Using post transplant 1 week Tc-99m DTPA renal scan as another method for predicting renal graft failure
-
 ,
,

Abstract
Purpose
The aims of this study were to determine whether post transplant renal scan performed at around 1 week can predict graft failure, and to identify the best predictive factors among easy-to-measure variables.
Materials and methods
We retrospectively evaluated patients who underwent Tc-99m DTPA renal scan at approximately 1 week after renal transplantation. They were separated into two categories at 3 months after the operation; graft failure and non-failure. Graft failure was confirmed by biopsy (rejection). Non-failure was confirmed either by biopsy or clinical follow-up with serum creatine (Cr). Scan parameters including glomerular filtration rate (GFR), Hilson perfusion index, peaks of the iliac and graft perfusion curves were analyzed. Clinical variables including age, sex, height, weight, systolic blood pressure, serum Cr, type of donated kidney, side of transplant, and immunosuppressant were also analyzed.
Results
Among total 45 patients, graft failure was present in 11 cases. The serum Cr level was significantly higher in the failure group. Among scan variables, only the GFR was significantly different between groups. GFR of <44.48 mL/min was predictive of graft failure (sen 88.9%). Serum Cr level >2.13 mg/dL was also predictive (sen 72.7%).
Conclusion
GFR on renal scan at approximately 1 week after kidney transplant can predict graft failure.
1 Introduction
Graft rejection after kidney transplant is a major problem, and a reliable predictor of graft function is necessary for optimal management of renal transplant patients [1]. The current gold standard for the diagnosis of transplant rejection is invasive core needle biopsy, which carries a risk of graft injury and, furthermore, is not immediately feasible in patients who are taking anticoagulants [2]. A non-invasive method to predict rejection after kidney transplant would be ideal.
Renal scintigraphy (scan) is now widely used to evaluate graft function [3]. Technetium-99m (Tc-99m) diethylenetriaminepentaacetic acid (DTPA) is a reliable tracer for renal scintigraphy, as is technetium-99m mercaptoacetyltriglycine (MAG3). Previous studies have revealed good results with scintigraphy in transplanted kidneys. Most of these studies have relied on early scanning, which was performed within 4 days, and even at 1 day, post transplant [3, 4, 5, 6, 7, 8, 9, 10, 11], and a comparison of post transplant scans at 3 days and 7 days postoperatively in the same patient seemed to show that only the post transplant day-3 scan could predict the graft outcome [10]. However, for various reasons, early scanning is not always possible, as is the situation at our institution, where renal scans are not routinely performed until approximately 1 week after transplant.
Among the parameters from DTPA scan, Kirchner’s index, Hilson’s index, the kidney-to-aorta ratio, graft washout, time difference between peak renal perfusion count and peak arterial count, peak renal perfusion count/counts at plateau, peak renal perfusion/peak renal uptake, renal counts at 20 min/renal counts at 3 min, and others, may be evaluated to assess graft function [8]. One group has recently reported a new index for predicting graft function based on a formula using existing variables [5], but as yet, there has been no consensus about which indices are most useful [6, 12]. In addition, in routine clinical practice, the parameters mentioned above are not all easy to obtain.
An easily measured parameter from renal scintigraphy performed at about 1 week after transplantation is needed. The aims of this study were to find out whether a renal scan performed at approximately 1 week post transplant can be used to predict graft failure and to identify the best predictive factors among easy-to-measure variables.
2 Materials and methods
2.1 Patients
This retrospective observational study was carried out in accordance with the Declaration of Helsinki. Patients who met all of the following inclusion criteria were enrolled: 1) renal transplantation performed at our institution between the years 2005 to 2010; 2) renal scan performed at approximately 1 week (5 to 8 days) after transplantation; 3) follow-up performed at our institution at approximately 3 months post transplant. We excluded patients whose follow-up data were missing and those whose renal scans were considered incorrect due to failure of DTPA bolus injection. They were categorized into two groups based on the status 3 months after the operation; graft failure group vs non-failure group. Graft failure was confirmed by renal biopsy (rejection). Non-failure group was confirmed either by renal biopsy or by clinical follow-up with normal serum creatinine (Cr) levels (<1.5 mg/dL) over 1 year. The study methods of patient enrolment and grouping is shown in Figure 1.
