Characteristics of BCR–ABL gene variants in patients of chronic myeloid leukemia
-
Huma Amin
 und
Suhaib Ahmed
und
Suhaib Ahmed

Abstract
Background
Depending on breakpoints of rearrangement different types of BCR–ABL fusion protein can be generated in patients of chronic myeloid leukemia (CML). The aim of this study is to observe frequencies of major transcripts in CML patients by reverse transcriptase polymerase chain reaction (RT-PCR) and their hematological features at the time of presentation.
Materials and methods
This cross sectional study was performed at Molecular Lab of Riphah International University, Islamabad from January to June 2019. Consecutive peripheral blood samples of 70 newly diagnosed CML patients in chronic phase were analyzed by RT-PCR to detect different BCR–ABL transcripts. Routine blood cell counts were assessed by an automated hematology analyzer.
Results
All samples expressed typical BCR–ABL rearrangement. Expression of either e14a2 or e13a2 transcript was detected in 38 (54%) and 30 (43%) patients, respectively. Coexpression of e13a2 + e14a2 was found in 2 (3%) patients. The mean total leukocyte count was higher in group expressing e13a2 (P = 0.01). Higher mean platelet count was noted in patients with e14a2 transcript, but this difference was statistically insignificant (P = 0.1). The association of male gender was observed with the group exhibiting e14a2 (P = 0.01). There was no statistically significant association between transcript type and different ranges of age, hemoglobin levels, and platelet and total leukocyte counts (P > 0.05).
Conclusion
e14a2 transcript was most common transcript in CML patients. Patients exhibiting e13a2 subgroup presented with significantly higher mean white blood cell count at the time of presentation. Significantly higher proportion of male patients was found to express e14a2 transcript over e13a2.
1 Introduction
CML is associated with a cytogenetic abnormality known as Philadelphia (Ph) chromosome. This is one of the definitive diagnostic markers for CML [1]. Ph chromosome arises from a reciprocal translocation t (9; 22) between chromosome 9 and 22 [2,3]. The Philadelphia chromosome is present in approximately 95% of patients with CML [4]. However, few CML patients do not demonstrate Ph chromosome or might have normal karyotype, but even in one third of these patients, there is occult BCR–ABL fusion gene (Ph chromosome negative and BCR–ABL positive) [5]. Molecular analysis confirms presence of BCR–ABL in these patients [6].
Break point in BCR gene occurs in three main regions: Major (M-BCR), minor (m-BCR), and micro (µ-BCR) breakpoint cluster regions [3]. Large majority of CML patients have breakpoints in M-BCR region on chromosome 22 [7]. This area consists of BCR exons 12–16 (previously referred to as exons b1–b5, respectively) [8] (Figure 1). The classic transcript found in majority of CML patients is b2a2 or b3a2, formed by fusing exon 13 (b2) or exon 14 (b3) of BCR to exon 2 (a2) of ABL gene, respectively. Both of them code for a 210 kDa (p210) novel protein [9]. More than 95% of BCR–ABL transcripts are either e13a2 or e14a2 in CML. “Atypical” transcripts with a breakpoint in ABL intron 1 and BCR intron 6 (e6a2) and breakpoint in ABL intron 2 and BCR intron 1 (e1a3), BCR intron 13 (e13a3), and BCR intron 14 (e14a3) have been sometimes reported [10]. Variable frequencies of these fusion transcripts in CML patients are observed around the world [11].
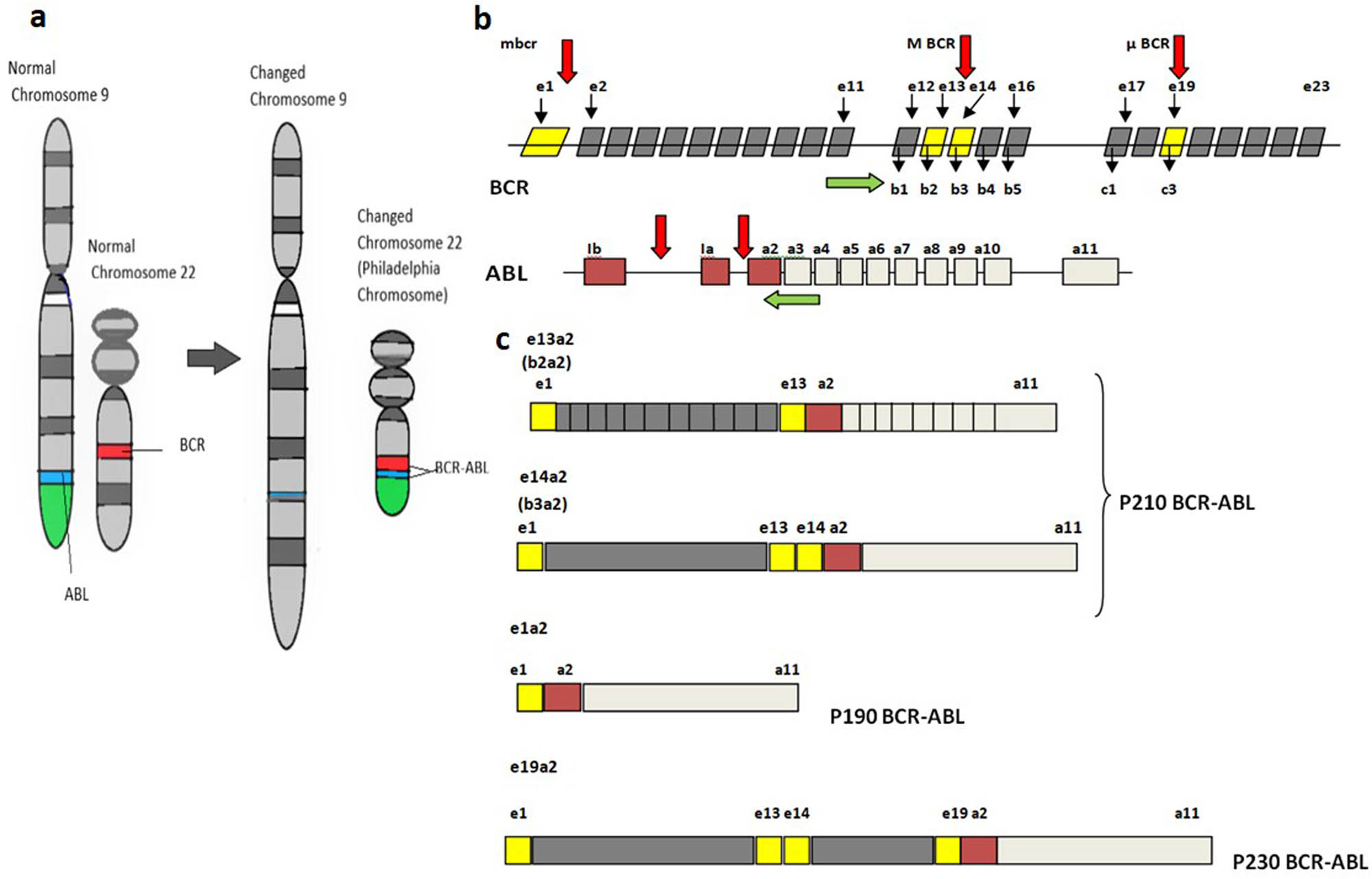
(a) Schematic diagram of the normal structure of chromosome 9 and 22 and translocation between chromosome 9 and 22, resulting in Philadelphia chromosome. (b) Schematic representation of the molecular structure of BCR and ABL genes. Red arrows indicate breakpoints in both genes. Green arrows show the placement of forward and reverse primer on the exons of BCR and ABL for detection of different transcripts by RT-PCR. (c) Schematic diagram of the structure of chimeric mRNA transcribed from different breakpoints of BCR–ABL fusion gene.
Clinical and hematological profile of CML patients with different fusion transcripts revealed some noticeable features [12]. The knowledge of differences in breakpoints might have some clinical importance, and disease phenotype of patients may vary with them. M-BCR usually presents with classical CML phenotype [11]. While an interesting finding associated with b3a2 fusion transcript is the higher platelet counts [13].
Reverse transcriptase PCR (RT-PCR) is one of the most sensitive techniques used for detection of BCR–ABL transcripts associated with CML [9]. Most of the current RT-PCR methods are designed and optimized for detecting the transcript of M-BCR and m-BCR breakpoints. Very large PCR products or atypical transcripts may get away with detection using these routine primers. The application of RT-PCR techniques can be improved by several methods including the development of multiplex RT-PCR to detect the BCR–ABL variants in patients with CML [14].
In this study, RT-PCR was used for the detection of all major BCR–ABL transcripts in CML patients, and the frequency of BCR–ABL transcripts was observed along with their presenting hematological features.
2 Material and methods
This cross-sectional study was carried out from January 2019 to June 2019. Patients were recruited from tertiary care hospital of Rawalpindi. Molecular analysis was carried out in the laboratory settings of Riphah International University. Informed consent was taken from each patient. The study was approved by the ethical review committee of the University.
Total of 70 consecutive newly diagnosed patients of CML in chronic phase irrespective of age and gender were included in this study. Diagnosis of CML was made based on clinical presentation and morphologic criteria of bone marrow aspirate. Patients who had started any kind of treatment previously with any dose or for any length of time were excluded from this study.
Peripheral blood samples in ethylene diamine tetra acetic acid (EDTA) tubes were collected and rapidly transported at 2–8°C to the laboratory to minimize mRNA degradation. Routine, blood cell counts were performed on automated hematology analyzer.
2.1 RNA extraction and cDNA synthesis
Extraction of total RNA was carried from whole blood by TRIzol® reagent (TRI Reagent L.S). The extracted RNA was reverse-transcribed to cDNA by using gene-specific primer (ABL-2). cDNA was used as a template for qualitative detection of type of BCR–ABL transcript by one-step RT-PCR.
2.2 RT-PCR conditions
Primer sequences to be used for qualitative RT-PCR are given below. Primers were obtained from Integrated DNA Technologies (IDT) in the lyophilized form and stored at −20°C.
Forward primer: BCR E-12 AGA ACA TCC GGG AGC AGC AGA AGA A; Reverse primer: ABL-2 TCC AAC GAG CGG ATT CAC T.
DNA amplification was done in 30 μL reaction mixture, which included 15 μL PCR Mix (Invitrogen PCR Super Mix includes PCR buffer (22 mM Tris HCL, pH 8.4), 1.65 mM MgCL2, 220 µM dNTPs, and 22 U recombinant TaqDNA polymerase/mL), 1 μL of 10 pM Primer Mix (forward and reverse primers), 0.25 μL enzyme RT (SuperScript™ III Reverse Transcriptase 200 U/μL Invitrogen, USA), 5 μL template RNA, and 9 μL nuclease-free water. The synthesis of complementary DNA and amplification of the target were done by using the recommended thermal cycling conditions outlined below:
Amplified products were electrophoresed on a 6% polyacrylamide gel electrophoresis. The gels were stained with 0.1% silver nitrate. The bands were detected at 310 and 385 bp for e13a2 and e14a2, respectively. Molecular variants of e1a2 and e19a2 products were expected to form bands at 481 and at 244 bp, respectively.
