
Clinical reasoning in the wild: premature closure during the COVID-19 pandemic
-
James G. Boyle
 ,
Matthew R. Walters
,
Matthew R. Walters

To the Editor,
Clinical reasoning has been defined as ‘the cognitive processes by which clinicians integrate clinical information (history, examination findings, and test results), preferences, medical knowledge, and contextual (situational) factors to make decisions about the care of an individual patient’ [1]. The study of clinical reasoning has traditionally been informed by theories that place emphasis on clinical reasoning residing in the mind of an individual physician at a moment in time [2]. Error is often attributed to the individual clinician, with other participants and the environment being broadly considered as noise. The COVID-19 pandemic affords a unique opportunity to look beyond the mind of a single clinician and consider how an unprecedented constellation of contextual (situational) factors might impact clinical reasoning performance and lead to error. We will use a family of social cognitive theories: Embodied Cognition, Ecological Psychology, and Situated Cognition, as lenses to magnify the potential implications of the pandemic on performance and error in an unfolding clinical story [2].
Peter, a redeployed resident in dermatology, walks into the new COVID-19 Special Assessment and Treatment Area (SATA) to review another case of suspected COVID-19 disease in a 62-year-old man with type 2 diabetes and ischaemic heart disease. As he enters the room alone, Peter feels invisible introducing himself in personal protective equipment (PPE). The patient appears anxious and has difficulty seeing Peter’s eyes through the visor or hearing any questions through the mask. Peter finds the PPE uncomfortable to wear and quickly moves to his physical examination by grasping a low-quality single patient stethoscope. Peter again notices that the percussion of the chest feels and sounds different through the gloves. Peter is unsure of his auscultation findings of bilateral crepitations despite adjusting the position of the stethoscope.
As Peter leaves the room the patient shares that he is worried that he has ‘the coronavirus’ and mentions his wife who is staying at home during the pandemic. Peter initially has difficulty finding a free computer to review the electronic medical record (EMR) and asks Sinead, a medical resident, to help. Sinead locates the image on her terminal and thinks to herself that the CXR is classic of pulmonary oedema. Professional distancing and noise prevent Sinead sharing her thoughts with Peter before she is interrupted to review a deteriorating patient. Peter reviews the CXR noting that there are bilateral opacities that could be consistent with COVID-19 disease. Peter is unable to locate a CXR report from the EMR as the radiology department is busy. He concludes that the diagnosis is COVID-19 disease and begins oxygen therapy while sending confirmatory samples.
Later, Peter attends handoff with Sinead, a senior nurse and the attending physician. The senior nurse informs the team that the patient’s wife had telephoned to say he had been getting chest pain recently, having run out of his cardiac medication while staying at home during the pandemic. The team review the CXR that has now been reported by the radiology team as consistent with pulmonary oedema. The attending asks to review the admission ECG which confirms an acute myocardial infarction. Peter realises that he hadn’t considered an alternative diagnosis and didn’t think to check the ECG before moving to the next case.
This story reinforces an often-cited cause of diagnostic error: premature closure [3] (which may be defined as accepting a diagnosis before it is fully verified). COVID-19 is a pervasive disease and current base rates in hospital settings are high. The virus is novel with incompletely understood pathophysiology and natural history. Daily guideline updates sometimes with conflicting information can create confusion and overwhelm short-term memory. Before concluding that the etiology of this diagnostic error was simply deficits in Peter’s knowledge, we should consider if there are any additional insights and useful lessons we can learn from a social cognitive lens by considering the environment and other participants in the encounter.
If we view Peter’s encounter with the patient through an embodied cognition lens, the body, mind and world are deeply connected and reciprocally dependent on guiding each other’s steps [3]. Reasoning occurs with the type of sensorimotor experiences that come from having one’s body dynamically interact within an environment, creating a continuous and inseparable perception-action loop that occurs throughout the clinical reasoning process. Reasoning can therefore be influenced by changes in the physician’s body and/or the environment. As Peter walked through the hospital to COVID-19 SATA, the environment is likely to have unduly influenced his early diagnostic hypothesis generation. Peter’s perception-action loop was clearly compromised by wearing PPE and applying an unfamiliar low-quality stethoscope during a hypothesis driven history and examination leading to incomplete or incorrect data collection.