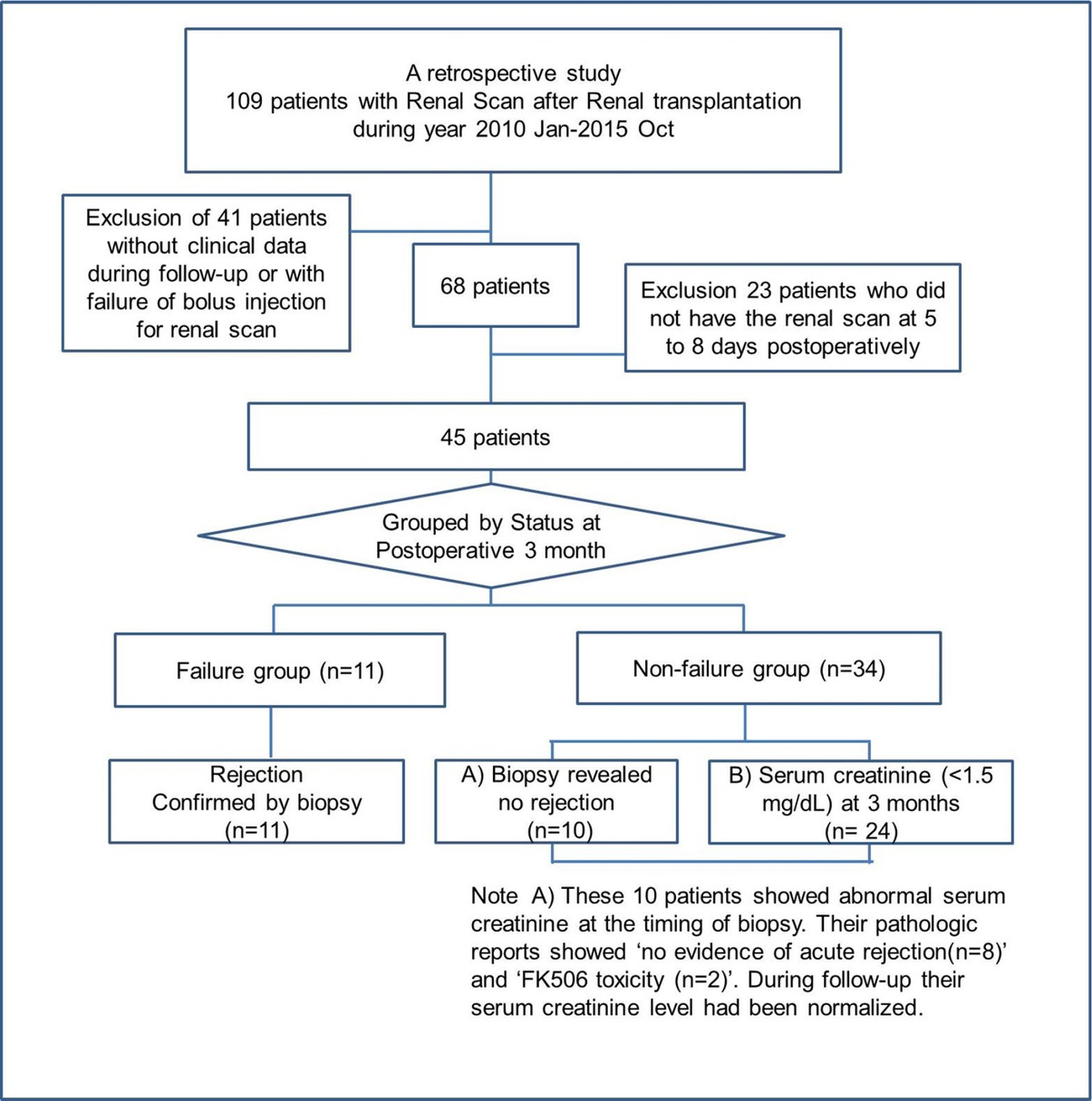
Enrolled patients and grouping
2.2 Renal scintigraphy (Renal scan)
Patients were instructed to have adequate hydration before scanning. Gamma camera (Dual head SPECT, INFINIA GP3, GE) Tc-99m DTPA (340 MBq intravenous bolus) scans, anterior views, were performed with patients lying in a supine position on the camera bed. The gamma camera was equipped with a low-energy, parallel-hole, all-purpose collimator. Sequential 60-s perfusion images (1 s/frame) and sequential 20-min images (30 s/frame) were obtained. Image processing was performed using Exeleris Functional Imaging Workstation software (GE). Regions-of-interest (ROIs) were defined for the cortex of the transplanted kidney, iliac artery, and background. Each ROI was firstly drawn automatically and then manually corrected by the same technician, and in every case, the same nuclear medicine physician confirmed the ROIs. Once the ROIs were drawn, the software automatically calculated the glomerular filtration rate (GFR), the Hilson perfusion index [9] (100 × [area under arterial curve to peak] / [area under renal curve]), time (s) between the peaks of the iliac and graft perfusion curves (ΔP)[13], and time (s) for the declining counts on the renal perfusion curve to reach half of the peak value (T½ of graft washout; GW½) [5, 13] of renal perfusion.
2.3 Statistical analysis
2.3.1 Variables
Variables from renal scan including GFR, Hilson perfusion index, ΔP, and GW½, were analyzed, along with clinical variables including age, sex, height, weight, diabetes mellitus, underlying renal disease, systolic blood pressure, serum Cr level at the time of the renal scan, type of donated kidney, side of the transplant, regimen of immunosuppressive therapy, infection, surgical complication and accompanying disease. In addition, we analyzed whether they had an episode of acute kidney injury (AKI) during the 3 months after transplantation (AKI was defined as increase in serum Cr by ≥0.3 mg/dl within 48 hours or increase in serum Cr to 1.5 times from baseline which is known or presumed to have occurred within the prior 7 days or urine volume <0.5 ml/kg/h for 6 h) [14]. P<0.05 was considered significant.
2.3.2 Statistical analysis
We used Shapiro-Wilk normality test to evaluate data for parametric tests including t-test, chi-squared, chi-square for trend, or simple correlation. Data rejected by the normality test were analyzed by non-parametric tests including the Mann-Whitney U test, Fisher’s exact test, or Wilcoxon signed-rank test. Receiver-operator curve (ROC) analysis was also performed. MedCalc software (ver. 13.3.3.0; MedCalc, Inc., Ostend, Belgium) was used for the analyses and p-values <0.05 were considered to be statistically significant.
2.4 Results
2.4.1 Enrolled patients
As shown in Figure 1, a total of 109 patients underwent renal scan after kidney transplantation at our institution from January 2010 to October 2015. Sixty-four patients were excluded due to lack of clinical data, failure of DTPA bolus injection, or too-long interval between transplantation and scan, and finally, 45 patients who underwent postoperative renal scan at approximately 1 week (day 5 to day 8) after kidney transplant were included.
There were 11 patients who had transplant rejection confirmed by biopsy (Graft failure group). The other 34 patients were in non-failure group. In the non-failure group, 10 patients underwent biopsy and their biopsy results were as follows; ‘no evidence of acute rejection (n=8)’ and ‘FK506 (tacrolimus) toxicity (n=2)’. They underwent renal biopsy due to increased serum Cr at that time and their serum Cr level had been normalized later. In all of the patients in the non-failure group, the serum Cr level remained normal through 1 year post operation. Table 1 shows the patient characteristics for both groups.
Patient characteristics at the time of renal scan
| Variable | |
|---|---|
| Malea | 27 (60%) |
| Ageb | 45±10.2 |
| Body weight, kgb | 64.6 ± 13.7 |
| Height, cmb | 164.6 ±7.8 |
| Body mass index (BMI)b | 23.71 ± 4.0 |
| Type of donated kidneya | |
| DDKT | 38 (84.4%) |
| LDKT | 4 (8.9%) |
| ABOi LDKT | 3 (6.7%) |
| Side of transplant, righta | 43 (95.6%) |
| Time from operation to renal biopsyb,c | 1.27 ± 0.87 months (0.3 to 3.0 months) |
| Time from operation to DTPA scanb | 7± 0.89 days (5 to 8 days) |
-
a n (%)
b mean ± standard deviation
c Renal biopsy was performed in 21 patients
Abbreviations: scan, scintigraphy; DDKT, deceased donor kidney transplant; LDKT, living donor kidney transplant; ABOi LDKT, ABO-incompatible LDKT.
