Regional patterns in cause-specific mortality in Montenegro, 1991–2019
-
Đoko Raičević


Abstract
This study examines regional mortality trends in Montenegro over the past three decades (1991–2019), focusing on the three leading causes of death: circulatory diseases, neoplasms, and ill-defined conditions. Mortality data were obtained from the Statistical Office of Montenegro (MONSTAT) and the Institute of Public Health of Montenegro. Analysis was performed using crude death rate by cause of death for three regions in Montenegro. Health (doctors and hospital beds per 10,000 inhabitants) and socio-economic indicators (GINI coefficient and Human Development Index) were sourced from the World Health Organization database. A structured three-stage analytical approach was employed to investigate regional patterns and determinants of cause-specific mortality: descriptive statistics and trend analysis using linear regression, t-test, and multiple linear regression. Circulatory diseases account for the highest proportion of deaths (42%), followed by neoplasms (17%) and ill-defined causes (15%), with all other causes contributing to the remaining 25%. The analysis reveals significant and persistent regional disparities in cause-specific mortality, with south–north gradient in mortality observed for circulatory diseases and neoplasms, while ill-defined conditions displayed a reversed north–south pattern. These patterns have remained relatively stable over time. Furthermore, multiple linear regression analysis underscores the influence of health and socio-economic factors on regional mortality variation. The findings highlight the urgent need for spatially targeted public health interventions, particularly those aimed at addressing noncommunicable disease risk factors. Integrating geographic and public health approaches offers a critical pathway for reducing mortality disparities and improving population health outcomes in Montenegro.
1 Introduction
In 1971, Omran developed the theory of epidemiological transition, suggesting changes in population shifts in health and diseases. According to this theory, parallel with development and transition, the human population experienced a gradual shift from high infant mortality, low life expectancy, and mostly infectious diseases, to low infant mortality, increasing life expectancy and increasing prevalence of chronic diseases [1,2]. However, this transition has not been uniform and has manifested differently across countries and regions depending on various socio-economic, demographic, and healthcare-related factors [2].
The noncommunicable diseases (NCDs), such as cardiovascular diseases (CVDs), cancers, chronic respiratory diseases, and diabetes, have become the leading causes of death globally. According to the World Health Organization [3], NCDs are responsible for 75% of all global deaths, with CVDs alone accounting for nearly 19 million deaths annually. In Europe, NCDs account for more than 90% of total deaths, with estimation that 4.2 million people in Europe dying from CVDs in 2019, representing 42.5% of all deaths in Europe attributed to them [4,5,6]. These diseases are largely influenced by modifiable behavioral risk factors, including tobacco use, unhealthy diet, physical inactivity, and harmful use of alcohol, as well as metabolic risk factors like hypertension, hyperglycemia, and obesity [7].
Despite overall improvements in health outcomes and a general decline in age-standardized mortality rates from NCDs across Europe, profound regional disparities persist. These disparities reflect long-standing differences in health systems, economic development, population behaviors, environmental exposures, and social determinants of health.
Countries in Western and Northern Europe have experienced significant declines in premature mortality due to CVDs, due to effective prevention, early detection, and advanced treatments [8]. Conversely, countries in Eastern and Southeastern Europe continue to struggle with high NCD burdens. In fact, the gap in life expectancy between Eastern and Western Europe remains significant, largely driven by higher mortality from preventable and treatable NCDs in the East [9].
Southeastern Europe, which includes countries such as Montenegro, Serbia, Bosnia and Herzegovina, North Macedonia, Albania, and others, is particularly affected by these disparities. In this region, CVDs remain the leading cause of mortality, often occurring at younger ages and at higher rates than in the EU-15 countries. For example, age-standardized death rates from ischemic heart disease and cerebrovascular disease are considerably higher in countries like Bulgaria, Romania, and Serbia compared to Western Europe [10]. These patterns reflect not only health system weaknesses but also socio-economic vulnerabilities, behavioral risk factor prevalence, and limited access to preventive and specialized care. The burden of cancer, particularly lung, breast, and colorectal cancers, has also risen, with survival rates lagging behind those of Western Europe due to delayed diagnosis and limited treatment availability [11].
The disparities within countries are equally concerning. Regional and sub-national variations in mortality and morbidity are evident in the Southeast Europe region, reflecting differences in urbanization, income levels, education, healthcare access, and public health infrastructure. For instance, urban areas may benefit from better health services and higher health literacy, while rural and economically deprived regions often face barriers to healthcare, exacerbating health inequalities [12]. Research from across Europe has emphasized that such geographic and socioeconomic inequalities in cause-specific mortality are persistent and even widening in some cases [13,14].
Given that national-level mortality measures can obscure significant within-country disparities [15], sub-national analyses are essential for identifying and addressing vulnerable areas in population health outcomes. Montenegro offers a particularly valuable case study for examining regional patterns in cause-specific mortality. Available health statistics indicate that CVDs, cancers, and other chronic conditions are leading causes of death, but data on their regional distribution within Montenegro remain underexplored. Therefore, this study aims to analyze mortality trends across Montenegro’s regions from 1991 to 2019, focusing on the leading causes of death and exploring the relationship with health and socio-economic factors.
2 Materials and methods
2.1 Study area
The Republic of Montenegro is located in the southern part of Europe. Its land area extends between 41°50′26″ and 43°33′23″ northern latitude and 18°26′00″ and 20°21′42″ eastern longitude. According to the Census 2023, Montenegro had a population of 623,633 [16].
Analysis in this article is based on mortality trends in the three main regions in the country: northern, central, and coastal (Figure 1). These regions are defined by the National Law on regional development and are adopted in the Spatial Plan of Montenegro.[1] According to this document, the northern region comprises the following municipalities: Andrijevica, Berane, Belo Polje, Kolašin, Mojkovac, Plav, Pljevlja, Plužine, Rozaje, Savnik, Zabalj, Petnjica i Gusinje. The central region includes: Podgorica, Cetinje, Danilovgrad, Nikšic, Tuzi i Zeta. The coastal includes: Bar, Budva, Herceg-Novi, Kotor, Tivat, and Ulcinj. Each of these regions has specific demographic, socioeconomic, social, and environmental features. The central region is the most settled area with around 300,000 inhabitants, while two other regions count significantly lower numbers of population (Table 1).
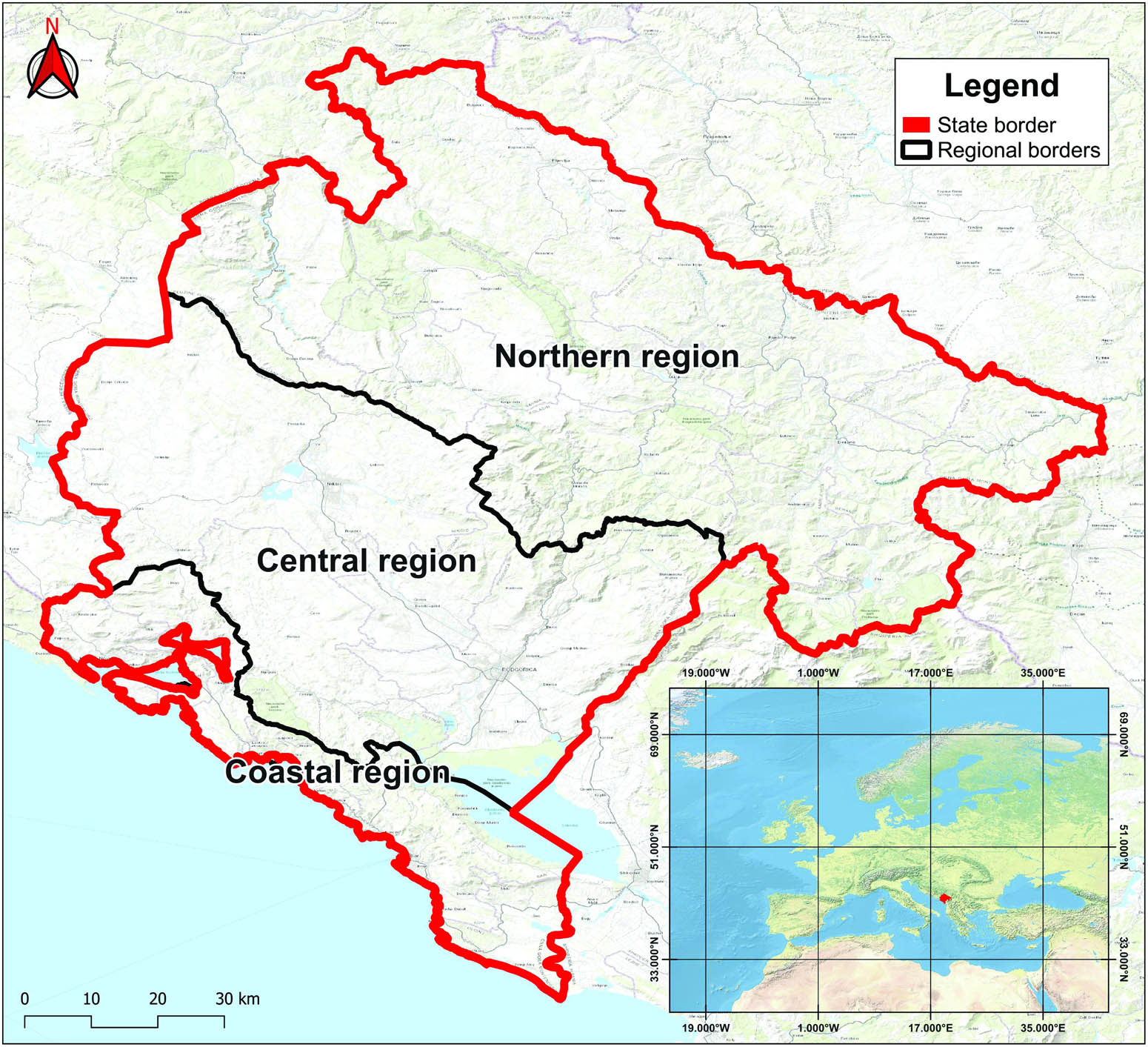
The location of Montenegro and the position of the regions (source: base map taken from https://www.arcgis.com/home/webmap/viewer.html?layers=10df2279f9684e4a9f6a7f08febac2a9, edited by the author in ArcGis).
