Pain and other symptoms in patients with chronic benign paroxysmal positional vertigo (BPPV)
-
Wenche Iglebekk
 und
Peter Borenstein
und
Peter Borenstein

Abstract
Background and aim
A diagnosis of chronic benign paroxysmal positional vertigo (BPPV) is based on brief attacks of rotatory vertigo and concomitant nystagmus elicited by rapid changes in head position relative to gravity. However, the clinical course of BPPV may vary considerably from a self-limiting to a persisting and/or recurrent disabling problem. The authors’ experience is that the most common complaints of patients with chronic BPPV are nautical vertigo or dizziness with other symptoms including neck pain, headache, widespread musculoskeletal pain, fatigue, and visual disturbances. Trauma is believed to be the major cause of BPPV in individuals younger than fifty years. Chronic BPPV is associated with high morbidity. Since these patients often suffer from pain and do not have rotatory vertigo, their symptoms are often attributed to other conditions. The aim of this study was to investigate possible associations between these symptoms and chronic BPPV.
Methods
During 2010 a consecutive prospective cohort observational study was performed. Diagnostic criteria: (A) BPPV diagnosis confirmed by the following: (1) a specific history of vertigo/dizziness evoked by acceleration/deceleration, (2) nystagmus in the first position of otolith repositioning maneuvers, and (3) appearing and disappearing nystagmus during the repositioning maneuvers; (B) the disorder has persisted for at least six months. (C) Normal MRI of the cerebrum. Exclusion criteria: (A) Any disorder of the central nervous system (CNS), (B) migraine, (C) active Ménière’s disease, and (D) severe eye disorders. Symptom questionnaire (‘yes or no’ answers during a personal interview) and Dizziness Handicap Inventory (DHI) were used.
Results
We included 69 patients (20 males and 49 females) with a median age of 45 years (range 21-68 years). The median duration of the disease was five years and three months. The video-oculography confirmed BPPV in more than one semicircular canal in all patients. In 15% there was a latency of more than 1 min before nystagmus occurred. The Dizziness Handicap Inventory (DHI) median score was 55.5 (score >60 indicates a risk of fall). Seventy-five percent were on 50-100% sick leave. Eighty-one percent had a history of head or neck trauma. Nineteen percent could not recall any history of trauma. In our cohort, nautical vertigo and dizziness (81%) was far more common than rotatory vertigo (20%). The majority of patients (87%) reported pain as a major symptom: neck pain (87%), headache (75%) and widespread pain (40%). Fatigue (85%), visual disturbances (84%), and decreased concentration ability (81%) were the most frequently reported symptoms. In addition, unexpected findings such as involuntary movements of the extremities, face, neck or torso were found during otolith repositioning maneuvers (12%). We describe one case, as an example, how treatment of his BPPV also resolved his chronic, severe pain condition.
Conclusion
This observational study demonstrates a likely connection between chronic BPPV and the following symptoms: nautical vertigo/dizziness, neck pain, headache, widespread pain, fatigue, visual disturbances, cognitive dysfunctions, nausea, and tinnitus.
Implications
Patients with complex pain conditions associated with nautical vertigo and dizziness should be evaluated with the Dizziness Handicap Inventory (DHI)-questionnaire which can identify treatable balance disorders in patients with chronic musculoskeletal pain.
1 Introduction
Benign paroxysmal positional vertigo (BPPV) was first described by Barany in 1921 [1] and coined by Dix and Hallpike in 1952 [2]. The condition is characterized by “.. .brief attacks of rotatory vertigo and concomitant positioning rotatory-linear nystagmus elicited by rapid changes in head position relative to gravity” [3]. According to this statement an individual without rotatory vertigo does not suffer from BPPV. However, in 1995 Norré [4] stated that BPPV is not always characterized by rotatory vertigo. The clinical course of BPPV may vary considerably from a self-treatable, self-limiting, to a persisting and/or recurrent disabling problem. Although it is named as such, there are a considerable number of patients who do not perceive it as a benign disease, but rather as an incapacitating condition that restricts their daily activities and has a significant impact on their quality of life [5, 6]. Furthermore, it is well recognized that BPPV secondary to trauma is associated with high morbidity [7, 8, 9, 10, 1112].
Also according to the authors’ experience the clinical picture of chronic BPPV can differ from the original descriptions of Dix and Hallpike [2] and Brandt and Daroff [3]. The description cited above is still the most frequently used when describing BPPV [3, 13]. However, in patients with chronic BPPV we find the most common complaints are nautical vertigo (sensory illusion reminding of movements experienced on board a ship in waves) and dizziness with various other symptoms including neck pain, headache, and widespread musculoskeletal pain. In addition, they suffer from photophobia, fatigue, visual disturbances (e.g. blurred vision, seeing “stars” of different colors even in darkness), and episodes of tunnel vision lasting a few minutes. Movements of the head evoke all of these associated symptoms. They dislike certain environments that may cause peripheral visual stimulation and provoke symptoms, e.g. busy shopping centers or driving through a tunnel.
Because these patients often complain of pain and do not have rotatory vertigo, their pain symptoms are frequently attributed to other conditions.
The aim of this observational study was to investigate associations between chronic BPPV and the following symptoms: nautical vertigo, dizziness, neck pain, headache, widespread musculoskeletal pain, fatigue, visual disturbances, and tinnitus.
2 Methods
This was a prospective observational study on patients referred to the Otoneurology Centre in Southern Norway during the period April 2010 to January 2011 by general practitioners or other specialists such as ENT surgeons and neurologists. Most patients referred were considered difficult cases due to the complexity of symptoms and their inability to function normally in society. Written informed consent was obtained from all patients. The procedures of the study are in accordance with ethical standards on human experimentation and with the Helsinki Declaration of 1975, as revised in 1983.The Regional Ethical Committee did not considerthat a formal approval was necessary.
2.1 Diagnostic criteria
BPPV diagnosis confirmed by the following:
specific history of vertigo or dizziness evoked by acceleration or deceleration,
nystagmus in the first position of otolith repositioning maneuvers,
appearing and disappearing nystagmus during the repositioning maneuvers;
the disorder had persisted for at least six months.
Normal MRI of the cerebrum.
2.2 Exclusion criteria
disorder of the central nervous system (CNS),
migraine (confirmed by positive effect of migraine specific medication),
consequent smooth pursuit eye movement ataxia, i.e. uni or bilateral ataxia characteristic for a CNS disorder (pontine or cerebellar lesion),
saccadic eye movement test disturbance, especially hyper-or hypometria, which are characteristic for a CNS disorder such as multiple sclerosis,
active Ménière’s disease,
severe eye disorders, i.e. conditions where optimal vision cannot be obtained by optical aids,
inability to fill in questionnaires.
2.3 Procedure
2.3.1 Dizziness handicap inventory (DHI) [15, 16]
This is validated for individuals with vestibular dysfunction. The tool consists of 25 items that are scored as always (4 points), some-times (2 points), and never (0 point) for a maximal score of 100. A score > 60 indicates an increased likelihood of having a fall.
