Concept and development of a telemedical supervision system for anesthesiology in operating rooms using the interoperable communication standard ISO/IEEE 11073 SDC
-

 ,
,

Abstract
Objectives
Discussion of a telemedical supervision system for anesthesiology in the operating room using the interoperable communication protocol SDC. Validation of a first conceptual demonstrator and highlight of strengths and weaknesses.
Methods
The system includes relevant medical devices, a central anesthesia workstation (AN-WS), and a remote supervision workstation (SV-WS) and the concept uses the interoperability standard ISO/IEEE 11073 SDC. The validation method involves a human patient simulator, and the system is tested in an intervention study with 16 resident anesthetists supervised by a senior anesthetist.
Results
This study presents a novel tele-supervision system that enables remote patient monitoring and communication between anesthesia providers and supervisors. It is composed of connected medical devices via SDC, a central AN-WS and a mobile remote SV-WS. The system is designed to handle multiple ORs and route the data to a single SV-WS. It enables audio/video connections and text chatting between the workstations and offers the supervisor to switch between cameras in the OR. Through a validation study the feasibility and usefulness of the system was assessed.
Conclusions
Validation results highlighted, that such system might not replace physically present supervisors but is able to provide supervision for scenarios where supervision is currently not available or only under adverse circumstances.
Introduction
Anesthesiology is a complex field that significantly affects surgical outcomes and patient safety. Annually, around 230 million people worldwide undergo anesthesia for major surgeries, and 7 million of them face severe complications, leading to 1 million deaths [1]. Continuous development and reevaluation of guidelines are necessary to minimize complications and enhance patient safety.
International declarations require anesthesia providers to possess adequate expertise for ensuring high patient safety standards, but implementation varies across countries [2]. Anesthetic nurses can administer anesthesia in some countries like the USA, France, and partially the UK. However, in countries such as Germany, only physicians are authorized to perform this task. Table 1 elucidates the guidelines and regulations regarding the responsibilities of nurses and physicians in anesthesiology and the practices for supervision and parallel anesthesia in four different countries [3], [4], [5], [6], [7]. While supervision by a specialist anesthetist varies based on the administering personnel, a skilled physician must be available in any critical situation, either present in the operating room (OR) or they are nearby and available whenever called upon in most countries [8]. The USA and France allow parallel anesthesia within specific boundaries, but it is generally not permitted in Germany and the UK except for specific situations [5], 9].
Guidelines and regulations regarding the responsibilities of nurses and physicians in anesthesiology and the practices for supervision and parallel anesthesia in different countries.
| Country | Nurse | Physician | Supervision | Parallel anesthesia |
|---|---|---|---|---|
| USA | Certified registered nurse anesthetists (CRNA) can perform anesthesia independently or under physician’s supervision | Physicians are not necessarily required, if “qualified anesthesia personnel” is present which includes physician anesthetists, anesthesiology fellows, resident physicians, anesthesiologist assistants and CRNAs | Depending on the state, the supervision of CRNAs is mandatory; Supervision is necessary for not fully “qualified anesthesia personnel”, e.g. non-physician anesthesia students |
Physicians can switch between patients perioperatively, if other “qualified anesthesia personnel” is present with the patient, e.g., CRNA |
| Germany | Assists the physician before, during and after anesthesia; not eligible to perform anesthesia | Physician needs to be present during the whole anesthesia | If anesthesia is provided by resident physician, then specialist needs to supervise in presence or by being available | No routine parallel anesthesia allowed |
| France | Nurse anesthetists (Infirmier Anesthésiste Diplômé d’État – IADE) can administer regional or general anesthesia supervised and participate in peri-operative resuscitation | Physician needs to be present at least during induction of anesthesia; afterwards, a delegation to an IADE is possible | Specialist anesthetist is supervising resident physicians and/or IADE | If the anesthesia is delegated to IADE, the physician might swap to another patient |
| UK | Anesthesia care team consists of physicians’ assistant (anesthesia) (PA(A)), operating department practitioner and anesthesia room nurses; however only PA(A) can administer anesthesia | Needs to be present during the whole anesthesia – if not delegated to a PA(A) | Supervision of resident physicians by specialists or supervision of PA(A) by anesthetists | No routine parallel anesthesia allowed; in “exceptional circumstances” possible and matter of individual judgement |
Although having the most experienced anesthetist providing one-to-one care would be ideal, economic constraints and varying national/regional numbers of anesthetists per population create challenges in ensuring adequate supervision [10], 11]. Whether a qualified nurse or a resident physician is caring for a patient, supervising staff may be responsible for patients in different locations facing severe situations simultaneously. Furthermore, resident physicians often feel inadequately supervised during their training [12].
A potential tool to maintain high patient safety requirements and improve supervision and education standards could be provided through telemedicine. Fast and adequate responses brought by audio/video connections to experts are already utilized in many fields of medicine and start to get introduced into anesthesiology. For preoperative telemedicine anesthesia evaluation, a 2015 study involving patients living in remote parts of Australia reported high satisfaction and perceived efficacy [13]. Our working group was also able to demonstrate the legally compliant feasibility of telemedical anesthesia preparation in Europe for the first time in 2021 [14]. To the best of our knowledge, intraoperative telemedical implementations in anesthesia have not yet been used routinely.
