Umbilical venous flow and maternal hemodynamics as predictors of impaired fetal growth in gestational diabetes: a prospective study
-
Daniele Farsetti
 ,
Sara Nardini
,
Sara Nardini


Abstract
Objectives
This study aims to evaluate the association between maternal cardiovascular function, umbilical vein blood flow (UV-Q), and impaired fetal growth in pregnancies complicated by gestational diabetes mellitus (GDM).
Methods
In this prospective observational study, 84 singleton pregnancies complicated by GDM between 28 and 32 weeks of gestation were enrolled. All participants underwent a standardized maternal hemodynamic assessment using USCOM device and fetal ultrasound including Doppler-based measurement of UV-Q. Impaired fetal growth was defined as either small for gestational age (SGA, birthweight <10th centile) or a ≥40 centile drop between estimated fetal weight (EFW) at enrolment and actual birthweight centile (“DROP”). Predictive performance was assessed using ROC analysis and multivariate logistic regression.
Results
Fetuses with impaired growth (n=24) had significantly lower UV-Q centiles (median 29.50 vs. 50.00, p=0.04), higher maternal systemic vascular resistance (SVR) (1,004.50 vs. 915.00 dyn s cm−5, p<0.01), lower cardiac output (CO) (6.5 vs. 7.2 L/min, p=0.03), and reduced oxygen delivery (DO2) (1,021.22 vs. 1,131.06 mL/min, p<0.01) compared to those with normal growth. Multivariate analysis identified UV-Q centile ≤24, SVR>916 dyn s cm−5, and DO2≤1,061.4 as independent predictors of impaired growth (AUC up to 0.78). These associations remained significant after adjusting for EFW at enrolment.
Conclusions
In pregnancies complicated by GDM, impaired fetal growth may reflect placental dysfunction and maternal cardiovascular maladaptation. Maternal hemodynamic parameters and UV-Q may enhance fetal growth surveillance, particularly when incorporating longitudinal metrics such as DROP. These findings suggest a potential role for integrating maternal-fetal hemodynamics into standard care to identify “hidden” growth restriction phenotypes in GDM pregnancies.
Introduction
Gestational diabetes mellitus (GDM) is a common pregnancy complication, affecting up to 10–15 % of pregnancies worldwide, and is traditionally associated with fetal overgrowth and increased risk of macrosomia-related complications. However, a growing body of evidence suggests that some fetuses in GDM pregnancies may experience impaired growth trajectories, potentially linked to placental dysfunction [1].
The mechanisms underlying impaired growth in GDM pregnancies remain poorly understood. Beyond glycemic control, maternal cardiovascular status and uteroplacental perfusion appear to play a crucial role in fetal growth [2]. In particular, maternal cardiovascular adaptation to pregnancy – characterized by a decrease in systemic vascular resistance (SVR) and an increase in cardiac output (CO) [3], 4] – is crucial to ensure proper development of the feto-placental unit and to support fetal growth [5], 6].
Similarly, umbilical vein blood flow (UV-Q), which represents the final output of placental transfer of oxygen and nutrients, may reflect placental vascular function more accurately than arterial Doppler alone. Although its clinical use remains limited, recent ultrasound advances and standardized protocols have improved measurement reliability and recent studies have assessed its capacity to identify fetal growth restriction (FGR) [7].
Despite their theoretical value, maternal hemodynamic parameters and UV-Q are not routinely integrated into growth surveillance in GDM pregnancies, which remain primarily focused on fetal overgrowth [8]. The aim of this prospective study was to investigate the association between maternal hemodynamics, UV-Q, and impaired fetal growth in a cohort of GDM pregnancies.
Materials and methods
This prospective observational study was conducted at the Department of Obstetrics and Gynecology, Policlinico Casilino, Rome, between December 2023 and May 2025. A total of 84 pregnant women with GDM, followed at the High-Risk Pregnancy Outpatient Clinic of our institution, were consecutively enrolled.
The primary outcome of the study was the identification of maternal hemodynamic and fetal ultrasound parameters associated with impaired fetal growth, defined as either newborn small for gestational age (SGA) or a significant decline (≥40 centiles) between estimated fetal weight (EFW) at enrolment and birthweight (BW) centile (referred to as “DROP”).
Secondary outcomes included the predictive performance (ROC analysis) of these parameters and the identification of independent predictors through multivariate logistic regression.
The inclusion criteria were:
singleton pregnancy,
diagnosis of GDM based on a 75-g oral glucose tolerance test (OGTT) performed between 24- and 28-weeks’ gestation,
pregnancy dating by first trimester ultrasound using crown-rump length (CRL),
gestational age between 28- and 32-weeks’ at the time of enrolment,
absence of known fetal anomalies at recruitment.
The exclusion criteria included:
pre-existing type 1 or type 2 diabetes mellitus,
hypertensive disorders at enrolment,
evidence of fetal chromosomal abnormalities or suspected major congenital malformations on ultrasound.
This study was conducted in accordance with the ethical principles of the World Medical Association Declaration of Helsinki.
Clinical and ultrasound assessment
At the time of enrolment, maternal demographic and clinical data were collected, including maternal age, body mass index (BMI), parity, ethnicity, mode of conception, GDM treatment modality (diet vs. pharmacological), glycemic control assessed at last prenatal visit, and smoking status.
Glycemic control was assessed at the last prenatal visit. Good glycemic control was defined according to the targets recommended by national scientific societies [9]. Pharmacological treatment for GDM followed our center’s protocol: insulin was prescribed as first-line therapy for patients with glucose values above target despite dietary and lifestyle interventions. Metformin was added in selected cases with suboptimal response to insulin or in rare patients with poor insulin compliance [9].
All participants underwent a standardized ultrasound assessment between 28- and 32-weeks’ gestation, including:
Umbilical Vein (UV) Doppler: the UV was sampled at a free-floating loop of the umbilical cord in the absence of fetal movements and respiratory acts [12]. Image magnification was applied to ensure the vessel occupied at least 30 % of the screen. UV diameter was measured inner-wall to inner-wall at three consecutive sites; the mean of these values was recorded. Time-averaged maximum velocity (TAMXV) was measured on a steady venous flow profile by adjusting the transducer to align the insonation angle with the vessel axis, maintaining an angle between 0° and 30°, and applying angle correction. Mean TAMXV was derived from three recordings taken during fetal quiescence. UV-Q was calculated as:
assuming a circular cross-sectional area derived from the mean diameter, with results expressed in mL/min. UV parameters centiles were determined using reference charts published by Flo et al. [13].
