Determining cardiac vagal threshold from short term heart rate complexity
-
Rami Abou Hamdan
 ,
Andy Schumann
,
Andy Schumann

Abstract
Evaluating individual aerobic exercise capacity is fundamental in sports and exercise medicine but associated with organizational and instrumental effort. Here, we extract an index related to common performance markers, the aerobic and anaerobic thresholds enabling the estimation of exercise capacity from a conventional sports watch supporting beatwise heart rate tracking. Therefore, cardiac vagal threshold (CVT) was determined in 19 male subjects performing an incremental maximum exercise test. CVT varied around the anaerobic threshold AnT with mean deviation of 7.9 ± 17.7 W. A high correspondence of the two thresholds was indicated by Bland-Altman plots with limits of agreement −27.5 W and 43.4 W. Additionally, CVT was strongly correlated AnT (rp = 0.86, p < 0.001) and reproduced this marker well (rc = 0.81). We conclude, that cardiac vagal threshold derived from compression entropy time course can be useful to assess physical fitness in an uncomplicated way.
1 Introduction
The assessment of aerobic exercise capacity is an essential part for the determination of physical fitness, evaluation of training effects as well as for exercise prescription and risk stratification. Most approaches of adequate performance diagnostics require sophisticated organizational and instrumental effort. Recently, attempts have been made to reproduce common performance markers by analyzing temporal change of heart rate variability during exercise [1], [2]. Investigating the decline of vagal mediated heart rate variability indices were shown to be a promising approach. At rest, compression entropy Hc has become an established information-theoretic method to assess complexity at small time scales [3], [4], [5]. We determined the minimum in Hc time course and compared this characteristic point to aerobic threshold (AeT) and anaerobic threshold (AnT).
Maximal parameters like maximal oxygen uptake and maximal power output attained during exercise testing are the most frequently applied indicators of aerobic endurance capacity and physical fitness. The determination of these maximal performance parameters requires an adequate motivation and maximal effort of participants. Therefore, the AeT and the AnT were often used to determine aerobic fitness. Both thresholds are common in clinical exercise testing and are known to be reproducible submaximal indicators of endurance and physical fitness. In contrast to peak parameters, the determination of these thresholds offers the great advantage that maximal effort and motivation in subjects are not mandatory. AeT demarcates the upper limit of a range of exercise intensities (moderate exercise domain) that can be accomplished almost entirely aerobically. AnT indicates the transition between heavy and very heavy exercise domains.
In this study we extract cardiac vagal threshold from compression entropy time course and relate this index to the individual aerobic and anaerobic threshold, for estimation of exercise capacity from a wearable heart rate monitor on beat-to-beat basis.
2 Methods
2.1 Incremental maximum exercise test IMET
Spiroergometries of 19 male students were conducted in a climate-controlled room at 22°C. Participants had no present or past history of any clinically significant disorders. Informed written consent was obtained in accordance with the protocols approved by the ethics committee of Jena University Hospital in accordance with the ethical guidelines of the Helsinki Declaration. A bicycle ergometer (SRM System, Schoberer Radmesstechnik, Jülich, Germany) was used to perform the IMET. The incremental bicycle protocol started after a resting period of 5 min at 50 W and increased by 50 W every 3 min until volitional exhaustion.
2.2 Data recordings
Breath-by-breath gas exchange measurements were carried out during the test (Ganshorn, Medizin Electronic GmbH, Niederlauer, Germany). VO2 data were time-averaged using 10 s intervals to assess maximum VO2. Power output was linearly interpolated throughout the stages to monotonically increasing load. Pmax was defined as the maximal achieved power output.
Capillary blood samples for lactate measurements (Enzymatic-Amperometric Measuring System, Eppendorf, Hamburg, Germany) were taken at the end of each stage. AeTs and AnTs were determined using the lactate-power output plot. Special software (ERGONIZER, Freiburg, Germany) was used for the calculation of AeTs, which represents the first increase in blood lactate concentrations above resting state values during incremental exercise. The AnT describes the maximal lactate steady state and refers to the exercise intensity above which a continuous increase in blood lactate is unavoidable. AeT and AnT were determined according to the method described by Dickhuth et al. [6].
The Borg 6-to-20 scale was used to assess the degree of subjective effort perceived by the participants. Maximal blood lactate concentration ≥8 mmol/l and Borg rating of perceived exertion ≥18 were applied to guarantee an accurate assessment of fitness and training indices during IMET.
2.3 Cardiac vagal threshold
During IMET heart rate was recorded by telemetric HR monitor (RS800CX, Polar Electro, Kempele, Finland). Time series exported from the device were post-processed by adaptive filtering [7]. To analyze temporal evolution of parasympathetic cardiac activity, compression entropy Hc was calculated in sliding windows of 512 BBI with 480 BBI overlap. In each window temporal change of heart beat intervals was transferred to symbols. An adaptive approach based on statistical properties of the BBI segment was used, in contrast to the conventional method [3], [4]. Thresholds li of i-th window were defined as multiple of standard deviation sd (li = 0.2sdi; 0.4sdi; 0.6sdi; … 2sdi) leading to an alphabet of 19 possible symbols.
In short, compression entropy estimates to which extend a symbol series can be reproduced by its own past, i.e. when patterns of the signal recur at frequent intervals. Information is compressed by encoding symbols in the look-ahead buffer regarding redundant symbol series that have already been encoded. Identical substrings can be passed and the number of iterations needed to encode the signal can be reduced without losing information. Standard sizes for analysis windows of memory window w = 7 BBI and buffer b = 3 BBI were used [4], [5].
