Prevalence, localization, perception and management of pain in dance: an overview
-


Abstract
Background and aims
Pain is a highly complex bio-psychosocial phenomenon that may present a (potential) health risk and either occurs as a warning sign or a symptom of injury. It cannot be ruled out that these rising or changing requirements in dance of all styles, are reflected in health-related outcomes such as pain. The aim of this narrative review article is to outline an overview of prevalence and localization, concepts of performance pain and injury pain, pain perception and pain management in dance. At that consequences of pain and influencing factors focusing on different dance styles or forms of professionalism are discussed.
Methods
The databases CINAHL, Cochrane, Google Scholar, Medline, MeSH and Web of Science were screened for relevant articles.
Results
Pain prevalence in dance is very high. Pain localizations can be related to high dance-specific mechanical stress on the musculoskeletal system. Depending on the pain characteristics, dancers perceive pain as “positive” (performance pain) or “negative” (injury pain). Concerning pain attitudes and management, dancers show an increasing pain tolerance. Pain seems to be accepted as a necessity, often ignored and dancing is continued despite pain.
Conclusions
The findings of this article suggest that occurrence of pain, pain perception, coping with pain and pain history appear to be connected to dance-specific mechanical stress as well as to socialization in dance culture. In dance, effects of pain on health seem to be associated with characteristics of pain and pain behavior.
Implications
The results highlight the high relevance of pain in dance and the need to take into account preventive as well as rehabilitative measures.
1 Introduction
Dance is a mixture of sport and art form. This results in very different, partly esthetic as well as psycho-physical demands on the body. For example, the dance can be classified according to professionalism and dance styles [1], [2], [3]. It cannot be ruled out that these rising or changing requirements, are reflected in health-related outcomes such as pain. According to studies, dancers considered pain as “normal” or an “everyday” experience [2], [3] with more than 50% of dancers stating to be affected by pain [4], [5], [6], [7]. An analysis of the existing literature on this topic has yet to be carried out. The aim of this article is to provide an overview of occurrence of pain, pain perception and pain management in dance under bio-psychosocial considerations.
2 Bio-psychosocial understanding of pain
In general, pain is a subjectively unpleasant sensation that can be associated with potential tissue damage [8]. Pain is understood as both a physiological and a psychological phenomenon [8]. In addition, pain perception is influenced by socio-cultural circumstances, the individual situation and previous experience with pain [8], [9].
From a physiological point of view, pain perception and processing can occur via nociception (“nociceptive pain”) [8], [10]. According to its place of origin, pain may be categorized into visceral pain (viscera) and somatic pain (musculoskeletal system and skin) [11]. In dance, somatic pain is predominant as the musculoskeletal system is highly strained [7], [12]. The pain sensation is partly related to the nociception, but also explained psychologically [8]. The sensation of pain can be differentiated into sensory and affective dimensions [8], [9], [11].
Pain may be divided into acute and chronic pain [8], [11]. Acute pain generally lasts less than 6 weeks and can be associated with nociception [8], [9]. Acute pain in particular is considered a warning signal, which should lead to cautious behavior to prevent further more serious injuries [8]. Chronic pain is said to persist regularly or consistently more than 3–6 months, or longer [8], [11]. Suffering is very high in chronic pain [11]. That may be the reason why dancers perceive chronic pain as “bad” pain [7]. In addition to the high importance of psychological factors of chronic pain (affective dimension) in sport or dance, culture social and environmental factors must be taken into account [10], [13].
Pain behavior is another component when analysing pain and is predominantly based on the evaluation of the different pain components described above [8]. Pain behavior implies all observable reactions to pain that can occur involuntarily or voluntarily [8]. Socio-cultural circumstances seem to have a very high influence on pain behavior in sports or dance. Pain-related cautious behavior during sports and dance activities can be prevented by high performance pressure [10], [13], [14] (Fig. 1).
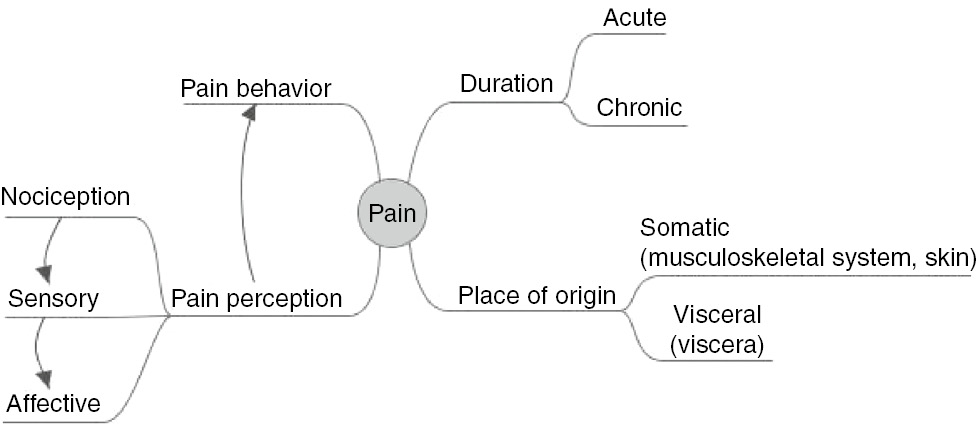
Overview of the phenomenon of pain.
