 blocks glutamine metabolism to improve the cisplatin sensitivity of hepatocarcinoma cells through modulating the mRNA stability of glutaminase
- A single center prospective study: Influences of different hip flexion angles on the measurement of lumbar spine bone mineral density by dual energy X-ray absorptiometry
- Clinical analysis of AN69ST membrane continuous venous hemofiltration in the treatment of severe sepsis
- Antibiotics therapy combined with probiotics administered intravaginally for the treatment of bacterial vaginosis: A systematic review and meta-analysis
- Construction of a ceRNA network to reveal a vascular invasion associated prognostic model in hepatocellular carcinoma
- A pan-cancer analysis of STAT3 expression and genetic alterations in human tumors
- A prognostic signature based on seven T-cell-related cell clustering genes in bladder urothelial carcinoma
- Pepsin concentration in oral lavage fluid of rabbit reflux model constructed by dilating the lower esophageal sphincter
- The antihypertensive felodipine shows synergistic activity with immune checkpoint blockade and inhibits tumor growth via NFAT1 in LUSC
- Tanshinone IIA attenuates valvular interstitial cells’ calcification induced by oxidized low density lipoprotein via reducing endoplasmic reticulum stress
- AS-IV enhances the antitumor effects of propofol in NSCLC cells by inhibiting autophagy
- Establishment of two oxaliplatin-resistant gallbladder cancer cell lines and comprehensive analysis of dysregulated genes
- Trial protocol: Feasibility of neuromodulation with connectivity-guided intermittent theta-burst stimulation for improving cognition in multiple sclerosis
- LncRNA LINC00592 mediates the promoter methylation of WIF1 to promote the development of bladder cancer
- Factors associated with gastrointestinal dysmotility in critically ill patients
- Mechanisms by which spinal cord stimulation intervenes in atrial fibrillation: The involvement of the endothelin-1 and nerve growth factor/p75NTR pathways
- Analysis of two-gene signatures and related drugs in small-cell lung cancer by bioinformatics
- Silencing USP19 alleviates cigarette smoke extract-induced mitochondrial dysfunction in BEAS-2B cells by targeting FUNDC1
- Menstrual irregularities associated with COVID-19 vaccines among women in Saudi Arabia: A survey during 2022
- Ferroptosis involves in Schwann cell death in diabetic peripheral neuropathy
- The effect of AQP4 on tau protein aggregation in neurodegeneration and persistent neuroinflammation after cerebral microinfarcts
- Activation of UBEC2 by transcription factor MYBL2 affects DNA damage and promotes gastric cancer progression and cisplatin resistance
- Analysis of clinical characteristics in proximal and distal reflux monitoring among patients with gastroesophageal reflux disease
- Exosomal circ-0020887 and circ-0009590 as novel biomarkers for the diagnosis and prediction of short-term adverse cardiovascular outcomes in STEMI patients
- Upregulated microRNA-429 confers endometrial stromal cell dysfunction by targeting HIF1AN and regulating the HIF1A/VEGF pathway
- Bibliometrics and knowledge map analysis of ultrasound-guided regional anesthesia
- Knockdown of NUPR1 inhibits angiogenesis in lung cancer through IRE1/XBP1 and PERK/eIF2α/ATF4 signaling pathways
- D-dimer trends predict COVID-19 patient’s prognosis: A retrospective chart review study
- WTAP affects intracranial aneurysm progression by regulating m6A methylation modification
- Using of endoscopic polypectomy in patients with diagnosed malignant colorectal polyp – The cross-sectional clinical study
- Anti-S100A4 antibody administration alleviates bronchial epithelial–mesenchymal transition in asthmatic mice
- Prognostic evaluation of system immune-inflammatory index and prognostic nutritional index in double expressor diffuse large B-cell lymphoma
- Prevalence and antibiogram of bacteria causing urinary tract infection among patients with chronic kidney disease
- Reactive oxygen species within the vaginal space: An additional promoter of cervical intraepithelial neoplasia and uterine cervical cancer development?
