Pituitary dysfunction from an unruptured ophthalmic internal carotid artery aneurysm with improved 2-year follow-up results: A case report
-
Meng Qi
 ,
Ming Ye
,
Ming Ye

Abstract
Internal carotid artery (ICA) supraclinoid segment aneurysms extending into the sellar region and leading to pituitary dysfunction are a rare occurrence. To date, long-term follow up of pituitary function 2 years post-treatment has never been reported. Herein, we present a case of pituitary dysfunction due to an unruptured ophthalmic segment internal carotid artery aneurysm and report improved 2-year follow-up results. A 76-year-old male presented with disturbed consciousness due to hyponatremia, which was caused by hypoadrenocorticism resulting from pituitary dysfunction complicated by hypogonadism and hypothyroidism. Computed tomography angiography revealed an intracranial aneurysm of the ophthalmic segment of the right ICA with an intrasellar extension. Thus, digital subtraction angiography and coil embolization were performed, followed by hormone replacement therapy. A 2-year follow-up revealed a partial improvement in the pituitary function, including complete restoration of thyroid-stimulating hormone level and other thyroid hormones levels, and partial restoration of testosterone levels, followed by discontinuation of thyroid hormone replacement therapy. However, the mechanisms of such pituitary dysfunction and the effects of various treatments, including clipping and coiling, on different hormones of pituitary function recovery remain unclear. A long-term follow-up of >2 years may elucidate the pituitary function recovery post-treatment and provide a medication adjustment for hormone replacement therapy.
1 Introduction
The occurrence of intracranial aneurysms extending into the sellar region and resulting in pituitary dysfunction is relatively rare. A large cohort study of more than 4000 patients with hypopituitarism at the Mayo Clinic reported that a prevalence of <0.2% pituitary dysfunction attributed to a sellar aneurysm [1]. To the best of our knowledge, only two cases of an unruptured internal carotid artery (ICA) supraclinoid segment aneurysm leading to pituitary dysfunction have been reported to date [2,3]. Herein, we present a case, which would be an addition to the previously reported cases of pituitary dysfunction due to an intracranial supraclinoid aneurysm, and report improved results with an extended 2-year follow-up.