3 Methods
Articles were selected by searching the following databases: CINAHL, Cochrane, Google Scholar, Medline, MeSH and Web of Science. The following keywords were applied to each data base (as single words or word combinations): “pain”, “pain perception”, “pain coping”, “dance”, “dancing”, “dancer”, “dance teacher” and “dance instructor”. The search was not limited to a specific period of time. All selected studies met the following inclusion criteria: studies with adult dancers, observational and experimental studies (qualitative and quantitative), intervention and studies on dance therapy. Studies in any other language than English or German were ignored. Articles were cross-referenced to identify publications that were not located during the original database search. Due to the paucity of specific studies regarding this topic any relevant findings were summarized.
4 Pain in dance
4.1 Prevalence and localization
In dance, pain prevalence is relatively high. Various studies show that about 50% of dancers, regardless of their dance style, are affected by pain (Table 1). Particularly in professional dance, a 12-month pain prevalence is very high [15]. Within 1 year, 73% (n=44) of professional ballet dancers affected by pain also showed pain-related limitations in their regular professional practice [15].
Pain prevalence in dance.
| Study | Study population | Prevalence |
|---|---|---|
| Aweto et al. [4] | Ambiguous professional level; Hip hop, contemporary, ballroom, African dance, jazz, ballet (n=180) |
Musculoskeletal disorders and pain: 12-month prevalence (86.1%); point prevalence (36%); prevalence within the last 1–2 weeks (58%) |
| Diogo et al. [5] | Professional and non-professional dancers; Ballet, jazz and street dance (n=150) |
Musculoskeletal pain (58.6%) |
| Dore and Guerra [6] | Professional dancers; Ballet (n=141) |
Pain while dancing (60.3%) |
| Ramel and Moritz [15] | Professional dancers; Ballet (n=64) |
Musculoskeletal pain: 12-month prevalence (93.8%) |
| Thomas and Tarr [7] | Professional dancers, dance students, dance teachers, choreographers, former dancers Modern and contemporary dance (n=204) |
Recent pain associated with dancing (78%) |
Sometimes various regions of a dancer’s body may be painful at the same time. In the study by Thomas and Tarr [7], 21% of modern and contemporary dancers had more than one pain location at the time of interview. Among these dancers, up to six pain locations were reported [7]. The number of painful body regions varies between 1.3 (in less experienced professional dancers) and 2.9 (in more experienced dancers) within a month. A significant predictor for the number of pain locations in these dancers was the number of years of ballet training [16]. In addition, Aweto et al. [4] showed a significant correlation between training time per week and pain prevalence in dance. In view of these findings, the extent of pain occurrence in dance shows a positive correlation with dance experience as well as training intensity.
Pain particularly affects the musculoskeletal system in dancers due to its physically highly demanding nature [7], [12], [17]. Musculoskeletal pain in dance can be associated with overuse of the musculoskeletal system [18]. As a result, pain locations may be related to dance-specific pressure on the musculoskeletal system.
Pain is often localized in the spinal region and lower extremities across various dance styles [4], [5], [7], [15], [19], [20]. These areas are also most frequently affected by acute or chronic pain symptoms in dance teachers [21]. Furthermore, the location of pain appears to differ according to the dance style performed. In classical ballet, the lower back and the lower limbs are very frequently affected by pain in comparison to other dance styles [5], [6], [16], [18]. In relation to all reported body regions, pain prevalence in the lower back is rated 75% [15] up to 85.8% [6] in classical ballet. In relation to all reported painful body regions, neck, hips, knees and feet are affected in approximately 50% of the professional ballet dancers [6], [15]. Wrists or hands represent a frequently involved painful body region in professional break dancers [19]. In Irish dance, feet and ankles are very often affected by pain [22]. In competitive ballroom dancing, Standard and Latin style, significant gender-specific differences could be observed. These were hips (f: 10%, m: 35%), calves (f: 6%, m: 24%) and toes (f: 45%, m: 22%) [23]. Similar gender-specific results could be seen in Latin American Formation Dance [24]. In addition, Miletic et al. [20] found a significantly higher toe injury frequency by using a pain status in Standard and Latin dancers compared to other dance styles (e.g. show dance, disco dance, cheerleading).
4.2 Performance pain and injury pain
The difficulty in sports or in dance is to classify pain in relation to its risk potential. Sports or dance medicine literature mainly distinguishes between two types of pain: performance pain or “good” pain and injury pain or “bad” pain [7], [13], [25], [26] both types of which are attributed with specific characteristics (Table 2).
