Is there a geographic and gender divide in Europe regarding the biopsychosocial approach to pain research? An evaluation of the 12th EFIC congress
-
Meghan A. Koop
 ,
Andrea C. Benson
,
Michiel F. Reneman
,
Gwendolyne G.M. Scholten-Peeters
and
Michel W. Coppieters
,
Andrea C. Benson
,
Michiel F. Reneman
,
Gwendolyne G.M. Scholten-Peeters
and
Michel W. Coppieters


Abstract
Objectives
All pain research combined advances the different domains of the biopsychosocial model and its interactions. However, there may be discrepancies between individual countries in their biomedical, psychological or social focus to pain research. As a proxy for this possible discrepancy, we analysed the biopsychosocial orientation of presentations at a recent major international pain conference.
Methods
The primary aim was to investigate whether there are geographical differences across Europe regarding the biopsychosocial orientation of workshop presentations at the 12th EFIC congress. The secondary aim was to investigate whether there were differences between female and male presenters regarding the biopsychosocial focus of their presentations. All available workshop abstracts were blinded and categorised by two independent reviewers as biomedical, psychosocial, biopsychosocial, or not applicable. Psychosocial and biopsychosocial were merged to non-biomedical.
Results
Of the 140 available abstracts, 126 abstracts could be categorised (biomedical: 51 %; non-biomedical: 49 %). Three clusters of countries emerged: (1) countries with a clear majority (≥80 %) of non-biomedical presentations (The Netherlands and Belgium); (2) countries with a balance between biomedical and non-biomedical presentations (United Kingdom, Denmark, Norway, Sweden and Finland); and (3) countries with a clear majority (71–100 %) of biomedical presentations (Italy, Germany, Switzerland and France). Overall, women delivered more presentations than men (70 vs. 56 presentations), and delivered proportionally more non-biomedical presentations (57 %) whereas men delivered proportionally more biomedical presentations (61 %).
Conclusions
Analysis of the 12th EFIC congress revealed geographical and gender differences in biopsychosocial orientation. Whether this reflects established differences in pain research requires further investigation.
Introduction
The biopsychosocial model of pain provides a framework for the assessment and management of acute and chronic pain [1]. This conceptual model describes pain and disability as a multidimensional, dynamic integration among biomedical (or biological), psychological, and social (or environmental) factors that reciprocally influence one another [2] The strength of the biopsychosocial model comes from its multidimensionality. Although the biopsychosocial model is widely accepted as the theoretical basis for multimodal and multidisciplinary treatments for pain [3, 4], the impact of the model on treatment outcomes remains unclear [5]. Breakthroughs in each of the domains of the biopsychosocial model, and in the dynamic interactions between its domains, may result in better treatment outcomes [6]. Although there is debate about the relative importance of the different domains within the model [7], we opine that advances in the biological and non-biological domains (i.e., the psychological and social domains) are both essential.
At international scientific conferences on pain, such as the Congress of the European Pain Federation (EFIC), emerging and established clinical researchers and basic scientists share their latest research on the various facets of pain and its management. One of the tasks of the scientific program committee at major pain conferences is to safeguard a diverse and multidisciplinary program that reflects advances in the biomedical, psychological and social domains of pain. Although the aim to balance contributions in each of these domains is likely achieved at the overarching conference level, we were interested to investigate whether this balance is also present at the level of individual countries. In other words, do presenters from certain member countries of EFIC present substantially more on biomedical advances, whereas presenters from other member countries present considerably more on psychosocial advances.
A geographical analysis provides an understanding of where (i.e., in which countries) recent research advances occur in which domains of the biopsychosocial model. The results of this analysis may also serve as a proxy measure for where biological, psychological and social innovations occur in the management of people in pain. If geographical differences would be identified, reasons may be sought to reveal underlying causes and whether research in certain domains may need to be stimulated in certain areas. Therefore, the primary aim of this study was to investigate whether there are geographical differences between countries regarding their contributions to the different domains of the biopsychosocial model of pain at a major international pain congress, namely the 12th EFIC Congress (2022). The secondary aim was to investigate whether there were differences between female and male presenters regarding the biopsychosocial focus of their presentations.
Methods
To address the aims of this study, we reviewed and categorised the abstracts of all workshop presentations delivered at the 12th EFIC Congress held in Dublin, Ireland, 27–30 April 2022. As this study was a review of published abstracts, ethical approval from the institutional review board was not applicable. EFIC is considered Europe’s most important multi-disciplinary and multi-professional organisation in the field of pain sciences and consists of the 38 European Chapters of the International Association for the Study of Pain (IASP) [8]. EFIC aims to advance research, education, clinical management and professional practice related to pain. An important avenue to achieve these aims is via the organisation of a biennial scientific congress on pain, showcasing the latest research and clinical management approaches [9].