2.3.2 Symptom questionnaire
“Yes” or “no” answers during a personal interview (shown in Table 1).
The definition of vertigo and of dizziness is according to Sted-man’s Medical Dictionary (26th edition) [17].
Vertigo is defined as:
“A sensation of spinning or whirling motion. Vertigo implies a definite sensation of rotation of the subject or of objects about the subject in any plane;
imprecisely used as a general term to describe dizziness commonly used by patients in an attempt to describe various symptoms such as faintness, giddiness, light-headedness, or unsteadiness”.
We chose to operate with either rotatory vertigo or nautical vertigo (=sensory illusion reminding of movements experienced on board a ship in waves) and dizziness.
The visual disturbances the patients report are blurred vision, seeing “stars” of different colors even in darkness, episodes of tunnel vision lasting a few minutes, all evoked by movements of the head.
Frequency of symptoms reported before treatment.
| N =69 | % | |
|---|---|---|
| Rotatory vertigo | 14 | 20 |
| Nautical vertigo/dizziness | 56 | 81 |
| Headache | 50 | 75 |
| Neck pain | 58 | 87 |
| Widespread pain | 27 | 40 |
| Visual disturbance | 58 | 84 |
| Phonophobia hyperacousis | 42 | 61 |
| Tinnitus | 37 | 54 |
| Peri-retroorbithal pressure/pain | 46 | 67 |
| Sensation of globus | 33 | 48 |
| Nausea | 51 | 74 |
| Temperature disturbances | 35 | 51 |
| Sleep disturbances | 46 | 67 |
| Impaired short term memory | 45 | 65 |
| Concentration problems | 56 | 81 |
| Impaired simultaneous capacity | 35 | 51 |
| Aggravation by physical activity | 54 | 78 |
| Fatigue | 59 | 85 |
-
The cipher indicates the number of individuals who has reported the specific symptom. The percent express the frequency of each symptom.
2.3.3 Diagnosing procedure
The diagnosing procedure was performed simultaneously by the two first authors. The nystagmus was registered by video-oculography (Interacoustics A/S, Assens, Denmark) (Fig. 1). Oculography is superior to oculoscopy as it is able to register the lowest amplitude nystagmus.
Otoliths and debris in the semicircular canals (SCCs) are the cause of BPPV, i.e. they are solid particles in fluid.
It is difficult to move solid floating particles in liquid by rapid movements; therefore the repositioning maneuvers are done in slow motion. Because of the possible long latency before nystagmus evokes in some patients, they were kept for 2 min in each position during the diagnostic procedure. Otoliths in one SSC give a specific nystagmus pattern. Otoliths in more than one SSC give various nystagmus patterns according to which SSC is activated and the amount of debris present.
The resulting nystagmus was analyzed like a vector-diagram. Divergence from one-SSC pattern was interpreted as a BPPV with otoliths in more than one SSC [18].
Polensek and Tusa in 2009 found the caloric test unnecessary in diagnosing BPPV [19]. The caloric test and the head impulse test were excluded in this study because they do not give reproducible results in patients with BPPV. This is because the otoliths in the SCC are influenced by the slightest movement and the latency and nystagmus duration are variable. The oculomotor test battery (i.e. smooth pursuit eye movement test and saccadic eye movement test) has been applied to exclude patients with CNS disorders.
2.3.4 Repositioning maneuvers
These were performed with the purpose (in addition to treatment) to confirm the BPPV diagnosis according to point (3) of the diagnostic criteria for BPPV.
2.3.4.1 Epley maneuver for otolith repositioning in posterior SSC [20, 21]
Relax in sitting position for 5 min. The maneuver was carried out in slow motion. The subject was kept in each position for 3 min.
2.3.4.2 Otolith repositioning in anterior SSC (Fig. 2)
This maneuver is developed by the authors and based on studying a dissected temporal bone. It was carried out in slow motion:
Relax in long sitting position on a tilting table for 5 min. Turn the head 20° toward the unaffected side.
The patient’s head is maintained in 20° of rotation and the table is slowly tilted backwards to an angle more than 70° under the horizontal level.
Hold the tilted position and slowly rotate the head 40° to the opposite side.
Finally, the table is tilted back to upright position.
Each position should be maintained for at least 3 min.
2.3.4.3 Modified 360° repositioning maneuver for repositioning of otoliths in the horizontal semicircular canal
The maneuver is also developed by the authors and is based on studying a dissected temporal bone.
Relax in sitting position for 5 min.
Slowly lie down toward the affected side. A pillow should be placed under the patient’s head.
Next, chin in and slowly turn into the supine position.
Then turn slowly toward the unaffected side.
Chin in and turn into the prone position (remove the pillow and rest on the forehead).
Finish by going back into the starting (sitting) position.
Each position should be maintained for at least 3 min.
2.3.5 Statistical analysis
The StatSoft-statistical program, copyright 2004 (Tulsa, OK 74104) was used for the analyses. Fischer 2 x 2 tables was used for comparing the frequency of symptoms during otolith repositioning maneuvers and symptoms reported in the questionnaire.
3 Results
3.1 Patients with the diagnosis of benign paroxysmal positioning vertigo – BPPV
During the nine month, period 203 patients were assessed. Eighty-six individuals fulfilled the diagnostic criteria. All participants were younger than 69 years of age. Five patients were excluded due to an earlier CNS-disorder (three with migraine, two with epilepsy); four were excluded due to active Ménière’s disease; two individuals were excluded due to severe eye disorders, and six were excluded due to inability to fill in the questionnaire.
Thus, 69 patients (20 males and 49 females) with a median age of 45 years (range 21–68 years) had BPPV. The median duration of the disease was 5 years and 3 months (range from half a year to 30 years). Of the 69 patients 52 (75%) were on 50–100% sick leave.
3.2 Trauma
Fifty-six patients (81%) had a history of head or neck trauma resulting from road traffic accidents, fall accidents, or sports injuries. Twenty-six patients (38%) fulfilled the Quebec Task Force criteria for the diagnosis Whiplash Associated Disorders (WAD) [14]. Thirty individuals (43%) had a history of trauma before debut of vertigo. The majority of these claimed that their disorder could be related to the trauma. Thirteen (19%) could not recall any trauma. Age, gender, duration of illness, and sick leave were equally distributed among the patients with WAD, with other trauma, and those without recalled history of trauma.