Characteristics of performance pain and injury pain.
| Performance pain | Injury pain |
|---|---|
| “Good” pain [7], [26] Training or stretching pain [7] |
“Bad” pain [7], [26] (potential) health risk [25] |
| Low pain intensity [7], [25] | Severe pain intensity [7], [25] |
| Tugging, tingling, throbbing [7] | Sharp, shooting, pinching, burning, searing, throbbing [7] |
| Harmless, tolerable, pleasant, tiring/exhaustive, motivating, positive experience of pain [7], [25], [26] | Threatening, dangerous, intolerable, paralyzing, evoking fear, demotivating, negative experience of pain [7], [25], [26] |
| Voluntarily produced [7], [25] | Difficult to control, limits or prevents dancing [7], [25], [26] |
| Acute, short duration [25] | Acute or chronic [7], [25] |
| Primarily muscle pain [7] | Pain in bones, joints, ligaments, partly in muscles; also nerve pain [7] |
Performance pain can be considered more as a natural consequence of the physical effort involved in sports or in dance, occurring especially when training at maximum capacity [7], [13], [14], [26]. It is therefore less perceived as a sign of serious injury [7]. It would appear that both athletes and dancers deliberately provoke positive pain to increase performance [2], [13], [14]. Nevertheless, performance pain should still be recognized as a warning signal for regeneration. Thomas and Tarr [7] found that recurring low-graded pain, not impairing dance activities, was not perceived as an injury by dancers. However, this might be an indication of overuse or chronic complaints [7]. There seems to be a fluent transition from performance pain to injury pain in this context.
Injury pain is associated with tissue injuries which may result in serious health risks [7], [25]. At that, it may limit or restrict the dancer’s training capabilities [7], [25]. In terms of injury pain, it becomes apparent that pain and injury are associated. In view of this correlation, dance injuries were sometimes also defined by pain. Allison [27], for instance, defined a “ballet-related injury” as “any pain or dysfunction having an effect on the dancers’ ability to dance”. Jacobs et al. [28] defined an injury of a body region based on the self-estimated functional inability because of pain (SEFIP) with a score of three or more. Some studies reported “pain and injury” in one context and therefore could not clearly be separated in these studies [4], [7], [29]. Not only the concepts of “pain” and “injury” seem to be difficult to differentiate, but also the perception of dancers concerning pain and injury. Injury pain appears to be particularly problematic in dance as it is often not adequately identified by dancers. According to Thomas and Tarr [7], 43% of dancers suffering from pain did not consider their pain to indicate an injury. Anderson and Hanrahan [25] found an inability to evaluate and adequately cope with pain in terms of its potential health risk in pre-professional and professional dancers. Consequences of injury pain can be chronic pain or overuse injuries [7].
Regarding the differentiation of performance pain and injury pain, it must be noted that certain pain characteristics cannot always be clearly assigned to a particular type of pain as shown in the study by Thomas and Tarr [7]: some qualitative pain descriptions were named by dancers both in terms of “good” and “bad” pain. It also appears that the evaluation of pain as “good” or “bad” could be more a case of quantity rather than quality of pain [7]. In this view, performance as well as injury pain may be interpreted less as two separate categories but more as elements of the same continuum.
4.3 Pain perception in dancers
Pain perception appears to vary in dancers. Tajet-Foxell and Rose [30] and Paparizos et al. [31] studied pain perception and pain tolerance in professional and non-professional ballet dancers with an experimental pain stimulus (Cold Pressor Test). The findings indicated that dancers had a significantly higher pain tolerance than non-dancers [30], [31]. Advanced non-professional dancers showed a significantly higher pain tolerance than non-dancers or less experienced dancers (beginner or intermediate level) [31]. Concerning pain intensity, there was no significant difference between non-professional dancers and non-dancers [31]. However, Tajet-Foxell and Rose [30] found significantly higher pain intensities in professional dancers than in non-dancers. That athletes, including dancers, have a higher pain tolerance than normally active controls (i.e. people whose physical activity was <3 h per week with no active participation in any form of organized sports) is also evident in the meta-analysis by Tesarz et al. [3]. Furthermore, the meta-analysis showed a heterogeneity concerning pain thresholds. It is not clear whether or to what extent pain thresholds differ between athletes and normally active controls [3]. As to pain intensities, the studies by Tajet-Foxell and Rose [30] as well as Paparizos et al. [31] showed a comparable ambivalence.
As the studies mentioned above worked with an experimental pain stimulus rather than a dance induced one [3], [30], [31] (internal validity), pain perception in dance is highly likely to be influenced by a more complex range of factors [32], [33] (external validity). In dance, the so called motion in space, pain perception can be modeled by complex sensorimotor processes [33]. In the study of Aalten [2], for instance, one female ballet dancer reported to perceive pain outside of her dancing activity, but not while dancing.
The perceived pain intensity in dance strongly varies in the different studies (Table 3). According to Aweto et al. [4] perceived pain intensities of dancers were most frequently reported in the middle level (4–5). The pain intensity decreased in frequency towards the extremes (level 1 resp. 10) [4]. It should be noted that this study [4] was based on a very heterogeneous sample in terms of dance styles and training intensities which suggests varying strain on the musculoskeletal system (as potential noxious stimulus caused by mechanical strain). This broad range of training loads may have resulted in the relatively equal distribution of dancers’ perceived pain intensities.
