Influence of distinct social contexts of long-term care facilities on the dynamics of spread of COVID-19 under predefine epidemiological scenarios
-
Aditi Ghosh
 ,
Pradyuta Padmanabhan
,
Pradyuta Padmanabhan

Abstract
More than half of the coronavirus disease 19 (COVID-19) related mortality rates in the United States and Europe are associated with long-term-care facilities (LTCFs) such as old-age organizations, nursing homes, and disability centers. These facilities are considered most vulnerable to spread of an pandemic like COVID-19 because of multiple reasons including high density of elderly population with a diverse range of medical requirements, limited resources, nursing activities/medications, and the role of external visitors. In this study, we aim to understand the role of visitor’s family members and specific interventions (such as use of face masks and restriction of visiting hours) on the dynamics of infection in a community using a mathematical model. The model considers two types of social contexts (community and LTCFs) with three different groups of interacting populations (non-mobile community individuals, mobile community individuals, and long-term facility residents). The goal of this work is to compare the outbreak burden between different centre of disease control (CDC) planning scenarios, which capture distinct types of intensity of diseases spread in LTCF observed during COVID-19 outbreak. The movement of community mobile members is captured via their average relative times in and out of the long-term facilities to understand the strategies that would work well in these facilities the CDC planning scenarios. Our results suggest that heterogeneous mixing worsens epidemic scenario as compared to homogeneous mixing and the epidemic burden is hundreds times greater for community spread than within the facility population.
1 Introduction
Ever since the coronavirus disease 19 (COVID-19) pandemic first surfaced in the United States, the number of cases and deaths in nursing homes and other long-term care facilities (LTCFs) has been increasing. In 2020, it is reported that at minimum 28,100 residents and workers passed away from COVID-19 infection at nursing homes and other LTCFs for senior adults in the United States, according to a New York Times database. The number of infected cases was more than 153,000 at some 7,700 facilities [30]. In at least six states, senior residents in LTCF accounted for 50% or more of all COVID-19 deaths. New York Times mentioned that 11% of the cases in United States resulted from these facilities. The number of deaths due to COVID-19 in these facilities attributed to more than a third of the country’s pandemic fatalities [30]. States varied with known cases in LTCFs, with New Jersey (528) and Pennsylvania (539) topping the list, and New York (430), California (525), Washington (243), Maine (9), Iowa (32), and New Mexico (27), Alabama (5) reporting the lowest number of facilities [15,30]. Highest number of cases over 11,000 cases in LTCFs were reported in New Jersey of all the 29 states, [15]. Lesser than 100 cases were reported from South Dakota and Montana in these facilities [30].
The steady increase in deaths among LTCF residents due to COVID-19 had become an urgent concern for federal and state policymakers, LTCFs, family members of residents, and residents themselves [16]. Many residents and staff members in LTCF identified with COVID-19 were asymptomatic and pre-symptomatic and hence spread the disease very rapidly in the facility. During the period of March 29–April 10 at the Veterans affairs Greater Los Angeles Healthcare System, many residents, staff had positive test results for COVID-19. About 19% residents and 6% staff members tested positive for COVID-19 [18]. In a LTCF in King County, Washington, the hospitalization rates as of March 18 due to COVID-19 were 54.5, 50.0, and 6% for facility residents, visitors, and staff, respectively. The case fatality rate for residents was 33.7% [22]. The findings from [22] indicate that outbreak of COVID-19 in LTCFs had a significant impact on vulnerable older adults with pre-existing health conditions and local health care systems.
While young adults may not be likely to become infected severely by COVID-19 as older adults, there is evidence that the youth and the middle-aged can potentially play an important in preventing the spread of COVID-19, so the most vulnerable can be protected from getting sick. A study in 2020 [2,13,26,27] indicate that the hospitalization rate and death are more closely correlated with older people. The Centers for Medicare and Medicaid Services recently directed all LTCFs to significantly restrict visitors and non-essential personnel, as well as restrict communal activities inside LTCFs. The guidance that is based upon centre of disease control (CDC) recommendations directed LTCFs to restrict visitation except in certain compassionate cases, like end-of-life. In those cases, visitors were equipped with personal protective equipment such as masks, and the visit will be limited to a specific room only.
While such measures were directed a couple of years back, there are, however, still gaps in controls at LTCFs. Given that 1.3 million elderly adults live permanently in about 15,000 LTCFs nationwide with more than half over the age of 75, more coronavirus outbreaks are expected. Visitors and staff going to visit LTCFs may be carrying the virus and transmit to the elderly LTCFs residents who are highly susceptible to the virus. Similarly, those in the resident homes that have the virus have the potential to transfer the disease to the visitors as well. This is the motivation for this work [23,29].
A review of important contributions to the mathematical theory of epidemics can be found in several articles from the pioneering work of Fred Brauer [1,3–7,19]. The Kermack-Mckendrick compartmental model was considered as one of the earliest attempts to formulate a simple mathematical model to predict the spread of an infectious disease where the population being studied is divided into compartments, namely, a susceptible class
Goal of the study: There are multiple objectives of the study, including: (i) to develop and analyze a mathematical model that will integrate two groups of adult population, one that does not visit LTCFs and the other that visits LTCFs along with a group of older vulnerable residents of a LCTF; (ii) to understand the role of visitors of the residents in LTCFs and specific nonpharmaceutical interventions such as the use of face masks and restriction of visiting hours on the dynamics of infection in a community using the developed model; (iii) to capture and compare the five standard CDC scenarios to evaluate ongoing non-pharmaceutical interventions; and (iv) to study the role of population mixing assumptions that can capture changes in human behaviors. In order to study these objectives, two types of social contexts (community and LTCFs) are considered in the model along with three different groups of interacting populations (non-mobile community individuals, mobile community individuals that frequents LTCFs, and the residents there).
