
Unsupervised short leave in forensic addiction treatment: Is there an influence on treatment progress?
-
Louisa Neumann
Louisa Neumann, M. Sc., is a clinical psychologist at the Clinic for Forensic Psychiatry and Psychotherapy in Wunstorf, Germany. Her research focuses on the treatment of individuals who committed offences.

 und
Merten Neumann
und
Merten Neumann
Merten Neumann, Dipl.-Psych., is a research associate at the Criminological Research Institute of Lower Saxony (KFN). His research focuses on different aspects of the correctional system with a special emphasis on risk prediction procedures in forensic mental health institutions.

Abstract
Short leave is an integral part of forensic addiction treatment in Germany. Individuals with addiction problems who have offended can be admitted to forensic addiction treatment institutions to receive treatment for their addiction disorder and reduce their risk of reoffending. During this treatment, short leave is implemented to allow the practising of an abstinent lifestyle, enhance treatment motivation, and enable the individual to stay connected with the community. A critical step is the unsupervised short leave, which comes with benefits but also risks for the individual and the community. Short leave (especially unsupervised short leave) bears the risk of incidents such as new offences, drug relapses or absconding. This study examines the influence of unsupervised short leave on treatment progress. It builds on the methodology from a previous study of patients in forensic psychiatric hospitals and uses a pre-post design with follow-up. Furthermore, the impact of incidents during short leave on treatment progress is analysed. The sample consists of 157 patients in forensic addiction treatment in Germany. The results suggest that unsupervised short leave can enhance the treatment progress of patients in forensic addiction treatment. However, incidents during short leave can have a negative effect on treatment progress.
1 Introduction
Based on Section 64 of the German criminal code (»Strafgesetzbuch«), individuals who have addiction problems and have offended can be admitted to forensic addiction treatment (FAT). The preconditions for this placement are a habit of consuming alcohol or another intoxicating substance, a relation between the substance abuse and the offence, a risk of reoffending due to the habit of consumption, and sufficiently reasonable prospects that treatment can reduce the risk of reoffending. The maximum duration of placement in FAT is two years (Section 67d of the German criminal code). If there is an additional prison sentence, then the FAT is implemented before the sentence unless the court determines that the prison sentence should be enforced first. This is usually the case when the ordered prison sentence is more than three years (Section 67 of the German criminal code). The number of admissions to FAT is continuously increasing, with about 4500 patients treated in FAT institutions in 2021 (Müller et al., 2021).
Section 64 of the German criminal code also defines the goal of FAT: curing the patient of their habit of consuming illicit substances or alcohol, or at least discouraging consumption for a significant period of time. It also aims to prevent patients from committing significant criminal offences due to their addiction.
There are three release modes of FAT, which are defined by the legislator. The first release mode results in the release of the patient on parole. This is applied when the patient receives a positive prognosis regarding future law-abiding behaviour, which points to a successful treatment. The second release mode comes into force when the patient has reached the legally defined maximum time limit of treatment in FAT, which is two years. The third release mode is an end of the accommodation due to a lack of prospect of success, often resulting in a transfer of the patient to prison. Thus, it implies an unsuccessful treatment. Unfortunately, this is the case for about half of the patients undergoing FAT (Müller et al., 2021).
1.1 Short leave in FAT
In Germany, detained individuals who have committed offences may be granted periods of short leave, also known as temporary absence, under certain circumstances and for a predetermined time period (Köhne & Lesting, 2012). The legal provision of short leave is applicable not only in correctional facilities but also in forensic psychiatric hospitals and FAT institutions as per the German prison act (»Strafvollzugsgesetz«), with individual implementation by the different federal states and their regulatory frameworks. The use of short leave is an essential component of both the treatment and gradual release processes (Müller, Saimeh, et al., 2017). In general, a prerequisite for short leave is that the patients are not expected to abuse their leave privileges (e. g., for absconding or new offences; Köhne & Lesting, 2012).
There are different types of short leave, which are completed by the patient in a step-by-step plan, beginning with minor freedoms granted (e. g., leaving with two staff members) and leading to the opportunity for home leave (Müller, Nedopil, et al., 2017; Neumann et al., 2019; Pollähne, 2018). It is possible to skip or alter some steps depending on the patient’s needs. An important step is the unsupervised short leave, which allows the patient to leave the hospital without a staff member for a fixed period and radius.
1.2 The potential benefits of short leave for individuals in FAT
Short leave is an important therapeutic tool for practising an abstinent lifestyle during FAT (Bezzel, 2008). Furthermore, short leave can allow patients in secure hospitals to remain connected with their community, work, receive an education and practice daily living skills (Walker et al., 2013).
It is assumed that the prospect of short leave can increase the motivation of the patient to participate in therapy (Müller, Nedopil, et al., 2017; Suhling et al., 2015). Results from a pre-post study with forensic psychiatric patients (admission based on Section § 63 of the German criminal code) indicate that granting unsupervised short leave is associated with an increase in the patient’s treatment progress, as rated by therapists (Neumann & Bauer, 2022).
These first findings are in line with theoretical assumptions about influences on the treatment readiness of individuals who have offended, such as those of the multifactor offender readiness model (MORM; Ward et al., 2004). The MORM model proposes that treatment readiness is a function of internal (person) factors and external (context) factors. The internal factors relate to the characteristics of the patient, such as behavioural properties (e. g., possessing basic communication and social skills) or the volitional state (e. g., motivation to change). The external factors refer primarily to characteristics of the treatment setting, such as the location of the treatment (prison vs community treatment) or program characteristics (program type). When internal and external factors combine in a favourable manner, a person’s readiness is enhanced, which ultimately results in increased program engagement and performance. Short leave may be able to positively influence the patient’s internal factors (e. g., by increasing motivation).
1.3 The potential risks of short leave
Short leave involves the risk of incidents happening while the patient is away. Such incidents during short leave (ISLs) are often broadly defined as types of behaviour that might disrupt the treatment progress, such as the abuse of alcohol or drugs, or more serious problematic behaviour, such as absconding or new offences (Neumann et al., 2019). A survey by Berthold and Riedemann (2021) with 17 participating FAT institutions in Germany treating 1703 patients showed that serious ISLs are quite rare. In 2021, 1132 patients had permission to leave the facility supervised or unsupervised. Only 35 (3.1 %) of these 1132 patients failed to return from short leave. In addition, only 23 (1.3 %) of all 1703 patients escaped or absconded (for more details about the classification, see Hearn et al., 2012). In total, these 58 patients caused 70 events with 13 new offences. Therefore, based on there being 1703 patients in the survey, only 0.76 % of the patients committed a new offence. This indicates that the risk of new crimes during short leave is low.
