Onset of Kawasaki disease immediately after birth
-
Cristina Medeiros Ribeiro de Magalhães



Abstract
Kawasaki disease (KD) is one of the most common causes of childhood systemic vasculitis, with the potential to cause significant cardiovascular complications, especially if undiagnosed. An investigation of coronary artery abnormalities with the application of appropriate therapeutic measures can improve the prognosis in these infants, decreasing the risk of coronary artery aneurysms. Neonatal KD is a rare event, often characterized only by few of the clinical features observed in older children. In this case report, we describe a newborn male who presented an incomplete clinical presentation of KD, where symptoms of the disease erupted immediately after birth. The objective of this report is to draw the attention of pediatricians and neonatologists to the possible presence of KD in an asymptomatic newborn during the immediate postnatal period, even in the absence of the classic features of KD, such as fever.
Introduction
Kawasaki disease (KD) is one of the most common causes of childhood systemic vasculitis, with potentially significant cardiovascular implications, especially if undiagnosed. Coronary artery aneurysms occur in up to 25% of untreated KD patients. However, treatment with high-dose intravenous immunoglobulin (IVIG) within the first 10 days of the onset of fever reduces the risk of coronary artery aneurysms [1]. Diagnostic confirmation based purely on clinical features is frequently difficult, especially in the neonatal period when the clinical presentation is often atypical [2]. KD has global distribution and affects all pediatric age groups with approximately 85% of cases occurring in children under 5 years of age [1]. KD is rare in the neonatal period [3], and less frequent in patients less than 6 months or more than 8 years of age. However, neonates are at a higher risk of coronary artery abnormalities, possibly due to delayed diagnosis and treatment [4]. We describe a case of neonatal KD in which the first symptoms of acute respiratory distress and severe tachycardia appeared shortly after birth.
Case
A boy, small for the gestational ag, (weight: 2550 g; length: 47 cm) was delivered with an Apgar score of 8/9. Two hours after birth, the child became acutely ill, developing progressive respiratory distress and tachycardia, and was admitted to the neonatal intensive care unit. He was afebrile and was found to have a normal blood count and normal blood sugar level. The 27-year-old mother had undergone prenatal follow-ups and was considered healthy aside from moderate hypertension (treated with methyldopa and furosemide). Prenatal testing for cytomegalovirus, rubella, toxoplasmosis, HIV and syphilis was negative. Pre-eclampsia complicated the last weeks of gestation and, following signs of acute fetal distress, a cesarean section was performed in the 39th gestational week.
On the 5th day a systolic murmur was detected, and an echocardiogram was performed, which revealed dilatation of both coronary arteries, as shown in Figure 1A (left CA 2.8 mm or 0.28 cm – Z score 5.07) and Figure 1B (right CA: 2.9 mm or 0.29 cm – Z score 6.09). The diagnosis of KD was considered. However, there were no other symptoms and the patient remained afebrile, therefore, the existence of a congenital coronary artery fistula [5] was considered as a possible diagnosis. It was only on the 6th day that other classic signs of KD progressively started to appear, such as a polymorphous rash (Figure 2), conjunctival injection, edema and erythema of the lips and strawberry tongue.