2 Case report
A 76-year-old male was admitted to our hospital because of disturbed consciousness due to hyponatremia two months before admission. His medical history comprised hypertension with good control under medication without diabetes and other complicated diseases. Magnetic resonance imaging (MRI) revealed a sellar mass that was considered to be a large intracranial aneurysm (Fig. 1a). Computed tomography angiography (CTA) as well as digital subtraction angiography (DSA) revealed a right ICA supraclinoid segment aneurysm (Figs. 1b and 2a). The patient’s endocrine profile suggested a severe decline of testosterone, and decrease of AM cortisol, luteinizing hormone, estradiol, thyroid-stimulating hormone (TSH), free T3 (FT3) and free T4 (FT4; free thyroxine) levels and elevation in prolactin levels (Table 1). Before admission to our department, the patient received sodium supplement and hormone replacement therapy with hydrocortisone and testosterone at a local hospital, leading to recovery from the disturbed consciousness. In addition, levothyroxine was prescribed for thyroid hormone replacement, and bromcriptine was not prescribed because of marginal elevation of prolactin.
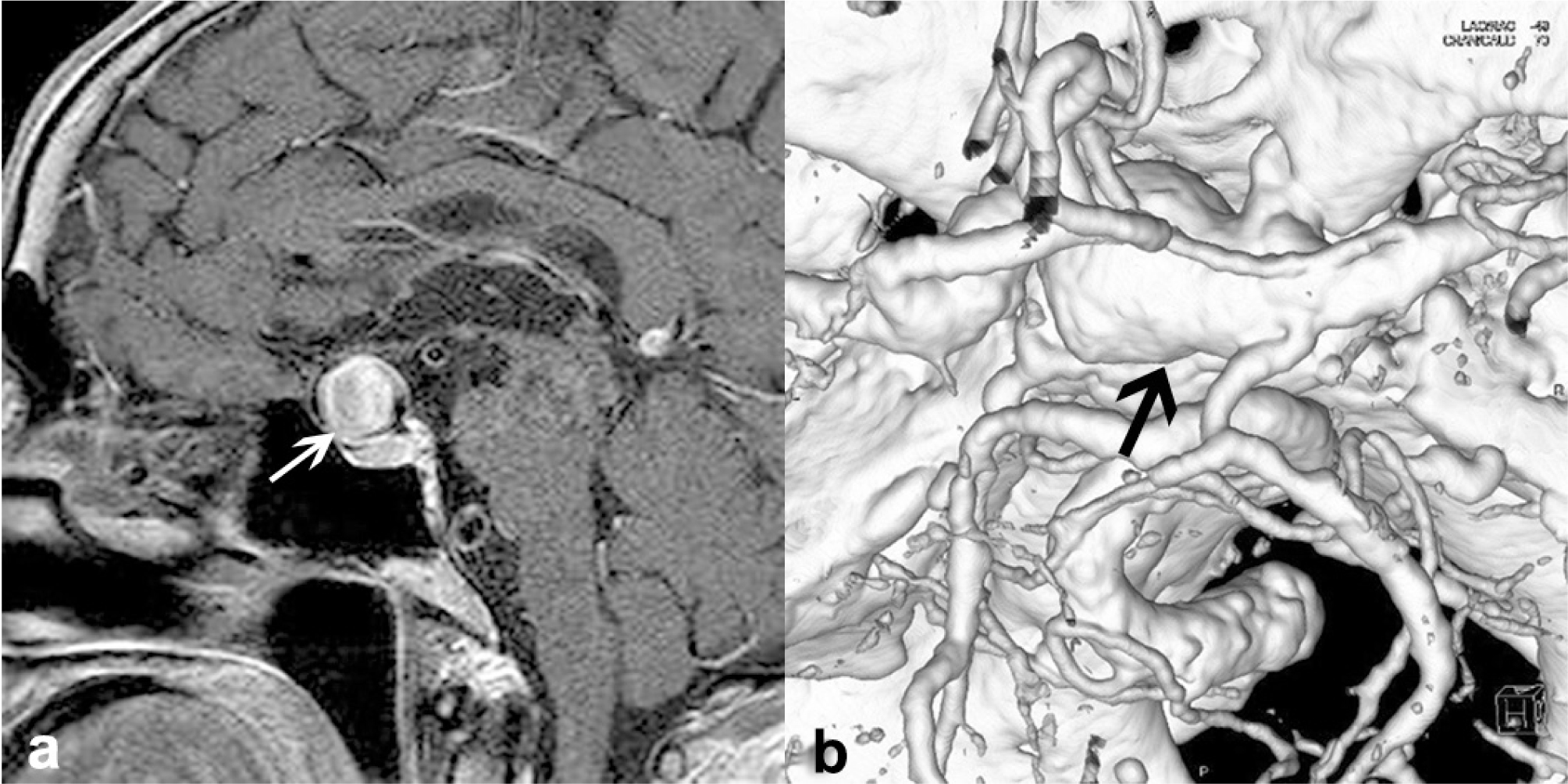
Pre-treatment magnetic resonance imaging (MRI) and computed tomography (CT) angiography of the aneurysm
MRI T1-weighted sequences mid-sagittal section with contrast (a) shows a large intrasellar lesion (white arrow) with an unusual pattern of enhancement, which is different from a pituitary adenoma and necessary for further investigation for an aneurysm. CT angiography 3D reconstruction (b) demonstrates a large right supraclinoid ICA aneurysm (black arrow) extending into the sellar region.
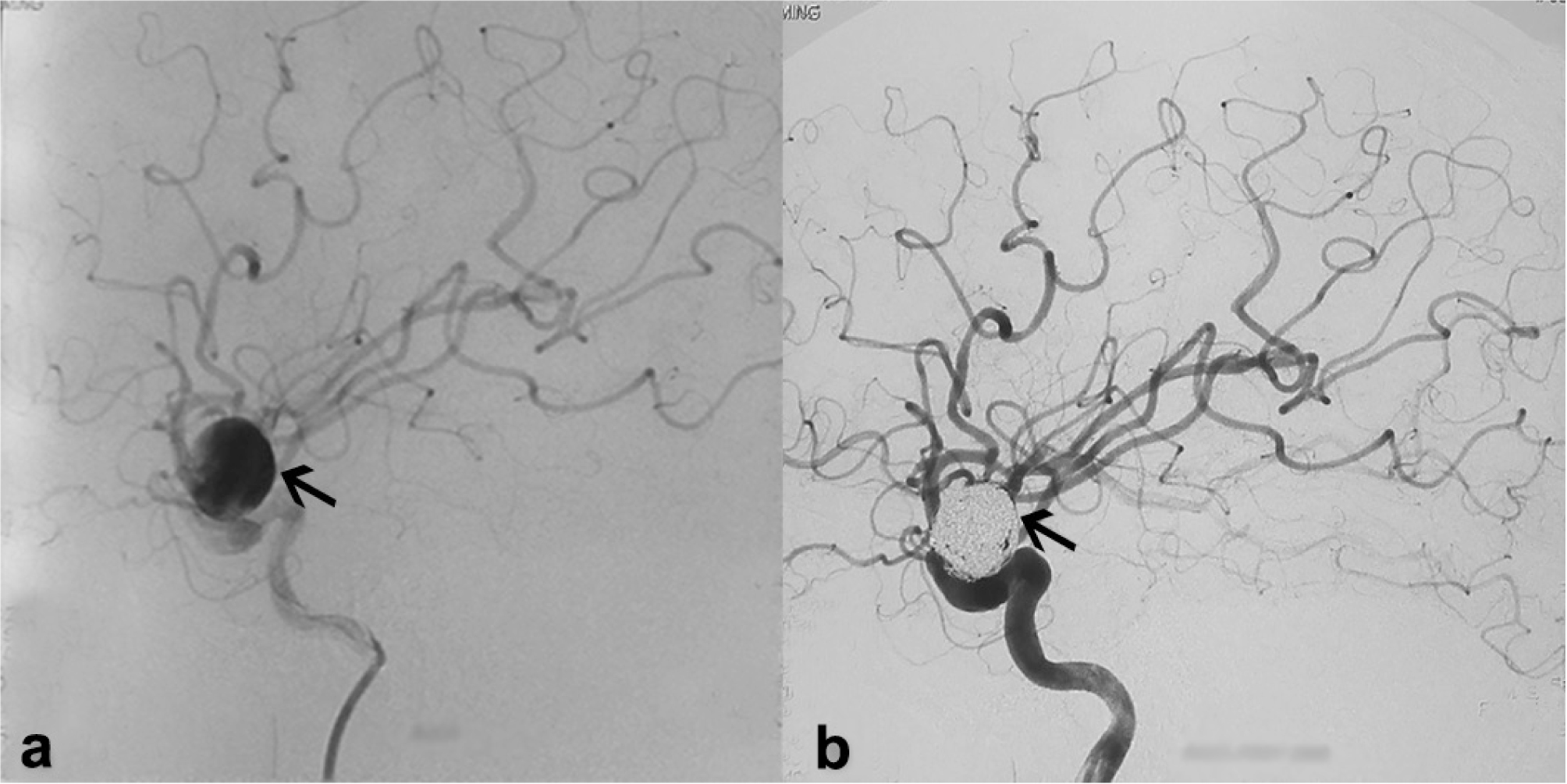
Digital subtraction angiography (DSA) of the aneurysm before and after coiling