Population and number of deaths by causes (ICD-10 codes), 1991–2019
| Region | Population in 1991 | Population in 2019 | Total number of deaths | Number of deaths by cause | |||
|---|---|---|---|---|---|---|---|
| I00–I99 | C00–D48 | R00–R99 | All other causes | ||||
| Northern | 218,592 | 163,030 | 52,025 | 21,395 | 6,917 | 10,761 | 12,952 |
| Central | 261,756 | 304,299 | 70,059 | 28,326 | 13,984 | 11,114 | 16,635 |
| Coastal | 134,841 | 154,699 | 40,015 | 19,049 | 6,725 | 2,919 | 11,322 |
Source: Statistical Office of Montenegro and Institute of Public Health of Montenegro.
2.2 Data and methods
Mortality data were obtained from the Statistical Office of Montenegro (MONSTAT) and the Institute of Public Health of Montenegro. Data were provided by cause of death, for the period 1991–2019, and the specific causes of death were coded as per the International Classification of Diseases (ICD-10). Analyses were focused on three leading causes of death: circulatory diseases (I00–I99), neoplasms (C00–D48), and ill-defined causes (R00–R99). Ill-defined diseases include causes from symptoms, signs, and abnormal clinical and laboratory findings not elsewhere classified. Analysis was performed using crude death rates by cause of death for three regions in Montenegro. The total population in each region was derived from the censuses 1991 and 2003 and an estimation for 2019 of the Statistical Office of Montenegro.
Data related to the health (doctors and hospital beds per 10,000 inhabitants) and socio-economic indicators (GINI coefficient and HDI) were obtained from the database of the World Health Organization.[2],[3],[4],[5] The GINI coefficient is an indicator used to measure income inequality within a country. A lower value of the GINI coefficient indicates a more equitable distribution of income, while a higher value suggests greater inequality. Human Development Index (HDI) is an indicator created using multiple data (life expectancy, education, and per capita income) for assessing the overall level of development in a country. Data about doctors and hospital beds were available for the period 2000–2019, while the GINI coefficient and HDI were observed for the period 2003–2015.
All data were organized in a specially designed database, and statistical analysis was conducted using STATISTICA software, version 14.1.0.8. This study employed a structured three-stage analytical approach to investigate regional patterns and determinants of cause-specific mortality in Montenegro. In the first phase, crude death rates were calculated, and descriptive statistics with trend analysis using linear regression were conducted for each region and cause of death to identify general mortality trends across the country. The second phase involved statistical testing, using the t-test to assess whether differences in mortality rates between regions were statistically significant for each specific cause of death. In the third phase, multiple linear regression analysis was performed to examine determinants of mortality patterns. The regression analysis explored the relationship between mortality rate and selected health and socio-economic indicators.
3 Results
3.1 Regional trends in cause-specific mortality
Figure 2 shows the general outlook of regional mortality trends by leading causes of death in Montenegro over the last three decades. The three main causes of death are circulatory diseases, neoplasms, and ill-defined causes. Circulatory diseases are responsible for about 42% of all deaths, neoplasms for 17%, and ill-defined causes have a share of about 15%. All other causes contributed to mortality, with approximately 25%. During the analyzed period, from 1991 to 2019, the average mortality rate from circulatory diseases was 451.6‰ in the coastal region, 387.6‰ in the northern region, and 344.1‰ in the central region. Average mortality rate from neoplasms was 168.2‰ in the central region, followed by the coastal (158.6‰) and northern (127‰) areas. And average mortality rate caused by ill-defined diseases was the highest in the northern (181.4‰) part of the country, subsequently 134.7‰ in the central region and 68.4‰ in the coastal region (Table S1).
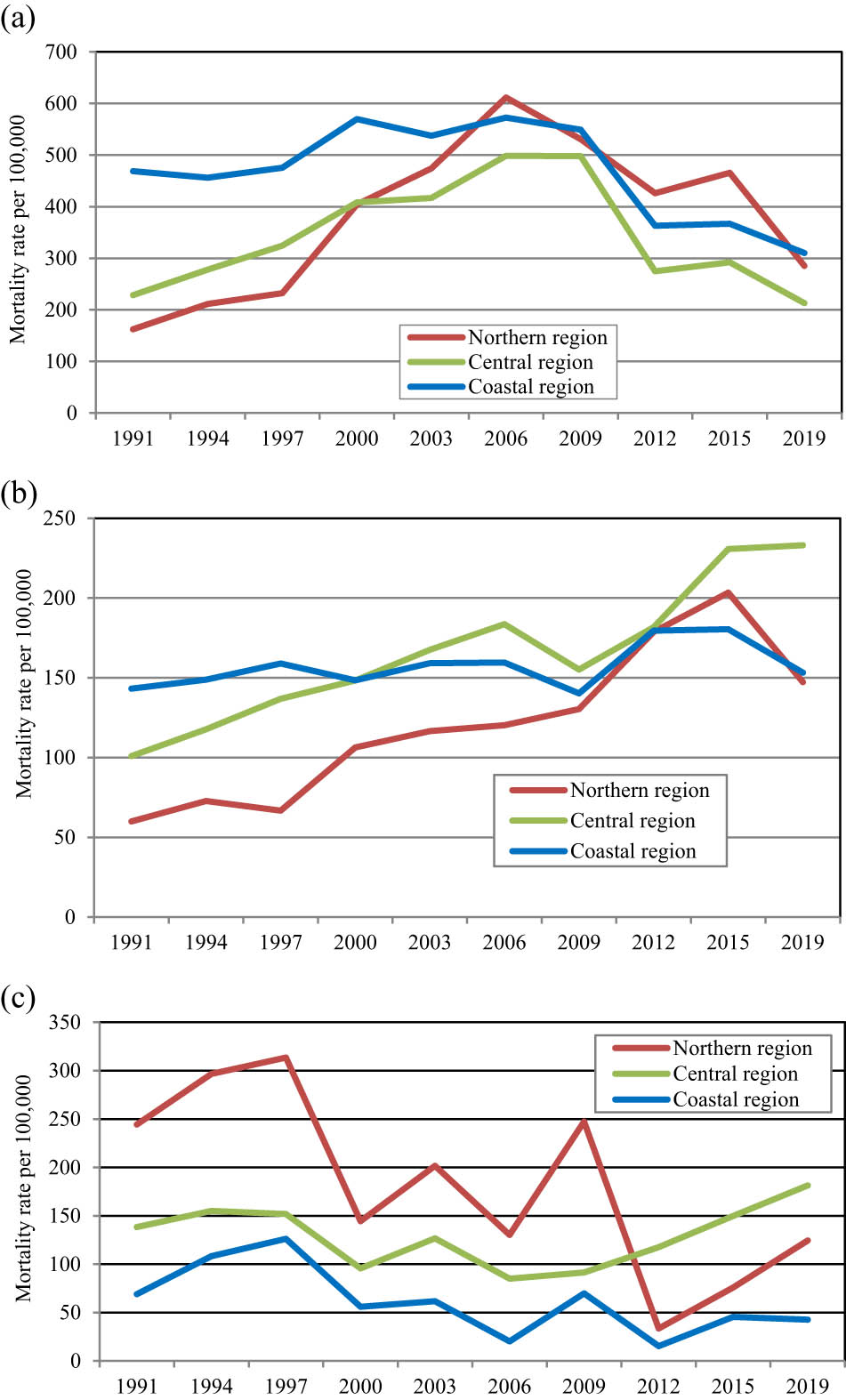
Mortality from leading causes of death by region in Montenegro, 1991–2019. (a) Circulatory diseases (I00–I99), (b) neoplasms (C00–D48), and (c) ill-defined diseases (R00–R99).