Maternal hemodynamics assessment
On the same day, all participants were studied using Ultra Sonic Cardiac Output Monitor (USCOM®, USCOM Ltd, Coffs Harbor, Australia). The measurements were performed by a trained operator under standardized conditions as described in previous studies [14], 15]. Blood pressure was measured using an automated device with appropriately sized cuffs.
We selected eight primary hemodynamic variables: SVR, CO, stroke volume (SV), heart rate (HR), flow time corrected (FTc), oxygen delivery (DO2), Smith-Madigan Inotropy Index (INO), potential to kinetic energy ratio (PKR).
INO and PKR are derived from the evaluation of maternal cardiovascular potential energy and kinetic energy. During systole, the left ventricle imparts two forms of energy to the circulating blood: potential energy, reflected by blood pressure, and kinetic energy, associated with blood flow. The INO index is calculated as the sum of these two energy components, normalized to body surface area. The PKR index expresses the ratio between potential and kinetic energy, providing an indication of the balance between vascular resistance (pressure) and blood flow [16].
DO2 was calculated as:
where CaO2 represents arterial oxygen content, Hb is hemoglobin concentration, and SaO2 is arterial oxygen saturation [17]. SpO2 was measured non-invasively using integrated or external pulse oximetry.
Delivery and neonatal outcomes
Patients were followed until delivery, and delivery outcomes were collected, including mode of delivery, induction of labor, gestational age at delivery, BW. BW was categorized using gestational-age-adjusted centiles [18]:
SGA: <10th centile,
Appropriate for gestational age (AGA): 10th–90th centile,
Large for gestational age (LGA): >90th centile.
Participants were stratified into two groups:
Group A (n=24): neonates with suspected impaired growth, including SGA and AGA with DROP ≥40 centiles, and
Group B (n=60): neonates with normal growth, including AGA with DROP <40 centiles and LGA.
Statistical analysis
Statistical analysis was performed using MedCalc (MedCalc Software, West-Vlaanderen, Belgium). Continuous variables were reported as median (interquartile range), while categorical variables were expressed as frequencies and percentages. Group comparisons were conducted using Student's t- or Mann-Whitney test (continuous variables) and Chi-square test or Fisher test (categorical variables). A p-value <0.05 was considered statistically significant.
Correlation analyses were performed between maternal hemodynamic parameters and fetal biometric/Doppler variables. Receiver operating characteristic (ROC) curve analysis was used to evaluate the predictive performance of the different variables in identifying neonatal with impaired growth. Finally, multivariate logistic regression analysis was conducted to identify independent predictors of impaired fetal growth, with calculation of odds ratios (ORs) and 95 % confidence intervals (CIs).
Results
Table 1 summarizes the maternal, fetal and neonatal characteristics. At the enrolment, there were no significant differences between the two groups in terms of maternal age, BMI, in vitro fertilization rate, nulliparous rate, therapeutic management, glycemic control, hemoglobin, gestational age at the enrolment, EFW. However, patients who subsequently developed impaired fetal growth had a significantly lower UV-Q centile (29.50 vs. 50.00, p=0.04).
Maternal and fetal characteristics.
| Gruppo A (Impaired growth) (n=24) |
Gruppo B (Normal growth) (n=60) |
p-Value | |
|---|---|---|---|
| Age, years | 37.00 (31.00–39.00) | 36.00 (32.75–39.25) | 0.88 |
| BMI, kg/m2 | 29.21 (26.20–30.84) | 30.04 (26.19–34.23) | 0.21 |
| BMI>30, n (%) | 8 (33.33 %) | 30 (50.00 %) | 0.24 |
| In vitro fertilization, n (%) | 1 (4.17 %) | 6 (10.00 %) | 0.64 |
| Nulliparous, n (%) | 12 (50.00 %) | 34 (56.67 %) | 0.73 |
| Therapy, n (%) Diet Insulin Metformin Insulin + metformin |
14 (58.33 %) 8 (33.33 %) 1 (4.17 %) 1 (4.17 %) |
28 (46.67 %) 25 (41.67 %) 2 (5.00 %) 5 (8.33 %) |
0.71 |
| Glycemic control at last visit, n (%) | 22 (91.67 %) | 49 (81.67 %) | 0.25 |
| Hb, g/dL | 11.55 (10.93–12.70) | 11.90 (11.30–12.80) | 0.28 |
| Gestational age at enrolment, days | 217.50 (209.00–223.75) | 218.00 (207.50–224.25) | 0.83 |
| EFW, g | 1,627.50 (1,508.50–1,697.50) | 1,694.00 (1,445.25–1,955.75) | 0.19 |
| EFW centile | 68.75 (22.05–87.63) | 66.65 (43.40–86.45) | 0.40 |
| UV-Q, mL/min | 175.00 (131.45–248.80) | 183.85 (158.73–231.82) | 0.51 |
| UV-Q centile | 29.50 (11.00–66.25) | 50.00 (36.50–80.00) | 0.04a |
| Gestational age at delivery, days | 268.00 (265.00–270.00) | 270.00 (267.00–273.00) | 0.07 |
| Birthweight, g | 2,632.50 (2,422.50–2,915.00) | 3,105.00 (2,817.50–3,480.00) | <0.01b |
| Birthweight, centile | 10.13 (5.64–36.61) | 52.00 (28.77–78.35) | <0.01b |
| DROP | −40,82 (−48.64 to −19.42) | −13.26 (−26.5 to −2,26) | <0.01b |
-
Data are expressed as median (interquartile range) for continuous variables and as count and percentage for categorical variables. BMI, body mass index; Hb, hemoglobin; EFW, estimated fetal weight; UV-Q, umbilical vein blood flow. DROP was defined as a decrease of ≥40 centile between the EFW centile at enrolment and the BW centile. ap<0.05; bp<0.01.