DSA lateral projection of the aneurysm (left black arrow) pre-treatment (a) and after coiling (right black arrow) (b) shows the right ophthalmic segment internal carotid artery aneurysm.
Endocrine tests of hormones before treatment and 2 years after coiling of the aneurysm
| Hormone type | Before treatment | 2-year follow up | Normal reference |
|---|---|---|---|
| Morning cortisol | 0.88↓ | 0.6↓ | 3.7-19.4ug/dL |
| Afternoon cortisol | 1.13 | 2.0 | <4ug/dL |
| FSH | 1.69 | 4.36 | 1.27-19.26IU/L |
| LH↓ | 1.05↓ | 0.32↓ | 3.1-34.6IU/L |
| PRL | 17.75↑ | 19.10↑ | 2.1-17.7ng/ml |
| TSH# | 0.32↓ | 1.91 | 0.34-5.6 mIU/ml |
| Testosterone* | 0.00↓↓↓ | 7.82↓↓ | 241-827ng/dL |
| Estradiol | 16.00 | 3.19 | 0-39.8pg/ml |
| FT3# | 1.89↓ | 3.19 | 2.77-6.31pmol/L |
| FT4# | 9.28↓ | 11.21 | 10.53-24.57pmol/L |
FSH, follicle-stimulating hormone; LH, luteinizing hormone; PRL, prolactin; TSH, thyroid-stimulating hormone; FT3, free T3; FT4, free thyroxine; ↓ decreased, ↑ elevated, more arrows mean severity, * partial or #full recovery of hormone after coiling compared to the same hormone before coiling
At our hospital, we performed placement of coils into the aneurysm for treatment (Fig. 2b) 7 days after admission followed by a continued hydrocortisone, levothyroxine, and testosterone replacement therapy. The post-treatment recovery of the patient was unremarkable without any neurological deficit. Furthermore, we performed a 2-year follow-up to check the patient’s hormone levels (Table 1) and observed an improvement in the levels of testosterone (partial), TSH (complete), FT3 (complete), and FT4 (complete), but not in those of other examined hormones. Eventually, levothyroxine was discontinued for complete restoration of thyroid hormone levels.
Informed consent
Informed consent has been obtained from the participant included in the study.
Ethical approval
The research related to human use has complied with all the relevant national regulations, institutional policies, and is in accordance to the tenets of the Helsinki Declaration, and has been approved by the authors’ institutional review board or equivalent committee.
