Offset analgesia is not affected by cold pressor induced analgesia
-
Thomas Dahl Nissen


Abstract
Background and aims
Offset analgesia (OA) is a pain modulating mechanism described as a disproportionately large decrease in pain intensity evoked by a minor decrease in stimulus intensity. Precise mechanisms of OA are still not elucidated and studies are needed to evaluate factors modulating OA. The aim of this study was to investigate OA before and during tonic cold pain (thought to induce descending inhibition), in a group of healthy volunteers.
Methods
A randomized, crossover study was performed in 17 healthy participants (8 males and 9 females). The OA paradigm lasted 35 s and was induced by the traditional method using thermal stimulation applied to the forearm. A constant control heat stimulus (CTL) paradigm was used as control to assess adaptation. Pain intensity was assessed continuously. For induction of tonic cold pain, the participants immersed their hand into 2°C water for 2 min. After 1 min and 25 s, the heat stimulation (OA or CTL paradigm) was repeated to assess the modulatory effect of the cold pressor test.
Results
It was possible to induce OA both before and during the cold pressor test. Tonic cold pain modulated the peak pain reported during both the OA (p=0.015) and CTL paradigms (p=0.001) reflecting endogenous pain modulation. However, the magnitude of OA was not modulated by tonic cold pain (p>0.05).
Conclusions
The offset analgesia magnitude was not modulated by simultaneously tonic cold pain, thought to reflect another endogenous pain modulation mechanism.
Implications
Neither offset analgesia magnitude nor adaptation were modulated by cold pressor induced endogenous analgesia. This could be explained by the fact, that offset analgesia was already at maximum in healthy participants. Hence, offset analgesia may not be a suitable assessment tool to investigate modulation induced by experimental methods or pharmacology in healthy participants.
1 Introduction
The pain modulating mechanism offset-analgesia (OA) is described as a disproportionately decrease in pain intensity evoked by a minor decrease in stimulus intensity and the decrease in pain is greater than that evoked by continuous noxious heat stimulation (adaptation) [1]. OA has been investigated in healthy volunteers and patients to explore the underlying mechanisms [2], [3], [4], [5], [6] and it has been suggested that OA functions as an edge enhancement filter where temporal contrast is enhanced [7], [8]. The effect may result from the active engagement of central neural circuits or the intrinsic response properties of the primary afferents processing this information [7]. Studies have shown that OA most likely involves a central component [7] and it has been suggested that supraspinal descending modulatory mechanisms involving periaqueductal grey (PAG) may be involved in the endogenous analgesia caused by OA [7]. The exploration of the fundamentals underlying OA has been slow, as no animal models exist to investigate the underlying neurobiological basis. It has been speculated that other known descending modulatory mechanisms may affect OA. One of those explored in humans is conditioned pain modulation (CPM). This is a paradigm where a painful stimulus (“conditioning-stimulus”) applied to a remote area of the body inhibit the pain response of a heterotrophic painful stimulus (“test-stimulus”) [9]. Previous studies have revealed different mechanistic properties of endogenous analgesia through CPM versus OA and indications suggest that both may influence one another [10].
Only one study have explored a possible additive effect of CPM and OA on pain inhibition and found that CPM resulted in an additive effects on OA only in males [11]. However, the conditioning stimulation consisted of immersing the hand into a hot water bath of 46°C, whereas another common method is the cold pressor test. The cold pressor test generally elicits a higher pain intensity and it is known that the intensity of the conditioning stimulus is important for the level of CPM induced analgesia [12]. Thus, further studies are warranted to evaluate if OA can be modulated by other pain modulatory mechanisms.
Recently it was demonstrated that a longer T2 period in the OA stimulation paradigm enhances the magnitude of OA both in patients and in healthy volunteers [13]. Therefore, it was proposed that OA requires sufficient temporal summation of pain before offset. This may explain some of the nonsignificant findings on modulation of OA in previous studies as no other studies have used the longer T2 period [13].
Thus, the hypothesis was that using the longer T2 period in the OA paradigm it was possible to modulate OA by the cold pressor test that is expected to induce concomitant endogenous analgesia.
The aim of this study was to investigate OA before and during cold pressor pain in a group of healthy participants and compare findings to the control session (to elucidate the impact of adaptation).
