Integrative medicine approaches to chronic depression: case studies of the recovery process with a three-step path to recovery and significant cure
-
Ronko Itamura


Abstract
Objectives
The support provided by conventional treatments centered on the administration of medication for chronic or other types of depression is limited. Integrative medicine, which is based on both modern Western medicine and a range of complementary and alternative medicine practices, is patient-centered and promotes natural healing in patients to achieve significant cure. This report focuses on the indications of recovery from depression using integrative medicine, especially homeopathy.
Methods
Thirty-one patients (9 males and 22 females) with depression underwent homeopathic treatment using various strategies over 3 months, in addition to antidepressants. All patients were diagnosed with Major Depressive Disorders, except bipolar disorders. Three steps were used to model indications of their recovery from depression: reducing difficulties in everyday life, reducing and stopping antidepressants, and reducing and stopping the homeopathic remedies. Patients were considered to have recovered when antidepressants had been stopped for 6 months or more and 3 or more months had passed since homeopathic medicines were stopped.
Results
Of the 31 patients with depression, 13 recovered within 2 years of starting homeopathic treatment, and 11 completely recovered from chronic depression.
Conclusions
This study suggests that integrative medicine can be a useful strategy for depression, including the use of a three-step strategy for reducing all dependence on clinical treatment. As most patients, especially chronic patients, significantly recovered from depression through homeopathy over 2 years, this model can help understand recovery from depression through integrative medicine.
Introduction
Depression is predicted to be the leading contributor to the global disease burden by 2030 [1]. In Japan, about 20,000 people die by suicide each year, and many are considered to have depression [2]. Whether chronic, long-term, or severe depression, the support provided by conventional treatments centered on drug administration is limited [3].
In previous clinical trials of antidepressants, remission rates were reported to be low (≤50%) for any given drug among the patient groups evaluated [4, 5]. Despite the success of pharmacologic treatment of depression in terms of remission, an unmet need for full symptomatic and functional recovery remains. Among the patients seeking this degree of recovery, some turn to complementary and alternative medicine (CAM) after undergoing prolonged antidepressant treatment because they continue to experience difficulties in daily life [6], [7], [8].
Integrative medicine goes beyond the framework of conventional medicine based on modern Western medicine to include various CAMs. Recently, integrative psychiatry has been selectively incorporating elements of CAM into practice [9]. This practice of psychiatry views patients holistically, considering not only mind–body issues and interactions but also spiritual values. In integrative psychiatry, homeopathic medicine can be used with conventional medicines. Homeopathy is a CAM and a patient-centered medicine considered to stimulate the patient’s own healing process; thus, the homeopathic process treats the “individual patient as a whole” [10, 11].
This study reports the progress of 31 patients with depression who received homeopathy over 3 months in addition to antidepressants, and presents one specific case of recovery from depression through homeopathy using a three-step path to recovery and significant cure.
Subjects and methods
This retrospective case study focused on patients with chronic depression treated with a combination of modern Western medicine and CAM in May 2005–December 2011. When homeopathy is used for depression in patients who initially received conventional treatment, it is important to assess the progress of these patients after receiving homeopathy. The three-step path to recovery from depression through homeopathy is shown in Figure 1 and summarized as follows: (1) Step I is to reduce difficulties in daily life, with the goal to improve the quality of life (QOL) without changing the conventional medicines; (2) Step II is to reduce or stop conventional medicines; and (3) Step III is to reduce or stop homeopathic medicines and ultimately to have no need for homeopathic medicine.
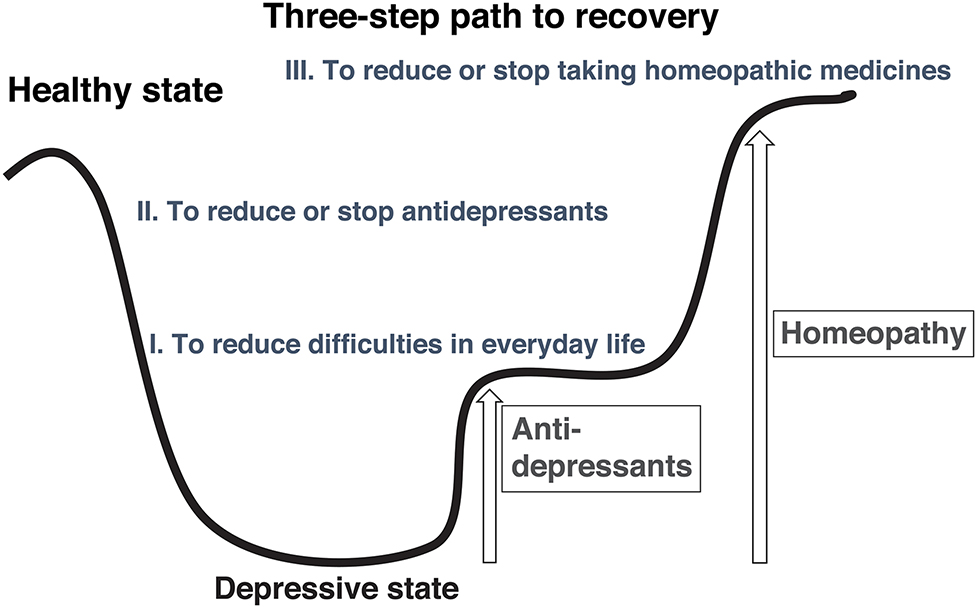
Step I is to reduce difficulties in daily life, which is defined as improvement of quality of life. Step II is to reduce or stop conventional medicines. Step III is to reduce or stop homeopathic medicines and ultimately to have no need for homeopathic medicine.
According to the patient’s disease pathology and degree of disease fluctuation, the homeopathic strategies used included a holistic approach based on totality, or the method of complexity, especially for patients with chronic or intractable disease who had deep and hidden personal conflicts at subconscious levels. In the pathologic approach, homeopathic repertorization was used. According to the Criteria for Major Depressive Episodes by the Diagnostic and Statistical Manual of Mental Disorders, fourth edition, text revision (DSM-IV-TR) [12], some computer-analyzed homeopathic medicine rubrics are available, such as MacRepertory (Synergy Homeopathic; https://www.synergyhomeopathic.com). Disease severity was determined using the Zung Self-Rating Depression Scale (SDS) [13] at the patient’s first consultation for integrative medicine. The SDS score was from 37 to 75 points, and the mean score was 52.5 (>50 is classified as severe). Cases considered recovered were those for which antidepressants had been stopped ≥6 months and homeopathic medicines had been stopped ≥3 months.