- Identification of disulfidptosis-related genes and immune infiltration in lower-grade glioma
- A new technique for uterine-preserving pelvic organ prolapse surgery: Laparoscopic rectus abdominis hysteropexy for uterine prolapse by comparing with traditional techniques
- Self-isolation of an Italian long-term care facility during COVID-19 pandemic: A comparison study on care-related infectious episodes
- A comparative study on the overlapping effects of clinically applicable therapeutic interventions in patients with central nervous system damage
- Low intensity extracorporeal shockwave therapy for chronic pelvic pain syndrome: Long-term follow-up
- The diagnostic accuracy of touch imprint cytology for sentinel lymph node metastases of breast cancer: An up-to-date meta-analysis of 4,073 patients
- Mortality associated with Sjögren’s syndrome in the United States in the 1999–2020 period: A multiple cause-of-death study
- CircMMP11 as a prognostic biomarker mediates miR-361-3p/HMGB1 axis to accelerate malignant progression of hepatocellular carcinoma
- Analysis of the clinical characteristics and prognosis of adult de novo acute myeloid leukemia (none APL) with PTPN11 mutations
- KMT2A maintains stemness of gastric cancer cells through regulating Wnt/β-catenin signaling-activated transcriptional factor KLF11
- Evaluation of placental oxygenation by near-infrared spectroscopy in relation to ultrasound maturation grade in physiological term pregnancies
- The role of ultrasonographic findings for PIK3CA-mutated, hormone receptor-positive, human epidermal growth factor receptor-2-negative breast cancer
- Construction of immunogenic cell death-related molecular subtypes and prognostic signature in colorectal cancer
- Long-term prognostic value of high-sensitivity cardiac troponin-I in patients with idiopathic dilated cardiomyopathy
- Establishing a novel Fanconi anemia signaling pathway-associated prognostic model and tumor clustering for pediatric acute myeloid leukemia patients
- Integrative bioinformatics analysis reveals STAT2 as a novel biomarker of inflammation-related cardiac dysfunction in atrial fibrillation
- Adipose-derived stem cells repair radiation-induced chronic lung injury via inhibiting TGF-β1/Smad 3 signaling pathway
- Real-world practice of idiopathic pulmonary fibrosis: Results from a 2000–2016 cohort
- lncRNA LENGA sponges miR-378 to promote myocardial fibrosis in atrial fibrillation
- Diagnostic value of urinary Tamm-Horsfall protein and 24 h urine osmolality for recurrent calcium oxalate stones of the upper urinary tract: Cross-sectional study
- The value of color Doppler ultrasonography combined with serum tumor markers in differential diagnosis of gastric stromal tumor and gastric cancer
- The spike protein of SARS-CoV-2 induces inflammation and EMT of lung epithelial cells and fibroblasts through the upregulation of GADD45A
- Mycophenolate mofetil versus cyclophosphamide plus in patients with connective tissue disease-associated interstitial lung disease: Efficacy and safety analysis
- MiR-1278 targets CALD1 and suppresses the progression of gastric cancer via the MAPK pathway
- Metabolomic analysis of serum short-chain fatty acid concentrations in a mouse of MPTP-induced Parkinson’s disease after dietary supplementation with branched-chain amino acids
- Cimifugin inhibits adipogenesis and TNF-α-induced insulin resistance in 3T3-L1 cells
- Predictors of gastrointestinal complaints in patients on metformin therapy
- Prescribing patterns in patients with chronic obstructive pulmonary disease and atrial fibrillation
- A retrospective analysis of the effect of latent tuberculosis infection on clinical pregnancy outcomes of in vitro fertilization–fresh embryo transferred in infertile women
- Appropriateness and clinical outcomes of short sustained low-efficiency dialysis: A national experience
- miR-29 regulates metabolism by inhibiting JNK-1 expression in non-obese patients with type 2 diabetes mellitus and NAFLD
- Clinical features and management of lymphoepithelial cyst
- Serum VEGF, high-sensitivity CRP, and cystatin-C assist in the diagnosis of type 2 diabetic retinopathy complicated with hyperuricemia
- ENPP1 ameliorates vascular calcification via inhibiting the osteogenic transformation of VSMCs and generating PPi
- Significance of monitoring the levels of thyroid hormone antibodies and glucose and lipid metabolism antibodies in patients suffer from type 2 diabetes
- The causal relationship between immune cells and different kidney diseases: A Mendelian randomization study
- Interleukin 33, soluble suppression of tumorigenicity 2, interleukin 27, and galectin 3 as predictors for outcome in patients admitted to intensive care units
- Identification of diagnostic immune-related gene biomarkers for predicting heart failure after acute myocardial infarction
- Long-term administration of probiotics prevents gastrointestinal mucosal barrier dysfunction in septic mice partly by upregulating the 5-HT degradation pathway
- miR-192 inhibits the activation of hepatic stellate cells by targeting Rictor
- Diagnostic and prognostic value of MR-pro ADM, procalcitonin, and copeptin in sepsis
- Review Articles
- Prenatal diagnosis of fetal defects and its implications on the delivery mode
- Electromagnetic fields exposure on fetal and childhood abnormalities: Systematic review and meta-analysis
- Characteristics of antibiotic resistance mechanisms and genes of Klebsiella pneumoniae
- Saddle pulmonary embolism in the setting of COVID-19 infection: A systematic review of case reports and case series
- Vitamin C and epigenetics: A short physiological overview
- Ebselen: A promising therapy protecting cardiomyocytes from excess iron in iron-overloaded thalassemia patients
- Aspirin versus LMWH for VTE prophylaxis after orthopedic surgery
- Mechanism of rhubarb in the treatment of hyperlipidemia: A recent review
- Surgical management and outcomes of traumatic global brachial plexus injury: A concise review and our center approach
- The progress of autoimmune hepatitis research and future challenges
- METTL16 in human diseases: What should we do next?