Some empirical findings suggest ISLs may have a negative impact on the patients themselves. A previous study by Neumann and Bauer (2022) with forensic psychiatric patients (admission based on section 63 of the German criminal code) indicated that ISLs can be associated with a decrease in therapist-rated treatment progress. Moreover, a study by Gericke and Kallert (2007) found that absconding during FAT is the strongest predictor of an end to the accommodation due to a lack of prospect of success. Bezzel (2008) identified the following as reasons for the termination of FAT: absconding, drug relapsing, using violence and committing offences. In line with the findings of Bezzel (2008), a survey by Querengässer (2014) with 35 therapists working in FAT in Baden-Wurttemberg found that reasons for termination of FAT included drug relapse, absconding and violent behaviour, among others. Lastly, the prospect of remaining offence-free after release is worse with continuous drug consumption during FAT (Bezzel, 2010).
It should be noted that the consumption of illicit substances happens not only on short leave but also inside the facility. A review by Norman (2022) concluded that an important drug smuggling route into prisons is available to prisoners upon release. To the best of our knowledge, there has been no study investigating drug smuggling into FAT institutions. However, it should be reasonable that the possibilities are similar to those in prisons. Furthermore, the survey by Berthold and Riedemann (2021) showed that half of the offences committed during absconding events are violations of German narcotics law (e. g., buying illicit substances). Therefore, it seems possible that short leave presents the opportunity for the patient to not only buy and consume drugs but also smuggle them back into the facility.
However, the above findings should be viewed with caution because none of the studies allows the establishment of a direct causal relationship between incidents such as absconding or substance abuse and termination of FAT. There are several possible explanations for the observed relationship. For example, it could be that patients who are prone to rule-breaking behaviour also possess unfavourable preconditions for FAT (such as antisocial personality disorder), which lead to an end of the accommodation due to a lack of prospect of success. Furthermore, it could be that the negative impact of an ISL on treatment progress is not directly due to the disruptive behaviour of the patient but to a failure to properly address the incident in treatment.
1.4 The present study
Although there is a risk of incidents, short leave from FAT institutions can serve as an important tool for practising an abstinent lifestyle outside of the institution, strengthening the rehabilitation of the patients and motivating them to continue treatment (Bezzel, 2008; Suhling et al., 2015; Walker et al., 2013). However, the potential benefits of short leave in FAT have not been sufficiently explored. Hence, the current study aims to investigate the influence of short leave on treatment progress and the impact of incidents during short leave. The first hypothesis is that unsupervised short leave has a positive effect on treatment progress for patients without an ISL, which means that the ratings of indicators of treatment progress will improve after permission for short leave is granted if no ISL is recorded. The second hypothesis is that incidents during unsupervised short leave will negatively impact treatment progress, with the ratings of indicators of treatment progress declining following an incident.
It should be noted that this study investigates a similar research question and uses the same methodological approach as our previous study with patients in forensic psychiatric hospitals (Neumann & Bauer, 2022). The main difference between the previous and the current study lies in the sample. There are discrepancies between the treatment in forensic psychiatric hospitals and FAT in terms of legal aspects. For example, the maximum duration of placement in FAT is two years, while the placement in forensic psychiatric hospitals is potentially unlimited (Section 67d of the German criminal code). This impacts the pace of FAT, as the duration of accommodation is a time constraint for the treatment. Therefore, leave is implemented earlier in FAT than in forensic psychiatric hospitals (Neumann et al., 2019). Furthermore, for patients to be admitted, there must be sufficiently reasonable prospects that FAT can reduce the risk of reoffending (Section 64 of the German criminal code). This is not a requirement for admission to a forensic psychiatric hospital (Section 63 of the German criminal code). Given these differences between the treatment in forensic psychiatric hospitals and FAT, we argue that it is reasonable to reexamine our research question in this context.
2 Method
2.1 Data collection
The current study draws upon data obtained from a research project conducted by the Criminological Research Institute of Lower Saxony (Neumann et al., 2019; funded by the Ministry of Social Affairs of Lower Saxony). The data utilized in this study were originally gathered and stored by the seven mental health institutions in Lower Saxony that treat patients who are admitted based on Section 64 of the German criminal code. This study utilized data from a comprehensive group of patients in FAT who underwent external risk assessments by a so-called prognosis team[1] as part of their application process for unsupervised short leave between 2006 and 2016 (N = 207). Patients who were admitted to FAT because of a homicide or a sexual offence must be assessed by a prognosis team before granting them unsupervised short leave for the first time. Furthermore, the FAT institutions can request a prognosis team if they deem it necessary, and they are especially encouraged to do so if the initial offence was a violent offence or posed a danger to the public (e. g., in the case of arson).[2] It is important to note that this means that the sample is not representative of the population of patients in FAT in general. The study sample consisted of those 178 patients who were granted short leave. Once granted permission, patients were allowed to take unsupervised short leave with predetermined restrictions (e. g., one hour twice per week). We know that the patients took their chance to leave the institution unsupervised at some point, but unfortunately, the frequency of their leaving remains unknown.
For the risk assessment, the patients’ main therapists completed a questionnaire containing demographic variables as well as static and dynamic risk and protective factors, including questions about the treatment progress (no validated instruments are included; the complete questionnaire can be found in Neumann et al., 2019). Whenever a patient was authorized for unsupervised short leave from the institution, the questionnaire on treatment progress was administered again following each of two consecutive six-month intervals. Furthermore, any instances of rule-breaking behaviour during the short leave were recorded at both the six-month and twelve-month measurement points. Consequently, the data set comprises three measurement points that provide insights into indicators of treatment progress: t0 = before permission for unsupervised short leave (pretest), t1 = six months after permission for unsupervised short leave (posttest), t2 = twelve months after permission for unsupervised short leave (follow-up). The data set also includes two points of measurement for incidents during short leave (t1, t2).