Ethical approval: The research related to human use is in accordance with the tenets of the Helsinki Declaration. Ethical approval was not necessary due to the retrospective nature of the study.
Informed consent was obtained from all individuals included in this study.
Results
This retrospective study analyzed 31 patients with depression (22 women, 9 men; age 20–59 years, mean age 41.5 years). The average duration of depression was 4 years and 2 months, ranging from 3 months to 15 years. All patients had a DSM-IV-TR diagnosis of a major depressive disorder, except bipolar disorders. All patients had already received antidepressant medication for 6 months to 15 years.
Patients had their first consultation for integrative medicine between May 2005 and December 2009. Chronic depression met the full criteria for a major depressive episode, and patients with chronic depression had continuously met these criteria for at least the past 2 years. Of the 31 patients assessed, 87% (27) had chronic depression.
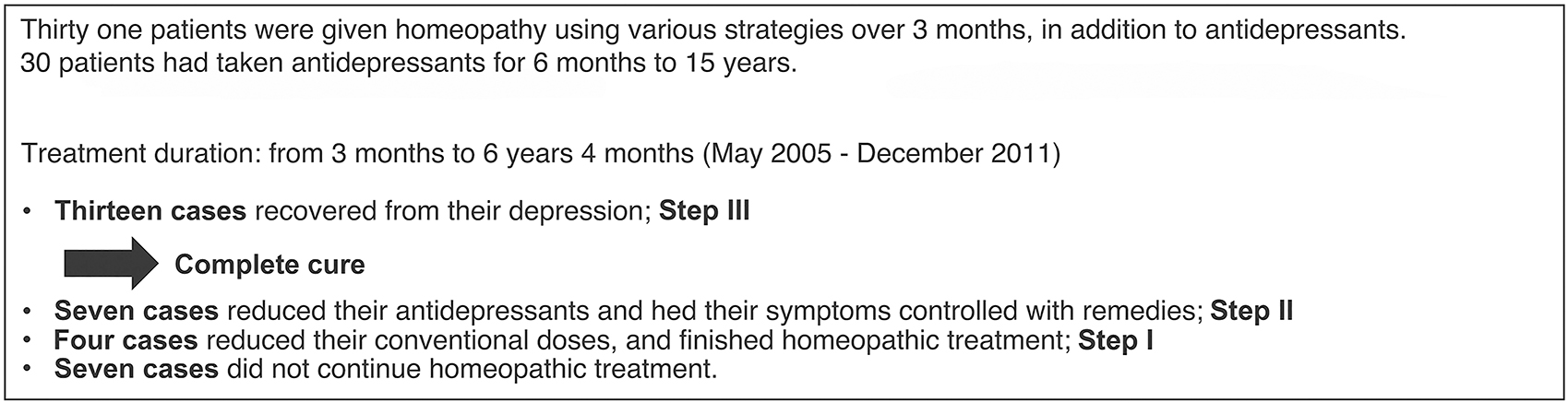
All 31 patients were given homeopathy using various strategies over 3 months, in addition to antidepressants. Treatment duration was from 3 months to 6 years and 4 months (May 2005–December 2011), as shown in Figure 2.
Results of 31 patients treated with homeopathy using various strategies over 3 months, in addition to antidepressants.
Of the 31 patients, 13 patients recovered from depression, defined as proceeding from Step III to a complete cure;7 patients reduced the dose or the number or frequency of antidepressants and experienced symptom control with homeopathic medicines, thus reaching Step II; 4 patients reduced their conventional drug doses and finished homeopathic treatment, defined as the incompletion of Step I; and 7 patients did not continue homeopathic treatment. Details for the specific patients cased are shown in the following tables: Table 1 presents 31 cases with their first consultation between July 2005 and December 2009. These data indicate whether a patient had a strong tendency toward suicide or had attempted suicide, include a list of the patient’s conventional medicines, and the results of a psychological test, the Cornell Medical Index [14].
Data of 31 patients with depression who had integrative medicine consultation in July 2005–December 2009.
| Case no. | Age | Sex (F/M) | Suicide idea/attempt | Duration of illness | Conventional medicines | SDS first visit | CMI first visit | Remedies | Progress Step I–III to recovery |
|---|---|---|---|---|---|---|---|---|---|
| 1. S.N | 36 | F | Idea ++ | 8 years | Fluvoxamine maleate (75 mg), mianserin hydrochloride (30 mg), bromazepam (15 mg), triazolam (0.25 mg), clotiazepam (15 mg) | 58 | IV | Thuja | 2 years later, reduce conventional medicines and finished treatment. Step I |
| Calcarea carbonica | |||||||||
| 2. H.T | 44 | F | Idea ++ | 2 years | Milnacipran hydrochloride (75 mg), lorazepam (3 mg) | 52 | IV | Aurum metallicum | 12 months later, did not continue treatment |
| Sepia | |||||||||
| Magnesia carbonica | |||||||||
| 3. A.I | 33 | F | Idea + | 2 years | Paroxetine hydrochloride (40 mg), mianserin hydrochloride (30 mg), ethyl loflazepate (3 mg), zolpidemtartrate (10 mg), rilmazefone hydrochloride (1 mg) | 54 | III | Silica | Gradually reduce conventional medicines. Continue homeopathic medicines. Step II |
| Ignatia amara | |||||||||
| Phosphoricum acidum | |||||||||
| Carcinosinum | |||||||||
| 4. C.H | 47 | F | No | 5 years | Milnacipran hydrochloride (100 mg), brotizolam (0.25 mg), etizolam (1 mg) | 50 | IV | Staphisagria | One year later, no conventional medicine, Step III to recovery |
| Causticum | |||||||||
| Magnesia muriatica | |||||||||
| 5. E.H | 47 | F | No | 2 years and 10 months | Maprotilinehydrochloride (75 mg), sulpiride (150 mg), alprazolam (1.2 mg) | 37 | II | Arsenicum album | 10 months later, no conventional medicines. 1 and 4 months later, Step III to recovery |
| Natrum muriaticum | |||||||||
| Casusticum | |||||||||
| 6. H.T | 40 | F | Idea ++ | 1 year | Fluvoxamine maleate (75 mg), sulpiride (150 mg) | 51 | II | Calccarea phosphorica | 3 months later, no conventional medicines. Continue homeopathic medicines. Step II |
| Magnesia muriatica | |||||||||
| 7. T.K | 50 | F | Idea + | 2 years and 6 months | Amixapine (25 mg), etizolam (1 mg) | 48 | II | Arsenicum album | 4 months later, no conventional medicines. 10 months later, Step III to recovery |
| 8. S.I | 29 | F | Idea+ | 2 years and 2 months | Amixapine (30 mg) | 59 | III | Staphisagria | 2 months later, no conventional medicines. 8 months later, Step III to recovery |
| 9. S.K | 57 | F | Attempt | 6 years | Milnacipran hydrochloride (25 mg) | 46 | III | Phosphorus arsenicum album | No conventional medicines after the first visit. 6 months later Step III to recovery |
| 10. M.F | 42 | F | Attempt | 2 years and 1 month | Fluvoxamine maleate (75 mg) | 45 | II | Argentum nitricum | 1 month later, no conventional medicines. 7 months later, Step III to recovery |