Ecological psychology understands cognition as emerging from continuous coupled interactions between a physician and their environment [4]. Briefly, this position accentuates affordances (what the environment provides, including other individuals and physical props) and effectivities (what the physician is able to do in the environment). In a small clinical team such affordances and effectivities are interdependent, affecting Sinead and Peter’s behaviour (professional distancing, noise and interruptions) and opportunities or impediments to action (EMR, reporting delay). Affordances and effectivities are grounded in a weaving of the participants within the clinical setting. In other words, clinical reasoning performed by small teams can be determined by a variety of situational (contextual) factors; from this perspective the other participants and the environment are essential considerations in clinical reasoning performance. These include physician factors (e.g., PPE, knowledge base), patient factors (e.g., anxiety, diagnostic suggestion of COVID-19, acuity) and environmental factors (e.g., COVID-19 SATA, no visiting of relatives, professional distancing, EMR, interruptions).
Through the lens of situated cognition (SitCog) there is a complex bi-directional dynamic interplay between physician factors, patient factors and environmental factors [5]. SitCog also emphasises that cognitive processes are spread across the minds of individuals (clinicians, patients, relatives) and across artifacts (shared physical objects such as COVID-19 decision support tools, EMR) where the products of past events can transform outcomes of future related events (e.g., lack of awareness of recent drug history and chest pain). Today, patients with suspected COVID-19 disease are quickly assessed by rapidly changing multi-professional clinical teams. This assessment often occurs in areas with the prefix ‘COVID-19’ using dedicated proformas/checklists that may not highlight the relative importance of alternative diagnoses or co-morbidities. Thus, Peter and Sinead’s clinical reasoning cannot sensibly be understood or assessed independently to the social context in which it occurs [5].
By analysing this clinical story using a social cognitive approach, we can understand the mechanisms of premature closure in relation to diagnosing COVID-19 disease during this pandemic, and we can appreciate that combining key elements of these social cognitive theories could serve as a fecund vehicle to learn new strategies to mitigate error within dynamic teams and systems (Figure 1). The ultimate message of this story is that attaching a diagnostic label is an ensemble process requiring collaboration with a diverse cast of actors and props who feature in an inherently complex sequence of narrative episodes. We hope that this perspective serves as a timely reminder that predictably processing which one of around 12,000 discrete diseases to manage, particularly in context of acuity and risk, has never been a more uncertain task for a diagnostic team; navigating the wild together using both mind and body may help us learn to maintain situation awareness in these unprecedented times [6], [7], [8].
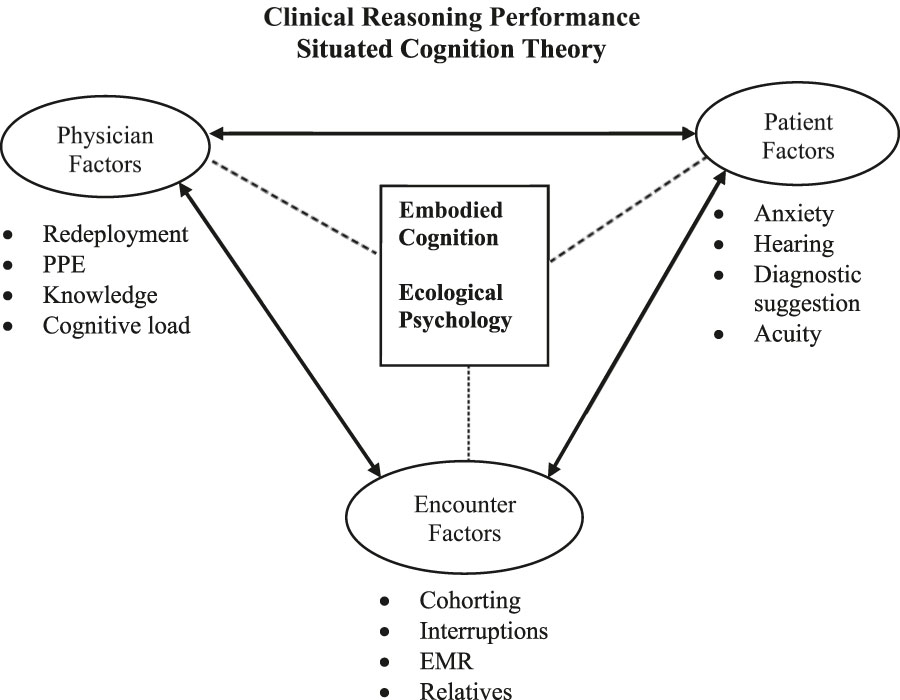
Clinical reasoning performance: situated cognition theory.
