Nanomedicines in the European translational process
-
Susanne Bremer-Hoffmann
Susanne Bremer-Hoffmann, Dr. rer nat, holds a PhD degree in Biology obtained from the Charite University Hospital Berlin in Germany for her work on the development of immunotherapies against leukemia. After post-doctoral research at the Federal Institute for Risk Assessment in Germany, Susanne joined the Institute for Health & Consumer Protection (IHCP) which is part of the Joint Research Centre (JRC) of the European Commission. Susanne became a team member of the European Centre for the Validation of Alternative Methods (ECVAM) in 1995 where she was involved in formal validation studies of toxicological in vitro tests detecting embryotoxicity and endocrine disruption and the regulatory acceptance of some tests at the OECD. She collaborated in several FP6 and FP 7 projects including the public/privat partnership initiative “SEURAT-1”. She contributed to more than 70 peer-reviewed scientific paper. In 2014 Susanne Bremer-Hoffmann joined the Nanobiosciences Unit of the same Institute and is currently participating in the establishment of the European Nanocharacterisation Laboratory.
 ,
Valeria Amenta
,
Valeria Amenta
Valeria Amenta holds a PhD in Supramolecular Chemistry from the University of Sheffield (UK), a Master’s degree in Pharmaceutical Chemistry and Technology and a master in Regulatory Disciplines of Medicines from the University of Catania (Italy). Her research has been focused on the synthesis of compounds that could potentially be used as a treatment for benign prostatic hyperplasia (Master’s degree research) and on the investigation of the effects of solvents on intermolecular interactions using UV-Vis and NMR techniques (PhD research). In 2012 she joined, as post-doctoral researcher, the Nanobiosciences Unit of Institute for Health & Consumer Protection (IHCP) at the European Commission’s Joint Research Centre (JRC), where she was involved in several projects and activities related to safety assessment and regulatory aspects of nanomaterials. Since November 2014 she works as scientific officer in the Substance Identity & Data Sharing Unit of the European Chemicals Agency (ECHA).
François Rossi studied Materials Science at Grenoble (DEng 1977) and obtained his PhD in 1989 from Université Claude Bernard in Lyon. After 2 years in industry in France and Germany, he joined the French Atomic Energy Commission (CEA) as R&D group leader in Nuclear Materials Engineering. He was then a guest scientist in Los Alamos National Laboratory USA in 1986–1987 (Center for Materials Science), and moved back to CEA in Grenoble “Advanced Technology Directorate” as section leader, working on Surface Engineering for Metallurgical Applications. In 1991, he moved to the JRC, Institute for Advanced Materials (IAM) in Petten where he was the manager of the Advanced Coating Centre. After his transfer to Ispra in 1996, he developed plasma based processes and surface modifications for metallurgical and biological applications. From 2002 to 2014, he has been the head of the JRC NanoBiotechnology laboratory in the JRC Institute for Health and Consumer Protection, managing a group of 35 scientists and students working on bio/non bio interfaces, nanobioscience and toxicology testing of nanomaterials. Since January 2014, he is the Scientific Coordinator of the NanoBioScience Unit. He is author and co-author of 260 peer reviewed articles (H-index 33), 12 book chapters, and 15 patents and has been involved in more than 25 RTD projects from FP3 to FP7.

Abstract
In 2013, the World Health Organisation (WHO) released an update of the report on “Priority Medicines for Europe and the World” with the aim to bridge the gap between public health needs and the current research and development priorities. A number of emerging technologies are currently explored for their potential to respond to the identified unmet medical needs. Nanotechnology has the potential to offer scientific/technical solutions for some of these pharmaceutical gaps. The present report investigates to what extent projects funded by the European Commission will lead to innovative formulations as well as new therapeutic concepts, if clinical studies in European Member States investigating nanomedicines and finally if nanotech based products authorised in the European Union will contribute to identified public health needs.
Introduction
In 2013, the World Health Organisation (WHO) released a second report on the Priority Medicines for Europe and the World with the aim to bridge the gap between public health needs and the research and development priorities (1).
Presently, various emerging technologies are exploited to address the identified unmet medical needs. Among these technologies, nanotechnology is widely accepted as a potential driver of biomedical innovation, since it provides unique means to treat diseases and limit side effects of therapies. Nanomaterials are similar in size to intra and extracellular biological structures and can be functionalised to allow targeting and repairing of biological systems at the origin of the disease. Possessing these unique characteristics, nanotechnology opens new diagnostic and therapeutic scenarios that could fill pharmaceutical gaps as identified by the WHO working groups. Often nanotechnology is combined with other, innovative technologies such as biomaterials, stem cells and gene therapy. Diseases of particular interest are those with a high disability adjusted life year (DALY) value (representing an integrated single measure of mortality and disability) and a high socio-economic burden but with a low proportion of newly identified chemical entities such as cardiovascular, neuropsychiatric diseases as well as respiratory diseases (2).
The European Commission has recognised the opportunities offered by nanotechnology in the health care sector and has financed a wide range of projects as part of the 7th framework programme. These research activities have generated ideas, knowledge and prototypes aiming i) to make active principles with challenging physical-chemical properties available to the patient (e.g. low solubility), ii) to optimise drug delivery by active targeting and controlled release into the diseased tissue, iii) to use the physical properties of the nanomaterial for the development of therapeutic and diagnostic tools, iv) to engineer tissues and v) to combine diagnostic and therapeutic tools allowing a direct monitoring of the therapeutic progress (Figure 1). However, the complete translational process from product design to the market is long and requires a number of approval steps with increasing data requirements. In addition, the regulatory pathway might be unclear in the beginning of the research activity since the principal intended action of the product is decisive to whether the product will be regulated as medicinal product or medical device (Table 1). However, the “next generation” of nanomedicines often combine immunological, pharmacological, metabolic and physical means in one product in order to treat, diagnose or prevent diseases which requires an in depth evaluation on how the product should be regulated. In the currently released strategy document, the European Medicine Agency (EMA) and the heads of Medicines Agency are calling for strengthening the collaboration of medicinal product and medical device regulators in various areas including combination and borderline products which are also of high relevance for nanomedicines (10).