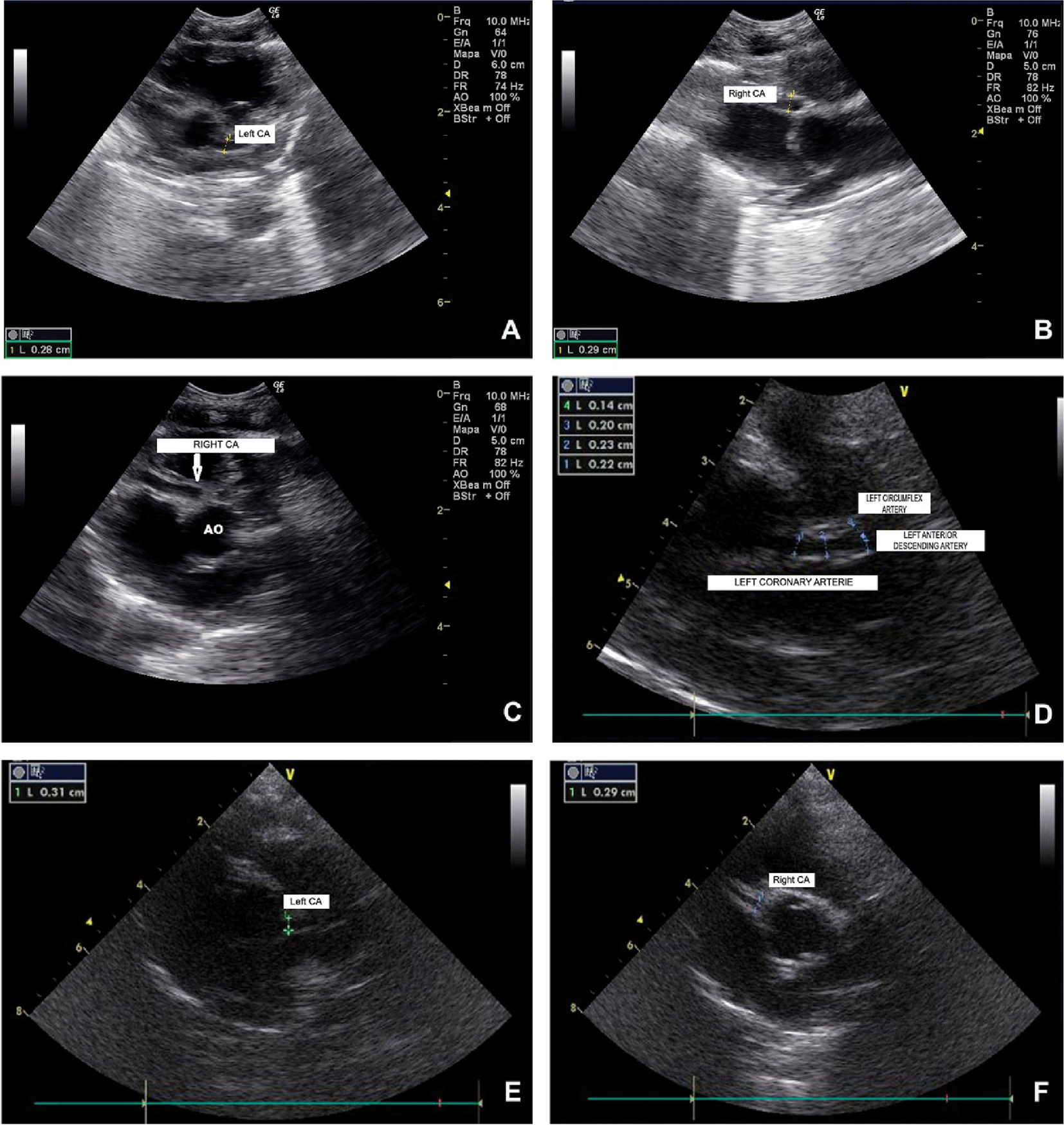
Consecutive echocardiograms of the newborn, performed on the 5th (1A and 1B) and the 10th day postpartum (1C), and subsequently on the 7th (1D) and the 10th month of life (1E and 1F), showing the appearance of bilateral coronary artery aneurysms and their eventual final normalization.

Polymorphic rash, characteristic of Kawasaki’s disease, appeared after the 5th day.
Laboratory investigations included hemoglobin (15.9 g/dL), white blood cells count (8.8 × 103/L, neutrophils 55%, lymphocytes 30%, eosinophils 9%, monocytes 6%), platelets (362 × 103/L), sodium (139 mEq/L), potassium (4.2 mEq/L), creatinine (0.50 mg/dL), glutamic oxaloacetic transaminase (51 U/L – normal values for newborn: 25–75 U/L), glutamic pyruvate transaminase (12 U/L – normal values for newborn: 13–105 U/L), and increased levels of C-reactive protein (9 mg/dL- normal values: 0–1 mg/dL), and of creatine kinase MB (66 U/L; normal value: 7–30). A new echocardiogram on the infant’s 10th day showed an aneurysm in both carotid arteries, with thickening of the intima, and wall abnormalities of both vessels that displayed diameters of 0.38 cm each, with corresponding Z score: right CA 8.94 (Figure 1C) and left CA 8.26 (image not shown). The diagnosis of KD was confirmed on the 10th day when an echocardiogram confirmed the evolution of the coronary artery aneurysm along with four of KD’s main clinical symptoms.