| 11. T.I | 50 | F | Idea + | 5 years | Fluvoxamine maleate (50 mg), milnacipran hydrochloride (100 mg), loprazolam (0.4 mg), flunitrasepam (1 mg) | 55 | Staphisagria | 4 months later, no conventional medicines. 10 months later, Step III to recovery | |
| Calcarea sulphurica | |||||||||
| 12. Y.S | 29 | F | Idea + | 2 years | Amixapine (75 mg), etizolam (1.5 mg), milnacipran hydrochloride (75 mg), flunitrazepam (3 mg), triazolam (0.25 mg) | 49 | III | Calcarea silicata | Amoxapine (50 mg) lorazepam (1 mg) 10 months later, finished. Step I |
| Staphisagria | |||||||||
| Silica | |||||||||
| 13.N.O | 34 | M | Attempt | 3 months | No | 59 | IV | Kali phosphoricum | 1 year and 2 months later, Step III to recovery |
| Rhus toxicodendron | |||||||||
| 14. K.F | 38 | F | Idea + | 5 years | Fluvoxamine maleate (150 mg), aloprazolam (1.2 mg), etizolam (2 mg), zopiclone (15 mg), brotizolam (0.5 mg) zolpidem tartrate (20 mg) | 68 | IV | Lycopodium | One year later, no conventional medicine. Continue homeopathic medicines. Step II |
| Staphisagria medorrhinum | |||||||||
| 15. Y.I | 59 | F | Idea++ | 15 years | Maprotiline hydrochloride (75 mg), sulpiride (100 mg), cloxazolam (2 mg) | 50 | IV | Natrum muriaticum | 2 years and 2 months later, no conventional medicine. Did not continue treatment |
| Arsenicum album | |||||||||
| Thuja | |||||||||
| Staphisagria | |||||||||
| 16. S.M | 43 | M | No | 2 years and 8 months | Amoxapine (30 mg), aloprazolam (1.2 mg) | 44 | Lycopodium | 3 years and 3 months later, no conventional medicines. Continued homeopathic medicines. Step II | |
| 17. KS | 42 | F | Idea ++ | 4 years | Nortriptyline hydrochloride (50 mg), amoxapine (50 mg), diazepam (4 mg) ethyl loflazepate (1 mg), flunitrazepam (4 mg), etizolam (1 mg) | 75 | III | Natrum muriaticum | Nortriptyline hydrochloride (20 mg), amoxapine (100 mg), sulpiride (100 mg), diazepam (4 mg). 1 year and 6 months later, did not continue treatment. |
| Gelsemium | |||||||||
| Lycopodium | |||||||||
| Cuprum | |||||||||
| 18. A.S | 41 | M | Idea+ | 6 months | Paroxetine hydrochloride (10 mg) | 57 | Lycopodium | 4 months later, Step III to recovery | |
| Aurum m-natronatum | |||||||||
| 19. S.K | 20 | M | No | 3 years | Paroxetine hydrochloride (40 mg), perospironehydrochloride hydrate (4 mg), lorazepam (0.5 mg), trazodone hydrochloride (25 mg) | 49 | IV | Lycopodium | 1 year and 11 months, paroxetine hydrochloride (10 mg). Did not continue treatment. |
| Arsenicum album | |||||||||
| 20. Y.N | 52 | M | No | 2 years and 3 months | Fluvoxamine maleate (75 mg), amitriptyline hydrochloride (75 mg), amoxapine (75 mg), brotizolam (50 mg) flunitrazepam (2 mg) | 41 | III | Lycopodium | 6 months later, did not continue treatment. |
| 21. H.T | 58 | M | No | 3 years | Fluvoxamine maleate (150 mg), brotizolam (0.25 mg), trazodone hydrochloride (1 mg) | 45 | III | Phosphrus | One year and 9 months later, no conventional medicine. One year and 11 months later, Step III to recovery |
| 22. T.O | 59 | F | Idea + | 5 years | Sulpiride (150 mg), fluvoxamine maleate (150 mg), lorazepam (0.5 mg), quazepam (15 mg), brotizolam (0.25,mg) | 58 | IV | Natrum muriaticum | 8 months later, did not continue treatment. |
| Lycopodium | |||||||||
| Bryonia | |||||||||
| 23. J.T | 46 | F | Idea + | 5 years | Sertraline hydrochloride (50 mg), alprazolam (1.2 mg), brotizolam (0.25 mg) | 58 | IV | Merrcurius solubilis | 11 months later, no conventional medicine. One year and 2 months later, Step III to recovery |
| Sepia | |||||||||
| 24. K.N | 47 | M | No | 3 years | Paroxetine hydrochloride (20 mg), etizolam (1 mg), zolpidem tartrate (5 mg) | 56 | IV | Aurum metalicum | 3 months later, less conventional medicine: Zolpidem tartrate (5 mg). 5 months later, finished. Step I |
| Aurum sulphratum | |||||||||
| 25. Y.S | 37 | F | Attempt | 6 years | Paroxetine hydrochloride (40 mg), cloxazolam (2 mg) | 59 | IV | Aurum m-natronatum | 1 year and 3 months later, Step III to recovery |
| Carcinosinum | |||||||||
| 26. N.T | 47 | M | Idea+ | 5 years | Paroxetine hydrochloride (40 mg), ethyl loflazepate (3 mg), bromazepam (15 mg), zopiclone (10 mg), flunitrasepam (2 mg) | 48 | IV | Aurum arsenicum | Paroxetine hydrochloride (5 mg), bromazepam (6 mg) zopiclone (10 mg) continue homeopathic medicines. Step II |
| Aurum sulphratum | |||||||||
| 27. M.S | 30 | F | No | 6 years | Sertraline hydrochloride (50 mg), flunitrazepam (2 mg), etizolam (1 mg) | 54 | IV | Ignatia amara | 4 months later, did not continue treatment. |
| Aurum m-natronatum | |||||||||
| Natronatum | |||||||||
| 28. S.I | 37 | F | Idea + | 8 years | Paroxetine hydrochloride (10 mg), sulpiride (50 mg), brotizolam (0.25 mg) | 59 | II | Lachesis | 1 year and 7 months later, mirtazapine (15 mg), brotizolam (0.125 mg). Continue homeopathic medicines. Step II |
| Chamomilla | |||||||||
| 29. H.M | 32 | F | Idea ++ | 10 years | Paroxetine hydrochloride (10 mg), alprazolam (1.2 mg), brotizolam (0.25 mg), zolpidem tartrate (10 mg) | 50 | III | Carcinosinum | 2 years later, paroxetine hydrochloride (5 mg), bromazepam (6 mg), brotizolam (0.25 mg), zolpidem tartrate (10 mg). Continue homeopathic medicines. Step II |