- New insights into the prevention of ureteral stents encrustation
- VISTA as a prospective immune checkpoint in gynecological malignant tumors: A review of the literature
- Case Reports
- Mycobacterium xenopi infection of the kidney and lymph nodes: A case report
- Genetic mutation of SLC6A20 (c.1072T > C) in a family with nephrolithiasis: A case report
- Chronic hepatitis B complicated with secondary hemochromatosis was cured clinically: A case report
- Liver abscess complicated with multiple organ invasive infection caused by hematogenous disseminated hypervirulent Klebsiella pneumoniae: A case report
- Urokinase-based lock solutions for catheter salvage: A case of an upcoming kidney transplant recipient
- Two case reports of maturity-onset diabetes of the young type 3 caused by the hepatocyte nuclear factor 1α gene mutation
- Immune checkpoint inhibitor-related pancreatitis: What is known and what is not
- Does total hip arthroplasty result in intercostal nerve injury? A case report and literature review
- Clinicopathological characteristics and diagnosis of hepatic sinusoidal obstruction syndrome caused by Tusanqi – Case report and literature review
- Synchronous triple primary gastrointestinal malignant tumors treated with laparoscopic surgery: A case report
- CT-guided percutaneous microwave ablation combined with bone cement injection for the treatment of transverse metastases: A case report
- Malignant hyperthermia: Report on a successful rescue of a case with the highest temperature of 44.2°C
- Anesthetic management of fetal pulmonary valvuloplasty: A case report
- Rapid Communication
- Impact of COVID-19 lockdown on glycemic levels during pregnancy: A retrospective analysis
- Erratum
- Erratum to “Inhibition of miR-21 improves pulmonary vascular responses in bronchopulmonary dysplasia by targeting the DDAH1/ADMA/NO pathway”
- Erratum to: “Fer exacerbates renal fibrosis and can be targeted by miR-29c-3p”
- Retraction
- Retraction of “Study to compare the effect of casirivimab and imdevimab, remdesivir, and favipiravir on progression and multi-organ function of hospitalized COVID-19 patients”
- Retraction of “circ_0062491 alleviates periodontitis via the miR-142-5p/IGF1 axis”
- Retraction of “miR-223-3p alleviates TGF-β-induced epithelial-mesenchymal transition and extracellular matrix deposition by targeting SP3 in endometrial epithelial cells”
- Retraction of “SLCO4A1-AS1 mediates pancreatic cancer development via miR-4673/KIF21B axis”
- Retraction of “circRNA_0001679/miR-338-3p/DUSP16 axis aggravates acute lung injury”
- Retraction of “lncRNA ACTA2-AS1 inhibits malignant phenotypes of gastric cancer cells”
- Special issue Linking Pathobiological Mechanisms to Clinical Application for cardiovascular diseases
- Effect of cardiac rehabilitation therapy on depressed patients with cardiac insufficiency after cardiac surgery
- Special issue The evolving saga of RNAs from bench to bedside - Part I
- FBLIM1 mRNA is a novel prognostic biomarker and is associated with immune infiltrates in glioma
- Special Issue Computational Intelligence Methodologies Meets Recurrent Cancers - Part III
- Development of a machine learning-based signature utilizing inflammatory response genes for predicting prognosis and immune microenvironment in ovarian cancer
Artikel in diesem Heft
- Research Articles
- Exosomes derived from mesenchymal stem cells overexpressing miR-210 inhibits neuronal inflammation and contribute to neurite outgrowth through modulating microglia polarization
- Current situation of acute ST-segment elevation myocardial infarction in a county hospital chest pain center during an epidemic of novel coronavirus pneumonia
- circ-IARS depletion inhibits the progression of non-small-cell lung cancer by circ-IARS/miR-1252-5p/HDGF ceRNA pathway
- circRNA ITGA7 restrains growth and enhances radiosensitivity by up-regulating SMAD4 in colorectal carcinoma
- WDR79 promotes aerobic glycolysis of pancreatic ductal adenocarcinoma (PDAC) by the suppression of SIRT4
- Up-regulation of collagen type V alpha 2 (COL5A2) promotes malignant phenotypes in gastric cancer cell via inducing epithelial–mesenchymal transition (EMT)
- Inhibition of TERC inhibits neural apoptosis and inflammation in spinal cord injury through Akt activation and p-38 inhibition via the miR-34a-5p/XBP-1 axis
- 3D-printed polyether-ether-ketone/n-TiO2 composite enhances the cytocompatibility and osteogenic differentiation of MC3T3-E1 cells by downregulating miR-154-5p
- Propofol-mediated circ_0000735 downregulation restrains tumor growth by decreasing integrin-β1 expression in non-small cell lung cancer
- PVT1/miR-16/CCND1 axis regulates gastric cancer progression
- Silencing of circ_002136 sensitizes gastric cancer to paclitaxel by targeting the miR-16-5p/HMGA1 axis
- Short-term outcomes after simultaneous gastrectomy plus cholecystectomy in gastric cancer: A pooling up analysis
- SCARA5 inhibits oral squamous cell carcinoma via inactivating the STAT3 and PI3K/AKT signaling pathways
- Molecular mechanism by which the Notch signaling pathway regulates autophagy in a rat model of pulmonary fibrosis in pigeon breeder’s lung
- lncRNA TPT1-AS1 promotes cell migration and invasion in esophageal squamous-cell carcinomas by regulating the miR-26a/HMGA1 axis
- SIRT1/APE1 promotes the viability of gastric cancer cells by inhibiting p53 to suppress ferroptosis
- Glycoprotein non-metastatic melanoma B interacts with epidermal growth factor receptor to regulate neural stem cell survival and differentiation
- Treatments for brain metastases from EGFR/ALK-negative/unselected NSCLC: A network meta-analysis