A single infusion of 2 mg/kg of IVIG was administered, in association with 1 mg/kg/day of prednisolone p.o. and 5 mg/kg/day of aspirin. The inflammatory phase progressively subsided, along with the emergence of periungual desquamation of fingers and toes. In the subacute phase, once inflammation subsided, the newborn presented significant thrombocytosis, reaching a total count of 823,000 platelets on the 15th day, during the convalescent stage of the disease. Table 1 shows the evolution of the patient’s main laboratory indices.
Evolution of the patient’s main laboratorial indices.
| Day of age | CRP | ESR | Hemoglobin | WBC count | Platelets count |
|---|---|---|---|---|---|
| 6 | 9 mg/dL | 12 mm | 15.9 g/dL | 8.8 × 103/L | 362 × 103/mm3 |
| 10 | 13 mg/dL | 22 mm | 11.8 g/dL | 13 × 103/L | 556 × 103/mm3 |
| 15 | 4.5 mg/dL | 10 mm | 13 g/dL | 10.1 × 103/L | 823 × 103/mm3 |
| 20 | 0.5 mg/dL | 2 mm | 14.3 g/dL | 9.2 × 103/L | 521 × 103/mm3 |
-
CRP = C-reactive protein; ESR m = erythrocyte sedimentation rate (Westergreen method); WBC = white blood cell.
A repeated echocardiogram, at 1 month, disclosed unchanged CA parameters. A new echocardiogram performed at 7 months showed decreasing diameters of the coronary arteries [right CA: 0.31 cm – Z score 5.04 (image not shown); left CA: 0.21 cm – Z score 3.83], and the appearance of a small aneurysm on the left anterior descending coronary artery (Figure 1D). On this same occasion, auditory evoked potentials and Doppler ultrasonography of the abdominal arteries were reported normal. A control echocardiogram was performed at 10 months and displayed left CA with a diameter of 0.31 cm (Z score 4.2) (Figure 1E), and right CA with 0.29 cm (Z score 4.15) (Figure 1F). A follow-up exam and echocardiogram were performed at 14 months, which revealed normalization of the coronary arteries. Furthermore, the child was in good clinical condition, with normal height and weight for age, and normal cognitive and motor development.
Discussion
Neonatal KD is a sporadic event, often characterized by only a few of the clinical features observed in older children [6]. In our case, the diagnosis of KD was not initially considered, mainly due to the absence of fever. KD diagnosis was only suspected on the 5th day when dilatation of both coronary arteries was detected on the echocardiogram and was confirmed retrospectively with the onset of polymorphous exanthema, conjunctival injection, edema and erythema of the lips, and strawberry tongue. Almost all described cases of neonatal KD showed an incomplete form of the disease and lack of fever had been previously described in a neonate with a presumed diagnosis of KD, presenting with dilatation of both coronaries within the first 24 h of life [6]. In a newborn, echocardiographic findings of coronary artery dilatation raise the possibility of the existence of a coronary artery fistula, which may appear as a continuous murmur in an otherwise asymptomatic child [7]. However, in the present case, the coronary artery dilatation was bilateral, which is very uncommon in cases of coronary artery fistulas. Additionally, a mild degree of intimal thickening could be observed, suggesting an ongoing inflammatory process.
During the 1st days post-delivery, KD is a rare event and few cases have been reported. Krapf et al. [8] described a neonatal case of mucocutaneous lymph node syndrome during the first 72 h of life, which disclosed CA abnormalities followed by a fatal myocardial infarction. Two previous cases [9], [10] were characterized by abnormal symptomatology appearing during the 1st day post-delivery, with echocardiography confirming dilatation of coronary arteries. Interestingly, persistent high fever, one of the main symptoms of KD, was not observed in any of the previously described cases. In all these cases, KD presentation was incomplete, and the final diagnosis was mainly based on the presence of coronary artery abnormalities.
The timing of the symptomatology appearance suggests a possible antenatal acquired disorder. However, there was no membrane rupture before the cesarean section eliminating the chance of a previous infection. Although KD has been associated with some form of unknown environmental factors, presumptively of immunological or infectious origin, the eventual occurrence of vertical transmission of any specific etiologic agent has not yet been determined. However, Kanno et al. [11] weakens the hypothesis of vertical transmission. In their report, a 32-year-old contracted KD on the 17th-week of gestation and gave birth to a healthy term infant that remained healthy.