For a telemedical supervision system to improve established methods, transmitting important data from the OR in addition to the audio/video connection is crucial. Currently, specialist anesthetists often have the option of being contacted by telephone/“Digital Enhanced Cordless Telecommunications” system (DECT). Yet, in multiple cases, additional visual information via video, vital signs of the patient and further medical device measures are required for adequate clinical assessment and decision-making. A telemedicine system can leverage technological advancements to efficiently transmit all pertinent information, significantly reducing the need for specialists to make physical visits or rely on elaborate verbal descriptions over the phone.
For access and connectivity to the relevant medical device data, standardized communication protocols for medical device data access and connectivity are necessary, according to the latest WHO recommendation for telemedicine implementation [15]. Interoperability is a crucial component that reduces siloed implementations and divergent developments while increasing productivity and reusability of new solutions. Broadly transitioning technologically feasible achievements to the medical sector can improve working conditions and enhance patient safety sustainably.
The ISO/IEEE has standardized the 11,073 Service-oriented Device Connectivity (SDC) protocol, which could lead to a fully interoperable OR soon [16], 17]. SDC enables any device from any manufacturer to provide data in a previously defined structure for consistent processing and display, addressing issues like limitations of toolsets in different vendor compounds or redundant data entry. Furthermore, it ensures a secure and bidirectional communication channel.
Initial use of the SDC communication standard in the OR has yielded encouraging results [18], 19]. Workstations have been developed to link anesthesiology devices, giving anesthetists a comprehensive view of vital signs, device settings, and alarms. Device connectors generate interoperable data that can be presented uniformly on the workstation, regardless of proprietary communication protocols.
This work aims to present a system to enable tele-supervision by senior anesthetists remotely based on an already existing prototype of an anesthesia workstation (AN-WS) [19] and an additional supervision workstation. The second aim of this study was to evaluate the feasibility, acceptance, and effectiveness of the system in anesthesia.
Materials and methods
Requirement analysis for the system
Within the research project “PriMed – Process optimization through integrated medical devices in the operating room and clinic” (funded by the German State of North-Rhine Westphalia and the European Commission – European Regional Development Fund (EFRE); grant no.: EFRE-0801359), requirement analyses were defined, regarding a fully integrated OR. For the anesthesiologic side, it was defined as an interoperable composite of the relevant medical devices, a central workstation for the anesthesia provider and a remote workstation for a supervising physician. The devices that were defined as the relevant tools to be integrated are a patient monitoring system, syringe pumps and an anesthesia machine/ventilator. Another requirement was the modularity of integrations of multiple other devices and information systems. The workstation should be capable of configuring a set of modules based on the needs for a specific surgical procedure and depending on the user. The focus is the interoperable integration of medical data and process optimization as a result.
System concept and design
A prototypical “anesthesia-workstation” (AN-WS) was already implemented as part of a research project in 2019, as a stand-alone.NET/C# application. The workstation is capable to combine information from syringe pumps, patient monitors and anesthesia machines, generated by a simulator and transferred via the IEEE 11073 SDC protocol [19].
Within the PriMed project, a modular and interdisciplinary “x-workstation” (X-WS) was defined and developed for surgical components. The Workstation is a cross-platform software framework developed to control and visualize medical device data in the OR. It addresses the challenge of integrating and controlling medical devices using the open communication SDC standard. The developed framework is modular, has reusable and configurable user interface elements. The architecture is a client-server model, where a Java-server handles the medical device communication and a web browser is used to access the workstation’s user interface to display or control medical device data. The X-WS was evaluated multiple times by clinical staff and demonstrated, that the SDC standards allows the implementation of a safe, secure and accessible central medical workstation [20].
The concepts of the two workstations – AN-WS and X-WS – were used in this work as a foundation to build on, adjust and extend with a telemedical module. Furthermore, this updated AN-WS stational OR workstation was supplemented with a second mobile supervision workstation (SV-WS) that can be carried by a senior physician, to give locally independent telemedical support.
There was no existing solution for the SV-WS that met the requirement analysis. Important requirements for such a system, which enables senior physicians to remotely supervise resident anesthetists, included the transmission of key parameters from medical devices and patients’ vital signs. All data provided to the AN-WS via the SDC protocol should be transferred to the SV-WS, without any functionality to modulate or manipulate settings or parameters. Additionally, the architecture should support the surveillance of multiple operating rooms (ORs) from a single SV-WS and use the same telemedical module to establish text or audio/video connections with each OR when necessary. Technically, the SV-WS should be easily accessible on mobile devices, such as tablet computers. Therefore, another requirement for the system was the development of a fast and lightweight web application that could be used on low-end mobile devices and accessed through common web browsers. Consequently, JavaScript using React.js, a library suitable for developing such web applications, was chosen.
Interoperability standard
In 2019, the ISO IEEE 11073 SDC Standard family was granted approval, which outlines the communication syntax, semantics, responsibilities, and specific device functionalities required to facilitate open interoperability [17]. Other approaches, such as the “Medical Device Plug and Play” (MD PnP) in the United States [21] and the “Smart Cyber Operating Theater” (SCOT) in Japan [22], also offer tools for implementing an open, manufacturer-independent communication protocol. However, the SDC standard provides distinct advantages, including flexibility and a language specifically designed for describing medical devices and their data. Moreover, SDC has multiple ISO and IEEE standards established since 2019, which are not available in the SCOT and MD PnP protocols. As a result, SDC offers widespread interoperability and has a clear advantage over the alternative options [16].