Pain intensity in dance.
| Study | Study population | Outcome measures | Findings |
|---|---|---|---|
| Aweto et al. [4] | Ambiguous professional level; Hip hop, contemporary, ballroom, African dance, jazz, ballet (n=180) |
Numeric rating scale (pain intensity on a scale of 0–10; 0=no pain, 10=highest level of pain) |
42.8% (level 0); 2.2% (level 1); 16.8% (level 2–3); 22.8% (level 4–5); 5.6% (level 6); 4.4% (level 7–8); 2.2% (level 9–10) |
| Diogo et al. [5] | Professional and non-professional dancers; Ballet, jazz and street dance (n=150) |
Brief pain inventory – short form (BPI-SF) (pain intensity on a scale from 0 to 10; 0=no pain, 10=highest level of pain) |
Mild pain (53.3%); Moderate pain (6%); Severe pain (0.6%) |
| Jacobs et al. [28] | Professional dancers; Ballet (n=178), Modern (n=82) |
Self-estimated functional inability because of pain (SEFIP) (pain intensity on a scale from 0 to 4; 0=no pain, 4=severe pain/unable to dance) | Ballet: 38.8% (level 3–4) Modern: 45.1% (level 3–4) |
| Dore and Guerra [6] | Professional dancers; Ballet (n=141) |
Pain intensity on a scale from 0 to 10; 0=no pain, 10=highest level of pain | Moderate (level 4–6) to severe pain (level 7–8) while dancing (60.3%) |
| Miletic et al. [23] | Competitive dancers; Standard and Latin (n=86) |
Self-estimated functional inability because of pain (SEFIP) (pain intensity on a scale from 0 to 4; 0=no pain, 4=severe pain/unable to dance) | Most of the subjects (level 1); 31.4% (level 2); 0.03% (level 3) |
Jacobs et al. [28] reported of pain intensities impairing dancing in 38.8% of professional ballet dancers and 45.1% of professional modern dancers. Perceived pain intensities seem to be higher in professional dance than in non-professional dance. In professional dance, 60.3% of the dancers suffered from moderate to severe pain [6]. However, Diogo et al. [5] determined mild pain in most dancers, one third of which were non-professionals. Hypothetically, this may be explained by professional dancers’ more sensitive pain perception compared to non-dancers as shown in the study of Tajet-Foxell and Rose [30].
Another influencing factor on perceived pain intensity could be the type of pain. Injury pain tends to be perceived as more intense than performance pain [7]. Therefore, in comparison to non-professional dance, higher levels of pain intensity in professional dance could be due to higher physical demands resulting more often in injury pain.
In view of these findings, it should be considered that the data base is insufficient in terms of quantity and comparability of study results, thus making an adequate representation of pain intensity as well as the potential influencing factors on pain intensity in dance difficult. Therefore, only assumptions can be made at present.
4.4 Pain management in dance
Pain is almost unavoidable in dance, but it also seems to be a taboo topic in dance culture [14], [26], [34]. Certain attitudes and forms of pain and injury management seem to emerge: pain is accepted as a necessity, often ignored and dancing is continued despite pain [2], [7], [14], [25], [26], [34], [35]. These attitudes and forms of pain management are observed in professional and semi-professional dancers as well as in dance teachers [2], [7], [21], [25], [34], [35]. The frequent confrontation with pain in dance practically ensures the integration of these socio-culturally based attitudes and forms of pain management into dancers’ behavior [14], [36].
Accepting and ignoring pain are common coping strategies in dance. Pain is accepted as inevitable by professional ballet dancers in order to overcome physical limitations and to achieve the desired ideals [2], [14], [25] with dancers of a semi-professional contemporary dance ensemble considering pain to be necessary [35]. They also tend to trivialize and ignore overuse injuries [35].
The described attitude concerning pain in dance often results in dancing being continued despite pain. Aweto et al. [4] reported that more than 50% of dancers of various dance styles continued their training unchanged despite pain or injury. The study by Allison [27] on advanced amateur ballet dancers showed that the continuation of dance training seems to be connected to the dancers’ self-assessment of the injury’s severity (on a scale from 0 to 10). While 66.7% of dancers with mild injuries [severity x̅(s)=1.33(0.58)] continued training without modification, only 25% of dancers with severe injuries [severity x̅(s)=6.31 (1.97)] did the same. In addition, dance teachers show an especially high disposition to continue their work despite pain. In the study by Wanke et al. [21], this behavior could be attributed to 89.4% of dance teachers.
Concerning the treatment of pain and injuries, dancers and dance teachers often seem to prefer self-treatment. Medical professionals are rarely consulted. In the study by Aweto et al. [4], 21.3% of dancers suffering from pain and injuries did not treat their complaints, while 35% treated themselves. In semi-professional dance, self-treatment or ignoring of injuries appear to be the primarily applied coping strategies (Latin American formation dance and contemporary dance) [24], [35]. Dancers apparently rarely make use of professional medical treatment. Only approximately one third of dancers consult medical professionals in case of complaints at an early stage [37]. Dance teachers often only consulate medical professionals if self-treatment is unsuccessful (45.5%) or in cases of severe pain (27.3%) [21].
The predominantly applied pain management in dance culture entails health risks. Ignoring pain is considered a risk factor for overuse injuries [2], [29], [31]. In accordance with this view, Mainwaring et al. [34] declared that dance culture is a “culture of injury, pain, and tolerance” with McEwan and Young [14] declaring it as “culture of risk”. Long-term consequences of this behavior could result in a chronification of complaints and a provocation of further injuries [13], [26], [32].