To determine the sensitivity of the PCR method, an assay was carried out by generating a 10-fold (1/1, 1/10, 1/100, and 1/1,000) of a RT-PCR positive BCR–ABL RNA in nuclease-free water. These serial dilutions and one negative sample were run under identical RT-PCR conditions (as described earlier) in five separate reaction tubes for cDNA synthesis and PCR amplifications.
2.3 PCR strategy
Initial PCR was performed with E12 forward and ABL 2 reverse primers to detect p210 kDa variants (Figure 1). Since atypical transcripts are rare, a second confirmatory PCR was to be performed in typical variant BCR–ABL-negative patient. Atypical transcripts could be easily suspected from their different product sizes on gel electrophoresis after preliminary PCR results. Second PCR was planned to be performed using the forward primers (E1, E6, E19, etc.) with common reverse ABL3 primers separately for the suspected breakpoint region. To further validate the finding, atypical transcript could be confirmed by DNA sequencing.
All statistical calculations were done using SPSS 22 software. Quantitative data were expressed as mean ± S.D. The variables included numerical data such as age, Hb concentration, WBC count, and platelet count. Independent t test was applied to compare the means of two different transcripts. Frequency and percentages were calculated for the qualitative data such as gender and type of transcript. Variables such as age, hemoglobin, WBC counts, and platelet counts were also presented as ranges, and their frequencies were calculated. Chi square test was performed to see the association of categorical variables with different transcripts. P value of <0.05 was considered as significant.
-
Ethics approval and consent to participate: The study was approved by the ethical review committee of Institutional review committee Islamic International Medical College (Ref No. Appl. # Riphah/ERC/15/0119).
-
Patient consent for publication: Consent was obtained from all the patients for the use of their medical data for research purposes.
3 Results
Molecular analysis was performed with conventional RT-PCR on total of 70 patients (64% males and 36% females) for the type of CML transcript. Demographic details of these patients are presented in Table 1.
Clinical and laboratory details of CML patients in study
| Number of patients (n) | 70 |
| Mean age (years) | 41.10 ± 14.14 |
| Range of age (years) | 15–70 |
| Male/female (n) | 45/25 |
| Male-to-female ratio | 1.8 |
| Mean leukocytes count (×109/L) | 145.12 ± 89.03 |
| Mean hemoglobin levels (g/dL) | 10.65 ± 2.42 |
| Mean platelets count (×109/L) | 441.77 ± 403.18 |
CML: chronic myeloid leukemia.
Clinical and laboratory data of patients in chronic phase at the time of presentation. Data are presented as mean ± standard deviation.
3.1 Qualitative analysis of BCR–ABL transcripts
RT-PCR was carried out with the aim that it should be able to primarily detect the most prevalent transcripts e13a2 and e14a2. An internal control (ABL gene) reaction was also included to correctly interpret negative results.
Initial PCR for the M-BCR transcripts was performed with BCR forward primer located on exon 12 (e12). The common reverse ABL primer was located in ABL exon 2 (Figure 1). This primer combination in RT-PCR can simultaneously detect both common types of BCR–ABL breakpoint (e14a2 and e13a2) on the M-BCR region in single reaction.
All studied patients 70/70 (100%) were found positive for typical BCR–ABL (p210 kDa). Either e13a2 or e14a2 transcript was detected in all the samples. The detected bands were as follows: 385 bp for e14a2 and 310 bp for e13a2. No atypical transcript was observed in any of the sample analyzed. Neither product of unexpected size was detected on gel electrophoresis after conventional RT-PCR. Common forward primer e12 was only used in this study to reveal the type of transcripts. Figure 2 represents the results of RT-PCR for some of the patients.
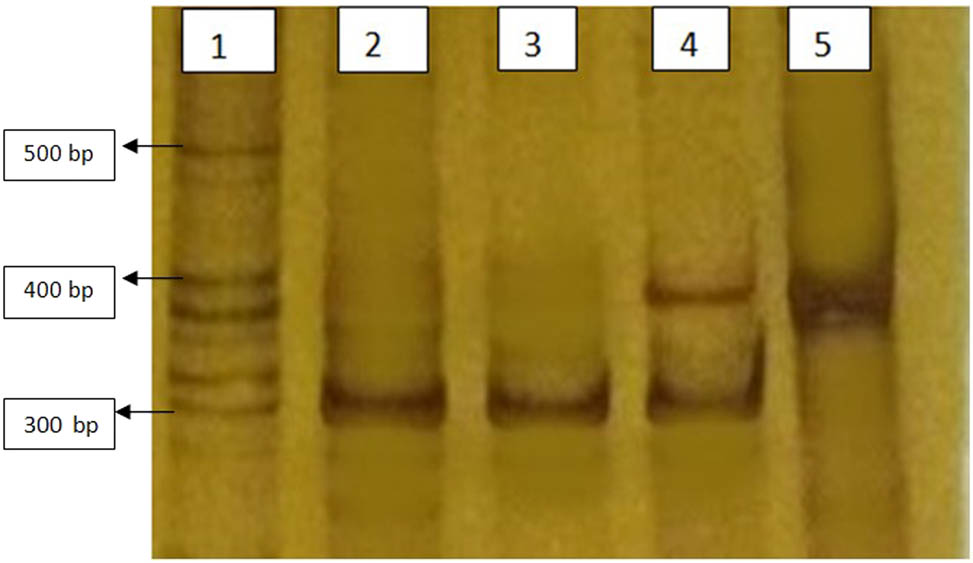
Silver stained polyacrylamide gel electrophoresis showing different transcripts of BCR–ABL after RT-PCR with e12a2 primer. All lanes are positive for BCR–ABL mutation typical p210 kDa (e13a2 and/or e14a2) transcripts. Lane 1 shows ladder (molecular weight marker) of various size fragments. bp (base pair). Lanes 2 and 3 are from chronic phase CML patients expressing 310 bp fragment of e13a2 BCR–ABL. Lane 4 is from a chronic phase CML patient co expressing both e13a2 and e14a2 BCR–ABL. Lane 5 is from a chronic phase CML patient expressing 385 bp fragment of e14a2 BCR–ABL.
Running the tenfold dilution on electrophoresis gel after RT-PCR revealed that the detection limit of this assay was up to 10−4 for each sample.
3.2 Frequency of different transcripts along with their presenting features in CML patients
Among 70 CML patients analyzed, e14a2 transcript was most commonly detected. Total of 38 (54%) cases had solitary expression of e14a2, and 30 (43%) of the remaining cases were positive for e13a2 transcripts exclusively. Co-expression of both types of transcripts (e13a2 + e14a2) was observed in only two (3%) patients and were excluded from further analysis (Figure 3).
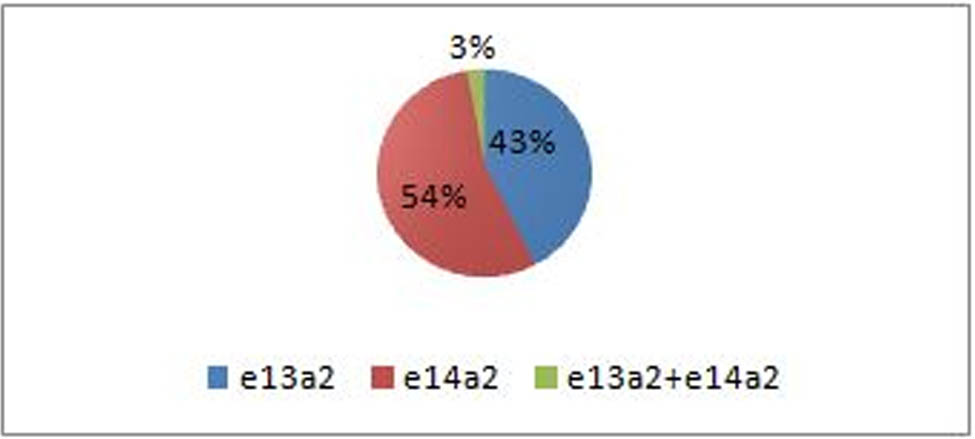
Frequency of different types of BCR–ABL transcripts among 70 CML patients in chronic phase analyzed in the study. Total of 38 (54%) patients had solitary expression of e14a2 transcript. Expression of e13a2 exclusively was found in 30 (43%) patients. Co-expression of both types of transcripts (e13a2 + e14a2) was observed in only two (3%) patients. The types of transcripts detected in all patients are color coded as shown in box.
The comparative analysis of quantitative data (expressed as means ± S.D) of the two groups with expression of either e13a2 or e14a2 transcript is presented in Table 2. Patients with e14a2 transcripts showed lower mean age, but the difference was not statistically significant (P = 0.4). The mean total white blood cell count was significantly higher in the group of patients expressing e13a2 than those with e14a2 transcript (P = 0.01). Higher mean platelet count was observed in patients with e14a2 transcript, but this difference was not statistically significant (P = 0.1). No significant difference in mean hemoglobin concentration between the two groups was found (P > 0.05; Table 2).
Characteristics of the CML patients with e13a2 and e14a2 transcripts
| Variables | e13a2 | e14a2 | P value |
|---|---|---|---|
| Mean age (years) | 42.90 ± 13.82 | 40.13 ± 14.93 | 0.4 |
| Mean leukocytes count (×109/L) | 173.75 ± 97.17 | 120.77 ± 77.67 | 0.01* |
| Mean hemoglobin levels (g/dL) | 10.84 ± 2.62 | 10.50 ± 2.34 | 0.5 |
| Mean platelets count (×109/L) | 352.33 ± 229.8 | 512.13 ± 495.78 | 0.1 |
CML: chronic myeloid leukemia.
Data on 68 CML patients in chronic phase at the time of presentation expressing either of the two transcripts. Co expression of transcripts was detected in only two patients (data not summarized). Data are presented as mean ± standard deviation. P < 0.05 was considered as significant.
*Statistically significant.
Figure 4 represents the frequency of all study patients with typical p210 kDa (e13a2 or e14a2) transcripts in different ranges of hemoglobin concentration, leukocyte count, and platelet count. The highest frequency of 38 (56%) patients at the time of diagnosis had hemoglobin concentration in the range of 7–11 g/dL. The majority of patients of typical transcript (43 (63%) patients) presented with TLC ranging from more than 100 × 109/L. The analysis of patients with typical transcript with different ranges of platelet count revealed that 39 (58%) patients had normal platelet count at the time of diagnosis followed by thrombocytosis in 22 (32%) patients (Figure 4).