- Association of osteoporosis and skeletal muscle loss with serum type I collagen carboxyl-terminal peptide β glypeptide: A cross-sectional study in elder Chinese population
- circ_0000376 knockdown suppresses non-small cell lung cancer cell tumor properties by the miR-545-3p/PDPK1 pathway
- Delivery in a vertical birth chair supported by freedom of movement during labor: A randomized control trial
- UBE2J1 knockdown promotes cell apoptosis in endometrial cancer via regulating PI3K/AKT and MDM2/p53 signaling
- Metabolic resuscitation therapy in critically ill patients with sepsis and septic shock: A pilot prospective randomized controlled trial
- Lycopene ameliorates locomotor activity and urinary frequency induced by pelvic venous congestion in rats
- UHRF1-induced connexin26 methylation is involved in hearing damage triggered by intermittent hypoxia in neonatal rats
- LINC00511 promotes melanoma progression by targeting miR-610/NUCB2
- Ultra-high-performance liquid chromatography-tandem mass spectrometry analysis of serum metabolomic characteristics in people with different vitamin D levels
- Role of Jumonji domain-containing protein D3 and its inhibitor GSK-J4 in Hashimoto’s thyroiditis
- circ_0014736 induces GPR4 to regulate the biological behaviors of human placental trophoblast cells through miR-942-5p in preeclampsia
- Monitoring of sirolimus in the whole blood samples from pediatric patients with lymphatic anomalies
- Effects of osteogenic growth peptide C-terminal pentapeptide and its analogue on bone remodeling in an osteoporosis rat model
- A novel autophagy-related long non-coding RNAs signature predicting progression-free interval and I-131 therapy benefits in papillary thyroid carcinoma
- WGCNA-based identification of potential targets and pathways in response to treatment in locally advanced breast cancer patients
- Radiomics model using preoperative computed tomography angiography images to differentiate new from old emboli of acute lower limb arterial embolism
- Dysregulated lncRNAs are involved in the progress of myocardial infarction by constructing regulatory networks
- Single-arm trial to evaluate the efficacy and safety of baclofen in treatment of intractable hiccup caused by malignant tumor chemotherapy
- Genetic polymorphisms of MRPS30-DT and NINJ2 may influence lung cancer risk
- Efficacy of immune checkpoint inhibitors in patients with KRAS-mutant advanced non-small cell lung cancer: A retrospective analysis
- Pyroptosis-based risk score predicts prognosis and drug sensitivity in lung adenocarcinoma
- Upregulation of lncRNA LANCL1-AS1 inhibits the progression of non-small-cell lung cancer via the miR-3680-3p/GMFG axis
- CircRANBP17 modulated KDM1A to regulate neuroblastoma progression by sponging miR-27b-3p
- Exosomal miR-93-5p regulated the progression of osteoarthritis by targeting ADAMTS9
- Downregulation of RBM17 enhances cisplatin sensitivity and inhibits cell invasion in human hypopharyngeal cancer cells
- HDAC5-mediated PRAME regulates the proliferation, migration, invasion, and EMT of laryngeal squamous cell carcinoma via the PI3K/AKT/mTOR signaling pathway
- The association between sleep duration, quality, and nonalcoholic fatty liver disease: A cross-sectional study
- Myostatin silencing inhibits podocyte apoptosis in membranous nephropathy through Smad3/PKA/NOX4 signaling pathway
- A novel long noncoding RNA AC125257.1 facilitates colorectal cancer progression by targeting miR-133a-3p/CASC5 axis
- Impact of omicron wave and associated control measures in Shanghai on health management and psychosocial well-being of patients with chronic conditions
- Clinicopathological characteristics and prognosis of young patients aged ≤45 years old with non-small cell lung cancer
- TMT-based comprehensive proteomic profiling identifies serum prognostic signatures of acute myeloid leukemia
- The dose limits of teeth protection for patients with nasopharyngeal carcinoma undergoing radiotherapy based on the early oral health-related quality of life
- miR-30b-5p targeting GRIN2A inhibits hippocampal damage in epilepsy
- Long non-coding RNA AL137789.1 promoted malignant biological behaviors and immune escape of pancreatic carcinoma cells
- IRF6 and FGF1 polymorphisms in non-syndromic cleft lip with or without cleft palate in the Polish population
- Comprehensive analysis of the role of SFXN family in breast cancer
- Efficacy of bronchoscopic intratumoral injection of endostar and cisplatin in lung squamous cell carcinoma patients underwent conventional chemoradiotherapy
- Silencing of long noncoding RNA MIAT inhibits the viability and proliferation of breast cancer cells by promoting miR-378a-5p expression
- AG1024, an IGF-1 receptor inhibitor, ameliorates renal injury in rats with diabetic nephropathy via the SOCS/JAK2/STAT pathway
- Downregulation of KIAA1199 alleviated the activation, proliferation, and migration of hepatic stellate cells by the inhibition of epithelial–mesenchymal transition
- Exendin-4 regulates the MAPK and WNT signaling pathways to alleviate the osteogenic inhibition of periodontal ligament stem cells in a high glucose environment
- Inhibition of glycolysis represses the growth and alleviates the endoplasmic reticulum stress of breast cancer cells by regulating TMTC3
- The function of lncRNA EMX2OS/miR-653-5p and its regulatory mechanism in lung adenocarcinoma
- Tectorigenin alleviates the apoptosis and inflammation in spinal cord injury cell model through inhibiting insulin-like growth factor-binding protein 6
- Ultrasound examination supporting CT or MRI in the evaluation of cervical lymphadenopathy in patients with irradiation-treated head and neck cancer