To characterize parasympathetic withdrawal, cardiac vagal threshold CVT was extracted by separating initial decline of Hc from subsequent saturation phase. Therefore, a polynomial of third order was fitted to the time course minimizing the squared error. The minimum of the fit was defined as vagal threshold. An example is illustrated in Figure 1.
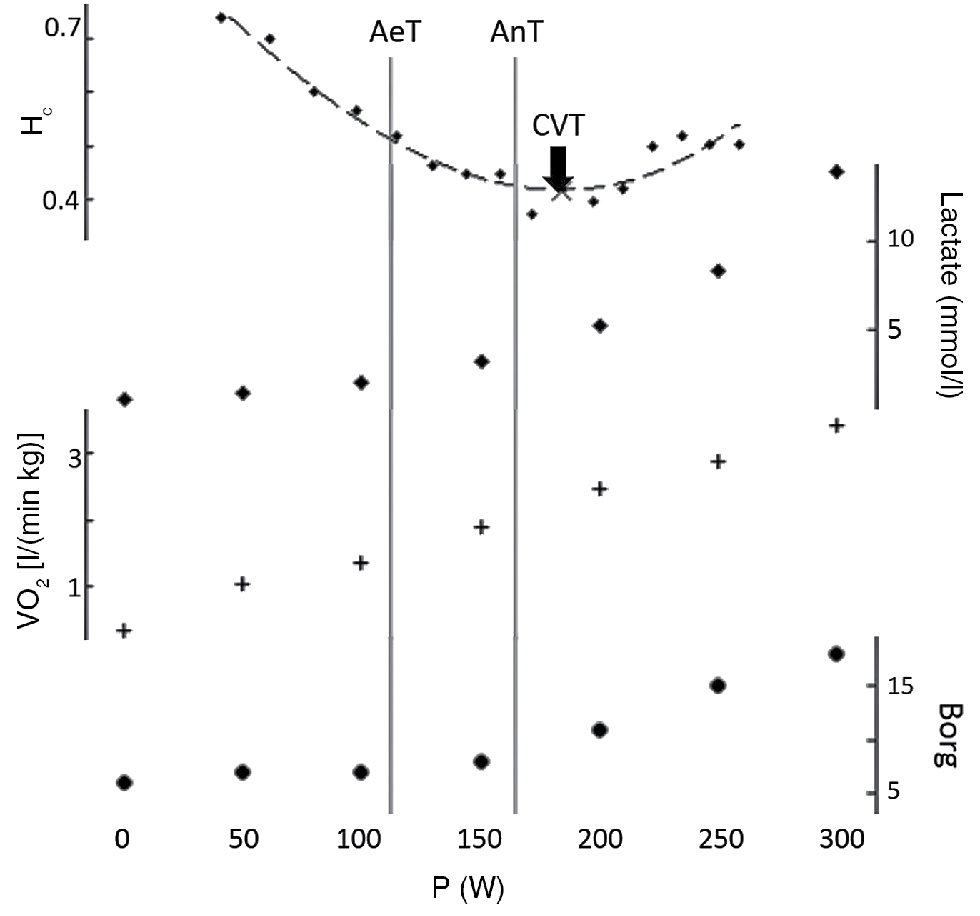
Example of CVT (black arrow) estimated on compression entropy time course (asterisks). AeT and AnT derived from lactate levels are indicated by vertical gray lines. Dashed line: polynomial of third order fitted to data points. crosses: Lactate concentration. diamonds: VO2. circles: Borg ratings, load of P = 0W equals baseline.
2.4 Statistical analysis
We assessed linear dependence of vagal cardiac threshold VCT and anaerobic threshold AnT by Pearson correlation coefficient rp, i.e. the quotient of covariance of X and Y (SXY) and the standard deviations of X and Y (SX, SY), with X = VCT, Y = AnT.
In Lin et al. concordance coefficient rc (eq. 4) was used to assess degree of reproducibility, that is not sufficiently covered by Pearson correlation coefficient [8].
Bland-Altman plots were generated by plotting differences of CVT and AnT against mean value of them. Limits of agreement were calculated by mean ± twice the standard deviation [9].
3 Results
In Figure 1 the determination of vagal and aerobic threshold is illustrated for one example recording. Compression entropy (asterisks) initially declines in a linear fashion and levels out around the AnT, which was determined from the lactate time course (crosses). The third order polynomial (dashed line) fits Hc anchor points quite well. For comparison the change of Borg scale (diamonds) and VO2 (circles) was plotted below.
Our study population was quite young (24.2 years) and normal weighted (BMI = 23.7, body fat = 15%, fat free mass FFM = 64.6%). Mean heart rate and global variability were 62.2/min and 82.7 ms. Short term vagal fluctuations estimated by RMSSD and Hc were 44.5 ms and 0.75 at rest. On average participants achieved maximum load of 300 W. Baseline lactate concentration and Borg rating increased from 0.8 mmol/l and 6.2 to 11.8 mmol/l and 19.4. Maximum heart was 190/min and oxygen uptake VO2max reached 45.2 l/min⋅kg. Mean aerobic and anaerobic thresholds achieved were AeT = 123 W and AnT = 184W. Cardiac vagal threshold derived from Hc time course was 192 W. Mean deviation of CVT from AeT was 69.0 ± 19.1 W and 7.9 ± 17.7 W from AnT. T-Test confirmed that the deviation from AeT was systematic (divergence high significantly greater zero). Whereas, the difference to AnT varies around zero (p < 0.05). In Figure 2 CVT was plotted against AnT. A linear correlation (rp = 0.86, p < 0.001) was apparent. Concordance coefficient of both thresholds was rc = 0.81. On the right side of Figure 2 the difference of AnT and CVT (ΔT) was drawn dependent on the mean of both (AnT-CVT)/2. Limits of agreement were −27.5 W and 43.4 W with one outlier under the lower limit. CVT was correlated to AeT (r = 0.85**), maximum load (r = 0.49*) and maximum lactate concentration (r = −0.48*). ΔT was not correlated to thresholds AeT (r = 0.17) and AnT (r = 0.11), Pmax (r = −0.18), HRmax (r = 0.27), HRrest (r = 0.04) and Hcrest (r = 0.27).