Their underlying renal diseases were chronic glomerulonephritis (n=10), hypertensive nephropathy (n=6), diabetic nephropathy (n=3), IgA nephropathy (n=2), chronic interstitial nephritis (n=1), lupus nephritis (n=1), obstructive nephropathy (n=1) and others were unknown origin. Surgical complications were shown in some patients as follows; seroma (n=4), lymphocele (n=3), hematoma (=1), leakage (n=1), hydronephrosis (n=1), and wound infection (n=1). Accompanying disease before kidney transplantation were shown in some patients as follows; chronic hepatitis C (n=2), dilated cardiomyopathy (n=2), gout (n=3), hepatitis B virus carrier (n=1), hypothyroidism (n=1), overlap syndrome of rheumatoid arthritis and systemic lupus erythematosus (n=1), thyroid cancer (n=2), Crohn’s disease (n=1).
Infection during follow-up were shown in some patients as follows; cytomegalovirus infection (n=1), pulmonary fungal infection (n=1), influenza (n=1), MRSA (n=1), VRE (n=1), and suprapubic abscess (n=1).
2.4.2 Comparison between groups
Table 2 shows the comparison of results between groups. Among clinical variables, serum Cr level at the time of renal scan was significantly higher in the Graft failure group, and type of kidney donation was also significantly different (p=0.0208) between groups. The extended chi-square test showed significantly different ratios of graft failure between donor types, and ABO-incompatible living donor showed a higher level of graft failure. The other clinical variables were not different between groups (Table 2).
Comparison between groups
| Non-failure group (n=34) | Graft failure group (n=11) | P-value | |
|---|---|---|---|
| Clinical variables | |||
| Age a | 45.4 ± 9.9 | 45.2 ±11.2 | 0.9489 b |
| Heighta | 163.0 ±7.3 | 168.0 ±6.1 | 0.0546b |
| Weighta | 63.9 ±14.7 | 66.8 ±10.3 | 0.5453b |
| Body mass index (BMI)a | 23.9 ±4.4 | 23.2 ±2.5 | 0.6251b |
| Diabetes mellitus (yes:no) | 9:25 | 6:5 | 0.0896c |
| Hypertension (yes:no) | 27:7 | 10:1 | 0.6568d |
| Serum creatinine (mg/dL) at the time of renal scintigraphye | 1.58 (0.55-5.886) | 3 (1.1-13.3) | 0.0208f |
| Systolic blood pressure (mmHg) at the time of renal scintigraphye | 135 (120-180) | 140 (120-160) | 0.2909f |
| Type of donated kidneyg (DDKT, ABOi-LDKT, LDKT) | 32, 0, 2 | 6, 3, 2 | 0.0022c |
| Right-sided transplantg | 33 | 10 | 0.4333d |
| Episode of acute kidney injury(AKI)h (yes:no) | 7:27 | 5:6 | 0.1089c |
| Regimen of immunosuppressant | 0.6568d | ||
| Cyclosporine, MMF, PDS | 7 | 1 | |
| Tacrolimus, MMF, PDS | 27 | 10 | |
| Renal scan variables | |||
| GFRe,i | 54.3 (14.2-178.4) | 34.2 (19.1-78.6) | 0.0394f |
| Hilson perfusion Indexe | 130.5 (24.7-594.1) | 141.4 (32.0-1002.5) | 0.6369f |
| ΔP e | 2.06 (1.09-4.48) | 1.74 (1.13-4.48) | 0.2259f |
| GW½ | 8.5 (3.5-93.81) | 16.75 (3.33-88.48) | 0.6446f |
-
a mean ± standard deviation
b T-test
c Chi-square test
d Fisher’s exact test
e median (range, minimum to maximum)
f Mann-Whitney test
g Number of cases
h Episode of AKI during 3 months after transplantation (AKI was defined as increase in serum Cr by ≥0.3 mg/dl within 48 hours or increase in serum Cr to 1.5 times from baseline which is known or presumed to have occurred within the prior 7 days or urine volume <0.5 ml/kg/h for 6 h [14]).
i In two cases of failure group, the renal uptake was too low. The program could not calculate GFR. Therefore, GFR of failure group was calculated with the scan of 9 patients.
Abbreviations: BMI, body mass index; DDKT, deceased donor kidney transplant; LDKT, living donor kidney transplant; ABOi-LDKT, ABO-incompatible LDKT; GFR, glomerular filtration rate; ΔP, time (s) between the peaks of the iliac and graft perfusion curves; GW½, time (s) for declining counts on the renal perfusion curve to reach half of the peak value (T½ of graft washout); MMF, Mycophenolate mofetil; PDS, prednisolone
Underlying renal disease was not significantly different between groups (chi-squared test, p=0.0601). Surgical complication was not significantly different between groups (chi-squared test, p=0.2192). Accompanying disease and infection were not significantly different between groups either.
Among renal scan variables, GFR was significantly different between groups, while there were no significant between-group differences in other renal scan variables. In two cases of failure group (rejection), the renal uptake was too low. The program could not calculate GFR. Therefore, GFR of failure group was calculated with the scan of 9 patients.
Table 3 shows that GFR of <44.48 mL/min at 1-week renal scintigraphy post operation could predict graft failure within 3 months (sensitivity 88.9%, specificity 64.7%; AUC 0.724; p=0.0067); among the clinical variables, serum Cr level of >2.13 mg/dL also predicted graft failure (sensitivity 72.7%, specificity 82.4%; AUC, 0.734; p=0.0158). Predictive value of both criteria together (serum Cr >2.13 mg/dL and GFR <44.48 mL/min) and of at least one criteria (serum Cr >2.13 mg/dL or GFR <44.48 mL/min) were analyzed, and AUC values were highest for “at least one criteria positive” (0.753), although there was no significant difference between scenarios.