The differences in maternal hemodynamics between the two groups are summarized in Table 2. Patients with subsequent impaired fetal growth (Group A) had higher SVR (1,004.50 vs. 915.00 dyn s cm−5, p<0.01), lower CO (6.65 vs. 7.20 L/min, p=0.03), lower SV (80.50 vs. 89.50 mL, p=0.04), and lower DO2 (1,021.22 vs. 1,131.06 mL/min, p<0.01), compared to patients with normal growth.
Maternal hemodynamic characteristics.
| Gruppo A (Impaired growth) (n=24) |
Gruppo B (Normal growth) (n=60) |
p-Value | |
|---|---|---|---|
| MAP, mmHg | 84.50 (80.00–92.25) | 83.00 (75.25–90.00) | 0.39 |
| SVR, d.s.cm−5 | 1,004.50 (935.00–1,283.05) | 915.00 (774.00–1,061.00) | <0.01b |
| CO, L/min | 6.65 (5.55–7.45) | 7.20 (6.50–8.12) | 0.03a |
| HR, bpm | 83.00 (75.50–87.00) | 84.00 (78.00–96.00) | 0.22 |
| SV, mL | 80.50 (67.75–90.15) | 89.50 (76.22–97.50) | 0.04a |
| FTc, ms | 368.00 (338.00–387.90) | 382.90 (356.00–404.00) | 0.06 |
| PKR | 19.50 (16.75–29.75) | 21.00 (16.77–25.00) | 0.30 |
| INO, W/m2 | 1.60 (1.45–2.05) | 1.70 (1.40–1.90) | 0.66 |
| DO2, mL/min | 1,021.22 (891.18–1,123.50) | 1,131.06 (1,005.50–1,286.93) | <0.01b |
-
Data are expressed as median (interquartile range). MAP, mean arterial pressure; SVR, systemic vascular resistance; CO, cardiac output; HR, heart rate; SV, stroke volume; FTc, flow time corrected; PKR, potential to kinetic energy ratio; INO, inotropy index; DO2, oxygen delivery. ap<0.05; bp<0.01.
The correlation analysis between fetal biometric parameters and fetal-maternal hemodynamic parameters is shown in Table 3. The BW centile showed a positive correlation with DROP (r=0.42, p<0.01), EFW centile (r=0.69, p<0.01), UV-Q centile (r=0.28, p<0.01; Figure 1), CO (r=0.31, p<0.01), and DO2 (r=0.22, p=0.04; Figure 2a), and negative correlation with SVR (r=−0.28, p=0.01; Figure 3a). DROP showed a positive correlation with CO (r=0.37, p<0.01) and DO2 (r=0.32, p<0.01; Figure 2b), and negative correlation with EFW (r=−0.36, p<0.01) and SVR (r=−0.35, p<0.01; Figure 3B). The EFW centile had a positive correlation with UV-Q (r=0.28, p<0.01).
Correlation between neonatal biometry, and fetal-maternal hemodynamic parameters.
| BW centile | DROP | EFW centile | |
|---|---|---|---|
| BW centile | / | ||
| DROP | 0.42b | / | |
| EFW centile | 0.69b | −0.36b | / |
| UV-Q centile | 0.28 b | −0.18 | 0.28 b |
| SVR | −0.28a | −0.35b | −0.02 |
| CO | 0.31b | 0.37b | 0.06 |
| DO2 | 0.22a | 0.32b | −0.02 |
-
BW, birthweight centile; CO, cardiac output; DO2, oxygen delivery; EFW, estimated fetal weight; SVR, systemic vascular resistance; UV-Q, umbilical vein flow. DROP was defined as a decrease of ≥40 centile between the EFW centile at enrolment and the BW centile. ap<0.05; bp<0.01.
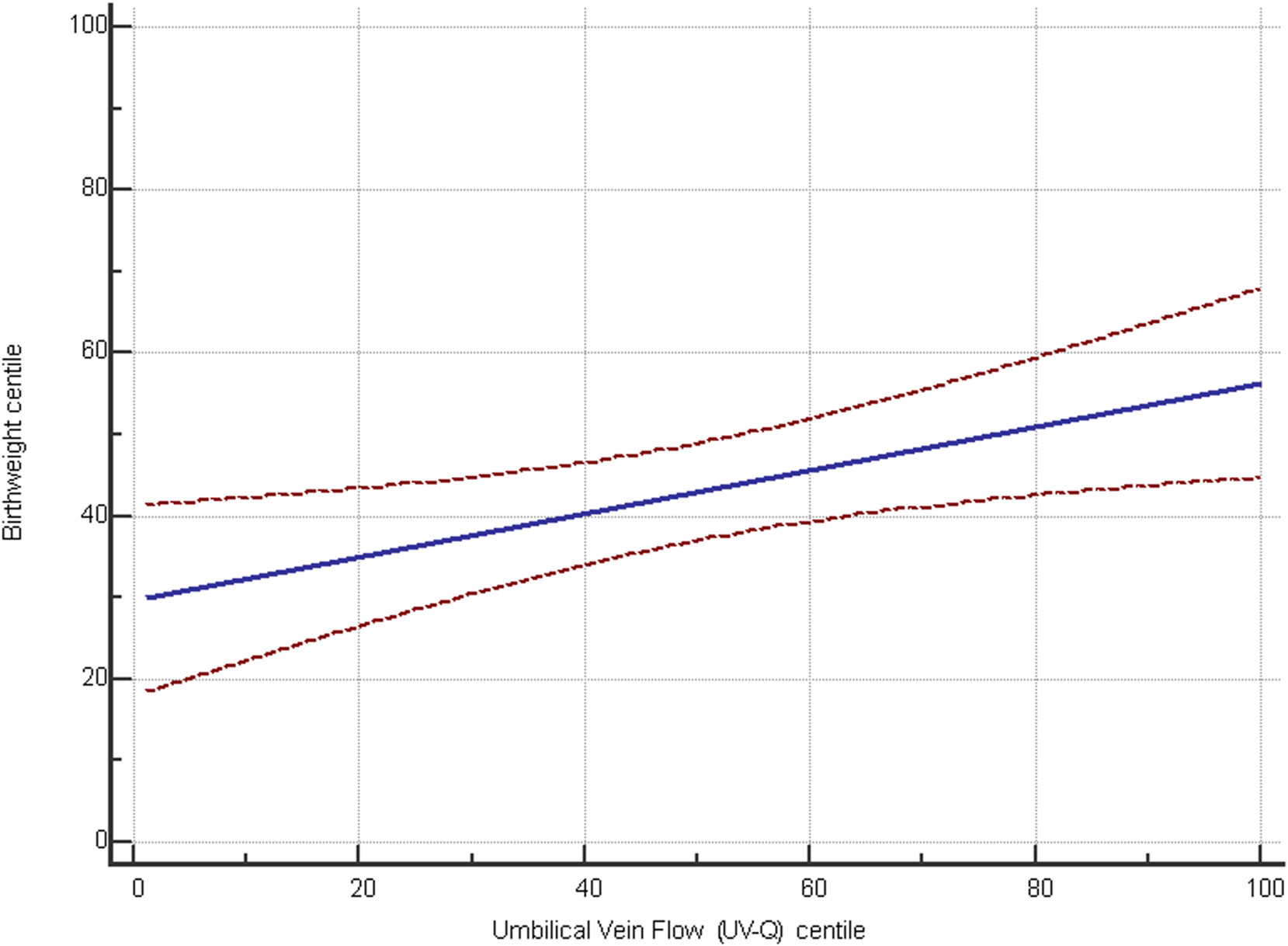
Scatter diagram showing the correlation between birthweight centile and UV-Q centile.

