
Effect of expectation on pain assessment of lower- and higher-intensity stimuli
-
Valentina Ružić
 ,
Dragutin Ivanec
,
Dragutin Ivanec

Abstract
Background and aims
Pain modulation via expectation is a well-documented phenomenon. So far it has been shown that expectations about effectiveness of a certain treatment enhance the effectiveness of different analgesics and of drug-free pain treatments. Also, studies demonstrate that people assess same-intensity stimuli differently, depending on the experimentally induced expectations regarding the characteristics of the stimuli. Prolonged effect of expectation on pain perception and possible symmetry in conditions of lower- and higher-intensity stimuli is yet to be studied. Aim of this study is to determine the effect of expectation on the perception of pain experimentally induced by the series of higher- and lower-intensity stimuli.
Methods
192 healthy participants were assigned to four experimental groups differing by expectations regarding the intensity of painful stimuli series. Expectations of two groups were congruent with actual stimuli; one group expected and received lower-intensity stimuli and the other expected and received higher-intensity stimuli. Expectations of the remaining two groups were not congruent with actual stimuli; one group expected higher-intensity stimuli, but actually received lower-intensity stimuli while the other group expected lower-intensity stimuli, but in fact received higher-intensity ones. Each group received a series of 24 varied-intensity electrical stimuli rated by the participants on a 30° intensity scale.
Results
Expectation manipulation had statistically significant effect on pain intensity assessment. When expecting lower-intensity stimuli, the participants underestimated pain intensity and when expecting higher-intensity stimuli, they overestimated pain intensity. The effect size of expectations upon pain intensity assessment was equal for both lower- and higher-intensity stimuli.
Conclusion
The obtained results imply that expectation manipulation can achieve the desired effect of decreasing or increasing both slight and more severe pain for a longer period of time. Manipulation via expectation before the stimuli series was proven to be effective for pain modulation in the entire series of stimuli which lasted around 10 min. The results suggest a potential benefit of manipulating expectations to alleviate emerging pain, since the obtained effects are moderate to large.
Implications
It seems that expectation effect is strong enough to “overcome” even the direct effect of stimulus intensity (at least in the low to moderate intensity range), which suggests potential benefits of verbal instructions even in rather painful stimuli.
1 Introduction
The role of expectation in pain modulation is studied within several research categories. The first category refers to the placebo effect. For the analgesic effect of some inactive substance to appear it is important that a person experience the matching (conditioning) of real and placebo treatment [1, 2]. The placebo effect is significantly greater and more stable if conditioning is accompanied by expectations of positive outcome [3, 4], but mere manipulation of expectation also leads to the placebo effect [5, 6, 7, 8]. A positive correlation was found between strength of expectations and the size of the placebo effect [9], and between the direction of expectation and the direction of placebo/nocebo effect [10]. The effect sizes of placebo analgesia are found to be greater in experimental than in clinical studies [11] which is attributed to more detailed instructions in clinical setting and therefore more specific and stronger expectations of a certain treatment [12], thus showing the importance of expectations in placebo analgesia.
The second research category refers to the open or hidden manner of drug administration. Unlike hidden drug administration, open administration is accompanied by verbal suggestions regarding its effectiveness. Open administration and verbal suggestions can double the analgesic effect of the drug [13, 14], but can also completely annul its effect (if the suggestions are negative) [15]. Expectations formed during open drug administration lead to greater drug effectiveness in patients suffering from pain, anxiety or Parkinsons’ disease [16], and influence the effectiveness of different drug-free pain treatments, e.g. acupuncture [17].
The third research category refers to the examination of the effect of expectation upon the experience of pain, without combining it with either placebo or actual treatment. These studies are mostly experimental, demonstrating that people assess same-intensity stimuli differently, depending on the experimentally induced expectations regarding the characteristics of the stimuli. When expecting a weak, non-painful stimulus, a person’s assessment of the received stimulus is lower than when expecting stimulus to be painful [18, 19, 20, 21]. Also, when participants are informed about the incoming stimulus intensity, they assess it as less intense or unpleasant [22, 23, 24].
Results within all three categories clearly illustrate the role of expectations as a cognitive modulator of pain and suggest practical implications of expectation-based pain modulation for people suffering from acute or chronic pain. Diversity of possible usage of expectations in research and practice makes expectations relevant for further investigation. This was also the reason why we conducted the present study. Between studies in the third research category, dominant are those that manipulate expectations by introducing a signal that suggests the quality of the following stimulus thus leading to the forming of expectation regarding the following stimulus. Those designs are especially eligible when testing the possible physiological basis of the expectation manipulation effect [25, 26] because of the possibility for the exact determination of time frames for the expected stimulus. There is, however, a deficiency of research which manipulates expectations for a longer period of time. If such an effect were found to be true, this would provide the basis for the usage of expectation in different pain treatments such as medical procedures with more than one short pain episode or prolonged pain that varies over time.
2 Methods
2.1 Participants
A total of 192 healthy participants (133 female) aged 18–51 (M = 22.97, SD = 4.55) volunteered to participate in the study. Participants were students and adults that answered adds on social networks or were recommended by other participants. Students got credits for their participation in the study and, after the data collection was over, all participant received written explanation of their results and general results of the study.