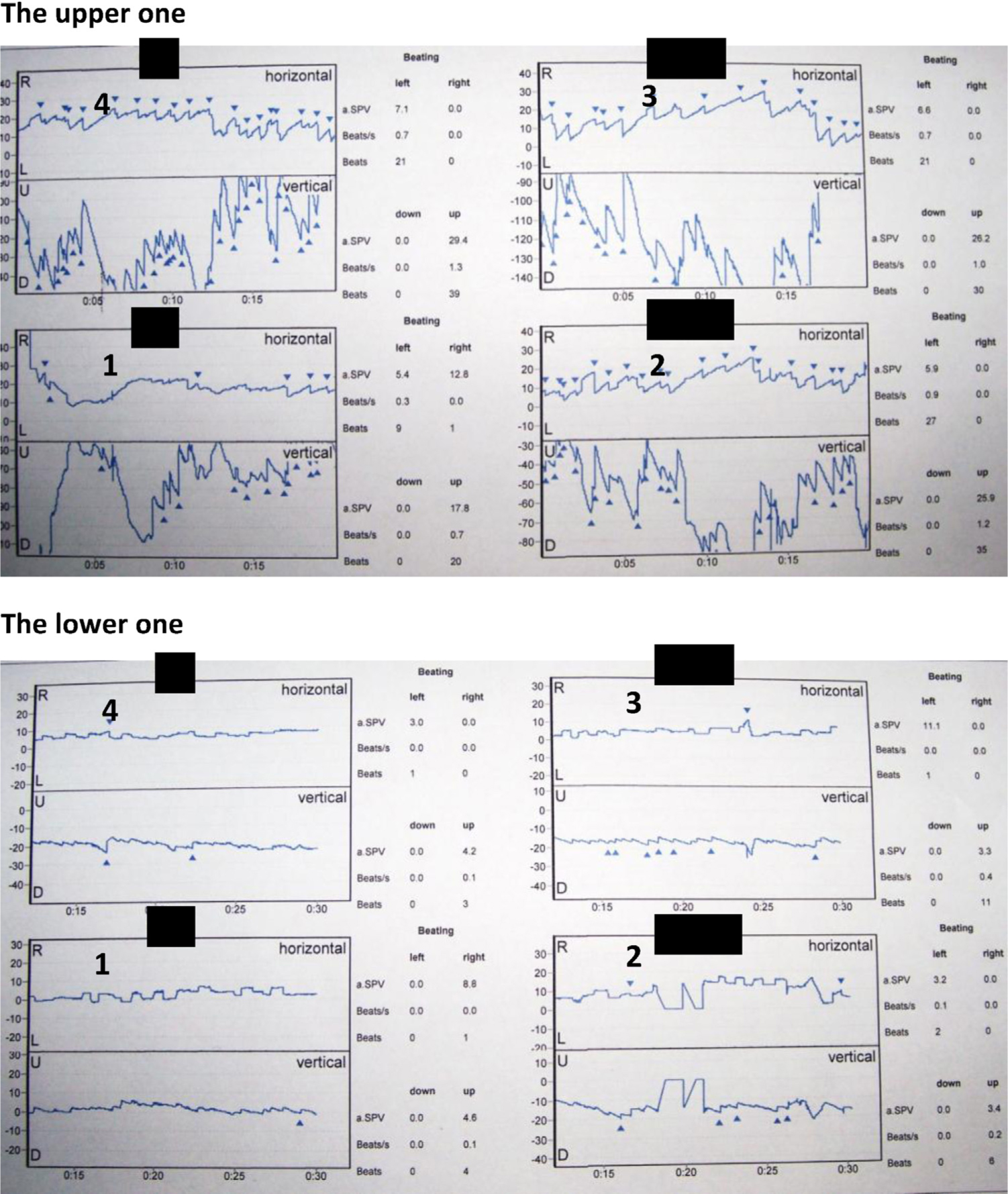
Video-oculographic documentations of BPPV pre-treatment (the upper one) and post-treatment (the lowerone). Equipment from Interacoustics A/S, Assens, Denmark was used. The patient was tested in the Dix-Hallpike position to the right for 2 min. Each of the four rectangles (1–4) shows the first 20s of a 30s period of time. At the right side of each period illustration (1–4) the quantitative details are given, i.e., the counts of nystagmus and their orientation (right, left, up and down) during a 30 s period, beats per second, and SPV, i.e. Slow Phase Velocity of nystagmus beats. The recordings are from a 38 year old man with an eight years history of chronic widespread pain and fatigue after a traffic road accident. His level of pain varied from 5 to 9 on a visual analog scale of pain (0–10). Pain was the absolutely devastating symptom. There was no report of vertigo but dizziness. DHI-score was 60. The test results are shown in the upper illustration. The patient underwent treatment of BPPV in the anterior, posterior and horizontal SSCs bilaterally. During a period of one year he improved significantly. During this year he had some relapses, which were treated. In total he received 15 treatments. The only recommendation given as a home-exercise program was walking (hiking) with gradual increase in distance and intensity. Exactly one year after the first examination he was reexamined (the lower one) in the Dix-Hallpike position to the right for 2 min. The illustration shows very few nystagmus beats compared with the pre-treatment figure. After this late control the patient has been working full time as a handyman without any complaints.
3.3 Analgesic drugs used
Thirty-four patients (49%) used either NSAIDs together with paracetamol or codeinphosphate, and 18 (26%) used tramadol for pain relief. Sixteen (23%) had stopped using analgesic drugs because they were ineffective. The other 18 patients used their pain medication only occasionally. They all answered that their vertigo/dizziness occurred whether medication was used or not.
3.4 Vertigo
The video-oculography confirmed BPPV in more than one semicircular canal in all patients. In 10 individuals (15%) there was a latency of more than 1 min before nystagmus occurred during the diagnosing procedure.
The Dizziness Handicap Inventory (DHI) median score was 55.5 (range 26–90 points) (Std. dev 16.52).
In these 69 patients, nautical vertigo and dizziness (81%) was far more common than rotatory vertigo (20%), see Table 1.
3.5 Pain
The majority of patients (87%) reported pain as a symptom, i.e., neck pain (87%), headache (75%) and widespread pain (40%).
3.6 Other associated symptoms
Fatigue (85%), visual disturbances (84%), as well as decreased ability to concentrate (81%) were the most frequent reported symptoms. Thirty-five patients (51%) (8 males and 27 females) suffered from temperature disturbances. Eight females were below forty years of age.
3.7 Repositioning maneuvers
Patients’ symptoms reported during the otolith repositioning maneuvers are listed in Table 2. In addition to the nystagmus (100%), involuntary movements of the extremities, face, neck, or torso (tremor-like, athetotic-like or hemiballism-like) were observed during otolith repositioning maneuvers (12%). Simultaneously with these involuntary movements intense hyperactivity in the eye muscles was registered. During repositioning most symptoms, apart from nausea (p <0.01) and visual disturbances (p <0.01), appeared with the same occurrence as reported in the questionnaire, i.e., rotatory vertigo, nautical vertigo and dizziness, pain, and change in tinnitus intensity (n.s.) (Tables 1 and 2).
Symptoms reported during otolith repositioning maneuvers for the posterior-, anterior-and horizontal semicircular canals.
| N = 69 | % | |
|---|---|---|
| Rotatory vertigo | 17 | 25 |
| Nautical vertigo/dizziness | 52 | 75 |
| Pain | 47 | 68 |
| Nausea | 35 | 51 |
| Visual disturbance | 31 | 45 |
| Change of tinnitus intensity | 32 | 46 |
-
The cipher indicates the number of individuals who has reported the specific symptom. The percent express the frequency of each symptom.