| Caisticum | |||||||||
| Kaliphosphoricum kali arsenicosum | |||||||||
| 30. T.K | 36 | M | Idea+ |
4 years | Sertraline hydrochloride (50 mg), aripiprazole (3 mg), mirtazapine (15 mg), tandospirone citrate (40 mg), lormetazepam (1 mg), lithium carbonate (200 mg) | 49 | II | Staphisagria | One year and 1 month later, no conventional medicines. One year and 4 months later, no remedies, Step III to recovery |
| Aurum sulphratum | |||||||||
| 31. A.N | 25 | F | Attempt | 1 year and 6 months | Sertraline hydrochloride (100 mg), amoxapine (50 mg), aripiprazole (3 mg), nortriptyline hydrochloride (150 mg), mianserin hydrochloride (30 mg), setiptiline maleate (1 mg), triazolam (0.25 mg) dosulepin hydrochloride (50 mg), zolpidem tartrate (10 mg) | 51 | IV | Calcarea carbonica | Less conventional medicines: Lorazepam (1.5 mg), zolpidem tartrate (5 mg). 1 year later, finished. Step I |
| Calcarea phosphoria | |||||||||
| Magnesia carbonica |
Four of the seven patients who did not continue treatment did not benefit from homeopathy, and the duration of homeopathic treatment ranged from 4 to 12 months (Nos. 2, 20, 22 and 27). The remaining three patients did not visit the clinic because they had completed their treatment or were in the process of reducing their antidepressant medications, and the duration of homeopathic treatment was >18 months (Nos. 15, 17 and 19).
The four Step I cases (Nos. 1, 12, 24, and 31) included those in whom the homeopathic treatment was terminated at the patients’ request when their daily life has improved and the treatment with antidepressants was completed or being reduced.
Seven patients in Step II (Nos. 3, 6, 14, 16, 26, 28, and 29) were receiving homeopathy for >2 years.
Table 2 presents the data of the 13 recovered patients. Except for 2 cases, the duration of depression was 2–6 years. The recovery point for 11 cases was 6–23 months after treatment initiation. One of the 11 cases is achieved complete cure through homeopathy based on the three-step path to recovery.
Data for 10 patients with depression who had integrative medicine consultation in June 2007–December 2008.
| Case no. | Age | Sex (F/M) | Suicide idea/attempt | Duration of illness | Conventional medicines | SDS first visit | CMI first visit | Remedies | Progress |
|---|---|---|---|---|---|---|---|---|---|
| 1. T.I | 50 | F | Idea + | 5 years | Fluvoxamine maleate (50 mg), milnacipran hydrochloride (100 mg), loprazolam (0.4 mg), flunitrasepam (1 mg) | 55 | Staphisagria | 4 months later, no conventional medicines. 10 months later, recovered. | |
| Calcarea sulphurica | |||||||||
| 2. Y.S | 29 | F | Idea + | 2 years | Amixapine (75 mg), etizolam (1.5 mg), milnacipran hydrochloride (75 mg), flunitrazepam (3 mg), triazolam (0.25 mg) | 49 | III | Calcarea silicata | Amoxapine (50 mg) lorazepam (1 mg) 10 months later, finished. |
| Staphisagria | |||||||||
| Silica | |||||||||
| 3.N.O | 34 | M | Attempt | 3 months | No | 59 | IV | Kali phosphoricum | 1 year and 2 months later, recovered. |
| Rhus toxicodendron | |||||||||
| 4. K.F | 38 | F | Idea + | 5 years | Fluvoxamine maleate (150 mg), aloprazolam (1.2 mg), etizolam (2 mg), zopiclone (15 mg), brotizolam (0.5 mg) zolpidem tartrate (20 mg) | 68 | IV | Lycopodium | One year later, no conventional medicine. Continue homeopathic medicines. |
| Staphisagria medorrhinum | |||||||||
| 5. Y.I | 59 | F | Idea++ | 15 years | Maprotiline hydrochloride (75 mg), sulpiride (100 mg), cloxazolam (2 mg) | 50 | IV | Natrum muriaticum | 2 years and 2 months later, no conventional medicine. Did not continue. |
| Arsenicum album | |||||||||
| Thuja | |||||||||
| Staphisagria | |||||||||
| 6. S.M | 43 | M | No | 2 years and 8 months | Amoxapine (30 mg), aloprazolam (1.2 mg) | 44 | Lycopodium | 3 years and 3 months later, no conventional medicines. Continue homeopathic medicines. | |
| 7. K.S | 42 | F | Idea ++ | 4 years | Nortriptyline hydrochloride (50 mg), amoxapine (50 mg), diazepam (4 mg) ethyl loflazepate (1 mg), flunitrazepam (4 mg), etizolam (1 mg) | 75 | III | Natrum muriaticum | Nortriptyline hydrochloride (20 mg), amoxapine (100 mg), sulpiride (100 mg), diazepam (4 mg). 1 year and 6 months later, did not continue. |
| Gelsemium | |||||||||
| Lycopodium | |||||||||
| Cuprum | |||||||||
| 8. A.S | 41 | M | Idea+ | 6 months | Paroxetine hydrochloride (10 mg) | 57 | Lycopodium | 4 months later, recovered. | |
| Aurum m-natronatum | |||||||||
| 9. S.K | 20 | M | No | 3 years | Paroxetine hydrochloride (40 mg), perospironehydrochloride hydrate (4 mg), lorazepam (0.5 mg), trazodone hydrochloride (25 mg) | 49 | IV | Lycopodium | 1 year and 11 months, paroxetine hydrochloride (10 mg). Did not continue. |
| Arsenicum album | |||||||||
| 10. Y.N | 52 | M | No | 2 years and 3 months | Fluvoxamine maleate (75 mg), amitriptyline hydrochloride (75 mg), amoxapine (75 mg), brotizolam (50 mg) flunitrazepam (2 mg) | 41 | III | Lycopodium | 6 months later, did not continue. |
-
SDS, Zung self-rating depression scale.