2.2 Stimulation
Electrical stimulation (DS5 Isolated Bipolar Constant Current Stimulator, Digitimer Ltd.) was applied to the upper side of the left index and ring fingers, near the fingernail. The size of the electrode was 1 cm2. Duration of each stimulus was 1.5 s.
2.3 Measurement of participants’ pain sensitivity
Measurement was conducted in isolated room of laboratory for psychological research. Participants were alone in the room but experimenter could see them at all times through glass that connected room for measurement with room in which aparates for electrical stimulation were.
The initial measurement was conducted prior to the main experiment for two reasons. The first was to introduce participants to the sensational quality of electrical stimulation. For that reason each participant received three different stimuli (1.96, 3.16 and 3.53 mA). The second purpose was to determine a participant’s individual sensitivity to electrical stimulation, which was done in two separate steps. First, participants received a series of 15 different stimuli (intensity range from 2.76 to 3.56 mA) in quasirandom sequence (differences between adjacent stimuli were 0.2 mA). Their task was to assess the pain intensity of each stimulus on a scale from 0 (weak, non-painful stimulus) to 10 (exceptionally strong, non-bearable stimulus). Second, 10 min later, participants were engaged in an electrical pain tolerance measurement. Electrical stimulation started at 1.96 mA and was sequentially increased by 0.2 mA until participants stated they could no longer tolerate pain. Pain tolerance was defined as the maximum stimulus intensity a participant was willing to endure. Based on these two measures (average assessment of 15 stimuli and individual pain tolerance) blocks of similarly sensitive participants were formed to ensure equivalence regarding sensitivity to electrical stimulation.
2.4 Design and experimental manipulation
One month later, we conducted the main experiment. There were four independent groups in concordance with the study design (Table 1). The groups differed in (a) expectation manipulation and (b) intensity of stimuli series. Expectation manipulation was primarily conducted through verbal instruction. The first experimental group was told that they would receive a series of lower-intensity stimuli and they actually received a series of lower-intensity electrocutaneous stimuli. The second group was told that they would receive a series of higher-intensity painful stimuli, but they in fact received the same series of lower-intensity electrocutaneous stimuli as the first group. The third group was told that they will receive a series of lower-intensity stimuli, but they in fact received a series of higher-intensity painful stimuli. The fourth group was told that they will receive a series of higher-intensity painful stimuli and they actually received a series of higher-intensity painful stimuli. The two groups where the intensity level of the stimuli in the series was in accordance with the verbally manipulated expectations (groups 1 and 4) are considered as referential groups.
Design of the study.
| Applied intensity of stimulation | Manipulated expectation | |
|---|---|---|
|
|
||
| Expectation of lower-intensity stimuli | Expectation of higher-intensity stimuli | |
| Series of lower-intensity stimuli (range: 1.96–3.36 mA) | Group 1 n = 48 (15) | Group 2 n = 49 (15) |
| Series of higher-intensity stimuli (range: 2.76–4.16 mA) | Group 3 n = 48 (14) | Group 4 n = 47( 15) |
-
In groups (1 and 4) expectations were congruent with the intensity of stimulation so these groups are treated as referent. In groups 2 and 3 expectations were not congruent with the intensity of stimulation. The difference between groups 1 and 2 indicates the effect of expectations in lower-intensity stimuli and the difference between groups 3 and 4 indicates the effect of expectations in higher-intensity painful stimuli. The number of male participants is displayed in parentheses.
To ensure that expectations regarding stimuli intensity would be firmly formed and plausible, in addition to the verbal instruction about the stimuli series, participants also received an initial set of stimuli (congruent with the verbal instruction) prior to measurement. Participants in the two groups that were told they were about to receive a series of lower-intensity stimuli received an initial set of 5 lower-intensity stimuli (range 2.16–3.14 mA), whilst participants in two groups that were told they were about to receive a series of higher-intensity stimuli received an initial set of 5 lower-intensity stimuli (range 2.94–3.92 mA). Participants were told that this was a trial series to prepare them before the real measurement and that the series of stimuli to follow would be approximately the same. For two groups this information was not true since they received trial series congruent with the instruction but not with the intensity of the series (groups 2 and 3). Participants were not informed of the real purpose of the study until the end.
2.5 Pain intensity assessments under manipulated expectations
After verbal instructions and 5 trial stimuli, each participant received a series of 24 stimuli. There were 8 different stimulus intensities within a series and each stimulus was presented 3 times in quasirandom sequence. Stimuli were induced at 15 s intervals. The participants task was to assess the intensity of each stimulus on a scale of 1–30 (adapted from Ellermeier and Westphal [27]). The participants were instructed to first categorize pain intensity of each stimulus within one of three categories (weak pain 1–10; moderate pain 11–20, and severe pain 21–30) and then to “fine tune” the assessment by choosing a number within the selected category. The experimental procedure, including both presentation of 24 stimuli and complementary assessment, lasted about 6–7 min.