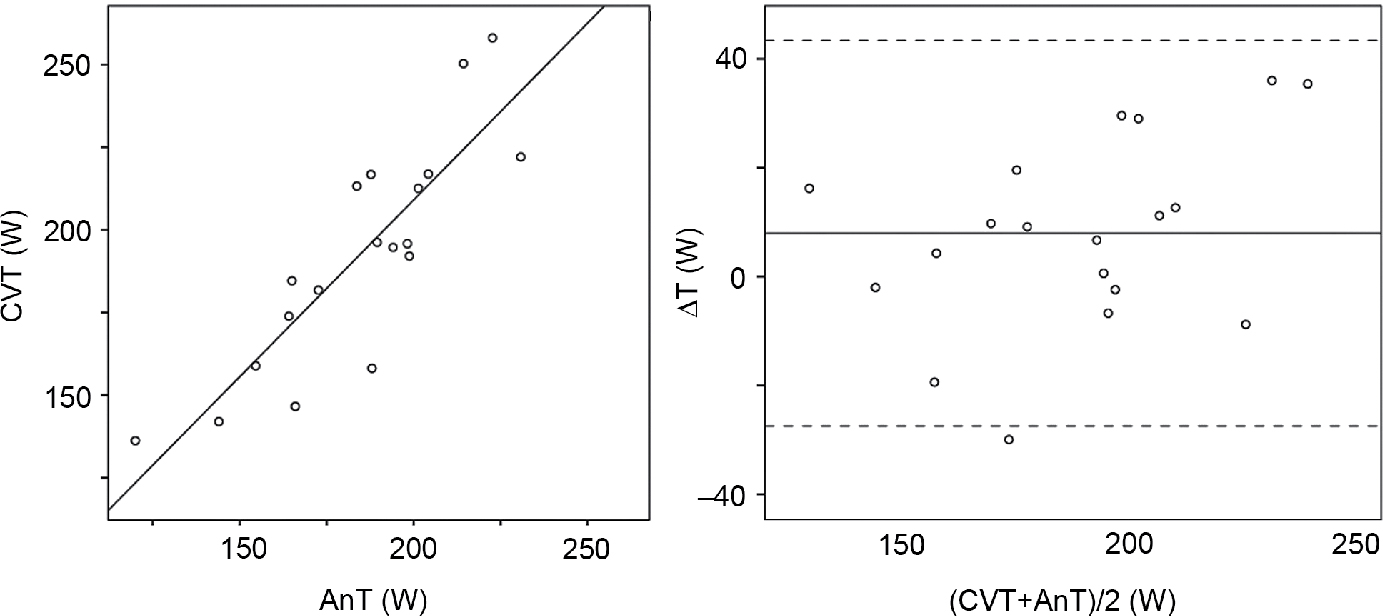
Left: cardiac vagal threshold (CVT) plottet against anaerobic threshold (AnT) with linear regression line. Right: Bland-Altman plot of deviation CVT-AnT dependent on their mean (AnT + CVT)/2.
Characterization of the data set. Results at rest and during exercise (maximum) are given in mean ± standard deviation.
| Parameter | Mean ± Standard deviation |
|---|---|
| Age (years) | 24.22 ± 1.06 |
| Height (cm) | 179 ± 4 |
| Weight (kg) | 76.2 ± 7.7 |
| BMI | 23.7 ± 2.4 |
| Body fat (%) | 15 ± 3 |
| FFM (%) | 65 ± 5 |
| Lactaterest (mmol/l) | 0.8 ± 0.2 |
| Borgrest | 6.2 ± 0.4 |
| HRrest (1/min) | 62.2 ± 7.5 |
| sdNNrest (ms) | 82.7 ± 23.5 |
| RMSSDrest (ms) | 44.5 ± 18.6 |
| Hcrest (ms) | 0.75 ± 0.04 |
| VO2max (l/min⋅kg) | 45.2 ± 4.6 |
| Lactatemax (mmol/l) | 11.8 ± 2.1 |
| Borgmax | 19.4 ± 0.6 |
| Pmax (W) | 300.0 ± 29.4 |
| HRmax (1/min) | 190.2 ± 6.4 |
| AeT (W) | 123 ± 21 |
| AnT (W) | 184 ± 28 |
| CVT (W) | 192 ± 34 |
BMI, body mass index; FFM, fat free mass; HR, heart rate; sdNN, standard deviation of BBI; RMSSD, root mean square of successive BBI; Hc, compression entropy; Pmax, maximum load; VO2, oxygen uptake; AeT, aerobic threshold; AnT, anaerobic threshold; CVT, cardiac vagal threshold.