2 Methods
2.1 Participants
The study sample included 17 healthy participants (8 males and 9 females). Participants were recruited among hospital staff. The study was carried out in the research laboratories at Mech-Sense, Department of Gastroenterology, Aalborg University Hospital, Denmark, between July and August 2017. Written informed consents were obtained from participants before the study procedures. The study was carried out according to the recommendations of the Helsinki declaration (2013) and approved by The North Denmark Region Committee on Health Research Ethics (N-2009008). Inclusion criteria were: [1] age between 18 and 65 years; [2] able to read and understand Danish; [3] Northern European descent. Exclusion criteria were: [1] history of persistent or recurring pain conditions; [2] use of any analgesic medication within 24 h prior to and during the study and [3] use of prescribed medicine and/or herbal medicine.
2.2 Heat stimulation
The contact heat stimulation was induced by using the PATHWAY Pain and Sensory Evaluation System (Medoc Ltd, Ramat Yishai, Israel). The standard thermode (contact heat evoked potential stimulator) stimulated a surface area of 6.6 cm2 using a computer controlled OA stimulus paradigm. The thermode was placed on the right volar forearm and moved to a new position in between the two heat stimulations in each session.
The OA paradigm lasted 35 s and consisted of three contiguous phases: T1) An initial temperature increase (6°C/s) to a noxious stimulus temperature (46°C, 5-s duration); T2) a 1°C increase (6°C/s) to a second temperature (47°C, 10-s duration), and then T3) a decrease (6°C/s) back to T1 temperature (46°C, 20-s duration). After T3, the temperature decreased back to baseline (6°C/s).
The constant control stimulus (CTL) paradigm consisted of a constant stimulus temperature of 46°C for 35 s and was used as a control condition for the OA trial to assess adaptation and the pain modulation evoked by the tonic cold pain.
During the heat stimulation sessions, the pain intensity was rated continuously using Medoc’s computerized visual analog scale ranging from 0=“no pain” to 100=“the worst pain imaginable”.
2.3 Cold pressor test
The cold pressor stimulation (Grant, Fischer Scientific, Slangerup, Denmark) was induced by immersing the left hand into the 2°C water up to the wrist for 2 min. After 1 min and 25 s the OA or CTL paradigm started. The cold pressor test was used to induce tonic cold pain.
2.4 Experimental protocol
Each test session lasted approximately 15 min and the two sessions were separated by at least 1 h. Participants were randomized to start with either CTL or OA paradigm and received the other stimulation paradigm in the second session (Fig. 1). Participants and the researcher informing participants and performing the stimulations were blinded to the stimulation protocol.
Flowchart showing the cross-over design. CTL=constant control stimulus; OA=offset-analgesia.
2.5 Statistical analysis