3 Results
3.1 Effect of intensity of stimulation
Results of average pain intensity assessments for each of the eight stimuli in all four groups are presented in Fig. 1. The figure clearly demonstrates a linear trend of average assessments regarding stimulus intensity. We conducted two separate mixed ANOVAs, one for the series of lower-intensity stimuli and another for the series of higher-intensity stimuli. Both analyses tested the possible effect of two factors: expectation congruent/non-congruent with the series intensity (2) and stimulus intensity (8). The effect of stimulus intensity was statistically significant and large – both for the series of lower-intensity stimuli (F7,665 = 236.5; p < 0.001;
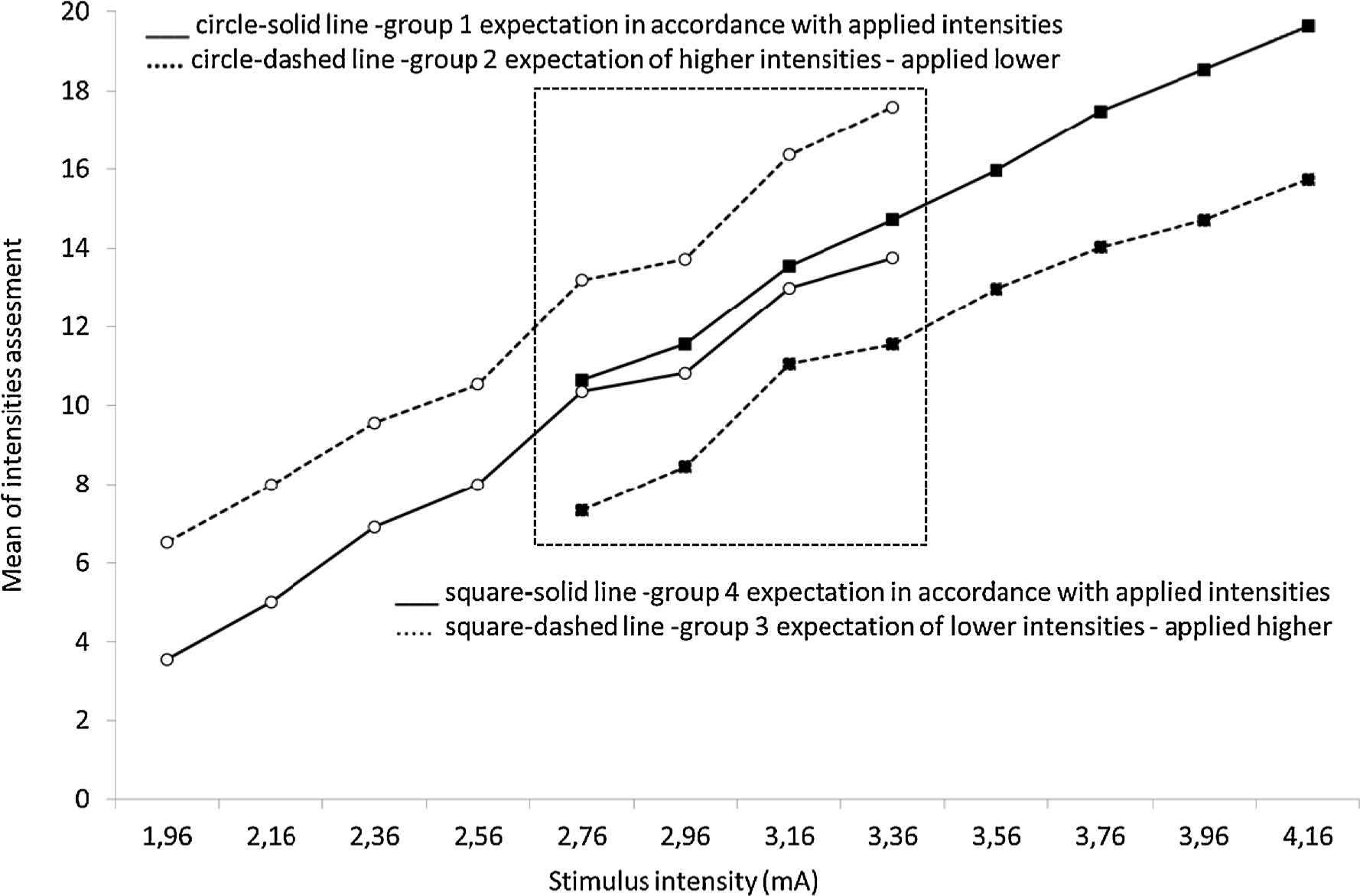
Mean pain intensity assessment for each of 8 stimuli intensities in four experimental groups. Full lines signify groups whose expectations were congruent with the actual series intensity (referent groups 1 and 4), whilst dashed lines signify groups whose expectations were not congruent with the actual series intensity (groups 2 and 3). Framed stimuli were identical in all four groups.