Abstract selection
Workshops at the 12th EFIC Congress typically consisted of 3 presentations and 3 separate abstracts. The abstracts provided for each workshop presentation were downloaded from the scientific program provided on the EFIC conference website (May 6, 2022) [10] As our analyses were focussed on the member countries of EFIC, abstracts from presenters whose primary affiliation was from a non-EFIC member country were removed. Duplicate abstracts were also removed. To blind the abstracts that were retained, the presenter’s name and affiliations were removed from each abstract.
Abstract classification
Two reviewers (MK & AS) independently assigned the blinded abstracts to one of four categories using a previously published biopsychosocial categorisation checklist [11]: The following principles were applied to the research topic of the abstract to classify the abstract as: ‘Predominantly biomedical’: the main focus was on biological disease processes and/or the search for an anatomical/physiological mechanisms to understand or influence pain or disability; ‘Predominantly psychosocial’: the main focus was on psychological and/or social factors to understand and/or influence pain or disability; and ‘Predominantly biopsychosocial’: the main focus included both biomedical and psychosocial approaches to understand and/or influence pain or disability. If the topic of the abstract did not lend itself for classification in the biopsychosocial framework (e.g., policy making, methodology/statistics, or continuing education), the abstract was labelled as ‘Not applicable’. Unresolved disagreements between the two independent raters were discussed with a third reviewer (MC, MR or GSP) in order to reach an agreement. If there was still doubt regarding how the abstract should be classified after consultation with a third reviewer, the video recording of the workshop (if available) was viewed by one of the reviewers (MK). Abstracts in the ‘Not applicable’ category were removed from further analyses. Abstracts pertaining to human and/or animal studies were both considered. The primary affiliation of the presenter determined the allocated origin of the presentation.
The abstracts that originated from non-EFIC member countries that were removed from the analyses were used by the investigator team to test the classification system. These abstracts were rated independently, and then discussed in batches of 15 abstracts in several group sessions. For the abstracts included in the study, the percentage agreement between the two reviewers (MK & AS) was calculated.
Analysis
Data were gathered and analysed using Microsoft Excel. The number of abstracts and the gender distribution of the presenters were calculated for each country. The percentage of abstracts per biopsychosocial category was calculated per country. The gender distribution was calculated for each biopsychosocial category. Countries with less than five included abstracts were excluded from further analysis. To visualise possible geographical differences in biopsychosocial focus between countries, a map chart was created (Microsoft Excel, Version 2210 Redmond, Washington, United States). For this map, data were dichotomised into biomedical (i.e., the ‘Predominantly biomedical’ category) and non-biomedical (i.e., the ‘Predominantly psychosocial’ and ‘Predominantly biopsychosocial’ categories).
Results
Abstract selection and classification
The 12th EFIC Congress had 76 topical workshops, with typically 3 presentations per workshop. Of the 231 workshop presentations, 56 did not provide an abstract, resulting in 175 available abstracts which were downloaded from the EFIC conference virtual program. After removal of abstracts originating from non-EFIC member countries (n=30) and duplicate abstracts (n=5), 140 abstracts could be categorised. Agreement between the two independent reviewers before deliberation was 67.1 % and reached 85.7 % following deliberation. Reasons for disagreement varied across classifications. For the 20 remaining abstracts (14.3 %), consultation of a third reviewer resulted in the classification of 10 abstracts. The remaining 10 abstracts required viewing of the video recording of the presentation to achieve categorisation of the presentation. Of the 140 categorised abstracts, 14 were classified as “Not Applicable” and removed from further analysis. A summary of the abstract selection and classification is provided in Figure 1.