The rest of this article is divided as follows. Section 2 discusses the model formulation along with the mixing probabilities and basic reproductive number. We also implemented the CDC strategies in Section 2. Numerical results are discussed in Section 3 and conclusion in Section 4.
2 Models and background
2.1 Model description
In our model, we consider a city where we subdivide the population into three categories: individuals of the community that do not visit LTCF (Q), individuals from the community who visit a long-term care (T), and the LTCF residents (P). We refer to the members of Q and T population to be non-mobile and mobile individuals, respectively. The third group in our model includes LTCF residents (P) who will be referred to as senior members. The members of the sub-population of T are expected to interact with both sub-populations Q and P, respectively. Besides, disease can also be passed on through interaction within each sub-group as well (Figure 1).
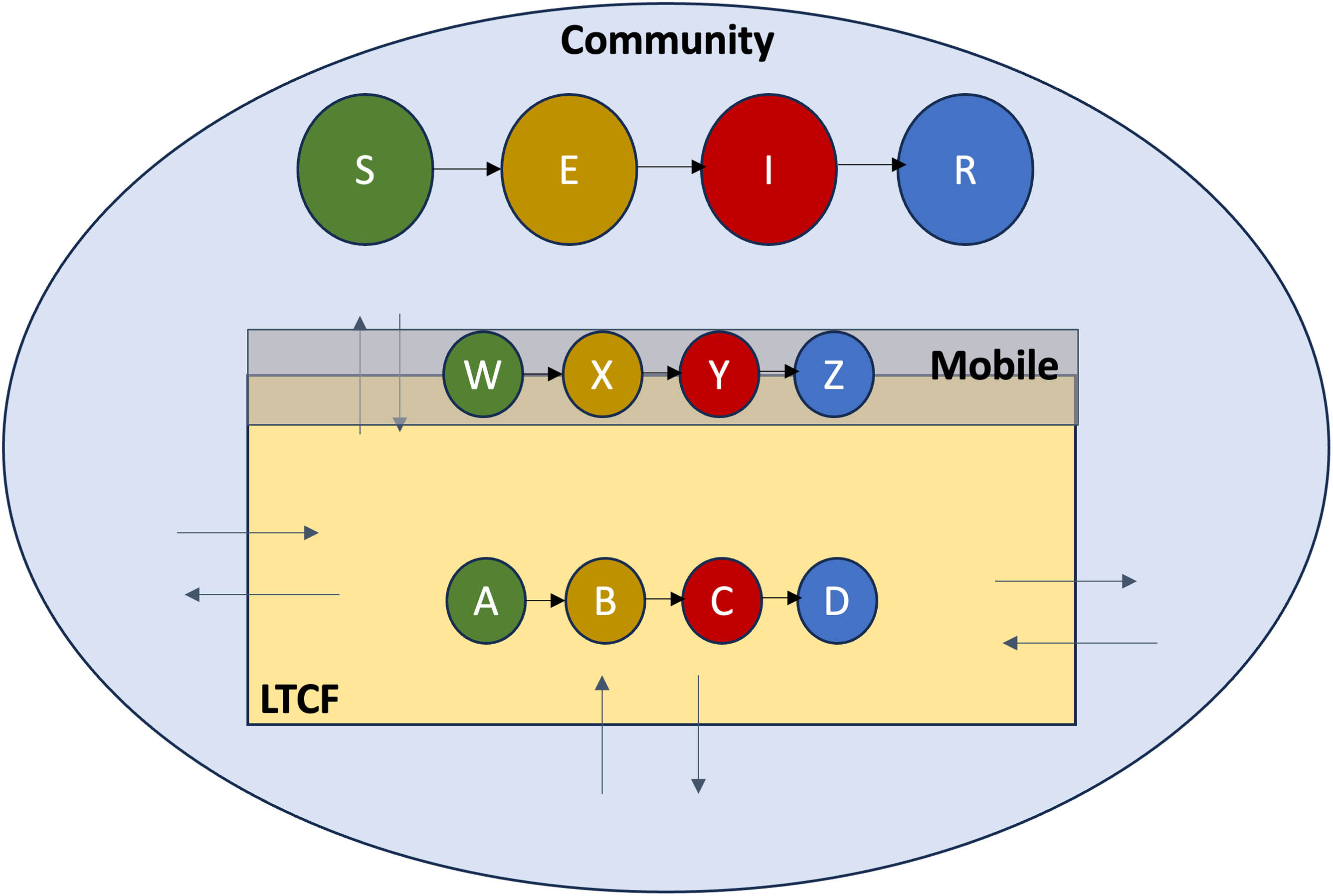
Model dynamics containing three sub-groups: non-mobile, mobile, and old-age home population.