4 Discussion
In this study we applied a new approach of deriving cardiac vagal threshold from temporal evolution of short-term complexity of heart rate assessed by compression entropy. In 19 young male participants we found a high correlation and concordance to the AnT. Accurate reproduction of this established marker of physical fitness (with 8 W mean deviation) indicates that cardiac vagal threshold is capable of revealing exercise performance.
In Figure 1 time course of compression entropy Hc, lactate levels, oxygen uptake (VO2) and Borg ratings. CVT was estimated at load 9.1 W after AnT was reached. An abrupt increase of lactate concentration and Borg rating is obvious at AnT. That indicates the importance of this characteristic time point.
Our group of male participants is young and sporty, with low BMI, body fat and resting heart rate. This sample is obviously not representative for normal population but probably quite adequate to represent active male people interested in sports. Maximum parameters indicate that subjects were relatively well-trained and performed the exercise test until individual limit of tolerance. CVT was close to the AnT with a mean error of about 8 W. Pearson correlation coefficient of r = 0.86 (p < 0.001) demonstrated a strong linear relationship. Reproducibility of AnT by CVT with rc = 0.81 seems high compared to the examples given in Lin et al. [8]. There was no systematic error evoked by resting heart rate and its compression entropy or maximum parameters of physical effort. Neither a dependency on the aerobic and anaerobic thresholds was found.
In comparison to other approaches using compression entropy to evaluate vagal short-term modulation of heart rate has some advantages. The symbolization procedure is robust against outliers, makes BBI efficient to store and is not dependent on highly precise r-wave detection allowing lower ECG sample rates. Compression algorithm can easily be implemented in analysis software as data compression based on string matching has become a common tool e.g. for producing zip-archives [4], [10]. We conclude, that CVT extracted from short term heart rate complexity is useful for evaluating aerobic exercise capacity. The presented strategy is simple and inexpensive and the findings of the present study offer an advance in the determination of the AnT, which is amongst other things important for developing health promotion exercise programs.
Author’s Statement
Research funding: The author state no funding involved. Conflict of interest: Authors state no conflict of interest. Ethical approval: The research has been complied with all the relevant national regulations, institutional policies and was performed in accordance with the tenets of the Helsinki Declaration, and has been approved by the ethics committee of Jena University.
References
[1] Flöter N, Schmidt T, Keck A, Reer R, Braumann K. Bestimmung der individuellen anaeroben Schwelle mittels der Herzfrequenzvariabilität in Abhängigkeit von der sympathoadrenergen Aktivität. Dtsch Z für Sportmed. 2012;63:41–5.10.5960/dzsm.2011.062Search in Google Scholar
[2] Horn A, Schulz H, Heck H. Minimum der HRV-Leistungs-Kurve im Vergleich zu objektiven Kriterien der Ausdauerleistungsfähigkeit. Sport-Prävention-Therapie. 2003;1:195–203Search in Google Scholar
[3] Ostermann S, Herbsleb M, Schulz S, Donath L, Berger S, Eisenträger D, et al. Exercise reveals the interrelation of physical fitness, inflammatory response, psychopathology, and autonomic function in patients with schizophrenia. Schizophr Bull. 2013;39:1139–49.10.1093/schbul/sbs085Search in Google Scholar PubMed PubMed Central
[4] Baumert M, Baier V, Haueisen J, et al. Forecasting of life threatening arrhythmias using the compression entropy of heart rate. Methods Inf Med. 2004;43:202–6.10.1055/s-0038-1633859Search in Google Scholar
[5] Bär KJ, Boettger MK, Koschke M, Schulz S, Chokka P, Yeragani VK, et al. Non-linear complexity measures of heart rate variability in acute schizophrenia. Clin Neurophysiol. 2007;118:2009–15.10.1016/j.clinph.2007.06.012Search in Google Scholar PubMed
[6] Dickhuth H-H, Röcker K, Mayer F, Nieß A, Horstmann T, Heitkamp H-Ch, et al. Bedeutung der Leistungsdiagnostik und Trainingssteuerung bei Ausdauer- und Spielsportarten. Deutsche Zeitschrift für Sportmedizin 1996;1:183–9.Search in Google Scholar
[7] Wessel N, Voss A, Malberg H, Ziehmann C, Voss HU, Schirdewan A, et al. Nonlinear analysis of complex phenomena in cardiological data. Herzschrittmachertherapie und Elektrophysiologie. 2000;11:159–7310.1007/s003990070035Search in Google Scholar
[8] Lin LI. A concordance correlation coefficient to evaluate reproducibility. Biometrics. 1989;45:255–68.10.2307/2532051Search in Google Scholar
[9] Bland JM, Altman DG. Measuring agreement in method comparison studies. Stat Methods Med Res. 1999;8:135–60.10.1177/096228029900800204Search in Google Scholar PubMed
[10] Baumert M, Baier V, Voss A. Estimating the complexity of heart rate fluctuations – an approach based on compression entropy. Fluct Noise. 2005;5:557–63.10.1142/S0219477505003026Search in Google Scholar
©2016 Rami Abou Hamdan et al., licensee De Gruyter.
This work is licensed under the Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 License.