Validation method and simulation setup
To evaluate the proposed tele-anesthesiology system, a safe simulation environment was used to examine usage behaviors, general usability, user acceptance, and feedback. The simulation was performed on a human patient simulator (HPS) at the AIXTRA (Competence Centre for Training and Patient Safety, Medical Faculty, RWTH Aachen University, Aachen, Germany). Three camera views, a livestream of vital signs, and a high-sensitivity ceiling microphone provided surveillance of the simulated operating theatre. An operating table, mobile operating light, anesthesia machine, and vital sign monitor formed the experimental set-up. The HPS was used as the patient, allowing for real patient monitoring and precise logging of parameters. Scenarios were individually tailored and could result in a range of outcomes from proactive problem solving to fatal results.
In this OR setting, the developed tele-supervision system was integrated (Figure 1). The patient monitor was connected via SDC to the AN-WS and therefore the vital parameters were available to the remote senior physician through the SV-WS. Other functions, like the OR plan or parameters of other interoperable devices that were included in the design of the SV-WS were not considered or evaluated within this study.

Validation setting in the simulation operating room – (left) with one-sided mirrored observation room; (middle) integrated anesthesia workstation that allowed the communication for resident anesthetists with a supervisor; (right) remote supervision workstation operated by senior physician.
The study was planned for resident anesthetists, supervised – in presence, by phone and via tele-supervision – by one senior anesthetist.
A total of 16 resident anesthetists of the University Hospital RWTH Aachen (Germany) within their first two years of further education to become a specialist were recruited and included into the study. Of which 9 were female and 7 were male, ranging from 25 to 35 years old. The experience, based on their time working as an anesthetist, ranged from 2 to 25 months.
The evaluation scenario involved a 71-year-old male patient with a history of atrial fibrillation and arterial hypertension who underwent a laparoscopic hemicolectomy. A possible postinduction hypotension was anticipated due to the patient’s fluid deficit, and an organizational issue was introduced where the surgeon would be absent for 30 min to attend an emergency, until finally the anesthetist will get informed that the OR needs to be cleared for the emergency trauma patient. The scenario aimed to test when and how participants contacted the senior physician, and the medium of contact and reasoning were noted.
A questionnaire (Appendix A) was given to each participant after the scenario, asking about their choice of communication with the senior physician. Furthermore, a subjective rating of communication channels in specific situations was requested, as well as general feedback on the system’s technology.
All participants were pseudonymized and data protection was ensured by submitting to the Data Protection Officer and Ethics Committee. Recorded videos were deleted after data acquisition.
This study has been approved by the Ethics Committee of the University Hospital RWTH Aachen (Aachen, Germany) (EK 314-21).
Results
Tele-supervision system
Within this work a novel, modular and interoperable tele-supervision system was designed and developed (Figure 2). The system is composed of connected medical devices that communicate bidirectionally with the central AN-WS via the SDC protocol. Vital parameters of a patient monitor and the current settings of syringe pumps and an anesthesia machine are provided. The AN-WS backend, implemented as a Java application, processes the received medical device data and provides it for further usage through a WebSocket handler. The AN-WS frontend, as a web application, gains full read/write access, and therefore provides the user a combined overview and the option to set device and alarm settings from a central interface instead of the necessity to perform adjustments on each device itself (Figure 3). The SV-WS, also implemented as web application, only receives the data in a read-only mode. Furthermore, both workstations are connected with a modified “TeleDoc” server (Docs in Clouds TeleCare GmbH, Aachen, Germany), running on a node.js server. It enables an audio/video connection, as well as a text chatting feature between both workstations, handles their roles and permission and thus offers the supervisor to switch between the cameras in the OR and gain their control. The architecture is designed to handle multiple ORs in the same network and route the data and communication channels to a single SV-WS.