3.2 Effect of expectation manipulation on pain assessment
To test the effect of expectation manipulation in a lower-intensity stimuli situation, we compared the average pain intensity assessment obtained by the group whose expectations were congruent with the presented lower intensity of the series (referent group 1) and the pain intensity assessment obtained by the group whose expectations were not congruent (participants expected higher intensity stimuli) with the presented lower intensity of the series (group 2). Pain intensity assessments were significantly higher when participants expected a higher intensity series (see Table 2). Analogously, we tested the effect of expectation manipulation in a high-intensity stimuli situation by comparing the differences between groups 3 and 4. Pain intensity assessments were significantly lower when participants expected a lower intensity series. In both cases, expectation manipulation modified assessment of pain intensity – induced by objectively equal intensity series – in the direction congruent with expectation. The effect size for the lower-intensity stimuli situation was almost identical to the effect size for the higher-intensity stimuli situation (see Cohen’s d in Table 2). To illustrate the relation of expectation more clearly within the same stimulus intensity, we additionally tested the differences between the four groups, but only for the average pain assessments of four stimuli intensities – those presented in all four groups (see square area in Fig. 1; the four strongest stimuli in the lower-intensity series were the weakest stimuli in the higher-intensity series - ranging from 2.76 to 3.36 mA). Mean pain intensity assessments for all four stimuli in each experimental situation (group) are shown in Fig. 2. Differences were tested with a one-way ANOVA, which demonstrated statistically significant differences in mean pain intensity assessments for all four stimuli in each experimental situation (F3=8.65; p < 0.001;
Average pain intensity assessments (for all stimuli within the entire series) in four experimental groups.
| Applied intensity of stimulation | Manipulated expectation | t | p | d | |||||
|---|---|---|---|---|---|---|---|---|---|
|
|
|||||||||
| Expectation of lower-intensity stimuli | Expectation of higher-intensity stimuli | ||||||||
|
|
|
||||||||
| n | M | SD | n | M | SD | ||||
| Series of lower-intensity stimuli | 48 | 8.93 | 4.42 | 49 | 11.94 | 5.19 | 3.07 | 0.003 | 0.62 |
| Series of higher-intensity stimuli | 48 | 11.98 | 4.18 | 47 | 15.27 | 5.76 | 3.17 | 0.002 | 0.66 |
-
Group differences were tested using t-test; effect size is Cohen’s d.

Mean pain intensity assessment for the four identical stimulus intensities (intensities from 2.76 to 3.36 mA) presented in all four experimental situations. Grey columns represent referent groups where expectations were congruent with the series intensity. The biggest effect of expectation can be observed between two extreme situations (black columns) where information was not congruent with the actually presented series, but also between groups with the same applied intensities and different expectations. *p < 0.05; **p < 0.01.
4 Discussion
The obtained results demonstrate the evident effect of expectation manipulation on pain assessment of the stimuli series. When participants expected lower stimuli then those they actually received, their pain intensity assessment was lower. Also, when participants expected higher stimuli then those they actually received, their pain intensity assessment was higher. Expectation had an equal effect in both lower- and higher-intensity stimulus settings, though in the opposite directions, depending on the direction of expectation. Specifically, the lower-intensity expectation decreased pain assessment to the same degree the higher-intensity expectation increased pain assessment.
The present experimental study differs somewhat in design from former studies because manipulation occurred before a series of stimuli and not before a single stimulus. The results suggest that expectation manipulation affected an entire series of stimuli that lasted about 7 min. This suggests that expectations can affect the pain experience for a period longer than few minutes, which implies a possible use of expectation manipulation before longer treatments in both the research and medical context. In this study duration of set of stimuli was around 10 min so there is a need for further research to see if the same can apply for even longer periods of time. The outcomes of this experimental study are similar to those obtained in studies that examine the difference between hidden and open drug administration. In those cases, expectation effect also lasts for a longer period of time and is general to an extent. The present study also demonstrated a long-lasting general effect, additionally revealing that expectations function in both ways – positive and negative – and that those effects are similar.
The findings of several studies indicate that expectation manipulation induced by signalling the intensity of each incoming stimulus effect not only the perception of pain intensity, but also lead to changes in the cerebral structures involved in processing signals from the nociceptors. Expectations of a higher-intensity stimulus and increase of pain additionally activate the thalamus, prefrontal cortex and anterior cingulate cortex – which leads to higher pain perception, even in non-painful stimuli [28, 29], whilst expectations of decreased pain additionally lower the activation in those brain areas, which leads to lower pain perception [15, 18, 30, 31]. Results of the present research suggest that obtained expectation effects probably have a real (and physiological) basis, i.e. it is not just a bias in pain perception. The obtained effects were rather stable, clear and quite large. It can be seen specifically from the difference between the two situations where expectations were not congruent with the presented stimuli intensity (groups 2 and 3) which demonstrates that opposite expectations lead to different pain intensity assessments of objectively equal stimulus intensity.
4.1 Methodological considerations
In the absence of some objective measures of the nociceptive signals processing level (physiological activation) we tried to come up with a design that will show that the positive effect of expectation is real and not just a perception bias or complying with the experimenter. Painful behaviour is also social behaviour so chances are that participants will behave in the way the experimenter suggests or expects them to behave, especially if he/she gives explicit instructions. To assure greater naivety of participants and prevent them from recognizing the real purpose of the study, we had four independent groups of participants that had minimal chances for communicating and mimicking one another. At the end of the experiment, participants stated their thoughts about what they believed was the real purpose of the measurement and none of them said they believed we were investigating the role of expectations on pain experience.