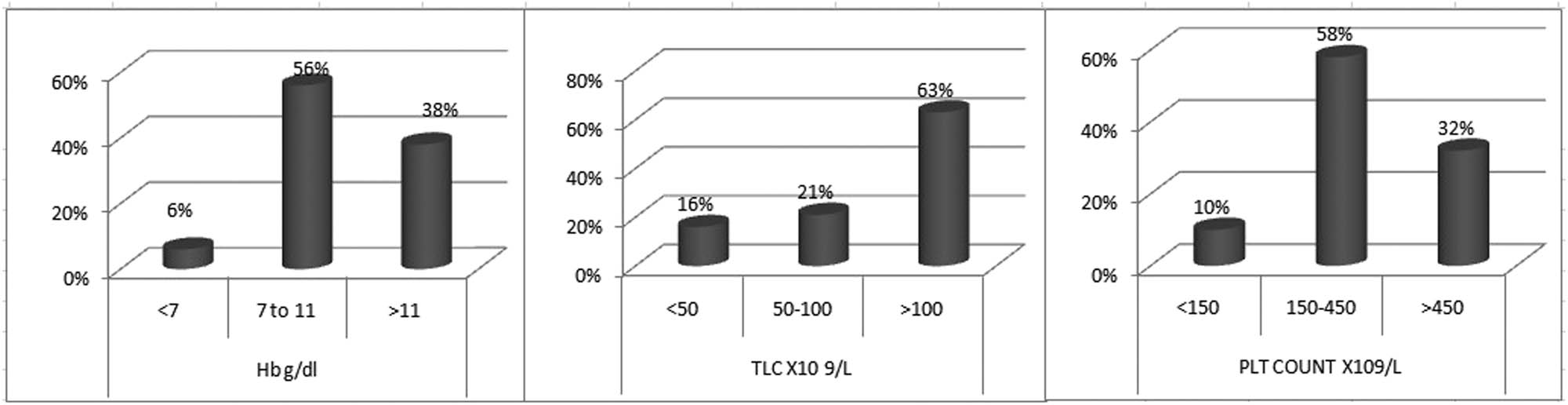
Frequency of CML patients with either e13a2 or e14a2 transcript in different hemoglobin levels, TLC (total leukocyte count), and PLT (platelets) count. Data on 68 patients in choric phase at the time of presentation were summarized.
Variables such as age, hemoglobin levels, and platelet and total leukocyte counts were further divided into ranges to see the distribution of patients with either e13a2 or e14a2 transcript. The comparison of categorical data in two transcripts group is summarized in Table 3. A significantly higher frequency of males 29 (76%) was observed in patients exhibiting e14a2 transcript compared to females (P = 0.01). Distribution of the transcript within two age groups showed no significant difference (P = 0.51). Similarly, no statistically significant difference in frequency of patients was observed in different ranges of hemoglobin levels and platelet and total leukocyte counts with specific transcript type (P > 0.05).
Distribution of patients exhibiting e13a2 and e14a2 transcripts according to gender and different ranges of age, hemoglobin levels, and total leukocyte and platelets counts
| Hematological variables | Transcript type | Total | P value | |
|---|---|---|---|---|
| e13a2 (n = 30) | e14a2 (n = 38) | |||
| Age (years) | 0.51 | |||
| <45 | 15 (50%) | 22 (58%) | 37 (54%) | |
| 45 and above | 15 (50%) | 16 (42%) | 31 (46%) | |
| Gender | 0.01* | |||
| Male | 14 (47%) | 29 (76%) | 43 (63%) | |
| Female | 16 (53%) | 09 (24%) | 25 (37%) | |
| Hemoglobin levels (g/dL) | 0.61 | |||
| <7 g/dL | 1 (3%) | 3 (8%) | 4 (6%) | |
| 7–11 g/dL | 16 (53.3%) | 22 (58%) | 38 (56%) | |
| >11 g/dL | 13 (43.3%) | 13 (34%) | 26 (38%) | |
| Total leukocyte count 10 9 /L | 0.15 | |||
| <50 | 2 (7%) | 9 (24%) | 11 (16%) | |
| 50–100 | 6 (20%) | 8 (21%) | 14 (21%) | |
| >100 | 22 (73%) | 21 (55%) | 43 (63%) | |
| Platelet count ×10 9 /L | 0.09 | |||
| <150 | 5 (16%) | 2 (5%) | 7 (10%) | |
| 150–450 | 19 (64%) | 20 (53%) | 39 (58%) | |
| >450 | 6 (20%) | 16 (42%) | 22 (32%) | |
Chi square test was performed to see the association of categorical variables with different transcripts. P < 0.05 is taken as significant. Data are summarized from 68 patient with either e13a2 or e14a2 transcript.
*Statistically significant.
Figure 5 exhibits the relation of e13a2 and e14a2 transcripts within different subsets of hematological parameters and gender. Association of male gender with e14a2 and female gender with e13a2 can be appreciated (P = 0.01). Larger proportion of e14a2 transcript was demonstrated in subgroups of (i) platelets count of >450 × 109/L and (ii) leukocyte count of <50 × 109/L, but statistically significant association between these subgroups and transcript could not be established (P > 0.05).
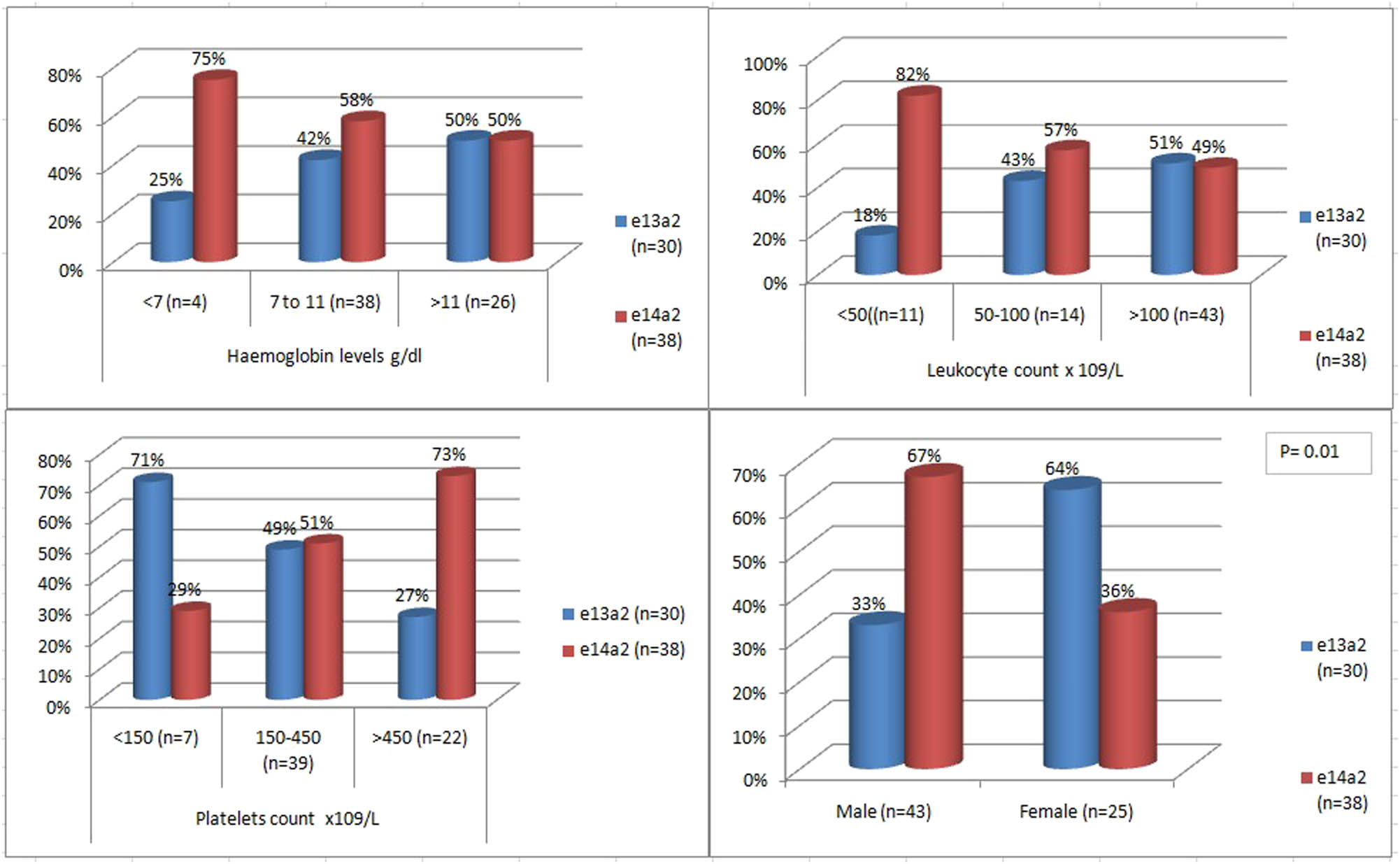
Transcript stratified frequency of CML patients within different subsets of hematological parameter and gender. Bar chart demonstrates association of these variables with e13a2 and e14a2 transcripts. The types of transcripts are color coded as shown in box. P value of <0.05 is taken as significant.
4 Discussion
The aim of this study is to detect and analyze the demographic and hematological characteristics according to the variants of BCR–ABL transcript in CML patients in our local population.
The technique used for detection of various transcripts consists of performing RT-PCR by choosing a primer specific for exon b1 (e12) on the BCR gene and reverse primer on ABL exon 2. The present approach has the benefit of simplifying and shortening the procedure of RT‑PCR for detection of these transcripts in single reaction. The need of independent sequence-specific primers were eliminated, which increases the complexity, workload, and cost of PCR.
The mean age of CML patients at diagnosis in this study group was found to be 41.10 ± 14.14 years (range, 15–70 years). This is much younger when compared with data from the western literature, showing older mean age (66, 52, and 59 years) at diagnosis in CML patients [15,16,17]. However, this finding is consistent with other Asian studies reported earlier [18,19,20]. Young age at diagnosis in CML patients is usually associated with low- and middle-income countries, and some possible environmental factors and under reporting of geriatric population in these countries could be the possible explanation for this [21].
This study revealed higher prevalence of males (63%) compare to females (37%) in CML patients. The male-to-female ratio was observed to be 1.8:1. This is almost similar to already reported figures from local [20,22] as well as studies from around the world [16,17,23]. Male predominance could be possibly because of the fact that hematological neoplasms are usually more common in males compared to females owing to genetic and hormonal differences [21].
This study demonstrated that the predominant transcript was e14a2 (b3a2) in CML patients. Comparable frequencies of e13a2, e14a2, and their co-expression were documented in some studies, but divergence from these results was also observed. The frequencies of common transcripts in CML patients in different populations have been summarized in Table 4.
Prevalence of BCR–ABL transcripts in different studies from various countries
| Countries | e14a2(b3a2) | e13a2(b3a2) | e14a2 + e13a2 | Others |
|---|---|---|---|---|
| Present study | 54% | 43% | 3% | — |
| Bulgaria [13] | 54% | 45% | 0% | — |
| India [24] | 56.25% | 41.25% | 0% | 2.5% |
| Pakistan [25] | 66.7% | 20.8% | 0% | 12.5%* |
| Brazil [26] | 64% | 34% | 2% | — |
| Malaysia [27] | 69% | 31% | 0% | — |
| Korea [28] | 68% | 32% | 0% | — |
| Iran [29] | 63% | 20% | 3% | 14% |
| India [30] | 68% | 24% | 0% | — |
| Argentina [31] | 37.5% | 41.7% | 8.3% | 12.5% |
| Syria [32] | 14.3% | 57% | — | 28.7% |
| Pakistan [33] | 26% | 56% | — | 18% |
| Brazil [34] | 48% | 36% | 16% | — |
Others include e1a2, e19a2, b3a3/b2a2, b3a3/b2a3, b3a3, and e1a3.