Scatter diagram showing the correlation between oxygen delivery (DO2) and (A) birthweight centile and (B) DROP between estimated fetal weight and birthweight centile.

Scatter diagram showing the correlation between systemic vascular resistance (SVR) and (A) birthweight centile and (B) DROP between estimated fetal weight and birthweight centile.
ROC curve analysis was performed to determine the optimal cut-off values for variables showing significant differences between the two groups. The best thresholds identified were UV-Q centile≤24 [AUC 0.640 (95 % CI 0.528–0.742), p<0.01], SVR>916 dyn s cm−5 [AUC 0.701 (95 % CI 0.592–0.796), p<0.01], CO≤5.6 L/min [AUC 0.655 (95 % CI 0.544–0.756), p=0.02], and DO2≤1,061.41 mL/min [AUC 0.682 (95 % CI 0.571–0.779), p<0.01].
Multivariate logistic regression analysis was then performed, incorporating EFW, UV-Q centile≤24, and SVR>916 dyn s cm−5 (Model 1), or DO2≤1,061.41 mL/min (Model 2) (Table 4). The final models demonstrated a moderate diagnostic performance [Model 1, AUC=0.78 (95 % CI 0.67–0.86); Model 2, AUC=0.75 (95 % CI 0.64–0.84)]. In the multivariate model, UV-Q centile≤24, SVR>916 dyn s cm−5, and DO2≤1,061.41 mL/min emerged as independent predictors of the outcome (Table 4).
Multivariate logistic regression model.
| Model 1 (multivariate model with SVR) | ||
|---|---|---|
| OR (95 % CI) | p-Value | |
| SVR >916 d.s.cm−5 | 5.91 (1.62–21.50) | <0.01 |
| UV-Q centile≤24 | 4.01 (1.34–12.03) | 0.01 |
| EFW centile | 0.99 (0.97–1.01) | 0.19 |
| Model 2 (multivariate model with DO2) | ||
|---|---|---|
| OR (95 % CI) | p-Value | |
| DO2≤1,061.41 mL/min | 3.85 (1.32–11.23) | 0.01 |
| UV-Q centile≤24 | 4.19 (1.41–12.47) | 0.01 |
| EFW centile | 0.99 (0.97–1.01) | 0.32 |
-
SVR, systemic vascular resistance; DO2, oxygen delivery; EFW, estimated fetal weight.
Discussion
Main findings
This study found that in pregnancies complicated by gestational diabetes, impaired fetal growth was associated with lower umbilical vein blood flow, higher maternal systemic vascular resistance, lower cardiac output, and reduced oxygen delivery measured between 28 and 32 weeks of gestation. Notably, UV-Q centile≤24, SVR>916 dyn s cm−5, and DO2≤1,061.41 mL/min emerged as independent predictors of impaired growth, regardless of fetal estimated weight.
Interpretation
Our findings support the growing recognition that impaired fetal growth in GDM pregnancies may not only result from glycemic factors but also from placental insufficiency and subclinical maternal cardiovascular maladaptation [1]. Maternal diabetes can worsen placental perfusion and fetal hemodynamics, potentially increasing FGR severity [19].
Women with GDM often exhibit impaired maternal hemodynamic adaptation to pregnancy ;– likely due to hyperglycemia and reduced cardiovascular reserve – characterized by a hypodynamic, high-resistance cardiovascular profile compared to controls [20].
It has previously been demonstrated that a hypodynamic maternal hemodynamic profile in the third trimester, characterized by high SVR and low CO, is associated with intrauterine growth restriction [21]. Our results confirm that FGR in pregnancies affected by GDM is associated with the same maternal cardiovascular alterations observed in FGR nondiabetic patients [22].
In fact, patients with impaired fetal growth exhibited a hypodynamic hemodynamic profile, and the maternal cardiovascular system showed a reduced capacity for oxygen delivery to the placenta. SVR and DO2 showed a significant correlation with BW and with drop in fetal growth and emerged as independent predictive factors.
UV-Q reflects the amount of oxygen and nutrients reaching the fetus, thereby serving as an indicator of placental vascular function. It has been reported a statistically significant reduction in UV-Q in fetuses showing a ≥20th centile drop in abdominal circumference, suggesting a potential role for these parameters in the early detection of fetal growth alterations, even in the absence of a fully developed FGR phenotype [23]. Previous studies demonstrated that UV-Q is an independent predictor of fetal growth velocity and adverse perinatal outcomes, highlighting its potential as a functional marker for early identification of fetuses at risk [7], 24]. In our study, UV-Q was lower in the group with impaired growth. We observed a significant negative correlation between UV-Q and BW, confirming its role as an independent predictor of BW.