For descriptive analysis, we assessed the number of participants with: (1) decreased VAS rating during the constant temperature in T2 in the OA paradigm; (2) VAS rating decreased to zero during T3 in the OA paradigm, and (3) VAS rating decreased to zero in the CTL paradigm.
Before statistical analyses, the following parameters were calculated for each participant (see Fig. 2A and B):
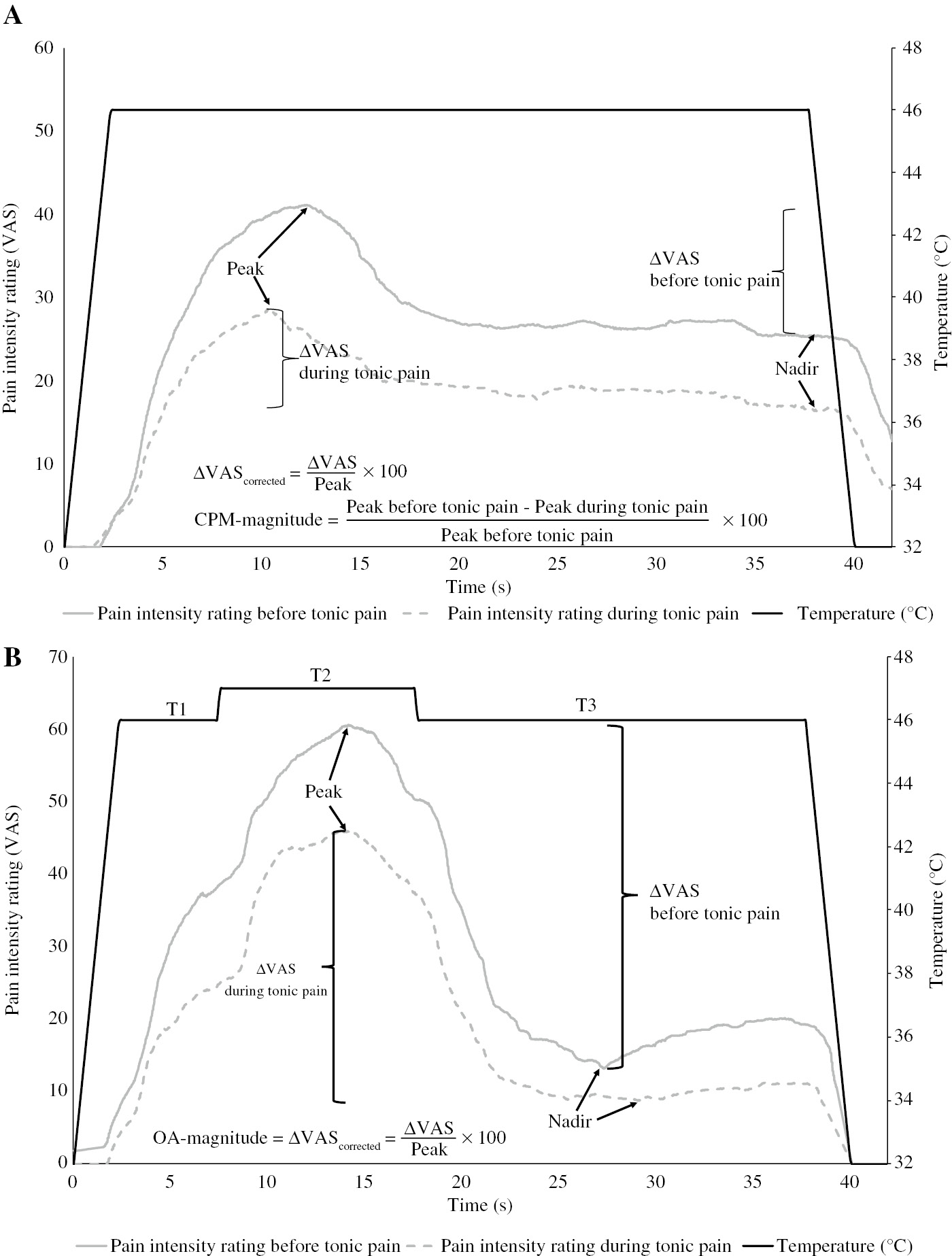
Pain intensity rating in response to heat stimulation. (A) Average pain intensity rating in response to the constant control stimulus (CTL) paradigm before (solid line) and during (dashed line) tonic cold pain. (B) Average pain intensity rating in response to the off-set analgesia stimulus paradigm before (solid line) and during (dashed line) tonic cold pain. VAS=Visual analog scale; CPM=conditioned pain modulation; OA=off-set analgesia.
Peak: maximum VAS rating during the CTL paradigm or within T2 during the OA paradigm).
Nadir: minimum VAS rating after the “Peak” during the CTL paradigm or within T3 during the OA paradigm.
∆VAS: decrease in pain ratings that occurred between peak and nadir (Peak – Nadir).
ΔVAScorrected: ΔVAS normalized with respect to peak value
Additionally, during the CTL paradigm the magnitude of CPM is calculated as the relative difference between the Peak before and during tonic cold pain.
Before analysis all data were visually inspected to secure data quality. Results are listed as means with standard deviations (SD) unless otherwise indicated. Data were analyzed using paired t-test in Stata (Stata 12.1, Stata Corporation, TX, USA). p-Values <0.05 were considered significant.
3 Results
Seventeen participants (8 men and 9 women) with mean age of 30.2±7.1 years were included in the study and all fulfilled the experimental protocol. Hence, results from all participants were included in the analysis.
A descriptive presentation of the VAS responses before tonic cold pain is reported in Table 1. From this analysis, it is apparent that a large portion of the participants had a decrease in VAS rating during the temperature plateau in T2 (65%). Moreover, a large portion of the participants reported a VAS decrease of 100% during T3 of the OA paradigm (76%).
Descriptive analysis of the VAS response, before tonic cold pain.
| n (%) | |
|---|---|
| Participants with decreased VAS rating during T2 in the OA paradigm | 11 (65%) |
| Participants with VAS rating decreased to zero during T3 in the OA paradigm | 13 (76%) |
| Participants with VAS rating decreased to zero in the CTL paradigm | 6 (35%) |
-
n=numbers; VAS=visual analog scale; OA=offset-analgesia; CTL=constant control stimulus.
3.1 Comparison of OA and CTL before tonic cold pain
Comparing adaptation during the CTL paradigm (ΔVAS before tonic pain) with the pain reduction in the OA paradigm (ΔVAS before tonic cold pain) reveals that adaption possibly account for 42.4±27.2% of the pain reduction in the OA paradigm, and that pain reduction in the OA paradigm (52.8±27.0) was significantly larger than adaptation during the CTL paradigm (21.9 ±17.3) (p<0.001).