- F-box and WD repeat domain containing 7 inhibits the activation of hepatic stellate cells by degrading delta-like ligand 1 to block Notch signaling pathway
- Knockdown of circ_0005615 enhances the radiosensitivity of colorectal cancer by regulating the miR-665/NOTCH1 axis
- Long noncoding RNA Mhrt alleviates angiotensin II-induced cardiac hypertrophy phenotypes by mediating the miR-765/Wnt family member 7B pathway
- Effect of miR-499-5p/SOX6 axis on atrial fibrosis in rats with atrial fibrillation
- Cholesterol induces inflammation and reduces glucose utilization
- circ_0004904 regulates the trophoblast cell in preeclampsia via miR-19b-3p/ARRDC3 axis
- NECAB3 promotes the migration and invasion of liver cancer cells through HIF-1α/RIT1 signaling pathway
- The poor performance of cardiovascular risk scores in identifying patients with idiopathic inflammatory myopathies at high cardiovascular risk
- miR-2053 inhibits the growth of ovarian cancer cells by downregulating SOX4
- Nucleophosmin 1 associating with engulfment and cell motility protein 1 regulates hepatocellular carcinoma cell chemotaxis and metastasis
- α-Hederin regulates macrophage polarization to relieve sepsis-induced lung and liver injuries in mice
- Changes of microbiota level in urinary tract infections: A meta-analysis
- Identification of key enzalutamide-resistance-related genes in castration-resistant prostate cancer and verification of RAD51 functions
- Falls during oxaliplatin-based chemotherapy for gastrointestinal malignancies – (lessons learned from) a prospective study
- Outcomes of low-risk birth care during the Covid-19 pandemic: A cohort study from a tertiary care center in Lithuania
- Vitamin D protects intestines from liver cirrhosis-induced inflammation and oxidative stress by inhibiting the TLR4/MyD88/NF-κB signaling pathway
- Integrated transcriptome analysis identifies APPL1/RPS6KB2/GALK1 as immune-related metastasis factors in breast cancer
- Genomic analysis of immunogenic cell death-related subtypes for predicting prognosis and immunotherapy outcomes in glioblastoma multiforme
- Circular RNA Circ_0038467 promotes the maturation of miRNA-203 to increase lipopolysaccharide-induced apoptosis of chondrocytes
- An economic evaluation of fine-needle cytology as the primary diagnostic tool in the diagnosis of lymphadenopathy
- Midazolam impedes lung carcinoma cell proliferation and migration via EGFR/MEK/ERK signaling pathway
- Network pharmacology combined with molecular docking and experimental validation to reveal the pharmacological mechanism of naringin against renal fibrosis
- PTPN12 down-regulated by miR-146b-3p gene affects the malignant progression of laryngeal squamous cell carcinoma
- miR-141-3p accelerates ovarian cancer progression and promotes M2-like macrophage polarization by targeting the Keap1-Nrf2 pathway
- lncRNA OIP5-AS1 attenuates the osteoarthritis progression in IL-1β-stimulated chondrocytes
- Overexpression of LINC00607 inhibits cell growth and aggressiveness by regulating the miR-1289/EFNA5 axis in non-small-cell lung cancer
- Subjective well-being in informal caregivers during the COVID-19 pandemic
- Nrf2 protects against myocardial ischemia-reperfusion injury in diabetic rats by inhibiting Drp1-mediated mitochondrial fission
- Unfolded protein response inhibits KAT2B/MLKL-mediated necroptosis of hepatocytes by promoting BMI1 level to ubiquitinate KAT2B
- Bladder cancer screening: The new selection and prediction model
- circNFATC3 facilitated the progression of oral squamous cell carcinoma via the miR-520h/LDHA axis
- Prone position effect in intensive care patients with SARS-COV-2 pneumonia
- Clinical observation on the efficacy of Tongdu Tuina manipulation in the treatment of primary enuresis in children
- Dihydroartemisinin ameliorates cerebral I/R injury in rats via regulating VWF and autophagy-mediated SIRT1/FOXO1 pathway
- Knockdown of circ_0113656 assuages oxidized low-density lipoprotein-induced vascular smooth muscle cell injury through the miR-188-3p/IGF2 pathway
- Low Ang-(1–7) and high des-Arg9 bradykinin serum levels are correlated with cardiovascular risk factors in patients with COVID-19
- Effect of maternal age and body mass index on induction of labor with oral misoprostol for premature rupture of membrane at term: A retrospective cross-sectional study
- Potential protective effects of Huanglian Jiedu Decoction against COVID-19-associated acute kidney injury: A network-based pharmacological and molecular docking study
- Clinical significance of serum MBD3 detection in girls with central precocious puberty
- Clinical features of varicella-zoster virus caused neurological diseases detected by metagenomic next-generation sequencing
- Collagen treatment of complex anorectal fistula: 3 years follow-up
- LncRNA CASC15 inhibition relieves renal fibrosis in diabetic nephropathy through down-regulating SP-A by sponging to miR-424
- Efficacy analysis of empirical bismuth quadruple therapy, high-dose dual therapy, and resistance gene-based triple therapy as a first-line Helicobacter pylori eradication regimen – An open-label, randomized trial
- SMOC2 plays a role in heart failure via regulating TGF-β1/Smad3 pathway-mediated autophagy
- A prospective cohort study of the impact of chronic disease on fall injuries in middle-aged and older adults
- circRNA THBS1 silencing inhibits the malignant biological behavior of cervical cancer cells via the regulation of miR-543/HMGB2 axis
- hsa_circ_0000285 sponging miR-582-3p promotes neuroblastoma progression by regulating the Wnt/β-catenin signaling pathway
- Long non-coding RNA GNAS-AS1 knockdown inhibits proliferation and epithelial–mesenchymal transition of lung adenocarcinoma cells via the microRNA-433-3p/Rab3A axis
