Diagnosis of cleft lip-palate during nuchal translucency screening – case report and review of the literature
-
Ashwin R. Jadhav
 ,
Ana Monteagudo
,
Ana Monteagudo

Abstract
Orofacial clefts are the most common group of craniofacial anomalies. The detection rate of cleft lip during the mid-trimester, using two-dimensional (2D) ultrasound screening, has improved over the last three decades. However, the detection rates of defects involving the hard palate or isolated cleft palate have remained poor. Over the last decade, many investigators have studied the use of 3D ultrasound to improve the detection rates of these defects. With the increasing use and acceptance of first-trimester aneuploidy screening in the US, there is growing interest in performing first-trimester fetal anatomy surveys. Reports of first-trimester diagnosis of cleft lip and palate are rare, and this aspect of prenatal sonographic diagnosis remains underexplored. We report a case of unilateral cleft lip and cleft palate diagnosed during a routine first-trimester screening at 12 weeks’ gestation and review the pertinent literature on first-trimester diagnosis of cleft lip/palate.
Introduction
Cleft lip and/or palate (CL±P) remains the most common group of craniofacial anomalies. In the second trimester, as part of the anatomic survey, evaluation of the fetal lips is routinely done using two-dimensional (2D) ultrasound. At this time in gestation, 2D ultrasound has excellent detection rates for defects involving the lip and alveolar ridge. However, prenatal detection of abnormalities involving the hard and secondary soft palate remains a challenge. Using 3D ultrasound, several techniques have been developed to improve on the detection rates of the secondary palate [1, 13, 14].
Ultrasound evaluation of the fetus during first-trimester screening provides a unique opportunity for the early evaluation of the fetal anatomy. Diagnosis of CL±P during the first trimester is rare but possible. In this report, we describe a case of CL±P diagnosed during first-trimester screening, using both 2D and 3D sonography, and confirmed during the second-trimester scan. Unilateral CL±P was ultimately confirmed at the birth of the child.
Case
A 36-year-old primigravida was referred to the New York University ultrasound unit for nuchal translucency (NT) screening at 12 weeks and 5 days’ gestation. The NT measured 1.7 mm, while the serum screen was normal. An early anatomical survey at the time of the first-trimester screen revealed unilateral left cleft lip and palate (Figure 1). Subsequently, a transvaginal 3D scan was performed using a GE E8 ultrasound machine with a 5–9 transvaginal transducer (General Electric Medical Division, Milwaukee, WI, USA), which further confirmed the diagnosis (Figure 2). No other anomalies were found during this anatomy survey. Subsequently, ultrasound at 21 weeks’ gestation showed the same anomaly detected during the first-trimester anomaly screening (Figure 3). Prenatal consultation with an orofacial surgeon was obtained at 22 weeks’ gestation. The pregnancy remained otherwise uncomplicated, and delivery was at term as planned. Delivery was attended by the “cleft team” for postnatal management.
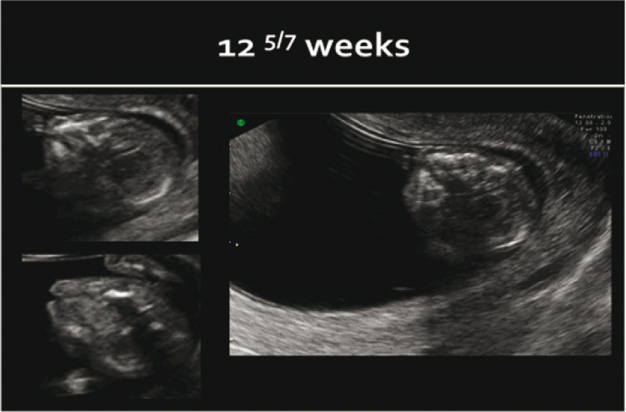
First-trimester anatomy survey during NT screening showing unilateral cleft lip and palate at 12 weeks and 5 days’ gestation.