Results of trend analysis for each region and cause of death confirmed a statistically significant trend (p < 0.05), particularly for mortality caused by neoplasms. Mortality from neoplasms is rising significantly in the northern (5.3‰ per year, p = 0.0000) and central (4.4‰ per year, p = 0.0000) regions, and in the coastal area, a slight increase of 0.5‰ was confirmed, but it was not statistically significant (p = 0.156294159). Mortality from circulatory diseases is increasing in the northern region (10.2‰ per year, p = 0.000142) but decreasing in the coastal region (6.8‰, p = 0.00095), while the central region experienced a slight decline (0.26‰ per year, p = 0.902247) not statistically significant. Causes from ill-defined diseases are declining across all regions, principally in the northern area (9.6 per year, ‰, p = 0.00000), followed by the coastal (2.9‰, p = 0.00000) and central regions (1.0‰, p = 0.207549) (Table S2).
Furthermore, analysis of t-test confirmed statistically significant differences (p < 0.05) in death rates between almost all regions for each cause of death. In terms of mortality caused by circulatory diseases, the coastal region is significantly different from both northern (t = 2.07147, p = 0.04293) and central (t = 4.24479, p = 0.00008) areas, while between the central and northern regions, anaysis did not confirmed statistically significant differences (t = −1.43508, p = 0.156825). Results for mortality from neoplasms confirmed that the northern part differs significantly from both central (t = 3.49128, p = 0.00095) and coastal (t = 3.26214, p = 0.00189), while central and coastal areas are statistically similar (t = −1.17954, p = 0.243171). All regions differ significantly from each other in ill-defined causes, respectively, coastal are differs from northern (t = −5.85857, p = 0.000000) and central (t = −7.3276, p = 0.000000) region, but central and northern are also confirmed statistical differences (t = −2.4078, p = 0.019370), (Table S3).
3.2 Analysis of health and socio-economic factors associated with mortality
Mortality is known to be a highly complex demographic and public health outcome, and indicators like cause-specific mortality rates could be determined by various factors. Using regression analysis, this article explored two health (number of doctors and hospital beds per 10,000 inhabitants) and two socio-economic (GINI coefficient and HDI) risk factors. In model analysis, the mortality rate was set as the dependent variable, while doctors and hospital beds per 10,000 inhabitants, GINI coefficient, and HDI are employed as independent variables. Data for health and socio-economic indicators were limited at the country level, which may mitigate the association. Results for health indicators show that higher numbers of doctors are significantly associated with higher mortality rates from neoplasms in the central region (b = 7.21542, p = 0.000879) and lower mortality rates from circulatory diseases in the northern (b = −14.365, p = 0.020782) and coastal (b = −20.397, p = 0.008536) areas. Changes in the mortality rate caused by ill-defined diseases were not associated with the number of doctors. Data about hospital beds did not show a statistically significant relationship for any cause of death or region (Table S4). The analysis of socio-economic variables reveals a statistically significant relationship between the GINI coefficient and mortality rates only in the coastal region, where a higher GINI is associated with lower mortality rates from circulatory diseases (b = −9.93, p = 0.030344), while HDI shows varying associations across regions. In the northern region, higher HDI is significantly related to higher mortality from neoplasms (b = 1319.140, p = 0.000296), but lower mortality rates from circulatory diseases in the central (b = −2948.99, p = 0.005718) and coastal (b = −3375.11, p = 0.000558) regions, as well as lower mortality rate for ill-defined causes in the northern area (b = −2587.07, p = 0.007782) (Table S5).
4 Discussion
4.1 Leading findings
This study analyzed regional trends and patterns of specific-cause mortality in Montenegro, focusing on three leading causes of death: circulatory diseases, neoplasms, and ill-defined conditions.
Circulatory diseases remain the leading cause of death, and regarding the regional pattern, a south–north gradient was found with significant differences in mortality rate due to circulatory diseases in the coastal region compared to the central and northern areas. Similar results were confirmed for mortality caused by neoplasms with south–north pattern, while for ill-defined diseases, a reversed slope north–south has been observed.
Related regional patterns have also been identified in other countries, such as Belarus, Germany, and Ukraine, as well as in the German-speaking area of Europe (Germany, Austria, and Switzerland), where north–south, west–east, and east–west gradients have been documented [9,17,18,19,20,21]. In Belarus and Ukraine, regional analyses have particularly highlighted inequalities in mortality from CVDs and external causes, including alcohol-related and injury-related deaths [17,21]. A study focused on Ukraine reveals that differences between the Western regions compared to the eastern and southestern parts of the country are likely influenced by local socioeconomic conditions, healthcare infrastructure, and cultural factors [21].
The study by Grigoriev et al. [19] discloses that smoking is a major factor behind regional mortality differences in Germany, while avoidable mortality has primarily contributed to the north–south pattern across the German-speaking area [20].
Wider regional disparities are evident across Europe, with east–west divides. Countries in western Europe generally have lower rates due to earlier adoption of preventive strategies, better control of risk factors (like hypertension and cholesterol), and more effective healthcare systems [22].
The increasing mortality rate due to neoplasms, particularly in the northern and central regions of Montenegro, aligns with persistent disparities across Europe, too. Countries in the Eastern European area continue to experience higher cancer mortality rates compared to Western Europe, primarily due to postponed implementation of screening programs, limited access to advanced treatments, and higher prevalence of risk factors such as tobacco and alcohol consumption [23]. Although this study did not analyze neoplasms subgroups, recent findings confirm that lung cancer remains the leading cause of cancer deaths, with Eastern Europe exhibiting higher mortality rates [24]. In Montenegro, according to the Global Burden of Disease (GBD) data, lung cancer is the leading cause of neoplasm-related deaths, with tobacco use being a major contributing factor.
This study’s analysis of factors associated with mortality trends and changes in mortality rate in Montenegro included health and socio-economic variables: number of doctors and hospital beds, GINI coefficient, and HDI. A positive relationship between neoplasms mortality and the number of doctors in the central region could possibly be explained by the fact that a higher number of doctors leads to higher quality of medical services and better diagnosis and reporting [25], whereas a negative relationship between the mortality rates of circulatory diseases and doctors indicates effective medical treatment and prevention. Mortality caused by ill-defined diseases was found not to be significantly associated with the number of doctors or hospital beds. With regard to socio-economic indicators, the GINI coefficient was found to be negatively associated with mortality rates from circulatory diseases in the coastal region. Similarly, HDI showed a negative association with mortality from circulatory diseases in both the central and coastal regions. In the northern region, HDI was positively associated with mortality from neoplasms and negatively associated with mortality from ill-defined causes. This suggests that higher HDI may be related to improved diagnostic capacity, leading to better detection and classification of neoplasms. At the same time, it may contribute to a reduction in deaths attributed to ill-defined causes, reflecting progress in overall diagnostic practices. These results are driven by various demographic and economic inequalities, considering that the coastal and central areas are more urbanized with higher economic development.
Risk factors for mortality are related to any characteristics or exposures of an individual, and they can be classified into various groups. Principally, contemporary research commonly identifies behavioral (e.g., tobacco use, alcohol consumption, physical inactivity, an unhealthy diet), metabolic (e.g., high systolic blood pressure, hypertension, overweight and obesity, high blood glucose levels and high levels of fat in the blood), and environmental risk factors (e.g., air poluttion, heat, safe chemical use, water sources) as primary contributors [26,27]. Behavioral risk factors, such as tobacco use, physical inactivity, harmful alcohol consumption, and unhealthy diets, play a significant role in the burden of NCDs in Montenegro. In particular, dietary risks, including high sodium intake and low fruit consumption, were responsible for 14.2% of total mortality. Montenegro faces a particularly high burden from tobacco use too and data from 2023 reported that about 32% of people aged 15 years and older are estimated to be daily smokers, which exceeds regional and EU rates. Notably, smoking prevalence was higher among females (33.2%) than males (30.7%) [27]. Alcohol consumption is one of the most analyzed behavioral risk factors, and in 2019, alcohol usage in Montenegro has increased above the average among countries in the South-eastern European Health Network. Opposite to tobacco use, alcohol consumption was higher among males. In addition to the above, dietary behavior such as excessive sugar and salt intake was also identified as an important factor contributing to NCD burden in Montenegro [28].
The top three metabolic risk factors in the population of Montenegro are high systolic blood pressure, high body mass index, and high fasting plasma glucose. In 2021, high systolic blood pressure alone accounted for approximately 25% of all deaths [27,29]. Similar trends have been observed in Hungary (in Central Europe) and other Southeastern and Eastern European countries, including Poland, Slovakia, the Republic of Srpska (Bosnia and Herzegovina) and Litvania, where the prevalence of metabolic risk factors have been raising, reinforcing the need for targeted public health interventions [30,31,32,33,34].
Among environmental risk factors, air pollution is one of the most important issues that affect human health and the mortality of the population in Montenegro. Air quality in Montenegro is estimated as “moderately unsafe,” with high concentrations of PM2.5 particles contributing to premature deaths [35]. Central and Eastern Europe record the highest PM2.5 emissions from residential heating using solid fuels. In South-East Europe, the biomass, especially wood, is commonly used for domestic heating due to its affordability and availability, particularly in rural areas, and the reliance on outdated and inefficient heating appliances leads to substantial emissions of particulate matter (PM2.5), black carbon, and polycyclic aromatic hydrocarbons, all of which significantly degrade air quality and increase health risks [36,37].