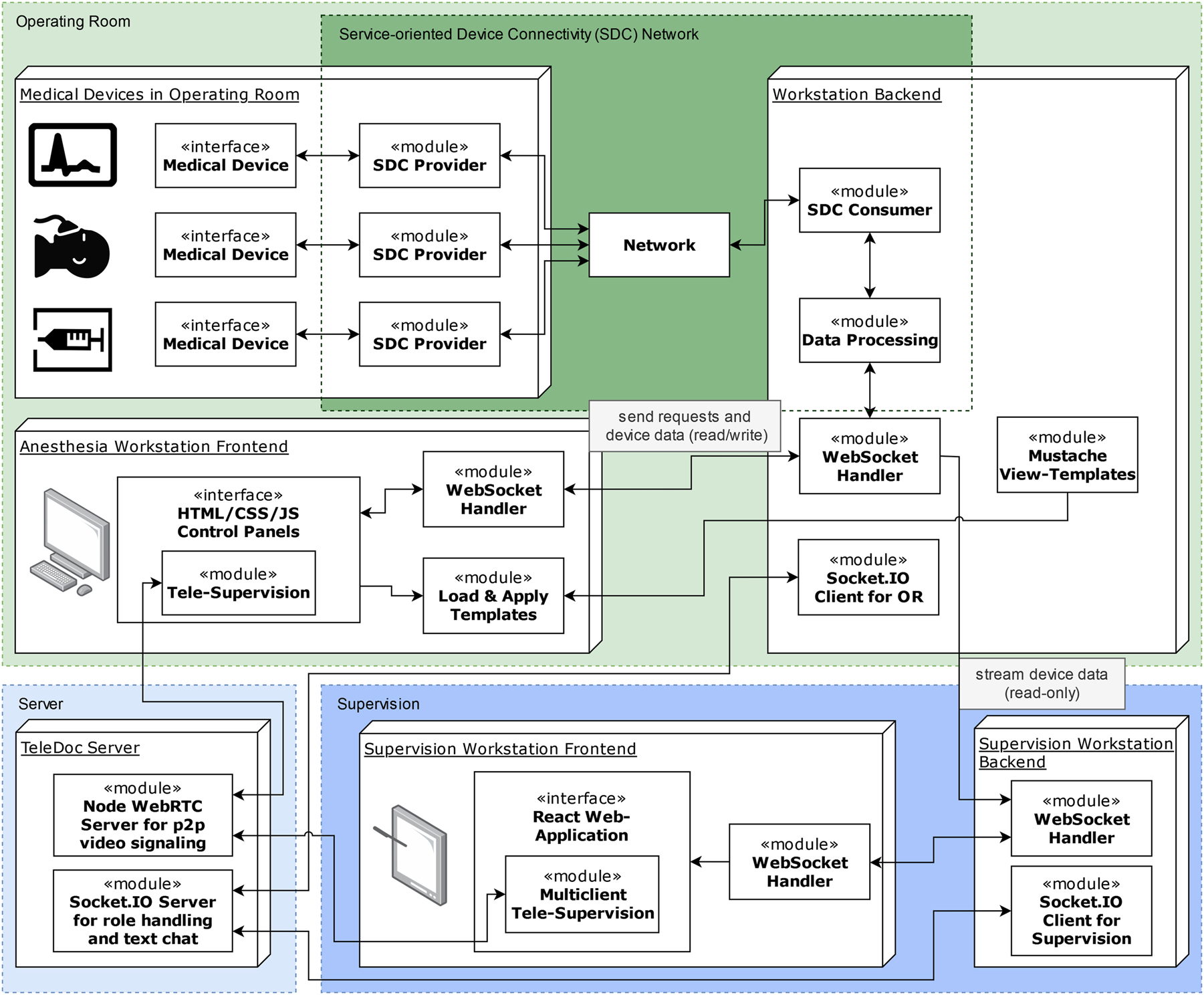
Tele-supervision system architecture – (top) components within the operating room: connected medical devices and anesthesia workstation with its backend and frontend structure; (bottom left) server for telemedical communication; (bottom right) remote supervision workstation with backend and frontend.

User interfaces for the anesthesia workstation (top) and the remote tele-supervision workstation (bottom): (1) general information about the patient, surgical procedure and global alarms; (2) compact view of vital parameters provided by the patient monitor; (3) device data and settings of the anesthesia machine; (4) medications and flowrates of the syringe pumps; (5) quick-access to a footswitch and key vital parameters available through all views of the workstation; (6) quick-access to documentation and communication modules; (A) displaying the most important information and vital parameters of one operating room (OR); (B) miniature view of key vital parameters provided by other ORs; (C) OR plan showing the scheduled interventions for all ORs; (D) communication module with chat and audio/video connection to the differents ORs.
The SV-WS displays the data from each OR and lets the user switch between the surgeries and contact any connected OR if needed (Figure 3). In the main frame the selected OR is displayed, mirroring the used medical devices: the patient monitor depicts the vital parameter curves, like the ECG, oxygen saturation and arterial blood pressure curves, as well as the corresponding numerical parameters. Furthermore, the ventilation settings from the anesthesia machine are transferred and displayed. By means of the SDC standard, every device can be allocated over the so-called “location context”, which uniquely defines the localization and therefore – on the supervision side – enables a clear distinction between different ORs. Below the main frame, other ORs display a selection of currently measured vital parameters in the miniature view and can be selected to be maximized. On the right side of the workstation, a concept for the OR plan is visualized. Beneath, the telemedical module is embedded, offering a direct text chat to each OR as well as handling the in- and out-going video calls utilizing an OEM module called “TeleDoc Web” (Docs in Clouds TeleCare GmbH, Aachen, Germany), which uses encrypted end-to-end communication. Furthermore, the module allows the supervising physician to switch between cameras in the OR, from a webcam showing the anesthetist to a pan-tilt-zoom camera mounted on the ceiling of the OR allowing an extended look, to inspect the patient, the medical devices, or the scene in general.
System validation
The participating resident physicians assessed the three potential ways of communication with a supervising physician – in person, via phone/DECT and via the newly developed tele-supervision system for different types of requests and situations (Figure 4). In emergencies, the presence of a supervisor was assessed as most suitable, while phone communication was evaluated as least suitable. For general advice on the strategy or specific advice related to specific situations, the three media were evaluated more evenly.

The participants indicated for different types of situations whether these could be resolved with the different communication options: Communicating with a supervisor in presence, through the tele-supervision system or by phone.
From all 45 requests for contact – on average around three per participant – with the senior physician, groups can be formed by concern of each question or reason (Figure 5). While most requests can be grouped as specific situational questions (e.g., which step to do next within an ongoing intubation), organizational questions and an information for the senior physician were often the reason for a contact. The request for a supervision in presence was only asked four times, which reflects 8.9 %. Tele-Supervision was chosen in 22.2 % and DECT in 68.9 % of cases.

Quantity of all requests for contact with the senior physician during the scenarios, grouped by matter of the requests and sorted by chosen medium.