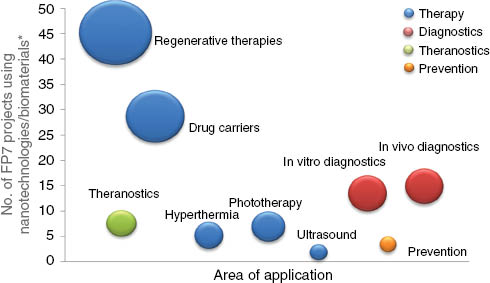
In 131 research projects funded within the 7th framework programme different diagnostic and therapeutic concepts were developed. Beside huge efforts for regenerative medicine a trend towards the exploitation of the physical properties of nanomaterial in order to develop in vivo imaging tools as well as hypothermic and phototherapeutic applications is remarkable. (*Status of published research activities in “Cordis” in March 2015.)
Databases that have been used for the analysis.
| Queries | Reference documents and databases | |
|---|---|---|
| Drug development projects (n=131) | Which kinds of platforms have been used? Which kinds of therapeutic/diagnostic concept were considered? Which pharmaceutical gaps are addressed? | Community Research and Development Information Service (Cordis) (3) Project specific websites Information retrieved from Frima et al. (4) |
| Clinical trials (n=69) | Which nanomedicines are listed in the EU clinical trial database? In which Member States the clinical trials have been performed? What kinds of nanovector platforms have been assessed in clinical trials? Which pharmaceutical gaps are addressed? Are the products developed based on active targeting of the diseased tissue? | Information retrieved from the databases of Etheridge et al. (5) and Hafner et al. (6) EU Clinical Trials Register (7) |
| Authorisation (n=30) | Which products have been authorised? What kinds of platforms have been used? What kinds of biological funtionalisations have been used? | European Medicines Agency (8) Heads of Medicines Agencies (9); |
The present report elucidates to which extent nanomedicines in Europe address pharmaceutical gaps as identified by the WHO and summarises some challenges that are ahead in order to fully exploit nanotechnology for human health care (Figure 2).
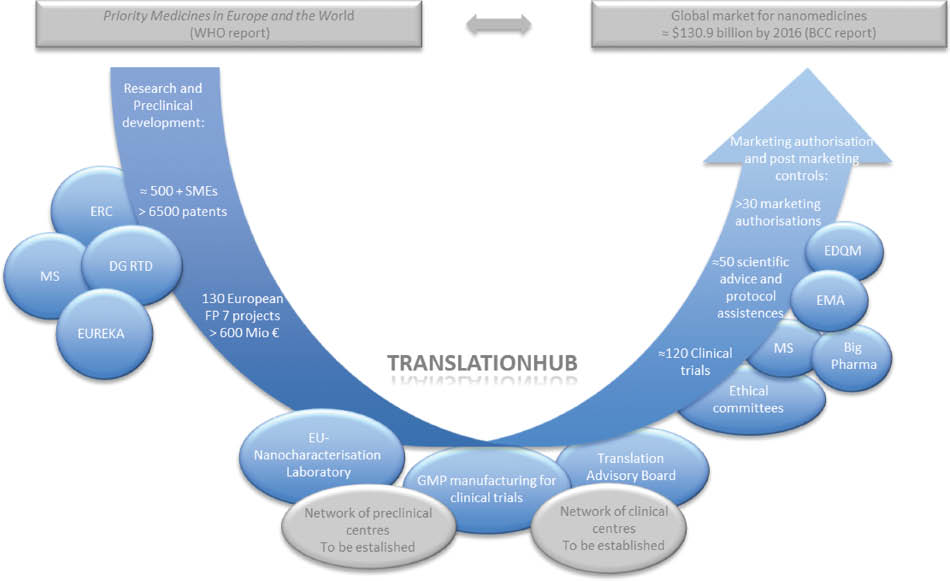
Overview of efforts undertaken by different players in Europe aiming to make nanomedicines available to the patients. The translation hub has been proposed by the European Technology Platform on Nanomedicine in order to overcome the “Valley of Death” (26). European Research Council (ERC); Member States (MS); Directorate-General for Research and Innovation (DG RTD), European Directorate for the Quality of Medicines and Healthcare (EDQM); European Medicines Agency (EMA).
Methodological approach
In order to assess whether nanotechnology can provide solutions for pharmaceutical gaps as identified by the WHO, European funded projects, European clinical trials as well as nanomedicinal products authorised in Europe have been analysed. The WHO report distinguish between three types of pharmaceutical gaps concerning
conditions for which pharmaceutical treatments are already ineffective or will soon become ineffective, e.g. antibacterial resistance and pandemic influenza.
diseases for which therapies are available but should be more adjusted to the patient’s needs, e.g. HIV, cardiovascular diseases, diabetes, tropical diseases, cancer etc.
diseases for which we currently do not have any sufficient therapy available such as stroke, Alzheimer disease, osteoarthritis, etc. Some diseases such as specific kind of cancer, e.g. pancreas carcinoma might also belong to pharmaceutical gap 3.
Furthermore, the WHO report provides data on the disability adjusted life years (DALY) related to various diseases. A DALY is an integrated single measure of mortality and disability due to a particular disease. One DALY represents a lost year of healthy living. These data have been used to investigate the contribution of nanomedicines that are currently in the translational process to address diseases with a high contribution to DALYs. Since there is no official definition of “nanomedicine” existing, we have used the most widely applied description: Nanomedicine is the application of nanotechnology for human health care products.
As shown in Table 1, databases hosting nanomedicine development projects, clinical trials and authorised products, respectively, have been analysed reflecting the status of the projects/products in March 2015.
In order to classify the used platforms the classification scheme of Wicky et al. has been used with a slight modification (11). The European Medicines Agency considers proteins that are acting as active principles as “biological” and these formulations have been excluded from the analysis.