2.2 Sample
In our sample of 178 patients, a total of 21 individuals were excluded due to missing data regarding treatment progress or incidents that occurred during short leave. Among these exclusions, seven participants had not yet reached the minimum one-year timeframe required since the risk assessment at the time of data collection. Twelve were excluded because they were not granted the opportunity for short leave during the second timeframe. For the remaining two patients, the reasons for the missing data could not be ascertained. The lack of data may be due to various scenarios, such as a patient transfer to a different federal state, a complete withdrawal of leave privileges (which also applies to the 12 patients without short leave in the second timeframe), or a patient death. Consequently, the final data set used for the analysis consisted of data obtained from 157 patients.
The patients in the final sample ranged in age from 19 to 70 years (M = 37.60; SD = 10.45), and most of them were male (98 %). The most common types of diagnoses were substance use disorders (F1X; 99 %). Here, diagnoses concerning alcohol consumption were the most frequent (F10; 71 %). A large proportion of patients had multiple substance use disorders (F19; 32 %). Less frequent were disorders related to cannabis use (F12; 13 %), cocaine use (F14; 10 %) and opioid use (F11; 5 %). Other relevant diagnoses were dissocial personality disorders (F60.2; 17 %) and mixed personality disorders (F61; 13 %). Common offences were minor assault[3] (48.4 %), aggravated assault[4] (46.5 %), sexual offences[5] (34.4 %) and homicide[6] (36.9 %).[7]
2.3 Measures
2.3.1 Dependent variable
The objective of this study is to evaluate the progress of FAT following the authorization of unsupervised short leave for patients. In this context, treatment progress refers to a positive transformation observed in patients within the therapeutic framework, such as changes in treatment readiness and engagement (Drieschner & Verschuur, 2010). The dependent variable is the Scale of Treatment Progress, which consists of five items (see Table 1)[8] derived from a questionnaire that was filled out by the main therapists at each time of measurement. The ratings were made on a 5-point rating scale (very low = 1 – very high = 5) and the final scale was computed as the mean of the five items. For more information on the theoretical derivation of the Scale of Treatment Progress, see Neumann and Bauer (2022). Table 2 shows a correlation matrix of the items for all three points of measurement. To test the unidimensionality assumption across all three points of measurement (including longitudinal measurement invariance regarding the measurement model and factor loadings; see Brown, 2015; Kline, 2011), we used a confirmatory factor analysis (robust DWLS estimator using the R-package lavaan; Rosseel, 2012; version 0.6–12). The resulting fit indices support a one-factor model (RMSEA: .026; SRMR: .047; CFI: .998; TLI: .997; see Hu & Bentler, 1999), fit for interpretation regarding multiple points of measurement (differences to model with no restrictions on factor loadings: Δdf: 8; ΔRMSEA: –.003; ΔSRMR: .003; ΔCFI: .000; ΔTLI: .001; see Chen, 2007). The internal consistency of the scale was investigated with ω-coefficients based on polychoric correlations using the package psych (Revelle, 2017). The scale shows good internal consistency regarding both omega total (ωtot,t0 = .89; ωtot,t1 = .93; ωtot,t2 = .94) and omega hierarchical (ωh,t0 = .74; ωh,t1 = .88; ωh,t2 = .91) for all three points of measurement.
Items of the Scale of Treatment Progress.
|
Items |
||
|
#1 |
Progress |
Progress of the treatment since the start of the confinement |
|
#2 |
Contact |
Contact with the patient in daily therapeutic practice |
|
#3 |
Cooperation |
Actual cooperation in treatment and day-to-day correctional routines |
|
#4 |
Motivation |
Motivation regarding treatment |
|
#5 |
Insight |
Insight into one’s illness |
2.3.2 Independent variables
Our first independent variable was the time of measurement. To investigate the influence of short leave on treatment progress, we analyzed the change in treatment progress over three points in time: t0 = before permission for unsupervised short leave (pretest), t1 = six months after permission for unsupervised short leave (posttest), t2 = twelve months after permission for unsupervised short leave (follow-up).
Correlation matrix for the items of the Scale of Treatment Progress using the Pearson correlation coefficient.
|
t0 |
t1 |
t2 |
||||||||||||||||
|
#1 |
#2 |
#3 |
#4 |
#5 |
#1 |
#2 |
#3 |
#4 |
#5 |
#1 |
#2 |
#3 |
#4 |
#5 |
||||
|
t0 |
||||||||||||||||||
|
#1 |
Progress |
– |
– |
– |
– |
– |
– |
– |
– |
– |
– |
– |
– |
– |
– |
– |
||
|
#2 |
Contact |
.41 |
– |
– |
– |
– |
– |
– |
– |
– |
– |
– |
– |
– |
– |
– |
||
|
#3 |
Cooperation |
.46 |
.49 |
– |
– |
– |
– |
– |
– |
– |
– |
– |
– |
– |
– |
– |
||
|
#4 |
Motivation |
.44 |
.38 |
.57 |
– |
– |
– |
– |
– |
– |
– |
– |
– |
– |
– |
– |
||
|
#5 |
Insight |
.45 |
.28 |
.48 |
.46 |
– |
– |
– |
– |
– |
– |
– |
– |
– |
– |
– |
||
|
t1 |
||||||||||||||||||
|
#1 |
Progress |
.27 |
.14 |
.15 |
.14 |
.18 |
– |
– |
– |
– |
– |
– |
– |
– |
– |
– |
||
|
#2 |
Contact |
.09 |
.38 |
.23 |
.25 |
.19 |
.51 |
– |
– |
– |
– |
– |
– |
– |
– |
– |
||
|
#3 |
Cooperation |
.13 |
.18 |
.34 |
.28 |
.27 |
.57 |
.54 |
– |
– |
– |
– |
– |
– |
– |
– |
||
|
#4 |
Motivation |
.18 |
.23 |
.33 |
.35 |
.29 |
.59 |
.62 |
.72 |
– |
– |
– |
– |
– |
– |
– |
||
|
#5 |
Insight |
.26 |
.25 |
.27 |
.26 |
.40 |
.61 |
.48 |
.56 |
.65 |
– |
– |
– |
– |
– |
– |
||
|
t2 |
||||||||||||||||||
|
#1 |
Progress |
.10 |
.05 |
.08 |
.10 |
.14 |
.38 |
.27 |
.34 |
.39 |
.35 |
– |
– |
– |
– |
– |
||
|
#2 |
Contact |
.00 |
.13 |
.09 |
.08 |
.15 |
.30 |
.40 |
.29 |
.38 |
.33 |
.50 |
– |
– |
– |
– |
||
|
#3 |
Cooperation |
.05 |
.05 |
.18 |
.18 |
.21 |
.32 |
.32 |
.47 |
.47 |
.35 |
.71 |
.59 |
– |
– |
– |
||
|
#4 |
Motivation |
.17 |
.10 |
.23 |
.31 |
.30 |
.36 |
.30 |
.42 |
.52 |
.43 |
.74 |
.61 |
.81 |
– |
– |
||
|
#5 |
Insight |
.08 |
.06 |
.11 |
.22 |
.26 |
.36 |
.32 |
.36 |
.45 |
.47 |
.71 |
.50 |
.71 |
.76 |
– |
||
Note: Significant correlations in bold (p < .05)
Our second independent variable was the occurrence of an ISL during short leave. ISLs had been recorded at t1 and t2 for the preceding six months by the main therapists (see Table 3 for the list of incidents). We formed binary variables for ISLs at t1 and t2 for descriptive analyses. We also created a categorical variable with the levels No incidents (no ISL was recorded), 0–6 months (at least one type of ISL was recorded at t1), 7–12 months (at least one type of ISL was recorded at t2), and Both (at least one type of ISL was recorded at t1 and t2) for the main analysis.