Articles in the same Issue
- Synthesis and characterization of PIL/pNIPAAm hybrid hydrogels
- Novel blood protein based scaffolds for cardiovascular tissue engineering
- Cell adhesion and viability of human endothelial cells on electrospun polymer scaffolds
- Effects of heat treatment and welding process on superelastic behaviour and microstructure of micro electron beam welded NiTi
- Long-term stable modifications of silicone elastomer for improved hemocompatibility
- The effect of thermal treatment on the mechanical properties of PLLA tubular specimens
- Biocompatible wear-resistant thick ceramic coating
- Protection of active implant electronics with organosilicon open air plasma coating for plastic overmolding
- Examination of dielectric strength of thin Parylene C films under various conditions
- Open air plasma deposited antimicrobial SiOx/TiOx composite films for biomedical applications
- Systemic analysis about residual chloroform in PLLA films
- A macrophage model of osseointegration
- Towards in silico prognosis using big data
- Technical concept and evaluation of a novel shoulder simulator with adaptive muscle force generation and free motion
- Usability evaluation of a locomotor therapy device considering different strategies
- Hypoxia-on-a-chip
- Integration of a semi-automatic in-vitro RFA procedure into an experimental setup
- Fabrication of MEMS-based 3D-μECoG-MEAs
- High speed digital interfacing for a neural data acquisition system
- Bionic forceps for the handling of sensitive tissue
- Experimental studies on 3D printing of barium titanate ceramics for medical applications
- Patient specific root-analogue dental implants – additive manufacturing and finite element analysis
- 3D printing – a key technology for tailored biomedical cell culture lab ware
- 3D printing of hydrogels in a temperature controlled environment with high spatial resolution
- Biocompatibility of photopolymers for additive manufacturing
- Biochemical piezoresistive sensors based on pH- and glucose-sensitive hydrogels for medical applications
- Novel wireless measurement system of pressure dedicated to in vivo studies
- Portable auricular device for real-time swallow and chew detection
- Detection of miRNA using a surface plasmon resonance biosensor and antibody amplification
- Simulation and evaluation of stimulation scenarios for targeted vestibular nerve excitation
- Deep brain stimulation: increasing efficiency by alternative waveforms
- Prediction of immediately occurring microsleep events from brain electric signals
- Determining cardiac vagal threshold from short term heart rate complexity
- Classification of cardiac excitation patterns during atrial fibrillation
- An algorithm to automatically determine the cycle length coverage to identify rotational activity during atrial fibrillation – a simulation study
- Deriving respiration from high resolution 12-channel-ECG during cycling exercise
- Reducing of gradient induced artifacts on the ECG signal during MRI examinations using Wilcoxon filter
- Automatic detection and mapping of double potentials in intracardiac electrograms
- Modeling the pelvic region for non-invasive pelvic intraoperative neuromonitoring
- Postprocessing algorithm for automated analysis of pelvic intraoperative neuromonitoring signals
- Best practice: surgeon driven application in pelvic operations
- Vasomotor assessment by camera-based photoplethysmography
- Classification of morphologic changes in photoplethysmographic waveforms
- Novel computation of pulse transit time from multi-channel PPG signals by wavelet transform
- Efficient design of FIR filter based low-pass differentiators for biomedical signal processing
- Nonlinear causal influences assessed by mutual compression entropy
- Comparative study of methods for solving the correspondence problem in EMD applications
- fNIRS for future use in auditory diagnostics
- Semi-automated detection of fractional shortening in zebrafish embryo heart videos
- Blood pressure measurement on the cheek
- Derivation of the respiratory rate from directly and indirectly measured respiratory signals using autocorrelation
- Left cardiac atrioventricular delay and inter-ventricular delay in cardiac resynchronization therapy responder and non-responder
- An automatic systolic peak detector of blood pressure waveforms using 4th order cumulants
- Real-time QRS detection using integrated variance for ECG gated cardiac MRI
- Preprocessing of unipolar signals acquired by a novel intracardiac mapping system
- In-vitro experiments to characterize ventricular electromechanics
- Continuous non-invasive monitoring of blood pressure in the operating room: a cuffless optical technology at the fingertip
- Application of microwave sensor technology in cardiovascular disease for plaque detection
- Artificial blood circulatory and special Ultrasound Doppler probes for detecting and sizing gaseous embolism
- Detection of microsleep events in a car driving simulation study using electrocardiographic features
- A method to determine the kink resistance of stents and stent delivery systems according to international standards
- Comparison of stented bifurcation and straight vessel 3D-simulation with a prior simulated velocity profile inlet
- Transient Euler-Lagrange/DEM simulation of stent thrombosis
- Automated control of the laser welding process of heart valve scaffolds
- Automation of a test bench for accessing the bendability of electrospun vascular grafts
- Influence of storage conditions on the release of growth factors in platelet-rich blood derivatives
- Cryopreservation of cells using defined serum-free cryoprotective agents
- New bioreactor vessel for tissue engineering of human nasal septal chondrocytes
- Determination of the membrane hydraulic permeability of MSCs
- Climate retainment in carbon dioxide incubators
- Multiple factors influencing OR ventilation system effectiveness
- Evaluation of an app-based stress protocol
- Medication process in Styrian hospitals
- Control tower to surgical theater
- Development of a skull phantom for the assessment of implant X-ray visibility
- Surgical navigation with QR codes
- Investigation of the pressure gradient of embolic protection devices
- Computer assistance in femoral derotation osteotomy: a bottom-up approach
- Automatic depth scanning system for 3D infrared thermography
- A service for monitoring the quality of intraoperative cone beam CT images
- Resectoscope with an easy to use twist mechanism for improved handling