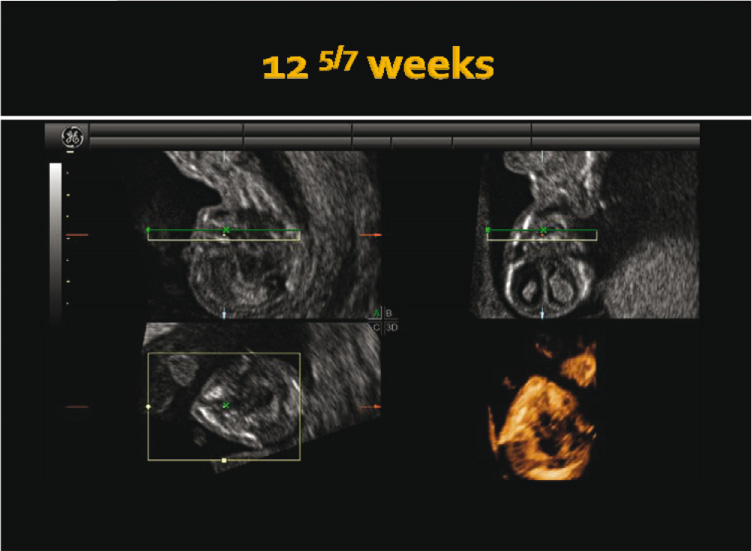
Three-dimensional rendered image of unilateral cleft lip and palate at 12 weeks and 5 days’ gestation.
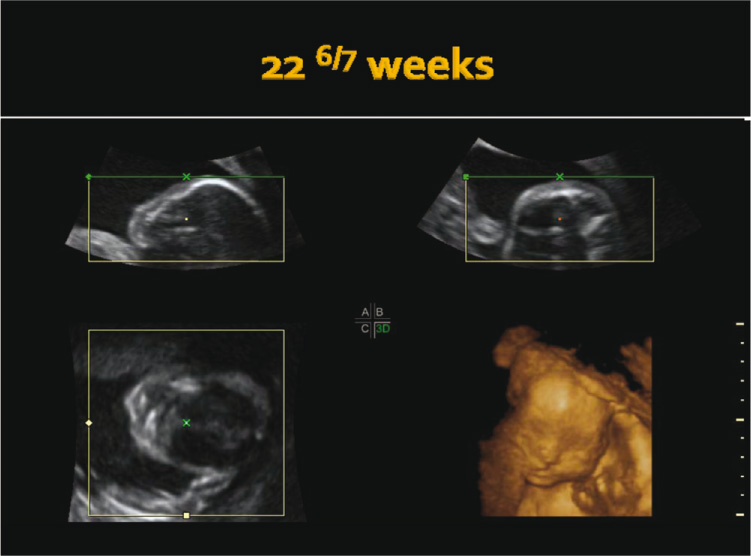
Three-dimensional rendering of cleft lip-palate at subsequent evaluation in the second trimester.
Discussion
Orofacial clefts are the second largest group of anomalies diagnosed during prenatal care, second only to congenital heart defects. In the US, cleft lip with or without cleft palate is estimated to affect 1 in 1000 live births, and isolated cleft palate affects approximately 0.6 in 1000 live births [2]. The first description of an ultrasound diagnosis of cleft lip/palate was published by Christ and Meininger in 1981 [4]. Over the last three decades, despite the use of significantly improved technology and experience, the detection rate using 2D ultrasound has continued to be far from expectations. Multiple population-based studies have demonstrated poor detection rates for orofacial clefts with the current standard of care of 2D ultrasound evaluation. Detection rates range from 0% to 70% for all types of clefts, 33% to 88% for CL±P, and 0% to 22% for isolated cleft palate [9].
During the last decade, efforts to improve antenatal diagnosis of orofacial clefts have led to the development of 3D techniques to aid the diagnosis, including 3D reverse face view [1], flipped face view [14], and also the oblique evaluation technique of the secondary palate described by Pilu and Segata [13]. The use of 3D techniques has been shown to improve the detection rate of orofacial clefts in cases suspicious of the pathology, using initial 2D ultrasound screening [3]. The same is true for the routine use of 3D ultrasound in high-risk groups [17]. The major downside is that 3D imaging techniques and expertise are available only at a few specialized and/or tertiary-care centers. Worldwide, there is increasing focus on early diagnosis of fetal anomalies and also on evaluation of the maternal-fetal-placental unit for predicting risks for adverse pregnancy outcomes. In the US, starting from the first description of NT [11] to completion of the FASTER trial [5, 6], the envelope of prenatal diagnosis is slowly shifting from mid-trimester to late first trimester.