4 Discussion
4.1 Nautical vertigo and dizziness, pain and other associated symptoms
Nautical vertigo and dizziness are more common than rotatory vertigo in patients with chronic BPPV. We found that nautical vertigo and dizziness, neck pain, headache, widespread pain fatigue, visual disturbances, and cognitive difficulties are the main symptoms of chronic BPPV.
Their symptoms have previously been attributed to other conditions such as basilar migraine, cervical dizziness, whiplash associated disorders (WAD), fibromyalgia, phobic postural vertigo, and chronic fatigue syndrome.
Furthermore, this study highlights that the majority of patients were on long term sick leave. This is a significant burden on both the individual and on society as a whole [6].
A diagnosis of BPPV is considered confirmed when all three criteria were fulfilled: a specific history of movement related vertigo and dizziness; nystagmus in a BPPV evoking position; as well as nystagmus that appears and disappears during the otolith repositioning [4].
Most reported symptoms in the questionnaire occurred with the same frequency as during the repositioning maneuver. This supports our claim of an association between the non-vestibular symptoms described and a chronic BPPV.
4.2 Migrainous vertigo, cervical dizziness, phobic postural vertigo, anxiety, and chronic fatigue syndrome
However, von Brevern et al. [22] claimed that 10 subjects from a cohort of 362 patients with positional vertigo suffered from migrainous vertigo mimicking BPPV. They have migrainous symptoms (e.g. visual disturbances) and atypical positional nystagmus. In our study all patients have atypical nystagmus due to involvement of more than one SCC [18].
Moreover, sixty percent of the patients in our study experienced visual disturbances. Therefore, we raise the question could the 10 patients of von Brevern et al. [22] with suspected migrainous vertigo instead be suffering from a chronic BPPV?
The existence of the diagnosis of “cervical dizziness” is debatable. Clinical studies on cervical dizziness have two weak points: (1) the inability to confirm the diagnosis and (2) the unexplained discrepancy between patients suffering from severe neck pain without vertigo and patients complaining of disabling vertigo with only moderate neck pain [23].
If phobic postural vertigo, anxiety, and chronic fatigue syndrome can provoke dizziness, they can definitely not elicit the nystagmus related to the BPPV canalith repositioning maneuvers [24].
Dizziness is a frequent side-effect in most pain medication. The majority of patients reported to have used medication sporadically. Vertigo and dizziness occurred whether medication was used or not.
4.3 Importance of long latency of provoked nystagmus
Fifteen percent of our patients with BPPV had a latency of more than 1 min before nystagmus occurred. Therefore, the diagnosis could be missed, if the patients are observed for half a minute in the test positions.
Patients with long latency have been sick for a long period. In analogy with the teleological purpose of immobilization in the anti-inflammatory response we consider a parallel attempt to immobilize free floating otoliths in the endolymph to obtain stability. This could possibly be achieved through increased viscosity by secretion of colloids.
4.4 Importance of nautical vertigo and pain for the diagnosis of BPPV
The two highest ranked symptoms observed are nautical vertigo and dizziness and pain. Therefore, we suggest that the “.. .brief attacks of rotatory vertigo and concomitant positioning rotatory-linear nystagmus elicited by rapid changes in head position relative to gravity” [3] cannot be used to diagnose chronic BPPV. It is noted that most patients suffer from pain, such as neck pain, headache, and widespread pain. It is assumed that this pain is caused by the chronic BPPV since treatment according to these principles has been successful in reducing the patients’ pain [25].
4.5 The balance dysfunction in a BPPV is a dynamic and not a static one
Afferent information from the vestibular, visual and somatosensory systems converges in multiple areas within the CNS and is important for general equilibrium, body orientation, and oculomotor control. Abnormal afferent input from these systems can result in abnormal postural control.
Resulting mismatch which may occur in the presence of conflicting afferent information is thought to underlay symptoms of dizziness or unsteadiness [26].
In a stable condition of impaired vestibular function, e.g. after a labyrinthectomy, the vestibular nuclei (VN) complex compensates this loss by adjusting facilitating and inhibitory activity of the contralateral VN complex [27], i.e. a static balance dysfunction.
It is impossible to compensate in the same way within a BPPV with its dislocated free-floating otoliths and debris, because the affected labyrinth(s) transmit(s) varying abnormal signals from time to time to the same stimuli. This is possibly why their symptoms are ongoing.
Thus in BPPV, the VN complex receives contradictive signals from the different receptors of the labyrinths. The VN complex is the origin of the different vestibular reflexes: the vestibulo-ocular reflex, the lateral and medial vestibulo-spinal reflexes as well as the vestibuloreticular reflex.
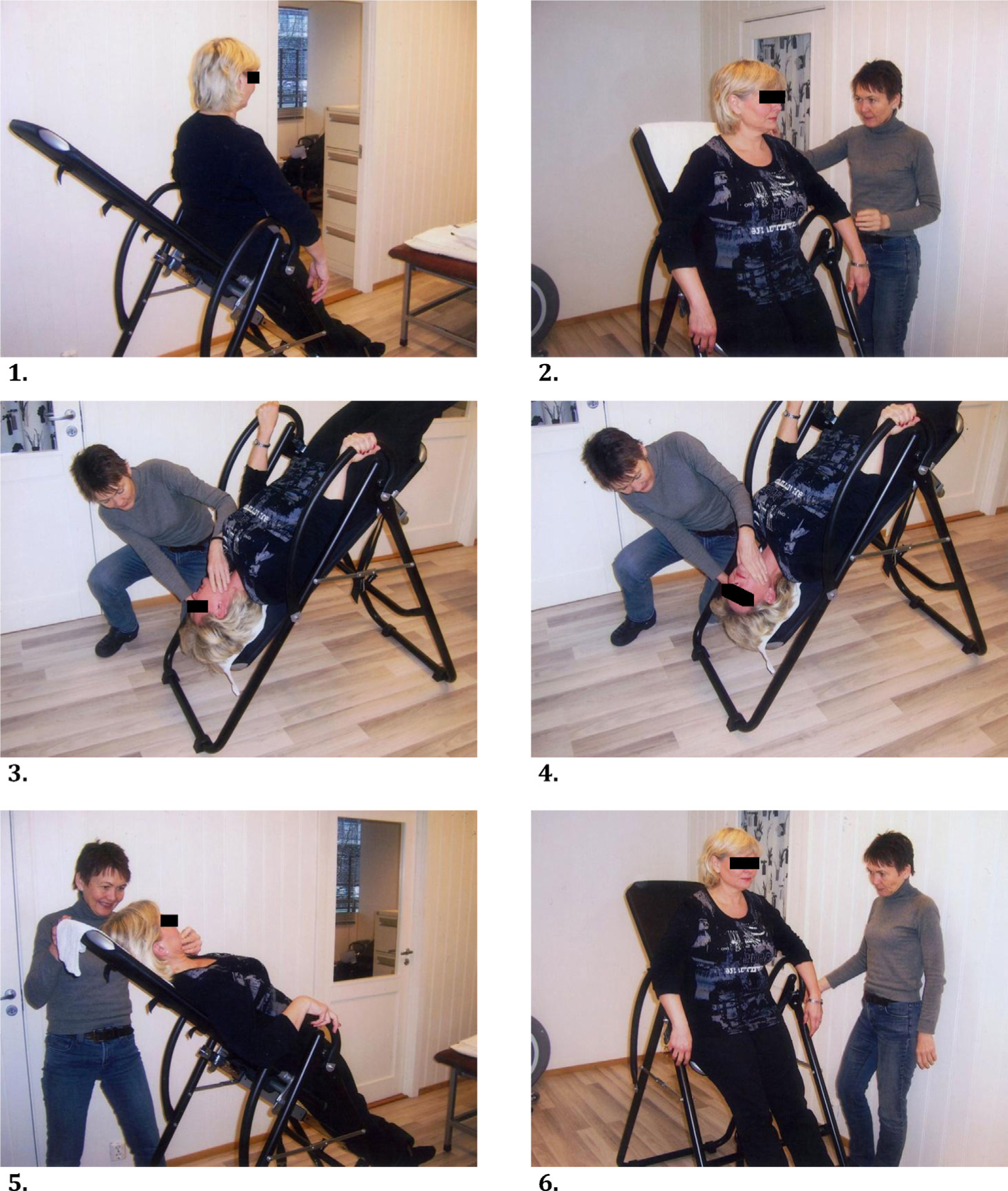
Repositioning of otoliths in anterior semicircular canal (right side). (1) Relax in long sitting position on a tilting table for 5 min. (2) Rotate the head 20° toward the unaffected side. (3) Slowly move the patient backwards until the head is at least 70° under the horizontal line. Hold this position for 3–5 min. (4) Hold the tilted position and slowly rotate the head 40° to the opposite side (i.e. the affected side). Hold this position for 3–5 min. (5) Finally, the table is tilted back to upright position in slow motion. (6) Stay in the upright position for 5 min before, if necessary, repeating the maneuver. The patient sits still for at least 15 min after treatment is completed.