This evidence supports the notion that the population with impaired growth exhibits impairment of the cardiac-fetal-placental unit like nondiabetic population [2], 25].
The use of a ≥40 centile decline between EFW at enrolment and BW centile (DROP) represents an attempt to identify clinically meaningful impairments in fetal growth trajectory that are not captured by the conventional SGA definition. Recent evidence supports the prognostic value of longitudinal growth deceleration in predicting adverse perinatal outcomes. It has been demonstrated that fetuses with a late gestational fall in EFW centile were at increased risk of stillbirth and neonatal complications, even when BW remained above the 10th centile [26]. Similarly, DROP may reflect fetal adaptive responses to chronic hypoxemia or reduced nutrient supply in a subset of pregnancies complicated by GDM, which are typically assumed to be at risk for overgrowth rather than restriction.
In our cohort, the inclusion of fetuses with a marked DROP allowed us to identify a clinically relevant group with abnormal maternal hemodynamics and impaired UV-Q, despite BW often falling within the AGA range. This underscores the potential utility of DROP as a tool for uncovering “hidden” growth restriction phenotypes in GDM pregnancies.
Importantly, while current surveillance strategies in GDM focus primarily on detecting macrosomia, our findings suggest that attention should also be directed toward fetuses at risk of growth deceleration. The integration of DROP into routine fetal growth surveillance may offer a more precise risk stratification model, leading to closer monitoring or earlier delivery when combined with abnormal maternal-fetal hemodynamic markers.
Clinical implications
To date, several biomarkers and composite scoring systems have been proposed to predict FGR, particularly in high-risk pregnancies. Among the most widely studied are uterine artery Doppler velocimetry, maternal serum markers, and fetal biometry-based growth velocity charts. Uterine artery pulsatility index, especially when combined with maternal characteristics, has shown moderate predictive value for early-onset FGR, but its performance is significantly lower in late-onset forms or in GDM pregnancies, where uteroplacental resistance may remain within normal range despite placental dysfunction [27], 28]. Similarly, biomarkers of angiogenesis have demonstrated utility in preeclampsia prediction and early-onset FGR, but their role in normotensive GDM pregnancies remains uncertain [29]. In contrast, the hemodynamic markers used in our study provide a real-time, functional assessment of the maternal-fetal unit, and may capture dynamic alterations preceding overt clinical manifestations [30].
Compared to composite scores such as the Fetal Medicine Foundation (FMF) algorithm for FGR – which integrates maternal factors, biometry, and Doppler [31] – our model offers the advantage of including direct functional measurements of maternal cardiovascular adaptation. The moderate diagnostic performance of our multivariate models (AUC up to 0.78) is comparable to existing algorithms, suggesting that maternal hemodynamics and UV-Q may represent valuable adjuncts to standard assessment tools, particularly in GDM populations where growth impairment is often underestimated.
Strengths
This study has several notable strengths. First, by focusing on pregnancies complicated by GDM, it provides novel insights into early predictors of impaired fetal growth, employing innovative technologies for maternal and fetal assessment. Second, maternal hemodynamic assessment and UV-Q evaluation were performed using standardized protocols by an experienced operator, ensuring reliable and reproducible measurements. Finally, the prospective observational design allowed systematic collection of both maternal and fetal parameters, as well as neonatal outcomes.
Limitations
Several methodological limitations should be acknowledged. First, the sample size, although adequate for an exploratory analysis, was relatively small and cannot be considered representative of the broader population of women GDM. Consequently, chronic maternal conditions (e.g., thyroid disorders, celiac disease, inflammatory bowel disease) were few and heterogeneous, preventing adjustment for their potential impact on maternal hemodynamics and fetal growth; this could be addressed in future studies with larger cohorts.
Additionally, the proportion of cases classified as impaired fetal growth in our cohort (28.5 %) was relatively high, which may reflect the specific characteristics of our study population and further limits the generalizability of the findings.
Both the maternal hemodynamic evaluation using USCOM® and the ultrasound assessment of fetal UV parameters are moderately operator-dependent techniques. Although all examinations were performed by the same expert following standardized protocols, and using modern ultrasound technology allows reliable measurements of the UV-Q and employing a rigorous methodology ensuring that this evaluation achieves moderate to good reproducibility.
Another limitation is the lack of detailed longitudinal data on the degree of glycemic control during pregnancy. While we reported the proportion of women achieving good glycemic control at the last prenatal visit (Table 1), subtle variations throughout gestation cannot be excluded. All women were managed according to standardized protocols, including close glucose monitoring and initiation of insulin or metformin as needed. Although different pharmacological approaches may theoretically influence maternal hemodynamics or fetal growth, the similar distribution of therapy between groups minimizes its potential impact.
Finally, although the ≥40 centiles DROP cutoff is clinically plausible, its choice remains arbitrary and not externally validated. In our cohort, the 10th centile of the observed DROP distribution corresponded to a DROP of 44.5 centiles, which provides some internal support for this threshold but should be interpreted with caution.
Conclusions
In this prospective study of GDM pregnancies, impaired fetal growth was significantly associated with abnormal maternal cardiovascular adaptation and reduced UV-Q. Our findings highlight the role of a hypodynamic maternal hemodynamic profile – characterized by elevated SVR, reduced CO, and decreased DO2 – as a key contributor to impaired fetal growth in GDM pregnancies. Moreover, UV-Q emerged as an independent predictor of growth restriction, supporting its value as a functional marker of placental efficiency.
These results suggest that integrating maternal hemodynamic assessment and UV-Q into growth surveillance protocols may improve risk stratification and early identification of fetuses at risk of underdiagnosed placental insufficiency in GDM pregnancies. Further research in larger cohorts is warranted to validate these findings and evaluate whether targeted surveillance or interventions based on maternal-fetal hemodynamic profiles can improve perinatal outcomes in this population.
-
Research ethics: For this observational study IRB approval was obtained preliminarily. Ethical approval was obtained from the Research Ethics Committee Lazio 2, Rome, Italy (13.23 CET RM2).
-
Informed consent: Informed consent was obtained from all individuals included in this study, or their legal guardians or wards.