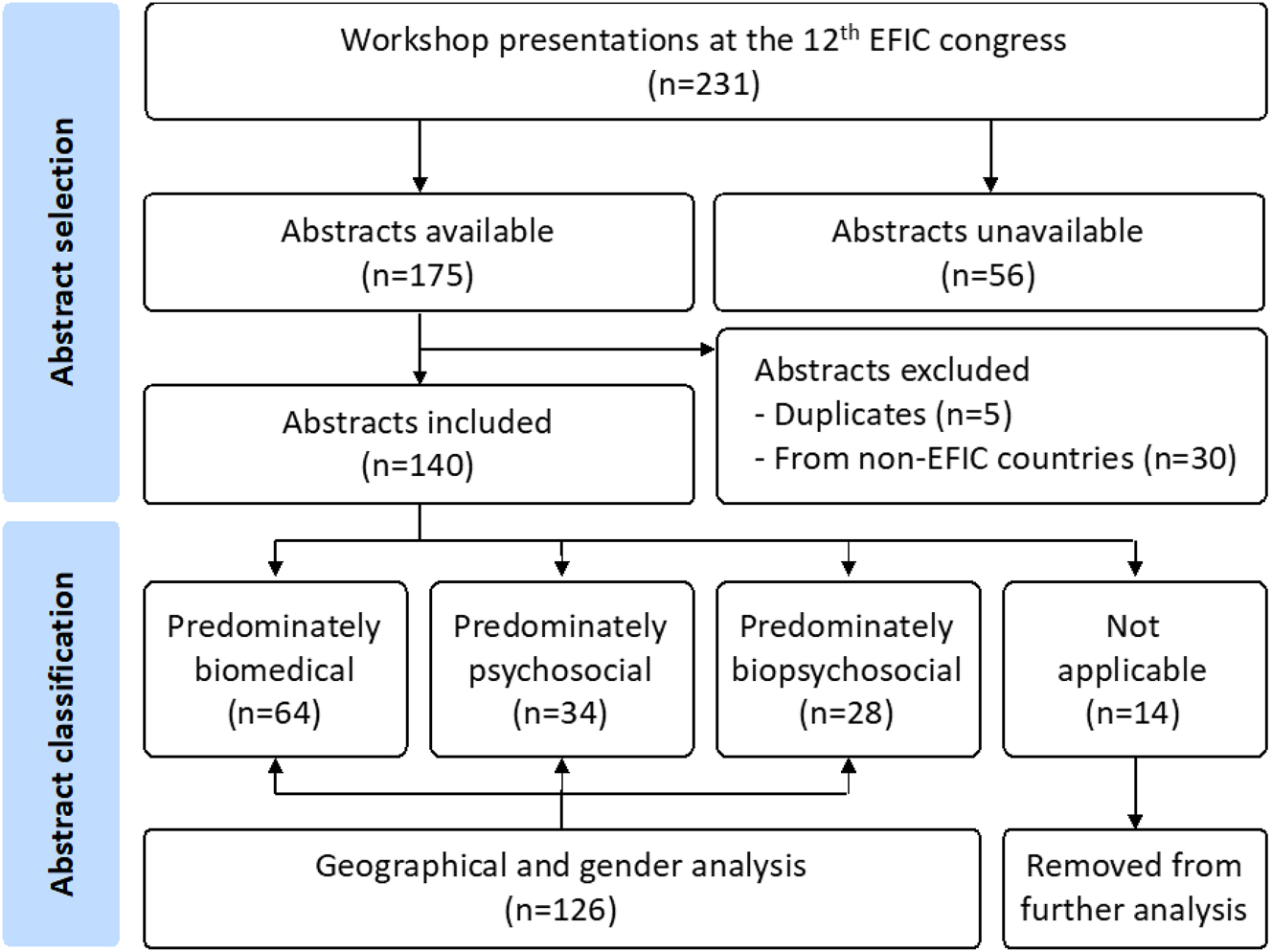
Flowchart of abstract selection, reviewer agreement and classification.
Geographical divide
The available abstracts originated from 18 different European countries. The countries that provided the most abstracts were the United Kingdom (n=31), Germany (n=14), Belgium (n=14), Denmark (n=14) and The Netherlands (n=10) (Table 1). Eight countries provided less than five abstracts. Of the 126 abstracts that were classified, 51 % were ‘Predominately biomedical’, 27 % ‘Predominately psychosocial’, and 22 % ‘Predominately biopsychosocial’. When dichotomised into having a biomedical or non-biomedical focus, there was a balance between the proportion of abstracts with a biomedical focus (51 %) and a non-biomedical focus (49 %) at the overall congress level. However, at country level, clear differences emerged between countries. For some countries, there was a large proportion of abstracts with a biomedical focus (e.g., Italy (100 %), Switzerland (86 %), Germany (86 %) and France (71 %)), whereas for other countries the focus was predominantly non-biomedical (e.g., The Netherlands (86 %) and Belgium (80 %)). Table 1 provides the data for all countries and Figure 2 visualises the overall orientation of the abstracts for each of the 11 European countries that contributed at least five abstracts.
Classification of abstracts per country.