Potential threat to validity of the obtained results might come from the way stimuli were presented. Namely, psychophysical studies demonstrated that assessment of the single stimulus within a series depends also on the intensity level of the series itself [32, 33, 34]. As we can see from the results of two referent groups, stimuli context probably did not affect the present research. In Fig. 1 we can see an almost identical relationship between stimuli intensity and pain intensity assessments in both groups (one line practically continues from the other); this implies that differences in series intensity did not affect the measurement i.e. that there probably was no stimuli context effect included within the expectation effect.
The range of stimuli intensities used in the present study limits generalization of the obtained findings. We did use intensities within the range from non-painful to painful, but the fact is that the average pain intensity assessment of the highest-intensity stimulus was in the area of moderate pain intensity. This means that we cannot be certain that expectation manipulation would have the same effect if the stimuli, along with associated pain sensation, were more intense. In the present study, the range of stimuli series was chosen based on initial measurement, making sure that difference between the verbal instructions (expectation manipulation) and stimuli intensity was not oversized. We chose not to use very high-intensity stimuli for both ethical and methodological reasons. If we told participants to expect low-intensity stimuli and presented them with very high-intensity stimuli, not only would this be ethically questionable, but also could make participants suspicious of the nature of the study. Although the results may have been even more comprehensive if we included a wider range of stimuli together with a control group that had no previous instructions about stimulus intensity, the present study contributes to pain research by demonstrating the robustness of prolonged expectation effect on pain intensity assessment. Specifically, the fact that expectations in the present study were formed prior to the series of stimuli makes manipulation more natural and more similar to real clinical conditions which increases ecological validity and broadens the practical implications of the present study.
5 Conclusions
The obtained results imply that expectations can be induced and have effect on pain perception in experimental conditions. Expectation manipulation can achieve the desired effect of decreasing or increasing both slight and more severe pain for a longer period of time (couple of minutes). Results show that when participants expected lower stimuli than those they actually received, their pain intensity assessment was lower. Also, when participants expected higher stimuli than those they actually received, their pain intensity assessment was higher. Expectation had an equal effect in both directions, i.e. the lower-intensity expectation decreased pain assessment to the same degree the higher-intensity expectation increased pain assessment.
6 Implications for practice
The obtained results imply that expectation manipulation can achieve the desired effect of decreasing or increasing both slight and more severe pain for a period of time of around 10 min. Considering previous findings, demonstrating that medical personnel and their approach towards the patient can decrease/increase pain experience [35, 36, 37], the results of the present study and all similar ones, can contribute to the design of more efficient medical practice for interacting with patients in pain. The present findings provide a rationale for suggesting pain intensity (primarily lower pain) to patients experiencing pain or patients who are about to undergo some painful medical procedure. A carefully given explanation of what is about to follow together with specific information regarding the length of the stimulus, can significantly affect a patient’s pain experience. If we observe Fig. 1, we can see that stimuli were assessed in congruence with expectation, but also that pain assessment of objectively lower-intensity stimuli preceded by the expectation of higher-intensity stimuli was in fact higher than the assessment of objectively higher-intensity stimuli preceded by the expectation of lower-intensity stimuli. It seems that expectation effect is strong enough to “overcome” even the direct effect of stimulus intensity (at least in the low to moderate intensity range), which suggests potential benefits of verbal instructions even in rather painful stimuli.
It should be noted, when inducing expectations, that one must be careful not to overdo it. Namely, though the present findings suggest expectations about incoming pain should be set to a lower level, setting them exceedingly far from the objective level of stimuli/pain might lead participants/patients to suspect that “something is not right”. This might not only annihilate the desired effect but also lead to unintended and potentially harmful consequences – mistrust towards the person conducting a procedure. In the present research, this was avoided by setting lower- and higher-intensity series relatively close to each other (even partially overlapping).
When observing these results in the context of drug effectiveness, the mere knowledge that one receives medication or not (and the expectation of its effectiveness) influences how well the drug will work [38, 39, 40, 41] it may be suggested that a combination of expectation manipulation and administration of real analgesics might additionally ameliorate effectiveness of analgesics. But one should note that this effect goes both ways – if rather low intensity stimuli are preceded by negative expectations (expectations that pain will be sizable) pain assessment can even be greater. This suggests the need for caution when giving instructions for medication or a medical procedure.
Highlights
Expectation can have prolonged effect on pain perception.
When expecting lower-intensity stimuli, participants underestimated pain intensity.
When expecting higher-intensity stimuli, participants overestimated pain intensity.
The effect size is moderate to large for both lower-and higher-intensity stimuli.
DOI of refers to article: http://dx.doi.org/10.1016/j.sjpain.2016.11.016.
-
Ethical issues: The research was approved by the Local Ethics Committee and all participants signed an informed consent form.
-
Conflicts of interest: There are no known conflicts of interest associated with this publication and there has been no significant financial support for this work that could have influenced its outcome. The manuscript has been read and approved by all named authors and that there are no other persons who satisfied the criteria for authorship but are not listed. Authors have given due consideration to the protection of intellectual property associated with this work and that there are no impediments to publication, including the timing of publication, with respect to intellectual property.