3 Discussion
Previous literature reported that aneurysms projecting into the sellar region account for <2% of all intracranial aneurysms [1]. Hanak et al. [4] classified intrasellar aneurysms into two types: (a) infradiaphragmatic, arising from the cavernous/clinoid segment ICA with medial extension into the sella; and (b) supradiaphragmatic, arising from the ophthalmic segment of ICA or anterior communicating artery with inferomedial extension into the sella. Our presented case belonged to the latter group, arising from the ophthalmic segment of ICA close to the origin of the anterior choroidal artery. In addition, pituitary dysfunction caused by a sellar aneurysm is relatively rare with a reported prevalence of 0.17% in a large cohort of over 4000 patients with hypopituitarism [1]. The aneurysm extended into the carotid cave and suprasellar region resulting in the mechanical compression of the pituitary stalk and gland or vascular compression of the artery supplying the pituitary gland, leading to pituitary ischemia [5,6], and causing pituitary dysfunction that manifested in the serum hormone levels of patients. It is reported that the leading endocrine insufficiencies are hyperprolactinemia and hypogonadism [4], and our patient apparently had hypogonadism and slight hyperprolactinemia, in addition to obvious hypoadrenocorticism and hypothyroidism.
Typically, the treatment of intracranial aneurysms of significant size is challenging, and includes microsurgical operation and endovascular obliteration. Recovery of endocrine function is rare even postoperatively [6]. For the treatment of such aneurysms, clinicians have established clipping of the aneurysm, proximal occlusion or trapping with/without distal bypass, and coiling embolization with or without the assistance of balloon or stent. However, the compression to the pituitary gland persists because of the coils in the aneurysm, thus, necessitating the hormone replacement therapy [7, 8]. A flow diversion device with pipeline stent placement has also been reported for treatment, with a certain rate of major complications such as major ipsilateral thrombosis, intraparenchymal hemorrhage, and neurologic death as well as delayed panhypopituitarism partly caused by a compromised blood supply to the pituitary gland because of the flow diversion to ICA [9,10,11].
To date, only two cases of supradiaphragmatic intrasellar aneurysms with pituitary insufficiency have been reported, which were treated by microsurgical clipping followed by resection or pipeline placement respectively [2,3]. In our case, the aneurysm had a narrow neck, which was suitable for embolization, and the patient was in his advanced age (76 years) at admission; thus, embolization with coils was selected as a prior treatment rather than surgery. In addition, we used coiling alone for treatment without stent placement in our patient.
Heshmati et al. reported that pituitary dysfunction secondary to an intrasellar aneurysm is usually permanent and unlikely to improve despite successful treatment of the aneurysm [1]. A 1-year follow-up of a supradiaphragmatic intrasellar aneurysm did not demonstrate recovery of the pituitary function [2]. Conversely, a 1-month follow-up of another patient with a supradiaphragmatic aneurysm and pituitary insufficiency exhibited excellent recovery with hormone supplementation; however, serum hormone levels were not specified in the follow-up [3]. In addition, an 8-year follow-up of a patient with pituitary dysfunction caused by a giant cavernous carotid aneurysm treated with high-flow bypass demonstrated pituitary function recovery and shrinkage of the aneurysm [12]. In our case, a 2-year follow-up of serum hormone levels performed without an intermediate-stage examination revealed complete or partial improvement of levels of certain hormones such as TSH, FT3, FT4, and testosterone. Notably, the complete restoration of TSH, FT3, and FT4 levels resulted in the discontinuation of levothyroxine administration. However, the mechanism of long-term pituitary dysfunction or the effects of microsurgical and endovascular treatment on the pituitary function recovery remain unclear. In addition, it remains unclear why levels of TSH and thyroid hormones restored to normal compared with those of other hormones. Nonetheless, pituitary hormone replacement could be prescribed with its synthetic equivalents, and reevaluation of hormone levels may suggest the medication adjustment for hormone replacement therapy. Therefore, a longer-term follow-up of >2 years may elucidate the condition of the pituitary function for this patient. In our patient, imaging tests such as CTA or DSA were not performed at follow-up, because of the denial of the family members considering the age of the patient (78 years at 2-year follow-up); thus, the post-treatment variation in the size of the aneurysm remains unknown.
Furthermore, the duration of pituitary insufficiency and the extent of pituitary compression may also play a role in the endocrine recovery after treatment [5]. While it cannot be precisely ascertained when hypopituitarism started in our patient, his symptoms appeared approximately 2 months before endovascular treatment of the aneurysm, suggesting that this relatively short period may have been a favorable factor for the partial recovery of the pituitary function.
To date, pituitary dysfunction secondary to supraclinoid ICA aneurysms remains partially specified. While microsurgical or endovascular techniques can help treat aneurysms, pituitary dysfunction warrants the administration of synthetic equivalents for replacement of insufficient hormones. In addition, as the mechanisms of such type of pituitary dysfunction and the effect of various treatments on different hormones of pituitary function recovery remain unclear, a long-term follow-up of >2 years may yield more information about the post-treatment pituitary function recovery and suggest the medication adjustment for hormone replacement therapy.