List of potential incidents during short leave that were queried by the main therapists.
|
ISL |
|
|
#1 |
Violation of communication requirements (e. g., not answering the phone) |
|
#2 |
Exceeding the specified time frame (e. g., late return) |
|
#3 |
Leaving the previously defined area (e. g., leaving the city for which the leave was granted) |
|
#4 |
Violation of situational or personal contact prohibitions (e. g., seeking contact with former victim) |
|
#5 |
Unauthorized use of media (e. g., procurement of a smartphone without permission) |
|
#6 |
Use of psychotropic substances (e. g., drinking alcohol) |
|
#7 |
New offences |
|
#8 |
Miscellaneous (e. g., gambling) |
2.4 Statistical Analysis
The statistical software R (R Core Team, 2022) was utilized for all data analysis and visualization (Wickham, 2016).
The study employed a pre-post design with follow-up and lacked a control group. To test our hypotheses, the primary analysis involved repeated measures ANOVA and post-hoc t-tests with the time of measurement as a within-subjects factor and the categorical ISL variable as a between-subjects factor. From both our hypotheses follows that we expect to find an interaction effect between the time of measurement and the ISL variable. In addition, the first hypothesis postulates a significant increase in treatment progress between t0 and t1 for the group of patients without an ISL which will be tested using a paired post-hoc t-test comparing treatment progress between t0 and t1 for patients without ISL. The second hypothesis is that incidents during unsupervised short leave will negatively impact treatment progress. To examine this hypothesis, we suspect a significant decrease in treatment progress during the time frame in which the ISL was recorded which will also be tested using paired post-hoc t-tests comparing treatment progress between the relevant times of measurement.
The following assumptions were tested for the repeated measures ANOVA: (1) absence of extreme outliers, (2) normality assumption for all conditions, and (3) sphericity. Extreme outliers were defined as values greater than the 75th percentile plus 3 times the interquartile range (IQR) or less than the 25th percentile minus 3 times the IQR within each condition (Kassambara, 2021). No extreme outliers were identified in the sample. Normality within each condition was assessed using QQ plots, which indicated some left-skewness in the distribution of the dependent variable. However, no significant deviations from the normality assumption were observed. Sphericity was tested using Mauchly’s W (Mauchly, 1940), revealing evidence of heteroskedasticity (W = .91; p < .01). To address this issue, the Huynh-Feldt correction (Huynh & Feldt, 1976; Lecoutre, 1991) was employed, given that the epsilon (ε) value exceeded .75 (.92).
Following an ISL, it is possible that a patient’s short leave privileges could be paused or completely revoked. Nonetheless, after excluding cases with missing values regarding treatment progress or the occurrence of ISLs, no patients with documented leave privilege revocations remained in the sample. However, it is still possible that leave privileges were paused without being documented. Unfortunately, this potential effect of ISL reactions could not be considered in the current study.
3 Results
3.1 Descriptive Statistics
Table 4 displays the descriptive measures for the Scale of Treatment Progress for all three measure points. Table 5 shows how frequently the different types of ISLs occurred.
In our sample, nine patients (6 %) had an ISL only in the first six months after being given permission to leave the institution unsupervised. Twenty-eight (18 %) patients had an ISL only between 7 and 12 months after their leave was granted. Thirteen patients (8 %) had an ISL in both time frames.
Mean, Median, Standard Deviation and Range for the Scale of Treatment Progress for each time of measurement.
|
M |
Med |
SD |
Range |
|
|
t0 |
3.37 |
3.40 |
0.60 |
1.80–4.80 |
|
t1 |
3.62 |
3.60 |
0.69 |
1.60–5.00 |
|
t2 |
3.52 |
3.60 |
0.85 |
1.00–5.00 |
3.2 Repeated measures ANOVA
Table 6 shows the results of the repeated-measures ANOVA. There is a significant main effect of ISLs as well as the time of measurement. Furthermore, the analysis reveals a significant interaction between the time of measurement and ISLs. We conducted post-hoc t-tests to further analyse where the differences between the time of measurements are within the groups of ISLs (Figure 1). For patients with no ISL, there is a significant increase in the Scale of Treatment Progress between t0 and t1 (t = –4.40; p < .001; d = –0.31) and t0 and t2 (t = –4.67; p < .001; d = –0.34). For patients with an ISL in the second time frame, there is a significant decrease between t1 and t2 (t = 3.15; p < .05; d = 0.56). Patients with an ISL in the first time frame or in both time frames showed no significant change in the Scale of Treatment Progress.