| Country | Workshop presentations | Available abstracts | Predominantly biomedical | Predominantly psychosocial | Predominantly biopsychosocial | Not applicable | Presenters (female/male) |
|---|---|---|---|---|---|---|---|
| United Kingdom | 41 | 31 | 41 % (12) | 41 % (12) | 17 % (5) | 2 | 29 (14/15) |
| Germany | 27 | 14 | 86 % (12) | 0 % (0) | 14 % (2) | 0 | 14 (6/8) |
| Belgium | 19 | 14 | 20 % (2) | 40 % (4) | 40 % (4) | 4 | 10 (7/3) |
| The Netherlands | 16 | 10 | 14 % (1) | 57 % (4) | 29 % (2) | 3 | 7 (4/3) |
| Denmark | 15 | 14 | 46 % (6) | 15 % (2) | 38 % (5) | 1 | 13 (4/9) |
| Sweden | 12 | 9 | 38 % (3) | 50 % (4) | 13 % (1) | 1 | 8 (4/4) |
| France | 9 | 8 | 71 % (5) | 14 % (1) | 14 % (1) | 1 | 7 (6/1) |
| Finland | 8 | 6 | 50 % (3) | 17 % (1) | 33 % (2) | 0 | 6 (3/3) |
| Norway | 7 | 6 | 50 % (3) | 17 % (1) | 33 % (2) | 0 | 6 (4/2) |
| Italy | 7 | 5 | 100 % (5) | 0 % (0) | 0 % (0) | 0 | 5 (2/3) |
| Switzerland | 6 | 7 | 86 % (6) | 0 % (0) | 14 % (1) | 0 | 7 (5/2) |
| Ireland | 5 | 4 | 50 % (1) | 0 % (0) | 50 % (1) | 2 | 2 (0/2) |
| Austria | 4 | 3 | 33 % (1) | 33 % (1) | 33 % (1) | 0 | 3 (2/1) |
| Spain | 3 | 3 | 0 % (0) | 100 % (3) | 0 % (0) | 0 | 3 (3/0) |
| Portugal | 3 | 2 | 100 % (2) | 0 % (0) | 0 % (0) | 0 | 2 (2/0) |
| Iceland | 2 | 2 | 0 % (0) | 50 % (1) | 50 % (1) | 0 | 2 (2/0) |
| Hungary | 2 | 1 | 100 % (1) | 0 % (0) | 0 % (0) | 0 | 1 (1/0) |
| Poland | 1 | 1 | 100 % (1) | 0 % (0) | 0 % (0) | 0 | 1 (1/0) |
| Israel | 1 | 0 | – | – | – | – | – |
| Australia | 6 | 5 | – | – | – | – | – |
| Brazil | 3 | 2 | – | – | – | – | – |
| Canada | 6 | 5 | – | – | – | – | – |
| Chile | 1 | 0 | – | – | – | – | – |
| China | 1 | 1 | – | – | – | – | – |
| South Africa | 1 | 1 | – | – | – | – | – |
| United States | 25 | 16 | – | – | – | – | – |
| Total | 231 | 170 | 51 % (64) | 27 % (34) | 22 % (28) | 14 | 126 (70) |
-
EFIC member countries who had delegates with workshop presentations are listed above the double line and are ranked based on the number of available abstracts. Countries above the dashed line met the cut-off of 5 available abstracts and were included in the map chart (Figure 1). Non-European countries with workshop presenters are listed below the double line.