-
Author contributions: DF contributed to conception and design of the study, statistical analysis and to writing the article. SN, LM, GG, RF contributed to data collection. HV contributed to the conception and design of the study. GPN and BV contributed to the statistical analysis and the interpretation of the analysis. All authors have accepted responsibility for the entire content of this manuscript and approved its submission.
-
Use of Large Language Models, AI and Machine Learning Tools: None declared.
-
Conflict of interest: The authors state no conflict of interest.
-
Research funding: None declared.
-
Data availability: The datasets generated and/or analyzed during the current study are available from the corresponding author on reasonable request.
References
1. Fasoulakis, Z, Koutras, A, Antsaklis, P, Theodora, M, Valsamaki, A, Daskalakis, G, et al.. Intrauterine growth restriction due to gestational diabetes: from pathophysiology to diagnosis and management. Medicina 2023;59:1139. https://doi.org/10.3390/medicina59061139.Suche in Google Scholar PubMed PubMed Central
2. Valensise, H, Farsetti, D, Pometti, F, Vasapollo, B, Novelli, GP, Lees, C. The cardiac-fetal-placental unit: fetal umbilical vein flow rate is linked to the maternal cardiac profile in fetal growth restriction. Am J Obstet Gynecol 2023;228:222.e1–222.e12. https://doi.org/10.1016/j.ajog.2022.08.004.Suche in Google Scholar PubMed
3. Valensise, H, Novelli, GP, Farsetti, D, Vasapollo, B. Cardiac function. In: Lees, C, Gyselaers, W, editors. Maternal hemodynamics. Cambridge: Cambridge University Press; 2018:24–33 pp.10.1017/9781316661925.003Suche in Google Scholar
4. Vasapollo, B, Novelli, GP, Maellaro, F, Gagliardi, G, Pais, M, Silvestrini, M, et al.. Maternal cardiovascular profile is altered in the preclinical phase of normotensive early and late intrauterine growth restriction. Am J Obstet Gynecol 2025;232:312.e1–312.e21. https://doi.org/10.1016/j.ajog.2024.05.015.Suche in Google Scholar PubMed
5. Vasapollo, B, Novelli, GP, Farsetti, D, Pometti, F, Gagliardi, G, Picone, S, et al.. Maternal hemodynamics in early and late fetal growth restriction. Best Pract Res Clin Obstet Gynaecol 2025;101:102618. https://doi.org/10.1016/j.bpobgyn.2025.102618.Suche in Google Scholar PubMed
6. Novelli, GP, Vasapollo, B, Silvestrini, M, Bertoldo, F, Biscosi, CMP, Maellaro, F, et al.. Definition, identification, implications and management of hypodynamic hypertension in pregnancy. Best Pract Res Clin Obstet Gynaecol 2025;101:102626. https://doi.org/10.1016/j.bpobgyn.2025.102626.Suche in Google Scholar PubMed
7. Farsetti, D, Barbieri, M, Magni, E, Zamagni, G, Monasta, L, Maso, G, et al.. The role of umbilical vein blood flow assessment in the prediction of fetal growth velocity and adverse outcome: a prospective observational cohort study. Am J Obstet Gynecol 2025;233:66.e1–66.e14.10.1016/j.ajog.2025.01.001Suche in Google Scholar PubMed
8. Vasapollo, B, Zullino, S, Novelli, GP, Farsetti, D, Ottanelli, S, Clemenza, S, et al.. Maternal hemodynamics from preconception to delivery: research and potential diagnostic and therapeutic implications: position statement by Italian association of preeclampsia and Italian society of perinatal medicine. Am J Perinatol 2024;41:1999–2013. Erratum in: Am J Perinatol 2024;41:e1. 10.1055/s-0044-1786746.10.1055/a-2267-3994Suche in Google Scholar PubMed
9. Associazione Medici Diabetologi, Italian Society of Diabetology. Italian standards for the treatment of diabetes mellitus 2018. AMD-SID; 2018. Available at: https://aemmedi.it/wp-content/uploads/2009/06/AMD-Standard-unico1.pdf.Suche in Google Scholar
10. Hadlock, FP, Harrist, RB, Sharman, RS, Deter, RL, Park, SK. Estimation of fetal weight with the use of head, body, and femur measurements--a prospective study. Am J Obstet Gynecol 1985;151:333–7.10.1016/0002-9378(85)90298-4Suche in Google Scholar PubMed
11. Papageorghiou, AT, Ohuma, EO, Altman, DG, Todros, T, Cheikh Ismail, L, Lambert, A, et al.. International standards for fetal growth based on serial ultrasound measurements: the fetal growth longitudinal study of the INTERGROWTH-21st project. Lancet 2014;384:869–79. Erratum in: Lancet 2014;384:1264.10.1016/S0140-6736(14)61490-2Suche in Google Scholar PubMed
12. Farsetti, D, Pometti, F, Vasapollo, B, Novelli, GP, Nardini, S, Lupoli, B, et al.. Nitric oxide donor increases umbilical vein blood flow and fetal oxygenation in fetal growth restriction. A pilot study. Placenta 2024;151:59–66. https://doi.org/10.1016/j.placenta.2024.04.014.Suche in Google Scholar PubMed
13. Flo, K, Wilsgaard, T, Acharya, G. Longitudinal reference ranges for umbilical vein blood flow at a free loop of the umbilical cord. Ultrasound Obstet Gynecol 2010;36:567–72. https://doi.org/10.1002/uog.7730.Suche in Google Scholar PubMed
14. Galanti, F, Pisani, I, Riccio, S, Farsetti, D, Vasapollo, B, Novelli, GP, et al.. Systemic vascular resistance may influence the outcome of in vitro fertilization. Gynecol Endocrinol 2022;38:569–72. https://doi.org/10.1080/09513590.2022.2082402.Suche in Google Scholar PubMed