Clinical case presentation (case 30 in Table 1)
A 36-year-old man first experienced depression 5 years before his integrative medicine consultation. He had been treated with antidepressants for >4 years. He reported intermittent unemployment as he had started and lost 4 jobs because he could not concentrate and exhibited an indifference and aversion to his work. His SDS score was 49. Medications were sertraline hydrochloride, aripiprazole, mirtazapine, tandospirone, citrate, lormetazepam, and lithium carbonate. His clinical and homeopathic history is shown in Figure 3. Based on the holistic approach, he was prescribed Staphisagria 30c, 1 pill daily. His three-step path to recovery is described as follows.
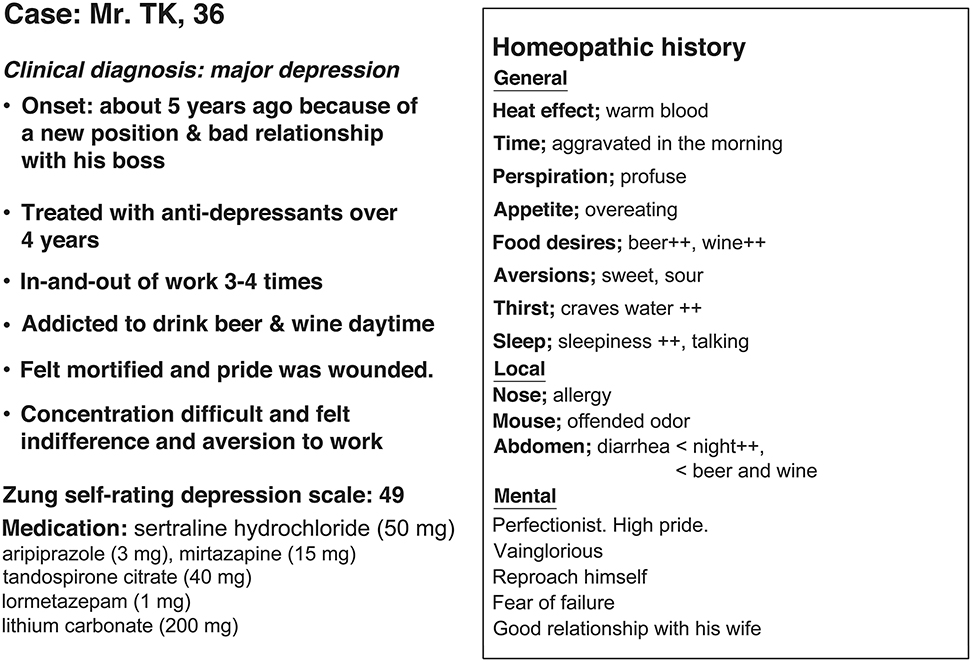
Homeopathic history of case 30 in Table 1.
Step I: To reduce difficulties in daily life (months 1–4)
At the 1-month follow-up after starting homeopathic treatment, the patient reported feeling less tired and sleeping well. At 2 months, however, his condition had not changed further. He reported feeling very “empty” and was concerned about his high alcohol intake. The treatment strategy was changed because the holistic approach was determined not to be working very well. Consequently, the method of complexity was used for understanding the deeper level of disease fluctuations, and Aurum sulphuratum 30c, one pill daily, was changed to a daily dose. At 4 months, the patient reported feeling better and had decreased emotional experience of emptiness. The depression level before starting homeopathy was 7 compared with 10 (7/10).
Step II: To reduce or stop conventional medicines (months 6–12)
At the 6-month follow-up, the patient was able to successfully reduce his antidepressant dose. He did not take tandospirone citrate and lithium carbonate. His depression level had fallen to 3/10. At 8 months, he was no longer in a depressive state, and he began to prepare to work again. At 10 months, he was preparing to restart work within the month. At the 1-year follow-up, he had stopped all conventional medicines and resumed working.
Step III: To reduce or stop homeopathic medicines (after 1 year)
After 1 year and 4 months of treatment with integrative medicine, the patient’s mental health status was good, and he no longer needed any homeopathic medicines. He reported feeling fulfilled in his life. He reported experiencing no recurrence of depression for >6 months, and he subsequently ended his treatment because he had recovered completely.
Discussion
The effect of antidepressants in preventing relapse and recurrence of depression is limited [15, 16]. Despite long-term treatment with antidepressants, difficulties in daily life persist for some patients. For patients with depression who have been treated with antidepressants, it is important to assess their progress after treatment with integrative psychiatry and homeopathy.
This study has suggested an approach to assess progress using the three-step path to recovery from depression through homeopathy. Step I is to decrease daily difficulties by adding homeopathic treatment, which improves the patient’s QOL. As patients improve, they can naturally reduce or stop their prescribed dose of antidepressants, which is Step II. Homeopathy aids their natural healing, so they can recover by themselves and subsequently not need any remedies, which is Step III, leading to a complete cure.
Recent research addressing the recurrence of depression reported that it is desirable to continue long-term conventional medicine for at least 1 year and preferably for 2 years [17]. However, an increasing number of patients with chronic depression do not improve with antidepressant treatment over 2 years [18].
The industry of psychopharmacology has been reported to be in crisis—the billions of dollars and decades of research spent on psychopharmacology are no longer producing new effective treatments [19]. Clinical evidence supports continuing the treatment of depression with pharmacotherapy, psychotherapy, and other nonpharmacotherapeutic approaches [20, 21]. Recent meta-analyses have found high dropout and low remission rates as well as clinically significant differences between antidepressants and placebos only for patients with severe depression [22], [23], [24]. This lack of effective treatment or cure may lead patients to search for CAM.