When the tele-supervision system was not chosen, most participants stated, that for non-critical matters, they preferred phone contact because it was familiar and sufficient. As another reason, they stated, that for specific physical support like during intubation, a request for presence was seen as necessary.
Within the general feedback, participants mentioned aspects they liked or disliked about the system. Positively commented were the simplicity to access an expert’s opinion on a medical matter and the certainty, that this expert can access all relevant data without the need of long explanations. The audio output of the system and the necessity to stay close to the screen were criticized.
Discussion
The present scientific paper introduces a novel tele-supervision system, consisting of an integrated anesthesia workplace in an OR and a remote supervision workstation. Based on a modular and interoperable concept, using a standardized communication protocol, the setup was developed and validated for the first time, receiving overall positive feedback and highlighting its potential as well as its current limitations.
The elaborated modular system architecture provides a versatile and extendable foundation for future connected OR environments. While previous integrated OR solutions were dependent on proprietary protocols or siloed solutions [23], [24], [25], the introduced system has the potential to be widely used and distributed, without any dependencies to locally used devices from certain manufacturers. The modular approach, based on the IEEE/ISO certified communication standard SDC, allows flexible use-cases and provides the foundation for more system extensions based on it, such as smart alarm management systems or decision support modules. Offering user interfaces as web applications also offers the advantage of achieving independence of the devices used. While the AN-WS provides full read/write access to properties of the medical devices that are meant to be controlled, the architecture prevents the remote SV-WS from any direct manipulations of settings. Thus, a level of safety can be assured, avoiding unintended actions, potentially risking the patients safety.
The developed AN-WS provides an overview of key parameters of the most important anesthesiologic medical devices and supplies the SV-WS with read-only access to its data. Design and Layout of the AN-WS were not subject of this work, but the implementation of its counterpart regarding surgical components has been evaluated in several previous works [26], 27], as well as similar approaches for specific fields of surgery [28]. This workstation can provide an unambiguous overview of all relevant data and allow quick and easy adjustments from a central point. Manufacturer dependent displays and user interfaces dispersed throughout the OR would become obsolete. In addition, the modular interoperable backend of the Workstation, allows flexible inclusion of any medical device supporting the SDC standard, allowing interdisciplinary use-cases where the OR staff could switch between e.g. surgical and anesthesiologic devices within an uniform user interface.
The mobile SV-WS gives insight in multiple ORs at once and thus enables a supervisor to gain a clear and extensive understanding of the situation within the OR. Long and potentially misleading explanations over the phone or distances to be covered to come around can be avoided. Just as for the AN-WS, such anesthesiologic supervision tool, based on the SDC communication standard, has not been evaluated before and is validated for the first time in this work. A similar telemedical supervision system, without the usage of a standardized communication protocol, was developed for the emergency medical service [29] and clearly showed an improvement of the patient’s safety due to the direct availability of a medical expert [30].
By implementing the proposed system into a teaching and training simulation center, a first evaluation and validation of the system and its acceptance was conducted under safe conditions for such early stage of development. The choice of young resident physicians as participants induced a generally high acceptance of new technologies, but at the same time implied a higher demand of supervision for the medical scenario and thus eased the observation of usage behaviors.
The participants rated the three potential communication channels for various situations differently, however, the contact by tele-supervision was generally evaluated more suitable than by phone. The superiority of supervision in presence for emergencies was clear, however, most participants could imagine a successful tele-supervision for such cases, too. As shown in studies applying telemedical support in emergency ambulances, the availability of an expert in situations where otherwise no support would be available, the outcome can be strongly improved [30]. For general advice on strategy and procedure, as well as for situational advice and specific requests, the necessity of a physically present supervisor was not rated high. In summary, the scope of application of the tele-supervision system is highlighted.
The study revealed that even in non-critical medical scenarios, each participant needed an average of three contacts with the senior physician within approximately 30 min of simulation. This highlights the importance of supervision in medical education for teaching purposes and legal protection. Furthermore, due to shortages and economic constraints, currently many physicians in training feel unsupported [12], 31]. A telemedical approach can address this issue by maintaining high supervision and teaching standards while ensuring efficient utilization of economic resources.
While none of the participants disagreed with the usefulness of such system and according to the participants’ inquiry the assessed suitability for it was high for almost every type of situation, within the scenario in only 22 % of contacts with the supervisor, the tele-supervision was chosen. A partial explanation was given by the questioned reasoning afterwards. The unfamiliarity of the system, in contrast with the daily used practices, might be the main explanation. But since the tele-supervision should be seen as an upgraded system compared to the audio-only phone connection, the comparison to the cases where the presence of the supervisor was requested is more interesting. Even though, in less than 10 % of the requests the supervisor was asked to come around, these cases show, that there are limits to the application possibilities. Situations might require the direct physical or manual support of an additional person in the OR. Such tele-supervision system however should not replace a physically present senior physician but instead add appropriate expertise to scenarios, where currently no supervisor is available. Smaller clinics and rural hospitals could benefit greatly by added supervision capabilities.
The overall positive feedback to the supervision system gives a good first impression of the current developed system. At the same time, pain points became evident, especially regarding the usage-behavior. Uncertainties of the physicians regarding the handling of the system, when to focus on the screen and how to communicate in parallel with a remote supervisor and other personnel within the OR, came up.