- In vitro simulation of distribution processes following intramuscular injection
- Adjusting inkjet printhead parameters to deposit drugs into micro-sized reservoirs
- A flexible standalone system with integrated sensor feedback for multi-pad electrode FES of the hand
- Smart control for functional electrical stimulation with optimal pulse intensity
- Tactile display on the remaining hand for unilateral hand amputees
- Effects of sustained electrical stimulation on spasticity assessed by the pendulum test
- An improved tracking framework for ultrasound probe localization in image-guided radiosurgery
- Improvement of a subviral particle tracker by the use of a LAP-Kalman-algorithm
- Learning discriminative classification models for grading anal intraepithelial neoplasia
- Regularization of EIT reconstruction based on multi-scales wavelet transforms
- Assessing MRI susceptibility artefact through an indicator of image distortion
- EyeGuidance – a computer controlled system to guide eye movements
- A framework for feedback-based segmentation of 3D image stacks
- Doppler optical coherence tomography as a promising tool for detecting fluid in the human middle ear
- 3D Local in vivo Environment (LivE) imaging for single cell protein analysis of bone tissue
- Inside-Out access strategy using new trans-vascular catheter approach
- US/MRI fusion with new optical tracking and marker approach for interventional procedures inside the MRI suite
- Impact of different registration methods in MEG source analysis
- 3D segmentation of thyroid ultrasound images using active contours
- Designing a compact MRI motion phantom
- Cerebral cortex classification by conditional random fields applied to intraoperative thermal imaging
- Classification of indirect immunofluorescence images using thresholded local binary count features
- Analysis of muscle fatigue conditions using time-frequency images and GLCM features
- Numerical evaluation of image parameters of ETR-1
- Fabrication of a compliant phantom of the human aortic arch for use in Particle Image Velocimetry (PIV) experimentation
- Effect of the number of electrodes on the reconstructed lung shape in electrical impedance tomography
- Hardware dependencies of GPU-accelerated beamformer performances for microwave breast cancer detection
- Computer assisted assessment of progressing osteoradionecrosis of the jaw for clinical diagnosis and treatment
- Evaluation of reconstruction parameters of electrical impedance tomography on aorta detection during saline bolus injection
- Evaluation of open-source software for the lung segmentation
- Automatic determination of lung features of CF patients in CT scans
- Image analysis of self-organized multicellular patterns
- Effect of key parameters on synthesis of superparamagnetic nanoparticles (SPIONs)
- Radiopacity assessment of neurovascular implants
- Development of a desiccant based dielectric for monitoring humidity conditions in miniaturized hermetic implantable packages
- Development of an artifact-free aneurysm clip
- Enhancing the regeneration of bone defects by alkalizing the peri-implant zone – an in vitro approach
- Rapid prototyping of replica knee implants for in vitro testing
- Protecting ultra- and hyperhydrophilic implant surfaces in dry state from loss of wettability
- Advanced wettability analysis of implant surfaces
- Patient-specific hip prostheses designed by surgeons
- Plasma treatment on novel carbon fiber reinforced PEEK cages to enhance bioactivity
- Wear of a total intervertebral disc prosthesis
- Digital health and digital biomarkers – enabling value chains on health data
- Usability in the lifecycle of medical software development
- Influence of different test gases in a non-destructive 100% quality control system for medical devices
- Device development guided by user satisfaction survey on auricular vagus nerve stimulation
- Empirical assessment of the time course of innovation in biomedical engineering: first results of a comparative approach
- Effect of left atrial hypertrophy on P-wave morphology in a computational model
- Simulation of intracardiac electrograms around acute ablation lesions
- Parametrization of activation based cardiac electrophysiology models using bidomain model simulations
- Assessment of nasal resistance using computational fluid dynamics
- Resistance in a non-linear autoregressive model of pulmonary mechanics
- Inspiratory and expiratory elastance in a non-linear autoregressive model of pulmonary mechanics
- Determination of regional lung function in cystic fibrosis using electrical impedance tomography
- Development of parietal bone surrogates for parietal graft lift training
- Numerical simulation of mechanically stimulated bone remodelling
- Conversion of engineering stresses to Cauchy stresses in tensile and compression tests of thermoplastic polymers
- Numerical examinations of simplified spondylodesis models concerning energy absorption in magnetic resonance imaging
- Principle study on the signal connection at transabdominal fetal pulse oximetry
- Influence of Siluron® insertion on model drug distribution in the simulated vitreous body
- Evaluating different approaches to identify a three parameter gas exchange model
- Effects of fibrosis on the extracellular potential based on 3D reconstructions from histological sections of heart tissue
- From imaging to hemodynamics – how reconstruction kernels influence the blood flow predictions in intracranial aneurysms
- Flow optimised design of a novel point-of-care diagnostic device for the detection of disease specific biomarkers
- Improved FPGA controlled artificial vascular system for plethysmographic measurements
- Minimally spaced electrode positions for multi-functional chest sensors: ECG and respiratory signal estimation
- Automated detection of alveolar arches for nasoalveolar molding in cleft lip and palate treatment
- Control scheme selection in human-machine- interfaces by analysis of activity signals
- Event-based sampling for reducing communication load in realtime human motion analysis by wireless inertial sensor networks
- Automatic pairing of inertial sensors to lower limb segments – a plug-and-play approach
- Contactless respiratory monitoring system for magnetic resonance imaging applications using a laser range sensor
- Interactive monitoring system for visual respiratory biofeedback
- Development of a low-cost senor based aid for visually impaired people
- Patient assistive system for the shoulder joint
- A passive beating heart setup for interventional cardiology training