Acknowledgement
This work was supported by a grant from Intramural Research Program of Basic and Clinical Study, Xuanwu Hospital, Capital Medical University and Beijing Municipal Human Resources and Social Security Bureau. The sponsors had no role in the design or conduct of this research.
Conflict of interest: Authors state no conflict of interest.
References
[1] Heshmati HM, Fatourechi V, Dagam SA, Piepgras DG. Hypopituitarism caused by intrasellar aneurysms. Mayo Clin Proc, 2001, 76(8): 789-79310.1016/S0025-6196(11)63222-9Search in Google Scholar PubMed
[2] Klose S, Kopf D, Lehnert H. Giant intrasellar carotid aneurysm - an unusual cause of panhypopituitarism. Exp Clin Endocrinol Diabetes, 2005, 113(9): 551-55310.1055/s-2005-865808Search in Google Scholar PubMed
[3] Ding D, Mehta GU, Liu KC. Pituitary insufficiency from large unruptured supraclinoid internal carotid artery aneurysm. Br J Neurosurg, 2014, 28(2): 290-29210.3109/02688697.2013.829559Search in Google Scholar PubMed
[4] Hanak BW, Zada G, Nayar VV, Thiex R, Du R, Day AL, et al. Cerebral aneurysms with intrasellar extension: a systematic review of clinical, anatomical, and treatment characteristics. J Neurosurg, 2012, 116(1): 164-17810.3171/2011.9.JNS11380Search in Google Scholar PubMed
[5] Tan LA, Sandler V, Todorova-Koteva K, Levine L, Lopes DK, Moftakhar R. Recovery of pituitary function following treatment of an unruptured giant cavernous carotid aneurysm using Surpass flow-diverting stents. J Neurointerv Surg, 2015, 7(6): e2010.1136/neurintsurg-2014-011233.repSearch in Google Scholar PubMed
[6] Tungaria A, Kumar V, Garg P, Jaiswal AK, Behari S. Giant, thrombosed, sellar-suprasellar internal carotid artery aneurysm with persistent, primitive trigeminal artery causing hypopituitarism. Acta Neurochir (Wien), 2011, 153(5): 1129-113310.1007/s00701-010-0931-zSearch in Google Scholar PubMed
[7] Fernandez-Real JM, Fernandez-Castaner M, Villabona C, Sagarra E, Gomez-Saez JM, Soler J. Giant intrasellar aneurysm presenting with panhypopituitarism and subarachnoid hemorrhage: case report and literature review. Clin Investig, 1994, 72(4): 302-30610.1007/BF00180045Search in Google Scholar PubMed
[8] Gungor A, Gokkaya N, Bilen A, Bilen H, Akbas EM, Karadeniz Y, et al. Pituitary Insufficiency and Hyperprolactinemia Associated with Giant Intra- and Suprasellar Carotid Artery Aneurysm. Case Rep Med, 2015, Article ID 53619110.1155/2015/536191Search in Google Scholar PubMed PubMed Central
[9] Becske T, Kallmes DF, Saatci I, McDougall CG, Szikora I, Lanzino G, et al. Pipeline for uncoilable or failed aneurysms: results from a multicenter clinical trial. Radiology, 2013, 267(3): 858-86810.1148/radiol.13120099Search in Google Scholar PubMed
[10] Becske T, Potts MB, Shapiro M, Kallmes DF, Brinjikji W, Saatci I, et al. Pipeline for uncoilable or failed aneurysms: 3-year follow-up results. J Neurosurg, 2017, 127(1): 81-8810.3171/2015.6.JNS15311Search in Google Scholar PubMed
[11] Hall J, Caputo C, Chung C, Holt M, Wang YY. Delayed pan-hypopituitarism as a complication following endovascular treatment of bilateral internal carotid artery aneurysms. A case report and review. Br J Neurosurg, 2015, 29(2): 303-30510.3109/02688697.2014.969681Search in Google Scholar PubMed
[12] Ono H, Inoue T, Kunii N, Tanishima T, Tamura A, Saito I, et al. Giant cavernous carotid aneurysm causing pituitary dysfunction: Pituitary function recovery with high-flow bypass. Surg Neurol Int, 2017, 8: 18010.4103/sni.sni_178_17Search in Google Scholar PubMed PubMed Central
© 2018 Meng Qi et al., published by De Gruyter
This work is licensed under the Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 License.