Within each of the sub-groups, we use an S-E-I-R type model that denotes the respective susceptible, exposed (asymptomatic), infectious (symptomatic), and recovered. For our model, the Q sub-population is modeled using
Definition of the population states
| Variable | Definition |
|---|---|
|
|
Non-mobile population compartments |
|
|
Mobile (to old-age homes) population compartments |
|
|
Old-age home population compartments |
|
|
Susceptible population compartments |
|
|
Exposed population compartments (Infectious) |
|
|
Infected population compartments (Infectious) |
|
|
Recovered population compartments |
Let
Contact rates among the population
| Group | Type of people | Contacting who | |||
|---|---|---|---|---|---|
| contacted by | NM | M-NV | M-V | LCO | |
| I | NM |
|
|
0 | 0 |
| II | M-NV |
|
|
0 | 0 |
| M-V | 0 | 0 |
|
|
|
| III | LCO | 0 | 0 |
|
|
Let
Definition of mixing probabilities
| Mixing probability | Formula |
|---|---|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Note that the mixing probabilities satisfy the following identities:
Let
The governing differential equations for the non-mobile population system can then be described by:
The governing differential equations for the mobile (to old-age homes) population system can then be described by:
The governing differential equations for the old-age home population system can then be described by:
In these model equations, the total population corresponding to the non-mobile youth is
Parameters that are used and their definitions are given in Table 4.
Parameter and variable description
| Variable | Definition | Value |
|---|---|---|
|
|
(Probability given a contact) effectiveness of successful transmission of infection | 0.1 estimated |
|
|
Number of contacts of an individual in a three categories (non-mobile (Q), mobile (T) and individuals in old-age home (P), respectively) of populations | 0.48 |
|
|
Rate of self-isolation | (
|
|
|
Proportion of individuals that rigorously isolate (effectiveness of isolation)) | (0.5 |
|
|
Efficacy of the face mask worn by population Q | 0.5 varied |
|
|
Efficacy of the face mask worn by population T | 0.5 varied |
|
|
Efficacy of the face mask worn by population P | 0.8 varied |
|
|
Average asymptomatic period | (6.4 days) [21] |
|
|
Proportion of asymptomatic that self-heals | 0.81 |
|
|
Average symptomatic period | (7.6 days) (2–14) [14] |
|
|
Average mortality rate | 0.034 [14] |
|
|
0.25 | |
|
|
Fraction of mobile individuals that are in community | 0.93 [20,24,25] |
|
|
Fraction of mobile individuals that are in old-age homes and hence | 0.07 [20,24,25] |
|
|
Non-mobile population | 4,617 [20,24,25] |
|
|
Mobile (to old-age homes) population | 376 [25] |
|
|
Old-age home population | 480 [20,24,28] |
|
|
4,617 | |
|
|
0 | |
|
|
0 | |
|
|
0 | |
|
|
376 | |
|
|
0 | |
|
|
0 | |
|
|
0 | |
|
|
480 | |
|
|
1 | |
|
|
0 | |
|
|
0 |
3 Mathematical analysis
3.1 Basic reproduction number
Reproductive number plays an important role in determining the dynamics of spread of a disease. We use here a general approach called the next-generation matrix approach [10,12,17] to find the basic reproduction number
where
Along with
where
Next, we compute the Jacobian
Note that
where
The characteristic polynomial therefore is the following equation given by:
where
The basic reproduction number
where
where
where
Corollary 1. If the adults in the long-term care are fully protected with face-masks (
where
Corollary 2. If the adults in the long-term care are fully protected with face-masks (
Corollary 3. If the adults in the long-term care are fully protected with face-masks (
Note that this suggests that
or this yields a restriction on effective face mask efficacy for the non-mobile youth as follows:
4 Computational experiments
4.1 Model implementation on CDC strategies
We consider here five scenarios given by CDC and implement in our model to understand the strategies that work in favor for LTCFs. We estimate the contact rate
Scenario 1 [14]:
– Lower-bound values for virus transmissibility and disease severity
– Lower percentage of transmission prior to onset of symptoms
– Lower percentage of infections that never have symptoms and lower contribution of those cases to transmission
Scenario 2 [14]:
– Lower-bound values for virus transmissibility and disease severity
– Higher percentage of transmission prior to the onset of symptoms
– Higher percentage of infections that never have symptoms and higher contribution of those cases to transmission
Scenario 3 [14]:
– Upper-bound values for virus transmissibility and disease severity
– Lower percentage of transmission prior to onset of symptoms
– Lower percentage of infections that never have symptoms and lower contribution of those cases to transmission
Scenario 4 [14]:
– Upper-bound values for virus transmissibility and disease severity
– Higher percentage of transmission prior to onset of symptoms
– Higher percentage of infections that never have symptoms and higher contribution of those cases to transmission
Scenario 5 [14]:
– Parameter values for disease severity, viral transmissibility, and pre-symptomatic and asymptomatic disease transmission represent the best estimate, based on the latest surveillance data and scientific knowledge.