*No transcript detected.
A study conducted in India and Bulgaria calculated the ratio of the two major transcripts of M-BCR region e14a2:e13a2 to be 1.3:1, which is almost in agreement to the ratio observed in the present study [13,24]. However, studies from our local population represent comparatively higher ratio of the two transcripts than reported here [9,25]. Two times higher (ratio 2:1) of e14a2 than e13a2 were also reported in CML patients in Brazil, Malaysia, and Korea [26,27,28], while studies from Iran and India demonstrated the frequency of e14a2 transcripts to be almost three times higher than that of e13a2 [29,30]. Few studies have also documented higher frequency of e13a2 compared to more common e14a2 transcript in CML patients [31,32,33]. The variation in frequencies of common transcript among different population and regions of the world can be explained based on the dissimilarities of natural genetic factors, environmental factors, and living style in different ethnic groups [34].
This study demonstrated co expression of e13a2/e14a2 in only two patients (3%) of 70 patients analyzed. Varying results from all over the world have been reported regarding the co-expression of both transcripts e13a2 and e14a2 in patients with CML. Incidence of this co expression has been reported to be as high as 16% in a study from Brazil [34]. However, in our local population, the frequency of co-expression was reported to be very low, which is in agreement to the result of the present study [25,33].
The highest percentage (63%) of CML patient at the time of presentation in the present study had the total leukocyte count of >100 × 109/L, which means greater tumor burden at the time of diagnosis. The majority (58%) of the study patients also had platelet count within normal range. Both these findings are in accordance to the previous studies [22,23].
Clinical features of the patients with two groups of typical transcript were not found to be starkly different in this study. When comparing the difference in means of numerical variable, it was found that patients with e14a2 transcript were younger than patients with e13a2 transcript although this difference was not statistically significant. A recent study from our local population [25] and report originating from the Syrian population endorsed this observation [35]. The only hematological variable significantly different in our study was higher mean WBC counts in the group of patients expressing e13a2 than in those with e14a2 transcript. Higher mean WBC count in patients carrying e13a2 transcript was also recognized in previous studies [26,36]. Many studies proved statistically significant association between e14a2 transcripts and higher mean platelets count in CML patients at the time of diagnosis [13,26,36,37]. Higher platelets count in patients with e14a2 transcript was also observed in this study, but the difference was not found to be statistically significant. Few other studies reported no differences in hematological parameters in both transcripts of BCR–ABL fusion gene [25, 34, 35].
While observing possible relationship between the BCR–ABL variants and clinical parameters in CML patient, significant association of male gender was observed in e14a2 transcript in this study. This finding is in accordance to the studies conducted in Iran, India, and Iraq [29,30,36]. However, other studies do not support this observation and report no significant association in male and female proportion in both types of fusion gene [13,28,35].
The association of fusion transcripts was also compared by dividing hemoglobin levels, TLC, and platelet count in different ranges. Although e14a2 did show a higher association with high platelet count compared to e13a2, but it was not found to be statistically significant (P = 0.09). Similarly by stratifying the patients on the basis of white blood cell (WBC) count and hemoglobin levels, no significant association could be established in both transcript groups. Data published previously in different studies regarding association between hematological variables at diagnosis and transcripts type remain controversial [38,39].
It is also believed that the type of transcript alone is not responsible for differences between the clinical and hematological parameters, and there must be some other factors that modify these parameters [34]. European Leukemia Net recommendations do not give any caution to patients with different transcripts and suggest that these variant translocations do not affect the prognosis of CML patients [16].
5 Conclusion
In this study group, 100% (70) of the CML patients were found to have typical BCR–ABL transcripts with preponderance of e14a2 subtype. The group of patients with e13a2 transcript presented with significantly higher mean leukocyte count compared to e14a2 group. There was gender skewed distribution with male prevalence in e14a2 and female predominance in e13a2 transcript. Difference in leukocyte counts at diagnosis and gender association in two groups might suggest a discrete pathobiology and phenotype of disease. Identification of transcript type is not only beneficial to monitor disease carefully in patients but can also help to select additional treatment regimen with specific transcript. Further studies with large sample size are needed to determine possible contribution of BCR–ABL transcripts types and the presentation of disease, which might help in prognosis and disease management.
-
Funding information: Special thanks to Riphah International University for supporting this study and Genetic Resource Centre for providing the laboratory facilities for conduction of this study.
-
Author contributions: H.A.: literature search, study design and concept, data collection, data analysis, data interpretation, and drafting of manuscript. S.A.: revising it critically for important intellectual content, technical assistance, and final approval of the version to be published.
-
Conflict of interest: There was no conflict of interest.
-
Data availability statement: The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
References
[1] Maru JE, Branford S. Current developments in molecular monitoring in chronic myeloid leukemia. Ther Adv Hematol. 2016;7:237–51. 10.1177/2040620716657994.Suche in Google Scholar
[2] Chasseriau J, Rivet J, Bilan F, Chomel JC, Guilhot F, Bourmeyster N, et al. Characterization of the different BCR–ABL transcripts with a single multiplex RT-PCR. J Mol Diagn. 2004;6:343–7.10.1016/S1525-1578(10)60530-2Suche in Google Scholar
[3] Kurzrock R, Kantarjian HM, Shtalrid M, Gutterman JU, Moshe T. Philadelphia chromosome-negative chronic myelogenous leukemia without breakpoint cluster region rearrangement: a chronic myeloid leukemia with a distinct clinical course. Blood. 1990;75:445–52.10.1182/blood.V75.2.445.445Suche in Google Scholar
[4] O’dwyer M. Multifaceted approach to the treatment of BCR–ABL-positive leukemias. Oncologist. 2002;7:30–8.10.1634/theoncologist.7-suppl_1-30Suche in Google Scholar PubMed
[5] Kim JE, Yoon S, Choi BR, Kim KP, Cho YH, Jung W, et al. Cleavage of BCR–ABL transcripts at the T315I point mutation by DNAzyme promotes apoptotic cell death in Imatinib-resistant BCR–ABL leukemic cells. Leukemia. 2013;27:1650–8. 10.1038/leu.2013.60.Suche in Google Scholar PubMed
[6] Reena RMZ, Julia Munchar MJ, Salwati S, Zubaidah Z, Hamidah NH, Sharifah NA, et al. Detection of BCR/ABL gene in chronic myloid leukaemia: comparison of fluorescence in situ hybridisation (FISH), conventional cytogenetics and polymerase chain reaction (PCR) Techniques. Med Health. 2006;1:5–13.Suche in Google Scholar
[7] Sugimoto T, Ijima K, Hisatomi H, Murayama T, Mizuno I, Hato A, et al. Second case of CML with aberrant BCR–ABL fusion transcript (e8/a2) with insertion of an inverted ABL intron 1b sequence. Am J Hematol. 2004;77:164–6. 10.1002/ajh.20138.Suche in Google Scholar PubMed
[8] Deininger MWN, Goldman JM, Melo JV. The molecular biology of chronic myeloid leukemia. Blood. 2000;96:3343–56.10.1182/blood.V96.10.3343Suche in Google Scholar
[9] Iqbal Z, Manzoor F, Iqbal M, Ali S, Sheikh N, Khan M, et al. Frequency of BCR–ABL fusion oncogene splice variants associated with chronic myeloid leukemia (CML). J Cancer Ther. 2011;2:176–80. 10.4236/jct.2011.22022.Suche in Google Scholar
[10] Burmeister T, Reinhardt R. A multiplex PCR for improved detection of typical and atypical BCR–ABL fusion transcripts. Leukemia Res. 2008;32:579–85. 10.1016/j.leukres.2007.08.017.Suche in Google Scholar PubMed
[11] Anand MS, Varma N, Varma S, Rana KS, Malhotra P. Cytogenetic and molecular analyses in adult chronic myelogenous leukaemia patients in north India. Indian J Med Res. 2012;135:42–8.10.4103/0971-5916.93423Suche in Google Scholar PubMed PubMed Central
[12] Laurent E, Talpaz M, Kantarjian H, Kurzrock R. The BCR Gene and Philadelphia Chromosome-positive Leukemogenesis. Cancer Res. 2001;61:2343–55.Suche in Google Scholar
[13] Balatzenko G, Vundinti BR, Margarita G. Correlation between the type of BCR–ABL transcripts and blood cell counts in chronic myeloid leukemia – a possible influence of mdr1 gene expression. Hematol Rep. 2011;3:5–9. 10.4081/hr.2011.e3.Suche in Google Scholar PubMed PubMed Central
[14] Bennour A, Saad A, Sennana H. Chronic myeloid leukemia: relevance of cytogenetic and molecular assays. Crit Rev Oncol/Hematol. 2016;97:263–74. org/10.1016/j.critrevonc.2015.08.020.Suche in Google Scholar
[15] Chen Y, Wang H, Kantarjian H, Cortes J. Trends in chronic myeloid leukemia survival in the United States from 1975–2009. Leuk Lymphoma. 2013;54:1411–7. 10.1007/s13238-010-0016-z.Suche in Google Scholar PubMed PubMed Central
[16] Marzocchi G, Castagnetti F, Luatti S, Baldazzi C, Stacchini M, Gugliotta G, et al. Variant Philadelphia translocations: molecular-cytogenetic characterization and prognostic influence on front line imatinib therapy, a GIMEMA working party on CML analysis. Blood. 2011;117:6793–800. 10.1182/blood-2011-01-328294.Suche in Google Scholar PubMed
[17] Smith A, Roman E, Howell D, Jones R, Patmore R, Jack A. The haematological malignancy research network (HMRN): a new information strategy for population based epidemiology and health service research. Br J Haematol. 2009;148:739–53. 10.1111/j.1365-2141.2009.08010.Suche in Google Scholar
[18] Ashariati A, Ugroseno S. Profile of BCR–ABL transcript levels based on sokal prognostic score in chronic myeloid leukemia patients treated with imatinib. Acta Med Indones-Indones J Intern. 2013;45:108–13.Suche in Google Scholar
[19] Kuan JW, Michael MS. The epidemiology of chronic myeloid leukaemia in southern Sarawak, Borneo Island. Med J Malays. 2018;73:78–85.Suche in Google Scholar
[20] Tashfeen S, Ahmed S, Bhatti FA, Ali N. Real time polymerase chain reaction in diagnosis of chronic myeloid leukemia. J Coll Phys Surg Pak. 2014;24:190–3.Suche in Google Scholar
[21] Nguyen LT, Guo M, Naugler C, Rashid-Kolvear F. Incidence of chronic myeloid leukemia in Calgary, Alberta, Canada. BMC Res Notes. 2018;11:780. org/10.1186/s13104-018-3890-8.Suche in Google Scholar