Homeopathy is a patient-centered and holistic medical system that utilizes the natural healing power of the sick person; it treats the person, not the disease. In homeopathy, the story told by a sick person is understood in a different context for each individual, and remedies are selected accordingly. In this process, a variety of strategies are used to respond to the “state” of the sick person at the time, including the use of different remedies with great precision [25], [26], [27].
In the present study, homeopathy has been integrated with conventional medicine since 2000, mainly for treating chronic diseases; 94% had already received conventional medicine, especially all psychiatry patients.
Owing to the variety and complexity of the remedies, they can be used in an integrated manner with conventional treatment for patients with depression who have not shown improvement with conventional treatment. For these patients, especially those with chronic depression who have difficulty in their daily lives despite receiving medications, homeopathy, as part of integrative psychiatry, will work according to the patient’s own natural recovery process.
Homeopathy is an individualized treatment; it has been difficult to report its efficacy in RCTs, especially for psychiatric disorders [28]. The reports of homeopathy as treatment for depression to date include a preliminary study by Katz et al. in 2005 and a study by Adler et al. in 2011, both of which included fluoxetine as treatment [29, 30]. They reported that homeopathy was as effective as fluoxetine in patients with acute depression. Subsequently, in 2020, they reported that homeopathy was more effective than fluoxetine in treating perimenopausal women with moderate to severe depression [31]. In 2020, the efficacy of homeopathy in the treatment of mental disorders was evaluated and the results showed that no difference in the outcomes between homeopathy and placebo treatment was found in patients with major depression [32].
It is worth noting that, in the current study, homeopathy resulted in complete healing within 2 years.These patients with chronic depression who have been treated with antidepressants for more than 2 and 6 years recovered in 6 months to 1 year and 11 months. All cases recovered within 2 years. Patients with depression for whom daily life remains difficult despite receiving medication may benefit from starting homeopathy as part of integrative psychiatry. The homeopathic recovery process leads to improvement of QOL, reduction of drug dosage, disappearance of symptoms, and complete recovery.The three-step path to recovery from depression illustrates and serves as a natural healing process for recovery, with homeopathy as an integrative medicine.
-
Research funding: None declared.
-
Author contributions: The author has accepted responsibility for the entire content of this manuscript and approved its submission.
-
Competing interests: Author states no conflict of interest.
-
Informed consent: Informed consent was obtained from all individuals included in this study.
-
Ethical approval: The research related to human use is in accordance with the tenets of the Helsinki Declaration. Ethical approval was not necessary due to the retrospective nature of the study.
References
1. World Health Organization. “Depression: let’s talk” say WHO, as depression tops list of causes of ill health [Online]. Available from: https://www.who.int/news-room/fact-sheets/detail/depression [Accessed 15 Nov 2020].Suche in Google Scholar
2. Ministry of Health, Labour and Welfare. Available from: https://www.mhlw.go.jp/wp/hakusyo/jisatsu/19/dl/1-1.pdf [Accessed 15 Nov 2020].Suche in Google Scholar
3. Carvalho, AF, Cavalcante, JL, Castelo, MS, Lima, MC. Augmentation strategies for treatment-resistant depression: a literature review. J Clin Pharm Therapeut 2007;32:415–28. https://doi.org/10.1111/j.1365-2710.2007.00846.x.Suche in Google Scholar PubMed
4. Thase, ME, Haight, BR, Richard, N, Rockett, CB, Mitton, M, Modell, JG. Remission rates following antidepressant therapy with bupropion or selective serotonin reuptake inhibitors: a meta-analysis of original data from 7 randomized controlled trials. J Clin Psychiatr 2005;66:974–81. https://doi.org/10.4088/jcp.v66n0803.Suche in Google Scholar PubMed
5. Machado, M, Iskedjian, M, Ruiz, I, Einarson, TR. Remission, dropouts, and adverse drug reaction rates in major depressive disorder: a meta-analysis of head-to-head trials. Curr Med Res Opin 2006;22:1825–37. https://doi.org/10.1185/030079906X132415.Suche in Google Scholar PubMed
6. Wang, PS, Aguilar-Gaxiola, S, Alonso, J, Angermeyer, MC, Borges, G, Bromet, EJ. Use of mental health services for anxiety, mood, and substance disorders in 17 countries in the WHO world mental health surveys. Lancet 2007;370:841–50. https://doi.org/10.1016/S0140-6736(07)61414-7.Suche in Google Scholar PubMed PubMed Central
7. Unützer, J, Klap, R, Sturm, R. Mental disorders and the use of alternative medicine: results from a national survey. Am J Psychiatr 2000;157:1851–7. https://doi.org/10.1176/appi.ajp.157.11.1851.Suche in Google Scholar PubMed
8. Solomon, D, Adams, J. The use of complementary and alternative medicine in adults with depressive disorders. A critical integrative review. J Affect Disord 2015;179:101–13. https://doi.org/10.1016/j.jad.2015.03.031.Suche in Google Scholar PubMed
9. Pratap, RC. Can an integrative approach to the management of depression help patients achieve functional recovery? A review of current literature. J Depress Anxiety 2013;2. https://doi.org/10.4172/2167-1044.1000141.Suche in Google Scholar