Results
Authorised products
Currently several nanomedicines are authorised in the European Union. These nanomedicines regulated as medicinal products mainly used nanotechnology in order to overcome limitations related to physical-chemical properties of the active principle such as a lack of solubility, and/or to reduce drugs side effects by achieving a better accumulation in diseased tissues, e.g. by using the enhanced permeation and retention (EPR) effect. These so-called first generation nanomedicines have been on the European market for a long time, e.g. Caelyx – one of the first nanomedicines – was authorised in 1996 and the corresponding patents will expire soon. The results are reported in Figure 3 which shows the following results: out of the 30 products analysed, 12 nanomedicines use lipid based carrier systems aiming to optimise kinetic properties of the drug and reducing the side effects of the active principle by passive targeting; nine nanomedicines are classified as inorganic nanomaterials; four products use the nanocrystalline form of the active principles optimising the physical-chemical properties. In addition, five iron nanocomplexes that are authorised to combat anemia have been included (Figure 3). In the cases considered, nanotechnology is mainly applied to improve the physical-chemical properties of the active principle as well as to optimise the kinetics and biodistribution of the active principle (Figure 4).
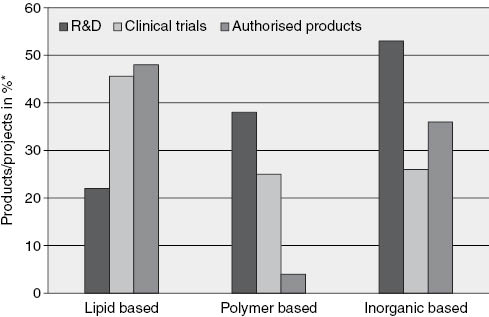
There is an increasing trend of using polymers and inorganic nanoparticles including nanocrystals and magnetic nanoparticles for the development of new nanomedicines. Lipid based carrier systems are less developed as new platforms in the FP 7 projects as compared to the two other types of products (authorised products n=30, clinical trials n=69, R&D n=131). (*Status of published research activities in “Cordis” in March 2015.)
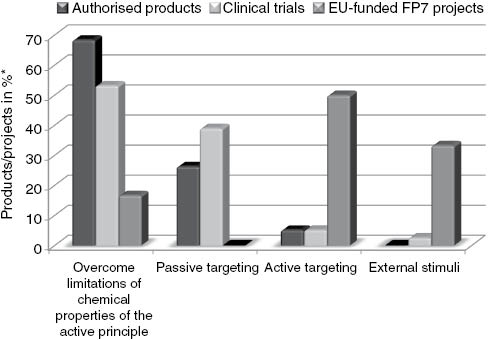
Authorised products use nanotechnologies mainly to optimise the physical-chemical properties of the active principle and the delivery of the active principle to the diseased tissue by passive targeting. In the recently performed research projects active targeting and controlled release of the cargo as well as the exploitation of the phys.chem. properties are more in the focus. (*Status of published research activities in “Cordis” in March 2015.)
Only eight of the investigated drugs address therapeutic gaps as identified by the WHO but 25 of the nanomedicines address diseases with a high DALY (Figures 5 and 6).
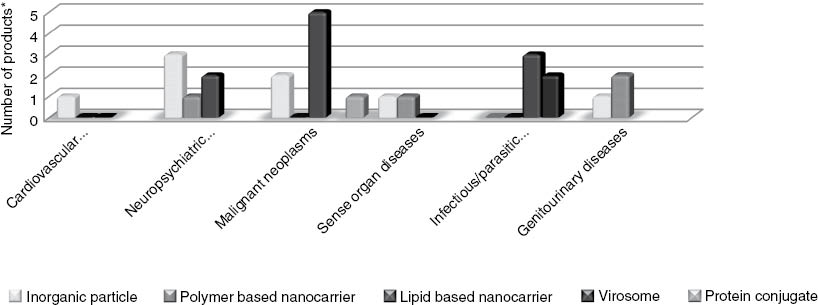
The majority of authorised nanomedicines address malignant neoplasms a disease with a high DALY value. (*Status of published research activities in “Cordis” in March 2015.)
Out of 131 research projects, 91 focus on therapeutic gaps as defined by the WHO and four projects are dedicated to coordination activities. Out of 69 products that are included in the EU clinical trials register 37 products are addressing priority diseases. Finally, out of 31 authorised products, only nine products address pharmaceutical gaps as defined by the WHO. (*Status of published research activities in “Cordis” in March 2015.)
Clinical trials
In order to get a better understanding on trends of nanotech based products in European clinical trials, potential nanomedicines as identified in the review articles of Hafner et al. (6), and Etheridge et al. (5) were assessed for their inclusion in the EU clinical trial data base. In total, clinical trials of 69 products were investigated and all Member States were involved in the approval process of clinical trials of different types of nanomedicines (Figure 7). The purposes of the clinical trials differed and covered aspects such as the assessment of future applicability domains of already approved formulations, e.g. different kind of neoplasms, the potential to combine nanomedicines with other therapeutic molecules in order to optimise therapeutic effects as well as safety/efficacy studies of new formulations. This non-exhaustive list of nanomedicines in clinical trials covers a wide range of diseases such as different types of solid tumours, schizophrenia, ADHD, growth disorder, hepatitis C, rheumatoid arthritis, pain relief, heart failure, HIV, etc. However, malignant neoplasms are the dominant target disease of nanomedicines (see Figure 6) and most of the nanoformulations identified are based on liposomes and polymeric nanoparticle (see Figure 3). Remarkably, at least three magnetic inorganic particle used for in vivo imaging are currently assessed in clinical trials. Nevertheless, the application of the marketing authorisation of the ironoxide “Sinerem”, an in vivo imaging diagnostic product, was withdrawn after EMA’s Committee for Medicinal Products for Human use raised concern on effectiveness of “Sinerem” in enhancing the images seen in the MRI scan. “Sinerem” is a diagnostic agent for the characterisation of lymph nodes in patients with pelvic cancer (12). Nevertheless, the data analysed in this study can only provide trends and additional clinical trials should to be included in order to complete the picture [e.g. those that are additionally reported in the “Bionest” report (13)].

Sixty-nine products included in published databases have been analysed for their registration in the European clinical trial database. All European Member states were involved in the authorisation of clinical trials to a different extent. The total number of clinical trials of nanomedicines/Member State is indicated in the map. (The analysis was performed in October 2014).