[22] Bhatti FA, Ahmed S, Ali N. Clinical and hematological features of 335 patients of chronic myelogenous leukemia diagnosed at single centre in Northern Pakistan. Clin Med Insights Blood Disord. 2012;5:16–24. 10.4137/CMBD.S10578.Suche in Google Scholar
[23] Khaled SAA, Nashwa MA, Aziz AE. Demographic, clinical, and hematologic characteristics of patients with chronic myeloid leukemia in Upper Egypt: association with treatment responses. Egypt J Haematol. 2015;40:195–200. 10.4103/1110-1067.170221.Suche in Google Scholar
[24] Deb P, Chakrabarti P, Chakrabarti S, Aich R, Nath U, Rav S, et al. Incidence of BCR–ABL transcript variants in patients with chronic myeloid leukemia: their correlation with presenting features, risk scores and response to treatment with imatinib mesylate. Indian J Med Paediatr Oncol. 2014;35:26–30. 10.4103/0971-5851.133707.Suche in Google Scholar PubMed PubMed Central
[25] Javed A, Mukhtar H, Kubra K, Lodhi S, Abaidullah S. Detection of BCR–ABL fusion gene and its transcript variants in chronic myeloid leukaemia patients – a multi-comparison study. JPMA. 2020;70:1748. http://doi.org/10.5455/JPMA.30606.Suche in Google Scholar PubMed
[26] Vasconcelos AP, Azevedo IF, Melo FCBC, Neves WB, Azevedo ACAC, Melo RAM. BCR–ABL1 transcript types showed distinct Laboratory characteristics in patients with chronic myeloid leukemia. Genet Mol Res. 2017;16(2):541. 10.4238/gmr16029541.Suche in Google Scholar PubMed
[27] Hassan R, Ramli M, Abdullah WZ, Mustaffa R, Ghazali S, Ankathil R, et al. One-step multiplex RT-PCR for detection of BCR/ABL gene in Malay patients with chronic myeloid leukaemia. AsPac J Mol Biol Biotechnol. 2008;16:41–4.Suche in Google Scholar
[28] Goh HG, Hwang JY, Kim SH, Lee YH, Kim YL, Kim DW. Comprehensive analysis of BCR–ABL transcript types in Korean CML patients using a newly developed multiplex RT-PCR. Transl Res. 2006;148:249–56. 10.1016/j.trsl.2006.07.002.Suche in Google Scholar PubMed
[29] Yaghmaie M, Ghaffari SH, Ghavamzadeh A, Alimoghaddam K, Jahani M, Mousavi SA, et al. Frequency of BCR–ABL fusion transcripts in iranian patients with chronic myeloid leukemia. Arch Iran Med. 2008;11:247–51.Suche in Google Scholar
[30] Mir R, Ahmad I, Javid J, Zuberi M, Yadav P, Shazia R, et al. Simple multiplex RT-PCR for identifying common fusion BCR–ABL transcript types and evaluation of molecular response of the a2b2 and a2b3 transcripts to Imatinib resistance in North Indian chronic myeloid leukemia patients. Indian J Cancer. 2015;52:314–8. 10.4103/0019-509X.176741.Suche in Google Scholar PubMed
[31] Sastre DA, Argarana CE, Heller VB, Gallo M, Fernández EN, Rodríguez CM. An analysis of multiplex-PCR in the detection of BCR–ABL transcripts in hematological disorders. Genet Mol Biol. 2007;30:520–3.10.1590/S1415-47572007000400003Suche in Google Scholar
[32] Farhat-Maghribi S, Habbal W, Monem F. Frequency of BCR–ABL transcript types in Syrian CML patients. J Oncol. 2016;1–5. org/10.1155/2016/8420853.Suche in Google Scholar
[33] Irshad S, Butt MA, Joyia A. Frequency of different BCR–ABL fusion transcripts in chronic myelogenous leukemia patients in Pakistan. IJAVMS. 2012;6:418–23. 10.5455/ijavms.25-1344841051.Suche in Google Scholar
[34] Filho TPA, Filho PAM, Barbosa MC, Dutra LLA, Castro MF, Duarte FBA, et al. Does BCR–ABL transcript type influence the prognosis of patients in chronic myelogenous leukemia chronic phase? Hematol Transfus Cell Ther. 2019;41:114–8. org/10.1016/j.htct.2018.10.003.Suche in Google Scholar
[35] Achkar WA, Moassass F, Youssef N, Wafa A. Correlation of p210 BCR–ABL transcript variants with clinical parameters and disease outcome in 45 chronic myeloid leukemia patients. JBUON. 2016;21:444–9.Suche in Google Scholar
[36] Khazaal MS, Hamdan FB, Al‐Mayah QS. Association of BCR/ABL transcript variants with different blood parameters and demographic features in Iraqi chronic myeloid leukemia patients. Mol Genet Genomic Med. 2019;7:e809. 10.1002/mgg3.809.Suche in Google Scholar PubMed PubMed Central
[37] Jain P, Kantarjian H, Patel KP, Gonzalez GN, Luthra R, Shamanna RK, et al. Impact of BCR–ABL transcript type on outcome in patients with chronic phase CML treated with tyrosine kinase inhibitors. Blood. 2016;127:1269–75. 10.1182/blood-2015-10-674242.Suche in Google Scholar PubMed PubMed Central
[38] Polampalli S, Choughule A, Negi N, Shinde S, Baisane C, Amre P, et al. Analysis and comparison of clinicohematological parameters and molecular and cytogenetic response of two BCR/Abl fusion transcripts. Genet Mol Res. 2008;7(4):1138–49.10.4238/vol7-4gmr485Suche in Google Scholar PubMed
[39] Mondal BC, Bandyopadhyay A, Majumdar S, Mukhopadhyay A, Chandra S, Chaudhuri U, et al. Molecular profiling of chronic myeloid leukemia in Eastern India. Am J Hematol. 2006;81:845–9. 10.1002/ajh.Suche in Google Scholar
© 2021 Huma Amin and Suhaib Ahmed, published by De Gruyter
This work is licensed under the Creative Commons Attribution 4.0 International License.
Artikel in diesem Heft
- Research Articles
- Identification of ZG16B as a prognostic biomarker in breast cancer
- Behçet’s disease with latent Mycobacterium tuberculosis infection
- Erratum
- Erratum to “Suffering from Cerebral Small Vessel Disease with and without Metabolic Syndrome”
- Research Articles
- GPR37 promotes the malignancy of lung adenocarcinoma via TGF-β/Smad pathway
- Expression and role of ABIN1 in sepsis: In vitro and in vivo studies
- Additional baricitinib loading dose improves clinical outcome in COVID-19
- The co-treatment of rosuvastatin with dapagliflozin synergistically inhibited apoptosis via activating the PI3K/AKt/mTOR signaling pathway in myocardial ischemia/reperfusion injury rats
- SLC12A8 plays a key role in bladder cancer progression and EMT
- LncRNA ATXN8OS enhances tamoxifen resistance in breast cancer
- Case Report
- Serratia marcescens as a cause of unfavorable outcome in the twin pregnancy
- Spleno-adrenal fusion mimicking an adrenal metastasis of a renal cell carcinoma: A case report and embryological background
- Research Articles
- TRIM25 contributes to the malignancy of acute myeloid leukemia and is negatively regulated by microRNA-137
- CircRNA circ_0004370 promotes cell proliferation, migration, and invasion and inhibits cell apoptosis of esophageal cancer via miR-1301-3p/COL1A1 axis
- LncRNA XIST regulates atherosclerosis progression in ox-LDL-induced HUVECs
- Potential role of IFN-γ and IL-5 in sepsis prediction of preterm neonates
- Rapid Communication
- COVID-19 vaccine: Call for employees in international transportation industries and international travelers as the first priority in global distribution
- Case Report
- Rare squamous cell carcinoma of the kidney with concurrent xanthogranulomatous pyelonephritis: A case report and review of the literature
- An infertile female delivered a baby after removal of primary renal carcinoid tumor
- Research Articles
- Hypertension, BMI, and cardiovascular and cerebrovascular diseases
- Case Report
- Coexistence of bilateral macular edema and pale optic disc in the patient with Cohen syndrome
- Research Articles
- Correlation between kinematic sagittal parameters of the cervical lordosis or head posture and disc degeneration in patients with posterior neck pain
- Review Articles
- Hepatoid adenocarcinoma of the lung: An analysis of the Surveillance, Epidemiology, and End Results (SEER) database
- Research Articles
- Thermography in the diagnosis of carpal tunnel syndrome
- Pemetrexed-based first-line chemotherapy had particularly prominent objective response rate for advanced NSCLC: A network meta-analysis
- Comparison of single and double autologous stem cell transplantation in multiple myeloma patients
- The influence of smoking in minimally invasive spinal fusion surgery
- Impact of body mass index on left atrial dimension in HOCM patients
- Expression and clinical significance of CMTM1 in hepatocellular carcinoma
- miR-142-5p promotes cervical cancer progression by targeting LMX1A through Wnt/β-catenin pathway
- Comparison of multiple flatfoot indicators in 5–8-year-old children
- Early MRI imaging and follow-up study in cerebral amyloid angiopathy
- Intestinal fatty acid-binding protein as a biomarker for the diagnosis of strangulated intestinal obstruction: A meta-analysis
- miR-128-3p inhibits apoptosis and inflammation in LPS-induced sepsis by targeting TGFBR2
- Dynamic perfusion CT – A promising tool to diagnose pancreatic ductal adenocarcinoma
- Biomechanical evaluation of self-cinching stitch techniques in rotator cuff repair: The single-loop and double-loop knot stitches
- Review Articles
- The ambiguous role of mannose-binding lectin (MBL) in human immunity
- Case Report
- Membranous nephropathy with pulmonary cryptococcosis with improved 1-year follow-up results: A case report
- Fertility problems in males carrying an inversion of chromosome 10
- Acute myeloid leukemia with leukemic pleural effusion and high levels of pleural adenosine deaminase: A case report and review of literature
- Metastatic renal Ewing’s sarcoma in adult woman: Case report and review of the literature
- Burkitt-like lymphoma with 11q aberration in a patient with AIDS and a patient without AIDS: Two cases reports and literature review
- Skull hemophilia pseudotumor: A case report
- Judicious use of low-dosage corticosteroids for non-severe COVID-19: A case report
- Adult-onset citrullinaemia type II with liver cirrhosis: A rare cause of hyperammonaemia
- Clinicopathologic features of Good’s syndrome: Two cases and literature review
- Fatal immune-related hepatitis with intrahepatic cholestasis and pneumonia associated with camrelizumab: A case report and literature review
- Research Articles
- Effects of hydroxyethyl starch and gelatin on the risk of acute kidney injury following orthotopic liver transplantation: A multicenter retrospective comparative clinical study
- Significance of nucleic acid positive anal swab in COVID-19 patients
- circAPLP2 promotes colorectal cancer progression by upregulating HELLS by targeting miR-335-5p
- Ratios between circulating myeloid cells and lymphocytes are associated with mortality in severe COVID-19 patients
- Risk factors of left atrial appendage thrombus in patients with non-valvular atrial fibrillation
- Clinical features of hypertensive patients with COVID-19 compared with a normotensive group: Single-center experience in China
- Surgical myocardial revascularization outcomes in Kawasaki disease: systematic review and meta-analysis
- Decreased chromobox homologue 7 expression is associated with epithelial–mesenchymal transition and poor prognosis in cervical cancer
- FGF16 regulated by miR-520b enhances the cell proliferation of lung cancer
- Platelet-rich fibrin: Basics of biological actions and protocol modifications
- Accurate diagnosis of prostate cancer using logistic regression
- miR-377 inhibition enhances the survival of trophoblast cells via upregulation of FNDC5 in gestational diabetes mellitus