During organogenesis, orofacial development – especially that of the primary palate – is completed by the 7th postconception week (9 postmenstrual weeks) [18]. Reports on first-trimester diagnosis of cleft lip and palate are rare, with only a few articles published over the last two decades [7, 8, 10, 12]. The pertinent literature attests to the fact that during first- trimester screening, one should concentrate on detecting facial clefts. Overall, the utility of first-trimester anatomy survey for prenatal diagnosis of orofacial clefts remains underexplored.
First-trimester screening presents a unique opportunity for early sonographic assessment of other pathologies in general and those of facial clefts in particular. With the relatively smaller size of the fetus, it is much easier to scan the orofacial region in trained hands. There is mounting evidence that increased NT is associated with structural anomalies, including orofacial clefts, even in chromosomally normal fetuses. Timmerman and colleagues [16] evaluated the association of increased NT (>95 percentile) with cleft lip/palate in a retrospective cohort study of 8638 fetuses. They found an increased risk of isolated cleft lip/palate [relative risk (RR), 7.6; 95% confidence interval (95% CI), 1.9–30.4]; the risk of cleft lip/palate as an associated finding with other anomalies was even higher (RR, 53.5; 95% CI, 11.1–256.6). Even though only 2 out of 10 cases of cleft lip/palate were diagnosed during the NT-scan, anatomy survey was not part of ultrasound evaluation.
Sepulveda and colleagues [15] used 2D and 3D ultrasound during NT scans for the evaluation of the “midfacial” area. They evaluated what they called the “retronasal triangle” for diagnosing cleft lip/palate. The base of the triangle is considered to represent the hard palate. The authors report successful evaluation of the retronasal triangle in 98 of 100 normal fetuses during NT screening, demonstrating the feasibility of screening for cleft palate. As there were no cases diagnosed during the study, larger prospective studies are needed to validate the authors’ approach.
As said above, we now routinely perform anatomy survey during first-trimester screening when we scan for NT. We suggest that screening for anomalies is possible in the late first trimester. This case demonstrates and emphasizes that early and accurate diagnosis of cleft lip and palate in the first trimester, as early as 12 weeks’ gestation, is a real possibility. It should be attempted at the time of ultrasound for first-trimester screening.
References
[1] Campbell S, Lees C, Moscoso G, Hall P. Ultrasound antenatal diagnosis of cleft palate by a new technique: the 3D “reverse face” view. Ultrasound Obstet Gynecol. 2005;25:12–8.10.1002/uog.1819Search in Google Scholar PubMed
[2] Canfield MA, Honein MA, Yuskiv N, Xing J, Mai CT, Collins JS, et al. National estimates and race/ethnic-specific variation of selected birth defects in the United States, 1999–2001. Birth Defects Res A Clin Mol Teratol. 2006;76:747–56.10.1002/bdra.20294Search in Google Scholar PubMed
[3] Chmait R, Pretorius D, Jones M, Hull A, James G, Nelson T, et al. Prenatal evaluation of facial clefts with two-dimensional and adjunctive three-dimensional ultrasonography: a prospective trial. Am J Obstet Gynecol. 2002;187:946–9.10.1067/mob.2002.127127Search in Google Scholar PubMed
[4] Christ JE, Meininger MG. Ultrasound diagnosis of cleft lip and cleft palate before birth. Plast Reconstr Surg. 1981;68:854–9.10.1097/00006534-198112000-00002Search in Google Scholar PubMed
[5] D’Alton M, Cleary-Goldman J. First and second trimester evaluation of risk for fetal aneuploidy: the secondary outcomes of the FASTER Trial. Semin Perinatol. 2005;29:240–6.10.1053/j.semperi.2005.06.006Search in Google Scholar PubMed