Ignoring pain as a natural signal of the body to apply more cautious behavior has many reasons: passion for dance, identity as a dancer, responsibility towards the dance group as well as self-discipline and perfection are more important factors in professional and semi-professional dance, influencing dancers’ forms of pain and injury management [2], [14], [34], [35]. Furthermore, performance pressure in competition phases by choreographers or dance competitors can be relevant in the area of competitive or professional dance [14], [24], [34]. If dance is practiced professionally (professional dancer or dance teacher), there are also existential fears to be considered [14], [17], [21], [34].
With regard to dancers’ unwillingness to make use of professional medical treatment, further reasons need to be considered. Dancers show a lack of confidence in medical professionals: they feel misunderstood in their existential and artistic needs and fear to receive inadequate treatment by medical professionals [14], [34], [35], [37], [38].
Concerning healthy behavior, dance teachers could be considered opinion leaders by virtue of their role model function and their attitudes and forms of pain management in dance culture [21]. Regarding pain management, dance teachers showed predominantly risky forms of health behavior, in accordance with the accepted dance culture [21], though.
5 Discussion and implications for further research
With regards to the literature cited in this article, some methodological limitations and research gaps should be pointed out. While pain prevalence can be found in some studies, other characteristics of pain and potential influencing factors on pain in dance are rarely presented. Taking into account dance-specific factors and socialization in dance culture, the occurrence of pain, pain perception, pain management and pain history in dance should be further investigated in more detailed research. It is relevant to take both quantitative and qualitative methods into consideration in order to generate comprehensive knowledge on physical, psychological and socio-cultural factors concerning pain in dance.
Hainline et al. [10] stated that “pain is not synonymous with dance or sport injury”. A further limitation of the cited studies is that they do not always clearly distinguish between pain and injury. Pain might not generally be correlated with a serious injury like in terms of performance pain for it can also be a warning signal of an impending injury. Furthermore, pain is an independent phenomenon which can also occur without injury (e.g. as chronic pain) [10], Therefore, the differentiation between pain and injury appears useful.
However, even in terms of performance pain, tissue damages cannot be waived and, therefore, is not automatically harmless.
As to the pathogenesis of injuries in dance, it often seems that only biomechanical factors are discussed. Since pain is not only understood physiologically but also psychologically and in a socio cultural context, these factors might possibly provide a more comprehensive insight into the emergence of dance injuries than primarily biomechanical approaches.
A further challenge to the representation of pain in dance is the heterogeneity of present studies. The study samples show a wide variety concerning the professional level of dancers (non-professional to professional) and dance styles. This heterogeneity of samples applies both within studies as well as in the comparison of different studies. Results did not always distinguish between different subgroups. In addition, the comparability of studies was made difficult by different outcome measures and differently structured presentation of findings, for instance, in pain intensity (Table 3). In addition, it is important to critically assess the measuring instruments used for pain evaluation in dance in the cited studies. The SEFIP is a measuring instrument based on the Nordic Musculoskeletal Questionnaire (NMQ), especially adapted for dance [39]. The nine pain regions of the NMQ were extended by another five regions in the SEFIP, however, without differentiating either side of the body [39]. In view of preferences and muscular dysbalances, especially of the lower extremity, in dancers [40], [41], a differentiated representation of the pain regions might be useful. Visual mapping of pain regions could be a promising instrument in this respect [36]. In addition, the validation of the SEFIP is based on a test battery of physical tests [39] and thus primarily represents a reference to the physical perspective to pain. However, since pain is understood as a biopsychosocial construct [8], [36], the primary physical validation of SEFIP is not sufficient. Furthermore, the SEFIP combines two pain components (pain intensity and pain behavior), which should be considered separately. As socio-cultural circumstances in dance culture can be so high (e.g. pressure from dance teachers, competition, etc.) that dancers continue to dance despite high pain intensities [14]. Therefore, a differentiated survey of pain components which also takes socio-cultural circumstances into account, seems to be useful. In future work, adequate measuring instruments for various pain components in dance should be adapted and validated for dancers.
With regard to the high complexity of this topic, a more structured research approach appears to be absolutely imperative. Retrospective self-reported questionnaires should be used very carefully, because memory may be distorted.
6 Conclusion
The findings concerning pain characteristics in dancers can be summarized as follows:
Pain prevalence in dance is very high.
Pain seems to occur predominantly in body regions exposed to high dance-specific mechanical stress.
In view of pain perception, dancers show an increased pain tolerance, fail to recognize pain as a warning signal and thus to accept it as a reason for cautious behavior.
These findings suggest that dancers are subject to potential health risks. Other risks include how pain is dealt with in dance culture. Ignoring pain and inadequate pain management can lead to injuries and chronification of pain. Therefore, pain management has a major influence on the further development of pain. Health hazardous attitudes and behaviors toward pain seem to exist predominately among dancers who are highly involved in dance culture (professionals and semi-professionals). For non-professional dancers a health hazard is obviously less relevant. Besides the health hazardous aspects of pain, it should be considered that pain can also have positive health effects. Regarding performance pain, pain is associated with positive sensations, increasing pain tolerance and performance. Summarizing it can be said that the effects of pain in dance on health seem to be associated with the characteristics of pain and the pain behavior.
-
Authors’ statements
-
Research funding: None.