Number of patients with an ISL subdivided by the type of ISL and the time frame after the short leave was granted (N = 157).
|
0–6 m onths |
7–12 months |
Any time |
|
|
Violation of communication requirements |
3 (1.9 %) |
11 (7.0 %) |
14 (8.9 %) |
|
Exceeding the specified time frame |
4 (2.5 %) |
8 (5.1 %) |
11 (7.0 %) |
|
Leaving the previously defined area |
5 (3.2 %) |
9 (5.7 %) |
14 (8.9 %) |
|
Violation of situational or personal contact prohibitions |
1 (0.6 %) |
2 (1.3 %) |
3 (1.9 %) |
|
Unauthorized use of media |
7 (4.5 %) |
7 (4.5 %) |
13 (8.3 %) |
|
Use of psychotropic substances |
12 (7.6 %) |
22 (14.0 %) |
27 (17.2 %) |
|
New offences |
0 (0.0 %) |
3 (1.9 %) |
3 (1.9 %) |
|
Any type |
22 (14.0 %) |
41 (26.1 %) |
50 (31.8 %) |
Repeated-measures ANOVA with the time of measurement as a within-subjects factor and ISLs as a between-subjects factor.
|
dfn |
dfd |
F |
p |
η2 |
|
|
ISLs |
3.00 |
153.00 |
14.52 |
<.001 |
0.135 |
|
Time of measurement |
1.86 |
284.54 |
3.65 |
<.05 |
0.011 |
|
ISLs*Time of measurement |
5.58 |
284.54 |
4.82 |
<.001 |
0.041 |
4 Discussion
The aim of this study was to investigate how unsupervised short leave is associated with treatment progress in FAT. For this purpose, we explored the change in therapist-rated treatment progress after the permission for unsupervised short leave was granted in a pre-post design with follow-up. Furthermore, we examined the influence of ISLs on the therapists’ ratings.
In our hypotheses, we expected differing trajectories of treatment progress over time depending on the occurrence of an ISL, and our analysis showed a significant interaction effect between time of measurement and ISL. Our first hypothesis stated that unsupervised short leave has a positive effect on treatment progress for patients without an ISL, meaning that the ratings of indicators of treatment progress should improve after permission for short leave is granted. The results of the post-hoc t-tests support this hypothesis, as we can see a significant increase in the ratings of the Scale of Treatment Progress after permission for unsupervised short leave was granted for patients who did not have an ISL. This effect remained stable in the follow-up assessment. These results are in line with our previous findings on the effect of unsupervised short leave on treatment progress in forensic psychiatric hospitals (Neumann & Bauer, 2022).
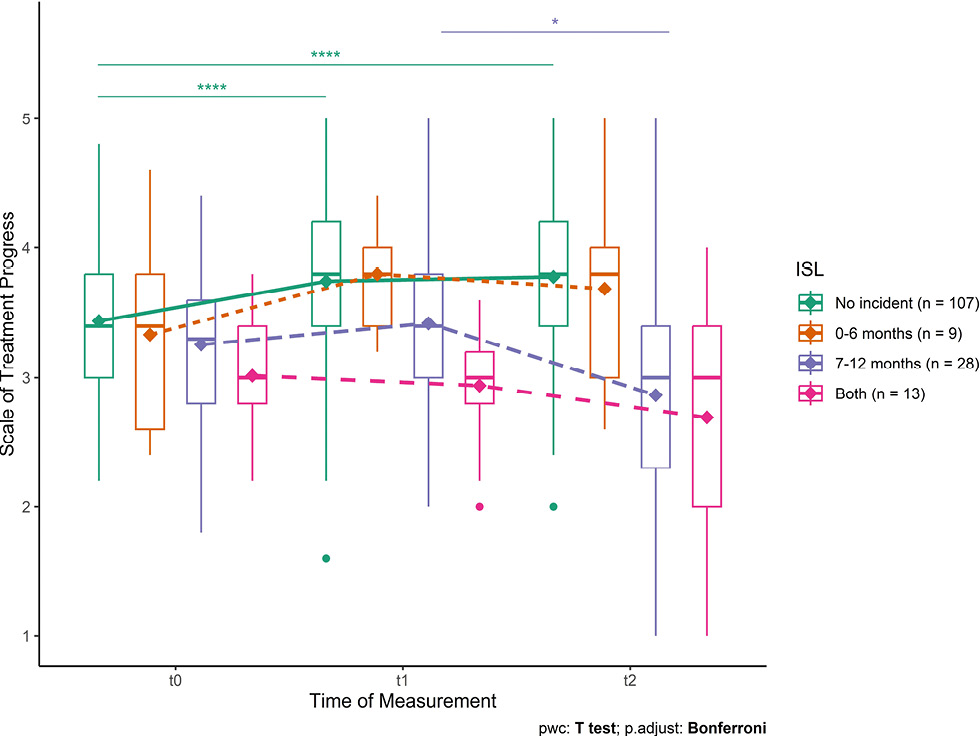
Change in the Scale of Treatment Progress over the multiple time points divided by ISLs
Note: The data is presented using box plots, with the means of the Scale of Treatment Progress represented by diamonds. The horizontal lines above the plots indicate significant changes over time based on post-hoc t-tests (*p <.05; ****p <.0001).
The second hypothesis was that incidents during unsupervised short leave negatively impact treatment progress, with the ratings of indicators of treatment progress declining following an incident. According to the results of the post-hoc t-tests, the findings are somewhat ambiguous. The occurrence of an ISL leads to a significant decrease in the ratings of the Scale of Treatment Progress, but only if the ISL happens in the second time frame. For patients with an ISL in the first time frame or in both time frames, there appears to be no significant change in treatment progress. In fact, the rating of the Scale of Treatment Progress seems to increase after the occurrence of an ISL in the first time frame, though this change is not statistically significant. Therefore, the results only partially support our second hypothesis and only for the group with an ISL in the second time frame.