The OA magnitude (ΔVAScorrected) induced a pain reduction (90.3±23.7%) that was significantly higher than the relative adaption (ΔVAScorrected) seen in the CTL paradigm (57.3±36.6%) (p=0.001).
3.2 The effect of tonic cold pain on OA
Results on OA before and during tonic cold pain are presented in Table 2. Peak pain in the OA paradigm decreased during tonic cold pain compared to before tonic cold pain (p=0.015), which led to a corresponding decrease in ΔVAS (p=0.019). The average magnitude of OA (ΔVAScorrected) at baseline (before tonic pain) was 90.3±23.7%. The average magnitude of OA during tonic cold pain was 89.3±27.6%. Thus, no difference was found in OA magnitude before and during tonic cold pain (p>0.05).
Results from the OA and CS paradigms.
| OA-paradigm |
CTL-paradigm |
|||
|---|---|---|---|---|
| Before tonic pain | During tonic pain | Before tonic pain | During tonic pain | |
| Peak | 61.7±28.8 (0.015)a | 50.0±29.0 | 44.7±24.8 (0.001)a | 31.5±26.1 |
| Nadir | 8.9±23.5 (0.26) | 5.4±12.7 | 22.8±21.0 (0.007)a | 13.6±17.1 |
| ΔVAS | 52.8±27.0 (0.019)a | 44.6±29.2 | 21.9±17.3 (0.29) | 17.8±18.5 |
| ΔVAScorrected | 90.3%±23.7 (0.67) | 89.3%±27.6 | 57.3%±36.6 (0.09) | 67.1%±34.9 |
-
Numbers represents mean VAS rating values ±SD. Values in brackets represents p-values, comparing data from experiment before and during tonic pain. aIndicates p-values below 0.05. VAS=visual analog scale; OA=off-set analgesia; CTL=constant control stimulus; ΔVAScorrected=ΔVAS normalized with respect to peak value. During the OA-paradigm, ΔVAScorrected is a measurement of OA magnitude.
Explorative analysis showed a decrease in pain rating (adaptation) during T2 in the OA paradigm both before and during tonic cold pain (−12.5±16.8 and −10.9±10.6, respectively) (Fig. 2B). There was no significant difference between the decrease seen before and during tonic cold pain (p=0.66).
3.3 The effect of tonic cold pain on CTL
Results on CTL before and during tonic cold pain are presented in Table 2. Peak pain and nadir of CTL decreased during tonic cold pain (p=0.001 and p=0.007, respectively) (Fig. 2A). ΔVAScorrected indicates relative adaptation during the CTL paradigm and was not significantly affected by tonic cold pain (p=0.09).
3.4 Comparison of OA and CPM response
OA magnitude (ΔVAScorrected during OA paradigm) resulted in 90.3±23.7% pain reduction. CPM magnitude assessed during the CTL paradigm resulted in 35.1±32.1% peak pain reduction (Fig. 2A). A significant difference between the magnitude of the OA and CPM responses was found (p<0.001).
4 Discussion
Neither offset analgesia magnitude nor adaptation were modulated by cold pressor induced endogenous analgesia. The cold pressor test only modulated the peak pain reported during the OA (T2 stimulation period) and CTL paradigms as the general pain inhibitory effect.
4.1 Comparison to previous studies
A previous study by Honigman et al. showed an additive effect of tonic pain (CPM) and OA on pain inhibition in males, suggesting that the two mechanisms may at least represent partially different aspects of endogenous descending analgesia [11]. It was suggested that the stronger OA is responsible for a certain set of descending fibers, the more tonic pain (CPM) will activate other fibers, resulting in accumulation of impulses at the spinal level resulting in synergistic inhibitory outcome [11]. However, in the study by Honigman et al. the conditioning stimulation consisted of immersing the non-dominant hand into a hot water bath (46°C) [11]. Additionally, Honigman et al. assessed pain at six specific time points and not continuously. These specific time points may not capture precise peak pain rating and nadir. Hence, a direct comparison to the present study is challenging. By using the cold pressor test and continuously pain rating, the present study will add new aspects to the description of interaction between OA and CPM. In the present study, we also found a significant effect of tonic cold pain on T2 scores. However, by using ΔVAScorrected, our data analysis was corrected for this analgesic effect, which is not related to OA.