References
[1] Voudouris NJ, Peck CL, Coleman G. Conditioned response models of placebo phenomena: further report. Pain 1989;38:109–16.Search in Google Scholar
[2] Benedetti F, Amanzio M. The neurobiology of placebo analgesia: from endogenous opioids to cholecystokinin. Prog Neurobiol 1997;51:109–25.Search in Google Scholar
[3] Voudouris NJ, Peck CL, Coleman G. The role of conditioning and verbal expectancy in the placebo response. Pain 1990;43:121–8.Search in Google Scholar
[4] Montgomery GH, Kirsh I. Classical conditioning and the placebo effect. Pain 1997;72:107–13.Search in Google Scholar
[5] Petrovic P, Dietrich T, Fransson P, Andersson J, Carlsson K, Ingvar M. Placebo in emotional processing – induced expectations of anxiety relief activate a generalized modulatory network. Neuron 2005;46:957–69.Search in Google Scholar
[6] Petrovic P, Kalso E, Peterson KM, Andersson J, Fransson P. A prefrontal nonopioid mechanism in placebo analgesia. Pain 2010;150:59–65.Search in Google Scholar
[7] Wager Tor D, Atlas LY, Leotti LA, Rilling JK. Predicting individual difference in placebo analgesia: contribution of brain activity anticipation and pain experience. J Neurosci 2011;31:439–52.Search in Google Scholar
[8] Schmid J, Theysohn N, Gaß F, Benson S, Gramsch C, Forsting M, Gizewski ER, Elsenbruch S. Neural mechanisms mediating positive and negative treatment expectations in visceral pain: a functional magnetic resonance imaging study on placebo and nocebo effects in healthy volunteers. Pain 2013;154:2372–80.Search in Google Scholar
[9] De Pascalis V, Chiaradia C, Carotenuto E. The contribution of suggestibility and expectation to placebo analgesia phenomenon in an experimental setting. Pain 2002;96:393–402.Search in Google Scholar
[10] Krummenacher P, Candia V, Folkers G, Schedlowski M, Schönbächler G. Prefrontal cortex modulates placebo analgesia. Pain 2010;148:368–74.Search in Google Scholar
[11] Sauro MD, Grenberg RP. Endogenous opiates and the placebo effect: a meta-analytic review. J Psychosom Res 2005;58:115–20.Search in Google Scholar
[12] Price DD, Chung SK, Robinson ME. Conditioning, expectation, and desire for relief in placebo analgesia. Semin Pain Med 2005;3:15–21.Search in Google Scholar
[13] Amanzio M, Pollo A, Maggi G, Benedetti F. Response variability to analgesics: a role for non-specific activation of endogenous opioids. Pain 2001;90:205–15.Search in Google Scholar
[14] Amanzio M, Benedetti F. Neuropharmacological dissection of placebo analgesia: expectation-activated opioid systems versus conditioning-activated specific subsystems. J Neurosci 1999;19:484–94.Search in Google Scholar
[15] Bingel U, Wanigasekera V, Wiech K, Ni Mhuircheartaigh R, Lee MC, Ploner M, Tracey I. The effects of treatment expectation on drug efficacy: imaging the analgesic benefit of the opioid remifentanil. Sci Transl Med 2011;3, http://dx.doi.org/10.1126/scitranslmed.3001244.Search in Google Scholar
[16] Colloca L, Lopiano L, Lanotte M, Benedetti F. Overt versus covert treatment for pain, anxiety and Parkinson’s disease. Lancet Neurol 2004;3:679–84.Search in Google Scholar
[17] Linde K, Witt CM, Streng A, Weidenhammer W, Wagenpfeil S, Brinkhaus B, Willich SN, Melchart D. The impact of patient expectations on outcomes in four randomized controlled trials of acupuncture in patients with chronic pain. Pain 2007;128:264–71.Search in Google Scholar
[18] Koyama T, McHaffie JG, Laurienti PJ, Coghill RC. The subjective experience of pain: where expectations become reality. Proc Natl Acad Sci U S A 2005;102:12950–5.Search in Google Scholar
[19] Colloca L, Sigaudo M, Benedetti F. The role of learning in nocebo and placebo effects. Pain 2008;136:211–8.Search in Google Scholar
[20] Benedetti F, Arduino C, Amanzio M. Somatotopic activation of opioid systems by target-directed expectations of analgesia. J Neurosci 1999;19:3639–48.Search in Google Scholar
[21] Brown CA, Seymour B, Boyle Y, El-Deredy W, Jones AKP. Modulation of pain ratings by expectation and uncertainty: behavioral characteristics and anticipatory neural correlates. Pain 2008;135:240–50.Search in Google Scholar
[22] Johnson JE. Effects of accurate expectations about sensations on the sensory and distress components of pain. J Pers Soc Psychol 1973;27:261–75.Search in Google Scholar
[23] Price DD, Barrell JJ, Gracely RH. A psychophysical analysis of experimental factors that selectively influence the affective dimension of pain. Pain 1980;8:137–49.Search in Google Scholar
[24] Wang Y, Wang J-Y, Luo F. Why self-induced pain feels less painful than externally generated pain: distinct brain activation patterns in self- and externally generated pain. PLoS ONE 2011;6, http://dx.doi.org/10.1371/journal.pone.0023536.Search in Google Scholar
[25] Lobanov OV, Zeidan F, McHaffie JG, Kraft RA, Coghill RC. From cue to meaning: brain mechanisms supporting the construction of expectations of pain. Pain 2014;155:129–36.Search in Google Scholar
[26] Atlas LY, Bolger N, Lindquist MA, Wager TD. Brian mediators of predictive cue effects on perceived pain. J Neurosci 2010;30:12964–77.Search in Google Scholar