Drug development projects
In the 7th framework programme, the European Commission funded a significant number of projects focussing on the exploitation of nanotechnology for health care, e.g. the research theme on “Nanosciences, Nanotechnologies, Materials and New Production Technologies” (NMP) has funded 86 projects with a budget of 446 M€. Additionally, 31 projects with a budget of around 150 M€ were sponsored as part of the health programme. The funding programme “Smart System Integration Challenge” of the Directorate General “Communication Networks, Content and Technology” (DG CNECT) included 35 projects for the development of Micro-Nano-Bio Systems for a total budget of 135 M€. In addition, other European funding schemes such the “European Research Council”, “People” and “ERANET” incorporated nanotechnology for medical applications into their agendas. These projects have mainly covered technology readiness levels 1–3 starting from the development of basic principles towards the experimental proof of concept. The currently ongoing European framework programme “Horizon 2020” puts a strong emphasis on the translational aspect covering further developments in a preclinical setting before demonstrating the relevance of the product in the clinical environment (also referred to as TRL 4-7) (14). The first projects addressing the translational aspects have just started. These projects belonging to the “Translation Hub” as suggested by the European Platform of Nanomedicine: i) The coordination and support action “ENATRANS” will focus on measures needed to support the networking of stakeholders; ii) The projects “Nanofacturing” and “Nanopilot” are dedicated to the scale up nanomedicines for clinical use; iii) The European Nanomedicine Characterization Laboratory “EU-NCL” will support the quality and safety assessment of nanomedicines in the preclinical phase incl. nanomedicines that have been developed within the FP7. In addition, the “EU-NCL” will develop cascades of characterisation protocols for quality and safety assessments relevant to the major nano platform and biological functionalisations that are currently used for the development of new nanomedicines (Figure 2).
131 projects have been included in the present analysis. A mapping exercise demonstrated that the majority of projects addressed diseases such as cardiovascular diseases, neuropychiatric conditions, cancer and infectious/parasitic diseases with a high DALY value (see Figure 8). A breakdown analysis of the type of products shows a slight decrease of lipid based platforms in comparison to platforms that are in clinical trials or have been already authorised (see Figure 3). However, liposomes can be multifunctionalised by decorating them with targeting moieties, cell penetration proteins including small molecules and non coding RNAs, the inclusion of different kind of active principles as well as inorganic particles for imaging. The related therapeutic actions have been investigated by several consortia as shown in Figure 4. As such, liposomes must be still considered as an important platform in particular for malignant neoplasm and infectious diseases. In contrary to the lipid based carrier systems, the use of polymer based carrier systems and inorganic nanoparticle has strongly increased for diseases with a high DALY value as can be observed in Figure 9. In order to get a better understanding on the reason why inorganic particle currently receive so much attention in research activities, a more detailed analysis of the inorganic particles used in the R&D projects has been performed and the results are presented in Figure 10. It can be seen that the magnetic properties of the particle are in the focus of the therapeutic and diagnostic concepts. This physical parameter allows the development of in vivo imaging tools and therapies based on hyperthermia. Furthermore, magnetic nanoparticle should also used for innovative concepts like theranostics allowing the direct monitoring of therapeutic effects as well as diagnosis and therapeutic intervention simultaneously (see Figure 10).
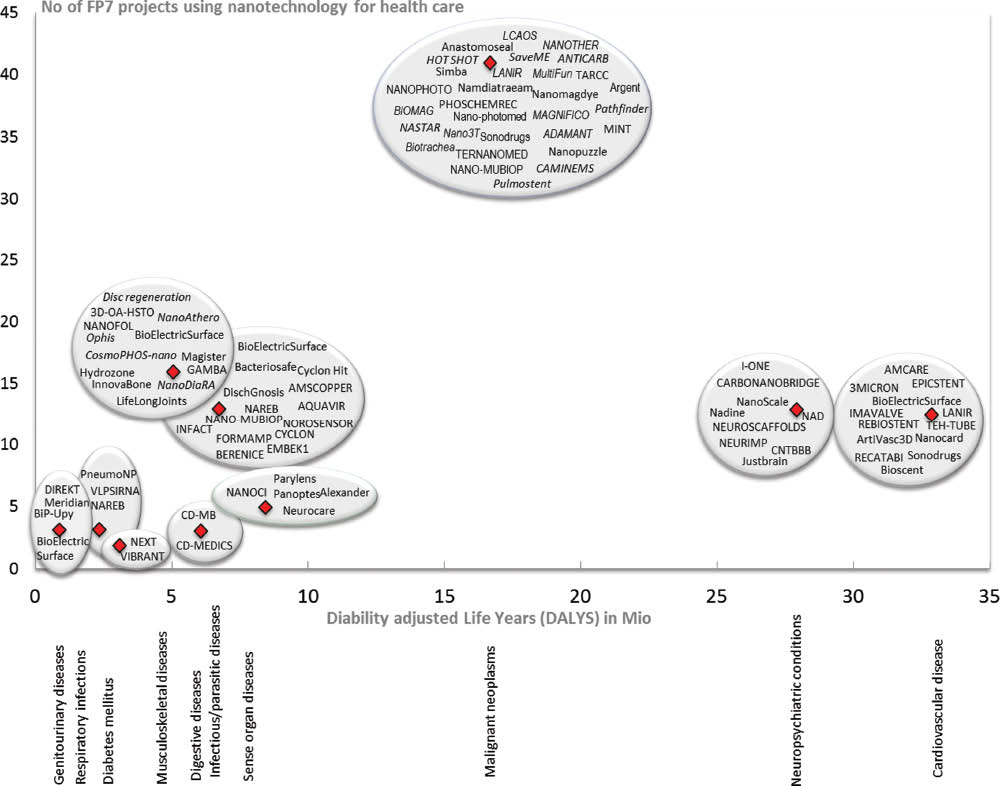
The burden of a disease on the European population in 2008 was measured in disability adjusted life years (DALYs). A DALY is an integrated single measure of mortality and disability due to a particular disease. One DALY represents a lost year of healthy living. This mapping exercise shows that a majority of FP7 projects address diseases contributing to a high value of DALY such as cancer, neuropsychiatric conditions and cardiovascular diseases.