-
Conflict of interest: None.
-
Informed consent: Not applicable.
-
Ethical approval: Not applicable.
References
[1] Koutedakis Y, Jamurtas A. The dancer as a performing athlete: physiological considerations. Sport Med 2004;34:651–61.10.2165/00007256-200434100-00003Search in Google Scholar PubMed
[2] Aalten A. In the presence of the body: theorizing training, injuries and pain in ballet. Danc Res J 2005;37:55–72.10.1017/S0149767700008561Search in Google Scholar
[3] Tesarz J, Schuster AK, Hartmann M, Gerhardt A, Eich W. Pain perception in athletes compared to normally active controls: a systematic review with meta-analysis. Pain 2012;153:1253–62.10.1016/j.pain.2012.03.005Search in Google Scholar PubMed
[4] Aweto HA, Awolesi OM, Alao RO. Musculoskeletal pain and injury in professional dancers: prevalence, predisposing factors and treatment. Indian J Phys Ther 2014;2:6–13.Search in Google Scholar
[5] Diogo MA, Ribas GG, Skare TL. Frequency of pain and eating disorders among professional and amateur dancers. Sao Paulo Med J 2016;134:501–7.10.1590/1516-3180.2016.0077310516Search in Google Scholar PubMed
[6] Dore BF, Guerra RO. Painful symptoms and associated factors in professional dancers. Rev Bras Med Do Esporte 2007;13:67–70.10.1590/S1517-86922007000100015Search in Google Scholar
[7] Thomas H, Tarr J. Dancers’ perceptions of pain and injury: positive and negative effects. J Dance Med Sci 2009;13:51–9.10.1177/1089313X0901300203Search in Google Scholar
[8] Marchand S. The phenomenon of pain. 2. Auflage. Seattle: IASP, 2012.Search in Google Scholar
[9] Loeser JD, Melzack R. Pain: an overview. Lancet 1999;353:1607–9.10.1016/S0140-6736(99)01311-2Search in Google Scholar PubMed
[10] Hainline B, Turner JA, Caneiro JP, Stewart M, Lorimer Moseley G. Pain in elite athletes – neurophysiological, biomechanical and psychosocial considerations: a narrative review. Br J Sports Med 2017;51:1259–64.10.1136/bjsports-2017-097890Search in Google Scholar PubMed
[11] Schmidt R, Willis W. Encyclopedia of pain. Berlin, Heidelberg, New York: Springer, 2007.10.1007/978-3-540-29805-2Search in Google Scholar
[12] Hincapié CA, Morton EJ, Cassidy JD. Musculoskeletal injuries and pain in dancers: a systematic review. Arch Phys Med Rehabil 2008;89:1819–29.10.1016/j.apmr.2008.02.020Search in Google Scholar PubMed
[13] Howe D. Sport, professionalism and pain: ethnographies of injury and risk. London, New York: Routledge, 2004.10.4324/9780203453261Search in Google Scholar
[14] McEwen K, Young K. Ballet and pain: reflections on a risk-dance culture. Qual Res Sport Exerc Heal 2011;3:152–73.10.1080/2159676X.2011.572181Search in Google Scholar
[15] Ramel EM, Moritz U. Psychosocial factors at work and their association with professional ballet dancers’ musculoskeletal disorders. Med Probl Perform Art 1998;13:66–74.Search in Google Scholar
[16] Nunes NMA, Haddad JJ, Bartlett DJ, Obright KD. Musculoskeletal injuries among young, recreational, female dancers before and after dancing in pointe shoes. Pediatr Phys Ther 2002;14:100–6.10.1097/00001577-200214020-00006Search in Google Scholar PubMed
[17] Wanke EM, Schmidt M, Leslie-Spinks J, Fischer A, Groneberg DA. Physical and mental workloads in professional dance teachers. Med Probl Perform Art 2015;30:54–60.10.21091/mppa.2015.1008Search in Google Scholar PubMed
[18] Ramel EM, Moritz U, Jarnlo G. Recurrent musculoskeletal pain in professional ballet dancers in Sweden: a six-year follow-up. J Dance Med Sci 1999;3:93–100.10.1177/1089313X9900300301Search in Google Scholar
[19] Kauther MD, Wedemeyer C, Wegner A, Kauther KM, Von Knoch M. Breakdance injuries and overuse syndromes in amateurs and professionals. Am J Sports Med 2009;37:797–802.10.1177/0363546508328120Search in Google Scholar PubMed
[20] Miletic A, Kostic R, Bozanic A, Durdica M. Pain status monitoring in adolescent dancers. Med Probl Perform Art 2009;24:119–23.10.21091/mppa.2009.3026Search in Google Scholar
[21] Wanke E, Schmitter J, Groneberg D. Analyse und Evaluation der Gesundheitssituation von Bewegung vermittelnden Lehrkräften am Beispiel der Tanzpädagogik. Sportverletz Sportschaden 2012;26:49–56.10.1055/s-0031-1281840Search in Google Scholar PubMed