The regional patterns of cause-specific mortality in Montenegro reflect the cumulative impact of the behavioral, metabolic, and environmental risk factors. These factors not only explain the south–north mortality gradient for circulatory diseases and neoplasms but also align Montenegro with broader East-West mortality divides observed across Europe.
Considering mortality changes in Montenegro, it is important to emphasize that, from the end of the 20th through the beginning of the 21st century, the country has undergone profound political and socio-economic transformations, which significantly influenced its demographic trends, including mortality rates. The disintegration of Yugoslavia, regional conflicts, and the transition from a socialist to a market-based economy in the 1990s led to structural shifts in the country’s economic landscape. These changes, combined with political transformations, triggered high unemployment, poverty, and reduced public services, which in turn had an impact on NCDs and mortality as well.
4.2 Study limitations
This study has some limitations that should be acknowledged. The major issue is the quality of data about causes of death, particularly related to the ill-defined conditions. Analyzing causes of death is an important diagnostic tool that can help in understanding the mechanisms of mortality change, monitoring epidemiological trends in a population, and formulating effective public health policies [38]. However, the comparability of cause-specific mortality data is often limited by the proportion of deaths attributed to ill-defined causes [39]. According to the ICD-10 codes, ill-defined causes are the symptoms, signs, and abnormal clinical and laboratory findings, not elsewhere classified. These codes refer to conditions that either cannot or should not be classified as underlying causes of death [40]. During the observed period (1991–2019) in Montenegro, ill-defined causes accounted for approximately 15% of all deaths. However, this proportion has shown substantial variation over time and across regions. The highest share of ill-defined causes was observed in the northern (22.4%) region, followed by the central (16.4%) and coastal (7.4%) areas. During the 1990s, a particular unfavorable situation was in the northern region, where ill-defined conditions accounted for more than 40% of all recorded deaths. In 1998, this share has decreased below 40%, and in 2010, has decreased below 20%. This phenomenon occurs in all classifications of death statistics globally, and the share of ill-defined causes varies largely across European countries, but without a clear regional pattern [41,42]. Depending on the proportion of ill-defined or incomplete data, cause of death statistics may lead to an underestimation of the mortality from the well-defined causes of death and cannot accurately reflect a country’s true mortality patterns, potentially hampering cross-country comparisons and leading to biased public health priorities [42]. A high share of ill-defined conditions can result from several factors, such as lack of information about the death cause or when the physician has insufficient knowledge of diseases causing death, or has not completed the death certificate adequately [41,43,44]. Existing literature suggests that ischemic heart disease or suicide, in particular, may be misclassified as ill-defined causes of death [41,45,46]. Misclassification of ischemic heart disease can occur when myocardial infarctions lead to sudden death, and when caused by cardiac arrhythmia, the underlying pathology may remain undetectable, even at autopsy [41,47].
This study’s analysis of regional mortality patterns did not account for differences by gender or other demographic characteristics (e.g., age, education level, marital status), which may have influenced the observed regional gradient. Additionally, the health (number of doctors, hospital beds) and socio-economic indicators (GINI coefficient, HDI) were only available at the national level, not for individual regions. As a result, the regression model’s findings may be limited or underestimated due to the absence of data at the subregional level.
5 Conclusion
This study highlights significant regional disparities in cause-specific mortality in Montenegro, and south–north gradient in mortality was observed for circulatory diseases and neoplasms, while ill-defined conditions displayed a reversed north–south pattern. These trends reflect the cumulative impact of behavioral, metabolic, and environmental risk factors, as well as the impact of political and socio-economic changes. Furthermore, these factors not only explain the south–north mortality gradient for circulatory diseases and neoplasms but also align Montenegro with broader east–west mortality divides observed across Europe.
Results in this study underscore the importance of targeted public health interventions, improved healthcare access, and policies aimed at reducing risk factors of NCDs. Addressing regional health inequalities in Montenegro requires a comprehensive, multisectoral approach that prioritizes prevention, strengthens health systems, and reduces socioeconomic disparities. This can be achieved through regionally tailored public health strategies that focuses on behavioral risk factors (such as reducing tobacco and alcohol use, especially in high-prevalence areas, improving dietary habits and promoting physical activity), metabolic risk factors (e.g., managing hypertension, obesity, and diabetes through primary care), and improving environmental policies to reduce pollution-related health risks.
The study’s main strength lies in its aim to position Montenegro within the Southeastern and broader European context of cause-specific mortality research, through a comprehensive, multifactorial approach and region-specific analysis. This is important not only for improving public health within the country but also for aligning Montenegro with wider European public health trends and goals.
In this study, priority was given to analyzing regions that are comparable, as health systems often differ across regions. Nonetheless, future research should go deeper into the specific causes of death that underlie these regional patterns. Particular attention should be given to risk factors such as tobacco and alcohol consumption, as well as the differential effects of urban versus rural areas.
Acknowledgments
The author Daniela Arsenović gratefully acknowledges the support of the Ministry of Science, Technological Development and Innovation of the Republic of Serbia (Grant No. 451-03-137/2025-03/200125 and No. 451-03-136/2025-03/200125).
-
Funding information: The authors state no funding involved.
-
Author contributions: Đ.R. and D.A. contributed equally to the conceptualization and design of the study. Đ.R. led the data collection and analysis, while D.A. contributed to the methodology and interpretation of the results. Both authors participated in writing the manuscript and approved the final version for publication.
-
Conflict of interest: The authors state no conflict of interest.
References
[1] Roth GA, Forouzanfar HM, Moran AE, Barber R, Nguyen G, Feigin VL, et al. Demographic and epidemiologic drivers of global cardiovascular mortality. N Engl J Med. 2015a;372(14):1333–41. 10.1056/nejmoa1406656.Search in Google Scholar
[2] Omran AR. The epidemiologic transition. A theory of the epidemiology of population change. Milbank Q. 1971;39(4):509–38. 10.2307/3349375.Search in Google Scholar
[3] World Health Organization (WHO). Noncommunicable diseases. 2024. https://www.who.int/news-room/fact-sheets/detail/noncommunicable-diseases.Search in Google Scholar
[4] Roth GA, Mensah GA, Johnson CO, Addolorato G, Ammirati E, Baddour LM, et al. Global burden of cardiovascular diseases and risk factors, 1990–2019: update from the GBD 2019 study. J Am Coll Cardiol. 2020;76(25):2982–3021. 10.1016/j.jacc.2020.11.010.Search in Google Scholar PubMed PubMed Central
[5] Timmis A, Vardas P, Townsend N, Torbica A, Katus H, De Smedt D, et al. European Society of Cardiology: cardiovascular disease statistics 2021. Eur Heart J. 2022;43(8):716–99. 10.1093/eurheartj/ehab892.Search in Google Scholar PubMed
[6] World Health Organization (WHO). Cardiovascular diseases. Key facts. 2024. https://www.who.int/europe/news-room/fact-sheets/item/cardiovascular-diseases.Search in Google Scholar
[7] Roth GA, Huffman DM, Moran AE, Feigin V, Mensah GA, Naghavi M, et al. Global and regional patterns in cardiovascular mortality from 1990 to 2013. Circulation. 2015b;132(17):1667–78. 10.1161/CIRCULATIONAHA.114.008720.Search in Google Scholar PubMed
[8] van Raalte AA, Klusener S, Oksuzyan A, Grigoriev P. Declining regional disparities in mortality in the context of persisting large inequalities in economic conditions: The case of Germany. Int J Epidemiol. 2020;49(2):486–96. 10.1093/ije/dyz265.Search in Google Scholar PubMed PubMed Central
[9] Kibele UBE, Klusener S, Scholz DR. Regional mortality disparities in Germany: Long-term dynamics and possible determinants. Köln Z Soziol. 2015;67:241–70. 10.1007/s11577-015-0329-2.Search in Google Scholar PubMed PubMed Central
[10] Eurostat. Causes of death statistics - standardised death rate. 2023. https://ec.europa.eu/eurostat/statisticsexplained/index.php? title = Causes\_of\_death\_statistics.Search in Google Scholar