Research funding: None declared.
Author contributions: All authors have accepted responsibility for the entire content of this manuscript and approved its submission.
Competing interests: Authors state no conflict of interest.
References
1. Cook, DA, Sherbino, J, Durning, SJ. Management reasoning: beyond the diagnosis. J Am Med Assoc 2018;319:2267–8. https://doi.org/10.1001/jama.2018.4385.Search in Google Scholar PubMed
2. Torre, D, Durning, SJ, Rencic, J, Lang, VM Holmboe, E, Daniel, M. Widening the lens on teaching and assessing clinical reasoning: from “in the head” to “out in the world”. Diagnosis 2020. https://doi.org/10.1515/dx-2019-0098 [Epub ahead of print].Search in Google Scholar PubMed
3. Graber, ML, Franklin, N, Gordon, R. Diagnostic error in internal medicine. Arch Inter Med 2005;165:1493–9. https://doi.org/10.1001/archinte.165.13.1493.Search in Google Scholar PubMed
4. Durning, SJ, Artino, AR, Boulet, JR, Dorrance, K, van der Vleuten, C, Schuwirth, L. The impact of selected contextual factors on experts’ clinical reasoning performance (does context impact clinical reasoning performance in experts?). Adv Health Sci Educ 2012;17:65–79. https://doi.org/10.1007/s10459-011-9294-3.Search in Google Scholar PubMed
5. Rencic, JT, Schuwirth, LT, Gruppen, LD, Durning, SJ. Clinical reasoning performance assessment: using situated cognition theory as a conceptual framework. Diagnosis 2020. https://doi.org/10.1515/dx-2019-0051 [Epub ahead of print].Search in Google Scholar PubMed
6. Hutchins, E. Cognition in the wild. Cambridge, MA: MIT Press; 1996.10.7551/mitpress/1881.001.0001Search in Google Scholar
7. Graber, M, Rencic, J, Rusz, D, Papa, F, Croskerry, P, Zierler, B, et al. Improving diagnosis by improving education: a policy brief on education in healthcare professions. Diagnosis 2018;5:107–18. https://doi.org/10.1515/dx-2018-0033.Search in Google Scholar PubMed
8. Schuwirth, LT, Durning, SJ, King, SM, Steven, J. Assessment of clinical reasoning: three evolutions of thought. Diagnosis 2020. https://doi.org/10.1515/dx-2019-0096 [Epub ahead of print].Search in Google Scholar PubMed
© 2020 Walter de Gruyter GmbH, Berlin/Boston
Articles in the same Issue
- Frontmatter
- Editorials
- Progress understanding diagnosis and diagnostic errors: thoughts at year 10
- Understanding the social in diagnosis and error: a family of theories known as situativity to better inform diagnosis and error
- Sapere aude in the diagnostic process
- Perspectives
- Situativity: a family of social cognitive theories for understanding clinical reasoning and diagnostic error
- Clinical reasoning in the wild: premature closure during the COVID-19 pandemic
- Widening the lens on teaching and assessing clinical reasoning: from “in the head” to “out in the world”
- Assessment of clinical reasoning: three evolutions of thought
- The genealogy of teaching clinical reasoning and diagnostic skill: the GEL Study
- Study design and ethical considerations related to using direct observation to evaluate physician behavior: reflections after a recent study
- Focused ethnography: a new tool to study diagnostic errors?