For these five scenarios, the values of
Five planning CDC scenarios
| CDC planning scenarios | ||||
|---|---|---|---|---|
| Scenario 1 | Scenario 2 | Scenario 3 | Scenario 4 | Scenario 5 |
| Lower-bound values for virus transmissibility and disease severity | Lower-bound values for virus transmissibility and disease severity | Upper-bound values for virus transmissibility and disease severity | Upper-bound values for virus transmissibility and disease severity | Parameter values for disease severity, viral transmissibility, and pre-symptomatic and asymptomatic disease transmission that represent the best estimate, based on the latest surveillance data and scientific knowledge. |
| Lower percentage of transmission prior to onset of symptoms | Higher percentage of transmission prior to onset of symptoms | Lower percentage of transmission prior to onset of symptoms | Higher percentage of transmission prior to onset of symptoms | |
| Lower percentage of infections that never have symptoms and lower contribution of those cases to transmission | Higher percentage of infections that never have symptoms and higher contribution of those cases to transmission | Lower percentage of infections that never have symptoms and lower contribution of those cases to transmission | Higher percentage of infections that never have symptoms and higher contribution of those cases to transmission | |
Parameter values for different CDC scenarios
| Parameter values | ||||||
|---|---|---|---|---|---|---|
| Parameters | Baseline | Scenario 1 | Scenario 2 | Scenario 3 | Scenario 4 | Scenario 5 |
|
|
5 | 2.88 | 3.17 | 4.5 | 4.89 | 3.43 |
|
|
5 | 2.88 | 3.17 | 4.5 | 4.89 | 3.43 |
|
|
5.42 | 4.32 | 4.76 | 6.75 | 7.34 | 5.15 |
|
|
4.58 | 1.44 | 1.56 | 2.25 | 2.45 | 1.72 |
The baseline case, defined to reflect early COVID-19 outbreak when interventions were yet to be initiated, is also considered in this analysis. The model parameter estimates for the baseline case were obtained from reference [26] and are collected in Table 6.
4.2 Numerical results
Using our model, we simulate the five scenarios given by CDC in Table 5 to understand and compare the dynamics of COVID-19 in LTCFs under different control strategies. We study the model for 30 days (to capture single outbreak burden) for the population of LTCF residents and visitors to the residents and non-visitors based on parameter estimates given in Table 6.
We divide the section into four subcases of the model describing different modeling assumptions on mixing and mortality. For each subcases, we simulate all the five scenarios. The cases are as follows:
negligible disease mortality rate, proportional mixing population, and constant total population
negligible disease mortality rate, heterogeneous mixing population, and constant total population
high disease mortality rate and proportional mixing population
high disease mortality rate, heterogeneous mixing population, and variable community population size.
Proportional mixing Case 1 for five different CDC scenarios applied after 30 days in comparison with baseline (without deaths)
| Proportional mixing (without deaths) | ||||||
|---|---|---|---|---|---|---|
| Parameters | Baseline | Scenario 1 | Scenario 2 | Scenario 3 | Scenario 4 | Scenario 5 |
|
|
3.2969 | 2.6473 | 2.7205 | 3.0493 | 3.1448 | 2.7853 |
| Non-visitors | ||||||
| Peak value | 0.1466 | 0.0008 | 0.0016 | 0.0993 | 0.1398 | 0.0074 |
| Peak time | 104 | 68 | 146 | 122 | 108 | 180 |
| Epidemic size | 0.6255 | 0.0066 | 0.0158 | 0.5106 | 0.6131 | 0.0426 |
| Visitors | ||||||
| Peak value | 0.1119 | 0.0022 | 0.0026 | 0.0939 | 0.1329 | 0.0069 |
| Peak time | 105 | 47 | 51 | 123 | 108 | 180 |
| Epidemic size | 0.5200 | 0.0130 | 0.0227 | 0.4982 | 0.6009 | 0.0491 |
| LTCF members | ||||||
| Peak value | 0.2101 | 0.0339 | 0.0330 | 0.0343 | 0.0350 | 0.0332 |
| Peak time | 68 | 31 | 30 | 35 | 46 | 30 |
| Epidemic size | 0.8118 | 0.0931 | 0.1017 | 0.2339 | 0.2997 | 0.11487 |
Heterogeneous Case 2 for five different CDC scenarios applied after 30 days in comparison with baseline (without deaths)
| Heterogeneous mixing (without deaths) | ||||||
|---|---|---|---|---|---|---|
| Parameters | Baseline | Scenario 1 | Scenario 2 | Scenario 3 | Scenario 4 | Scenario 5 |
|
|
3.2969 | 2.6473 | 2.7205 | 3.0493 | 3.1448 | 2.7853 |
| Non-visitors | ||||||
| Peak value | 0.4461 | 0.1373 | 0.1874 | 0.3791 | 0.4224 | 0.2304 |
| Peak time | 62 | 109 | 95 | 68 | 64 | 86 |