The OA magnitude has only been reported in few previous studies [3], [5]. Niesters et al. have reported OA magnitude of 91–96.2% [5], which is comparable to our findings where OA magnitude was 90.3%. Another study by Naugle and Riley showed an OA magnitude of 69.2–75.5% [14]. However, as their study was conducted in 18–76 years old healthy people, age may have affected the results. Other previous studies did not report Peak, Nadir and ΔVAScorrected values, thus comparison is difficult [7], [11], [15], [16], [17]. Especially peak values may be relevant as we saw that the effect of tonic cold pain on OA was only related to the peak value and not the OA magnitude. Thus, future studies should report at least peak, nadir, ΔVAS and ΔVAScorrected for proper interpretation of results.
4.2 Spatial versus temporal filtering of pain
The “pain inhibits pain” phenomenon in CPM represents spatial filtering of pain whereas OA as an inhibitory processing mechanism reflects temporal filtering of sensory information [16]. Thus, a previous study investigated if spatial filtering of nociceptive information is accomplished by mechanisms that are similar to those engaged by temporal filtering of noxious information. It was found that spatial and temporal filtering of nociceptive information instantiated by CPM and OA represent dissociable analgesic phenomena that modulate afferent nociceptive information processing in different ways [16]. Additionally, it was shown that brain activation during CPM was markedly distinct from that during OA [16]. It was suggested that the OA brain activation mirrors the activity of brain regions engaged in the modulation of pain by cognitive processes related to the prediction of the time course of pain [16]. Our study showed a larger magnitude of OA compared to CPM, indicating that the temporal filtering and modulation of pain by cognitive processes is more pronounced than the spatial filtering of pain by CPM. However, as calculation of OA and CPM are based on different aspects of the pain rating, direct comparison between magnitude of OA and CPM can be difficult.
4.3 Central vs. peripheral phenomenon
It is debatable if OA is a peripheral or central phenomenon. Peripheral changes may also explain the OA response and it has been demonstrated that peripheral fibers alone can provide the information necessary to detect noxious stimuli and to encode intensity of pain elicited by fluctuating noxious stimuli. Therefore, it has been suggested that the observed effects may be due to changes in the periphery rather than in the brain [17]. A recent study showed that OA could be elicited when the stimuli were applied both to the same and to different locations indicating that peripheral as well as central mechanisms are involved in mediating OA [15]. However, the traditional unilaterally generated OA, within the same dermatome, was the most potent [15]. The present study was not designed to distinguish between peripheral and central mechanisms, thus no further support can be added to this aspect.
4.4 Methodological considerations
We chose to include the CTL paradigm, as it was included in the first studies of OA [1], [7], and lately inclusion of the constant stimulus paradigm in a study of OA has demonstrated that adaptation contributes to ΔVAScorrected [13]. Thus, a constant stimulus paradigm was included to assess the magnitude of adaptation and for the first time to evaluate if cold pressor modulation affected adaptation differently from OA. Results showed that adaptation (during the CTL paradigm) was not affected by the tonic cold pain. Adaptation (CTL paradigm) accounted for 41% of the decrease in VAS rating seen during the OA paradigm. Therefore, our results demonstrated the importance of including a control paradigm in future studies to differentiate between OA and adaptation.
A previous study showed that the paradigm 48-49-48°C (T1-T2-T3) resulted in frequent intolerability and led participants to drop out of the experiment [13]. Therefore, the present study used slightly lower temperatures of 46-47-46°C. The applied temperatures resulted in mean peak VAS scoring of 61.7 in T2, thus, the stimuli were clearly painful.
It has been demonstrated that the T2 duration affects magnitude of OA both in healthy participants and in patients, where a longer T2 enhanced OA magnitude [13]. Thus, it was proposed that OA requires sufficient temporal summation of pain by thermal stimulus before offset. Therefore, in the present study a T2 duration of 10 s was used. However, using this duration, it was seen that adaptation, assessed as decreased pain rating during T2, occurred in 65% of the participants. It has been demonstrated that part of the apparent OA effect is due to with-in session adaptation, and similar to our results, about 40–45% of the observed OA effect were possibly caused by the effects of within-session adaptation [17]. Recently, adaptation during T2 has also been demonstrated [13]. It was suggested that adaptation may add to increased ΔVAScorrected, but OA was still significantly larger than adaptation during constant temperature stimulation [13]. This was confirmed in our study where we found that the magnitude of OA was significantly larger than adaptation in the CTL paradigm.