- Phenomenological analysis of diagnostic radiology: description and relevance to diagnostic errors
- Original Articles
- A situated cognition model for clinical reasoning performance assessment: a narrative review
- Clinical reasoning performance assessment: using situated cognition theory as a conceptual framework
- Direct observation of depression screening: identifying diagnostic error and improving accuracy through unannounced standardized patients
- Understanding context specificity: the effect of contextual factors on clinical reasoning
- The effect of prior experience on diagnostic reasoning: exploration of availability bias
- The Linguistic Effects of Context Specificity: Exploring Affect, Cognitive Processing, and Agency in Physicians’ Think-Aloud Reflections
- Sequence matters: patterns in task-based clinical reasoning
- Challenges in mitigating context specificity in clinical reasoning: a report and reflection
- Examining the patterns of uncertainty across clinical reasoning tasks: effects of contextual factors on the clinical reasoning process
- Teamwork in clinical reasoning – cooperative or parallel play?
- Clinical problem solving and social determinants of health: a descriptive study using unannounced standardized patients to directly observe how resident physicians respond to social determinants of health
- Sociocultural learning in emergency medicine: a holistic examination of competence
- Scholarly Illustrations
- Expanding boundaries: a transtheoretical model of clinical reasoning and diagnostic error
- Embodied cognition: knowing in the head is not enough
- Ecological psychology: diagnosing and treating patients in complex environments
- Situated cognition: clinical reasoning and error are context dependent
- Distributed cognition: interactions between individuals and artifacts
Articles in the same Issue
- Frontmatter
- Editorials
- Progress understanding diagnosis and diagnostic errors: thoughts at year 10
- Understanding the social in diagnosis and error: a family of theories known as situativity to better inform diagnosis and error
- Sapere aude in the diagnostic process
- Perspectives
- Situativity: a family of social cognitive theories for understanding clinical reasoning and diagnostic error
- Clinical reasoning in the wild: premature closure during the COVID-19 pandemic
- Widening the lens on teaching and assessing clinical reasoning: from “in the head” to “out in the world”
- Assessment of clinical reasoning: three evolutions of thought
- The genealogy of teaching clinical reasoning and diagnostic skill: the GEL Study
- Study design and ethical considerations related to using direct observation to evaluate physician behavior: reflections after a recent study
- Focused ethnography: a new tool to study diagnostic errors?
- Phenomenological analysis of diagnostic radiology: description and relevance to diagnostic errors
- Original Articles
- A situated cognition model for clinical reasoning performance assessment: a narrative review
- Clinical reasoning performance assessment: using situated cognition theory as a conceptual framework
- Direct observation of depression screening: identifying diagnostic error and improving accuracy through unannounced standardized patients
- Understanding context specificity: the effect of contextual factors on clinical reasoning
- The effect of prior experience on diagnostic reasoning: exploration of availability bias
- The Linguistic Effects of Context Specificity: Exploring Affect, Cognitive Processing, and Agency in Physicians’ Think-Aloud Reflections
- Sequence matters: patterns in task-based clinical reasoning
- Challenges in mitigating context specificity in clinical reasoning: a report and reflection
- Examining the patterns of uncertainty across clinical reasoning tasks: effects of contextual factors on the clinical reasoning process
- Teamwork in clinical reasoning – cooperative or parallel play?
- Clinical problem solving and social determinants of health: a descriptive study using unannounced standardized patients to directly observe how resident physicians respond to social determinants of health
- Sociocultural learning in emergency medicine: a holistic examination of competence
- Scholarly Illustrations
- Expanding boundaries: a transtheoretical model of clinical reasoning and diagnostic error
- Embodied cognition: knowing in the head is not enough
- Ecological psychology: diagnosing and treating patients in complex environments
- Situated cognition: clinical reasoning and error are context dependent
- Distributed cognition: interactions between individuals and artifacts