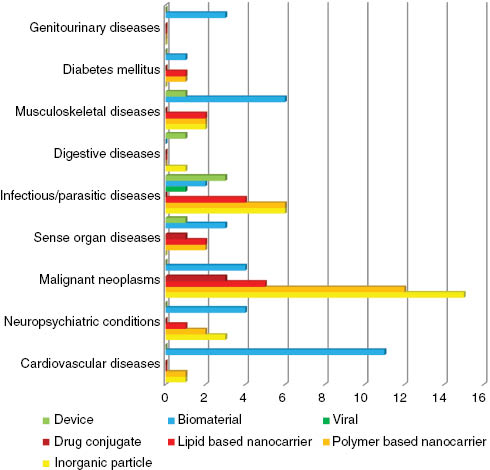
In the analysis biomaterials play a major role for adressing cardiovascular diseases whereas a drastic increase of inorganic material adressing maligne neoplasms can be observed. (*Status of published research activities in “Cordis” in March 2015.)
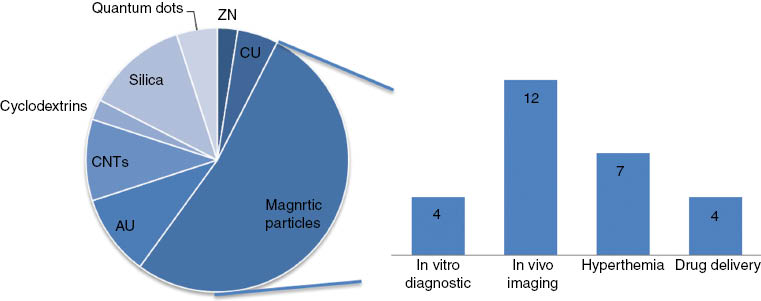
A breakdown of the inorganic material used for cancer applications demonstrated that magnetic nanoparticles such as magnetosomes produced by magnetoactic bacteria, supraparamagnetic nanoparticles, iron-platinum alloys, ferrites, magnetites and maghemites etc were the major contributor to the increase of using inorganic particle for the diagnostic/therapy of cancer. In particular, the possibility to use the magnetic property for in vivo imaging and hyperthemic applications is intensively studied within the projects. (*Status of published research activities in “Cordis” in March 2015.)
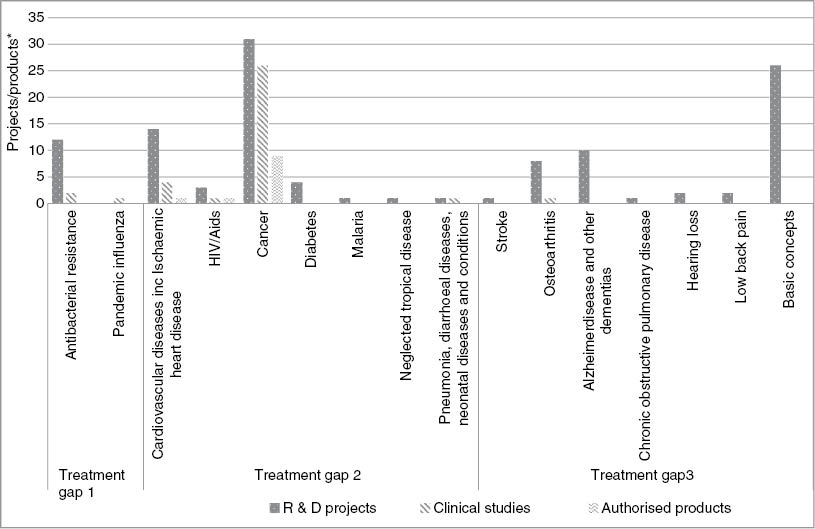
The majority of R&D projects address pharmaceutical gaps such as cancer, cardiovascular diseases including Ischemic heart disease and – to a lesser extent – the antibacterial resistance. Other priority diseases such as depression, tuberculosis, neglected tropical diseases, post haemorrhage, maternal mortality, acute stroke and rare diseases have not received so much attention in the FP7 projects on nanomedicines. However, a significant amount of projects addresses basic concepts that – once progressing in the technological development – might lead to a variety of therapeutic indications including the above mentioned priority diseases.
Discussion
Selection of the regulatory pathway
As already indicated a challenge for regulating nanomedicines is related to the selection of the regulatory pathway. Therapeutic and diagnostic agents can be either classified as medicinal products (15) or as medical devices (16) and this distinction is mostly based on the principal mode of action of the product. The principal intended action is achieved by physical means for medical devices and by pharmacological, immunological or metabolic means for medicinal products (see Table 2). However, sometimes the principal mode of action is blurry and nanomedicines can exhibit complex mechanisms involving mechanical, chemical, pharmacological and immunological mode of actions as seen for examples in the research activities of the projects such as “Nanother”, “NAD”, “Namdiatream” etc. Such borderline products are often subject of discussion in the Medical Devices Expert Group on Borderline and Classification (17). The uncertainty that is related to the regulation of such products has been addressed previously (18, 19) and the European Medicines Agency acknowledged the fact in its reflection paper on Nanotechnology based medicinal products for human use, that … many novel applications of nanotechnology will span the regulatory boundaries…. (20). The proposal of the European Commission on the medical device regulation is referring to nanomaterials and is requesting that …the manufacturer should take special care when using nanoparticles that can be released to the human body and those devices should be subject to the most severe conformity assessment procedure…. (21). As such the regulation of nanomedicines requires a close collaboration between the regulatory bodies and a harmonisation of information requirements and associated methods characterising the nanospecific properties of the product.