[6] Dugoff L, Hobbins JC, Malone FD, Porter TF, Luthy D, Comstock CH, et al. First-trimester maternal serum PAPP-A and free-β subunit human chorionic gonadotropin concentrations and nuchal translucency are associated with obstetric complications: a population-based screening study (the FASTER Trial). Am J Obstet Gynecol. 2004;191:1446–51.10.1016/j.ajog.2004.06.052Search in Google Scholar PubMed
[7] Ghi T, Arcangeli T, Radico D, Cavallotti D, Contro E, Pelusi G. Three-dimensional sonographic imaging of fetal bilateral cleft lip and palate in the first trimester. Ultrasound Obstet Gynecol. 2009;34:119–20.10.1002/uog.6430Search in Google Scholar PubMed
[8] Gullino E, Serra M, Ansaldi C, Massobrio M, Pagliano M. Bilateral cleft lip and palate diagnosed sonographically at 11 weeks of pregnancy. J Clin Ultrasound. 2006;34:398–401.10.1002/jcu.20238Search in Google Scholar PubMed
[9] Maarse W, Bergé SJ, Pistorius L, van Barneveld T, Kon M, Breugem C, et al. Diagnostic accuracy of transabdominal ultrasound in detecting prenatal cleft lip and palate: a systematic review. Ultrasound Obstet Gynecol. 2010;35:495–502.10.1002/uog.7472Search in Google Scholar PubMed
[10] Markov D, Jacquemyn Y, Leroy Y. Bilateral cleft lip and palate associated with increased nuchal translucency and maternal cocaine abuse at 14 weeks of gestation. Clin Exp Obstet Gynecol. 2003;30:109–10.Search in Google Scholar
[11] Nicolaides KH, Azar G, Byrne D, Mansur C, Marks K. Fetal nuchal translucency: ultrasound screening for chromosomal defects in first trimester of pregnancy. Br Med J. 1992;304:867–9.10.1136/bmj.304.6831.867Search in Google Scholar PubMed PubMed Central
[12] Picone O, de Keersmaecker B, Ville Y. [Ultrasonographic features of orofacial clefts at first trimester of pregnancy: report of two cases]. J Gynecol Obstet Biol Reprod (Paris). 2003;32:736–9.Search in Google Scholar
[13] Pilu G, Segata M. A novel technique for visualization of the normal and cleft fetal secondary palate: angled insonation and three-dimensional ultrasound. Ultrasound Obstet Gynecol. 2007;29:166–9.10.1002/uog.3877Search in Google Scholar PubMed
[14] Platt LD, Devore GR, Pretorius DH. Improving cleft palate/cleft lip antenatal diagnosis by 3-dimensional sonography: the “flipped face” view. J Ultrasound Med. 2006;25:1423–30.10.7863/jum.2006.25.11.1423Search in Google Scholar PubMed
[15] Sepulveda W, Wong AE, Martinez-Ten P, Perez-Pedregosa J. Retronasal triangle: a sonographic landmark for the screening of cleft palate in the first trimester. Ultrasound Obstet Gynecol. 2010;35:7–13.10.1002/uog.7484Search in Google Scholar PubMed
[16] Timmerman E, Pajkrt E, Maas SM, Bilardo CM. Enlarged nuchal translucency in chromosomally normal fetuses: strong association with orofacial clefts. Ultrasound Obstet Gynecol. 2010;36:427–32.10.1002/uog.7650Search in Google Scholar PubMed
[17] Wang LM, Leung KY, Tang M. Prenatal evaluation of facial clefts by three-dimensional extended imaging. Prenat Diagn. 2007;27:722–9.10.1002/pd.1766Search in Google Scholar PubMed
[18] Wantia N, Rettinger G. The current understanding of cleft lip malformations. Facial Plast Surg. 2002;18:147–53.10.1055/s-2002-33061Search in Google Scholar PubMed
-
The authors stated that there are no conflicts of interest regarding the publication of this article.
©2012 by Walter de Gruyter Berlin Boston
Articles in the same Issue
- Masthead
- Masthead
- Editorial
- Editorial
- Case reports – Obstetrics
- Sonographic presentations of uterine rupture following vaginal birth after cesarean – report of two cases 12 h apart
- Prenatal diagnosis of thrombocytopenia-absent radius syndrome
- Cervico-isthmic pregnancy with cervical placenta accreta
- Prelabor uterine rupture and extrusion of fetus with intact amniotic membranes: a case report
- Hyperreactio luteinalis in a spontaneously conceived pregnancy associated with polycystic ovarian syndrome and high levels of human chorionic gonadotropin
- Should clinicians advise terminating a pregnancy following the diagnosis of a serious fetal cardiac abnormality?