ROC analysis to predict graft failure
| Variable | AUC | SE | 95% CI | p |
|---|---|---|---|---|
| Serum Cra | 0.734 | 0.0970 | 0.581 to 0.854 | 0.0158 |
| GFRb | 0.725 | 0.0832 | 0.568 to 0.850 | 0.0067 |
| Positive both criteriac | 0.730 | 0.0830 | 0.577 to 0.083 | 0.0056 |
| Positive at least one criteriad | 0.763 | 0.0621 | 0.613 to 0.877 | <0.0001 |
-
Foot note
a, Serum Cr at the time of renal scan >2.13 ng/dL
b, GFR on renal scan <44.48 mL/min (n=43)
In two cases, renal uptake was so low that GFR could not be calculated.
c, serum Cr >2.13 ng/dL AND GFR<44.48 mL/min
d, serum Cr >2.13 ng/dL or GFR<44.48 mL/min
Abbreviation: AUC, area under curve; SE, standard error; CI, confidence interval
3 Discussion
Our results indicate that renal scan performed within 5 to 8 days after kidney transplant could predict graft failure. GFR <44.48 mL/min on renal scan can predict graft failure. Also, when it was impossible to get automatically calculated GFR due to too-low renal uptake, both of those two cases were all in failure group in our study. We also found that serum Cr level of >2.13 mg/dL predicted graft failure. Transplant recipients who meet either or both of these criteria should be closely monitored. Our result is well-correlated with previous studies that mention the importance of GFR as a prognostic factor in renal transplantation[15], and our study confirms that GFR measured by renal scan at approximately 1 week after transplantation can predict the graft outcome.
As mentioned above, in a previous study comparing post transplant on day-3 and day-7 scans, postoperative day-3 scans could predict graft failure, while the day-7 scans could not [10]. That study defined graft failure by long term follow-up (average follow-up duration approximately 67.4 months), whereas the follow-up to graft failure in our study (approximately 3 months) was much shorter. In addition, the previous study used a MAG3 tracer, but it has been reported that DTPA is more sensitive than MAG3 for diagnosing dysfunction [16]. These differences of follow-up period and tracer might have caused the different results, and additional study with a larger number of patients and longer follow-up is needed.
Other variables from renal scintigraphy, including the Hilson perfusion index, ΔP, and GW½, did not predict graft failure in our study. Yazici et al. have reported that patients whose grafts were failing at 3 months after transplant had high GW½ or high ΔP on renal scans performed within 2 days after transplant [6]. Those authors determined graft function by serum Cr levels. GW½ and ΔP were also high in the failure group in our study, but the finding was not statistically significant. Gupta SK et al. have also reported that among several variables, only Hilson’s perfusion index proved to be useful for correlation with pathologic results [7]. However, the goal was correlation between renal scan and pathologic results. Therefore, in their study, most of the enrolled patients underwent biopsy, and the interval between renal scan and biopsy was short (within five days). In our study, the goal was to predict graft failure and not to compare the results of examinations which were done at almost the same time.
In analyzing renal function by scintigraphy, it is very important to draw the ROI in the right place [17]. A purely automated definition of the ROI cannot accurately identify the boundaries of the kidneys [18]. We used a combination of automatic and manual methods, and the same technician drew the ROIs, all of which were confirmed by a nuclear medicine physician.
Three of the patients who had ABO-incompatible living donor transplants had graft failure in this study. Due to the small number of cases, we did not analyze this type of transplant separately. Once again, further study with a larger number of cases and more information will be needed.
There are several limitations in this study. This is a retrospective study. In some cases, clinical information, such as the need for dialysis in the first week, was not available. Delayed graft function is typically defined in patients who need dialysis in the first week after transplant, and lacking those clinical data, we could not distinguish delayed graft function in our analysis. Renal scans were performed 5 to 8 days after transplantation, so patients with delayed graft function might have been included among the patients who were categorized as non-failure group in our analysis. However, in all of the patients in the non-failure group, the serum Cr level remained normal during the 1st year post operation which means our “non-failure group” was really “non-failure” and remained “non-failure” for a year. Acute tubular necrosis (ATN), also known as acute vasomotor nephropathy, is a common cause of delayed graft function [5, 17], but the presence of ATN was not analyzed in our study because of the timing (3 months post transplant) of the renal biopsy. Patients with other complications, including cyclosporin toxicity, were also categorized as non-failure group because of these limitations. The small study population is also a limitation.
4 Conclusion
DTPA renal scan performed at approximately 1 week after renal transplantation can predict graft outcome at 3 months. Lower GFR can be used to predict graft failure at 3 months.
Acknowledgement
This study was supported by the Chosun University research fund (2017).
-
Conflict of Interest: The authors declare that they have no conflicts of interest.