10. Leckridge, B. Homeopathy in primary care. New York: Churchill Livingstone; 1997.Suche in Google Scholar
11. Kaye, BS. Homeopathic practice. London: Pharmaceutical Press; 2007.Suche in Google Scholar
12. First, MB, Pincus, HA. The DSM-IV text revision: rationale and potential impact on clinical practice. Psychiatr Serv 2002;53:288–92. https://doi.org/10.1176/appi.ps.53.3.288.Suche in Google Scholar PubMed
13. Zung, WWK. A self-rating depression scale. Arch Gen Psychiatr 1965;12:63–70. https://doi.org/10.1001/archpsyc.1965.01720310065008.Suche in Google Scholar PubMed
14. Broadman, K, Erdmann, AJ, Lorge, I, Wolf, HG. The Cornell Medical Index-health questionnaire. II. As a diagnostic instrument. J Am Med Assoc 1951;145:152–7. https://doi.org/10.1001/jama.1951.02920210024006.Suche in Google Scholar PubMed
15. Hirschfeld, RM, Montgomery, SA, Aguglia, E, Amore, M, Delgado, PL, Gastpar, M, et al.. Partial response and nonresponse to antidepressant therapy: current approaches and treatment options. J Clin Psychiatr 2002;63:826–37. https://doi.org/10.4088/jcp.v63n0913.Suche in Google Scholar PubMed
16. Geddes, JR, Carney, SM, Davies, C, Furukawa, TA, Kupfer, DJ, Frank, E, et al.. Relapse prevention with antidepressant drug treatment in depressive disorders: a systematic review. Lancet 2003;361:653–61. https://doi.org/10.1016/S0140-6736(03)12599-8.Suche in Google Scholar PubMed
17. Prien, RF, Kupfer, DJ. Continuation drug therapy for major depressive episodes: how long should it be maintained? Am J Psychiatr 1986;143:18–23. https://doi.org/10.1176/ajp.143.1.18.Suche in Google Scholar PubMed
18. American Psychiatric Association. Practice guideline for the treatment of patients with major depressive disorder (revision). Am J Psychiatr 2000;157:1–45.Suche in Google Scholar
19. Fibiger, HC. Psychiatry, the pharmaceutical industry, and the road to better therapeutics. Schizophr Bull 2012;38:649–50. https://doi.org/10.1093/schbul/sbs073.Suche in Google Scholar PubMed PubMed Central
20. Möller, HJ. Outcomes in major depressive disorder: the evolving concept of remission and its implications for treatment. World J Biol Psychiatr 2008;9:102–14. https://doi.org/10.1080/15622970801981606.Suche in Google Scholar PubMed
21. Rief, W, Nestoriuc, Y, Weiss, S, Welzel, E, Barsky, A, Hofmann, S. Meta-Analysis of the placebo response in antidepressant trials. J Affect Disord 2009;118:1–8. https://doi.org/10.1016/j.jad.2009.01.029.Suche in Google Scholar PubMed
22. Forneris, CA, Nussbaumer, B, Kaminski-Hartenthaler, A, Morgan, LC, Gaynes, BN, Sonis, JH, et al.. Psychological therapies for preventing seasonal affective disorder. Cochrane Database Syst Rev 2015;46:CD011270.10.1002/14651858.CD011270Suche in Google Scholar
23. Gartlehner, G, Nussbaumer, B, Gaynes, BN, Forneris, CA, Morgan, LC, Greenblatt, A, et al.. Second-Generation antidepressants for preventing seasonal affective disorder in adults. Cochrane Database Syst Rev 2015;58:CD011268.10.1002/14651858.CD011268.pub2Suche in Google Scholar PubMed
24. Benjamin, JS, Virginia, AS. Kaplan & Sadock’s synopsis of psychiatry. Behavioral science/clinical psychiatry, 10th ed. New York: Wolters Kluwer; 2007. p. 839.Suche in Google Scholar
25. Hahnemann, S. Organon of the medicl art, 6th ed. Redmond, Washington: O’reilly W.B.; 1996:65 p.Suche in Google Scholar
26. Itamura, R, Hosoya, R. Homeopathic treatment of patients with intractable atopic dermatitis. Homeopathy 2003;92:108–14. https://doi.org/10.1016/s1475-4916(03)00017-1.Suche in Google Scholar PubMed
27. Itamura, R. Effect of homeopathic treatment of sixty Japanese patients with chronic skin disease. Compl Ther Med 2007;15:115–20. https://doi.org/10.1016/j.ctim.2006.04.005.Suche in Google Scholar PubMed
28. Davidson, JR, Crawford, C, Ives, JA, Jonas, WB. Homeopathic treatments in psychiatry: a systematic review of randomized placebo-controlled studies. J Clin Psychiatr 2011;72:795–805. https://doi.org/10.4088/jcp.10r06580.Suche in Google Scholar
29. Rotella, F, Cassioli, E, Falone, A, Ricca, V, Mannucci, E. Homeopathic remedies in psychiatric disorders: a meta-analysis of randomized controlled trials. J Clin Psychopharmacol 2020;40:269–75. https://doi.org/10.1097/jcp.0000000000001196.Suche in Google Scholar
30. Katz, T, Fisher, P, Katz, A, Davidson, J, Feder, G. The feasibility of randomized, placebo-controlled clinical trial of homeopathic treatment of depression in general practice. Homeopathy 2005;94:145–52. https://doi.org/10.1016/j.homp.2005.04.002.Suche in Google Scholar PubMed
31. Adler, UC, Paiva, NMP, Cesar, AT, Adler, MS, Molina, A, Padula, AE, et al.. Homeopathic individualized Q-potencies versus fluoxetine for moderate to severe depression: double-blind, randomized non-inferiority trial. Evid Complement Alternat Med 2011;2011:520182. https://doi.org/10.1093/ecam/nep114.Suche in Google Scholar PubMed PubMed Central
32. del Carmen Macias-Cortes, E, Llanes-Gonzales, L, Aguilar-Faisal, L, Asbun-Bojalil, J. Individualized Homeopathic treatment and fluoxetine for moderate to severe depression in peri-and postmenopausal women (HOMDEP-MENOP Study): a randomized, double-dummy, double-blind, placebo-controlled trial. PLoS One 2015;10:e0118440. https://doi.org/10.1371/journal.pone.0118440.Suche in Google Scholar PubMed PubMed Central
© 2022 the author(s), published by De Gruyter, Berlin/Boston
This work is licensed under the Creative Commons Attribution 4.0 International License.