| Epidemic size | 0.9219 | 0.6079 | 0.6941 | 0.8825 | 0.9089 | 0.7502 |
| Visitors | ||||||
| Peak value | 0.4287 | 0.1619 | 0.2175 | 0.4195 | 0.4636 | 0.2641 |
| Peak time | 62 | 107 | 94 | 66 | 63 | 85 |
| Epidemic size | 0.9067 | 0.7126 | 0.7935 | 0.9420 | 0.9587 | 0.8423 |
| LTCF members | ||||||
| Peak value | 0.4077 | 0.3437 | 0.3439 | 0.3563 | 0.3571 | 0.3545 |
| Peak time | 36 | 30 | 30 | 31 | 31 | 31 |
| Epidemic size | 0.9198 | 0.6157 | 0.6337 | 0.7238 | 0.7456 | 0.6637 |
Proportional mixing Case 3 for five different CDC scenarios applied after 30 days in comparison with baseline (with deaths)
| Proportional mixing (with deaths) | ||||||
|---|---|---|---|---|---|---|
| Parameters | Baseline | Scenario 1 | Scenario 2 | Scenario 3 | Scenario 4 | Scenario 5 |
|
|
3.2969 | 2.6473 | 2.7205 | 3.0493 | 3.1448 | 2.7853 |
| Non-visitors | ||||||
| Peak value | 0.1325 | 0.0002 | 0.0003 | 0.0908 | 0.1290 | 0.00204 |
| Peak time | 121 | 44 | 180 | 143 | 123 | 180 |
| Epidemic size | 0.5323 | 0.0013 | 0.0032 | 0.4021 | 0.5225 | 0.0093 |
| Deaths | 0.0788 | 0.0002 | 0.0005 | 0.0591 | 0.0774 | 0.0014 |
| Visitors | ||||||
| Peak value | 0.1010 | 0.0004 | 0.0004 | 0.0862 | 0.1230 | 0.0018 |
| Peak time | 122 | 37 | 40 | 144 | 124 | 180 |
| Epidemic size | 0.4158 | 0.0018 | 0.0037 | 0.3824 | 0.5007 | 0.0094 |
| Deaths | 0.0616 | 0.0003 | 0.0005 | 0.0562 | 0.0741 | 0.0014 |
| LTCF members | ||||||
| Peak value | 0.0429 | 0.0083 | 0.0085 | 0.0086 | 0.0087 | 0.00855 |
| Peak time | 104 | 30 | 31 | 31 | 31 | 31 |
| Epidemic size | 0.1584 | 0.0095 | 0.0100 | 0.0199 | 0.0267 | 0.0105 |
| Deaths | 0.3010 | 0.0180 | 0.0191 | 0.0379 | 0.0507 | 0.0199 |
Heterogeneous mixing Case 4 for five different CDC scenarios applied after 30 days in comparison with baseline (with deaths)
| Heterogeneous mixing (with deaths) | ||||||
|---|---|---|---|---|---|---|
| Parameters | Baseline | Scenario 1 | Scenario 2 | Scenario 3 | Scenario 4 | Scenario 5 |
|
|
3.2969 | 2.6473 | 2.7205 | 3.0493 | 3.1448 | 2.7853 |
| Non-visitors | ||||||
| Peak value | 0.4283 | 0.1281 | 0.1758 | 0.3621 | 0.4048 | 0.2170 |
| Peak time | 64 | 114 | 100 | 70 | 66 | 91 |
| Epidemic size | 0.8027 | 0.5271 | 0.6039 | 0.7684 | 0.7914 | 0.65313 |
| Deaths | 0.1192 | 0.0782 | 0.0897 | 0.1141 | 0.1175 | 0.0970 |
| Visitors | ||||||
| Peak value | 0.4133 | 0.1519 | 0.2052 | 0.4030 | 0.4468 | 0.25028 |
| Peak time | 64 | 112 | 98 | 69 | 65 | 89 |
| Epidemic size | 0.7883 | 0.6170 | 0.6895 | 0.8197 | 0.8344 | 0.7324 |
| Deaths | 0.1171 | 0.0915 | 0.1024 | 0.1218 | 0.1239 | 0.1088 |
| LTCF members | ||||||
| Peak value | 0.2547 | 0.2159 | 0.2139 | 0.2124 | 0.2136 | 0.2118 |
| Peak time | 36 | 31 | 30 | 30 | 31 | 30 |
| Epidemic size | 0.2934 | 0.1673 | 0.1708 | 0.1959 | 0.2052 | 0.17425 |
| Deaths | 0.5575 | 0.3179 | 0.3244 | 0.3723 | 0.3899 | 0.3310 |
The dynamics of the non-visitors, visitors, and LTCF members for the five CDC scenarios applied after 30 days compared with baseline are shown for proportional mixing without deaths (Figure 2, i.e., Case 1), heterogeneous mixing without deaths (Figure 3, i.e., Case 2), proportional mixing with deaths (Figure 4, i.e., Case 3), and heterogeneous mixing with deaths (Figure 5, i.e., Case 4).

Dynamics of the non-visitors, visitors, and LTCF members for five CDC scenarios applied after 30 days compared with baseline for proportional mixing without deaths.

Dynamics of the non-visitors, visitors, and LTCF members for five CDC scenarios applied after 30 days compared with baseline for heterogeneous mixing without deaths.

Dynamics of the non-visitors, visitors, and LTCF members for five CDC scenarios applied after 30 days compared with baseline for proportional mixing with deaths.

Dynamics of the non-visitors, visitors, and LTCF members for five CDC scenarios applied after 30 days compared with baseline for heterogeneous mixing with deaths.
We observe that heterogeneous mixing population makes epidemic worse as compared to epidemic size in homogeneous mixing population. Moreover, in the heterogeneous mixing population, the epidemic burden is about 100 times more for community members (visitors and non-visitors) than for the LTCF population. That is, under heterogeneous mixing situation, which may occur due to continuous changes in the population behaviors, can create worse epidemic and particularly for long term care residents, with respect to metrics considered in this study.