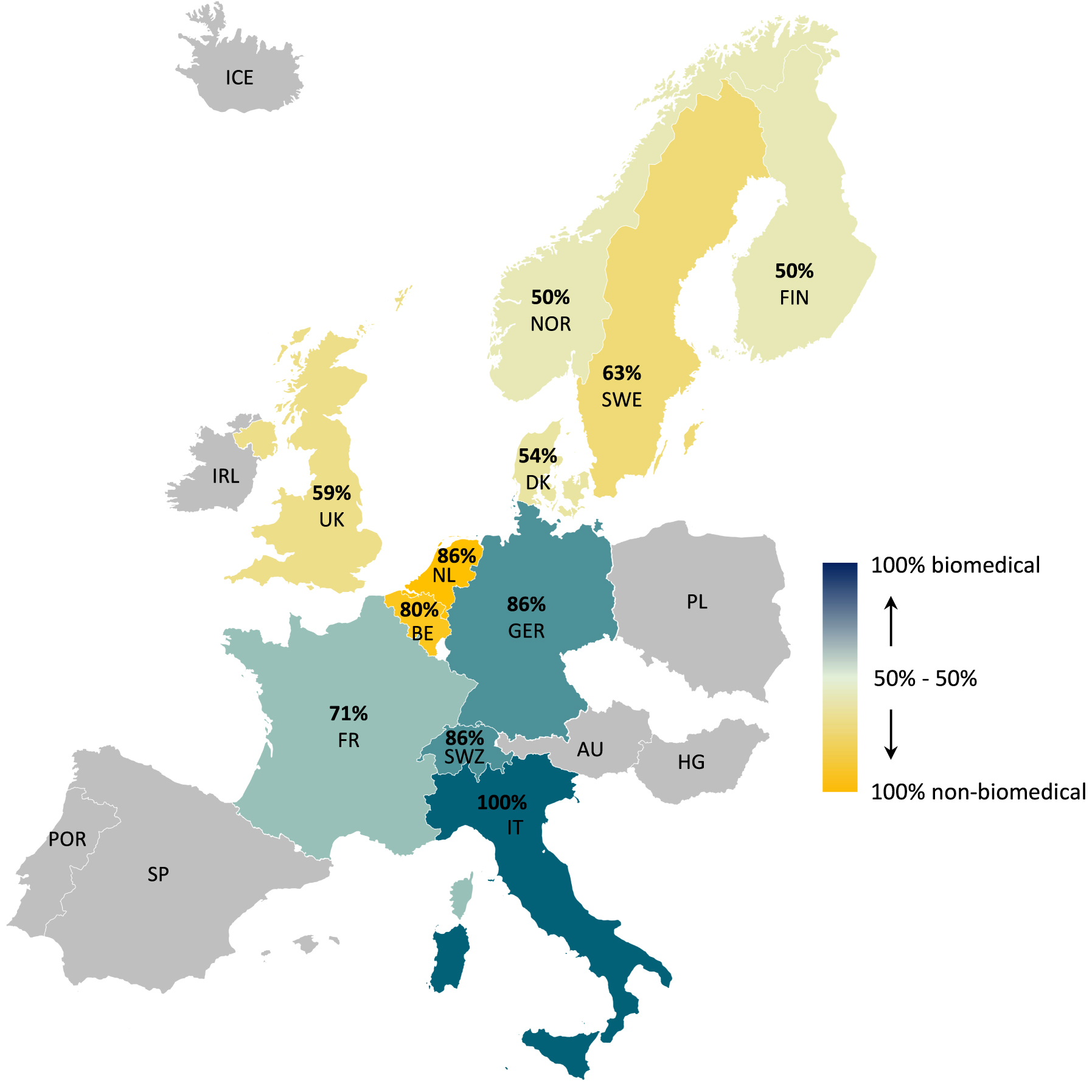
Geographical differences for the proportion of biomedical and non-biomedical presentations at the 12th EFIC congress. Countries shaded in grey or white delivered less than 5 or no eligible presentations, respectively. AU, Austria; BE, Belgium; DK, Denmark; FIN, Finland; FR, France; GER, Germany; HG, Hungary; ICE, Iceland; IRL, Ireland; IT, Italy; NL, The Netherlands; NOR, Norway; PL, Poland; POR, Portugal; SP, Spain; SWE, Sweden; SWZ, Switzerland; UK, United Kingdom.
Gender divide
Of the 126 classified abstracts, 70 presentations (i.e., 56 %) were delivered by female presenters and 56 presentations (i.e., 44 %) by male presenters. Figure 3 illustrates the proportion of female and male presenters across the different biopsychosocial domains. Women presented more non-biomedically focused abstracts (i.e., 57 vs. 43 % biomedically focused abstracts), whereas men predominately presented biomedically focused abstracts (i.e., 61 vs. 39 % non-biomedically focused abstracts).
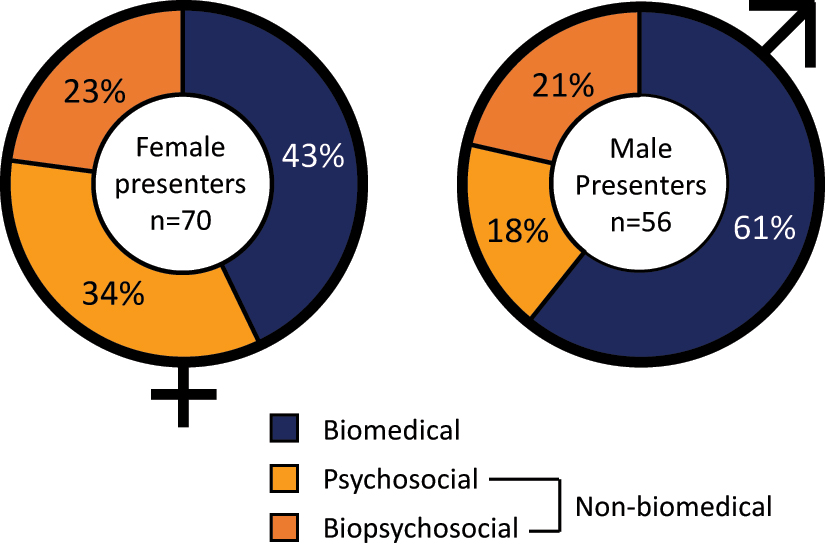
Differences between female and male presenters regarding the biopsychosocial focus of their presentations.
Discussions
In this study, we investigated whether there were geographical and/or gender differences in the biopsychosocial focus of the workshop presentations delivered at the 12th EFIC Congress (2022). Although the proportion of biomedical and non-biomedical presentations was balanced at the overall European level, geographical differences were observed between countries. Moreover, the map chart (Figure 2) revealed three geographical clusters: (1) countries with a clear majority of ‘Predominantly non-biomedical presentations’ (The Netherlands and Belgium); (2) countries with a fairly balanced ratio of biomedical and non-biomedical presentations (United Kingdom, Denmark, Norway, Sweden and Finland); and (3) countries with a clear majority of ‘Predominantly biomedical presentations’ (Italy, Germany, Switzerland and France). The geographical analysis also revealed that presenters from only 19 of the 38 EFIC member countries delivered workshop presentations at the 12th EFIC Congress.