There are some possible explanations for these rather ambiguous findings regarding the second hypothesis. One potential explanation is that in the first time frame, which is closer to the beginning of the treatment, ISLs may be more leniently tolerated or may have a lesser impact on the assessment of therapeutic progress. This may be because patients are in the early stages of treatment, in which fewer demands are placed upon them, and deviations from rule-compliant behaviour may be perceived as normal. Alternatively, this observation could be attributed to variations in the definition of treatment progress at the beginning and end of therapy. Another possible explanation could lie in the definition of ISLs in our study. Many different forms of behaviour are summarized in the variable, which could differ greatly regarding their effects on treatment progress. In particular, it may not be reasonable to expect a negative impact of substance abuse during leave on treatment progress. Substance abuse is a core symptom of substance use disorder, and relapses are often treated as a part of the recovery process (Melemis, 2015). Relapses can be used to work out a functional way of coping and to better recognize risky situations. Therefore, it could be possible that drug or alcohol relapse during short leave, if handled well, has a positive effect on treatment progress in FAT. Another reason for these unclear results could be rooted in the small sample sizes of the groups of patients with an ISL. Fortunately, the prevalence of ISLs is quite low, but this leads to small group sizes for the ISL variable and, subsequently, to a high uncertainty regarding the post-hoc comparisons between these small groups.
The present study contributes to our understanding of the potential benefits of unsupervised short leave for improving progress in FAT and the potential negative influence of ISLs. However, due to the ambiguity of the effects as well as the methodological limitations, which will be discussed in more detail below, the results should be interpreted with caution.
4.1 Limitations
While the study yielded significant findings similar to those of our previous study about unsupervised short leave in forensic psychiatric hospitals, we must consider several limitations when interpreting the results (Neumann & Bauer, 2022).
One major limitation is the lack of a control group, which makes it challenging to determine whether the observed changes in the Scale of Treatment Progress were due to the permission for unsupervised short leave, other factors such as the passage of time, or other external factors that were not controlled in the study. This is especially problematic for the interpretation of the findings regarding our first hypothesis. Although it should not be a problem that patients are only granted short leave when no substantial risk of ISL is identified (because the baseline measurement took place immediately before short leave was granted), it could be assumed that short leave is granted precisely when the change in treatment progress is on an upward trajectory. In this case, the increase in treatment progress would be an effect of the time of measurement. Further research is needed to rule out this alternative explanation.
Another limitation of the present study is that the dependent variable, treatment progress, was only measured using therapist ratings. This could be problematic because the therapists’ expectations and biases could have influenced the ratings, leading to distorted results. For example, if therapists had high expectations for the effect of unsupervised short leave, they may have rated their patients’ progress more positively than they otherwise would have. This potential source of bias should be considered when interpreting the results.
A further limitation is that we don’t know the extent to which the patients actually used their opportunities for unsupervised short leave. This issue raises questions about the validity of the results, as the frequency of unsupervised short leave may vary widely between patients.
We also cannot rule out that some patients could not be included in our analysis because they had committed a serious ISL and had, as a consequence, their leave privilege completely revoked, or their FAT terminated due to a lack of prospect of success.
4.2 Suggestions for future research
This study offers insights into the relationship between unsupervised short leave and progress in FAT. Future research should aim to use multiple sources of data and validated instruments to measure treatment progress, such as self-assessment questionnaires concerning the therapeutic alliance (e. g., WAI-SR; Wilmers et al., 2008) or treatment readiness (e. g., CVTRQ; Casey et al., 2007). Furthermore, the actual frequency of the use of unsupervised short leave should be assessed to control for differences between patients.
To examine the effect of an intervention, randomized controlled trials (RCTs) are the gold standard. As noted previously, without a control group, it is difficult to determine whether observed effects are caused by the intervention or other influencing factors. Regarding the research on short leave, implementing a control group is especially difficult, as there is a legal right to short leave in Germany (Pollähne, 2018). However, more rigorous methodological designs could be used to verify the results found in this study. Ideally, a prospective longitudinal design with several pre-treatment measurements should be employed to compare the slopes of change in treatment progress before and after short leave is granted. Another approach might be to construct a control group of patients without short leave via statistical matching procedures (e. g., Stuart, 2010).
As mentioned above, the sample sizes of the groups of patients with ISLs were quite small. Larger sample sizes are needed to better determine the effects of ISLs on treatment progress and to ensure adequate statistical power. This would also allow consideration of the nature of the incident in the analysis. As already described, there could be differences in the disruptive impacts of ISLs regarding the kind of incident.
Previous studies showed a relationship between rule-breaking behaviour in FAT and termination of the treatment due to a lack of prospect of success (Bezzel, 2008; Querengässer, 2014). Future research should examine in detail the relationship between ISLs, treatment progress, and termination of FAT to improve recognition of difficult treatment developments and allow intervention at an early stage.
Another study topic within the scope of this research could involve the comparison of patients based on the timing of their permission for short leave and the subsequent impact on treatment progress. An exploration of the factors influencing the varying timing of the permission for short leave, such as why some receive them earlier than others, could also be considered. In addition, an alternative approach would involve investigating other criteria besides short leave that may influence treatment progress.
About the authors
Louisa Neumann, M. Sc., is a clinical psychologist at the Clinic for Forensic Psychiatry and Psychotherapy in Wunstorf, Germany. Her research focuses on the treatment of individuals who committed offences.
Merten Neumann, Dipl.-Psych., is a research associate at the Criminological Research Institute of Lower Saxony (KFN). His research focuses on different aspects of the correctional system with a special emphasis on risk prediction procedures in forensic mental health institutions.
Acknowledgements
We thank the Legal Psychology Division of the German Psychological Society (DGPs) for providing funds for the open access fee.