Artikel in diesem Heft
- Frontmatter
- Reviews
- Does acupuncture improve sexual dysfunction? A systematic review
- Non-alcoholic fatty liver disease – discussed under the light of Unani medicine
- Phytochemistry and pharmacology of Celastrus paniculatus Wild.: a nootropic drug
- Low back pain patients’ perceived effectiveness of utilizing complementary and alternative medicine: a systematic review of qualitative studies
- Efficacy and tolerability of Lavandula angustifolia in treating patients with the diagnosis of depression: a systematic review of randomized controlled trials
- Research Articles
- Psychobiotic interventions attenuate chronic alcohol use-mediated exacerbation of posttraumatic stress disorder in rats: the role of gut-liver axis response
- Evaluation of the toxicity of crude aqueous Pleurotus tuber-regium (Fr.) Singer extract in mice
- Effects of crude methanol extract of Adansonia digitata fruit pulp on Naja nigricollis venom-induce toxicity in Wistar rats
- Integrative medicine approaches to chronic depression: case studies of the recovery process with a three-step path to recovery and significant cure
- Antimicrobial, anti-adhesion, anti-biofilm properties of goji berry (Lycium barbarum) against periodontal bacteria: potential benefits for periodontal diseases
- Method development and validation for quantification of six bioactive compounds (andrographolide, columbin, piperine, gallic, paracoumaric and oleanolic acids) by HPTLC
- Gallic acid a flavonoid isolated from Euphorbia hirta antagonizes gamma radiation induced radiotoxicity in lymphocytes in vitro
- Naturopathic knowledge and approaches to managing endometriosis: a cross-sectional survey of naturopaths with experience in endometriosis care
- Halimeda gracilis (Kadarpassi chooranam) Phytochemical analysis and biological significance – a novel Siddha drug
- Trends in the St. John’s wort (Hypericum perforatum) research literature: a bibliometric analysis
- Use and perception of complementary and alternative medicine among Iranian psychologists
- Innovative histological and histochemical characterization of tongue biopsies from patients with burning mouth syndrome
- A randomized, double-blind, placebo-controlled, cross-over trial to evaluate the effect of EstroSense® on 2-hydroxyestrone:16α-hydroxyestrone ratio in premenopausal women
- Comparing the influence of foot reflexology and fasting mimicking diet on quality of life and sleep quality in obesity hypoventilation syndrome
- The effects of Cynodon dactylon (Poaceae family) and Dolichos biflorus (Fabaceae family) extracts on decreasing size and excretion of kidney and urinary tract stones: a randomized, double-blind controlled trial
- Role of Bifidobacterium spp. intake in improving depressive mood and well-being and its link to kynurenine blood level: an interventional study
- A randomized controlled clinical trial to evaluate safety and efficacy of a Unani formulation in the management of Kalaf (Melasma)
- Impact of yoga and physical exercise on psychological wellbeing among substance abusers: a randomized controlled trial
- A non-inferiority randomized controlled clinical trial comparing Unani formulations and PUVAsol in non-segmental vitiligo
- Efficacy of individualized homeopathic medicines in primary dysmenorrhea: a double-blind, randomized, placebo-controlled, clinical trial
- A comparative study of chemical constituents and safety of Thai herbal medicated oil formula and traditional medicated oil
- Efficacy of Ayurvedic treatment protocol in gouty arthritis – a clinical study
- Knowledge, attitude and perception of complementary and alternative system of medicine in Tamilnadu and Pudhucherry, South India
- Discussion Forum
- Time to say good-bye? Homeopathy, skeptics and thoughts on how to proceed
- Congress Abstracts
- 2022 INCAM Research Symposium
Artikel in diesem Heft
- Frontmatter
- Reviews
- Does acupuncture improve sexual dysfunction? A systematic review
- Non-alcoholic fatty liver disease – discussed under the light of Unani medicine
- Phytochemistry and pharmacology of Celastrus paniculatus Wild.: a nootropic drug
- Low back pain patients’ perceived effectiveness of utilizing complementary and alternative medicine: a systematic review of qualitative studies
- Efficacy and tolerability of Lavandula angustifolia in treating patients with the diagnosis of depression: a systematic review of randomized controlled trials
- Research Articles
- Psychobiotic interventions attenuate chronic alcohol use-mediated exacerbation of posttraumatic stress disorder in rats: the role of gut-liver axis response
- Evaluation of the toxicity of crude aqueous Pleurotus tuber-regium (Fr.) Singer extract in mice
- Effects of crude methanol extract of Adansonia digitata fruit pulp on Naja nigricollis venom-induce toxicity in Wistar rats
- Integrative medicine approaches to chronic depression: case studies of the recovery process with a three-step path to recovery and significant cure
- Antimicrobial, anti-adhesion, anti-biofilm properties of goji berry (Lycium barbarum) against periodontal bacteria: potential benefits for periodontal diseases
- Method development and validation for quantification of six bioactive compounds (andrographolide, columbin, piperine, gallic, paracoumaric and oleanolic acids) by HPTLC
- Gallic acid a flavonoid isolated from Euphorbia hirta antagonizes gamma radiation induced radiotoxicity in lymphocytes in vitro
- Naturopathic knowledge and approaches to managing endometriosis: a cross-sectional survey of naturopaths with experience in endometriosis care
- Halimeda gracilis (Kadarpassi chooranam) Phytochemical analysis and biological significance – a novel Siddha drug
- Trends in the St. John’s wort (Hypericum perforatum) research literature: a bibliometric analysis
- Use and perception of complementary and alternative medicine among Iranian psychologists
- Innovative histological and histochemical characterization of tongue biopsies from patients with burning mouth syndrome
- A randomized, double-blind, placebo-controlled, cross-over trial to evaluate the effect of EstroSense® on 2-hydroxyestrone:16α-hydroxyestrone ratio in premenopausal women
- Comparing the influence of foot reflexology and fasting mimicking diet on quality of life and sleep quality in obesity hypoventilation syndrome
- The effects of Cynodon dactylon (Poaceae family) and Dolichos biflorus (Fabaceae family) extracts on decreasing size and excretion of kidney and urinary tract stones: a randomized, double-blind controlled trial
- Role of Bifidobacterium spp. intake in improving depressive mood and well-being and its link to kynurenine blood level: an interventional study
- A randomized controlled clinical trial to evaluate safety and efficacy of a Unani formulation in the management of Kalaf (Melasma)
- Impact of yoga and physical exercise on psychological wellbeing among substance abusers: a randomized controlled trial
- A non-inferiority randomized controlled clinical trial comparing Unani formulations and PUVAsol in non-segmental vitiligo
- Efficacy of individualized homeopathic medicines in primary dysmenorrhea: a double-blind, randomized, placebo-controlled, clinical trial
- A comparative study of chemical constituents and safety of Thai herbal medicated oil formula and traditional medicated oil
- Efficacy of Ayurvedic treatment protocol in gouty arthritis – a clinical study
- Knowledge, attitude and perception of complementary and alternative system of medicine in Tamilnadu and Pudhucherry, South India
- Discussion Forum
- Time to say good-bye? Homeopathy, skeptics and thoughts on how to proceed
- Congress Abstracts
- 2022 INCAM Research Symposium