- Prognostic significance of TRIM28 expression in patients with breast carcinoma
- Integrative bioinformatics analysis of KPNA2 in six major human cancers
- Exosomal-mediated transfer of OIP5-AS1 enhanced cell chemoresistance to trastuzumab in breast cancer via up-regulating HMGB3 by sponging miR-381-3p
- A four-lncRNA signature for predicting prognosis of recurrence patients with gastric cancer
- Knockdown of circ_0003204 alleviates oxidative low-density lipoprotein-induced human umbilical vein endothelial cells injury: Circulating RNAs could explain atherosclerosis disease progression
- Propofol postpones colorectal cancer development through circ_0026344/miR-645/Akt/mTOR signal pathway
- Knockdown of lncRNA TapSAKI alleviates LPS-induced injury in HK-2 cells through the miR-205/IRF3 pathway
- COVID-19 severity in relation to sociodemographics and vitamin D use
- Clinical analysis of 11 cases of nocardiosis
- Cis-regulatory elements in conserved non-coding sequences of nuclear receptor genes indicate for crosstalk between endocrine systems
- Four long noncoding RNAs act as biomarkers in lung adenocarcinoma
- Real-world evidence of cytomegalovirus reactivation in non-Hodgkin lymphomas treated with bendamustine-containing regimens
- Relation between IL-8 level and obstructive sleep apnea syndrome
- circAGFG1 sponges miR-28-5p to promote non-small-cell lung cancer progression through modulating HIF-1α level
- Nomogram prediction model for renal anaemia in IgA nephropathy patients
- Effect of antibiotic use on the efficacy of nivolumab in the treatment of advanced/metastatic non-small cell lung cancer: A meta-analysis
- NDRG2 inhibition facilitates angiogenesis of hepatocellular carcinoma
- A nomogram for predicting metabolic steatohepatitis: The combination of NAMPT, RALGDS, GADD45B, FOSL2, RTP3, and RASD1
- Clinical and prognostic features of MMP-2 and VEGF in AEG patients
- The value of miR-510 in the prognosis and development of colon cancer
- Functional implications of PABPC1 in the development of ovarian cancer
- Prognostic value of preoperative inflammation-based predictors in patients with bladder carcinoma after radical cystectomy
- Sublingual immunotherapy increases Treg/Th17 ratio in allergic rhinitis
- Prediction of improvement after anterior cruciate ligament reconstruction
- Effluent Osteopontin levels reflect the peritoneal solute transport rate
- circ_0038467 promotes PM2.5-induced bronchial epithelial cell dysfunction
- Significance of miR-141 and miR-340 in cervical squamous cell carcinoma
- Association between hair cortisol concentration and metabolic syndrome
- Microvessel density as a prognostic indicator of prostate cancer: A systematic review and meta-analysis
- Characteristics of BCR–ABL gene variants in patients of chronic myeloid leukemia
- Knee alterations in rheumatoid arthritis: Comparison of US and MRI
- Long non-coding RNA TUG1 aggravates cerebral ischemia and reperfusion injury by sponging miR-493-3p/miR-410-3p
- lncRNA MALAT1 regulated ATAD2 to facilitate retinoblastoma progression via miR-655-3p
- Development and validation of a nomogram for predicting severity in patients with hemorrhagic fever with renal syndrome: A retrospective study
- Analysis of COVID-19 outbreak origin in China in 2019 using differentiation method for unusual epidemiological events
- Laparoscopic versus open major liver resection for hepatocellular carcinoma: A case-matched analysis of short- and long-term outcomes
- Travelers’ vaccines and their adverse events in Nara, Japan
- Association between Tfh and PGA in children with Henoch–Schönlein purpura
- Can exchange transfusion be replaced by double-LED phototherapy?
- circ_0005962 functions as an oncogene to aggravate NSCLC progression
- Circular RNA VANGL1 knockdown suppressed viability, promoted apoptosis, and increased doxorubicin sensitivity through targeting miR-145-5p to regulate SOX4 in bladder cancer cells
- Serum intact fibroblast growth factor 23 in healthy paediatric population
- Algorithm of rational approach to reconstruction in Fournier’s disease
- A meta-analysis of exosome in the treatment of spinal cord injury
- Src-1 and SP2 promote the proliferation and epithelial–mesenchymal transition of nasopharyngeal carcinoma
- Dexmedetomidine may decrease the bupivacaine toxicity to heart
- Hypoxia stimulates the migration and invasion of osteosarcoma via up-regulating the NUSAP1 expression
- Long noncoding RNA XIST knockdown relieves the injury of microglia cells after spinal cord injury by sponging miR-219-5p
- External fixation via the anterior inferior iliac spine for proximal femoral fractures in young patients
- miR-128-3p reduced acute lung injury induced by sepsis via targeting PEL12
- HAGLR promotes neuron differentiation through the miR-130a-3p-MeCP2 axis
- Phosphoglycerate mutase 2 is elevated in serum of patients with heart failure and correlates with the disease severity and patient’s prognosis
- Cell population data in identifying active tuberculosis and community-acquired pneumonia
- Prognostic value of microRNA-4521 in non-small cell lung cancer and its regulatory effect on tumor progression
- Mean platelet volume and red blood cell distribution width is associated with prognosis in premature neonates with sepsis
- 3D-printed porous scaffold promotes osteogenic differentiation of hADMSCs
- Association of gene polymorphisms with women urinary incontinence
- Influence of COVID-19 pandemic on stress levels of urologic patients
- miR-496 inhibits proliferation via LYN and AKT pathway in gastric cancer
- miR-519d downregulates LEP expression to inhibit preeclampsia development
- Comparison of single- and triple-port VATS for lung cancer: A meta-analysis
- Fluorescent light energy modulates healing in skin grafted mouse model
- Silencing CDK6-AS1 inhibits LPS-induced inflammatory damage in HK-2 cells
- Predictive effect of DCE-MRI and DWI in brain metastases from NSCLC
- Severe postoperative hyperbilirubinemia in congenital heart disease
- Baicalin improves podocyte injury in rats with diabetic nephropathy by inhibiting PI3K/Akt/mTOR signaling pathway
- Clinical factors predicting ureteral stent failure in patients with external ureteral compression
- Novel H2S donor proglumide-ADT-OH protects HUVECs from ox-LDL-induced injury through NF-κB and JAK/SATA pathway
- Triple-Endobutton and clavicular hook: A propensity score matching analysis
- Long noncoding RNA MIAT inhibits the progression of diabetic nephropathy and the activation of NF-κB pathway in high glucose-treated renal tubular epithelial cells by the miR-182-5p/GPRC5A axis
- Serum exosomal miR-122-5p, GAS, and PGR in the non-invasive diagnosis of CAG
- miR-513b-5p inhibits the proliferation and promotes apoptosis of retinoblastoma cells by targeting TRIB1
- Fer exacerbates renal fibrosis and can be targeted by miR-29c-3p
- The diagnostic and prognostic value of miR-92a in gastric cancer: A systematic review and meta-analysis
- Prognostic value of α2δ1 in hypopharyngeal carcinoma: A retrospective study
- No significant benefit of moderate-dose vitamin C on severe COVID-19 cases
- circ_0000467 promotes the proliferation, metastasis, and angiogenesis in colorectal cancer cells through regulating KLF12 expression by sponging miR-4766-5p
- Downregulation of RAB7 and Caveolin-1 increases MMP-2 activity in renal tubular epithelial cells under hypoxic conditions
- Educational program for orthopedic surgeons’ influences for osteoporosis
- Expression and function analysis of CRABP2 and FABP5, and their ratio in esophageal squamous cell carcinoma
- GJA1 promotes hepatocellular carcinoma progression by mediating TGF-β-induced activation and the epithelial–mesenchymal transition of hepatic stellate cells
- lncRNA-ZFAS1 promotes the progression of endometrial carcinoma by targeting miR-34b to regulate VEGFA expression
- Anticoagulation is the answer in treating noncritical COVID-19 patients
- Effect of late-onset hemorrhagic cystitis on PFS after haplo-PBSCT
- Comparison of Dako HercepTest and Ventana PATHWAY anti-HER2 (4B5) tests and their correlation with silver in situ hybridization in lung adenocarcinoma
- VSTM1 regulates monocyte/macrophage function via the NF-κB signaling pathway
- Comparison of vaginal birth outcomes in midwifery-led versus physician-led setting: A propensity score-matched analysis
- Treatment of osteoporosis with teriparatide: The Slovenian experience
- New targets of morphine postconditioning protection of the myocardium in ischemia/reperfusion injury: Involvement of HSP90/Akt and C5a/NF-κB
- Superenhancer–transcription factor regulatory network in malignant tumors
- β-Cell function is associated with osteosarcopenia in middle-aged and older nonobese patients with type 2 diabetes: A cross-sectional study
- Clinical features of atypical tuberculosis mimicking bacterial pneumonia
- Proteoglycan-depleted regions of annular injury promote nerve ingrowth in a rabbit disc degeneration model
- Effect of electromagnetic field on abortion: A systematic review and meta-analysis
- miR-150-5p affects AS plaque with ASMC proliferation and migration by STAT1
- MALAT1 promotes malignant pleural mesothelioma by sponging miR-141-3p
- Effects of remifentanil and propofol on distant organ lung injury in an ischemia–reperfusion model
- miR-654-5p promotes gastric cancer progression via the GPRIN1/NF-κB pathway
- Identification of LIG1 and LIG3 as prognostic biomarkers in breast cancer
- MitoQ inhibits hepatic stellate cell activation and liver fibrosis by enhancing PINK1/parkin-mediated mitophagy
- Dissecting role of founder mutation p.V727M in GNE in Indian HIBM cohort
- circATP2A2 promotes osteosarcoma progression by upregulating MYH9
- Prognostic role of oxytocin receptor in colon adenocarcinoma
- Review Articles
- The function of non-coding RNAs in idiopathic pulmonary fibrosis
- Efficacy and safety of therapeutic plasma exchange in stiff person syndrome
- Role of cesarean section in the development of neonatal gut microbiota: A systematic review
- Small cell lung cancer transformation during antitumor therapies: A systematic review
- Research progress of gut microbiota and frailty syndrome
- Recommendations for outpatient activity in COVID-19 pandemic
- Rapid Communication
- Disparity in clinical characteristics between 2019 novel coronavirus pneumonia and leptospirosis
- Use of microspheres in embolization for unruptured renal angiomyolipomas
- COVID-19 cases with delayed absorption of lung lesion
- A triple combination of treatments on moderate COVID-19
- Social networks and eating disorders during the Covid-19 pandemic
- Letter
- COVID-19, WHO guidelines, pedagogy, and respite
- Inflammatory factors in alveolar lavage fluid from severe COVID-19 pneumonia: PCT and IL-6 in epithelial lining fluid
- COVID-19: Lessons from Norway tragedy must be considered in vaccine rollout planning in least developed/developing countries
- What is the role of plasma cell in the lamina propria of terminal ileum in Good’s syndrome patient?