15. Farsetti, D, Pometti, F, Novelli, GP, Vasapollo, B, Khalil, A, Valensise, H. Longitudinal maternal hemodynamic evaluation in uncomplicated twin pregnancies according to chorionicity: physiological cardiovascular dysfunction in monochorionic twin pregnancy. Ultrasound Obstet Gynecol 2024;63:198–205.10.1002/uog.26288Suche in Google Scholar PubMed
16. Valensise, H, Farsetti, D, Pisani, I, Tiralongo, GM, Lo Presti, D, Gagliardi, G, et al.. Friendly help for clinical use of maternal hemodynamics. J Matern-Fetal Neonat Med 2021;34:3075–9. https://doi.org/10.1080/14767058.2019.1678136.Suche in Google Scholar PubMed
17. Valensise, H, Pometti, F, Farsetti, D, Novelli, GP, Vasapollo, B. Hemodynamic assessment in patients with preterm premature rupture of the membranes (pPROM). Eur J Obstet Gynecol Reprod Biol 2022;274:1–4. https://doi.org/10.1016/j.ejogrb.2022.04.027.Suche in Google Scholar PubMed
18. Villar, J, Cheikh Ismail, L, Victora, CG, Ohuma, EO, Bertino, E, Altman, DG, et al.. International standards for newborn weight, length, and head circumference by gestational age and sex: the newborn cross-sectional study of the INTERGROWTH-21st project. Lancet 2014;384:857–68.10.1016/S0140-6736(14)60932-6Suche in Google Scholar PubMed
19. Baschat, AA. Fetal growth restriction - from observation to intervention. J Perinat Med 2010;38:239–46. https://doi.org/10.1515/jpm.2010.041.Suche in Google Scholar PubMed
20. Mecacci, F, Ottanelli, S, Vannuccini, S, Clemenza, S, Lisi, F, Serena, C, et al.. Maternal hemodynamic changes in gestational diabetes: a prospective case-control study. Arch Gynecol Obstet 2022;306:357–63. https://doi.org/10.1007/s00404-021-06288-0.Suche in Google Scholar PubMed
21. Farsetti, D, Vasapollo, B, Pometti, F, Frantellizzi, R, Novelli, GP, Valensise, H. Maternal hemodynamics for the identification of early fetal growth restriction in normotensive pregnancies. Placenta 2022;129:12–14. https://doi.org/10.1016/j.placenta.2022.09.005.Suche in Google Scholar PubMed
22. Vasapollo, B, Novelli, GP, Farsetti, D, Valensise, H. Maternal peripheral vascular resistance at mid gestation in chronic hypertension as a predictor of fetal growth restriction. J Matern-Fetal Neonat Med 2022;35:9834–6. https://doi.org/10.1080/14767058.2022.2056443.Suche in Google Scholar PubMed
23. Stampalija, T, Monasta, L, Barbieri, M, Chiodo, A, Quadrifoglio, M, Fantasia, I, et al.. Late-term fetuses with reduced umbilical vein blood flow volume: an under-recognized population at increased risk of growth restriction. Eur J Obstet Gynecol Reprod Biol 2022;272:182–7.10.1016/j.ejogrb.2022.03.032Suche in Google Scholar PubMed
24. Farsetti, D, Pometti, F, Tiralongo, GM, Lo Presti, D, Pisani, I, Gagliardi, G, et al.. Fetal umbilical vein flow in the classification of fetuses with growth restriction. Reprod Med 2021;2:50–6. https://doi.org/10.3390/reprodmed2010006.Suche in Google Scholar
25. Farsetti, D, Pometti, F, Tiralongo, GM, Lo Presti, D, Pisani, I, Gagliardi, G, et al.. Distinction between SGA and FGR by means of fetal umbilical vein flow and maternal hemodynamics. J Matern-Fetal Neonat Med 2022;35:6593–9. https://doi.org/10.1080/14767058.2021.1918091.Suche in Google Scholar PubMed
26. Sovio, U, White, IR, Dacey, A, Pasupathy, D, Smith, GCS. Screening for fetal growth restriction with universal third trimester ultrasonography in nulliparous women in the pregnancy outcome prediction (POP) study: a prospective cohort study [published correction appears in Lancet 2015 Nov 21;386(10008):2058. 10.1016/S0140-6736(15)00976-9]. Lancet 2015;386:2089–97.10.1016/S0140-6736(15)00131-2Suche in Google Scholar PubMed PubMed Central
27. Gómez, O, Figueras, F, Martínez, JM, del Río, M, Palacio, M, Eixarch, E, et al.. Sequential changes in uterine artery blood flow pattern between the first and second trimesters of gestation in relation to pregnancy outcome. Ultrasound Obstet Gynecol 2006;28:802–8. https://doi.org/10.1002/uog.2814.Suche in Google Scholar PubMed
28. Chatzakis, C, Eleftheriades, M, Demertzidou, E, Eleftheriades, A, Koletsos, N, Lavasidis, L, et al.. Uterine arteries resistance in pregnant women with gestational diabetes mellitus, diabetes mellitus type 1, diabetes mellitus type 2, and uncomplicated pregnancies. Biomedicines 2023;11:3106. https://doi.org/10.3390/biomedicines11123106.Suche in Google Scholar PubMed PubMed Central
29. Zeisler, H, Llurba, E, Chantraine, F, Vatish, M, Staff, AC, Sennström, M, et al.. Predictive value of the sFlt-1:PlGF ratio in women with suspected preeclampsia. N Engl J Med 2016;374:13–22. https://doi.org/10.1056/nejmoa1414838.Suche in Google Scholar PubMed
30. Masini, G, Tay, J, McEniery, CM, Wilkinson, IB, Valensise, H, Tiralongo, GM, et al.. Maternal cardiovascular dysfunction is associated with hypoxic cerebral and umbilical Doppler changes. J Clin Med 2020;9:2891. https://doi.org/10.3390/jcm9092891.Suche in Google Scholar PubMed PubMed Central
31. Poon, LC, Karagiannis, G, Leal, A, Romero, XC, Nicolaides, KH. Hypertensive disorders in pregnancy: screening by uterine artery Doppler and mean arterial pressure at 11–13 weeks. Ultrasound Obstet Gynecol 2009;34:497–502. https://doi.org/10.1002/uog.7439.Suche in Google Scholar PubMed
© 2025 the author(s), published by De Gruyter, Berlin/Boston
This work is licensed under the Creative Commons Attribution 4.0 International License.