[11] Vrdoljak E, Bodoky G, Jassem J, Popescu RA, Mardiak J, Pirker R, et al. Cancer control in central and eastern europe: current situation and recommendations for improvement. Oncologist. 2016;21(10):1183–90. 10.1634/theoncologist.2016-0137.Search in Google Scholar PubMed PubMed Central
[12] Baeten R, Spasova S, Vanhercke B, Coster S. Inequalities in access to healthcare. A study of national policies. Brussels: European Social Policy Network (ESPN), European Commission; 2018.Search in Google Scholar
[13] Sauerberg M, Klüsener S, Mühlichen M, Grigoriev P. Sex differences in cause-specific mortality: regional trends in seven European countries, 1996-2019. Eur J Public Health. 2023;33(6):1052–9. 10.1093/eurpub/ckad111.Search in Google Scholar PubMed PubMed Central
[14] Mackenbach JP, Rubio Valverde J, Bopp M, Bronnum-Hansen H, Costa G, Deboosere P, et al. Progress against inequalities in mortality: register-based study of 15 European countries between 1990 and 2015. Eur J Epidemiol. 2019;34:1131–42. 10.1007/s10654-019-00580-9.Search in Google Scholar PubMed PubMed Central
[15] Suulamo U, Tarkiainen L, Remes H, Martikainen P. Changes in regional variation in mortality over five decades – The contribution of age and socioeconomic population composition. SSM Popul Health. 2021;15:100850. 10.1016/j.ssmph.2021.100850.Search in Google Scholar PubMed PubMed Central
[16] Statistical Office of Montenegro (MONSTAT). Statistical yearbook. 2024, https://monstat.org/eng/novosti.php?id=4064.Search in Google Scholar
[17] Grigoriev P, Doblhammer-Reiter G, Shkolnikov V. Trends, patterns, and determinants of regional mortality in Belarus, 1990-2007. Popul Stud. 2013;67(1):61–81. 10.1080/00324728.2012.724696.Search in Google Scholar PubMed PubMed Central
[18] Grigoriev P, Pechholdova M. Health convergence between East and West Germany as reflected in long-term cause-specific mortality trends: To what extent was it due to reunification? Eur J Popul. 2017;33:701–31. 10.1007/s10680-017-9455-z.Search in Google Scholar PubMed PubMed Central
[19] Grigoriev P, Klüsener S, van Raalte A. Quantifying the contribution of smoking to regional mortality disparities in Germany: a cross-sectional study. BMJ Open. 2022;12:e064249. 10.1136/bmjopen-2022-064249.Search in Google Scholar PubMed PubMed Central
[20] Mühlichen M, Lerch M, Sauerberg M, Grigoriev P. Different health systems - Different mortality outcomes? Regional disparities in avoidable mortality across German-speaking Europe, 1992-2019. Soc Sci Med. 2023;329:115976. 10.1016/j.socscimed.2023.115976.Search in Google Scholar PubMed PubMed Central
[21] Grigoriev P, Levchuk N, Shevchuk P, Poniakina S, Klüsener S. Spatial disparities in cause-specific mortality in Ukraine: A district-level analysis, 2006–19. Popul Stud. 2024;79(2):1–22. 10.1080/00324728.2024.2371283.Search in Google Scholar PubMed
[22] Muller-Nordhorn J, Binting S, Roll S, Willich SN. An update on regional variation in cardiovascular mortality within Europe. Eur Heart J. 2008;29:1316–26. 10.1093/eurheartj/ehm604.Search in Google Scholar PubMed
[23] Santucci C, Patel L, Malvezzi M, Wojtyla C, La Vecchia C, Negri E, et al. Persisting cancer mortality gap between Western and Eastern Europe. Eur J Cancer. 2022;165:1–12. 10.1016/j.ejca.2022.01.007.Search in Google Scholar PubMed
[24] Elmadani M, Mokaya PO, Omer AAA, Kiptulon EK, Klara S, Orsolya M. Cancer burden in Europe: a systematic analysis of the GLOBOCAN database (2022). BMC Cancer. 2025;25:447. 10.1186/s12885-025-13862-1.Search in Google Scholar PubMed PubMed Central
[25] OECD/European Commission. Health at a Glance: Europe 2022 – State of Health in the EU Cycle. Paris: OECD Publishing; 2022.Search in Google Scholar
[26] Mubarik S, Luo L, Naeem S, Mubarak R, Iqbal M, Hak E, et al. Epidemiology and demographic patterns of cardiovascular diseases and neoplasms deaths in Western Europe: a 1990–2019 analysis. Public Health. 2024;221:187–97. 10.1016/j.puhe.2024.04.003.Search in Google Scholar PubMed
[27] Mosca I, Tille F. Health Systems in Action (HSiA) Insights – Montenegro. Copenhagen: WHO Regional Office for Europe; 2025.Search in Google Scholar
[28] D’Elia L, Brajović M, Klisic A, Breda J, Jewell J, Cadjenović V, et al. Sodium and potassium intake, knowledge attitudes and behaviour towards salt consumption amongst adults in Podgorica, Montenegro. Nutrients. 2019;11(1):160. 10.3390/nu11010160.Search in Google Scholar PubMed PubMed Central
[29] World Health Organization (WHO). WHO European Primary Health Care Impact, Performance and Capacity Tool (PHC-IMPACT). Copenhagen, Montenegro: WHO; 2020.Search in Google Scholar
[30] Luksiene DI, Baceviciene M, Tamosiunas A. Population-based study in Lithuania: lifestyle factors and risk of metabolic syndrome. Cent Eur J Med. 2010;5:387–98. 10.2478/s11536-010-0007-8.Search in Google Scholar
[31] Low R, Regulska-Ilow B, Różańska D, Kowalisko A, Biernat J. Prevalence of metabolic syndrome among 40- and 50-year-old inhabitants of Wroclaw, Poland. Ann Agric Environ Med. 2012;19(3):551–6.Search in Google Scholar
[32] Ostrihonova T, Rimarova K, Beresova J, Kontrosova S, Dorko E, Diabelkova J. Prevalence and trends of metabolic syndrome in clients of Health Advice Centres during the years 2003–2012. Cent Eur J Public Health. 2017;25(4):313–20. 10.21101/cejph.a4968.Search in Google Scholar PubMed
[33] Piko P, Dioszegi J, Sandor J, Adany R. Changes in the prevalence of metabolic syndrome and its components as well as in relevant preventive medication between 2006 and 2018 in the Northeast Hungarian population. J Pers Med. 2021;11(1):52. 10.3390/jpm11010052.Search in Google Scholar PubMed PubMed Central
[34] Majić A, Arsenović D, Čvokić DD. Behavioral and metabolic risk factors for noncommunicable diseases among population in the Republic of Srpska (Bosnia and Herzegovina. Healthcare. 2023;11(4):483. 10.3390/healthcare11040483.Search in Google Scholar PubMed PubMed Central
[35] European Environment Agency (EEA). Air quality in Europe: 2020 report. Copenhagen: EEA; 2021. https://www.eea.europa.eu/publications/air-quality-in-europe-2020-report.Search in Google Scholar
[36] Li Q, Jiang J, Wang S, Rumchev K, Mead-Hunter R, Morawska L, et al. Impacts of household coal and biomass combustion on indoor and ambient air quality in China: current status and implication. Sci Total Environ. 2017;576:347–61. 10.1016/j.scitotenv.2016.10.080.Search in Google Scholar PubMed
[37] Belis CA, Pisoni E, Degraeuwe B, Peduzzi E, Thunis P, Monforti-Ferrario F, et al. Urban pollution in the Danube and Western Balkans regions: The impact of major PM2.5 sources. Environ Int. 2019;133(Part A):105158. 10.1016/j.envint.2019.105158.Search in Google Scholar PubMed PubMed Central
[38] Danilova I, Rau R, Barbieri M, Grigoriev P, Jdanov DA, Meslé F, et al. Subnational consistency in cause-of-death data: the cases of Russia, Germany, the United States, and France. Population. 2021;76(4):645–74. 10.3917/popu.2104.0693.Search in Google Scholar
[39] Grigoriev P, Bonnet F, Perdrix E. Method for redistributing ill-defined causes of death. Popul Stud. 2025;79(1):187–97. 10.1080/00324728.2024.2332629.Search in Google Scholar PubMed PubMed Central
[40] World Health Organization (WHO). International statistical classification of diseases and related health problems, 10th revision. Instruction manual. Vol. 2, 5th edn. Geneva: WHO; 2016.Search in Google Scholar
[41] Kulhanova I, Menviell G, Bopp M, Borrell C, Deboosere P, Eikemo AT, et al. Socioeconomic differences in the use of ill-defined causes of death in 16 European countries. BMC Public Health. 2014;14:1295. 10.1186/1471-2458-14-1295.Search in Google Scholar PubMed PubMed Central
[42] Wengler A, Gruhl H, Plaß D, Leddin J, Rommel A, von der Lippe E, et al. Redistributing ill-defined causes of death – A case study from the BURDEN 2020 project in Germany. Arch Public Health. 2021;79:33. 10.1186/s13690-021-00535-1.Search in Google Scholar PubMed PubMed Central
[43] D’Amico M, Agozzino E, Biagino A, Simonetti A, Marinelli P. Ill-defined and multiple causes on death certificates – A study of misclassification in mortality statistics. Eur J Epidemiol. 1999;15(2):141–8. 10.1023/a:1007570405888.Search in Google Scholar PubMed
[44] Ukolova E. A comparative analysis of regional mortality differences using underlying and multiple causes of death: a case study of Czechia. Spat Demogr. 2024;12:8. 10.1007/s40980-024-00130-2.Search in Google Scholar
[45] Armstrong DL, Wing SB, Tyroler HA. United States mortality from ill-defined causes, 1968–1988: potential effects on heart disease mortality trends. Int J Epidemiol. 1995;24(3):522–7. 10.1093/ije/24.3.522.Search in Google Scholar PubMed
[46] Snowdon J, Choi NG. Undercounting of suicides: Where suicide data lie hidden. Glob Public Health. 2020;15(12):1894–901. 10.1080/17441692.2020.1801789.Search in Google Scholar PubMed
[47] Rockett IR, Wang S, Stack S, De Leo D, Frost LJ, Ducatman MA, et al. Race/ethnicity and potential suicide misclassification: Window on a minority suicide paradox? BMC Psychiatry. 2010;10:35. 10.1186/1471-244X-10-35.Search in Google Scholar PubMed PubMed Central
© 2025 the author(s), published by De Gruyter
This work is licensed under the Creative Commons Attribution 4.0 International License.