Reference
[1] Santos, J. and L.S. Martins, Estimating glomerular filtration rate in kidney transplantation: Still searching for the best marker. World Journal of Nephrology, 2015. 4(3): p. 345-35310.5527/wjn.v4.i3.345Search in Google Scholar PubMed PubMed Central
[2] Thölking, G., et al., Imaging-based diagnosis of acute renal allograft rejection. World Journal of Transplantation, 2016. 6(1): p. 174-18210.5500/wjt.v6.i1.174Search in Google Scholar PubMed PubMed Central
[3] Benjamens, S., et al., Can transplant renal scintigraphy predict the duration of delayed graft function? A dual center retrospective study. PloS One, 2018. 13(3): p. e019379110.1371/journal.pone.0193791Search in Google Scholar PubMed PubMed Central
[4] Barba, J.F., et al., [Study on the findings of an immediate renal gammagraphy and its effect on the survival of a kidney graft]. Actas Urologicas Espanolas, 2011. 35(4): p. 218-22410.1016/S2173-5786(11)70054-3Search in Google Scholar
[5] Yazici, B., et al., A New Quantitative Index for Baseline Renal Transplant Scintigraphy With 99mTc-DTPA in Evaluation of Delayed Graft Function and Prediction of 1-Year Graft Function. Clinical Nuclear Medicine, 2016. 41(3): p. 182-18810.1097/RLU.0000000000001020Search in Google Scholar PubMed
[6] Yazici, B., et al., Evaluation of Renal Transplant Scintigraphy and Resistance Index Performed Within 2 Days After Transplantation in Predicting Long-Term Graft Function. Clinical Nuclear Medicine, 2015. 40(7): p. 548-55210.1097/RLU.0000000000000789Search in Google Scholar PubMed
[7] Gupta, S.K., et al., Quantitative (99m)Tc DTPA renal transplant scintigraphic parameters: assessment of interobserver agreement and correlation with graft pathologies. American Journal of Nuclear Medicine and Molecular Imaging, 2014. 4(3): p. 213-224Search in Google Scholar
[8] Gupta, S.K., et al., Quantitative Tc-99m DTPA renal transplant scintigraphy predicts graft survival in the very early postoperative period. Nuclear Medicine Communications, 2012. 33(12): p. 1292-129910.1097/MNM.0b013e328359db96Search in Google Scholar PubMed
[9] Hilson, A.J., et al., Dynamic renal transplant imaging with Tc-99m DTPA (Sn) supplemented by a transplant perfusion index in the management of renal transplants. Journal of Nuclear Medicine: Official Publication, Society of Nuclear Medicine, 1978. 19(9): p. 994-1000Search in Google Scholar
[10] Park, U.-J., et al., Use of early postoperative MAG3 renal scan to predict long-term outcomes of renal transplants. Experimental and Clinical Transplantation: Official Journal of the Middle East Society for Organ Transplantation, 2013. 11(2): p. 118-12110.6002/ect.2012.0090Search in Google Scholar PubMed
[11] Gençoğlu, E.A., et al., Scintigraphic evaluation of paired renal allografts from the same cadaveric donor. Transplantation Proceedings, 2004. 36(1): p. 95-9810.1016/j.transproceed.2003.11.030Search in Google Scholar PubMed
[12] Ell, P.J. and S.S. Gambhir, Nuclear medicine in clinical diagnosis and treatment. 3rd ed ed. 2004: Edinburgh ; New York: Churchill Livingstone10.1097/01.mnm.0000134716.56011.bbSearch in Google Scholar
[13] Preston, D.F. and R.G. Luke, Radionuclide Evaluation of Renal Transplants. Journal of Nuclear Medicine, 1979. 20(10): p. 1095-1097Search in Google Scholar
[14] Nagarajan, M., et al., Impact of acute kidney injury on renal allograft survival. Ren Fail, 2017. 39(1): p. 40-4410.1080/0886022X.2016.1244076Search in Google Scholar PubMed PubMed Central
[15] First, M.R., Renal function as a predictor of long-term graft survival in renal transplant patients. Nephrology, Dialysis, Transplantation: Official Publication of the European Dialysis and Transplant Association - European Renal Association, 2003. 18 Suppl 1: p. i3-610.1093/ndt/gfg1027Search in Google Scholar PubMed
[16] Aktaş, A., et al., Comparison of Tc-99m DTPA and Tc-99m MAG3 perfusion time-activity curves in patients with renal allograft dysfunction. Transplantation Proceedings, 2006. 38(2): p. 449-45310.1016/j.transproceed.2006.01.006Search in Google Scholar PubMed
[17] Kampa, N., et al., Effect of region of interest selection and uptake measurement on glomerular filtration rate measured by 99mTc-DTPA scintigraphy in dogs. Veterinary Radiology & Ultrasound: The Official Journal of the American College of Veterinary Radiology and the International Veterinary Radiology Association, 2002. 43(4): p. 383-39110.1111/j.1740-8261.2002.tb01022.xSearch in Google Scholar PubMed
[18] Tian, C., et al., A semi-automated region of interest detection method in the scintigraphic glomerular filtration rate determination for patients with abnormal low renal function. Clinical Nuclear Medicine, 2013. 38(11): p. 855-86210.1097/RLU.0000000000000223Search in Google Scholar PubMed
© 2019 Ari Chong et al., published by De Gruyter
This work is licensed under the Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
Articles in the same Issue
- Research Article
- Prostate Cancer-Specific of DD3-driven oncolytic virus-harboring mK5 gene
- Case Report
- Pediatric acute paradoxical cerebral embolism with pulmonary embolism caused by extremely small patent foramen ovale
- Research Article
- Associations between ambient temperature and acute myocardial infarction
- Case Report
- Discontinuation of imatinib mesylate could improve renal impairment in chronic myeloid leukemia
- Research Article
- METTL3 promotes the proliferation and mobility of gastric cancer cells
- The C677T polymorphism of the methylenetetrahydrofolate reductase gene and susceptibility to late-onset Alzheimer’s disease
- microRNA-1236-3p regulates DDP resistance in lung cancer cells
- Review Article
- The link between thyroid autoimmunity, depression and bipolar disorder
- Research Article
- Effects of miR-107 on the Chemo-drug sensitivity of breast cancer cells
- Analysis of pH dose-dependent growth of sulfate-reducing bacteria
- Review Article
- Musculoskeletal clinical and imaging manifestations in inflammatory bowel diseases
- Research Article
- Regional hyperthermia combined with chemotherapy in advanced gastric cancer
- Analysis of hormone receptor status in primary and recurrent breast cancer via data mining pathology reports
- Morphological and isokinetic strength differences: bilateral and ipsilateral variation by different sport activity
- The reliability of adjusting stepped care based on FeNO monitoring for patients with chronic persistent asthma
- Comparison of the clinical outcomes of two physiological ischemic training methods in patients with coronary heart disease
- Analysis of ticagrelor’s cardio-protective effects on patients with ST-segment elevation acute coronary syndrome accompanied with diabetes
- Computed tomography findings in patients with Samter’s Triad: an observational study
- Case Report
- A spinal subdural hematoma induced by guidewire-based lumbar drainage in a patient with ruptured intracranial aneurysms
- Research Article
- High expression B3GAT3 is related with poor prognosis of liver cancer
- Effects of light touch on balance in patients with stroke