Artikel in diesem Heft
- Frontmatter
- Editorial
- The fetus as a patient in the 21st century: science, ethics, technology and global responsibility
- Vision, Education, and the Future of Perinatal Medicine
- Opening – field direction, education, and AI
- Quo vadis neonatologia? Where is neonatology heading in the 21st century?
- Shaping the future: advancing maternal-fetal medicine through educational standards and innovations
- Integrating generative AI in perinatology: applications for literature review
- Maternal Hemodynamics, Fetal Physiology, and Surveillance
- Core fetal physiology and maternal-fetal interaction
- Cardiac output-guided maternal positioning may protect the fetal oxygen supply and thereby reduce pregnancy complications
- Effect of antenatal betamethasone on fetal heart rate short-term variability in growth restricted fetuses
- Umbilical venous flow and maternal hemodynamics as predictors of impaired fetal growth in gestational diabetes: a prospective study
- The impact of maternal cardiovascular status prior to labor on birth outcomes: an observational study
- Complex Pregnancies, Placenta, and Fetal Therapy
- Twins, placental disease, fetal intervention, and periviability
- Complications in monochorionic twin pregnancies
- Association of discordance in birth weights of dichorionic twins with the incidence of preeclampsia in pregnant women
- Management and outcomes of periviable infants in Slovenia: a decade of experience
- Successful management of severe hemolytic disease of the fetus and newborn (HDFN) due to anti-Kell
- Systems of Care, Screening, and Population-Level Perinatal Medicine
- Public health, structured care, and national data
- Structured stillbirth management in Slovenia: outcomes and comparison with international guidelines
- Newborn screening for rare diseases: expanding the paradigm in the genomic era
- Ten years of experience with screening for diabetes in pregnancy according to IADPSG criteria in Slovenia
- Gestational diabetes and fetal macrosomia: a dissenting opinion
- Advanced Prenatal Diagnosis
- Imaging and fetal anomaly detectionata
- Detection of isolated fetal limb anomalies using 3D/4D ultrasound
- Ethics, Professional Responsibility, and Patient-Centered Counseling
- The moral and communicative core of “Fetus as a Patient”
- The fetus as a patient: professional responsibility in contemporary Perinatal Medicine
- Placenta-oriented counseling: challenges and opportunities in obstetric practice
- Patient education materials: improving readability to advance health equity
- Global Health, Pandemic, and Humanitarian Perinatal Medicine
- COVID-19, war, immunity, and respectful care
- Clinical factors in SARS-CoV-2 antibody response in unvaccinated mothers
- Serum vitamin D and inflammatory markers in SARS-CoV-2 positive pregnant women
- Perceptions of respectful maternity care in Ukraine during a time of war
- Role of prelabour midwifery consultation in enhancing maternal satisfaction and preparedness for birth
- Obstetric Decision-Making and Postpartum Outcomes
- Clinical controversies and maternal outcomes
- Should we conduct a trial of labor in women with a macrosomic fetus?
- Postpartum maternal complications: a retrospective single-center study
- Annual Reviewer Acknowledgment
- Reviewer Acknowledgment
Artikel in diesem Heft
- Frontmatter
- Editorial
- The fetus as a patient in the 21st century: science, ethics, technology and global responsibility
- Vision, Education, and the Future of Perinatal Medicine
- Opening – field direction, education, and AI
- Quo vadis neonatologia? Where is neonatology heading in the 21st century?
- Shaping the future: advancing maternal-fetal medicine through educational standards and innovations
- Integrating generative AI in perinatology: applications for literature review
- Maternal Hemodynamics, Fetal Physiology, and Surveillance
- Core fetal physiology and maternal-fetal interaction
- Cardiac output-guided maternal positioning may protect the fetal oxygen supply and thereby reduce pregnancy complications
- Effect of antenatal betamethasone on fetal heart rate short-term variability in growth restricted fetuses
- Umbilical venous flow and maternal hemodynamics as predictors of impaired fetal growth in gestational diabetes: a prospective study
- The impact of maternal cardiovascular status prior to labor on birth outcomes: an observational study
- Complex Pregnancies, Placenta, and Fetal Therapy
- Twins, placental disease, fetal intervention, and periviability
- Complications in monochorionic twin pregnancies
- Association of discordance in birth weights of dichorionic twins with the incidence of preeclampsia in pregnant women
- Management and outcomes of periviable infants in Slovenia: a decade of experience
- Successful management of severe hemolytic disease of the fetus and newborn (HDFN) due to anti-Kell
- Systems of Care, Screening, and Population-Level Perinatal Medicine
- Public health, structured care, and national data
- Structured stillbirth management in Slovenia: outcomes and comparison with international guidelines
- Newborn screening for rare diseases: expanding the paradigm in the genomic era
- Ten years of experience with screening for diabetes in pregnancy according to IADPSG criteria in Slovenia
- Gestational diabetes and fetal macrosomia: a dissenting opinion
- Advanced Prenatal Diagnosis
- Imaging and fetal anomaly detectionata
- Detection of isolated fetal limb anomalies using 3D/4D ultrasound
- Ethics, Professional Responsibility, and Patient-Centered Counseling
- The moral and communicative core of “Fetus as a Patient”
- The fetus as a patient: professional responsibility in contemporary Perinatal Medicine
- Placenta-oriented counseling: challenges and opportunities in obstetric practice
- Patient education materials: improving readability to advance health equity
- Global Health, Pandemic, and Humanitarian Perinatal Medicine
- COVID-19, war, immunity, and respectful care
- Clinical factors in SARS-CoV-2 antibody response in unvaccinated mothers
- Serum vitamin D and inflammatory markers in SARS-CoV-2 positive pregnant women
- Perceptions of respectful maternity care in Ukraine during a time of war
- Role of prelabour midwifery consultation in enhancing maternal satisfaction and preparedness for birth
- Obstetric Decision-Making and Postpartum Outcomes
- Clinical controversies and maternal outcomes
- Should we conduct a trial of labor in women with a macrosomic fetus?
- Postpartum maternal complications: a retrospective single-center study
- Annual Reviewer Acknowledgment
- Reviewer Acknowledgment