Strategies 1, 2, and 5 result in almost similar burden and are the best followed by Strategy 3, whereas Strategy 4 is the worst among all the strategies. This statement is true for both homogeneous and heterogeneous mixing population. Figure 6 shows the influence of face masks on

Influence of face mask on
5 Discussion
The role of LTCFs population is important for understanding outbreak of COVID-19 in the community. This is because the rate of spread could be high in LTCF as it consists of vulnerable adults with pre-existing health conditions and compromised immune system. The infectious disease model capturing mixing strategies of populations interacting with residents is thus one of the powerful methods to quickly understand the dynamics of disease spread.
We consider here two types of social contexts (community and LTCFs) and three different groups of interacting populations (non-mobile individuals in the community who do not visit LTCFs, mobile individuals in the community who visit LTCFs, and residents of LTCFs). We use a susceptible-exposed-infectious-recovered-type model within each sub-group and define mixing probabilities to understand the strategies that would work well in these facilities for five different CDC planning scenarios. Here, we aim to identify and quantify the roles of different subpopulations (residents, visitors, non-visitors) and the mixing strategies associated with them to better control COVID-19 in these facilities.
Our results suggest that heterogeneous mixing worsens the epidemic as compared to homogeneous mixing: the epidemic burden is hundreds of times greater for community spread (between visitors and non-visitors) than within the facility population. In both mixing scenarios, CDC Strategies 1, 2, and 5 have similarly best outcomes, followed by Strategies 3 and 4 is the worst approach. We also studied the influence of face mask on
Due to the lack of comprehensive data, the study considered only aggregated estimates from multiple unrelated studies. However, the impact of parameter estimates on the results captured uncertainty associated with key model parameters. Limited epidemiological scenarios were considered that capture situations in the United States only.
In the future, we would like to exercise this model with more data-extensive work that will incorporate explicit human behaviors through mixing empirical studies. Extension of the model can be considered that will require epidemiological states such as states consisting of individuals who are vaccinated and/or under other interventions.
Acknowledgments
We certify that the submission is original work and is not under review at any other publication.
-
Funding information: All co-authors have seen and agree with the contents of the manuscript, and there is no financial interest to report.
-
Author contributions: All authors contributed equally to this work.
-
Conflict of interest: The authors have no conflicts of interest to declare.
Appendix
We compute the Jacobian
and the Jacobian
Using matrices
References
[1] Ajbar, A., Alqahtani, R. T., & Boumaza, M. (2021). Dynamics of an SIR-based COVID-19 model with linear incidence rate, nonlinear removal rate, and public awareness. Frontiers in Physics, 9, 13. doi: 10.3389/fphy.2021.634251. Search in Google Scholar
[2] Akman, O., Chauhan, S., Ghosh, A., Liesman, S., Michael, E., Mubayi, A., …, Tripathi, J. P. (2022). The hard lessons and shifting modeling trends of COVID-19 dynamics: Multiresolution modeling approach. Bulletin of Mathematical Biology, 84, 1–30. 10.1007/s11538-021-00959-4Search in Google Scholar PubMed PubMed Central
[3] Brauer, F. (1990). Models for the spread of universally fatal diseases. Journal of Mathematical Biology, 28(4), 451–462. 10.1007/BF00178328Search in Google Scholar PubMed
[4] Brauer, F. (2005). The Kermack-McKendrick epidemic model revisited. Mathematical Biosciences, 198(2), 119–131. 10.1016/j.mbs.2005.07.006Search in Google Scholar PubMed
[5] Brauer, F. (2006). Some simple epidemic models. Mathematical Biosciences & Engineering, 3(1), 1. 10.3934/mbe.2006.3.1Search in Google Scholar PubMed
[6] Brauer, F. (2008). Age-of-infection and the final size relation. Mathematical Biosciences & Engineering, 5(4), 681. 10.3934/mbe.2008.5.681Search in Google Scholar PubMed
[7] Brauer, F., Castillo-Chavez, C., & Castillo-Chavez, C. (2012). Mathematical models in population biology and epidemiology (Vol. 2, p. 508). New York: Springer. 10.1007/978-1-4614-1686-9Search in Google Scholar
[8] Brauer, F., Castillo-Chavez, C., & Feng, Z. (2019). Mathematical models in epidemiology (Vol. 32). New York: Springer. 10.1007/978-1-4939-9828-9Search in Google Scholar
[9] Busenberg, S., & Castillo-Chavez, C. (1991). A general solution of the problem of mixing of subpopulations and its application to risk-and age-structured epidemic models for the spread of AIDS. Mathematical Medicine and Biology: A Journal of the IMA, 8(1), 1–29. 10.1093/imammb/8.1.1Search in Google Scholar PubMed
[10] Castillo-Chavez, C., Cooke, K., Huang, W., & Levin, S. A. (1989). The role of long periods of infectiousness in the dynamics of acquired immunodeficiency syndrome (AIDS). In: Mathematical Approaches to Problems in Resource Management and Epidemiology (pp. 177–189). Berlin, Heidelberg: Springer. 10.1007/978-3-642-46693-9_14Search in Google Scholar