- Case Report
- Rivaroxaban triggered multifocal intratumoral hemorrhage of the cabozantinib-treated diffuse brain metastases: A case report and review of literature
- CTU findings of duplex kidney in kidney: A rare duplicated renal malformation
- Synchronous primary malignancy of colon cancer and mantle cell lymphoma: A case report
- Sonazoid-enhanced ultrasonography and pathologic characters of CD68 positive cell in primary hepatic perivascular epithelioid cell tumors: A case report and literature review
- Persistent SARS-CoV-2-positive over 4 months in a COVID-19 patient with CHB
- Pulmonary parenchymal involvement caused by Tropheryma whipplei
- Mediastinal mixed germ cell tumor: A case report and literature review
- Ovarian female adnexal tumor of probable Wolffian origin – Case report
- Rare paratesticular aggressive angiomyxoma mimicking an epididymal tumor in an 82-year-old man: Case report
- Perimenopausal giant hydatidiform mole complicated with preeclampsia and hyperthyroidism: A case report and literature review
- Primary orbital ganglioneuroblastoma: A case report
- Primary aortic intimal sarcoma masquerading as intramural hematoma
- Sustained false-positive results for hepatitis A virus immunoglobulin M: A case report and literature review
- Peritoneal loose body presenting as a hepatic mass: A case report and review of the literature
- Chondroblastoma of mandibular condyle: Case report and literature review
- Trauma-induced complete pacemaker lead fracture 8 months prior to hospitalization: A case report
- Primary intradural extramedullary extraosseous Ewing’s sarcoma/peripheral primitive neuroectodermal tumor (PIEES/PNET) of the thoracolumbar spine: A case report and literature review
- Computer-assisted preoperative planning of reduction of and osteosynthesis of scapular fracture: A case report
- High quality of 58-month life in lung cancer patient with brain metastases sequentially treated with gefitinib and osimertinib
- Rapid response of locally advanced oral squamous cell carcinoma to apatinib: A case report
- Retrieval of intrarenal coiled and ruptured guidewire by retrograde intrarenal surgery: A case report and literature review
- Usage of intermingled skin allografts and autografts in a senior patient with major burn injury
- Retraction
- Retraction on “Dihydromyricetin attenuates inflammation through TLR4/NF-kappa B pathway”
- Special Issue Computational Intelligence Methodologies Meets Recurrent Cancers - Part I
- An artificial immune system with bootstrap sampling for the diagnosis of recurrent endometrial cancers
- Breast cancer recurrence prediction with ensemble methods and cost-sensitive learning
Artikel in diesem Heft
- Research Articles
- Identification of ZG16B as a prognostic biomarker in breast cancer
- Behçet’s disease with latent Mycobacterium tuberculosis infection
- Erratum
- Erratum to “Suffering from Cerebral Small Vessel Disease with and without Metabolic Syndrome”
- Research Articles
- GPR37 promotes the malignancy of lung adenocarcinoma via TGF-β/Smad pathway
- Expression and role of ABIN1 in sepsis: In vitro and in vivo studies
- Additional baricitinib loading dose improves clinical outcome in COVID-19
- The co-treatment of rosuvastatin with dapagliflozin synergistically inhibited apoptosis via activating the PI3K/AKt/mTOR signaling pathway in myocardial ischemia/reperfusion injury rats
- SLC12A8 plays a key role in bladder cancer progression and EMT
- LncRNA ATXN8OS enhances tamoxifen resistance in breast cancer
- Case Report
- Serratia marcescens as a cause of unfavorable outcome in the twin pregnancy
- Spleno-adrenal fusion mimicking an adrenal metastasis of a renal cell carcinoma: A case report and embryological background
- Research Articles
- TRIM25 contributes to the malignancy of acute myeloid leukemia and is negatively regulated by microRNA-137
- CircRNA circ_0004370 promotes cell proliferation, migration, and invasion and inhibits cell apoptosis of esophageal cancer via miR-1301-3p/COL1A1 axis
- LncRNA XIST regulates atherosclerosis progression in ox-LDL-induced HUVECs
- Potential role of IFN-γ and IL-5 in sepsis prediction of preterm neonates
- Rapid Communication
- COVID-19 vaccine: Call for employees in international transportation industries and international travelers as the first priority in global distribution
- Case Report
- Rare squamous cell carcinoma of the kidney with concurrent xanthogranulomatous pyelonephritis: A case report and review of the literature
- An infertile female delivered a baby after removal of primary renal carcinoid tumor
- Research Articles
- Hypertension, BMI, and cardiovascular and cerebrovascular diseases
- Case Report
- Coexistence of bilateral macular edema and pale optic disc in the patient with Cohen syndrome
- Research Articles
- Correlation between kinematic sagittal parameters of the cervical lordosis or head posture and disc degeneration in patients with posterior neck pain
- Review Articles
- Hepatoid adenocarcinoma of the lung: An analysis of the Surveillance, Epidemiology, and End Results (SEER) database
- Research Articles
- Thermography in the diagnosis of carpal tunnel syndrome
- Pemetrexed-based first-line chemotherapy had particularly prominent objective response rate for advanced NSCLC: A network meta-analysis
- Comparison of single and double autologous stem cell transplantation in multiple myeloma patients
- The influence of smoking in minimally invasive spinal fusion surgery
- Impact of body mass index on left atrial dimension in HOCM patients
- Expression and clinical significance of CMTM1 in hepatocellular carcinoma
- miR-142-5p promotes cervical cancer progression by targeting LMX1A through Wnt/β-catenin pathway
- Comparison of multiple flatfoot indicators in 5–8-year-old children
- Early MRI imaging and follow-up study in cerebral amyloid angiopathy
- Intestinal fatty acid-binding protein as a biomarker for the diagnosis of strangulated intestinal obstruction: A meta-analysis
- miR-128-3p inhibits apoptosis and inflammation in LPS-induced sepsis by targeting TGFBR2
- Dynamic perfusion CT – A promising tool to diagnose pancreatic ductal adenocarcinoma
- Biomechanical evaluation of self-cinching stitch techniques in rotator cuff repair: The single-loop and double-loop knot stitches
- Review Articles
- The ambiguous role of mannose-binding lectin (MBL) in human immunity
- Case Report
- Membranous nephropathy with pulmonary cryptococcosis with improved 1-year follow-up results: A case report
- Fertility problems in males carrying an inversion of chromosome 10
- Acute myeloid leukemia with leukemic pleural effusion and high levels of pleural adenosine deaminase: A case report and review of literature
- Metastatic renal Ewing’s sarcoma in adult woman: Case report and review of the literature
- Burkitt-like lymphoma with 11q aberration in a patient with AIDS and a patient without AIDS: Two cases reports and literature review
- Skull hemophilia pseudotumor: A case report
- Judicious use of low-dosage corticosteroids for non-severe COVID-19: A case report
- Adult-onset citrullinaemia type II with liver cirrhosis: A rare cause of hyperammonaemia
- Clinicopathologic features of Good’s syndrome: Two cases and literature review
- Fatal immune-related hepatitis with intrahepatic cholestasis and pneumonia associated with camrelizumab: A case report and literature review
- Research Articles
- Effects of hydroxyethyl starch and gelatin on the risk of acute kidney injury following orthotopic liver transplantation: A multicenter retrospective comparative clinical study
- Significance of nucleic acid positive anal swab in COVID-19 patients
- circAPLP2 promotes colorectal cancer progression by upregulating HELLS by targeting miR-335-5p
- Ratios between circulating myeloid cells and lymphocytes are associated with mortality in severe COVID-19 patients
- Risk factors of left atrial appendage thrombus in patients with non-valvular atrial fibrillation
- Clinical features of hypertensive patients with COVID-19 compared with a normotensive group: Single-center experience in China
- Surgical myocardial revascularization outcomes in Kawasaki disease: systematic review and meta-analysis
- Decreased chromobox homologue 7 expression is associated with epithelial–mesenchymal transition and poor prognosis in cervical cancer
- FGF16 regulated by miR-520b enhances the cell proliferation of lung cancer
- Platelet-rich fibrin: Basics of biological actions and protocol modifications
- Accurate diagnosis of prostate cancer using logistic regression
- miR-377 inhibition enhances the survival of trophoblast cells via upregulation of FNDC5 in gestational diabetes mellitus
- Prognostic significance of TRIM28 expression in patients with breast carcinoma
- Integrative bioinformatics analysis of KPNA2 in six major human cancers
- Exosomal-mediated transfer of OIP5-AS1 enhanced cell chemoresistance to trastuzumab in breast cancer via up-regulating HMGB3 by sponging miR-381-3p
- A four-lncRNA signature for predicting prognosis of recurrence patients with gastric cancer
- Knockdown of circ_0003204 alleviates oxidative low-density lipoprotein-induced human umbilical vein endothelial cells injury: Circulating RNAs could explain atherosclerosis disease progression
- Propofol postpones colorectal cancer development through circ_0026344/miR-645/Akt/mTOR signal pathway
- Knockdown of lncRNA TapSAKI alleviates LPS-induced injury in HK-2 cells through the miR-205/IRF3 pathway
- COVID-19 severity in relation to sociodemographics and vitamin D use
- Clinical analysis of 11 cases of nocardiosis
- Cis-regulatory elements in conserved non-coding sequences of nuclear receptor genes indicate for crosstalk between endocrine systems
- Four long noncoding RNAs act as biomarkers in lung adenocarcinoma
- Real-world evidence of cytomegalovirus reactivation in non-Hodgkin lymphomas treated with bendamustine-containing regimens
- Relation between IL-8 level and obstructive sleep apnea syndrome
- circAGFG1 sponges miR-28-5p to promote non-small-cell lung cancer progression through modulating HIF-1α level
- Nomogram prediction model for renal anaemia in IgA nephropathy patients
- Effect of antibiotic use on the efficacy of nivolumab in the treatment of advanced/metastatic non-small cell lung cancer: A meta-analysis
- NDRG2 inhibition facilitates angiogenesis of hepatocellular carcinoma
- A nomogram for predicting metabolic steatohepatitis: The combination of NAMPT, RALGDS, GADD45B, FOSL2, RTP3, and RASD1
- Clinical and prognostic features of MMP-2 and VEGF in AEG patients
- The value of miR-510 in the prognosis and development of colon cancer
- Functional implications of PABPC1 in the development of ovarian cancer
- Prognostic value of preoperative inflammation-based predictors in patients with bladder carcinoma after radical cystectomy
- Sublingual immunotherapy increases Treg/Th17 ratio in allergic rhinitis
- Prediction of improvement after anterior cruciate ligament reconstruction
- Effluent Osteopontin levels reflect the peritoneal solute transport rate
- circ_0038467 promotes PM2.5-induced bronchial epithelial cell dysfunction
- Significance of miR-141 and miR-340 in cervical squamous cell carcinoma
- Association between hair cortisol concentration and metabolic syndrome
- Microvessel density as a prognostic indicator of prostate cancer: A systematic review and meta-analysis
- Characteristics of BCR–ABL gene variants in patients of chronic myeloid leukemia
- Knee alterations in rheumatoid arthritis: Comparison of US and MRI
- Long non-coding RNA TUG1 aggravates cerebral ischemia and reperfusion injury by sponging miR-493-3p/miR-410-3p
- lncRNA MALAT1 regulated ATAD2 to facilitate retinoblastoma progression via miR-655-3p
- Development and validation of a nomogram for predicting severity in patients with hemorrhagic fever with renal syndrome: A retrospective study
- Analysis of COVID-19 outbreak origin in China in 2019 using differentiation method for unusual epidemiological events
- Laparoscopic versus open major liver resection for hepatocellular carcinoma: A case-matched analysis of short- and long-term outcomes
- Travelers’ vaccines and their adverse events in Nara, Japan
- Association between Tfh and PGA in children with Henoch–Schönlein purpura
- Can exchange transfusion be replaced by double-LED phototherapy?