The definition of medicinal products vs. medical devices is crucial for the selection of the regulatory pathway and the authorisation process.
| Definition of the a medicinal product (Directive on medicinal products 2001/83/EC (15) |
| (a) Any substance or combination of substances presented as having properties for treating or preventing disease in human beings; or |
| (b) Any substance or combination of substances which may be used in or administered to human beings either with a view to restoring, correcting or modifying physiological functions by exerting a pharmacological, immunological or metabolic action, or to making a medical diagnosis. |
| And |
| Definition of a medical device (Directive on Medical Devices 93/42/EEC (16)a |
| “Any instrument, apparatus, appliance, software, material or other article, whether used alone or in combination, including the software intended by its manufacturer to be used specifically for diagnostic and/or therapeutic purposes and necessary for its proper application, intended by the manufacturer to be used for human beings for the purpose of: |
| – diagnosis, prevention, monitoring, treatment or alleviation of disease, |
| – diagnosis, monitoring, treatment, alleviation of or compensation for an injury or handicap, – investigation, replacement or modification of the anatomy or of a physiological process, |
| – control of conception, |
| and which does not achieve its principal intended action in or on the human body by pharmacological, immunological or metabolic means, but which may be assisted in its function by such means; |
aLegislation in revision: Proposal on medical devices (COM(2012)542) and a Proposal on in vitro diagnostic medical devices (COM(2012)541) which should revise the current regulatory framework for medical devices. Both regulations include a definition of nanomaterial taken from Commission Recommendation 2011/969/EU on the definition of nanomaterial and provisions on the risk classification, the labelling and the instructions for use of medical devices containing nanomaterial.
Assessment tools
The requested assessment procedures are directly linked to another challenge concering the evaluation of the nanospecific properties of the nanomedicine. As demonstrated by this study there is a trend towards sophisticated products using, e.g. chemical and biological functionalisations such as targeting moieties and proteins optimising drug release mechanisms. Other active nanostructures are designed to modify the behaviour depending on changes in their environment or a set of received signals (upon exposure to mechanical forces, electromagnetic radiation, pH and temperature changes, etc.). All these approaches can also be combined in complex multi-component nanomedicines. For such “next generation” nanotechnology-based products, the nanoscale size is still important, but above all the functional design of the nanomaterial matters and might pose new challenges, as risks may change as the material changes during therapeutic action. The regulation of such drugs therefore require the optimisation of existing tools for safety, efficacy and quality assessments or even the development and validation of new methods and testing strategies. Flexible validation strategies are needed as each product is unique and standard operation procedures for testing might need to be adapted to the various physical-chemical properties of the product and its functionalizations. Since no specific regulation in relation to nanomedicines exists, additional information with regard to the nanomaterial is requested on a case-by-case basis and creates an uncertainty for the product developer. Nevertheless, the regulatory community is well aware of that challenge and has started to provide guidances such as EMA’s reflection paper on the nanotechnology-based medicinal products for human use.
The European Commission’s Scientific Committee on Emerging and Newly Identified Health Risks (SCENIHR) released recently an opinion on the determination of potential health effects of nanomaterials used in medical devices (22). Furthermore, new initiatives such as the project EU-NCL financed within the European Commissions framework programme “Horizon 2020” will provide scientific/technical solutions and will develop new strategies for characterisation of advanced nanomedicine products.
Nanosimilars
The expiry of patents of the first nanomedicines will pose additional challenges since company will apply for marketing authorization of generic drugs (23). The first liposomal nanoformulations received their marketing authorisation in the late 1990s beginning or the beginning of the new century; e.g. Caelyx, one of the first nanomedicines, was authorised in 1996. A prominent example illustrating the regulatory challenge of so-called “nanosimilars” is the evaluation of doxorubicin SUN/Lipodox that is manufactured in India by SUN Pharma Global FZE. The product was authorised by the FDA but received a “not approvable” opinion from EMA’s Committee for Medicinal Products for Human use (CMPH). The CMPH had objections related to the clinical and preclinical evaluation (24). The US Nanocharacterisation Laboratory of the National Cancer Institute and the EU-NCL initiative might contribute to this harmonisation needs by developing cascades of advanced characterisation protocols to identify the possible difference between the nanosimilars and the original products.
Conclusion
Our analysis of 210 projects/products carried out for the reference period of 1996–2015 has led to the following conclusions
The authorised nanomedicines use mainly i) liposomes to reduce the toxic side effects of, e.g. well-established drugs and improve their bioavailability; ii) nanocrystals of active principles can improve challenging physical-chemical properties; iii) iron-oxides are used for the treatment of anemia. Only a small percentage of the authorised nanomedicines address pharmaceutical gaps as identified by the WHO. The main target disease is cancer.
Clinical trials in Europe are addressing a wider range of nanotechnology platforms including polymeric drugs and virosomes. However, the major target remains malignant neoplasms.
The FP7 Projects developed new therapeutic concepts and complex drugs that allow active targeting of the diseased tissue, the direct monitoring of the therapeutical success and/or the development of stimulus responsive drug delivery strategies.
Nanomedicines developed as part of the 7th Framework programme focus on “priority” diseases with no or insufficient treatments as well as diseases with a high influence on disability-adjusted live years (DALYS) such as neuropsychiatric, cardiovascular, respiratory diseases
Upcoming preclinical assessments of multifunctionalised nanomedicines as currently under development will include a specific nanocharacterisation step that eventually requires the development, optimisation and validation of new tools and testing strategies for quality and safety assessments (25). The EU-NCL will contribute to this demand by providing regulatory relevant methods addressing platforms and functionalisations that currently used in the development of new nanoformulations.
The current study can only elucidate trends. A deeper evaluation by complementing the data with other studies such as the “Bionest” report should provide a better understanding of what kind of knowledge and tools should be developed in order to prevent a possible delay in the authorisation process of needed drugs.
Nanomedicine can offer solutions for the identified pharmaceutical gaps and the development of new nanomedicines might be rewarding since the proportion of newly discovered chemical entities vs. the DALY burden are currently under-represented for several of the above mentioned diseases.
About the authors

Susanne Bremer-Hoffmann, Dr. rer nat, holds a PhD degree in Biology obtained from the Charite University Hospital Berlin in Germany for her work on the development of immunotherapies against leukemia. After post-doctoral research at the Federal Institute for Risk Assessment in Germany, Susanne joined the Institute for Health & Consumer Protection (IHCP) which is part of the Joint Research Centre (JRC) of the European Commission. Susanne became a team member of the European Centre for the Validation of Alternative Methods (ECVAM) in 1995 where she was involved in formal validation studies of toxicological in vitro tests detecting embryotoxicity and endocrine disruption and the regulatory acceptance of some tests at the OECD. She collaborated in several FP6 and FP 7 projects including the public/privat partnership initiative “SEURAT-1”. She contributed to more than 70 peer-reviewed scientific paper. In 2014 Susanne Bremer-Hoffmann joined the Nanobiosciences Unit of the same Institute and is currently participating in the establishment of the European Nanocharacterisation Laboratory.