Articles in the same Issue
- Regular Articles
- Cleidocranial dysplasia-dental disorder treatment and audiology diagnosis
- A hybrid neural network – world cup optimization algorithm for melanoma detection
- Early administration of venovenous extracorporeal life support for status asthmaticus during anaesthetic induction: case report and literature review
- Assessment of maximal isometric hand grip strength in school-aged children
- Evaluation of a neurokinin-1 antagonist in preventing multiple-day cisplatin-induced nausea and vomiting
- Value of continuous video EEG and EEG responses to thermesthesia stimulation in prognosis evaluation of comatose patients after cardiopulmonary resuscitation
- Platelet-rich plasma protects HUVECs against oX-LDL-induced injury
- Pharmacoeconomics of three therapeutic schemes for anti-tuberculosis therapy induced liver injury in China
- Small-cell lung cancer presenting as fatal pulmonary hemorrhage
- Correlation of retinopathy of prematurity with bronchopulmonary dysplasia
- Prognosis of treatment outcomes by cognitive and physical scales
- The efficacy of radiofrequency hyperthermia combined with chemotherapy in the treatment of advanced ovarian cancer
- Arcuate Fasciculus in Autism Spectrum Disorder Toddlers with Language Regression
- Aesthetic dental procedures: legal and medico-legal implications
- Blood transfusion in children: the refusal of Jehovah’s Witness parents’
- Burnout among anesthetists and intensive care physicians
- Relationship of HS CRP and sacroiliac joint inflammation in undifferentiated spondyloarthritis
- Ethical and legal issues in gestational surrogacy
- Effects of arginine vasopressin on migration and respiratory burst activity in human leukocytes
- Associations of diabetic retinopathy with retinal neurodegeneration on the background of diabetes mellitus. Overview of recent medical studies with an assessment of the impact on healthcare systems
- Pituitary dysfunction from an unruptured ophthalmic internal carotid artery aneurysm with improved 2-year follow-up results: A case report
- Effectiveness of treatment with endostatin in combination with emcitabine, carboplatin, and gemcitabine in patients with advanced non-small cell lung cancer: a retrospective study
- Piercing and tattoos in adolescents: legal and medico-legal implications
- The central importance of information in cosmetic surgery and treatments
- Penile calciphylaxis in a patient with end-stage renal disease: a case report and review of the literature
- Serum CA72-4 as a biomarker in the diagnosis of colorectal cancer: A meta-analysis
- Association between uric acid and metabolic syndrome in elderly women
- Distinct expression and prognostic value of MS4A in gastric cancer
- MAPK pathway involved in epidermal terminal differentiation of normal human epidermal keratinocytes
- Association of central obesity with sex hormonebinding globulin: a cross-sectional study of 1166 Chinese men
- Successful endovascular therapy in an elderly patient with severe hemorrhage caused by traumatic injury
- Inflammatory biomarkers and risk of atherosclerotic cardiovascular disease
- Related factors of early mortality in young adults with cerebral hemorrhage
- Growth suppression of glioma cells using HDAC6 inhibitor, tubacin
- Post-stroke upper limb spasticity incidence for different cerebral infarction site
- The esophageal manometry with gas-perfused catheters
- MMP-2 and TIMP-2 in patients with heart failure and chronic kidney disease
- Genetic testing: ethical aspects
- Intervention for physician burnout: A systematic review
- The melanin-concentrating hormone system in human, rodent and avian brain
- Clinical effects of piribedil in adjuvant treatment of Parkinson’s Disease: A meta-analysis
- Identification of a novel BRAF Thr599dup mutation in lung adenocarcinoma
- Adrenal incidentaloma – diagnostic and treating problem – own experience
- Common illnesses in tropical Asia and significance of medical volunteering
- Genetic risk in insurance field
- Genetic testing and professional responsibility: the italian experience
- The mechanism of mitral regurgitant jets identified by 3-dimensional transesophageal echocardiography
- Control of blood pressure and cardiovascular outcomes in type 2 diabetes
- Pseudomesotheliomatous primary squamous cell lung carcinoma: The first case reported in Turkey and a review of the literature
- Diagnostic efficacy of serum 1,3-β-D-glucan for invasive fungal infection: An update meta-analysis based on 37 case or cohort studies
- GPER was associated with hypertension in post-menopausal women
- Metabolic activity of sulfate-reducing bacteria from rodents with colitis
- Association of miRNA122 & ADAM17 with lipids among hypertensives in Nigeria
- The efficacy and safety of enoxaparin: a meta-analysis
- Cuffed versus uncuffed endotracheal tubes in pediatrics: a meta-analysis
- Thresholding for medical image segmentation for cancer using fuzzy entropy with level set algorithm
- Sleep deprivation in Intensive Care Unit – systematic review
- Benefits of computed tomography in reducing mortality in emergency medicine
- Ipragliflozin ameliorates liver damage in non-alcoholic fatty liver disease
- Limits of professional competency in nurses working in Nicu
- MDA-19 suppresses progression of melanoma via inhibiting the PI3K/Akt pathway
- The effect of smoking on posttraumatic pseudoarthrosis healing after internal stabilization, treated with platelet rich plasma (PRP)
- Partial deletion of the long arm of chromosome 7: a case report
- Meta-analysis of PET/CT detect lymph nodes metastases of cervical cancer
- High Expression of NLRC5 is associated with prognosis of gastric cancer
- Is monitoring mean platelet volume necessary in breast cancer patients?