The present study is not without limitations, and these must be taken into account when interpreting the results. One major limitation is the relatively small number of cases and participants included in the study. While efforts were made to recruit a diverse range of participants, the sample size may not be representative of the larger population of anesthetists. Another limitation is that only one medical scenario was observed, and it is possible that the results would differ with other interventions, especially more critical scenarios. Additionally, the study was conducted in a simulator environment rather than a real operating room, which may limit the generalizability of the findings to real-world settings. These limitations suggest the need for future research with larger sample sizes, different types of medical interventions, and evaluation in real operating rooms. Furthermore, local legal and ethical restrictions and limitations, that would need to be met before implementation into real ORs, have not yet been evaluated. The potential of such system and positive feedback on the other hand should encourage further research and developments to improve patient care quality and supervision and teaching of less experienced physicians.
Conclusions
A telemedical tool for anesthesiology in the OR appears to provide a potentially highly adequate extension for supervision. While such system will not substitute the presence of a senior physician in cases where extra hands are needed, it might offer the chance to augment health care infrastructure in its current state. Hospitals with no continuous support provided by senior physicians, could strongly benefit from such system. An interoperability standard as the foundation of such system will allow reusability and a wide distribution and compatibility. Independence of existing technological infrastructures and sustainability in terms of further extensions and functional upgrades can be achieved. The further development of such system is hereby strongly encouraged to improve working conditions in the OR and increase patient safety and care.
Funding source: German State of North-Rhine Westphalia and the European Commission – European Regional Development Fund (EFRE)
Award Identifier / Grant number: EFRE-0801359
Acknowledgments
We would like to thank every physician of the University Hospital RWTH Aachen that participated in the study and gave their valuable feedback. Furthermore, we would like to thank the team at the AIXTRA, Competence Centre for Training and Patient Safety, for the excellent collaboration.
-
Research ethics: The study was conducted according to the guidelines of the Declaration of Helsinki and approved by the Ethics Committee of the University Hospital RWTH Aachen and is registered under “EK 314-21”.
-
Informed consent: Written informed consent was obtained from all subjects involved in the study.
-
Author contributions (for double- anonymized journals: please use initials): Conceptualization, J.R., M.C. and V.V.; Methodology, J.R., M.S. and V.V.; Validation, J.R., M.C. and V.V.; Formal Analysis, J.R., C.B.P.; Investigation, J.R., O.Y., M.S. and V.V.; Resources, O.Y., A.F., C.B.P. and M.C.; Data Curation, J.R. and V.V.; Writing – Original Draft Preparation, J.R.; Writing – Review & Editing, J.R., M.S., O.Y., V.V., M.C., A.F., C.B.P.; Visualization, J.R.; Supervision, A.F., C.B.P. and M.C.; Project Administration, J.R., V.V. and M.C.; Funding Acquisition, V.V., A.F. and C.B.P.
-
Use of Large Language Models, AI and Machine Learning Tools: None declared.
-
Conflict of interest: The authors J.R., C.B.P. and M.C. are/were employed by Docs in Clouds TeleCare GmbH (Aachen, Germany), providing telemedical services and consulting regarding smart hospital solutions. M.C. is CEO. M.C. is CEO of Ilara GmbH (Herzogenrath, Germany), a provider of medical software, including OR.NET device simulators and connectors. M.C. is member of the executive board of the nonprofit association OR.NET e.V. At the time of submission J.R. is now employed by Drägerwerk AG & Co. KGaA, a manufacturer of medical devices, however the research and writing for this article were performed beforehand.
-
Research funding: The study, as a part of the research project “PriMed – Process optimization through integrated medical devices in the operating room and clinic” was funded by the German State of North-Rhine Westphalia and the European Commission – European Regional Development Fund (EFRE); grant no.: EFRE-0801359.
-
Data availability: The raw data can be obtained on request from the corresponding author.
References
1. Weiser, TG, Regenbogen, SE, Thompson, KD, Haynes, AB, Lipsitz, SR, Berry, WR, et al.. An estimation of the global volume of surgery: a modelling strategy based on available data. Lancet 2008;372:139–44. https://doi.org/10.1016/s0140-6736(08)60878-8.Search in Google Scholar PubMed
2. Mellin-Olsen, J, Staender, S, Whitaker, DK, Smith, AF. The Helsinki declaration on patient safety in anaesthesiology. Eur J Anaesthesiol 2010;27:592–7. https://doi.org/10.1097/eja.0b013e32833b1adf.Search in Google Scholar PubMed
3. Tenedios, C, O’Leary, S, Capocci, M, Desai, SP. History of anaesthesia. Eur J Anaesthesiol 2018;35:158–64. https://doi.org/10.1097/eja.0000000000000774.Search in Google Scholar PubMed