Valeria Amenta holds a PhD in Supramolecular Chemistry from the University of Sheffield (UK), a Master’s degree in Pharmaceutical Chemistry and Technology and a master in Regulatory Disciplines of Medicines from the University of Catania (Italy). Her research has been focused on the synthesis of compounds that could potentially be used as a treatment for benign prostatic hyperplasia (Master’s degree research) and on the investigation of the effects of solvents on intermolecular interactions using UV-Vis and NMR techniques (PhD research). In 2012 she joined, as post-doctoral researcher, the Nanobiosciences Unit of Institute for Health & Consumer Protection (IHCP) at the European Commission’s Joint Research Centre (JRC), where she was involved in several projects and activities related to safety assessment and regulatory aspects of nanomaterials. Since November 2014 she works as scientific officer in the Substance Identity & Data Sharing Unit of the European Chemicals Agency (ECHA).

François Rossi studied Materials Science at Grenoble (DEng 1977) and obtained his PhD in 1989 from Université Claude Bernard in Lyon. After 2 years in industry in France and Germany, he joined the French Atomic Energy Commission (CEA) as R&D group leader in Nuclear Materials Engineering. He was then a guest scientist in Los Alamos National Laboratory USA in 1986–1987 (Center for Materials Science), and moved back to CEA in Grenoble “Advanced Technology Directorate” as section leader, working on Surface Engineering for Metallurgical Applications. In 1991, he moved to the JRC, Institute for Advanced Materials (IAM) in Petten where he was the manager of the Advanced Coating Centre. After his transfer to Ispra in 1996, he developed plasma based processes and surface modifications for metallurgical and biological applications. From 2002 to 2014, he has been the head of the JRC NanoBiotechnology laboratory in the JRC Institute for Health and Consumer Protection, managing a group of 35 scientists and students working on bio/non bio interfaces, nanobioscience and toxicology testing of nanomaterials. Since January 2014, he is the Scientific Coordinator of the NanoBioScience Unit. He is author and co-author of 260 peer reviewed articles (H-index 33), 12 book chapters, and 15 patents and has been involved in more than 25 RTD projects from FP3 to FP7.
Acknowledgments
The authors would like to thank Monica Diaz, European Medicines Agency and Heico Frima, EC-RTD for valuable suggestions and Kirsten Rasmussen, JRC for her contributions to improve the clarity of the manuscript.
References
1. Priority diseases and reasons for inclusions. In: Kaplan W, Wirtz VJW, Mantel-Teuiwisse A, Stolk P, Duthey B, Laing R, editors. Priority medicines for Europe and the World – 2013 Update. Geneve: WHO Library Cataloguing-in-Publication Data, 2013:67–165.Search in Google Scholar
2. Catalá-López F, García-Altés A, Álvarez-Martín E, Gènova-Maleras R, Morant-Ginestar C. Does the development of new medicinal products in the European Union address global and regional health concerns. Popul Health Metrics 2010;8:34.10.1186/1478-7954-8-34Search in Google Scholar PubMed PubMed Central
3. Community Research and Development Information Service. Cited 16.5.2015. Available from: http://cordis.europa.eu/home_en.html.Search in Google Scholar
4. Frima HJ, Gabellieri C, Nilsson MI. Drug delivery research in the European Union’s Seventh framework programme for research. J Control Release 2012;161:409–15.10.1016/j.jconrel.2012.01.044Search in Google Scholar PubMed
5. Etheridge ML, Campbell SA, ErdmanAG, Haynes CL. Wolf SM, De J, et al. The big picture on nanomedicine: the state of investigational and approved nanomedicine products. Nanomedicine 2013;9:1–14.10.1016/j.nano.2012.05.013Search in Google Scholar PubMed PubMed Central
6. Hafner A, Lakoš GP, Pepić I. Nanotherapeutics in the EU: an overview on current state and future directions. Int J Nanomed 2014;9:1005–1023.Search in Google Scholar
7. European Medicines Agency. EU Clinical Trials Register.1995-2015. cited 25.3.2015. Available from: https://www.clinicaltrialsregister.eu.Search in Google Scholar
8. European Medicines Ageny. Medicines. Cited 25.3.2015. Available from: http://www.ema.europa.eu/ema/index.jsp?curl=pages/includes/medicines/medicines_landing_page.jsp&mid=.Search in Google Scholar
9. Heads of Medicines Agencies. MRI product Index Cited 25.3.2015. Available from http://www.hma.eu/mriproductindex.html.Search in Google Scholar
10. European Medicines Agency and Heads of Medicines Agencies. EU Medicines Agencies Network Strategy to 2020. cited 23.4.2015. Available from: https://http://www.ema.europa.eu/docs/en_GB/document_library/Other/2015/03/WC500185138.pdf.Search in Google Scholar
11. Wicki WD, Balasubramanian V, Huwyler J. Nanomedicine in cancer therapy: challenges, opportunities, and clinical applications. J Control Release 2015;200:138–57.10.1016/j.jconrel.2014.12.030Search in Google Scholar PubMed
12. European Medicines Agency. Withdrawal assessment report for sinerem. Cited 25.3.2015. Available from: http://www.ema.europa.eu/docs/en_GB/document_library/Application_withdrawal_assessment_report/2010/01/WC500067463.pdf.Search in Google Scholar
13. Biotech LC. Applications des nanotechnologies à la médecine. Cited 25.3.2015. Available from: http://wwwetp-nanomedicineeu/public/press-documents/publications/public-documents/bionest-partners-2014-nanomedicine-study-leem/Rapport%20final%20version%20definitivepdf/view.Search in Google Scholar
14. European Commission. Technology readiness levels (TRL), HORIZON 2020 – WORK PROGRAMME 2014-2015 General Annexes, Extract from Part 19- Commision Decision C(2014)4995 Cited 25.3.2015. Available from: http://ec.europa.eu/research/participants/data/ref/h2020/wp/2014_2015/annexes/h2020-wp1415-annex-g-trl_en.pdf.Search in Google Scholar
15. European Parliament and Council. Directive 2001/83/EC of the European Parliament and of the Council of 6 November 2001 on the Community code relating to medicinal products for human use. Official Journal of the European Union 2001;L 311:0067–128.Search in Google Scholar