Articles in the same Issue
- Ionization hotspots near waterfalls in Eastern Serbia’s Stara Planina Mountain
- Research Articles
- Seismic response and damage model analysis of rocky slopes with weak interlayers
- Multi-scenario simulation and eco-environmental effect analysis of “Production–Living–Ecological space” based on PLUS model: A case study of Anyang City
- Remote sensing estimation of chlorophyll content in rape leaves in Weibei dryland region of China
- GIS-based frequency ratio and Shannon entropy modeling for landslide susceptibility mapping: A case study in Kundah Taluk, Nilgiris District, India
- Natural gas origin and accumulation of the Changxing–Feixianguan Formation in the Puguang area, China
- Spatial variations of shear-wave velocity anomaly derived from Love wave ambient noise seismic tomography along Lembang Fault (West Java, Indonesia)
- Evaluation of cumulative rainfall and rainfall event–duration threshold based on triggering and non-triggering rainfalls: Northern Thailand case
- Pixel and region-oriented classification of Sentinel-2 imagery to assess LULC dynamics and their climate impact in Nowshera, Pakistan
- The use of radar-optical remote sensing data and geographic information system–analytical hierarchy process–multicriteria decision analysis techniques for revealing groundwater recharge prospective zones in arid-semi arid lands
- Effect of pore throats on the reservoir quality of tight sandstone: A case study of the Yanchang Formation in the Zhidan area, Ordos Basin
- Hydroelectric simulation of the phreatic water response of mining cracked soil based on microbial solidification
- Spatial-temporal evolution of habitat quality in tropical monsoon climate region based on “pattern–process–quality” – a case study of Cambodia
- Early Permian to Middle Triassic Formation petroleum potentials of Sydney Basin, Australia: A geochemical analysis
- Micro-mechanism analysis of Zhongchuan loess liquefaction disaster induced by Jishishan M6.2 earthquake in 2023
- Prediction method of S-wave velocities in tight sandstone reservoirs – a case study of CO2 geological storage area in Ordos Basin
- Ecological restoration in valley area of semiarid region damaged by shallow buried coal seam mining
- Hydrocarbon-generating characteristics of Xujiahe coal-bearing source rocks in the continuous sedimentary environment of the Southwest Sichuan
- Hazard analysis of future surface displacements on active faults based on the recurrence interval of strong earthquakes
- Structural characterization of the Zalm district, West Saudi Arabia, using aeromagnetic data: An approach for gold mineral exploration
- Research on the variation in the Shields curve of silt initiation
- Reuse of agricultural drainage water and wastewater for crop irrigation in southeastern Algeria
- Assessing the effectiveness of utilizing low-cost inertial measurement unit sensors for producing as-built plans
- Analysis of the formation process of a natural fertilizer in the loess area
- Machine learning methods for landslide mapping studies: A comparative study of SVM and RF algorithms in the Oued Aoulai watershed (Morocco)
- Chemical dissolution and the source of salt efflorescence in weathering of sandstone cultural relics
- Molecular simulation of methane adsorption capacity in transitional shale – a case study of Longtan Formation shale in Southern Sichuan Basin, SW China
- Evolution characteristics of extreme maximum temperature events in Central China and adaptation strategies under different future warming scenarios
- Estimating Bowen ratio in local environment based on satellite imagery
- 3D fusion modeling of multi-scale geological structures based on subdivision-NURBS surfaces and stratigraphic sequence formalization
- Comparative analysis of machine learning algorithms in Google Earth Engine for urban land use dynamics in rapidly urbanizing South Asian cities
- Study on the mechanism of plant root influence on soil properties in expansive soil areas
- Simulation of seismic hazard parameters and earthquakes source mechanisms along the Red Sea rift, western Saudi Arabia
- Tectonics vs sedimentation in foredeep basins: A tale from the Oligo-Miocene Monte Falterona Formation (Northern Apennines, Italy)
- Investigation of landslide areas in Tokat-Almus road between Bakımlı-Almus by the PS-InSAR method (Türkiye)
- Predicting coastal variations in non-storm conditions with machine learning
- Cross-dimensional adaptivity research on a 3D earth observation data cube model
- Geochronology and geochemistry of late Paleozoic volcanic rocks in eastern Inner Mongolia and their geological significance
- Spatial and temporal evolution of land use and habitat quality in arid regions – a case of Northwest China
- Ground-penetrating radar imaging of subsurface karst features controlling water leakage across Wadi Namar dam, south Riyadh, Saudi Arabia
- Rayleigh wave dispersion inversion via modified sine cosine algorithm: Application to Hangzhou, China passive surface wave data
- Fractal insights into permeability control by pore structure in tight sandstone reservoirs, Heshui area, Ordos Basin
- Debris flow hazard characteristic and mitigation in Yusitong Gully, Hengduan Mountainous Region
- Research on community characteristics of vegetation restoration in hilly power engineering based on multi temporal remote sensing technology
- Identification of radial drainage networks based on topographic and geometric features
- Trace elements and melt inclusion in zircon within the Qunji porphyry Cu deposit: Application to the metallogenic potential of the reduced magma-hydrothermal system
- Pore, fracture characteristics and diagenetic evolution of medium-maturity marine shales from the Silurian Longmaxi Formation, NE Sichuan Basin, China
- Study of the earthquakes source parameters, site response, and path attenuation using P and S-waves spectral inversion, Aswan region, south Egypt
- Source of contamination and assessment of potential health risks of potentially toxic metal(loid)s in agricultural soil from Al Lith, Saudi Arabia
- Regional spatiotemporal evolution and influencing factors of rural construction areas in the Nanxi River Basin via GIS
- An efficient network for object detection in scale-imbalanced remote sensing images
- Effect of microscopic pore–throat structure heterogeneity on waterflooding seepage characteristics of tight sandstone reservoirs
- Environmental health risk assessment of Zn, Cd, Pb, Fe, and Co in coastal sediments of the southeastern Gulf of Aqaba
- A modified Hoek–Brown model considering softening effects and its applications
- Evaluation of engineering properties of soil for sustainable urban development
- The spatio-temporal characteristics and influencing factors of sustainable development in China’s provincial areas
- Application of a mixed additive and multiplicative random error model to generate DTM products from LiDAR data
- Gold vein mineralogy and oxygen isotopes of Wadi Abu Khusheiba, Jordan
- Prediction of surface deformation time series in closed mines based on LSTM and optimization algorithms
- 2D–3D Geological features collaborative identification of surrounding rock structural planes in hydraulic adit based on OC-AINet
- Spatiotemporal patterns and drivers of Chl-a in Chinese lakes between 1986 and 2023
- Land use classification through fusion of remote sensing images and multi-source data
- Nexus between renewable energy, technological innovation, and carbon dioxide emissions in Saudi Arabia
- Analysis of the spillover effects of green organic transformation on sustainable development in ethnic regions’ agriculture and animal husbandry
- Factors impacting spatial distribution of black and odorous water bodies in Hebei
- Large-scale shaking table tests on the liquefaction and deformation responses of an ultra-deep overburden
- Impacts of climate change and sea-level rise on the coastal geological environment of Quang Nam province, Vietnam
- Reservoir characterization and exploration potential of shale reservoir near denudation area: A case study of Ordovician–Silurian marine shale, China
- Seismic prediction of Permian volcanic rock reservoirs in Southwest Sichuan Basin
- Application of CBERS-04 IRS data to land surface temperature inversion: A case study based on Minqin arid area
- Geological characteristics and prospecting direction of Sanjiaoding gold mine in Saishiteng area
- Research on the deformation prediction model of surrounding rock based on SSA-VMD-GRU
- Geochronology, geochemical characteristics, and tectonic significance of the granites, Menghewula, Southern Great Xing’an range
- Hazard classification of active faults in Yunnan base on probabilistic seismic hazard assessment
- Characteristics analysis of hydrate reservoirs with different geological structures developed by vertical well depressurization
- Estimating the travel distance of channelized rock avalanches using genetic programming method
- Landscape preferences of hikers in Three Parallel Rivers Region and its adjacent regions by content analysis of user-generated photography
- New age constraints of the LGM onset in the Bohemian Forest – Central Europe
- Characteristics of geological evolution based on the multifractal singularity theory: A case study of Heyu granite and Mesozoic tectonics
- Soil water content and longitudinal microbiota distribution in disturbed areas of tower foundations of power transmission and transformation projects
- Oil accumulation process of the Kongdian reservoir in the deep subsag zone of the Cangdong Sag, Bohai Bay Basin, China
- Investigation of velocity profile in rock–ice avalanche by particle image velocimetry measurement
- Optimizing 3D seismic survey geometries using ray tracing and illumination modeling: A case study from Penobscot field
- Sedimentology of the Phra That and Pha Daeng Formations: A preliminary evaluation of geological CO2 storage potential in the Lampang Basin, Thailand