4.6 Headache
The varying contradictive signals through the vestibulo-ocular reflex in patients with BPPV are the cause of visual disturbances [28]. Hypertonus in the intra- and periorbital muscles is a part of the explanation of the frontal headache [29].
4.7 Neck pain and generalized musculoskeletal pain
The postural control is secured through vestibulo-spinal [30, 31, 32, 33] and vestibulo-reticular reflexes [34].
The teleological purpose is to secure vertical balance. The vestibulo-spinal reflexes are involved in control of neck, torso and extremity muscle tension. The reticular formation maintains a level of tonus and integrates information from several neural centers.
Postural mismatch in BPPV occurs in all situations when the otoliths in the semicircular canals are activated, i.e. when the head is moved. There are individual strategies to compensate for this postural mismatch. The most common way to compensate a dynamic balance disturbance seems to be static use of muscles. It is well documented that static use of muscles generates accumulation of pain generating substances, i.e. arachnoid acid, bradykinin, and histamin [35]. Pain leads to lack of motor control, i.e. a sensorimotor control disturbance [36, 37]. Furthermore, according to O’Sullivan et al. [38] proprioceptive deficit may lead to delayed neuromuscular protective reflexes and coordination such that muscle contraction occurs too late to protect the joint from excessive joint movement, and possible damage of articular surfaces through repetitive abnormal loading.
Furthermore, these deficits lead to a destructive abnormal movement pattern.
There is a very high density of gamma-muscle spindles in the cranio-cervical joint related deep muscles [39, 40, 41]. These are the most important muscles in delivering proprioceptive signals. The proprioceptive information from muscle spindles is crucial for optimal motor control [42, 43].
Therefore, according to O’Sullivan et al. [38] it seems reasonable to presume that improper proprioceptive activity would lead to impaired postural control and pain. This is consistent with the observed high frequency of neck pain in our study. There is evidence to suggest that the vicious circle of the equilibrium control system is the motor for the vicious circle of pain.
4.8 Fatigue and involuntary muscle movements
The high frequency of fatigue is a consequence of the above-described continuously working postural control system. A disturbance in the delicate integration of facilitatory and inhibitory signals in the myostatic spinal reflexes [44] might explain the observation of rhythmic involuntary movements of neck, face, torso or extremities during otolith repositioning.
Simultaneously, involuntary rhythmic intense eye muscle movements were registered. A few patients had the ability to control the involuntary neck, face, torso, or extremities movements for a short period by focusing straight ahead. The pathway of the smooth pursuit eye movement goes via the inferior olive [45]. This may possibly indicate a connection between the semicircular canals and the olivocerebellar system. The inferior olive acts as a generator of temporal patterns, and acts as a pacemaker with a rhythmical firing [46, 47].
A disturbed vestibulo-reticular activity has the potential of creating various symptoms since the paramedian pontine reticular formation (PPRF) has a moderating influence on several functions [34].
4.9 Cognitive deficits
Over the last decade, there has been a steady accumulation of evidence to suggest that vestibular lesions may also lead to cognitive deficits, including deficits in attention, learning and memory [48].
From PPRF there are pathways to the hippocampus, which are responsible for short-term memory, concentration ability, and simultaneous capacity [49].
4.10 Temperature disturbances and intensity of tinnitus
The reported temperature disturbances are not gender or age related. Most likely they are due to activation of the autonomous nervous system. The acoustic symptoms were found to be more common than previously recognized [50, 51]. The proprioceptive effect on tinnitus can be explained through afferent proprioceptive activity to the dorsal cochlear nucleus and rostrally in the central auditory system [52, 53].
4.11 Treatment of BPPV may resolve most associated symptoms, such as pain
We illustrate how the specific treatment of BPPV will resolve the associated pain condition in Fig. 2. An ongoing prospective treatment study on patients with chronic BPPV will follow in a separate publication.
5 Conclusions
This study demonstrates a likely connection between chronic BPPV and the following symptoms: Nautical vertigo and dizziness, neck pain, headache, widespread pain, fatigue, visual disturbances, cognitive dysfunctions, nausea, and tinnitus.
The balance dysfunction in BPPV is dynamic and not static. This leads to a perpetual postural mismatch. Thus, the vicious circle of the equilibrium control system is the motor for the vicious circle of pain. Specific treatment of the BPPV may resolve many of the associated symptoms, which is focus for a separate publication.
Authors’ contributions
The first two authors have equally been involved in examination and treatment of all patients. Both authors have equally contributed to conception, design, and acquisition of data, analysis and interpretation of data. Moreover, both of the two first authors have equally been involved in drafting the manuscript and have given final approval of the version to be published. The third author has contributed to design and discussion. He has given the final approval of the version to be published.