- Oncoprotein LAMTOR5 activates GLUT1 via upregulating NF-κB in liver cancer
- Effects of budesonide combined with noninvasive ventilation on PCT, sTREM-1, chest lung compliance, humoral immune function and quality of life in patients with AECOPD complicated with type II respiratory failure
- Prognostic significance of lymph node ratio in ovarian cancer
- Case Report
- Brainstem anaesthesia after retrobulbar block
- Review Article
- Treating infertility: current affairs of cross-border reproductive care
- Research Article
- Serum inflammatory cytokines comparison in gastric cancer therapy
- Behavioural and psychological symptoms in neurocognitive disorders: Specific patterns in dementia subtypes
- MRI and bone scintigraphy for breast cancer bone metastase: a meta-analysis
- Comparative study of back propagation artificial neural networks and logistic regression model in predicting poor prognosis after acute ischemic stroke
- Analysis of the factors affecting the prognosis of glioma patients
- Compare fuhrman nuclear and chromophobe tumor grade on chromophobe RCC
- Case Report
- Signet ring B cell lymphoma: A potential diagnostic pitfall
- Research Article
- Subparaneural injection in popliteal sciatic nerve blocks evaluated by MRI
- Loneliness in the context of quality of life of nursing home residents
- Biological characteristics of cervical precancerous cell proliferation
- Effects of Rehabilitation in Bankart Lesion in Non-athletes: A report of three cases
- Management of complications of first instance of hepatic trauma in a liver surgery unit: Portal vein ligation as a conservative therapeutic strategy
- Matrix metalloproteinase 2 knockdown suppresses the proliferation of HepG2 and Huh7 cells and enhances the cisplatin effect
- Comparison of laparoscopy and open radical nephrectomy of renal cell cancer
- Case Report
- A severe complication of myocardial dysfunction post radiofrequency ablation treatment of huge hepatic hemangioma: a case report and literature review
- Solar urticaria, a disease with many dark sides: is omalizumab the right therapeutic response? Reflections from a clinical case report
- Research Article
- Binge eating disorder and related features in bariatric surgery candidates
- Propofol versus 4-hydroxybutyric acid in pediatric cardiac catheterizations
- Nasointestinal tube in mechanical ventilation patients is more advantageous
- The change of endotracheal tube cuff pressure during laparoscopic surgery
- Correlation between iPTH levels on the first postoperative day after total thyroidectomy and permanent hypoparathyroidism: our experience
- Case Report
- Primary angiosarcoma of the kidney: case report and comprehensive literature review
- Research Article
- miR-107 enhances the sensitivity of breast cancer cells to paclitaxel
- Incidental findings in dental radiology are concerning for family doctors
- Suffering from cerebral small vessel disease with and without metabolic syndrome
- A meta-analysis of robot assisted laparoscopic radical prostatectomy versus laparoscopic radical prostatectomy
- Indications and outcomes of splenectomy for hematological disorders
- Expression of CENPE and its prognostic role in non-small cell lung cancer
- Barbed suture and gastrointestinal surgery. A retrospective analysis
- Using post transplant 1 week Tc-99m DTPA renal scan as another method for predicting renal graft failure
- The pseudogene PTTG3P promotes cell migration and invasion in esophageal squamous cell carcinoma
- Lymph node ratio versus TNM system as prognostic factor in colorectal cancer staging. A single Center experience
- Review Article
- Minimally invasive pilonidal sinus treatment: A narrative review
- Research Article
- Anatomical workspace study of Endonasal Endoscopic Transsphenoidal Approach
- Hounsfield Units on Lumbar Computed Tomography for Predicting Regional Bone Mineral Density
- Communication
- Aspirin, a potential GLUT1 inhibitor in a vascular endothelial cell line
- Research Article
- Osteopontin and fatty acid binding protein in ifosfamide-treated rats
- Familial polyposis coli: the management of desmoid tumor bleeding
- microRNA-27a-3p down-regulation inhibits malignant biological behaviors of ovarian cancer by targeting BTG1
- PYCR1 is associated with papillary renal cell carcinoma progression
- Prediction of recurrence-associated death from localized prostate cancer with a charlson comorbidity index–reinforced machine learning model
- Colorectal cancer in the elderly patient: the role of neo-adjuvant therapy
- Association between MTHFR genetic polymorphism and Parkinson’s disease susceptibility: a meta-analysis
- Metformin can alleviate the symptom of patient with diabetic nephropathy through reducing the serum level of Hcy and IL-33
- Case Report
- Severe craniofacial trauma after multiple pistol shots
- Research Article
- Echocardiography evaluation of left ventricular diastolic function in elderly women with metabolic syndrome
- Tailored surgery in inguinal hernia repair. The role of subarachnoid anesthesia: a retrospective study
- The factors affecting early death in newly diagnosed APL patients
- Review Article
- Oncological outcomes and quality of life after rectal cancer surgery
- Research Article
- MiR-638 repressed vascular smooth muscle cell glycolysis by targeting LDHA
- microRNA-16 via Twist1 inhibits EMT induced by PM2.5 exposure in human hepatocellular carcinoma
- Analyzing the semantic space of the Hippocratic Oath
- Fournier’s gangrene and intravenous drug abuse: an unusual case report and review of the literature
- Evaluation of surgical site infection in mini-invasive urological surgery
- Dihydromyricetin attenuates inflammation through TLR4/NF-kappaB pathway
- Clinico-pathological features of colon cancer patients undergoing emergency surgery: a comparison between elderly and non-elderly patients
- Case Report
- Appendix bleeding with painless bloody diarrhea: A case report and literature review
- Research Article
- Protective effects of specneuzhenide on renal injury in rats with diabetic nephropathy
- PBF, a proto-oncogene in esophageal carcinoma
- Use of rituximab in NHL malt type pregnant in I° trimester for two times
- Cancer- and non-cancer related chronic pain: from the physiopathological basics to management
- Case report
- Non-surgical removal of dens invaginatus in maxillary lateral incisor using CBCT: Two-year follow-up case report
- Research Article
- Risk factors and drug resistance of the MDR Acinetobacter baumannii in pneumonia patients in ICU
- Accuracy of tumor perfusion assessment in Rat C6 gliomas model with USPIO
- Lemann Index for Assessment of Crohn’s Disease: Correlation with the Quality of Life, Endoscopic Disease activity, Magnetic Resonance Index of Activity and C- Reactive Protein
- Case report
- Münchausen syndrome as an unusual cause of pseudo-resistant hypertension: a case report
- Research Article
- Renal artery embolization before radical nephrectomy for complex renal tumour: which are the true advantages?