16. Council. Council Directive 93/42/EEC of 14 June 1993 concerning medical devices. Offical Journal of the European Union 1993; L 169:1–60.Search in Google Scholar
17. European Commission. Borderline and Classification issues. Cited 25.3.2015. Available from: http://ec.europa.eu/growth/sectors/medical-devices/documents/borderline/index_en.htm.Search in Google Scholar
18. Dorbeck-Jung CN. Is the European medical products authorisation regulation equipped to cope with the challenges of nanomedicines? Law Policy 2011;33:276–303.10.1111/j.1467-9930.2011.00339.xSearch in Google Scholar
19. Spyridoula P. Nanomedicine in Europe: Regulating under uncertainty. Thesis for Master Program in Law and Technology, Universiteit van Tilburg Master Thesis In Law and Technology. Cited 25.3.2015. Available from: http://arno.uvt.nl/show.cgi?fid=132431.Search in Google Scholar
20. European Medicines Agency. Reflection paper on nanotechnology-based medicinal products for human use. Cited 25.3.2015. Available from: http://www.ema.europa.eu/docs/en_GB/document_library/Regulatory_and_procedural_guideline/2010/01/WC500069728.pdf.Search in Google Scholar
21. European Commission. Proposal for a regulation of the European Parliament and of the Council on medical devices, and amending Directive 2001/83/EC, Regulation (EC) No 178/2002 and Regulation (EC) No 1223/2009 In: COM/2012/0542 final EUR-Lex; 2012. Cited 25.3.2015. Available from: http://ec.europa.eu/growth/sectors/medical-devices/documents/revision/files/revision_docs/proposal_2012_542_en.pdf.Search in Google Scholar
22. Scientific Committee on Emerging and Newly Identified Health Risks Guidance on the Determination of Potential Health Effects of Nanomaterials Used in Medical Devices opinion on the Guidance on the Determination of Potential Health Effects of Nanomaterials Used in Medical Devices. Cited 25.3.2015. Available from: http://ec.europa.eu/health/scientific_committees/emerging/docs/scenihr_o_045.pdf.Search in Google Scholar
23. Ehmann FS, Duncan R, Hernán Pérez de la Ossa D, Pita R, Vidal JM, Kohli A, et al. Next-generation nanomedicines and nanosimilars: EU regulators’ initiatives relating to the development and evaluation of nanomedicines. Nanomedicines 2013;8:849–56.10.2217/nnm.13.68Search in Google Scholar PubMed
24. European Medicines Agency. Doxorubicin SUN. Cited 25.3.2015. Available from: http://www.ema.europa.eu/ema/index.jsp?curl=pages/medicines/human/medicines/002049/wapp/Initial_authorisation/human_wapp_000122.jsp&mid=WC0b01ac058001d128.Search in Google Scholar
25. Khorasani AA Weaver JL, Salvador-Morales C. Closing the gap: accelerating the translational process in nanomedicine by proposing standardized characterization techniques. Int J Nanomed 2014;9:5729–51.Search in Google Scholar
26. European Technology Platform. Nanomedicine 2020 Contribution of Nanomedicine to Horizon 2020. cited 25.3.2015. Available from: http://www.etp-nanomedicine.eu/public/press-documents/publications/etpn-publications/etpn-white-paper-H2020.Search in Google Scholar
©2015 by De Gruyter
Articles in the same Issue
- Frontmatter
- In this issue
- News
- News from the European Foundation for Clinical Nanomedicine (CLINAM)
- What’s up in nanomedicine?
- Special Section Nanosafety
- Guest Editorial
- Sizing up the safety of nanomaterials
- Essay
- Keeping it small: towards a molecular definition of nanotoxicology
- Reviews
- The bio-corona and its impact on nanomaterial toxicity
- In vitro-ex vivo model systems for nanosafety assessment
- Meeting Report
- Nanosafety forum for young scientists: a meeting report
- Short Communication
- Nanomedicines in the European translational process
- Special Section CARPA Part 2
- Guest Editorial
- Complement activation-related pseudoallergy: an innate response to nanomedicines acting as pseudo-viruses
- Reviews
- Exosomes: potential model for complement-stealth delivery systems
- Lessons learned from the porcine CARPA model: constant and variable responses to different nanomedicines and administration protocols
- Mini Review
- Blood cell changes in complement activation-related pseudoallergy
- Short Communications
- Membrane attack complex formation on a supported lipid bilayer: initial steps towards a CARPA predictor nanodevice
- Paradoxical rise of hemolytic complement in the blood of mice during zymosan- and liposome-induced CARPA: a pilot study
- Commentary
- Insidious pathogen-mimicking properties of nanoparticles in triggering the lectin pathway of the complement system
Articles in the same Issue
- Frontmatter
- In this issue
- News
- News from the European Foundation for Clinical Nanomedicine (CLINAM)
- What’s up in nanomedicine?
- Special Section Nanosafety
- Guest Editorial
- Sizing up the safety of nanomaterials
- Essay
- Keeping it small: towards a molecular definition of nanotoxicology
- Reviews
- The bio-corona and its impact on nanomaterial toxicity
- In vitro-ex vivo model systems for nanosafety assessment
- Meeting Report
- Nanosafety forum for young scientists: a meeting report
- Short Communication
- Nanomedicines in the European translational process
- Special Section CARPA Part 2
- Guest Editorial
- Complement activation-related pseudoallergy: an innate response to nanomedicines acting as pseudo-viruses
- Reviews
- Exosomes: potential model for complement-stealth delivery systems
- Lessons learned from the porcine CARPA model: constant and variable responses to different nanomedicines and administration protocols
- Mini Review
- Blood cell changes in complement activation-related pseudoallergy
- Short Communications
- Membrane attack complex formation on a supported lipid bilayer: initial steps towards a CARPA predictor nanodevice
- Paradoxical rise of hemolytic complement in the blood of mice during zymosan- and liposome-induced CARPA: a pilot study
- Commentary
- Insidious pathogen-mimicking properties of nanoparticles in triggering the lectin pathway of the complement system