- Absence of hemolytic disease of fetus and newborn (HDFN) in a pregnancy with anti-Yka (York) red cell antibody
- Congenital midgut malrotation causing intestinal obstruction in midpregnancy managed by prolonged total parenteral nutrition: case report and review of the literature
- Skin popping scars – a telltale sign of past and present subcutaneous drug abuse
- Botulinum toxin for the treatment of achalasia in pregnancy
- Thrombotic stroke in association with ovarian hyperstimulation and early pregnancy rescued by thrombectomy
- Normal pregnancy outcome in a woman with chronic myeloid leukemia and epilepsy: a case report and review of the literature
- Three-dimensional power Doppler assessment of pelvic structures after unilateral uterine artery embolization for postpartum hemorrhage
- Deep congenital hemangioma: prenatal diagnosis and follow-up
- Case reports – Fetus
- Diagnosis of cleft lip-palate during nuchal translucency screening – case report and review of the literature
- Vein of Galen aneurysm that was diagnosed prenatally and supracardiac obstructed total anomalous pulmonary venous return with pulmonary hypertension: case report
- A fetus with 19q13.11 microdeletion presenting with intrauterine growth restriction and multiple cystic kidneya
- Prenatal detection of periventricular pseudocysts by ultrasound: diagnosis and outcome
- Twin-to-twin transfusion syndrome and limb ischemia: a case report
- Prenatal surgery in a triplet pregnancy complicated by a double twin reversed arterial perfusion (TRAP) sequence
- A case of a four-vessel umbilical cord: don’t stop counting at three!
- Case reports – Newborn
- Supratentorial hemorrhage suggested on susceptibility-weighted magnetic resonance imaging in an infant with hydranencephaly
- Differential diagnosis of pseudotrisomy 13 syndrome
- Carey-Fineman-Ziter syndrome: a spectrum of presentations
Articles in the same Issue
- Masthead
- Masthead
- Editorial
- Editorial
- Case reports – Obstetrics
- Sonographic presentations of uterine rupture following vaginal birth after cesarean – report of two cases 12 h apart
- Prenatal diagnosis of thrombocytopenia-absent radius syndrome
- Cervico-isthmic pregnancy with cervical placenta accreta
- Prelabor uterine rupture and extrusion of fetus with intact amniotic membranes: a case report
- Hyperreactio luteinalis in a spontaneously conceived pregnancy associated with polycystic ovarian syndrome and high levels of human chorionic gonadotropin
- Should clinicians advise terminating a pregnancy following the diagnosis of a serious fetal cardiac abnormality?
- Absence of hemolytic disease of fetus and newborn (HDFN) in a pregnancy with anti-Yka (York) red cell antibody
- Congenital midgut malrotation causing intestinal obstruction in midpregnancy managed by prolonged total parenteral nutrition: case report and review of the literature
- Skin popping scars – a telltale sign of past and present subcutaneous drug abuse
- Botulinum toxin for the treatment of achalasia in pregnancy
- Thrombotic stroke in association with ovarian hyperstimulation and early pregnancy rescued by thrombectomy
- Normal pregnancy outcome in a woman with chronic myeloid leukemia and epilepsy: a case report and review of the literature
- Three-dimensional power Doppler assessment of pelvic structures after unilateral uterine artery embolization for postpartum hemorrhage
- Deep congenital hemangioma: prenatal diagnosis and follow-up
- Case reports – Fetus
- Diagnosis of cleft lip-palate during nuchal translucency screening – case report and review of the literature
- Vein of Galen aneurysm that was diagnosed prenatally and supracardiac obstructed total anomalous pulmonary venous return with pulmonary hypertension: case report
- A fetus with 19q13.11 microdeletion presenting with intrauterine growth restriction and multiple cystic kidneya
- Prenatal detection of periventricular pseudocysts by ultrasound: diagnosis and outcome
- Twin-to-twin transfusion syndrome and limb ischemia: a case report
- Prenatal surgery in a triplet pregnancy complicated by a double twin reversed arterial perfusion (TRAP) sequence
- A case of a four-vessel umbilical cord: don’t stop counting at three!
- Case reports – Newborn
- Supratentorial hemorrhage suggested on susceptibility-weighted magnetic resonance imaging in an infant with hydranencephaly
- Differential diagnosis of pseudotrisomy 13 syndrome
- Carey-Fineman-Ziter syndrome: a spectrum of presentations