[22] Cahalan R, Purtill H, O’Sullivan P, Kieran O. Foot and ankle pain and injuries in elite adult irish dancers. From Med Probl Perform Artist 2014;29:198–206.10.21091/mppa.2014.4041Search in Google Scholar PubMed
[23] Miletic A, Kostic R, Miletic D. Pain prevalence among competitive international dancers. Int J Athl Ther Train 2011;16:13–6.10.1123/ijatt.16.1.13Search in Google Scholar
[24] Wanke EM, Fischer T, Pieper H, Groneberg DA. Tanzsport: Verletzungsmuster im Lateinamerikanischen Formationstanz. Sportverletz Sportschaden 2014;28:132–8.10.1055/s-0034-1384851Search in Google Scholar PubMed
[25] Anderson R, Hanrahan S. Dancing in pain. Pain appraisal and coping in dancers. J Dance Med Sci 2008;12:9–16.10.1177/1089313X0801200102Search in Google Scholar
[26] Harrison C, Ruddock-Hudson M. Perceptions of pain, injury, and transition-retirement: the experiences of professional dancers. J Dance Med Sci 2017;21:43–52.10.12678/1089-313X.21.2.43Search in Google Scholar PubMed
[27] Allison K. Associations between musculoskeletal injury and selected lower limb biomechanical measurements in female amateur ballet dancers. Durban (South Africa): Durban University of Technology, 2014.Search in Google Scholar
[28] Jacobs CL, Cassidy JD, Côté P, Boyle E, Ramel E, Ammendolia C, Hartvigson J, Schwartz I. Musculoskeletal injury in professional dancers: prevalence and associated factors: an international cross-sectional study. Clin J Sport Med 2017;27:153–60.10.1097/JSM.0000000000000314Search in Google Scholar PubMed
[29] Rivera DC, Alexander JL, Nehrenz GM, Fields BJ. Dancers’ perceptions of injuries. J Music Danc 2012;2:9–12.Search in Google Scholar
[30] Tajet-Foxell B, Rose FD. Pain and pain tolerance in professional ballet dancers. Br J Sports Med 1995;29:31–4.10.1136/bjsm.29.1.31Search in Google Scholar PubMed PubMed Central
[31] Paparizos AL, Tripp DA, Sullivan MJL, Rubenstein ML. Catastrophizing and pain perception in recreational ballet dancers. J Sport Behav 2005;28:35–50.Search in Google Scholar
[32] Claus AP, MacDonald DA. Interpreting pain symptoms and how pain affects neuromuscular control in dancers: if I’m in pain, how should I train? J Dance Med Sci 2017;21:5–12.10.12678/1089-313X.21.1.5Search in Google Scholar PubMed
[33] Wallwork S, Bellan V, Moseley GL. Applying current concepts in pain-related brain science to dance rehabilitation. J Dance Med Sci 2017;21:13–23.10.12678/1089-313X.21.1.13Search in Google Scholar PubMed
[34] Mainwaring LM, Krasnow D, Kerr G. And the dance goes on: psychological impact of injury. J Dance Med Sci 2001;5:105–15.10.1177/1089313X0100500402Search in Google Scholar
[35] Markula P. (Im)Mobile bodies: contemporary semi-professional dancers’ experiences with injuries. Int Rev Sociol Sport 2015;50:840–64.10.1177/1012690213495745Search in Google Scholar
[36] Tarr J, Thomas H. Mapping embodiment: methodologies for representing pain and injury. Qual Res 2011;11:141–57.10.1177/1468794110394067Search in Google Scholar
[37] Lai RY, Krasnow D, Thomas M. Communication between medical practitioners and dancers. J Dance Med Sci 2008;12:47–53.10.1177/1089313X0801200202Search in Google Scholar
[38] Sabo M. Physical therapy rehabilitation strategies for dancers: a qualitative study. J Dance Med Sci 2013;17:11–7.10.12678/1089-313X.17.1.11Search in Google Scholar
[39] Ramel EM, Moritz U, Jarnlo GB. Validation of a pain question-naire (SEFIP) for dancers with a specially created test battery. Med Probl Perform Art 1999;14:196–203.Search in Google Scholar
[40] Gupta A, Fernihough B, Bailey G, Bombeck P, Clarke A, Hopper D. An evaluation of differences in hip external rotation strength and range of motion between female dancers and non-dancers. Br J Sports Med 2004;38:778–83.10.1136/bjsm.2003.010827Search in Google Scholar PubMed PubMed Central
[41] Hamilton WG, Hamilton LH, Marshall P, Molnar M. A profile of the musculoskeletal characteristics of elite professional ballet dancers. Am J Sports Med 1992;20:267–73.10.1177/036354659202000306Search in Google Scholar PubMed
©2018 Scandinavian Association for the Study of Pain. Published by Walter de Gruyter GmbH, Berlin/Boston. All rights reserved.