DOI of refers to article: http://dx.doi.org/10.1016/j.sjpain.2013.06.005.
-
Conflict of interest
The authors declare that they have no conflict of interest.
References
[1] Barány R. Diagnose von Krankheitserscheinungen im Bereiche des Otolithenapparates. Acta Otolaryngol (Stockh) 1921;2:334–7.Suche in Google Scholar
[2] Dix R, Hallpike CS. The pathology, symptomatology and diagnosis of certain common disorders of the vestibular system. Ann Otol Rhinol Laryngol 1952;8:151–8.Suche in Google Scholar
[3] Brandt T, Daroff RB. Physical therapy for benign paroxysmal positional vertigo. Arch Otolaryngol 1980;106:484–5.Suche in Google Scholar
[4] Norré ME. Reliability of examination data in the diagnosis of benign paroxysmal positional vertigo. AmJ Otol 1995;16:806–10.Suche in Google Scholar
[5] Lopez-Escamez JA, Gamiz MJ, Fernandez-Perez A, Gomez-Fiñana M, Sanchez-Canet I. Impact of treatment on health-related quality of life in patients with posterior canal benign paroxysmal positional vertigo. Otol Neurotol 2003;24:637–41.Suche in Google Scholar
[6] Korres S, Luxon L, Vannucchi P, Gibson B. Benign paroxysmal positional vertigo. Int J Otolaryngol 2011:353865.Suche in Google Scholar
[7] Gordon CR, Levite R, Joffe V, Gadoth N. Is posttraumatic benign paroxysmal positional vertigo different from the idiopathic form? Arch Neurol 2004;61: 1590–3.Suche in Google Scholar
[8] Jackson LE, Morgan B, Fletcher Jr JC, Krueger WW. Anterior canal benign paroxysmal positional vertigo: an underappreciated entity. Otol Neurotol 2007;28:218–22.Suche in Google Scholar
[9] Kansu L, Avci S, Yilmaz I, Ozluoglu LN. Long-term follow-up of patients with posterior canal benign paroxysmal positional vertigo. Acta Otolaryngol 2010;130:1009–12.Suche in Google Scholar
[10] Ahn SK, Jeon SY, Kim JP, Hur DG, Kim DW, Woo SH, Kwon OJ, Kim JY. Clinical characteristics and treatment of benign paroxysmal positional vertigo after traumatic brain injury. J Trauma 2011;70:442–6.Suche in Google Scholar
[11] Dlugaiczyk J, Siebert S, Hecker DJ, Brase C, Schick B. Involvement of the anterior semicircular canal in posttraumatic benign paroxysmal positioningvertigo. Otol Neurotol 2011;32:1285–90.Suche in Google Scholar
[12] Hornibrook J. Benign paroxysmal positional vertigo (BPPV). History, pathophysiology. Office treatment and future directions. Int J Otolaryngol 2011;2011:1–13.Suche in Google Scholar
[13] Bhattacharyya N, Baugh RF, Orvidas L, Barrs D, Bronston LJ, Cass S, Chalian AA, Desmond AL, Earll JM, Fife TD, Fuller DC, Judge JO, Mann NR, Rosenfeld RM, Schuring LT, Steiner RW, Whitney SL, Haidari J. Clinical practice guideline: benign paroxysmal positional vertigo. American Academy of Otolaryngology-Head and Neck Surgery Foundation. Otolaryngol Head Neck Surg 2008;139:S47–81.Suche in Google Scholar
[14] Spitzer WO, Skovron ML, Salmi LR, Cassidy JD, Duranceau J, Suissa S, Zeiss E. Scientific monograph of the Quebec Task Force on Whiplash-Associated Disorders: redefining “whiplash”and its management. Spine 1995;20:1S-73S (Phila Pa 1976).Suche in Google Scholar
[15] Jacobson GP, Newman CW. The development of the dizziness handicap inventory. Arch Otolaryngol Head Neck Surg 1990;116:424–7.Suche in Google Scholar
[16] Whitney SL, Marchetti GF, Morris LO. Usefulness of the dizziness handicap inventory in the screening for benign paroxysmal positional vertigo. Otol Neurotol 2005;26:1027–33.Suche in Google Scholar
[17] Stedman’s Medical Dictionary. 26th ed. Baltimore: Williams & Wilkins; 1995.Suche in Google Scholar
[18] Lopez-Escamez JA, Molina MI, Gamiz M, Fernandez-Perez AJ, Gomez M, Palma MJ, Zapata C. Multiple positional nystagmus suggests multiple canal involvement in benign paroxysmal vertigo. Acta Otolaryngol 2005;125:954–61.Suche in Google Scholar
[19] Polensek SH, Tusa R. Unnecessary diagnostic tests often obtained for benign paroxysmal positional vertigo. Med Sci Monit 2009;15:MT89–94.Suche in Google Scholar
[20] Epley JM. The canalith repositioning procedure: for treatment of benign paroxysmal positional vertigo. Otolaryngol Head Neck Surg 1992;107:399–404.Suche in Google Scholar
[21] Epley JM. Positional vertigo related to semicircular canalithiasis. Otolaryngol Head NeckSurg 1995;112:154–61.Suche in Google Scholar
[22] von Brevern M, Radtke A, Clarke AH, Lempert T. Migrainous vertigo presenting as episodic positional vertigo. Neurology 2004;62:469–72.Suche in Google Scholar
[23] Brandt T. Vertigo, its multisensory syndromes. London: Springer; 1999. p. 445.Suche in Google Scholar
[24] Staab JP. Chronic subjective dizziness. Continuum (Minneap Minn) Neurootology 2012;18:1118–41.Suche in Google Scholar
[25] Tjell C, Iglebekk W. Postural mismatch in musculoskeletal disorders. In: Alricsson M, editor. Musculoskeletal disorder. Rijeka: InTech; 2012., http://dx.doi.org/10.5772/38880.Suche in Google Scholar
[26] Baloh R, Halmagyi G. Disorders of the vestibular system. New York: Oxford University Press; 1996.Suche in Google Scholar
[27] Hillier SL, McDonnell M. Vestibular rehabilitation for unilateral peripheral vestibular dysfunction. Cochrane Database Syst Rev 2011;2. CD005397, doi:10.1002/14651858.CD005397.pub3.Suche in Google Scholar
[28] Peters BT, Mulavara AP, Cohen HS, Sangi-Haghpeykar H, Bloomberg JJ. Dynamic visual acuity testing for screening patients with vestibular impairments. J Vestib Res 2012;22:145–51.Suche in Google Scholar
[29] Fernández-de-Las-Peñas C, Cuadrado ML, Gerwin RD, Pareja JA. Referred pain elicited by manual exploration of the lateral rectus muscle in chronic tension-type headache. Pain Med 2009;10:43–8.Suche in Google Scholar
[30] Peterson BW, Goldberg J, Biolotto G, Fuller JH. Cervicocollic reflex: its dynamic properties and interaction with vestibular reflexes. J Neurophys 1985;54:90–109.Suche in Google Scholar
[31] Peterson BW. Current approaches and future directions to understanding control of head movement. Brain mechanisms for the integration of posture and movement. Prog Brain Res 2004;143:369–81.Suche in Google Scholar