Articles in the same Issue
- Synthesis and characterization of PIL/pNIPAAm hybrid hydrogels
- Novel blood protein based scaffolds for cardiovascular tissue engineering
- Cell adhesion and viability of human endothelial cells on electrospun polymer scaffolds
- Effects of heat treatment and welding process on superelastic behaviour and microstructure of micro electron beam welded NiTi
- Long-term stable modifications of silicone elastomer for improved hemocompatibility
- The effect of thermal treatment on the mechanical properties of PLLA tubular specimens
- Biocompatible wear-resistant thick ceramic coating
- Protection of active implant electronics with organosilicon open air plasma coating for plastic overmolding
- Examination of dielectric strength of thin Parylene C films under various conditions
- Open air plasma deposited antimicrobial SiOx/TiOx composite films for biomedical applications
- Systemic analysis about residual chloroform in PLLA films
- A macrophage model of osseointegration
- Towards in silico prognosis using big data
- Technical concept and evaluation of a novel shoulder simulator with adaptive muscle force generation and free motion
- Usability evaluation of a locomotor therapy device considering different strategies
- Hypoxia-on-a-chip
- Integration of a semi-automatic in-vitro RFA procedure into an experimental setup
- Fabrication of MEMS-based 3D-μECoG-MEAs
- High speed digital interfacing for a neural data acquisition system
- Bionic forceps for the handling of sensitive tissue
- Experimental studies on 3D printing of barium titanate ceramics for medical applications
- Patient specific root-analogue dental implants – additive manufacturing and finite element analysis
- 3D printing – a key technology for tailored biomedical cell culture lab ware
- 3D printing of hydrogels in a temperature controlled environment with high spatial resolution
- Biocompatibility of photopolymers for additive manufacturing
- Biochemical piezoresistive sensors based on pH- and glucose-sensitive hydrogels for medical applications
- Novel wireless measurement system of pressure dedicated to in vivo studies
- Portable auricular device for real-time swallow and chew detection
- Detection of miRNA using a surface plasmon resonance biosensor and antibody amplification
- Simulation and evaluation of stimulation scenarios for targeted vestibular nerve excitation
- Deep brain stimulation: increasing efficiency by alternative waveforms
- Prediction of immediately occurring microsleep events from brain electric signals
- Determining cardiac vagal threshold from short term heart rate complexity
- Classification of cardiac excitation patterns during atrial fibrillation
- An algorithm to automatically determine the cycle length coverage to identify rotational activity during atrial fibrillation – a simulation study
- Deriving respiration from high resolution 12-channel-ECG during cycling exercise
- Reducing of gradient induced artifacts on the ECG signal during MRI examinations using Wilcoxon filter
- Automatic detection and mapping of double potentials in intracardiac electrograms
- Modeling the pelvic region for non-invasive pelvic intraoperative neuromonitoring
- Postprocessing algorithm for automated analysis of pelvic intraoperative neuromonitoring signals
- Best practice: surgeon driven application in pelvic operations
- Vasomotor assessment by camera-based photoplethysmography
- Classification of morphologic changes in photoplethysmographic waveforms
- Novel computation of pulse transit time from multi-channel PPG signals by wavelet transform
- Efficient design of FIR filter based low-pass differentiators for biomedical signal processing
- Nonlinear causal influences assessed by mutual compression entropy
- Comparative study of methods for solving the correspondence problem in EMD applications
- fNIRS for future use in auditory diagnostics
- Semi-automated detection of fractional shortening in zebrafish embryo heart videos
- Blood pressure measurement on the cheek
- Derivation of the respiratory rate from directly and indirectly measured respiratory signals using autocorrelation
- Left cardiac atrioventricular delay and inter-ventricular delay in cardiac resynchronization therapy responder and non-responder
- An automatic systolic peak detector of blood pressure waveforms using 4th order cumulants
- Real-time QRS detection using integrated variance for ECG gated cardiac MRI
- Preprocessing of unipolar signals acquired by a novel intracardiac mapping system
- In-vitro experiments to characterize ventricular electromechanics
- Continuous non-invasive monitoring of blood pressure in the operating room: a cuffless optical technology at the fingertip
- Application of microwave sensor technology in cardiovascular disease for plaque detection
- Artificial blood circulatory and special Ultrasound Doppler probes for detecting and sizing gaseous embolism
- Detection of microsleep events in a car driving simulation study using electrocardiographic features
- A method to determine the kink resistance of stents and stent delivery systems according to international standards
- Comparison of stented bifurcation and straight vessel 3D-simulation with a prior simulated velocity profile inlet
- Transient Euler-Lagrange/DEM simulation of stent thrombosis
- Automated control of the laser welding process of heart valve scaffolds
- Automation of a test bench for accessing the bendability of electrospun vascular grafts
- Influence of storage conditions on the release of growth factors in platelet-rich blood derivatives
- Cryopreservation of cells using defined serum-free cryoprotective agents
- New bioreactor vessel for tissue engineering of human nasal septal chondrocytes
- Determination of the membrane hydraulic permeability of MSCs
- Climate retainment in carbon dioxide incubators
- Multiple factors influencing OR ventilation system effectiveness
- Evaluation of an app-based stress protocol
- Medication process in Styrian hospitals
- Control tower to surgical theater
- Development of a skull phantom for the assessment of implant X-ray visibility
- Surgical navigation with QR codes
- Investigation of the pressure gradient of embolic protection devices
- Computer assistance in femoral derotation osteotomy: a bottom-up approach
- Automatic depth scanning system for 3D infrared thermography
- A service for monitoring the quality of intraoperative cone beam CT images
- Resectoscope with an easy to use twist mechanism for improved handling