- circ_0005962 functions as an oncogene to aggravate NSCLC progression
- Circular RNA VANGL1 knockdown suppressed viability, promoted apoptosis, and increased doxorubicin sensitivity through targeting miR-145-5p to regulate SOX4 in bladder cancer cells
- Serum intact fibroblast growth factor 23 in healthy paediatric population
- Algorithm of rational approach to reconstruction in Fournier’s disease
- A meta-analysis of exosome in the treatment of spinal cord injury
- Src-1 and SP2 promote the proliferation and epithelial–mesenchymal transition of nasopharyngeal carcinoma
- Dexmedetomidine may decrease the bupivacaine toxicity to heart
- Hypoxia stimulates the migration and invasion of osteosarcoma via up-regulating the NUSAP1 expression
- Long noncoding RNA XIST knockdown relieves the injury of microglia cells after spinal cord injury by sponging miR-219-5p
- External fixation via the anterior inferior iliac spine for proximal femoral fractures in young patients
- miR-128-3p reduced acute lung injury induced by sepsis via targeting PEL12
- HAGLR promotes neuron differentiation through the miR-130a-3p-MeCP2 axis
- Phosphoglycerate mutase 2 is elevated in serum of patients with heart failure and correlates with the disease severity and patient’s prognosis
- Cell population data in identifying active tuberculosis and community-acquired pneumonia
- Prognostic value of microRNA-4521 in non-small cell lung cancer and its regulatory effect on tumor progression
- Mean platelet volume and red blood cell distribution width is associated with prognosis in premature neonates with sepsis
- 3D-printed porous scaffold promotes osteogenic differentiation of hADMSCs
- Association of gene polymorphisms with women urinary incontinence
- Influence of COVID-19 pandemic on stress levels of urologic patients
- miR-496 inhibits proliferation via LYN and AKT pathway in gastric cancer
- miR-519d downregulates LEP expression to inhibit preeclampsia development
- Comparison of single- and triple-port VATS for lung cancer: A meta-analysis
- Fluorescent light energy modulates healing in skin grafted mouse model
- Silencing CDK6-AS1 inhibits LPS-induced inflammatory damage in HK-2 cells
- Predictive effect of DCE-MRI and DWI in brain metastases from NSCLC
- Severe postoperative hyperbilirubinemia in congenital heart disease
- Baicalin improves podocyte injury in rats with diabetic nephropathy by inhibiting PI3K/Akt/mTOR signaling pathway
- Clinical factors predicting ureteral stent failure in patients with external ureteral compression
- Novel H2S donor proglumide-ADT-OH protects HUVECs from ox-LDL-induced injury through NF-κB and JAK/SATA pathway
- Triple-Endobutton and clavicular hook: A propensity score matching analysis
- Long noncoding RNA MIAT inhibits the progression of diabetic nephropathy and the activation of NF-κB pathway in high glucose-treated renal tubular epithelial cells by the miR-182-5p/GPRC5A axis
- Serum exosomal miR-122-5p, GAS, and PGR in the non-invasive diagnosis of CAG
- miR-513b-5p inhibits the proliferation and promotes apoptosis of retinoblastoma cells by targeting TRIB1
- Fer exacerbates renal fibrosis and can be targeted by miR-29c-3p
- The diagnostic and prognostic value of miR-92a in gastric cancer: A systematic review and meta-analysis
- Prognostic value of α2δ1 in hypopharyngeal carcinoma: A retrospective study
- No significant benefit of moderate-dose vitamin C on severe COVID-19 cases
- circ_0000467 promotes the proliferation, metastasis, and angiogenesis in colorectal cancer cells through regulating KLF12 expression by sponging miR-4766-5p
- Downregulation of RAB7 and Caveolin-1 increases MMP-2 activity in renal tubular epithelial cells under hypoxic conditions
- Educational program for orthopedic surgeons’ influences for osteoporosis
- Expression and function analysis of CRABP2 and FABP5, and their ratio in esophageal squamous cell carcinoma
- GJA1 promotes hepatocellular carcinoma progression by mediating TGF-β-induced activation and the epithelial–mesenchymal transition of hepatic stellate cells
- lncRNA-ZFAS1 promotes the progression of endometrial carcinoma by targeting miR-34b to regulate VEGFA expression
- Anticoagulation is the answer in treating noncritical COVID-19 patients
- Effect of late-onset hemorrhagic cystitis on PFS after haplo-PBSCT
- Comparison of Dako HercepTest and Ventana PATHWAY anti-HER2 (4B5) tests and their correlation with silver in situ hybridization in lung adenocarcinoma
- VSTM1 regulates monocyte/macrophage function via the NF-κB signaling pathway
- Comparison of vaginal birth outcomes in midwifery-led versus physician-led setting: A propensity score-matched analysis
- Treatment of osteoporosis with teriparatide: The Slovenian experience
- New targets of morphine postconditioning protection of the myocardium in ischemia/reperfusion injury: Involvement of HSP90/Akt and C5a/NF-κB
- Superenhancer–transcription factor regulatory network in malignant tumors
- β-Cell function is associated with osteosarcopenia in middle-aged and older nonobese patients with type 2 diabetes: A cross-sectional study
- Clinical features of atypical tuberculosis mimicking bacterial pneumonia
- Proteoglycan-depleted regions of annular injury promote nerve ingrowth in a rabbit disc degeneration model
- Effect of electromagnetic field on abortion: A systematic review and meta-analysis
- miR-150-5p affects AS plaque with ASMC proliferation and migration by STAT1
- MALAT1 promotes malignant pleural mesothelioma by sponging miR-141-3p
- Effects of remifentanil and propofol on distant organ lung injury in an ischemia–reperfusion model
- miR-654-5p promotes gastric cancer progression via the GPRIN1/NF-κB pathway
- Identification of LIG1 and LIG3 as prognostic biomarkers in breast cancer
- MitoQ inhibits hepatic stellate cell activation and liver fibrosis by enhancing PINK1/parkin-mediated mitophagy
- Dissecting role of founder mutation p.V727M in GNE in Indian HIBM cohort
- circATP2A2 promotes osteosarcoma progression by upregulating MYH9
- Prognostic role of oxytocin receptor in colon adenocarcinoma
- Review Articles
- The function of non-coding RNAs in idiopathic pulmonary fibrosis
- Efficacy and safety of therapeutic plasma exchange in stiff person syndrome
- Role of cesarean section in the development of neonatal gut microbiota: A systematic review
- Small cell lung cancer transformation during antitumor therapies: A systematic review
- Research progress of gut microbiota and frailty syndrome
- Recommendations for outpatient activity in COVID-19 pandemic
- Rapid Communication
- Disparity in clinical characteristics between 2019 novel coronavirus pneumonia and leptospirosis
- Use of microspheres in embolization for unruptured renal angiomyolipomas
- COVID-19 cases with delayed absorption of lung lesion
- A triple combination of treatments on moderate COVID-19
- Social networks and eating disorders during the Covid-19 pandemic
- Letter
- COVID-19, WHO guidelines, pedagogy, and respite
- Inflammatory factors in alveolar lavage fluid from severe COVID-19 pneumonia: PCT and IL-6 in epithelial lining fluid
- COVID-19: Lessons from Norway tragedy must be considered in vaccine rollout planning in least developed/developing countries
- What is the role of plasma cell in the lamina propria of terminal ileum in Good’s syndrome patient?
- Case Report
- Rivaroxaban triggered multifocal intratumoral hemorrhage of the cabozantinib-treated diffuse brain metastases: A case report and review of literature
- CTU findings of duplex kidney in kidney: A rare duplicated renal malformation
- Synchronous primary malignancy of colon cancer and mantle cell lymphoma: A case report
- Sonazoid-enhanced ultrasonography and pathologic characters of CD68 positive cell in primary hepatic perivascular epithelioid cell tumors: A case report and literature review
- Persistent SARS-CoV-2-positive over 4 months in a COVID-19 patient with CHB
- Pulmonary parenchymal involvement caused by Tropheryma whipplei
- Mediastinal mixed germ cell tumor: A case report and literature review
- Ovarian female adnexal tumor of probable Wolffian origin – Case report
- Rare paratesticular aggressive angiomyxoma mimicking an epididymal tumor in an 82-year-old man: Case report
- Perimenopausal giant hydatidiform mole complicated with preeclampsia and hyperthyroidism: A case report and literature review
- Primary orbital ganglioneuroblastoma: A case report
- Primary aortic intimal sarcoma masquerading as intramural hematoma
- Sustained false-positive results for hepatitis A virus immunoglobulin M: A case report and literature review
- Peritoneal loose body presenting as a hepatic mass: A case report and review of the literature
- Chondroblastoma of mandibular condyle: Case report and literature review
- Trauma-induced complete pacemaker lead fracture 8 months prior to hospitalization: A case report
- Primary intradural extramedullary extraosseous Ewing’s sarcoma/peripheral primitive neuroectodermal tumor (PIEES/PNET) of the thoracolumbar spine: A case report and literature review
- Computer-assisted preoperative planning of reduction of and osteosynthesis of scapular fracture: A case report
- High quality of 58-month life in lung cancer patient with brain metastases sequentially treated with gefitinib and osimertinib
- Rapid response of locally advanced oral squamous cell carcinoma to apatinib: A case report
- Retrieval of intrarenal coiled and ruptured guidewire by retrograde intrarenal surgery: A case report and literature review
- Usage of intermingled skin allografts and autografts in a senior patient with major burn injury
- Retraction
- Retraction on “Dihydromyricetin attenuates inflammation through TLR4/NF-kappa B pathway”
- Special Issue Computational Intelligence Methodologies Meets Recurrent Cancers - Part I
- An artificial immune system with bootstrap sampling for the diagnosis of recurrent endometrial cancers
- Breast cancer recurrence prediction with ensemble methods and cost-sensitive learning