4. American Society of Anesthesiologists. Standards for basic anesthetic monitoring. https://www.asahq.org/standards-and-guidelines/standards-for-basic-anesthetic-monitoring [Accessed 12 Feb 2023].Search in Google Scholar
5. Berufsverband Deutscher Anästhesisten und Deutsche Gesellschaft für Anästhesiologie und Intensivmedizin. Erneute gemeinsame stellungnahme des berufsverbandes deutscher anästhesisten (BDA) und der Deutschen gesellschaft für anästhesiologie und intensivmedizin (DGAI) zu zulässigkeit und grenzen der parallelverfahren in der anästhesiologie („Münsteraner Erklärung II 2007“). Anasthesiol Intensivmed 2007;223–9.Search in Google Scholar
6. Royal College of Anaesthetists. Guidelines for the provision of anaesthesia services for the perioperative care of elective and urgent care patients; 2023. https://rcoa.ac.uk/gpas/chapter-2 [Accessed 12 Feb 2023].Search in Google Scholar
7. Legifrance - Le service public de la diffusion du droit. Code de la santé publique: ReplierParagraphe 2 Consultation préanesthésique. (Article D6124-92). https://www.legifrance.gouv.fr/codes/section_lc/LEGITEXT000006072665/LEGISCTA000006196702/2022-02-20/ [Accessed 12 Feb 2023].Search in Google Scholar
8. American Society of Anesthesiologists. Statement on the anesthesia care team. https://www.asahq.org/standards-and-guidelines/statement-on-the-anesthesia-care-team [Accessed 12 Feb 2023].Search in Google Scholar
9. Checketts, MR, Alladi, R, Ferguson, K, Gemmell, L, Handy, JM, Klein, AA, et al.. Recommendations for standards of monitoring during anaesthesia and recovery 2015: association of anaesthetists of great britain and Ireland. Anaesthesia 2016;71:85–93. https://doi.org/10.1111/anae.13316.Search in Google Scholar PubMed PubMed Central
10. Warner, MA, Arnal, D, Cole, DJ, Hammoud, R, Haylock-Loor, C, Ibarra, P, et al.. Anesthesia patient safety: next steps to improve worldwide perioperative safety by 2030. Anesth Analg 2022;135:6–19. https://doi.org/10.1213/ane.0000000000006028.Search in Google Scholar
11. Papenfuß, T, Roch, C. Ärztemangel am Beispiel der Anästhesie und Intensivmedizin - Ursachen, Folgen und Lösungsansätze. Anasthesiol Intensivmed Notfallmed Schmerzther 2012;47:352–7. https://doi.org/10.1055/s-0032-1313574.Search in Google Scholar PubMed
12. Ertmer, C, Aken, H, Skorning, M, Hahnenkamp, K. Postgraduate education in a changing occupational environment - evaluation of postgraduate education in anaesthesiology over a period of five years (2006-2011). Anasthesiol Intensivmed 2012;53:452–69.Search in Google Scholar
13. Roberts, S, Spain, B, Hicks, C, London, J, Tay, S. Telemedicine in the Northern Territory: an assessment of patient perceptions in the preoperative anaesthetic clinic. Aust J Rural Health 2015;23:136–41. https://doi.org/10.1111/ajr.12140.Search in Google Scholar PubMed
14. Wienhold, J, Mösch, L, Rossaint, R, Kemper, I, Derwall, M, Czaplik, M, et al.. Teleconsultation for preoperative evaluation during the coronavirus disease 2019 pandemic: a technical and medical feasibility study. Eur J Anaesthesiol 2021;38:1284–92. https://doi.org/10.1097/eja.0000000000001616.Search in Google Scholar PubMed PubMed Central
15. World Health Organisation. Consolidated telemedicine implementation guide. [Accessed 12 Feb 2023].Search in Google Scholar
16. Kasparick, M. Zuverlässige und herstellerübergreifende Medizingeräteinteroperabilität - Beiträge zur IEEE 11073 SDC-normenfamilie. Rostock, Germany: Universität Rostock; 2020.Search in Google Scholar
17. Kasparick, M, Schmitz, M, Andersen, B, Rockstroh, M, Franke, S, Schlichting, S, et al.. OR.NET: a service-oriented architecture for safe and dynamic medical device interoperability. Biomed Tech 2018;63:11–30. https://doi.org/10.1515/bmt-2017-0020.Search in Google Scholar PubMed
18. Czaplik, M, Voigt, V, Kenngott, H, Clusmann, H, Hoffmann, R, Will, A. Why OR.NET? Requirements and perspectives from a medical user’s, clinical operator’s and device manufacturer’s points of view. Biomed Tech 2018;63:5–10. https://doi.org/10.1515/bmt-2017-0043.Search in Google Scholar PubMed
19. Ohligs, M, Pereira, C, Voigt, V, Koeny, M, Janß, A, Rossaint, R, et al.. Evaluation of an anesthesia dashboard functional model based on a manufacturer-independent communication standard: comparative feasibility study. JMIR Hum Factors 2019;6:e12553. https://doi.org/10.2196/12553.Search in Google Scholar PubMed PubMed Central
20. Yilmaz, O, Janß, A, Radermacher, K. Applying user interface profiles to ensure safe remote control within the open networked operating room in accordance with ISO IEEE 11073 SDC. In: Healthcare and medical devices. New York, USA: AHFE International; 2022.10.54941/ahfe1002094Search in Google Scholar
21. Arney, D, Plourde, J, Goldman, JM. OpenICE medical device interoperability platform overview and requirement analysis. Biomed Tech 2018;63:39–47. https://doi.org/10.1515/bmt-2017-0040.Search in Google Scholar PubMed
22. Okamoto, J, Masamune, K, Iseki, H, Muragaki, Y. Development concepts of a smart cyber operating theater (SCOT) using ORiN technology. Biomed Tech 2018;63:31–7. https://doi.org/10.1515/bmt-2017-0006.Search in Google Scholar PubMed