[32] Bacsi AM, Colebatch JG. Evidence for reflex and perceptual vestibular contributions to postural control. Exp Brain Res 2005;160:22–8.Suche in Google Scholar
[33] Goldberg JM, Cullen KE. Vestibular control of the head: possible functions of the vestibulocollic reflex. Exp Brain Res 2011;210:331–45.Suche in Google Scholar
[34] Tellegen AJ, Arends JJ, Dubbeldam JL. The vestibular nuclei and vestibuloreticular connections in the mallard (Anas platyrhynchos L.) An anterograde and retrograde tracing study. Brain Behav Evol 2001;58:205–17.Suche in Google Scholar
[35] Larsson B, Søgaard K, Rosendal L. Work related neck-shoulder pain: a review on magnitude, risk factors, biochemical characteristics, clinical picture and preventive interventions. Best Pract Res Clin Rheumatol 2007;21: 447–63.Suche in Google Scholar
[36] Jull G, Kristjansson E, Dall’Alba P. Impairment in the cervical flexors: a comparison of whiplash and insidious onset neck pain patients. Man Ther 2004;9:89–94.Suche in Google Scholar
[37] Falla D, Jull G, Hodges PW. Patients with neck pain demonstrate reduced electromyographic activity of the deep cervical flexor muscles during performance of the craniocervical flexiontest. Spine 2004;29:2108–14.Suche in Google Scholar
[38] O’Sullivan PB, Burnett A, Floyd AN, Gadsdon K, Logiudice J, Miller D, Quirke H. Lumbar repositioning deficit in a specific low back pain population. Spine 2003;28:1074–9 (Phila Pa 1976).Suche in Google Scholar
[39] Kulkarni V, Chandy MJ, Babu KS. Quantitative study of muscle spindles in suboccipital muscles of human foetuses. Neurol India 2001;49:355–9.Suche in Google Scholar
[40] Boyd-Clarc LC, Briggs CA, Galea MP. Muscle spindle distribution, morphology, and density in longus colli and multifidus muscles of the cervical spine. Spine 2002;27:694–701.Suche in Google Scholar
[41] Liu J, Thornell L, Pedrosa-Domellof F. Muscle spindles in the deep muscles of the human neck: a morphological and immunocytochemical study. J Histochem Cytochem 2003;51:175–86.Suche in Google Scholar
[42] Ghez C, Sainburg R. Proprioceptive control of interjoint coordination. Can J Physiol Pharmacol 1995;73:273–84.Suche in Google Scholar
[43] Messier J, Adamovich S, Berkinblit M, Tunik E, Poizner H. Influence of movement speed on accuracy and coordination of reaching movements to memorized targets in three-dimensional space in a deafferented subject. Exp Brain Res 2003;150:399–416.Suche in Google Scholar
[44] Delwaide PJ, Juprelle M. The effects of caloric stimulation of the labyrinth on the soleus motor pool in man. Acta Neurol Scand 1977;55:310–22.Suche in Google Scholar
[45] Fukushima K, Fukushima J, Ito N, Takei H, Ikeno K, Olley PM, Chiba S, Kobayashi N, Inoue K, Warabi T. Cerebellum and eye movement control -Neuronal mechanisms of memory-based smooth-pursuit and their early clinical application. Rinsho Shinkeigaku 2012;52:1001–5.Suche in Google Scholar
[46] Hillman D, Chen S, Aung TT, Cherksey B, Sugimori M, Llinas RR. Localization of P-type calciumchannels in the central nervous system. Proc Natl Acad Sci U S A 1991;88:7076–80.Suche in Google Scholar
[47] Yarom Y, Cohen D. The olivocerebellar system as a generator of temporal patterns. Ann N Y Acad Sci 2002;978:122–34.Suche in Google Scholar
[48] Smith PF, Zheng Y, Horii A, Darlington CL. Does vestibular damage cause cognitive dysfunction in humans? J Vestib Res 2005;15:1–9.Suche in Google Scholar
[49] McKinney M, Jacksonville MC. Brain cholinergic vulnerability: relevance to behavior and disease. Biochem Pharmacol 2005;70:1115–24.Suche in Google Scholar
[50] Tjell C, Tenenbaum A, Rosenhall U. Auditory function in whiplash associated disorders. Scand Audiology 1999;28:203–9.Suche in Google Scholar
[51] Lew HL, Jerger JF, Guillory SB, Henry JA. Auditory dysfunction in traumatic brain injury. J Rehabil Res Dev 2007;44:921–8.Suche in Google Scholar
[52] Shore SE, Zhou J. Somatosensory influence on the cochlear nucleus and beyond. Hear Res 2006;216–217:90–9.Suche in Google Scholar
[53] Shore SE, Koehler S, Oldakowski M, Hughes LF, Syed S. Dorsal cochlear nucleus responses to somatosensory stimulation are enhanced after noise-induced hearing loss. Eur J Neurosci 2008;27:155–68.Suche in Google Scholar
© 2013 Scandinavian Association for the Study of Pain
Artikel in diesem Heft
- Editorial comment
- Chronic pain – The invisible disease? Not anymore!
- Clinical pain research
- New objective findings after whiplash injuries: High blood flow in painful cervical soft tissue: An ultrasound pilot study
- Editorial comment
- Chronic pain is strongly associated with work disability
- Observational studies
- Chronic pain: One year prevalence and associated characteristics (the HUNT pain study)
- Editorial comment
- Pain rehabilitation in general practice in rural areas? It works!
- Clinical pain research
- Effectiveness of multidisciplinary rehabilitation treatment for patients with chronic pain in a primary health care unit
- Editorial comment
- Mirror-therapy: An important tool in the management of Complex Regional Pain Syndrome (CRPS)
- Topical review
- Mirror therapy for Complex Regional Pain Syndrome (CRPS)—A literature review and an illustrative case report
- Editorial comment
- New insight in migraine pathogenesis: Vasoactive intestinal peptide (VIP) and pituitary adenylate cyclase-activating polypeptide (PACAP) in the circulation after sumatriptan
- Original experimental
- Vasoactive intestinal peptide (VIP) and pituitary adenylate cyclase-activating polypeptide (PACAP) in the circulation after sumatriptan
- Editorial comment
- Statistical pearls: Importance of effect-size, blinding, randomization, publication bias, and the overestimated p-values
- Topical review
- Significance tests in clinical research—Challenges and pitfalls
- Editorial comment
- Biomarkers of pain – Zemblanity?