The underlying reasons for this geographical divide are largely unknown. Whether it reflects differences in the current dominant way of thinking regarding pain management requires further research. Interestingly, the four countries with the highest proportion of ‘Predominantly biomedical’ workshop presentations at the 12th EFIC Congress are also the top-4 countries with the strongest pharmaceutical industry in Europe according to the 2021 report of the European Federation of Pharmaceutical Industries and Associations (EFPIA) (1: Switzerland; 2: France; 3: Italy; 4: Germany) [12]. Although remarkable, a direct link between industry funding and biomedical research bias cannot be established from this study as funding sources for projects were typically not mentioned. Another factor could be the presence of well-established research centres with strong research agendas in a specific domain of the biopsychosocial model, with a strong presence at international pain conferences. Further research is also needed to analyse whether this disbalance may be related to differences in national health system settings or funding arrangements [13]. It could also reflect differences in content and level of education of healthcare professionals, both medical [14] and non-medical [15], [16], [17]. Importantly, the differences identified between countries are not a criticism and hold no judgement. Rather, we believe that scientific developments in both the biomedical and the non-biomedical domains (and their interactions) are both crucial to improve pain management outcomes.
The gender analysis revealed that slightly more workshop presentations were delivered by women than by men (56 vs. 44 %). Pain is more common in women, and sex and gender differences have been identified for the biological and non-biological dimensions of pain [18], [19], [20]. Because providing first-hand female perspectives to all aspects of pain research is essential, we commend the EFIC scientific committee for providing this balance. The gender analysis also revealed that female presenters delivered proportionally more non-biomedical presentations (57 %) whereas male presenters delivered proportionally more biomedical presentations (61 %). Further research is required, but these findings may relate to differences in representation of women and men in STEM disciplines (Science, Technology, Engineering, and Mathematics). For example, women are overrepresented in Social Sciences, but are still underrepresented in many science disciplines more aligned with biomedical research, such as Biological Sciences, Natural and Physical Sciences, Computer Science and Engineering [21].
As for any study, there are several considerations and limitations to this study. We analysed the workshop presentations, rather than the keynote or poster presentations. The reason for this was that the workshop presentations are the topics that are submitted by the researchers themselves (bottom-up), whereas the keynote speakers are selected by the scientific program committee (top-down). We acknowledge that selection bias may be present as the scientific committee elected the workshops. However, we assume that the most worthwhile workshops were selected, reflecting principal pain research across Europe. More preliminary work is often presented as poster presentations. For these reasons, the workshop presentations were considered best suited to address the aims of the study. The number of workshop presentations that could be analysed was substantial (n=126), but it should be noted that 56 presentations did not provide an abstract. For the geographical analysis, we used an arbitrary cut-off of at least five workshop presentations per country to be included in the map chart. Data analyses would have been less trustworthy when a lower threshold was used and raising the threshold would have excluded more countries from the analyses. As all data are provided in Table 1, readers can easily see the impact of adjusting this threshold. Another limitation of the present study is that only analysing the 12th EFIC Congress only provides a snapshot in time and resembles only a proportion of conducted research in each country. However, strong research groups and research agendas do not develop overnight, so we assume some continuity in the topics as there is also some continuity in presenters across conferences [22].
In conclusion, the findings of this study suggest that there are substantial geographical differences between countries regarding the biopsychosocial focus of workshop presentations at the 12th EFIC Congress. With slightly more female than male presenters, there seems no gender gap, although women present more frequently on non-biomedical topics whereas men present more frequently on biomedical topics. Future research will have to reveal whether this geographical divide is a momentary occurrence or a more entrenched phenomenon, and whether a more balanced biopsychosocial approach to pain research across countries has to be stimulated.
-
Research funding: None.
-
Author contributions: All authors have accepted responsibility for the entire content of this manuscript and approved its submission.
-
Competing interests: The authors have no conflicts of interest to declare.