It has been demonstrated that repeated stimulation with noxious heat at the same site can lead to long-term attenuation of pain perception [18]. Therefore, in the present study, the thermode was repositioned after each test although kept in the same area of the volar forearm. However, it was previously suggested [16] that the probable plasticity underlying these perceptual changes occurred in cerebral areas. Thus, if the attenuation has a central cause, repositioning the thermode within the same region of the arm, may not exclude attenuation. Contrary to these findings another study did not find any evidence of across session attenuation [17]. The present study included a control stimulus and was randomized, thus if attenuation between tests affected results, the effect should be similar in CS and OA paradigm.
Previous studies have used different methods to assess the OA effect. Some have quantified the magnitude of OA by subtracting minimal VAS values obtained during T3 from the maximal VAS values during T2 [2], [19]. Others have used the minimum VAS within the first 10 s. in T3 for the same calculation [13]. Others have calculated the ∆VAScorrected (magnitude of OA) relative to peak VAS which corrects for the variation in the peak response among participants [3], [5]. The corrected values were used in the present analysis and demonstrated that the OA magnitude was 90% before any modulation and 76% of participants had an OA magnitude of 100%.
4.5 Clinical significance
From the present and previous findings on modulation of OA, it appears that OA is mainly affected by deficiencies in the pain system [5], [6] and not by pharmacological or physiological modulation [3]. Thus, OA may be used to evaluate pain patients and modulation of OA may be possible in patients where the OA magnitude is reduced. However, as OA magnitude is at maximum in healthy participants it seems unaffected by modulation induced by experimental methods or pharmacology. Thus, mechanisms behind OA remains inexplicable.
In conclusion, offset analgesia magnitude was not modulated by cold pressor induced endogenous analgesia. This may indicate the two pain modulatory mechanisms utilize different pain modulatory pathways or be caused by methodological limitations, as offset analgesia magnitude was close to 100% before any modulation.
-
Authors’ statements
-
Research funding: The study received no funding. Professor L. Arendt-Nielsen was supported by The Shionogi Science Program and TaNeDS Europe.
-
Conflict of interest: TDN, CDM, LAN, AMD and AEO declare no conflicts of interest.
-
Informed consent: Written informed consents were obtained from participants before the study procedures.
-
Ethical approval: The study was carried out according to the recommendations of the Helsinki declaration (2013) and approved by The North Denmark Region Committee on Health Research Ethics (N-2009008).
References
[1] Grill JD, Coghill RC. Transient analgesia evoked by noxious stimulus offset. J Neurophysiol 2002;87:2205–8.10.1152/jn.00730.2001Search in Google Scholar PubMed
[2] Martucci KT, Eisenach JC, Tong C, Coghill RC. Opioid-independent mechanisms supporting offset analgesia and temporal sharpening of nociceptive information. Pain 2012;153:1232–43.10.1016/j.pain.2012.02.035Search in Google Scholar PubMed PubMed Central
[3] Niesters M, Dahan A, Swartjes M, Noppers I, Fillingim RB, Aarts L, Sarton EY. Effect of ketamine on endogenous pain modulation in healthy volunteers. Pain 2011;152:656–63.10.1016/j.pain.2010.12.015Search in Google Scholar PubMed
[4] Niesters M, Proto PL, Aarts L, Sarton EY, Drewes AM, Dahan A. Tapentadol potentiates descending pain inhibition in chronic pain patients with diabetic polyneuropathy. Br J Anaesth 2014;113:148–56.10.1093/bja/aeu056Search in Google Scholar PubMed
[5] Niesters M, Hoitsma E, Sarton E, Aarts L, Dahan A. Offset analgesia in neuropathic pain patients and effect of treatment with morphine and ketamine. Anesthesiology 2011;115:1063–71.10.1097/ALN.0b013e31822fd03aSearch in Google Scholar PubMed
[6] Oudejans LCJ, Smit JM, van Velzen M, Dahan A, Niesters M. The influence of offset analgesia on the onset and offset of pain in patients with fibromyalgia. Pain 2015;156:2521–7.10.1097/j.pain.0000000000000321Search in Google Scholar PubMed
[7] Yelle MD, Rogers JM, Coghill RC. Offset analgesia: a temporal contrast mechanism for nociceptive information. Pain 2008;134:174–86.10.1016/j.pain.2007.04.014Search in Google Scholar PubMed PubMed Central