- lncRNA UCA1 regulates miR-132/Lrrfip1 axis to promote vascular smooth muscle cell proliferation
- Twenty-four-color full spectrum flow cytometry panel for minimal residual disease detection in acute myeloid leukemia
- Hsa-miR-223-3p participates in the process of anthracycline-induced cardiomyocyte damage by regulating NFIA gene
- Anti-inflammatory effect of ApoE23 on Salmonella typhimurium-induced sepsis in mice
- Analysis of somatic mutations and key driving factors of cervical cancer progression
- Hsa_circ_0028007 regulates the progression of nasopharyngeal carcinoma through the miR-1179/SQLE axis
- Variations in sexual function after laparoendoscopic single-site hysterectomy in women with benign gynecologic diseases
- Effects of pharmacological delay with roxadustat on multi-territory perforator flap survival in rats
- Analysis of heroin effects on calcium channels in rat cardiomyocytes based on transcriptomics and metabolomics
- Risk factors of recurrent bacterial vaginosis among women of reproductive age: A cross-sectional study
- Alkbh5 plays indispensable roles in maintaining self-renewal of hematopoietic stem cells
- Study to compare the effect of casirivimab and imdevimab, remdesivir, and favipiravir on progression and multi-organ function of hospitalized COVID-19 patients
- Correlation between microvessel maturity and ISUP grades assessed using contrast-enhanced transrectal ultrasonography in prostate cancer
- The protective effect of caffeic acid phenethyl ester in the nephrotoxicity induced by α-cypermethrin
- Norepinephrine alleviates cyclosporin A-induced nephrotoxicity by enhancing the expression of SFRP1
- Effect of RUNX1/FOXP3 axis on apoptosis of T and B lymphocytes and immunosuppression in sepsis
- The function of Foxp1 represses β-adrenergic receptor transcription in the occurrence and development of bladder cancer through STAT3 activity
- Risk model and validation of carbapenem-resistant Klebsiella pneumoniae infection in patients with cerebrovascular disease in the ICU
- Calycosin protects against chronic prostatitis in rats via inhibition of the p38MAPK/NF-κB pathway
- Pan-cancer analysis of the PDE4DIP gene with potential prognostic and immunotherapeutic values in multiple cancers including acute myeloid leukemia
- The safety and immunogenicity to inactivated COVID-19 vaccine in patients with hyperlipemia
- Circ-UBR4 regulates the proliferation, migration, inflammation, and apoptosis in ox-LDL-induced vascular smooth muscle cells via miR-515-5p/IGF2 axis
- Clinical characteristics of current COVID-19 rehabilitation outpatients in China
- Luteolin alleviates ulcerative colitis in rats via regulating immune response, oxidative stress, and metabolic profiling
- miR-199a-5p inhibits aortic valve calcification by targeting ATF6 and GRP78 in valve interstitial cells
- The application of iliac fascia space block combined with esketamine intravenous general anesthesia in PFNA surgery of the elderly: A prospective, single-center, controlled trial
- Elevated blood acetoacetate levels reduce major adverse cardiac and cerebrovascular events risk in acute myocardial infarction
- The effects of progesterone on the healing of obstetric anal sphincter damage in female rats
- Identification of cuproptosis-related genes for predicting the development of prostate cancer
- Lumican silencing ameliorates β-glycerophosphate-mediated vascular smooth muscle cell calcification by attenuating the inhibition of APOB on KIF2C activity
- Targeting PTBP1 blocks glutamine metabolism to improve the cisplatin sensitivity of hepatocarcinoma cells through modulating the mRNA stability of glutaminase
- A single center prospective study: Influences of different hip flexion angles on the measurement of lumbar spine bone mineral density by dual energy X-ray absorptiometry
- Clinical analysis of AN69ST membrane continuous venous hemofiltration in the treatment of severe sepsis
- Antibiotics therapy combined with probiotics administered intravaginally for the treatment of bacterial vaginosis: A systematic review and meta-analysis
- Construction of a ceRNA network to reveal a vascular invasion associated prognostic model in hepatocellular carcinoma
- A pan-cancer analysis of STAT3 expression and genetic alterations in human tumors
- A prognostic signature based on seven T-cell-related cell clustering genes in bladder urothelial carcinoma
- Pepsin concentration in oral lavage fluid of rabbit reflux model constructed by dilating the lower esophageal sphincter
- The antihypertensive felodipine shows synergistic activity with immune checkpoint blockade and inhibits tumor growth via NFAT1 in LUSC
- Tanshinone IIA attenuates valvular interstitial cells’ calcification induced by oxidized low density lipoprotein via reducing endoplasmic reticulum stress
- AS-IV enhances the antitumor effects of propofol in NSCLC cells by inhibiting autophagy
- Establishment of two oxaliplatin-resistant gallbladder cancer cell lines and comprehensive analysis of dysregulated genes
- Trial protocol: Feasibility of neuromodulation with connectivity-guided intermittent theta-burst stimulation for improving cognition in multiple sclerosis
- LncRNA LINC00592 mediates the promoter methylation of WIF1 to promote the development of bladder cancer
- Factors associated with gastrointestinal dysmotility in critically ill patients
- Mechanisms by which spinal cord stimulation intervenes in atrial fibrillation: The involvement of the endothelin-1 and nerve growth factor/p75NTR pathways
- Analysis of two-gene signatures and related drugs in small-cell lung cancer by bioinformatics
- Silencing USP19 alleviates cigarette smoke extract-induced mitochondrial dysfunction in BEAS-2B cells by targeting FUNDC1