[11] Castillo-Chavez, C., Song, B., & Zhang, J. (2003). An epidemic model with virtual mass transportation: The case of smallpox in a large city. In: Bioterrorism: Mathematical Modeling Applications in Homeland Security (pp. 173–197). Society for Industrial and Applied Mathematics. Germany: Springer International Publishing Berlin.10.1137/1.9780898717518.ch8Search in Google Scholar
[12] Castillo-Chavez, C., Velasco-Hernandez, J. X., & Fridman, S. (1994). Modeling contact structures in biology. In Frontiers in Mathematical Biology (pp. 454–491). Berlin, Heidelberg: Springer. 10.1007/978-3-642-50124-1_27Search in Google Scholar
[13] CDC COVID-19 Response Team, CDC COVID-19 Response Team, CDC COVID-19 Response Team, Bialek, S., Boundy, E., Bowen, V., Chow, N., Cohn, A., Dowling, N., …, Gierke, R. (2020). Severe outcomes among patients with coronavirus disease 2019 (COVID-19)-?United States, February 12-March 16, 2020. Morbidity and Mortality Weekly Report, 69(12), 343–346. 10.15585/mmwr.mm6912e2Search in Google Scholar PubMed PubMed Central
[14] COVID-19 Pandemic Planning Scenarios, Uniform Resource Locator: https://www.cdc.gov/coronavirus/2019-ncov/hcp/planning-scenarios.html. 2021. Search in Google Scholar
[15] Chidambaram P. (2020). https://www.kff.org/coronavirus-covid-19/issue-brief/state-reporting-of-cases-and-deaths-due-to-covid-19-in-long-term-care-facilities/. Search in Google Scholar
[16] Comas-Herrera, A., Zalakaín, J., Lemmon, E., Henderson, D., Litwin, C., Hsu, A. T., …, Fernández, J. L. (2020). Mortality associated with COVID-19 in care homes: International evidence. Article in LTCcovid.org, International Long-term Care Policy Network, CPEC-LSE, 14. Search in Google Scholar
[17] Diekmann, O., Heesterbeek, J. A. P., & Metz, J. A. (1990). On the definition and the computation of the basic reproduction ratio R 0 in models for infectious diseases in heterogeneous populations. Journal of Mathematical Biology, 28(4), 365–382. 10.1007/BF00178324Search in Google Scholar PubMed
[18] Dora, A. V., Winnett, A., Jatt, L. P., Davar, K., Watanabe, M., Sohn, L., …, Goetz, M. B., (2020). Universal and serial laboratory testing for SARS-CoV-2 at a long-term care skilled nursing facility for veterans-?Los Angeles, California, 2020. Morbidity and Mortality Weekly Report, 69(21), 651. 10.15585/mmwr.mm6921e1Search in Google Scholar PubMed PubMed Central
[19] Kimball, A., Hatfield, K. M., Arons, M., James, A., Taylor, J., Spicer, K., …, Bell, J. M. (2020). Asymptomatic and presymptomatic SARS-CoV-2 infections in residents of a long-term care skilled nursing facility-?King County, Washington, March 2020. Morbidity and Mortality Weekly Report, 69(13), 377. 10.15585/mmwr.mm6913e1Search in Google Scholar PubMed PubMed Central
[20] King County, Update: King County COVID-19 case numbers for March 6, 2020, kingcounty.gov, 2020. Search in Google Scholar
[21] Lauer, S. A., Grantz, K. H., Bi, Q., Jones, F. K., Zheng, Q., Meredith, H. R., …, Lessler, J. (2020). The incubation period of coronavirus disease 2019 (COVID-19) from publicly reported confirmed cases: Estimation and application. Annals of Internal Medicine, 172(9), 577–582. 10.7326/M20-0504Search in Google Scholar PubMed PubMed Central
[22] McMichael, T. M., Currie, D. W., Clark, S., Pogosjans, S., Kay, M., Schwartz, N. G., …, Ferro, J. (2020). Epidemiology of COVID-19 in a long-term care facility in King County, Washington. New England Journal of Medicine, 382(21), 2005–2011. 10.1056/NEJMoa2005412Search in Google Scholar PubMed PubMed Central
[23] Nuño, M., Reichert, T. A., Chowell, G., & Gumel, A. B. (2008). Protecting residential care facilities from pandemic influenza. Proceedings of the National Academy of Sciences, 105(30), 10625–10630. 10.1073/pnas.0712014105Search in Google Scholar PubMed PubMed Central
[24] Pare, M. (2020). Five coronavirus deaths at Washington facility belonging to Cleveland, Tennessee, company. https://www.timesfreepress.com/news/2020/mar/02/cleveland-tennessee-based-life-care-centers-americ/. Search in Google Scholar
[25] Population of South Juanita, Kirkland, Washington, Statisticalatlas.com/neighborhood/Washington/Kirkland/South-Juanita/Population, Statistical Atlas, 2020. Search in Google Scholar
[26] Rojas, J. H., Paredes, M., Banerjee, M., Akman, O., & Mubayi, A. (2022). Mathematical modeling and dynamics of SARS-CoV-2 in Colombia. Letters in Biomathematics, 9(1), 41–56. Search in Google Scholar
[27] Saade, M., Ghosh, S., Banerjee, M., & Volpert, V. (2023). An epidemic model with time delays determined by the infectivity and disease durations. Mathematical Biosciences and Engineering, 20(7), 12864–12888. 10.3934/mbe.2023574Search in Google Scholar PubMed
[28] Sacchetti, M., Nguyen, A., & Kirkland, W. (2020). Becomes epicenter of coronavirus response as cases spread. Washington Post. Search in Google Scholar
[29] Worldometer, D. (2020). COVID-19 coronavirus pandemic. World Health Organization. www.worldometers.info. Search in Google Scholar
[30] Yourish, K., Rebecca Lai, K. K., Ivory, D., & Smith, M. (2020). Home residents or workers. The NewYork Times. Search in Google Scholar
© 2023 the author(s), published by De Gruyter
This work is licensed under the Creative Commons Attribution 4.0 International License.