The reason for the appearance of KD immediately after birth remains unclear. However, the importance of this case and the previously reported neonate cases is to call the attention of neonatologists and pediatricians to the fact that KD can appear in the immediate postpartum period, frequently in an atypical or incomplete form. Faulty diagnosis, delayed intervention and inappropriate treatment can severely hinder the future development of the child.
-
Competing interests: The authors declare there is no conflict of interest.
-
Ethics approval and consent to participate: The patient included in the study was approved by CEP-FEPECS/SES-DF n°1.037.234
-
Permissions: Permission for publication and use of echocardiogram images was obtained from the patient’s legal guardians.
-
Financial Support: The authors declare no financial support.
-
Authors’ Contributors: C.M.R. Magalhães attended the patient and followed the clinical case, R. Pratesi conceived the study and drafted the manuscript, L. Gandolfi and R. Uenishi participated in the study analysis. C.B. Pratesi reviewed the article, cataloged the data, analyzed and supervised the study design and E.M. Garcia performed all echocardiograms in the patient and helped with data analysis. All authors read and approved the final manuscript.
References
[1] Newburger JW. Diagnosis, treatment, and long-term management of Kawasaki disease: a statement for health professionals from the Committee on Rheumatic Fever, Endocarditis and Kawasaki Disease, Council on Cardiovascular Disease in the Young, American Heart Association. Circulation. 2004;110:2747–71.10.1161/01.CIR.0000145143.19711.78Suche in Google Scholar PubMed
[2] McCrindle BW, Rowley AH, Newburger JW, Burns JC, Bolger AF, Gewitz M, et al. Diagnosis, treatment, and long-term management of Kawasaki disease: a scientific statement for health professionals from the American Heart Association. Circulation. 2017;135:e927–99.10.1161/CIR.0000000000000484Suche in Google Scholar PubMed
[3] Stanley TV, Grimwood K. Classical Kawasaki disease in a neonate. Arch Dis Child-Fetal Neonatal Ed. 2002;86:F135–6.10.1136/fn.86.2.F135Suche in Google Scholar PubMed PubMed Central
[4] Manlhiot C, Yeung RSM, Clarizia NA, Chahal N, McCrindle BW. Kawasaki disease at the extremes of the age spectrum. Am Acad Pediatr [Internet]. 2009;124. Available from: http://pediatrics.aappublications.org/content/124/3/e410?sso=1&sso_redirect_count=1&nfstatus=401&nftoken=00000000-0000-0000-0000-000000000000&nfstatusdescription=ERROR%3a+No+local+token.10.1542/peds.2009-0099Suche in Google Scholar PubMed
[5] Song G, Zhang J, Ren W, Li Y, Zhou K. Pediatric coronary artery fistula: echocardiographic case reports and literature review of treatment strategy. SpringerPlus [Internet]. 2016 [cited 2017 Dec 8];5. Available from: http://springerplus.springeropen.com/articles/10.1186/s40064-016-3276-0.10.1186/s40064-016-3276-0Suche in Google Scholar PubMed PubMed Central
[6] Hangai M, Kubota Y, Kagawa J, Yashiro M, Uehara R, Nakamura Y, et al. Neonatal Kawasaki disease: case report and data from nationwide survey in Japan. Eur J Pediatr. 2014;173:1533–6.10.1007/s00431-014-2347-xSuche in Google Scholar PubMed
[7] Ismail AQT, Gandhi A, Desai T, Stumper O. A neonatal case of congenital coronary artery fistula. Case Rep. 2012;2012(feb07 1):bcr0920114773-bcr0920114773.10.1136/bcr.09.2011.4773Suche in Google Scholar PubMed PubMed Central
[8] Krapf R, Zimmermann A, Stocker F. Lethal vasculitis of coronary arteries in a neonate and two infants: possible neonatal variant of the MLNS/IPN complex? Helv Paediatr Acta. 1981;36:589–98.Suche in Google Scholar
[9] Bolz D, Arbenz U, Fanconi S, Bauersfeld U. Myocarditis and coronary dilatation in the 1st week of life: neonatal incomplete Kawasaki disease? Eur J Pediatr. 1998;157:589–91.10.1007/s004310050885Suche in Google Scholar PubMed