- Improved classification algorithm for hyperspectral remote sensing images based on the hybrid spectral network model
- Map analysis of soil erodibility rates and gully erosion sites in Anambra State, South Eastern Nigeria
- Identification and driving mechanism of land use conflict in China’s South-North transition zone: A case study of Huaihe River Basin
- Evaluation of the impact of land-use change on earthquake risk distribution in different periods: An empirical analysis from Sichuan Province
- A test site case study on the long-term behavior of geotextile tubes
- An experimental investigation into carbon dioxide flooding and rock dissolution in low-permeability reservoirs of the South China Sea
- Detection and semi-quantitative analysis of naphthenic acids in coal and gangue from mining areas in China
- Comparative effects of olivine and sand on KOH-treated clayey soil
- YOLO-MC: An algorithm for early forest fire recognition based on drone image
- Earthquake building damage classification based on full suite of Sentinel-1 features
- Potential landslide detection and influencing factors analysis in the upper Yellow River based on SBAS-InSAR technology
- Assessing green area changes in Najran City, Saudi Arabia (2013–2022) using hybrid deep learning techniques
- An advanced approach integrating methods to estimate hydraulic conductivity of different soil types supported by a machine learning model
- Hybrid methods for land use and land cover classification using remote sensing and combined spectral feature extraction: A case study of Najran City, KSA
- Streamlining digital elevation model construction from historical aerial photographs: The impact of reference elevation data on spatial accuracy
- Analysis of urban expansion patterns in the Yangtze River Delta based on the fusion impervious surfaces dataset
- A metaverse-based visual analysis approach for 3D reservoir models
- Late Quaternary record of 100 ka depositional cycles on the Larache shelf (NW Morocco)
- Integrated well-seismic analysis of sedimentary facies distribution: A case study from the Mesoproterozoic, Ordos Basin, China
- Study on the spatial equilibrium of cultural and tourism resources in Macao, China
- Urban road surface condition detecting and integrating based on the mobile sensing framework with multi-modal sensors
- Review Articles
- Humic substances influence on the distribution of dissolved iron in seawater: A review of electrochemical methods and other techniques
- Applications of physics-informed neural networks in geosciences: From basic seismology to comprehensive environmental studies
- Ore-controlling structures of granite-related uranium deposits in South China: A review
- Shallow geological structure features in Balikpapan Bay East Kalimantan Province – Indonesia
- A review on the tectonic affinity of microcontinents and evolution of the Proto-Tethys Ocean in Northeastern Tibet
- Special Issue: Natural Resources and Environmental Risks: Towards a Sustainable Future - Part II
- Depopulation in the Visok micro-region: Toward demographic and economic revitalization
- Special Issue: Geospatial and Environmental Dynamics - Part II
- Advancing urban sustainability: Applying GIS technologies to assess SDG indicators – a case study of Podgorica (Montenegro)
- Spatiotemporal and trend analysis of common cancers in men in Central Serbia (1999–2021)
- Minerals for the green agenda, implications, stalemates, and alternatives
- Spatiotemporal water quality analysis of Vrana Lake, Croatia
- Functional transformation of settlements in coal exploitation zones: A case study of the municipality of Stanari in Republic of Srpska (Bosnia and Herzegovina)
- Hypertension in AP Vojvodina (Northern Serbia): A spatio-temporal analysis of patients at the Institute for Cardiovascular Diseases of Vojvodina
- Regional patterns in cause-specific mortality in Montenegro, 1991–2019
- Spatio-temporal analysis of flood events using GIS and remote sensing-based approach in the Ukrina River Basin, Bosnia and Herzegovina
- Flash flood susceptibility mapping using LiDAR-Derived DEM and machine learning algorithms: Ljuboviđa case study, Serbia
- Geocultural heritage as a basis for geotourism development: Banjska Monastery, Zvečan (Serbia)
- Assessment of groundwater potential zones using GIS and AHP techniques – A case study of the zone of influence of Kolubara Mining Basin
- Impact of the agri-geographical transformation of rural settlements on the geospatial dynamics of soil erosion intensity in municipalities of Central Serbia
- Where faith meets geomorphology: The cultural and religious significance of geodiversity explored through geospatial technologies
- Applications of local climate zone classification in European cities: A review of in situ and mobile monitoring methods in urban climate studies
- Complex multivariate water quality impact assessment on Krivaja River
Articles in the same Issue
- Ionization hotspots near waterfalls in Eastern Serbia’s Stara Planina Mountain
- Research Articles
- Seismic response and damage model analysis of rocky slopes with weak interlayers
- Multi-scenario simulation and eco-environmental effect analysis of “Production–Living–Ecological space” based on PLUS model: A case study of Anyang City
- Remote sensing estimation of chlorophyll content in rape leaves in Weibei dryland region of China
- GIS-based frequency ratio and Shannon entropy modeling for landslide susceptibility mapping: A case study in Kundah Taluk, Nilgiris District, India
- Natural gas origin and accumulation of the Changxing–Feixianguan Formation in the Puguang area, China
- Spatial variations of shear-wave velocity anomaly derived from Love wave ambient noise seismic tomography along Lembang Fault (West Java, Indonesia)
- Evaluation of cumulative rainfall and rainfall event–duration threshold based on triggering and non-triggering rainfalls: Northern Thailand case
- Pixel and region-oriented classification of Sentinel-2 imagery to assess LULC dynamics and their climate impact in Nowshera, Pakistan
- The use of radar-optical remote sensing data and geographic information system–analytical hierarchy process–multicriteria decision analysis techniques for revealing groundwater recharge prospective zones in arid-semi arid lands
- Effect of pore throats on the reservoir quality of tight sandstone: A case study of the Yanchang Formation in the Zhidan area, Ordos Basin
- Hydroelectric simulation of the phreatic water response of mining cracked soil based on microbial solidification
- Spatial-temporal evolution of habitat quality in tropical monsoon climate region based on “pattern–process–quality” – a case study of Cambodia
- Early Permian to Middle Triassic Formation petroleum potentials of Sydney Basin, Australia: A geochemical analysis
- Micro-mechanism analysis of Zhongchuan loess liquefaction disaster induced by Jishishan M6.2 earthquake in 2023
- Prediction method of S-wave velocities in tight sandstone reservoirs – a case study of CO2 geological storage area in Ordos Basin
- Ecological restoration in valley area of semiarid region damaged by shallow buried coal seam mining
- Hydrocarbon-generating characteristics of Xujiahe coal-bearing source rocks in the continuous sedimentary environment of the Southwest Sichuan
- Hazard analysis of future surface displacements on active faults based on the recurrence interval of strong earthquakes
- Structural characterization of the Zalm district, West Saudi Arabia, using aeromagnetic data: An approach for gold mineral exploration
- Research on the variation in the Shields curve of silt initiation
- Reuse of agricultural drainage water and wastewater for crop irrigation in southeastern Algeria
- Assessing the effectiveness of utilizing low-cost inertial measurement unit sensors for producing as-built plans
- Analysis of the formation process of a natural fertilizer in the loess area
- Machine learning methods for landslide mapping studies: A comparative study of SVM and RF algorithms in the Oued Aoulai watershed (Morocco)
- Chemical dissolution and the source of salt efflorescence in weathering of sandstone cultural relics
- Molecular simulation of methane adsorption capacity in transitional shale – a case study of Longtan Formation shale in Southern Sichuan Basin, SW China
- Evolution characteristics of extreme maximum temperature events in Central China and adaptation strategies under different future warming scenarios
- Estimating Bowen ratio in local environment based on satellite imagery
- 3D fusion modeling of multi-scale geological structures based on subdivision-NURBS surfaces and stratigraphic sequence formalization
- Comparative analysis of machine learning algorithms in Google Earth Engine for urban land use dynamics in rapidly urbanizing South Asian cities
- Study on the mechanism of plant root influence on soil properties in expansive soil areas
- Simulation of seismic hazard parameters and earthquakes source mechanisms along the Red Sea rift, western Saudi Arabia
- Tectonics vs sedimentation in foredeep basins: A tale from the Oligo-Miocene Monte Falterona Formation (Northern Apennines, Italy)
- Investigation of landslide areas in Tokat-Almus road between Bakımlı-Almus by the PS-InSAR method (Türkiye)
- Predicting coastal variations in non-storm conditions with machine learning
- Cross-dimensional adaptivity research on a 3D earth observation data cube model
- Geochronology and geochemistry of late Paleozoic volcanic rocks in eastern Inner Mongolia and their geological significance
- Spatial and temporal evolution of land use and habitat quality in arid regions – a case of Northwest China
- Ground-penetrating radar imaging of subsurface karst features controlling water leakage across Wadi Namar dam, south Riyadh, Saudi Arabia