- In vitro simulation of distribution processes following intramuscular injection
- Adjusting inkjet printhead parameters to deposit drugs into micro-sized reservoirs
- A flexible standalone system with integrated sensor feedback for multi-pad electrode FES of the hand
- Smart control for functional electrical stimulation with optimal pulse intensity
- Tactile display on the remaining hand for unilateral hand amputees
- Effects of sustained electrical stimulation on spasticity assessed by the pendulum test
- An improved tracking framework for ultrasound probe localization in image-guided radiosurgery
- Improvement of a subviral particle tracker by the use of a LAP-Kalman-algorithm
- Learning discriminative classification models for grading anal intraepithelial neoplasia
- Regularization of EIT reconstruction based on multi-scales wavelet transforms
- Assessing MRI susceptibility artefact through an indicator of image distortion
- EyeGuidance – a computer controlled system to guide eye movements
- A framework for feedback-based segmentation of 3D image stacks
- Doppler optical coherence tomography as a promising tool for detecting fluid in the human middle ear
- 3D Local in vivo Environment (LivE) imaging for single cell protein analysis of bone tissue
- Inside-Out access strategy using new trans-vascular catheter approach
- US/MRI fusion with new optical tracking and marker approach for interventional procedures inside the MRI suite
- Impact of different registration methods in MEG source analysis
- 3D segmentation of thyroid ultrasound images using active contours
- Designing a compact MRI motion phantom
- Cerebral cortex classification by conditional random fields applied to intraoperative thermal imaging
- Classification of indirect immunofluorescence images using thresholded local binary count features
- Analysis of muscle fatigue conditions using time-frequency images and GLCM features
- Numerical evaluation of image parameters of ETR-1
- Fabrication of a compliant phantom of the human aortic arch for use in Particle Image Velocimetry (PIV) experimentation
- Effect of the number of electrodes on the reconstructed lung shape in electrical impedance tomography
- Hardware dependencies of GPU-accelerated beamformer performances for microwave breast cancer detection
- Computer assisted assessment of progressing osteoradionecrosis of the jaw for clinical diagnosis and treatment
- Evaluation of reconstruction parameters of electrical impedance tomography on aorta detection during saline bolus injection
- Evaluation of open-source software for the lung segmentation
- Automatic determination of lung features of CF patients in CT scans
- Image analysis of self-organized multicellular patterns
- Effect of key parameters on synthesis of superparamagnetic nanoparticles (SPIONs)
- Radiopacity assessment of neurovascular implants
- Development of a desiccant based dielectric for monitoring humidity conditions in miniaturized hermetic implantable packages
- Development of an artifact-free aneurysm clip
- Enhancing the regeneration of bone defects by alkalizing the peri-implant zone – an in vitro approach
- Rapid prototyping of replica knee implants for in vitro testing
- Protecting ultra- and hyperhydrophilic implant surfaces in dry state from loss of wettability
- Advanced wettability analysis of implant surfaces
- Patient-specific hip prostheses designed by surgeons
- Plasma treatment on novel carbon fiber reinforced PEEK cages to enhance bioactivity
- Wear of a total intervertebral disc prosthesis
- Digital health and digital biomarkers – enabling value chains on health data
- Usability in the lifecycle of medical software development
- Influence of different test gases in a non-destructive 100% quality control system for medical devices
- Device development guided by user satisfaction survey on auricular vagus nerve stimulation
- Empirical assessment of the time course of innovation in biomedical engineering: first results of a comparative approach
- Effect of left atrial hypertrophy on P-wave morphology in a computational model
- Simulation of intracardiac electrograms around acute ablation lesions
- Parametrization of activation based cardiac electrophysiology models using bidomain model simulations
- Assessment of nasal resistance using computational fluid dynamics
- Resistance in a non-linear autoregressive model of pulmonary mechanics
- Inspiratory and expiratory elastance in a non-linear autoregressive model of pulmonary mechanics
- Determination of regional lung function in cystic fibrosis using electrical impedance tomography
- Development of parietal bone surrogates for parietal graft lift training
- Numerical simulation of mechanically stimulated bone remodelling
- Conversion of engineering stresses to Cauchy stresses in tensile and compression tests of thermoplastic polymers
- Numerical examinations of simplified spondylodesis models concerning energy absorption in magnetic resonance imaging
- Principle study on the signal connection at transabdominal fetal pulse oximetry
- Influence of Siluron® insertion on model drug distribution in the simulated vitreous body
- Evaluating different approaches to identify a three parameter gas exchange model
- Effects of fibrosis on the extracellular potential based on 3D reconstructions from histological sections of heart tissue
- From imaging to hemodynamics – how reconstruction kernels influence the blood flow predictions in intracranial aneurysms
- Flow optimised design of a novel point-of-care diagnostic device for the detection of disease specific biomarkers
- Improved FPGA controlled artificial vascular system for plethysmographic measurements
- Minimally spaced electrode positions for multi-functional chest sensors: ECG and respiratory signal estimation
- Automated detection of alveolar arches for nasoalveolar molding in cleft lip and palate treatment
- Control scheme selection in human-machine- interfaces by analysis of activity signals
- Event-based sampling for reducing communication load in realtime human motion analysis by wireless inertial sensor networks
- Automatic pairing of inertial sensors to lower limb segments – a plug-and-play approach
- Contactless respiratory monitoring system for magnetic resonance imaging applications using a laser range sensor
- Interactive monitoring system for visual respiratory biofeedback
- Development of a low-cost senor based aid for visually impaired people
- Patient assistive system for the shoulder joint
- A passive beating heart setup for interventional cardiology training