[10] Parashar R, Lysecki PJ, Mondal T. Diffuse coronary artery dilatation in a neonate: A case report. J Neonatal-Perinat Med. 2013;6:263–6.10.3233/NPM-1365612Suche in Google Scholar PubMed
[11] Kanno K, Sakai H, Nakajima M, Satake A, Konishi T, Iizuka H. An adult case of Kawasaki disease in a rregnant Japanese woman: a case report. Case Rep Dermatol. 2011;3:98–102.10.1159/000327937Suche in Google Scholar PubMed PubMed Central
©2018 Walter de Gruyter GmbH, Berlin/Boston
Artikel in diesem Heft
- Case Reports – Obstetrics
- Trisomy 9 presenting in the first trimester as a fetal lateral neck cyst and increased nuchal translucency
- A case of intrauterine closure of the ductus arteriosus and non-immune hydrops
- Pregnancy luteoma: a rare presentation and expectant management
- A pregnant woman with an operated bladder extrophy and a pregnancy complicated by placenta previa and preterm labor
- Consecutive successful pregnancies of a patient with nail-patella syndrome
- A multidisciplinary management approach for patients with Klippel-Trenaunay syndrome and multifetal gestation with successful outcomes
- A uterus didelphys with a spontaneous labor at term of pregnancy: a rare case and a review of the literature
- Case Reports – Fetus
- Prenatal diagnosis of ring chromosome 13: a rare chromosomal aberration
- Case Reports – Newborn
- Late-onset pubic-phallic idiopathic edema in premature recovering infants
- An unusual cause of neonatal shock: a case report
- Early ultrasonographic follow up in neonatal pneumatocele. Two case reports
- Nonsyndromic extremely premature eruption of teeth in preterm neonates – a report of three cases and a review of the literature
- Successful outcome of a preterm infant with severe oligohydramnios and suspected pulmonary hypoplasia following premature rupture of membranes (PPROM) at 18 weeks’ gestation
- Onset of Kawasaki disease immediately after birth
- Short rib-polydactyly syndrome (Saldino-Noonan type) undetected by standard prenatal genetic testing
- Severe congenital autoimmune neutropenia in preterm monozygotic twins: case series and literature review
- Verona integron-encoded metallo-β-lactamase-producing Klebsiella pneumoniae sepsis in an extremely premature infant
Artikel in diesem Heft
- Case Reports – Obstetrics
- Trisomy 9 presenting in the first trimester as a fetal lateral neck cyst and increased nuchal translucency
- A case of intrauterine closure of the ductus arteriosus and non-immune hydrops
- Pregnancy luteoma: a rare presentation and expectant management
- A pregnant woman with an operated bladder extrophy and a pregnancy complicated by placenta previa and preterm labor
- Consecutive successful pregnancies of a patient with nail-patella syndrome
- A multidisciplinary management approach for patients with Klippel-Trenaunay syndrome and multifetal gestation with successful outcomes
- A uterus didelphys with a spontaneous labor at term of pregnancy: a rare case and a review of the literature
- Case Reports – Fetus
- Prenatal diagnosis of ring chromosome 13: a rare chromosomal aberration
- Case Reports – Newborn
- Late-onset pubic-phallic idiopathic edema in premature recovering infants
- An unusual cause of neonatal shock: a case report
- Early ultrasonographic follow up in neonatal pneumatocele. Two case reports
- Nonsyndromic extremely premature eruption of teeth in preterm neonates – a report of three cases and a review of the literature
- Successful outcome of a preterm infant with severe oligohydramnios and suspected pulmonary hypoplasia following premature rupture of membranes (PPROM) at 18 weeks’ gestation
- Onset of Kawasaki disease immediately after birth
- Short rib-polydactyly syndrome (Saldino-Noonan type) undetected by standard prenatal genetic testing
- Severe congenital autoimmune neutropenia in preterm monozygotic twins: case series and literature review
- Verona integron-encoded metallo-β-lactamase-producing Klebsiella pneumoniae sepsis in an extremely premature infant