References
Berthold, D., & Riedemann, C. (2021). Auswertung der Daten der deutschlandweiten Stichtagserhebung im Maßregelvollzug nach § 64 StGB. MRVZN Bad Rehburg. Verfügbar unter: https://www.mrvzn-badrehburg.niedersachsen.de/startseite/veroffentlichungen/veroeffentlichungen-106184.htmlSuche in Google Scholar
Bezzel, A. (2008). Therapie im Maßregelvollzug – und dann? Eine Verlaufsuntersuchung an forensischen Patienten. (Dissertation).Suche in Google Scholar
Bezzel, A. (2010). Können Patienten aus dem Maßregelvollzug (§ 64 StGB) resozialisiert werden? Forensische Psychiatrie, Psychologie, Kriminologie, 4(4), 264–268. https://doi.org/10.1007/s11757-010-0083-210.1007/s11757-010-0083-2Suche in Google Scholar
Brown, T. A. (2015). Confirmatory factor analysis for applied research (2. ed.). Methodology In The Social Sciences. Guilford Press. http://site.ebrary.com/lib/alltitles/detail.action?docID=11001916Suche in Google Scholar
Casey, S., Day, A., Howells, K., & Ward, T. (2007). Assessing Suitability for Offender Rehabilitation. Criminal Justice and Behavior – CRIM JUSTICE BEHAV, 34(11), 1427–1440. https://doi.org/10.1177/009385480730582710.1177/0093854807305827Suche in Google Scholar
Chen, F. F. (2007). Sensitivity of Goodness of Fit Indexes to Lack of Measurement Invariance. Structural Equation Modeling: A Multidisciplinary Journal, 14(3), 464–504. https://doi.org/10.1080/1070551070130183410.1080/10705510701301834Suche in Google Scholar
Drieschner, K. H., & Verschuur, J. (2010). Treatment engagement as a predictor of premature treatment termination and treatment outcome in a correctional outpatient sample. Criminal Behaviour and Mental Health: CBMH, 20(2), 86–99. https://doi.org/10.1002/cbm.75710.1002/cbm.757Suche in Google Scholar
Gericke, B., & Kallert, T. W. (2007). Zum Outcome der Maßregelvollzugsbehandlung nach § 64 StGB [On the outcome of the treatment of mentally disordered criminal offenders (according to section 64 German Penal Code) suffering from addictive disorders]. Psychiatrische Praxis, 34, 218–226. https://doi.org/10.1055/s-2006-95200610.1055/s-2006-952006Suche in Google Scholar
Hearn, D., Ndegwa, D., Norman, P., Hammond, N., & Chaplin, E. (2012). Developing the leave/abscond risk assessment (LARA) from the absconding literature: An aide to risk management in secure services. Advances in Mental Health and Intellectual Disabilities, 6(6), 280–290. https://doi.org/10.1108/2044128121128591910.1108/20441281211285919Suche in Google Scholar
Hu, L., & Bentler, P. M. (1999). Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Structural Equation Modeling: A Multidisciplinary Journal, 6(1), 1–55. https://doi.org/10.1080/1070551990954011810.1080/10705519909540118Suche in Google Scholar
Huynh, H., & Feldt, L. S. (1976). Estimation of the Box Correction for Degrees of Freedom from Sample Data in Randomized Block and Split-Plot Designs. Journal of Educational Statistics, 1(1), 69–82. https://doi.org/10.3102/1076998600100106910.3102/10769986001001069Suche in Google Scholar
Kassambara, A. (2021). rstatix (Version 0.7.0) [Computer software]. https://CRAN.R-project.org/package=rstatixSuche in Google Scholar
Kline, R. B. (2011). Principles and practice of structural equation modeling (3. ed.). Research methods. Guilford Press.Suche in Google Scholar
Köhne, M., & Lesting, W. (2012). § 11: Lockerungen des Vollzuges. In J. Feest & W. Lesting (Eds.), StVollzG: Kommentar zum Strafvollzugsgesetz; (AK-StVollzG) (6th ed., pp. 102–125). Heymann.Suche in Google Scholar
Lecoutre, B. (1991). A Correction for the ε̃ Approximate Test in Repeated Measures Designs With Two or More Independent Groups. Journal of Educational Statistics, 16(4), 371–372. https://doi.org/10.3102/1076998601600437110.3102/10769986016004371Suche in Google Scholar
Mauchly, J. W. (1940). Significance test for sphericity of a normal n-variate distribution. The Annals of Mathematical Statistics, 11(2), 204–209. https://doi.org/10.1214/aoms/117773191510.1214/aoms/1177731915Suche in Google Scholar
Melemis, S. M. (2015). Relapse Prevention and the Five Rules of Recovery. The Yale Journal of Biology and Medicine, 88(3), 325–332.Suche in Google Scholar
Müller, J. L., Böcker, F. M., Eusterschulte, B., Koller, M., Muysers, J., & Pollmächer, T. (2021). Neuregelung des § 64 StGB aus psychiatrischer Sicht – Positionspapier einer Task-Force der DGPPN [Revision of § 64 of the German Penal Code from a psychiatric perspective-Position paper of a task force of the German Association for Psychiatry, Psychotherapy and Psychosomatics]. Der Nervenarzt, 92(11), 1155–1162. https://doi.org/10.1007/s00115-021-01109-w10.1007/s00115-021-01109-wSuche in Google Scholar
Müller, J. L., Nedopil, N., Freisleder, F. J., Graf, M., & Haller, R. (2017). Forensische Psychiatrie: Klinik, Begutachtung und Behandlung zwischen Psychiatrie und Recht (5., überarbeitete Auflage). Georg Thieme Verlag.10.1055/b-005-146531Suche in Google Scholar
Müller, J. L, Saimeh, N., Briken, P., Eucker, S., Hoffmann, K., Koller, M., Wolf, T., Dudeck, M., Hartl, C., Jakovljevic, A.-K., Klein, V., Knecht, G., Müller-Isberner, R., Muysers, J., Schiltz, K., Seifert, D., Simon, A., Steinböck, H., Stuckmann, W., Zeidler, R. (2017). Standards für die Behandlung im Maßregelvollzug nach §§ 63 und 64 StGB: Interdisziplinäre Task-Force der DGPPN [Standards for treatment in forensic committment according to § 63 and § 64 of the German criminal code: Interdisciplinary task force of the DGPPN]. Der Nervenarzt, 88, 1–29. https://doi.org/10.1007/s00115-017-0382-310.1007/s00115-017-0382-3Suche in Google Scholar
Neumann, M., & Bauer, L. (2022). The influence of unsupervised short leave on treatment progress in forensic psychiatric hospitals: A pre-post study with follow-up. International Journal of Forensic Mental Health, 1–9. https://doi.org/10.1080/14999013.2022.215167010.1080/14999013.2022.2151670Suche in Google Scholar