- Menstrual irregularities associated with COVID-19 vaccines among women in Saudi Arabia: A survey during 2022
- Ferroptosis involves in Schwann cell death in diabetic peripheral neuropathy
- The effect of AQP4 on tau protein aggregation in neurodegeneration and persistent neuroinflammation after cerebral microinfarcts
- Activation of UBEC2 by transcription factor MYBL2 affects DNA damage and promotes gastric cancer progression and cisplatin resistance
- Analysis of clinical characteristics in proximal and distal reflux monitoring among patients with gastroesophageal reflux disease
- Exosomal circ-0020887 and circ-0009590 as novel biomarkers for the diagnosis and prediction of short-term adverse cardiovascular outcomes in STEMI patients
- Upregulated microRNA-429 confers endometrial stromal cell dysfunction by targeting HIF1AN and regulating the HIF1A/VEGF pathway
- Bibliometrics and knowledge map analysis of ultrasound-guided regional anesthesia
- Knockdown of NUPR1 inhibits angiogenesis in lung cancer through IRE1/XBP1 and PERK/eIF2α/ATF4 signaling pathways
- D-dimer trends predict COVID-19 patient’s prognosis: A retrospective chart review study
- WTAP affects intracranial aneurysm progression by regulating m6A methylation modification
- Using of endoscopic polypectomy in patients with diagnosed malignant colorectal polyp – The cross-sectional clinical study
- Anti-S100A4 antibody administration alleviates bronchial epithelial–mesenchymal transition in asthmatic mice
- Prognostic evaluation of system immune-inflammatory index and prognostic nutritional index in double expressor diffuse large B-cell lymphoma
- Prevalence and antibiogram of bacteria causing urinary tract infection among patients with chronic kidney disease
- Reactive oxygen species within the vaginal space: An additional promoter of cervical intraepithelial neoplasia and uterine cervical cancer development?
- Identification of disulfidptosis-related genes and immune infiltration in lower-grade glioma
- A new technique for uterine-preserving pelvic organ prolapse surgery: Laparoscopic rectus abdominis hysteropexy for uterine prolapse by comparing with traditional techniques
- Self-isolation of an Italian long-term care facility during COVID-19 pandemic: A comparison study on care-related infectious episodes
- A comparative study on the overlapping effects of clinically applicable therapeutic interventions in patients with central nervous system damage
- Low intensity extracorporeal shockwave therapy for chronic pelvic pain syndrome: Long-term follow-up
- The diagnostic accuracy of touch imprint cytology for sentinel lymph node metastases of breast cancer: An up-to-date meta-analysis of 4,073 patients
- Mortality associated with Sjögren’s syndrome in the United States in the 1999–2020 period: A multiple cause-of-death study
- CircMMP11 as a prognostic biomarker mediates miR-361-3p/HMGB1 axis to accelerate malignant progression of hepatocellular carcinoma
- Analysis of the clinical characteristics and prognosis of adult de novo acute myeloid leukemia (none APL) with PTPN11 mutations
- KMT2A maintains stemness of gastric cancer cells through regulating Wnt/β-catenin signaling-activated transcriptional factor KLF11
- Evaluation of placental oxygenation by near-infrared spectroscopy in relation to ultrasound maturation grade in physiological term pregnancies
- The role of ultrasonographic findings for PIK3CA-mutated, hormone receptor-positive, human epidermal growth factor receptor-2-negative breast cancer
- Construction of immunogenic cell death-related molecular subtypes and prognostic signature in colorectal cancer
- Long-term prognostic value of high-sensitivity cardiac troponin-I in patients with idiopathic dilated cardiomyopathy
- Establishing a novel Fanconi anemia signaling pathway-associated prognostic model and tumor clustering for pediatric acute myeloid leukemia patients
- Integrative bioinformatics analysis reveals STAT2 as a novel biomarker of inflammation-related cardiac dysfunction in atrial fibrillation
- Adipose-derived stem cells repair radiation-induced chronic lung injury via inhibiting TGF-β1/Smad 3 signaling pathway
- Real-world practice of idiopathic pulmonary fibrosis: Results from a 2000–2016 cohort
- lncRNA LENGA sponges miR-378 to promote myocardial fibrosis in atrial fibrillation
- Diagnostic value of urinary Tamm-Horsfall protein and 24 h urine osmolality for recurrent calcium oxalate stones of the upper urinary tract: Cross-sectional study
- The value of color Doppler ultrasonography combined with serum tumor markers in differential diagnosis of gastric stromal tumor and gastric cancer
- The spike protein of SARS-CoV-2 induces inflammation and EMT of lung epithelial cells and fibroblasts through the upregulation of GADD45A
- Mycophenolate mofetil versus cyclophosphamide plus in patients with connective tissue disease-associated interstitial lung disease: Efficacy and safety analysis
- MiR-1278 targets CALD1 and suppresses the progression of gastric cancer via the MAPK pathway
- Metabolomic analysis of serum short-chain fatty acid concentrations in a mouse of MPTP-induced Parkinson’s disease after dietary supplementation with branched-chain amino acids
- Cimifugin inhibits adipogenesis and TNF-α-induced insulin resistance in 3T3-L1 cells
- Predictors of gastrointestinal complaints in patients on metformin therapy
- Prescribing patterns in patients with chronic obstructive pulmonary disease and atrial fibrillation
- A retrospective analysis of the effect of latent tuberculosis infection on clinical pregnancy outcomes of in vitro fertilization–fresh embryo transferred in infertile women