[27] Ellermeier W, Westphal W. On the “absoluteness” of category and magnitude scales of pain. Percept Psychophys 1991;49:159–66.Search in Google Scholar
[28] Sawamoto N, Honda M, Okada T, Hanakawa T, Kanda M, Fukuyama H, Konishi J, Shibasaki H. Expectation of pain enhances responses to nonpainful somatosensory stimulation in the anterior cingulate cortex and parietal operculum/posterior insula: an event-related functional magnetic resonance imaging study. J Neurosci 2010;20:7438–45.Search in Google Scholar
[29] Pollo A, Torre E, Lopiano L, Rizzone M, Lanotte M, Cavanna A, Bergamasco B, Benedetti F. Expectation modulates the response to subthalamic nucleus stimulation in Parkinsonian patients. Neuroreport 2002;13:1383–6.Search in Google Scholar
[30] Lichtman AH, Fanselow MS. Opioid and nonopioid conditional analgesia: the role of spinal opioid, noradrenergic, and serotonergic systems. Behav Neurosci 1991;105:687–98.Search in Google Scholar
[31] Ploghaus A, Becerra L, Borras C, Borsook D. Neural circuitry underlying pain modulation: expectation, hypnosis, placebo. Trends Cogn Sci 2003;7:197–200.Search in Google Scholar
[32] Poulton EC. Models for biases in judging sensory magnitude. Psychol Bull 1979;86:777–803.Search in Google Scholar
[33] Gescheider GA, Bolanowski SJ, Verrillo RT. Sensory, cognitive and response factors in the judgment of sensory magnitude. In: Algom D, editor. Psychophysical approaches to cognition. Amsterdam: North-Holland; 1992. p. 575–621.Search in Google Scholar
[34] Petzold P. Context effects in judgments of attributes: an information-integration approach. In: Geissler H-G, Link SW, Townsend JT, editors. Cognition, information processing, and psychophysics. Basic issues. Hillsdale, NJ: Lawrence Erlbaum Associates; 1992. p. 175–205.Search in Google Scholar
[35] Gracely RH, Dubner R, Deeter WD, Wolskee PJ. Clinicians’ expectations influence placebo analgesia. Lancet 1985;325:43.Search in Google Scholar
[36] Benedetti F. How the doctor’s words affect the patient’s brain. Eval Health Prof 2002;25:369–86.Search in Google Scholar
[37] Benedetti F. Placebo and the new physiology of the doctor–patient relationship. Physiol Rev 2013;93:1207–46.Search in Google Scholar
[38] Geers AL, Weiland PE, Kosbab K, Landry SJ, Helfer SG. Goal activation, expectations, and placebo effect. J Pers Soc Psychol 2005;89:143–59.Search in Google Scholar
[39] Levine JD, Gordon NC. Influence of the method of drug administration on analgesic response. Nature 1984;312:755–6.Search in Google Scholar
[40] Price DD, Milling LS, Kirsch I, Duff A, Montgomery GH, Nicholls SS. An analysis of factor that contribute to the magnitude of placebo analgesia in an experimental paradigm. Pain 1999;83:147–56.Search in Google Scholar
[41] Volkow ND, Wang G, Ma Y, Fowler JS, Zhu W, Maynard L, Telang F, Vaska P, Ding Y, Wong C, Swanson JM. Expectation enhances the regional brain metabolic and the reinforcing effects of stimulants in cocaine abusers. J Neurosci 2003;23:11461–8.Search in Google Scholar
© 2016 Scandinavian Association for the Study of Pain
Articles in the same Issue
- Scandinavian Journal of Pain
- Editorial comment
- Patients with chronic neck-pain after trauma do not differ in type of symptoms and signs, but suffer more than patients with chronic neck pain without a traumatic onset
- Observational study
- Chronic neck pain patients with traumatic or non-traumatic onset: Differences in characteristics. A cross-sectional study
- Editorial Comment
- Re-enforcing therapeutic effect by positive expectations of pain-relief from our interventions
- Original experimental
- Effect of expectation on pain assessment of lower- and higher-intensity stimuli
- Editorial comment
- Objective methods for the assessment of the spinal and supraspinal effects of opioids
- Topical review
- Objective methods for the assessment of the spinal and supraspinal effects of opioids
- Editorial Comment
- Multi-target treatment of bone cancer pain using synergistic combinations of pharmacological compounds in experimental animals
- Original experimental
- Synergistic combinations of the dual enkephalinase inhibitor PL265 given orally with various analgesic compounds acting on different targets, in a murine model of cancer-induced bone pain
- Editorial comment
- Terminal cancer pain intractable by conventional pain management can be effectively relieved by intrathecal administration of a local anaesthetic plus an opioid and an alfa2-agonist into the cerebro-spinal-fluid
- Observational study
- Multimodal intrathecal analgesia in refractory cancer pain
- Editorial comment
- Treatment success in neck pain: The added predictive value of psychosocial variables in addition to clinical variables
- Observational study
- Treatment success in neck pain: The added predictive value of psychosocial variables in addition to clinical variables
- Editorial comment
- Why are some patients with chronic pain from anterior abdominal nerve entrapment syndrome (ACNES) refractory to peripheral treatment with neurectomy?