[8] Yelle MD, Oshiro Y, Kraft RA, Coghill RC. Temporal filtering of nociceptive information by dynamic activation of endogenous pain modulatory systems. J Neurosci 2009;29:10264–71.10.1523/JNEUROSCI.4648-08.2009Search in Google Scholar PubMed PubMed Central
[9] Pud D, Granovsky Y, Yarnitsky D. The methodology of experimentally induced diffuse noxious inhibitory control (DNIC)-like effect in humans. Pain 2009;144:16–9.10.1016/j.pain.2009.02.015Search in Google Scholar PubMed
[10] Hermans L, Calders P, Van Oosterwijck J, Verschelde E, Bertel E, Meeus M. An overview of offset analgesia and the comparison with conditioned pain modulation: a systematic literature review. Pain Physician 2016;19:307–26.10.36076/ppj/2016.19.307Search in Google Scholar
[11] Honigman L, Yarnitsky D, Sprecher E, Weissman-Fogel I. Psychophysical testing of spatial and temporal dimensions of endogenous analgesia: conditioned pain modulation and offset analgesia. Exp Brain Res 2013;228:493–501.10.1007/s00221-013-3580-7Search in Google Scholar PubMed
[12] Oono Y, Wang K, Svensson P, Arendt-Nielsen L. Conditioned pain modulation evoked by different intensities of mechanical stimuli applied to the craniofacial region in healthy men and women. J Orofac Pain 2011;25:364–75.Search in Google Scholar
[13] Kobinata H, Ikeda E, Zhang S, Li T, Makita K, Kurata J. Disrupted offset analgesia distinguishes chronic pain patients from healthy controls. Pain 2017;158:1951–9.10.1097/j.pain.0000000000000989Search in Google Scholar PubMed
[14] Naugle KM, Cruz-Almeida Y, Fillingim RB, Riley JL. Offset analgesia is reduced in older adults. Pain 2013;154: 2381–7.10.1016/j.pain.2013.07.015Search in Google Scholar PubMed PubMed Central
[15] Ligato D, Petersen KK, Mørch CD, Arendt-Nielsen L. Offset analgesia: the role of peripheral and central mechanisms. Eur J Pain 2018;22:142–9.10.1002/ejp.1110Search in Google Scholar PubMed
[16] Nahman-Averbuch H, Martucci KT, Granovsky Y, Weissman-Fogel I, Yarnitsky D, Coghill RC. Distinct brain mechanisms support spatial vs temporal filtering of nociceptive information. Pain 2014;155:2491–501.10.1016/j.pain.2014.07.008Search in Google Scholar PubMed PubMed Central
[17] Derbyshire SWG, Osborn J. Enhancement of offset analgesia during sequential testing. Eur J Pain 2008;12:980–9.10.1016/j.ejpain.2008.01.008Search in Google Scholar PubMed
[18] Gallez A, Albanese M-C, Rainville P, Duncan GH. Attenuation of sensory and affective responses to heat pain: evidence for contralateral mechanisms. J Neurophysiol 2005;94:3509–15.10.1152/jn.01006.2004Search in Google Scholar PubMed
[19] Suzan E, Treister R, Pud D, Haddad M, Eisenberg E. The effect of hydromorphone therapy on psychophysical measurements of the descending inhibitory pain systems in patients with chronic radicular pain. Pain Med (United States) 2015;16:168–75.10.1111/pme.12565Search in Google Scholar PubMed
©2018 Scandinavian Association for the Study of Pain. Published by Walter de Gruyter GmbH, Berlin/Boston. All rights reserved.
Articles in the same Issue
- Frontmatter
- Editorial comment
- Support for mirror therapy for phantom and stump pain in landmine-injured patients
- Lifting with straight legs and bent spine is not bad for your back
- Bipolar radiofrequency neurotomy for spinal pain – a promising technique but still some steps to go
- Topical review
- Prevalence, localization, perception and management of pain in dance: an overview
- Clinical pain research
- Pain assessment in native and non-native language: difficulties in reporting the affective dimensions of pain
- Colored body images reveal the perceived intensity and distribution of pain in women with breast cancer treated with adjuvant taxanes: a prospective multi-method study of pain experiences
- Physiotherapy pain curricula in Finland: a faculty survey
- Mirror therapy for phantom limb and stump pain: a randomized controlled clinical trial in landmine amputees in Cambodia
- Pain and alcohol: a comparison of two cohorts of 60 year old women and men: findings from the Good Aging in Skåne study
- Prolonged, widespread, disabling musculoskeletal pain of adolescents among referrals to the Pediatric Rheumatology Outpatient Clinic from the Päijät-Häme Hospital District in southern Finland
- Impact of the economic crisis on pain research: a bibliometric analysis of pain research publications from Ireland, Greece, and Portugal between 1997 and 2017
- Measurement of skin conductance responses to evaluate procedural pain in the perioperative setting
- Original experimental
- An observational study of pain self-management strategies and outcomes: does type of pain, age, or gender, matter?