- Resectable single hepatic epithelioid hemangioendothelioma in the left lobe of the liver: a case report
- Epidemiological study of carbapenem-resistant Klebsiella pneumoniae
- The CCR5-Delta32 genetic polymorphism and HIV-1 infection susceptibility: a meta-analysis
- Phenotypic and molecular characterisation of Staphylococcus aureus with reduced vancomycin susceptibility derivated in vitro
- Preliminary results of Highly Injectable Bi-Phasic Bone Substitute (CERAMENT) in the treatment of benign bone tumors and tumor-like lesions
- Analysis of patient satisfaction with emergency medical services
- Guillain-Barré syndrome and Low back pain: two cases and literature review
- HELLP syndrome complicated by pulmonary edema: a case report
- Pharmacokinetics of vancomycin in patients with different renal function levels
- Recurrent chronic subdural hematoma: Report of 13 cases
- Is awareness enough to bring patients to colorectal screening?
- Serum tumor marker carbohydrate antigen 125 levels and carotid atherosclerosis in patients with coronary artery disease
- Plastic treatment for giant pseudocyst after incisional hernia mesh repair: a case report and comprehensive literature review
- High expression levels of fascin-1 protein in human gliomas and its clinical relevance
- Thromboembolic complications following tissue plasminogen activator therapy in patients of acute ischemic stroke - Case report and possibility for detection of cardiac thrombi
- The effects of gastrointestinal function on the incidence of ventilator-associated pneumonia in critically ill patients
- A report of chronic intestinal pseudo-obstruction related to systemic lupus erythematosus
- Risk model in women with ovarian cancer without mutations
- Direct oral anticoagulants and travel-related venous thromboembolism
- How bispectral index compares to spectral entropy of the EEG and A-line ARX index in the same patient
- Henoch-schonlein purpura nephritis with renal interstitial lesions
- Cardiovascular risk estimated by UKPDS risk engine algorithm in diabetes
- CD5 and CD43 expression are associate with poor prognosis in DLBCL patients
- Combination of novoseven and feiba in hemophiliac patients with inhibitors
Articles in the same Issue
- Regular Articles
- Cleidocranial dysplasia-dental disorder treatment and audiology diagnosis
- A hybrid neural network – world cup optimization algorithm for melanoma detection
- Early administration of venovenous extracorporeal life support for status asthmaticus during anaesthetic induction: case report and literature review
- Assessment of maximal isometric hand grip strength in school-aged children
- Evaluation of a neurokinin-1 antagonist in preventing multiple-day cisplatin-induced nausea and vomiting
- Value of continuous video EEG and EEG responses to thermesthesia stimulation in prognosis evaluation of comatose patients after cardiopulmonary resuscitation
- Platelet-rich plasma protects HUVECs against oX-LDL-induced injury
- Pharmacoeconomics of three therapeutic schemes for anti-tuberculosis therapy induced liver injury in China
- Small-cell lung cancer presenting as fatal pulmonary hemorrhage
- Correlation of retinopathy of prematurity with bronchopulmonary dysplasia
- Prognosis of treatment outcomes by cognitive and physical scales
- The efficacy of radiofrequency hyperthermia combined with chemotherapy in the treatment of advanced ovarian cancer
- Arcuate Fasciculus in Autism Spectrum Disorder Toddlers with Language Regression
- Aesthetic dental procedures: legal and medico-legal implications
- Blood transfusion in children: the refusal of Jehovah’s Witness parents’
- Burnout among anesthetists and intensive care physicians
- Relationship of HS CRP and sacroiliac joint inflammation in undifferentiated spondyloarthritis
- Ethical and legal issues in gestational surrogacy
- Effects of arginine vasopressin on migration and respiratory burst activity in human leukocytes
- Associations of diabetic retinopathy with retinal neurodegeneration on the background of diabetes mellitus. Overview of recent medical studies with an assessment of the impact on healthcare systems
- Pituitary dysfunction from an unruptured ophthalmic internal carotid artery aneurysm with improved 2-year follow-up results: A case report
- Effectiveness of treatment with endostatin in combination with emcitabine, carboplatin, and gemcitabine in patients with advanced non-small cell lung cancer: a retrospective study
- Piercing and tattoos in adolescents: legal and medico-legal implications
- The central importance of information in cosmetic surgery and treatments
- Penile calciphylaxis in a patient with end-stage renal disease: a case report and review of the literature
- Serum CA72-4 as a biomarker in the diagnosis of colorectal cancer: A meta-analysis
- Association between uric acid and metabolic syndrome in elderly women
- Distinct expression and prognostic value of MS4A in gastric cancer
- MAPK pathway involved in epidermal terminal differentiation of normal human epidermal keratinocytes