- Clinical pain research
- Treatment response and central pain processing in Anterior Cutaneous Nerve Entrapment Syndrome: An explorative study
- Editorial comment
- Gain in functions before pain reduction during intensive multidisciplinary paediatric pain rehabilitation programme
- Clinical pain research
- Physical and occupational therapy outcomes: Adolescents’ change in functional abilities using objective measures and self-report
- Editorial comment
- Complex Regional Pain Syndrome (CRPS): High risk of CRPS after trauma in another limb in patients who already have CRPS in one hand or foot: Lasting changes in neural pain modulating systems?
- Clinical pain research
- The risk of pain syndrome affecting a previously non-painful limb following trauma or surgery in patients with a history of complex regional pain syndrome
- Editorial Comment
- Positive affect could reduce the impact of pain
- Original experimental
- The buffering role of positive affect on the association between pain intensity and pain related outcomes
- Editorial comment
- The meaning and consequences of amputation and mastectomy from the perspective of pain and suffering – Lessons to be learned and relearned
- Clinical pain research
- The meaning and consequences of amputation and mastectomy from the perspective of pain and suffering
- Editorial comment
- Invasive intervention for “intractable” Complex Regional Pain Syndromes (CRPS)?
- Educational case report
- Intrathecal management of complex regional pain syndrome: A case report and literature
- Observational study
- Item response theory analysis of the Pain Self-Efficacy Questionnaire
- Announcement
- Scandinavian Association for the Study of Pain (SASP): Annual Meeting 2017
Articles in the same Issue
- Scandinavian Journal of Pain
- Editorial comment
- Patients with chronic neck-pain after trauma do not differ in type of symptoms and signs, but suffer more than patients with chronic neck pain without a traumatic onset
- Observational study
- Chronic neck pain patients with traumatic or non-traumatic onset: Differences in characteristics. A cross-sectional study
- Editorial Comment
- Re-enforcing therapeutic effect by positive expectations of pain-relief from our interventions
- Original experimental
- Effect of expectation on pain assessment of lower- and higher-intensity stimuli
- Editorial comment
- Objective methods for the assessment of the spinal and supraspinal effects of opioids
- Topical review
- Objective methods for the assessment of the spinal and supraspinal effects of opioids
- Editorial Comment
- Multi-target treatment of bone cancer pain using synergistic combinations of pharmacological compounds in experimental animals
- Original experimental
- Synergistic combinations of the dual enkephalinase inhibitor PL265 given orally with various analgesic compounds acting on different targets, in a murine model of cancer-induced bone pain
- Editorial comment
- Terminal cancer pain intractable by conventional pain management can be effectively relieved by intrathecal administration of a local anaesthetic plus an opioid and an alfa2-agonist into the cerebro-spinal-fluid
- Observational study
- Multimodal intrathecal analgesia in refractory cancer pain
- Editorial comment
- Treatment success in neck pain: The added predictive value of psychosocial variables in addition to clinical variables
- Observational study
- Treatment success in neck pain: The added predictive value of psychosocial variables in addition to clinical variables
- Editorial comment
- Why are some patients with chronic pain from anterior abdominal nerve entrapment syndrome (ACNES) refractory to peripheral treatment with neurectomy?
- Clinical pain research
- Treatment response and central pain processing in Anterior Cutaneous Nerve Entrapment Syndrome: An explorative study
- Editorial comment
- Gain in functions before pain reduction during intensive multidisciplinary paediatric pain rehabilitation programme
- Clinical pain research
- Physical and occupational therapy outcomes: Adolescents’ change in functional abilities using objective measures and self-report
- Editorial comment
- Complex Regional Pain Syndrome (CRPS): High risk of CRPS after trauma in another limb in patients who already have CRPS in one hand or foot: Lasting changes in neural pain modulating systems?
- Clinical pain research
- The risk of pain syndrome affecting a previously non-painful limb following trauma or surgery in patients with a history of complex regional pain syndrome
- Editorial Comment
- Positive affect could reduce the impact of pain
- Original experimental
- The buffering role of positive affect on the association between pain intensity and pain related outcomes
- Editorial comment
- The meaning and consequences of amputation and mastectomy from the perspective of pain and suffering – Lessons to be learned and relearned
- Clinical pain research
- The meaning and consequences of amputation and mastectomy from the perspective of pain and suffering
- Editorial comment
- Invasive intervention for “intractable” Complex Regional Pain Syndromes (CRPS)?
- Educational case report
- Intrathecal management of complex regional pain syndrome: A case report and literature
- Observational study
- Item response theory analysis of the Pain Self-Efficacy Questionnaire
- Announcement
- Scandinavian Association for the Study of Pain (SASP): Annual Meeting 2017