Articles in the same Issue
- Special Issue: Infectious Disease Modeling In the Era of Post COVID-19
- A comprehensive and detailed within-host modeling study involving crucial biomarkers and optimal drug regimen for type I Lepra reaction: A deterministic approach
- Application of dynamic mode decomposition and compatible window-wise dynamic mode decomposition in deciphering COVID-19 dynamics of India
- Role of ecotourism in conserving forest biomass: A mathematical model
- Impact of cross border reverse migration in Delhi–UP region of India during COVID-19 lockdown
- Cost-effective optimal control analysis of a COVID-19 transmission model incorporating community awareness and waning immunity
- Evaluating early pandemic response through length-of-stay analysis of case logs and epidemiological modeling: A case study of Singapore in early 2020
- Special Issue: Application of differential equations to the biological systems
- An eco-epidemiological model with predator switching behavior
- A numerical method for MHD Stokes model with applications in blood flow
- Dynamics of an eco-epidemic model with Allee effect in prey and disease in predator
- Optimal lock-down intensity: A stochastic pandemic control approach of path integral
- Bifurcation analysis of HIV infection model with cell-to-cell transmission and non-cytolytic cure
- Special Issue: Differential Equations and Control Problems - Part I
- Study of nanolayer on red blood cells as drug carrier in an artery with stenosis
- Influence of incubation delays on COVID-19 transmission in diabetic and non-diabetic populations – an endemic prevalence case
- Complex dynamics of a four-species food-web model: An analysis through Beddington-DeAngelis functional response in the presence of additional food
- A study of qualitative correlations between crucial bio-markers and the optimal drug regimen of Type I lepra reaction: A deterministic approach
- Regular Articles
- Stochastic optimal and time-optimal control studies for additional food provided prey–predator systems involving Holling type III functional response
- Stability analysis of an SIR model with alert class modified saturated incidence rate and Holling functional type-II treatment
- An SEIR model with modified saturated incidence rate and Holling type II treatment function
- Dynamic analysis of delayed vaccination process along with impact of retrial queues
- A mathematical model to study the spread of COVID-19 and its control in India
- Within-host models of dengue virus transmission with immune response
- A mathematical analysis of the impact of maternally derived immunity and double-dose vaccination on the spread and control of measles
- Influence of distinct social contexts of long-term care facilities on the dynamics of spread of COVID-19 under predefine epidemiological scenarios
Articles in the same Issue
- Special Issue: Infectious Disease Modeling In the Era of Post COVID-19
- A comprehensive and detailed within-host modeling study involving crucial biomarkers and optimal drug regimen for type I Lepra reaction: A deterministic approach
- Application of dynamic mode decomposition and compatible window-wise dynamic mode decomposition in deciphering COVID-19 dynamics of India
- Role of ecotourism in conserving forest biomass: A mathematical model
- Impact of cross border reverse migration in Delhi–UP region of India during COVID-19 lockdown
- Cost-effective optimal control analysis of a COVID-19 transmission model incorporating community awareness and waning immunity
- Evaluating early pandemic response through length-of-stay analysis of case logs and epidemiological modeling: A case study of Singapore in early 2020
- Special Issue: Application of differential equations to the biological systems
- An eco-epidemiological model with predator switching behavior
- A numerical method for MHD Stokes model with applications in blood flow
- Dynamics of an eco-epidemic model with Allee effect in prey and disease in predator
- Optimal lock-down intensity: A stochastic pandemic control approach of path integral
- Bifurcation analysis of HIV infection model with cell-to-cell transmission and non-cytolytic cure
- Special Issue: Differential Equations and Control Problems - Part I
- Study of nanolayer on red blood cells as drug carrier in an artery with stenosis
- Influence of incubation delays on COVID-19 transmission in diabetic and non-diabetic populations – an endemic prevalence case
- Complex dynamics of a four-species food-web model: An analysis through Beddington-DeAngelis functional response in the presence of additional food
- A study of qualitative correlations between crucial bio-markers and the optimal drug regimen of Type I lepra reaction: A deterministic approach
- Regular Articles
- Stochastic optimal and time-optimal control studies for additional food provided prey–predator systems involving Holling type III functional response
- Stability analysis of an SIR model with alert class modified saturated incidence rate and Holling functional type-II treatment
- An SEIR model with modified saturated incidence rate and Holling type II treatment function
- Dynamic analysis of delayed vaccination process along with impact of retrial queues
- A mathematical model to study the spread of COVID-19 and its control in India
- Within-host models of dengue virus transmission with immune response
- A mathematical analysis of the impact of maternally derived immunity and double-dose vaccination on the spread and control of measles
- Influence of distinct social contexts of long-term care facilities on the dynamics of spread of COVID-19 under predefine epidemiological scenarios