- Association of central obesity with sex hormonebinding globulin: a cross-sectional study of 1166 Chinese men
- Successful endovascular therapy in an elderly patient with severe hemorrhage caused by traumatic injury
- Inflammatory biomarkers and risk of atherosclerotic cardiovascular disease
- Related factors of early mortality in young adults with cerebral hemorrhage
- Growth suppression of glioma cells using HDAC6 inhibitor, tubacin
- Post-stroke upper limb spasticity incidence for different cerebral infarction site
- The esophageal manometry with gas-perfused catheters
- MMP-2 and TIMP-2 in patients with heart failure and chronic kidney disease
- Genetic testing: ethical aspects
- Intervention for physician burnout: A systematic review
- The melanin-concentrating hormone system in human, rodent and avian brain
- Clinical effects of piribedil in adjuvant treatment of Parkinson’s Disease: A meta-analysis
- Identification of a novel BRAF Thr599dup mutation in lung adenocarcinoma
- Adrenal incidentaloma – diagnostic and treating problem – own experience
- Common illnesses in tropical Asia and significance of medical volunteering
- Genetic risk in insurance field
- Genetic testing and professional responsibility: the italian experience
- The mechanism of mitral regurgitant jets identified by 3-dimensional transesophageal echocardiography
- Control of blood pressure and cardiovascular outcomes in type 2 diabetes
- Pseudomesotheliomatous primary squamous cell lung carcinoma: The first case reported in Turkey and a review of the literature
- Diagnostic efficacy of serum 1,3-β-D-glucan for invasive fungal infection: An update meta-analysis based on 37 case or cohort studies
- GPER was associated with hypertension in post-menopausal women
- Metabolic activity of sulfate-reducing bacteria from rodents with colitis
- Association of miRNA122 & ADAM17 with lipids among hypertensives in Nigeria
- The efficacy and safety of enoxaparin: a meta-analysis
- Cuffed versus uncuffed endotracheal tubes in pediatrics: a meta-analysis
- Thresholding for medical image segmentation for cancer using fuzzy entropy with level set algorithm
- Sleep deprivation in Intensive Care Unit – systematic review
- Benefits of computed tomography in reducing mortality in emergency medicine
- Ipragliflozin ameliorates liver damage in non-alcoholic fatty liver disease
- Limits of professional competency in nurses working in Nicu
- MDA-19 suppresses progression of melanoma via inhibiting the PI3K/Akt pathway
- The effect of smoking on posttraumatic pseudoarthrosis healing after internal stabilization, treated with platelet rich plasma (PRP)
- Partial deletion of the long arm of chromosome 7: a case report
- Meta-analysis of PET/CT detect lymph nodes metastases of cervical cancer
- High Expression of NLRC5 is associated with prognosis of gastric cancer
- Is monitoring mean platelet volume necessary in breast cancer patients?
- Resectable single hepatic epithelioid hemangioendothelioma in the left lobe of the liver: a case report
- Epidemiological study of carbapenem-resistant Klebsiella pneumoniae
- The CCR5-Delta32 genetic polymorphism and HIV-1 infection susceptibility: a meta-analysis
- Phenotypic and molecular characterisation of Staphylococcus aureus with reduced vancomycin susceptibility derivated in vitro
- Preliminary results of Highly Injectable Bi-Phasic Bone Substitute (CERAMENT) in the treatment of benign bone tumors and tumor-like lesions
- Analysis of patient satisfaction with emergency medical services
- Guillain-Barré syndrome and Low back pain: two cases and literature review
- HELLP syndrome complicated by pulmonary edema: a case report
- Pharmacokinetics of vancomycin in patients with different renal function levels
- Recurrent chronic subdural hematoma: Report of 13 cases
- Is awareness enough to bring patients to colorectal screening?
- Serum tumor marker carbohydrate antigen 125 levels and carotid atherosclerosis in patients with coronary artery disease
- Plastic treatment for giant pseudocyst after incisional hernia mesh repair: a case report and comprehensive literature review
- High expression levels of fascin-1 protein in human gliomas and its clinical relevance
- Thromboembolic complications following tissue plasminogen activator therapy in patients of acute ischemic stroke - Case report and possibility for detection of cardiac thrombi
- The effects of gastrointestinal function on the incidence of ventilator-associated pneumonia in critically ill patients
- A report of chronic intestinal pseudo-obstruction related to systemic lupus erythematosus
- Risk model in women with ovarian cancer without mutations
- Direct oral anticoagulants and travel-related venous thromboembolism
- How bispectral index compares to spectral entropy of the EEG and A-line ARX index in the same patient
- Henoch-schonlein purpura nephritis with renal interstitial lesions
- Cardiovascular risk estimated by UKPDS risk engine algorithm in diabetes
- CD5 and CD43 expression are associate with poor prognosis in DLBCL patients
- Combination of novoseven and feiba in hemophiliac patients with inhibitors