References
1. Fillingim, RB. Individual differences in pain: understanding the mosaic that makes pain personal. Pain 2017;158(Suppl 1):S11–8. https://doi.org/10.1097/J.PAIN.0000000000000775.Search in Google Scholar PubMed PubMed Central
2. Meints, SM, Edwards, RR. Evaluating psychosocial contributions to chronic pain outcomes. Prog NeuroPsychopharmacol Biol Psychiatry 2018;87:168–82. https://doi.org/10.1016/J.PNPBP.2018.01.017.Search in Google Scholar
3. Kamper, S, Apeldoorn, A, Chiarotto, A, Smeets, R, Ostelo, R, Guzman, J, et al.. Multidisciplinary biopsychosocial rehabilitation for chronic low back pain: cochrane systematic review and meta-analysis. BMJ 2015;350:h444:1–11. https://doi.org/10.1136/BMJ.H444.Search in Google Scholar PubMed PubMed Central
4. Nicholas, M, Vlaeyen, JWS, Rief, W, Barke, A, Aziz, Q, Benoliel, R, et al.. The IASP classification of chronic pain for ICD-11: chronic primary pain. Pain 2019;160:28–37. https://doi.org/10.1097/J.PAIN.0000000000001390.Search in Google Scholar PubMed
5. Nicholas, MK. The biopsychosocial model of pain 40 years on: time for a reappraisal? Pain 2022;163:S3–14. https://doi.org/10.1097/J.PAIN.0000000000002654.Search in Google Scholar
6. Pincus, T, Kent, P, Bronfort, G, Loisel, P, Pransky, G, Hartvigsen, J. Twenty-five years with the biopsychosocial model of low back pain-is it time to celebrate? A report from the twelfth international forum for primary care research on low back pain. Spine 2013;38:2118–23. https://doi.org/10.1097/BRS.0B013E3182A8C5D6.Search in Google Scholar PubMed
7. Carr, DB, Bradshaw, YS. Time to flip the pain curriculum? Anesthesiology 2014;120:12–4. https://doi.org/10.1097/ALN.0000000000000054.Search in Google Scholar PubMed
8. National chapters of EFIC – European pain federation 2018. EFIC. https://europeanpainfederation.eu/organisation/national-chapters-of-efic/ [Accessed 3 Nov 2022].Search in Google Scholar
9. Objectives – European pain federation 2022. EFIC. https://europeanpainfederation.eu/history/objectives/ [Accessed 3 Nov 2022].Search in Google Scholar
10. Scientific programme – European pain federation 2022. EFIC. https://efic2022.abstractserver.com/program/#/details/sessions/179 [Accessed 6 May 2022].Search in Google Scholar
11. Black, NM, Sullivan, SJ, Mani, R. A biopsychosocial understanding of lower back pain: content analysis of online information. Eur J Pain 2018;22:728–44. https://doi.org/10.1002/ejp.1158.Search in Google Scholar PubMed
12. EFPIA. The pharmaceutical industry in figures (2021). Brussels, Belgium; 2021. Available from: https://www.efpia.eu/publications/downloads/efpia/the-pharmaceutical-industry-in-figures-2021/#/.Search in Google Scholar
13. Traeger, AC, Buchbinder, R, Elshaug, AG, Croft, PR, Maher, CG. Care for low back pain: can health systems deliver? Bull World Health Organ 2019;97:423–33. https://doi.org/10.2471/BLT.18.226050.Search in Google Scholar PubMed PubMed Central
14. Shipton, EE, Bate, F, Garrick, R, Steketee, C, Shipton, EA, Visser, EJ. Systematic review of pain medicine content, teaching, and assessment in medical school curricula internationally. Pain Ther 2018;7:139. https://doi.org/10.1007/S40122-018-0103-Z.Search in Google Scholar
15. Chatchumni, M, Eriksson, H, Mazaheri, M. A scoping review of pain management education programs (PMEPs): do they prepare nurses to deal with patients’ postoperative pain? Pain Res Manag 2020;15:4062493. https://doi.org/10.1155/2020/4062493.Search in Google Scholar PubMed PubMed Central
16. Darnall, BD, Scheman, J, Davin, S, Burns, JW, Murphy, JL, Wilson, AC, et al.. Pain psychology: a global needs assessment and national call to action. Pain Med 2016;17:250. https://doi.org/10.1093/PM/PNV095.Search in Google Scholar
17. Hoeger Bement, MK, stMarie, BJ, Nordstrom, TM, Christensen, N, Mongoven, JM, Koebner, IJ, et al.. An interprofessional consensus of core competencies for prelicensure education in pain management: curriculum application for physical therapy. Phys Ther 2014;94:451–65. https://doi.org/10.2522/PTJ.20130346.Search in Google Scholar
18. Bartley, EJ, Fillingim, RB. Sex differences in pain: a brief review of clinical and experimental findings. Br J Anaesth 2013;111:52–8. https://doi.org/10.1093/BJA/AET127.Search in Google Scholar
19. Rosen, S, Ham, B, Mogil, JS. Sex differences in neuroimmunity and pain. J Neurosci Res 2017;95:500–8. https://doi.org/10.1002/jnr.23831.Search in Google Scholar PubMed
20. Keogh, E. Sex and gender differences in pain: past, present, and future. Pain 2022;163:S108–16. https://doi.org/10.1097/j.pain.0000000000002738.Search in Google Scholar PubMed
21. Su, R, Rounds, J. All STEM fields are not created equal: people and things interests explain gender disparities across STEM fields. Front Psychol 2015;6:189. https://doi.org/10.3389/FPSYG.2015.00189/BIBTEX.Search in Google Scholar
22. Meet the speakers – pain in Europe 2019. EFIC. https://efic-congress.org/2019/meet-the-speakers/ [Accessed 15 Nov 2022].Search in Google Scholar
© 2023 the author(s), published by De Gruyter, Berlin/Boston
This work is licensed under the Creative Commons Attribution 4.0 International License.