Articles in the same Issue
- Frontmatter
- Editorial comment
- Support for mirror therapy for phantom and stump pain in landmine-injured patients
- Lifting with straight legs and bent spine is not bad for your back
- Bipolar radiofrequency neurotomy for spinal pain – a promising technique but still some steps to go
- Topical review
- Prevalence, localization, perception and management of pain in dance: an overview
- Clinical pain research
- Pain assessment in native and non-native language: difficulties in reporting the affective dimensions of pain
- Colored body images reveal the perceived intensity and distribution of pain in women with breast cancer treated with adjuvant taxanes: a prospective multi-method study of pain experiences
- Physiotherapy pain curricula in Finland: a faculty survey
- Mirror therapy for phantom limb and stump pain: a randomized controlled clinical trial in landmine amputees in Cambodia
- Pain and alcohol: a comparison of two cohorts of 60 year old women and men: findings from the Good Aging in Skåne study
- Prolonged, widespread, disabling musculoskeletal pain of adolescents among referrals to the Pediatric Rheumatology Outpatient Clinic from the Päijät-Häme Hospital District in southern Finland
- Impact of the economic crisis on pain research: a bibliometric analysis of pain research publications from Ireland, Greece, and Portugal between 1997 and 2017
- Measurement of skin conductance responses to evaluate procedural pain in the perioperative setting
- Original experimental
- An observational study of pain self-management strategies and outcomes: does type of pain, age, or gender, matter?
- Fibromyalgia patients and healthy volunteers express difficulties and variability in rating experimental pain: a qualitative study
- Effect of the market withdrawal of dextropropoxyphene on use of other prescribed analgesics
- Observational study
- Winning or not losing? The impact of non-pain goal focus on attentional bias to learned pain signals
- Gabapentin and NMDA receptor antagonists interacts synergistically to alleviate allodynia in two rat models of neuropathic pain
- Offset analgesia is not affected by cold pressor induced analgesia
- Central and peripheral pain sensitization during an ultra-marathon competition
- Reduced endogenous pain inhibition in adolescent girls with chronic pain
- Evaluation of implicit associations between back posture and safety of bending and lifting in people without pain
- Assessment of CPM reliability: quantification of the within-subject reliability of 10 different protocols
- Cerebrospinal fluid cutaneous fistula after neuraxial anesthesia: an effective treatment approach
- Pain in the hand caused by a previously undescribed mechanism with possible relevance for understanding regional pain
- The response to radiofrequency neurotomy of medial branches including a bipolar system for thoracic facet joints
- Letter to the Editor
- Diagnosis of carpal tunnel syndrome – implications for therapy
- Reply to the Letter to the Editor by Ly-Pen and Andréu
- Letter to the Editor regarding “CT guided neurolytic blockade of the coeliac plexus in patients with advanced and intractably painful pancreatic cancer”
- Reply to comments from Ulf Kongsgaard to our study
Articles in the same Issue
- Frontmatter
- Editorial comment
- Support for mirror therapy for phantom and stump pain in landmine-injured patients
- Lifting with straight legs and bent spine is not bad for your back
- Bipolar radiofrequency neurotomy for spinal pain – a promising technique but still some steps to go
- Topical review
- Prevalence, localization, perception and management of pain in dance: an overview
- Clinical pain research
- Pain assessment in native and non-native language: difficulties in reporting the affective dimensions of pain
- Colored body images reveal the perceived intensity and distribution of pain in women with breast cancer treated with adjuvant taxanes: a prospective multi-method study of pain experiences
- Physiotherapy pain curricula in Finland: a faculty survey
- Mirror therapy for phantom limb and stump pain: a randomized controlled clinical trial in landmine amputees in Cambodia
- Pain and alcohol: a comparison of two cohorts of 60 year old women and men: findings from the Good Aging in Skåne study
- Prolonged, widespread, disabling musculoskeletal pain of adolescents among referrals to the Pediatric Rheumatology Outpatient Clinic from the Päijät-Häme Hospital District in southern Finland
- Impact of the economic crisis on pain research: a bibliometric analysis of pain research publications from Ireland, Greece, and Portugal between 1997 and 2017
- Measurement of skin conductance responses to evaluate procedural pain in the perioperative setting
- Original experimental
- An observational study of pain self-management strategies and outcomes: does type of pain, age, or gender, matter?
- Fibromyalgia patients and healthy volunteers express difficulties and variability in rating experimental pain: a qualitative study
- Effect of the market withdrawal of dextropropoxyphene on use of other prescribed analgesics
- Observational study
- Winning or not losing? The impact of non-pain goal focus on attentional bias to learned pain signals
- Gabapentin and NMDA receptor antagonists interacts synergistically to alleviate allodynia in two rat models of neuropathic pain
- Offset analgesia is not affected by cold pressor induced analgesia
- Central and peripheral pain sensitization during an ultra-marathon competition
- Reduced endogenous pain inhibition in adolescent girls with chronic pain
- Evaluation of implicit associations between back posture and safety of bending and lifting in people without pain
- Assessment of CPM reliability: quantification of the within-subject reliability of 10 different protocols
- Cerebrospinal fluid cutaneous fistula after neuraxial anesthesia: an effective treatment approach
- Pain in the hand caused by a previously undescribed mechanism with possible relevance for understanding regional pain
- The response to radiofrequency neurotomy of medial branches including a bipolar system for thoracic facet joints
- Letter to the Editor
- Diagnosis of carpal tunnel syndrome – implications for therapy
- Reply to the Letter to the Editor by Ly-Pen and Andréu
- Letter to the Editor regarding “CT guided neurolytic blockade of the coeliac plexus in patients with advanced and intractably painful pancreatic cancer”
- Reply to comments from Ulf Kongsgaard to our study