- Prognostic significance of CD276 in non-small cell lung cancer
- Potential drug-drug interactions in acute ischemic stroke patients at the Neurological Intensive Care Unit
- Effect of vitamin D3 on lung damage induced by cigarette smoke in mice
- CircRNA-UCK2 increased TET1 inhibits proliferation and invasion of prostate cancer cells via sponge miRNA-767-5p
- Case report
- Partial hydatidiform mole and coexistent live fetus: a case report and review of the literature
- Research Article
- Effect of NGR1 on the atopic dermatitis model and its mechanisms
- Clinical features of infertile men carrying a chromosome 9 translocation
- Review Article
- Expression and role of microRNA-663b in childhood acute lymphocytic leukemia and its mechanism
- Case Report
- Mature cystic teratoma of the pancreas: A rare cystic neoplasm
- Research Article
- Application of exercised-based pre-rehabilitation in perioperative period of patients with gastric cancer
- Case Report
- Predictive factors of intestinal necrosis in acute mesenteric ischemia
- Research Article
- Application of exercised-based pre-rehabilitation in perioperative period of patients with gastric cancer
- Effects of dexmedetomidine on the RhoA /ROCK/ Nox4 signaling pathway in renal fibrosis of diabetic rats
- MicroRNA-181a-5p regulates inflammatory response of macrophages in sepsis
- Intraventricular pressure in non-communicating hydrocephalus patients before endoscopic third ventriculostomy
- CyclinD1 is a new target gene of tumor suppressor miR-520e in breast cancer
- CHL1 and NrCAM are primarily expressed in low grade pediatric neuroblastoma
- Epidemiological characteristics of postoperative sepsis
- Association between unstable angina and CXCL17: a new potential biomarker
- Cardiac strains as a tool for optimization of cardiac resynchronization therapy in non-responders: a pilot study
- Case Report
- Resuscitation following a bupivacaine injection for a cervical paravertebral block
- Research Article
- CGF treatment of leg ulcers: A randomized controlled trial
- Surgical versus sequential hybrid treatment of carotid body tumors
Articles in the same Issue
- Research Article
- Prostate Cancer-Specific of DD3-driven oncolytic virus-harboring mK5 gene
- Case Report
- Pediatric acute paradoxical cerebral embolism with pulmonary embolism caused by extremely small patent foramen ovale
- Research Article
- Associations between ambient temperature and acute myocardial infarction
- Case Report
- Discontinuation of imatinib mesylate could improve renal impairment in chronic myeloid leukemia
- Research Article
- METTL3 promotes the proliferation and mobility of gastric cancer cells
- The C677T polymorphism of the methylenetetrahydrofolate reductase gene and susceptibility to late-onset Alzheimer’s disease
- microRNA-1236-3p regulates DDP resistance in lung cancer cells
- Review Article
- The link between thyroid autoimmunity, depression and bipolar disorder
- Research Article
- Effects of miR-107 on the Chemo-drug sensitivity of breast cancer cells
- Analysis of pH dose-dependent growth of sulfate-reducing bacteria
- Review Article
- Musculoskeletal clinical and imaging manifestations in inflammatory bowel diseases
- Research Article
- Regional hyperthermia combined with chemotherapy in advanced gastric cancer
- Analysis of hormone receptor status in primary and recurrent breast cancer via data mining pathology reports
- Morphological and isokinetic strength differences: bilateral and ipsilateral variation by different sport activity
- The reliability of adjusting stepped care based on FeNO monitoring for patients with chronic persistent asthma
- Comparison of the clinical outcomes of two physiological ischemic training methods in patients with coronary heart disease
- Analysis of ticagrelor’s cardio-protective effects on patients with ST-segment elevation acute coronary syndrome accompanied with diabetes
- Computed tomography findings in patients with Samter’s Triad: an observational study
- Case Report
- A spinal subdural hematoma induced by guidewire-based lumbar drainage in a patient with ruptured intracranial aneurysms
- Research Article
- High expression B3GAT3 is related with poor prognosis of liver cancer
- Effects of light touch on balance in patients with stroke
- Oncoprotein LAMTOR5 activates GLUT1 via upregulating NF-κB in liver cancer
- Effects of budesonide combined with noninvasive ventilation on PCT, sTREM-1, chest lung compliance, humoral immune function and quality of life in patients with AECOPD complicated with type II respiratory failure
- Prognostic significance of lymph node ratio in ovarian cancer
- Case Report
- Brainstem anaesthesia after retrobulbar block
- Review Article
- Treating infertility: current affairs of cross-border reproductive care
- Research Article
- Serum inflammatory cytokines comparison in gastric cancer therapy
- Behavioural and psychological symptoms in neurocognitive disorders: Specific patterns in dementia subtypes
- MRI and bone scintigraphy for breast cancer bone metastase: a meta-analysis
- Comparative study of back propagation artificial neural networks and logistic regression model in predicting poor prognosis after acute ischemic stroke
- Analysis of the factors affecting the prognosis of glioma patients
- Compare fuhrman nuclear and chromophobe tumor grade on chromophobe RCC
- Case Report
- Signet ring B cell lymphoma: A potential diagnostic pitfall
- Research Article
- Subparaneural injection in popliteal sciatic nerve blocks evaluated by MRI
- Loneliness in the context of quality of life of nursing home residents
- Biological characteristics of cervical precancerous cell proliferation
- Effects of Rehabilitation in Bankart Lesion in Non-athletes: A report of three cases
- Management of complications of first instance of hepatic trauma in a liver surgery unit: Portal vein ligation as a conservative therapeutic strategy
- Matrix metalloproteinase 2 knockdown suppresses the proliferation of HepG2 and Huh7 cells and enhances the cisplatin effect
- Comparison of laparoscopy and open radical nephrectomy of renal cell cancer
- Case Report
- A severe complication of myocardial dysfunction post radiofrequency ablation treatment of huge hepatic hemangioma: a case report and literature review
- Solar urticaria, a disease with many dark sides: is omalizumab the right therapeutic response? Reflections from a clinical case report
- Research Article
- Binge eating disorder and related features in bariatric surgery candidates
- Propofol versus 4-hydroxybutyric acid in pediatric cardiac catheterizations
- Nasointestinal tube in mechanical ventilation patients is more advantageous