- Fibromyalgia patients and healthy volunteers express difficulties and variability in rating experimental pain: a qualitative study
- Effect of the market withdrawal of dextropropoxyphene on use of other prescribed analgesics
- Observational study
- Winning or not losing? The impact of non-pain goal focus on attentional bias to learned pain signals
- Gabapentin and NMDA receptor antagonists interacts synergistically to alleviate allodynia in two rat models of neuropathic pain
- Offset analgesia is not affected by cold pressor induced analgesia
- Central and peripheral pain sensitization during an ultra-marathon competition
- Reduced endogenous pain inhibition in adolescent girls with chronic pain
- Evaluation of implicit associations between back posture and safety of bending and lifting in people without pain
- Assessment of CPM reliability: quantification of the within-subject reliability of 10 different protocols
- Cerebrospinal fluid cutaneous fistula after neuraxial anesthesia: an effective treatment approach
- Pain in the hand caused by a previously undescribed mechanism with possible relevance for understanding regional pain
- The response to radiofrequency neurotomy of medial branches including a bipolar system for thoracic facet joints
- Letter to the Editor
- Diagnosis of carpal tunnel syndrome – implications for therapy
- Reply to the Letter to the Editor by Ly-Pen and Andréu
- Letter to the Editor regarding “CT guided neurolytic blockade of the coeliac plexus in patients with advanced and intractably painful pancreatic cancer”
- Reply to comments from Ulf Kongsgaard to our study
Articles in the same Issue
- Frontmatter
- Editorial comment
- Support for mirror therapy for phantom and stump pain in landmine-injured patients
- Lifting with straight legs and bent spine is not bad for your back
- Bipolar radiofrequency neurotomy for spinal pain – a promising technique but still some steps to go
- Topical review
- Prevalence, localization, perception and management of pain in dance: an overview
- Clinical pain research
- Pain assessment in native and non-native language: difficulties in reporting the affective dimensions of pain
- Colored body images reveal the perceived intensity and distribution of pain in women with breast cancer treated with adjuvant taxanes: a prospective multi-method study of pain experiences
- Physiotherapy pain curricula in Finland: a faculty survey
- Mirror therapy for phantom limb and stump pain: a randomized controlled clinical trial in landmine amputees in Cambodia
- Pain and alcohol: a comparison of two cohorts of 60 year old women and men: findings from the Good Aging in Skåne study
- Prolonged, widespread, disabling musculoskeletal pain of adolescents among referrals to the Pediatric Rheumatology Outpatient Clinic from the Päijät-Häme Hospital District in southern Finland
- Impact of the economic crisis on pain research: a bibliometric analysis of pain research publications from Ireland, Greece, and Portugal between 1997 and 2017
- Measurement of skin conductance responses to evaluate procedural pain in the perioperative setting
- Original experimental
- An observational study of pain self-management strategies and outcomes: does type of pain, age, or gender, matter?
- Fibromyalgia patients and healthy volunteers express difficulties and variability in rating experimental pain: a qualitative study
- Effect of the market withdrawal of dextropropoxyphene on use of other prescribed analgesics
- Observational study
- Winning or not losing? The impact of non-pain goal focus on attentional bias to learned pain signals
- Gabapentin and NMDA receptor antagonists interacts synergistically to alleviate allodynia in two rat models of neuropathic pain
- Offset analgesia is not affected by cold pressor induced analgesia
- Central and peripheral pain sensitization during an ultra-marathon competition
- Reduced endogenous pain inhibition in adolescent girls with chronic pain
- Evaluation of implicit associations between back posture and safety of bending and lifting in people without pain
- Assessment of CPM reliability: quantification of the within-subject reliability of 10 different protocols
- Cerebrospinal fluid cutaneous fistula after neuraxial anesthesia: an effective treatment approach
- Pain in the hand caused by a previously undescribed mechanism with possible relevance for understanding regional pain
- The response to radiofrequency neurotomy of medial branches including a bipolar system for thoracic facet joints
- Letter to the Editor
- Diagnosis of carpal tunnel syndrome – implications for therapy
- Reply to the Letter to the Editor by Ly-Pen and Andréu
- Letter to the Editor regarding “CT guided neurolytic blockade of the coeliac plexus in patients with advanced and intractably painful pancreatic cancer”
- Reply to comments from Ulf Kongsgaard to our study