- Rayleigh wave dispersion inversion via modified sine cosine algorithm: Application to Hangzhou, China passive surface wave data
- Fractal insights into permeability control by pore structure in tight sandstone reservoirs, Heshui area, Ordos Basin
- Debris flow hazard characteristic and mitigation in Yusitong Gully, Hengduan Mountainous Region
- Research on community characteristics of vegetation restoration in hilly power engineering based on multi temporal remote sensing technology
- Identification of radial drainage networks based on topographic and geometric features
- Trace elements and melt inclusion in zircon within the Qunji porphyry Cu deposit: Application to the metallogenic potential of the reduced magma-hydrothermal system
- Pore, fracture characteristics and diagenetic evolution of medium-maturity marine shales from the Silurian Longmaxi Formation, NE Sichuan Basin, China
- Study of the earthquakes source parameters, site response, and path attenuation using P and S-waves spectral inversion, Aswan region, south Egypt
- Source of contamination and assessment of potential health risks of potentially toxic metal(loid)s in agricultural soil from Al Lith, Saudi Arabia
- Regional spatiotemporal evolution and influencing factors of rural construction areas in the Nanxi River Basin via GIS
- An efficient network for object detection in scale-imbalanced remote sensing images
- Effect of microscopic pore–throat structure heterogeneity on waterflooding seepage characteristics of tight sandstone reservoirs
- Environmental health risk assessment of Zn, Cd, Pb, Fe, and Co in coastal sediments of the southeastern Gulf of Aqaba
- A modified Hoek–Brown model considering softening effects and its applications
- Evaluation of engineering properties of soil for sustainable urban development
- The spatio-temporal characteristics and influencing factors of sustainable development in China’s provincial areas
- Application of a mixed additive and multiplicative random error model to generate DTM products from LiDAR data
- Gold vein mineralogy and oxygen isotopes of Wadi Abu Khusheiba, Jordan
- Prediction of surface deformation time series in closed mines based on LSTM and optimization algorithms
- 2D–3D Geological features collaborative identification of surrounding rock structural planes in hydraulic adit based on OC-AINet
- Spatiotemporal patterns and drivers of Chl-a in Chinese lakes between 1986 and 2023
- Land use classification through fusion of remote sensing images and multi-source data
- Nexus between renewable energy, technological innovation, and carbon dioxide emissions in Saudi Arabia
- Analysis of the spillover effects of green organic transformation on sustainable development in ethnic regions’ agriculture and animal husbandry
- Factors impacting spatial distribution of black and odorous water bodies in Hebei
- Large-scale shaking table tests on the liquefaction and deformation responses of an ultra-deep overburden
- Impacts of climate change and sea-level rise on the coastal geological environment of Quang Nam province, Vietnam
- Reservoir characterization and exploration potential of shale reservoir near denudation area: A case study of Ordovician–Silurian marine shale, China
- Seismic prediction of Permian volcanic rock reservoirs in Southwest Sichuan Basin
- Application of CBERS-04 IRS data to land surface temperature inversion: A case study based on Minqin arid area
- Geological characteristics and prospecting direction of Sanjiaoding gold mine in Saishiteng area
- Research on the deformation prediction model of surrounding rock based on SSA-VMD-GRU
- Geochronology, geochemical characteristics, and tectonic significance of the granites, Menghewula, Southern Great Xing’an range
- Hazard classification of active faults in Yunnan base on probabilistic seismic hazard assessment
- Characteristics analysis of hydrate reservoirs with different geological structures developed by vertical well depressurization
- Estimating the travel distance of channelized rock avalanches using genetic programming method
- Landscape preferences of hikers in Three Parallel Rivers Region and its adjacent regions by content analysis of user-generated photography
- New age constraints of the LGM onset in the Bohemian Forest – Central Europe
- Characteristics of geological evolution based on the multifractal singularity theory: A case study of Heyu granite and Mesozoic tectonics
- Soil water content and longitudinal microbiota distribution in disturbed areas of tower foundations of power transmission and transformation projects
- Oil accumulation process of the Kongdian reservoir in the deep subsag zone of the Cangdong Sag, Bohai Bay Basin, China
- Investigation of velocity profile in rock–ice avalanche by particle image velocimetry measurement
- Optimizing 3D seismic survey geometries using ray tracing and illumination modeling: A case study from Penobscot field
- Sedimentology of the Phra That and Pha Daeng Formations: A preliminary evaluation of geological CO2 storage potential in the Lampang Basin, Thailand
- Improved classification algorithm for hyperspectral remote sensing images based on the hybrid spectral network model
- Map analysis of soil erodibility rates and gully erosion sites in Anambra State, South Eastern Nigeria
- Identification and driving mechanism of land use conflict in China’s South-North transition zone: A case study of Huaihe River Basin
- Evaluation of the impact of land-use change on earthquake risk distribution in different periods: An empirical analysis from Sichuan Province
- A test site case study on the long-term behavior of geotextile tubes
- An experimental investigation into carbon dioxide flooding and rock dissolution in low-permeability reservoirs of the South China Sea
- Detection and semi-quantitative analysis of naphthenic acids in coal and gangue from mining areas in China
- Comparative effects of olivine and sand on KOH-treated clayey soil
- YOLO-MC: An algorithm for early forest fire recognition based on drone image
- Earthquake building damage classification based on full suite of Sentinel-1 features
- Potential landslide detection and influencing factors analysis in the upper Yellow River based on SBAS-InSAR technology
- Assessing green area changes in Najran City, Saudi Arabia (2013–2022) using hybrid deep learning techniques
- An advanced approach integrating methods to estimate hydraulic conductivity of different soil types supported by a machine learning model
- Hybrid methods for land use and land cover classification using remote sensing and combined spectral feature extraction: A case study of Najran City, KSA
- Streamlining digital elevation model construction from historical aerial photographs: The impact of reference elevation data on spatial accuracy
- Analysis of urban expansion patterns in the Yangtze River Delta based on the fusion impervious surfaces dataset
- A metaverse-based visual analysis approach for 3D reservoir models
- Late Quaternary record of 100 ka depositional cycles on the Larache shelf (NW Morocco)
- Integrated well-seismic analysis of sedimentary facies distribution: A case study from the Mesoproterozoic, Ordos Basin, China
- Study on the spatial equilibrium of cultural and tourism resources in Macao, China
- Urban road surface condition detecting and integrating based on the mobile sensing framework with multi-modal sensors
- Review Articles
- Humic substances influence on the distribution of dissolved iron in seawater: A review of electrochemical methods and other techniques
- Applications of physics-informed neural networks in geosciences: From basic seismology to comprehensive environmental studies
- Ore-controlling structures of granite-related uranium deposits in South China: A review
- Shallow geological structure features in Balikpapan Bay East Kalimantan Province – Indonesia
- A review on the tectonic affinity of microcontinents and evolution of the Proto-Tethys Ocean in Northeastern Tibet
- Special Issue: Natural Resources and Environmental Risks: Towards a Sustainable Future - Part II
- Depopulation in the Visok micro-region: Toward demographic and economic revitalization
- Special Issue: Geospatial and Environmental Dynamics - Part II
- Advancing urban sustainability: Applying GIS technologies to assess SDG indicators – a case study of Podgorica (Montenegro)
- Spatiotemporal and trend analysis of common cancers in men in Central Serbia (1999–2021)
- Minerals for the green agenda, implications, stalemates, and alternatives
- Spatiotemporal water quality analysis of Vrana Lake, Croatia
- Functional transformation of settlements in coal exploitation zones: A case study of the municipality of Stanari in Republic of Srpska (Bosnia and Herzegovina)
- Hypertension in AP Vojvodina (Northern Serbia): A spatio-temporal analysis of patients at the Institute for Cardiovascular Diseases of Vojvodina
- Regional patterns in cause-specific mortality in Montenegro, 1991–2019
- Spatio-temporal analysis of flood events using GIS and remote sensing-based approach in the Ukrina River Basin, Bosnia and Herzegovina
- Flash flood susceptibility mapping using LiDAR-Derived DEM and machine learning algorithms: Ljuboviđa case study, Serbia
- Geocultural heritage as a basis for geotourism development: Banjska Monastery, Zvečan (Serbia)
- Assessment of groundwater potential zones using GIS and AHP techniques – A case study of the zone of influence of Kolubara Mining Basin
- Impact of the agri-geographical transformation of rural settlements on the geospatial dynamics of soil erosion intensity in municipalities of Central Serbia
- Where faith meets geomorphology: The cultural and religious significance of geodiversity explored through geospatial technologies
- Applications of local climate zone classification in European cities: A review of in situ and mobile monitoring methods in urban climate studies
- Complex multivariate water quality impact assessment on Krivaja River