- Appropriateness and clinical outcomes of short sustained low-efficiency dialysis: A national experience
- miR-29 regulates metabolism by inhibiting JNK-1 expression in non-obese patients with type 2 diabetes mellitus and NAFLD
- Clinical features and management of lymphoepithelial cyst
- Serum VEGF, high-sensitivity CRP, and cystatin-C assist in the diagnosis of type 2 diabetic retinopathy complicated with hyperuricemia
- ENPP1 ameliorates vascular calcification via inhibiting the osteogenic transformation of VSMCs and generating PPi
- Significance of monitoring the levels of thyroid hormone antibodies and glucose and lipid metabolism antibodies in patients suffer from type 2 diabetes
- The causal relationship between immune cells and different kidney diseases: A Mendelian randomization study
- Interleukin 33, soluble suppression of tumorigenicity 2, interleukin 27, and galectin 3 as predictors for outcome in patients admitted to intensive care units
- Identification of diagnostic immune-related gene biomarkers for predicting heart failure after acute myocardial infarction
- Long-term administration of probiotics prevents gastrointestinal mucosal barrier dysfunction in septic mice partly by upregulating the 5-HT degradation pathway
- miR-192 inhibits the activation of hepatic stellate cells by targeting Rictor
- Diagnostic and prognostic value of MR-pro ADM, procalcitonin, and copeptin in sepsis
- Review Articles
- Prenatal diagnosis of fetal defects and its implications on the delivery mode
- Electromagnetic fields exposure on fetal and childhood abnormalities: Systematic review and meta-analysis
- Characteristics of antibiotic resistance mechanisms and genes of Klebsiella pneumoniae
- Saddle pulmonary embolism in the setting of COVID-19 infection: A systematic review of case reports and case series
- Vitamin C and epigenetics: A short physiological overview
- Ebselen: A promising therapy protecting cardiomyocytes from excess iron in iron-overloaded thalassemia patients
- Aspirin versus LMWH for VTE prophylaxis after orthopedic surgery
- Mechanism of rhubarb in the treatment of hyperlipidemia: A recent review
- Surgical management and outcomes of traumatic global brachial plexus injury: A concise review and our center approach
- The progress of autoimmune hepatitis research and future challenges
- METTL16 in human diseases: What should we do next?
- New insights into the prevention of ureteral stents encrustation
- VISTA as a prospective immune checkpoint in gynecological malignant tumors: A review of the literature
- Case Reports
- Mycobacterium xenopi infection of the kidney and lymph nodes: A case report
- Genetic mutation of SLC6A20 (c.1072T > C) in a family with nephrolithiasis: A case report
- Chronic hepatitis B complicated with secondary hemochromatosis was cured clinically: A case report
- Liver abscess complicated with multiple organ invasive infection caused by hematogenous disseminated hypervirulent Klebsiella pneumoniae: A case report
- Urokinase-based lock solutions for catheter salvage: A case of an upcoming kidney transplant recipient
- Two case reports of maturity-onset diabetes of the young type 3 caused by the hepatocyte nuclear factor 1α gene mutation
- Immune checkpoint inhibitor-related pancreatitis: What is known and what is not
- Does total hip arthroplasty result in intercostal nerve injury? A case report and literature review
- Clinicopathological characteristics and diagnosis of hepatic sinusoidal obstruction syndrome caused by Tusanqi – Case report and literature review
- Synchronous triple primary gastrointestinal malignant tumors treated with laparoscopic surgery: A case report
- CT-guided percutaneous microwave ablation combined with bone cement injection for the treatment of transverse metastases: A case report
- Malignant hyperthermia: Report on a successful rescue of a case with the highest temperature of 44.2°C
- Anesthetic management of fetal pulmonary valvuloplasty: A case report
- Rapid Communication
- Impact of COVID-19 lockdown on glycemic levels during pregnancy: A retrospective analysis
- Erratum
- Erratum to “Inhibition of miR-21 improves pulmonary vascular responses in bronchopulmonary dysplasia by targeting the DDAH1/ADMA/NO pathway”
- Erratum to: “Fer exacerbates renal fibrosis and can be targeted by miR-29c-3p”
- Retraction
- Retraction of “Study to compare the effect of casirivimab and imdevimab, remdesivir, and favipiravir on progression and multi-organ function of hospitalized COVID-19 patients”
- Retraction of “circ_0062491 alleviates periodontitis via the miR-142-5p/IGF1 axis”
- Retraction of “miR-223-3p alleviates TGF-β-induced epithelial-mesenchymal transition and extracellular matrix deposition by targeting SP3 in endometrial epithelial cells”
- Retraction of “SLCO4A1-AS1 mediates pancreatic cancer development via miR-4673/KIF21B axis”
- Retraction of “circRNA_0001679/miR-338-3p/DUSP16 axis aggravates acute lung injury”
- Retraction of “lncRNA ACTA2-AS1 inhibits malignant phenotypes of gastric cancer cells”
- Special issue Linking Pathobiological Mechanisms to Clinical Application for cardiovascular diseases
- Effect of cardiac rehabilitation therapy on depressed patients with cardiac insufficiency after cardiac surgery
- Special issue The evolving saga of RNAs from bench to bedside - Part I
- FBLIM1 mRNA is a novel prognostic biomarker and is associated with immune infiltrates in glioma
- Special Issue Computational Intelligence Methodologies Meets Recurrent Cancers - Part III
- Development of a machine learning-based signature utilizing inflammatory response genes for predicting prognosis and immune microenvironment in ovarian cancer