- The change of endotracheal tube cuff pressure during laparoscopic surgery
- Correlation between iPTH levels on the first postoperative day after total thyroidectomy and permanent hypoparathyroidism: our experience
- Case Report
- Primary angiosarcoma of the kidney: case report and comprehensive literature review
- Research Article
- miR-107 enhances the sensitivity of breast cancer cells to paclitaxel
- Incidental findings in dental radiology are concerning for family doctors
- Suffering from cerebral small vessel disease with and without metabolic syndrome
- A meta-analysis of robot assisted laparoscopic radical prostatectomy versus laparoscopic radical prostatectomy
- Indications and outcomes of splenectomy for hematological disorders
- Expression of CENPE and its prognostic role in non-small cell lung cancer
- Barbed suture and gastrointestinal surgery. A retrospective analysis
- Using post transplant 1 week Tc-99m DTPA renal scan as another method for predicting renal graft failure
- The pseudogene PTTG3P promotes cell migration and invasion in esophageal squamous cell carcinoma
- Lymph node ratio versus TNM system as prognostic factor in colorectal cancer staging. A single Center experience
- Review Article
- Minimally invasive pilonidal sinus treatment: A narrative review
- Research Article
- Anatomical workspace study of Endonasal Endoscopic Transsphenoidal Approach
- Hounsfield Units on Lumbar Computed Tomography for Predicting Regional Bone Mineral Density
- Communication
- Aspirin, a potential GLUT1 inhibitor in a vascular endothelial cell line
- Research Article
- Osteopontin and fatty acid binding protein in ifosfamide-treated rats
- Familial polyposis coli: the management of desmoid tumor bleeding
- microRNA-27a-3p down-regulation inhibits malignant biological behaviors of ovarian cancer by targeting BTG1
- PYCR1 is associated with papillary renal cell carcinoma progression
- Prediction of recurrence-associated death from localized prostate cancer with a charlson comorbidity index–reinforced machine learning model
- Colorectal cancer in the elderly patient: the role of neo-adjuvant therapy
- Association between MTHFR genetic polymorphism and Parkinson’s disease susceptibility: a meta-analysis
- Metformin can alleviate the symptom of patient with diabetic nephropathy through reducing the serum level of Hcy and IL-33
- Case Report
- Severe craniofacial trauma after multiple pistol shots
- Research Article
- Echocardiography evaluation of left ventricular diastolic function in elderly women with metabolic syndrome
- Tailored surgery in inguinal hernia repair. The role of subarachnoid anesthesia: a retrospective study
- The factors affecting early death in newly diagnosed APL patients
- Review Article
- Oncological outcomes and quality of life after rectal cancer surgery
- Research Article
- MiR-638 repressed vascular smooth muscle cell glycolysis by targeting LDHA
- microRNA-16 via Twist1 inhibits EMT induced by PM2.5 exposure in human hepatocellular carcinoma
- Analyzing the semantic space of the Hippocratic Oath
- Fournier’s gangrene and intravenous drug abuse: an unusual case report and review of the literature
- Evaluation of surgical site infection in mini-invasive urological surgery
- Dihydromyricetin attenuates inflammation through TLR4/NF-kappaB pathway
- Clinico-pathological features of colon cancer patients undergoing emergency surgery: a comparison between elderly and non-elderly patients
- Case Report
- Appendix bleeding with painless bloody diarrhea: A case report and literature review
- Research Article
- Protective effects of specneuzhenide on renal injury in rats with diabetic nephropathy
- PBF, a proto-oncogene in esophageal carcinoma
- Use of rituximab in NHL malt type pregnant in I° trimester for two times
- Cancer- and non-cancer related chronic pain: from the physiopathological basics to management
- Case report
- Non-surgical removal of dens invaginatus in maxillary lateral incisor using CBCT: Two-year follow-up case report
- Research Article
- Risk factors and drug resistance of the MDR Acinetobacter baumannii in pneumonia patients in ICU
- Accuracy of tumor perfusion assessment in Rat C6 gliomas model with USPIO
- Lemann Index for Assessment of Crohn’s Disease: Correlation with the Quality of Life, Endoscopic Disease activity, Magnetic Resonance Index of Activity and C- Reactive Protein
- Case report
- Münchausen syndrome as an unusual cause of pseudo-resistant hypertension: a case report
- Research Article
- Renal artery embolization before radical nephrectomy for complex renal tumour: which are the true advantages?
- Prognostic significance of CD276 in non-small cell lung cancer
- Potential drug-drug interactions in acute ischemic stroke patients at the Neurological Intensive Care Unit
- Effect of vitamin D3 on lung damage induced by cigarette smoke in mice
- CircRNA-UCK2 increased TET1 inhibits proliferation and invasion of prostate cancer cells via sponge miRNA-767-5p
- Case report
- Partial hydatidiform mole and coexistent live fetus: a case report and review of the literature
- Research Article
- Effect of NGR1 on the atopic dermatitis model and its mechanisms
- Clinical features of infertile men carrying a chromosome 9 translocation
- Review Article
- Expression and role of microRNA-663b in childhood acute lymphocytic leukemia and its mechanism
- Case Report
- Mature cystic teratoma of the pancreas: A rare cystic neoplasm
- Research Article
- Application of exercised-based pre-rehabilitation in perioperative period of patients with gastric cancer
- Case Report
- Predictive factors of intestinal necrosis in acute mesenteric ischemia
- Research Article
- Application of exercised-based pre-rehabilitation in perioperative period of patients with gastric cancer
- Effects of dexmedetomidine on the RhoA /ROCK/ Nox4 signaling pathway in renal fibrosis of diabetic rats
- MicroRNA-181a-5p regulates inflammatory response of macrophages in sepsis
- Intraventricular pressure in non-communicating hydrocephalus patients before endoscopic third ventriculostomy
- CyclinD1 is a new target gene of tumor suppressor miR-520e in breast cancer
- CHL1 and NrCAM are primarily expressed in low grade pediatric neuroblastoma
- Epidemiological characteristics of postoperative sepsis
- Association between unstable angina and CXCL17: a new potential biomarker
- Cardiac strains as a tool for optimization of cardiac resynchronization therapy in non-responders: a pilot study
- Case Report
- Resuscitation following a bupivacaine injection for a cervical paravertebral block
- Research Article
- CGF treatment of leg ulcers: A randomized controlled trial
- Surgical versus sequential hybrid treatment of carotid body tumors