- Topical review
- Mechanistic, translational, quantitative pain assessment tools in profiling of pain patients and for development of new analgesic compounds
- Editorial comment
- Chronic Benign Paroxysmal Positional Vertigo (BPPV): A possible cause of chronic, otherwise unexplained neck-pain, headache, and widespread pain and fatigue, which may respond positively to repeated particle repositioning manoeuvres (PRM)
- Observational studies
- Pain and other symptoms in patients with chronic benign paroxysmal positional vertigo (BPPV)
- Editorial comment
- The most important step forward in modern medicine, “a giant leap for mankind”: Insensibility to pain during surgery and painful procedures
- Topical review
- In praise of anesthesia: Two case studies of pain and suffering during major surgical procedures with and without anesthesia in the United States Civil War-1861–65
- Editorial comment
- Intravenous non-opioids for immediate postop pain relief in day-case programmes: Paracetamol (acetaminophen) and ketorolac are good choices reducing opioid needs and opioid side-effects
- Clinical pain research
- Intravenous acetaminophen vs. ketorolac for postoperative analgesia after ambulatory parathyroidectomy
- Editorial comment
- Scandinavian Association for the Study of Pain 2013—Annual scientific meeting abstracts of pain research presentations and greetings from incoming President
- Abstracts
- Why does the impact of multidisciplinary pain management on quality of life differ so much between chronic pain patients?
- Abstracts
- Health care utilization in chronic pain—A population based study
- Abstracts
- Pain treatment in rural Ghana—A qualitative study
- Abstracts
- Pain psychology specialist training 2012–2014
- Abstracts
- Pain assessment, documentation, and management in a university hospital
- Abstracts
- Promising effects of donepezil when added to patients treated with gabapentin for neuropathic pain
- Abstracts
- A pediatric patients’ pain evaluation in the emergency unit
- Abstracts
- Proteomic analysis of cerebrospinal fluid gives insight into the pain relief of spinal cord stimulation
- Abstracts
- The DQB1(*)03:02 HLA haplotype is associated with increased risk of chronic pain after inguinal hernia surgery and lumbar disc herniation
- Abstracts
- On the pharmacological effects of two lidocaine concentrations tested on spontaneous and evoked pain in human painful neuroma: A new clinical model of neuropathic pain
- Abstracts
- The mineralocorticoid receptor antagonist spironolactone enhances morphine antinociception
- Abstracts
- Expression of calcium/calmodulin-dependent protein kinase II in dorsal root ganglia in diabetic rats 6 months and 1 year after diabetes induction
- Abstracts
- Histamine in the locus coeruleus attenuates neuropathic hypersensitivity
- Abstracts
- Pronociceptive effects of a TRPA1 channel agonist methylglyoxal in healthy control and diabetic animals
- Abstracts
- Human inducible pluripotent stem cell-derived sensory neurons express multiple functional ion channels and GPCRs
Artikel in diesem Heft
- Editorial comment
- Chronic pain – The invisible disease? Not anymore!
- Clinical pain research
- New objective findings after whiplash injuries: High blood flow in painful cervical soft tissue: An ultrasound pilot study
- Editorial comment
- Chronic pain is strongly associated with work disability
- Observational studies
- Chronic pain: One year prevalence and associated characteristics (the HUNT pain study)
- Editorial comment
- Pain rehabilitation in general practice in rural areas? It works!
- Clinical pain research
- Effectiveness of multidisciplinary rehabilitation treatment for patients with chronic pain in a primary health care unit
- Editorial comment
- Mirror-therapy: An important tool in the management of Complex Regional Pain Syndrome (CRPS)
- Topical review
- Mirror therapy for Complex Regional Pain Syndrome (CRPS)—A literature review and an illustrative case report
- Editorial comment
- New insight in migraine pathogenesis: Vasoactive intestinal peptide (VIP) and pituitary adenylate cyclase-activating polypeptide (PACAP) in the circulation after sumatriptan
- Original experimental
- Vasoactive intestinal peptide (VIP) and pituitary adenylate cyclase-activating polypeptide (PACAP) in the circulation after sumatriptan
- Editorial comment
- Statistical pearls: Importance of effect-size, blinding, randomization, publication bias, and the overestimated p-values
- Topical review
- Significance tests in clinical research—Challenges and pitfalls
- Editorial comment
- Biomarkers of pain – Zemblanity?
- Topical review
- Mechanistic, translational, quantitative pain assessment tools in profiling of pain patients and for development of new analgesic compounds
- Editorial comment
- Chronic Benign Paroxysmal Positional Vertigo (BPPV): A possible cause of chronic, otherwise unexplained neck-pain, headache, and widespread pain and fatigue, which may respond positively to repeated particle repositioning manoeuvres (PRM)
- Observational studies
- Pain and other symptoms in patients with chronic benign paroxysmal positional vertigo (BPPV)
- Editorial comment
- The most important step forward in modern medicine, “a giant leap for mankind”: Insensibility to pain during surgery and painful procedures
- Topical review
- In praise of anesthesia: Two case studies of pain and suffering during major surgical procedures with and without anesthesia in the United States Civil War-1861–65
- Editorial comment
- Intravenous non-opioids for immediate postop pain relief in day-case programmes: Paracetamol (acetaminophen) and ketorolac are good choices reducing opioid needs and opioid side-effects
- Clinical pain research
- Intravenous acetaminophen vs. ketorolac for postoperative analgesia after ambulatory parathyroidectomy
- Editorial comment
- Scandinavian Association for the Study of Pain 2013—Annual scientific meeting abstracts of pain research presentations and greetings from incoming President
- Abstracts
- Why does the impact of multidisciplinary pain management on quality of life differ so much between chronic pain patients?
- Abstracts
- Health care utilization in chronic pain—A population based study
- Abstracts
- Pain treatment in rural Ghana—A qualitative study
- Abstracts
- Pain psychology specialist training 2012–2014
- Abstracts
- Pain assessment, documentation, and management in a university hospital
- Abstracts
- Promising effects of donepezil when added to patients treated with gabapentin for neuropathic pain
- Abstracts
- A pediatric patients’ pain evaluation in the emergency unit
- Abstracts
- Proteomic analysis of cerebrospinal fluid gives insight into the pain relief of spinal cord stimulation
- Abstracts
- The DQB1(*)03:02 HLA haplotype is associated with increased risk of chronic pain after inguinal hernia surgery and lumbar disc herniation
- Abstracts
- On the pharmacological effects of two lidocaine concentrations tested on spontaneous and evoked pain in human painful neuroma: A new clinical model of neuropathic pain
- Abstracts
- The mineralocorticoid receptor antagonist spironolactone enhances morphine antinociception
- Abstracts
- Expression of calcium/calmodulin-dependent protein kinase II in dorsal root ganglia in diabetic rats 6 months and 1 year after diabetes induction
- Abstracts
- Histamine in the locus coeruleus attenuates neuropathic hypersensitivity
- Abstracts
- Pronociceptive effects of a TRPA1 channel agonist methylglyoxal in healthy control and diabetic animals
- Abstracts
- Human inducible pluripotent stem cell-derived sensory neurons express multiple functional ion channels and GPCRs