Neumann, M., Heintzsch, R., Glaubitz, C., Killig, L., Schumann, R., & Bliesener, T. (2019). Analyse der Vollzugslockerungen im niedersächsischen Maßregelvollzug (KFN-Forschungsbericht No. 150). Hannover. Kriminologisches Forschungsinstitut Niedersachsen e.V. (KFN).Suche in Google Scholar
Norman, C. (2022). A global review of prison drug smuggling routes and trends in the usage of drugs in prisons. WIREs Forensic Science. Advance online publication. https://doi.org/10.1002/wfs2.147310.1002/wfs2.1473Suche in Google Scholar
Pollähne, H. (2018). Das Maß des Freiheitsentzugs (Vollzugslockerungen). In H. Pollähne & H. Kammeier (Eds.), Maßregelvollzugsrecht (4th ed., pp. 229–306). De Gruyter.10.1515/9783110352047-006Suche in Google Scholar
Querengässer, J. (2014). Abbruchgründe und Risikofaktoren für Therapieabbrüche nach § 64 Strafgesetzbuch (StGB) [Dissertation]. Universität Konstanz. http://nbn-resolving.de/urn:nbn:de:bsz:352-0-266214Suche in Google Scholar
R Core Team. (2022). R: A language and environment for statistical computing (Version 4.2.1) [Computer software]. R Foundation for Statistical Computing. Vienna, Austria. https://www.R-project.org/Suche in Google Scholar
Revelle, W. R. (2017). Psych: Procedures for Personality and Psychological Research. https://www.scholars.northwestern.edu/en/publications/psych-procedures-for-personality-and-psychological-researchSuche in Google Scholar
Rosseel, Y. (2012). lavaan: An R Package for Structural Equation Modeling. Journal of Statistical Software, 48(2), 1–36. https://doi.org/10.18637/jss.v048.i0210.18637/jss.v048.i02Suche in Google Scholar
Stuart, E. A. (2010). Matching methods for causal inference: A review and a look forward. Statistical Science: A Review Journal of the Institute of Mathematical Statistics, 25(1), 1–21. https://doi.org/10.1214/09-STS31310.1214/09-STS313Suche in Google Scholar
Suhling, S., Pucks, M., & Bielenberg, G. (2015). Ansätze zum Umgang mit Gefangenen mit geringer Veränderungs- und Behandlungsmotivation. In B. Wischka, W. Pecher, & H. van den Boogaart (Eds.), Studien und Materialien zum Straf- und Maßregelvollzug: v.26. Behandlung von Straftätern: Sozialtherapie, Maßregelvollzug, Sicherungsverwahrung (pp. 233–293). Centaurus Verlag & Media.10.1007/978-3-86226-849-8_9Suche in Google Scholar
Walker, A., Farnworth, L., & Lapinksi, S. (2013). A recovery perspective on community day leaves. The Journal of Forensic Practice, 15(2), 109–118. https://doi.org/10.1108/1463664131132229610.1108/14636641311322296Suche in Google Scholar
Ward, T., Day, A., Howells, K., & Birgden, A. (2004). The multifactor offender readiness model. Aggression and Violent Behavior, 9(6), 645–673. https://doi.org/10.1016/j.avb.2003.08.00110.1016/j.avb.2003.08.001Suche in Google Scholar
Wickham, H. (2016). Ggplot2: Elegant graphics for data analysis (Second edition). Use R! Springer. https://doi.org/10.1007/978-3-319-24277-410.1007/978-3-319-24277-4Suche in Google Scholar
Wilmers, F., Munder, T., Leonhart, R., Herzog, T., Plassmann, R., Barth, J., & Linster, H. W. (2008). Die deutschsprachige Version des Working Alliance Inventory – short revised (WAI-SR) – Ein schulübergreifendes, ökonomisches und empirisch validiertes Instrument zur Erfassung der therapeutischen Allianz. https://doi.org/10.7892/boris.27962Suche in Google Scholar
Conflict of Interest: The authors declare that they have no conflict of interest.
Data availability: The data and the code of the analysis can be found here: https://osf.io/rytuk/
Funding: The research was funded by the Ministry of Social Affairs of Lower Saxony. The Legal Psychology Division of the German Psychological Society (DGPs) provided funds for the open access fee.
© 2023 bei den Autoren, publiziert von De Gruyter.
Dieses Werk ist lizensiert unter einer Creative Commons Namensnennung 4.0 International Lizenz.
Artikel in diesem Heft
- Frontmatter
- Editorial
- Lockerungen im Straf- und Maßregelvollzug: Aktueller Forschungsstand und Einleitung zum Themenheft
- Artikel
- Vollzugsöffnende Maßnahmen und Entlassungsvorbereitung – Gesetzgebung und Praxis in den Bundesländern
- Die Prüfung der Wirkungen von Lockerungen
- Unsupervised short leave in forensic addiction treatment: Is there an influence on treatment progress?
- Lockerungen im österreichischen Maßnahmenvollzug –
- Effekte unbegleiteter Lockerungen aus der Sozialtherapie auf die Beschäftigungssituation bei Entlassung
- Vollzugslockerungen und Legalbewährung bei inhaftierten Sexualstraftätern
- Predictors of incidents during short leave: An analysis of prisoner personal files in the Lower Saxony prison system
- Buchbesprechung
- Derin, Benjamin & Singelnstein, Tobias (2022): Die Polizei. Helfer Gegner, Staatsgewalt. Inspektion einer mächtigen Organisation. Ullstein: Berlin (438 Seiten)
Artikel in diesem Heft
- Frontmatter
- Editorial
- Lockerungen im Straf- und Maßregelvollzug: Aktueller Forschungsstand und Einleitung zum Themenheft
- Artikel
- Vollzugsöffnende Maßnahmen und Entlassungsvorbereitung – Gesetzgebung und Praxis in den Bundesländern
- Die Prüfung der Wirkungen von Lockerungen
- Unsupervised short leave in forensic addiction treatment: Is there an influence on treatment progress?
- Lockerungen im österreichischen Maßnahmenvollzug –
- Effekte unbegleiteter Lockerungen aus der Sozialtherapie auf die Beschäftigungssituation bei Entlassung
- Vollzugslockerungen und Legalbewährung bei inhaftierten Sexualstraftätern
- Predictors of incidents during short leave: An analysis of prisoner personal files in the Lower Saxony prison system
- Buchbesprechung
- Derin, Benjamin & Singelnstein, Tobias (2022): Die Polizei. Helfer Gegner, Staatsgewalt. Inspektion einer mächtigen Organisation. Ullstein: Berlin (438 Seiten)