Articles in the same Issue
- Frontmatter
- Editorial Comment
- What do we mean by “biopsychosocial” in pain medicine?
- Systematic Review
- The efficacy of manual therapy on HRV in those with long-standing neck pain: a systematic review
- Clinical Pain Research
- Development of a binary classifier model from extended facial codes toward video-based pain recognition in cancer patients
- Experience and usability of a website containing research-based knowledge and tools for pain self-management: a mixed-method study in people with high-impact chronic pain
- Effect on orofacial pain in patients with chronic pain participating in a multimodal rehabilitation programme – a pilot study
- Analysis of Japanese nationwide health datasets: association between lifestyle habits and prevalence of neuropathic pain and fibromyalgia with reference to dementia-related diseases and Parkinson’s disease
- Impact of antidepressant medication on the analgetic effect of repetitive transcranial magnetic stimulation treatment of neuropathic pain. Preliminary findings from a registry study
- Does lumbar spinal decompression or fusion surgery influence outcome parameters in patients with intrathecal morphine treatment for persistent spinal pain syndrome type 2 (PSPS-T2)
- Original Experimentals
- Low back-pain among school-teachers in Southern Tunisia: prevalence and predictors
- Economic burden of osteoarthritis – multi-country estimates of direct and indirect costs from the BISCUITS study
- Demographic and clinical factors associated with psychological wellbeing in people with chronic, non-specific musculoskeletal pain engaged in multimodal rehabilitation: –a cross-sectional study with a correlational design
- Interventional pathway in the management of refractory post cholecystectomy pain (PCP) syndrome: a 6-year prospective audit in 60 patients
- Original Articles
- Preoperatively assessed offset analgesia predicts acute postoperative pain following orthognathic surgery
- Oxaliplatin causes increased offset analgesia during chemotherapy – a feasibility study
- Effects of conditioned pain modulation on Capsaicin-induced spreading muscle hyperalgesia in humans
- Effects of oral morphine on experimentally evoked itch and pain: a randomized, double-blind, placebo-controlled trial
- The potential effect of walking on quantitative sensory testing, pain catastrophizing, and perceived stress: an exploratory study
- What matters to people with chronic musculoskeletal pain consulting general practice? Comparing research priorities across different sectors
- Is there a geographic and gender divide in Europe regarding the biopsychosocial approach to pain research? An evaluation of the 12th EFIC congress
Articles in the same Issue
- Frontmatter
- Editorial Comment
- What do we mean by “biopsychosocial” in pain medicine?
- Systematic Review
- The efficacy of manual therapy on HRV in those with long-standing neck pain: a systematic review
- Clinical Pain Research
- Development of a binary classifier model from extended facial codes toward video-based pain recognition in cancer patients
- Experience and usability of a website containing research-based knowledge and tools for pain self-management: a mixed-method study in people with high-impact chronic pain
- Effect on orofacial pain in patients with chronic pain participating in a multimodal rehabilitation programme – a pilot study
- Analysis of Japanese nationwide health datasets: association between lifestyle habits and prevalence of neuropathic pain and fibromyalgia with reference to dementia-related diseases and Parkinson’s disease
- Impact of antidepressant medication on the analgetic effect of repetitive transcranial magnetic stimulation treatment of neuropathic pain. Preliminary findings from a registry study
- Does lumbar spinal decompression or fusion surgery influence outcome parameters in patients with intrathecal morphine treatment for persistent spinal pain syndrome type 2 (PSPS-T2)
- Original Experimentals
- Low back-pain among school-teachers in Southern Tunisia: prevalence and predictors
- Economic burden of osteoarthritis – multi-country estimates of direct and indirect costs from the BISCUITS study
- Demographic and clinical factors associated with psychological wellbeing in people with chronic, non-specific musculoskeletal pain engaged in multimodal rehabilitation: –a cross-sectional study with a correlational design
- Interventional pathway in the management of refractory post cholecystectomy pain (PCP) syndrome: a 6-year prospective audit in 60 patients
- Original Articles
- Preoperatively assessed offset analgesia predicts acute postoperative pain following orthognathic surgery
- Oxaliplatin causes increased offset analgesia during chemotherapy – a feasibility study
- Effects of conditioned pain modulation on Capsaicin-induced spreading muscle hyperalgesia in humans
- Effects of oral morphine on experimentally evoked itch and pain: a randomized, double-blind, placebo-controlled trial
- The potential effect of walking on quantitative sensory testing, pain catastrophizing, and perceived stress: an exploratory study
- What matters to people with chronic musculoskeletal pain consulting general practice? Comparing research priorities across different sectors
- Is there a geographic and gender divide in Europe regarding the biopsychosocial approach to pain research? An evaluation of the 12th EFIC congress