23. Murray-Torres, T, Casarella, A, Bollini, M, Wallace, F, Avidan, MS, Politi, MC. Anesthesiology control tower-feasibility assessment to support translation (ACTFAST): mixed-methods study of a novel telemedicine-based support system for the operating room. JMIR Hum Factors 2019;6:e12155. https://doi.org/10.2196/12155.Search in Google Scholar PubMed PubMed Central
24. Gregory, S, Murray-Torres, TM, Fritz, BA, Ben Abdallah, A, Helsten, DL, Wildes, TS, et al.. Study protocol for the Anesthesiology Control Tower-Feedback Alerts to Supplement Treatments (ACTFAST-3) trial: a pilot randomized controlled trial in intraoperative telemedicine. F1000Res 2018;7:623. https://doi.org/10.12688/f1000research.14897.2.Search in Google Scholar PubMed PubMed Central
25. Miyashita, T, Mizuno, Y, Sugawara, Y, Nagamine, Y, Koyama, Y, Miyazaki, T, et al.. A pilot study of tele-anaesthesia by virtual private network between an island hospital and a mainland hospital in Japan. J Telemed Telecare 2015;21:73–9. https://doi.org/10.1177/1357633x14562735.Search in Google Scholar PubMed
26. Yilmaz, O, Wieschebrock, D, Heibeyn, J, Rademacher, K, Janß, A. Development and evaluation of a platform-independent surgical workstation for an open networked operating theatre using the IEEE 11073 SDC communication standard. In: Duffy, VG, editor. Digital human modeling and applications in health, safety, ergonomics and risk management. posture, motion and health. Cham: Springer International Publishing; 2020:79–92 pp.10.1007/978-3-030-49904-4_6Search in Google Scholar
27. Heibeyn, J, Jans, A, Radermacher, K. Multimodal touchless human machine interface for an IEEE 11073 SDC interconnected surgical workstation. In: 2020 IEEE conference on industrial cyberphysical systems (ICPS). Piscataway, USA: IEEE; 2020:437–41 pp.10.1109/ICPS48405.2020.9274767Search in Google Scholar
28. Weber-Chüo, T, Rockstroh, M, Franke, S, Hofer, M, Dietz, A, Neumuth, T, et al.. Evaluation eines integrierten OP-Saals auf Basis offener Standards in der Cochlea-Implantat-Chirurgie. Laryngo-Rhino-Otol 2021;100:987–96. https://doi.org/10.1055/a-1346-9227.Search in Google Scholar PubMed
29. Czaplik, M, Bergrath, S, Rossaint, R, Brodziak, T, Valentin, B, Hirsch, F, et al.. Employment of telemedicine in emergency medicine. Clinical requirement analysis, system development and first test results. Methods Inf Med 2014;53:99–107. https://doi.org/10.3414/me13-01-0022.Search in Google Scholar
30. Schröder, H, Beckers, SK, Ogrodzki, K, Borgs, C, Ziemann, S, Follmann, A, et al.. Tele-EMS physicians improve life-threatening conditions during prehospital emergency missions. Sci Rep 2021;11:14366. https://doi.org/10.1038/s41598-021-93287-5.Search in Google Scholar PubMed PubMed Central
31. Angerer, P, Glaser, J, Petru, R, Weigl, M. Gezielte Maßnahmen, die sich lohnen. Deutsche Ärzteblatt 2011;108:832–3.Search in Google Scholar
Supplementary Material
This article contains supplementary material (https://doi.org/10.1515/bmt-2024-0378).
© 2024 the author(s), published by De Gruyter, Berlin/Boston
This work is licensed under the Creative Commons Attribution 4.0 International License.
Articles in the same Issue
- Frontmatter
- Editorial
- Change of publication model for Biomedical Engineering/Biomedizinische Technik
- Research Articles
- Mechano-responses of quadriceps muscles evoked by transcranial magnetic stimulation
- A type-2 fuzzy inference-based approach enables walking speed estimation that adapts to inter-individual gait patterns
- DeepCOVIDNet-CXR: deep learning strategies for identifying COVID-19 on enhanced chest X-rays
- Prediction of muscular-invasive bladder cancer using multi-view fusion self-distillation model based on 3D T2-Weighted images
- Evaluation of the RF depositions at 3T in routine clinical scans with respect to the SAR safety to improve efficiency of MRI utilization
- A software tool for fabricating phantoms mimicking human tissues with designated dielectric properties and frequency
- MedShapeNet – a large-scale dataset of 3D medical shapes for computer vision
- Concept and development of a telemedical supervision system for anesthesiology in operating rooms using the interoperable communication standard ISO/IEEE 11073 SDC
Articles in the same Issue
- Frontmatter
- Editorial
- Change of publication model for Biomedical Engineering/Biomedizinische Technik
- Research Articles
- Mechano-responses of quadriceps muscles evoked by transcranial magnetic stimulation
- A type-2 fuzzy inference-based approach enables walking speed estimation that adapts to inter-individual gait patterns
- DeepCOVIDNet-CXR: deep learning strategies for identifying COVID-19 on enhanced chest X-rays
- Prediction of muscular-invasive bladder cancer using multi-view fusion self-distillation model based on 3D T2-Weighted images
- Evaluation of the RF depositions at 3T in routine clinical scans with respect to the SAR safety to improve efficiency of MRI utilization
- A software tool for fabricating phantoms mimicking human tissues with designated dielectric properties and frequency
- MedShapeNet – a large-scale dataset of 3D medical shapes for computer vision
- Concept and development of a telemedical supervision system for anesthesiology in operating rooms using the interoperable communication standard ISO/IEEE 11073 SDC