
Toxic Injury to the Gastrointestinal Tract After Ipilimumab Therapy for Advanced Melanoma
-
Benjamin Shepard

Abstract
Ipilimumab, cytotoxic T-lymphocyte-associated protein 4–blocking antibody, is known to precipitate tissue-specific immune-related adverse events. The second most common site for immune-related adverse events is the gastrointestinal tract, with toxic injury resulting in diarrhea, colitis, and enterocolitis. In the present case, a woman who received ipilimumab 2 weeks prior was found to have severe, diffuse corticosteroid-refractory gastrointestinal tract toxic injury affecting the stomach, small bowel, and colon.
Ipilimumab is a fully human, monoclonal antibody that, can promote antitumor activity against advanced melanoma by inhibiting cytotoxic T-lymphocyte-associated protein 4 (CTLA-4).1,2 Inhibition of CTLA-4 potentiates T-cell activation and proliferation, which produces tissue-specific inflammatory events referred to as immune-related adverse events (irAEs).3 Most commonly, gastrointestinal (GI) tract irAEs result in mild to moderate diarrhea or colitis. Enterocolitis can also be a result of a GI tract irAE, and it is classified as severe in approximately half of the reported cases.4,5 Although less frequent, diffuse upper and lower GI tract toxic injury can be caused by blockade of CTLA-4.5 Gastrointestinal tract toxic injury is the second most frequently encountered site of toxic injury, after skin, occurring in approximately 30% to 35% of patients presenting with toxic injury.6 The severity of GI tract toxic injury varies from asymptomatic to life threatening. This report describes a case of severe, diffuse corticosteroid-refractory GI toxic injury affecting the stomach, small bowel, and colon.
Report of Case
A 22-year-old white woman with stage IIIA melanoma presented to the emergency department with a 1-week history of nonbloody diarrhea, nausea, diffuse abdominal pain, and fever. Two weeks previously, the patient received intravenous ipilimumab, 565 mg. At the current presentation, she was unable to tolerate oral intake, and she reported having more than 10 bowel movements per day. She was admitted to the hospital and given fluids intravenously. A computed tomographic image of the abdomen and pelvis showed diffuse small bowel wall thickening. Stool, urine, and blood cultures were negative for infectious diseases, including Escherichia coli, Salmonella species, Shigella species, and Campylobacter jejuni. Results of a Clostridium difficile molecular assay were negative. She was treated empirically for severe immune-mediated enterocolitis with 2 mg/kg/d of methylprednisolone for 2 days. The patient's frequency of bowel movements and overall symptoms improved after 24 hours. She was discharged 48 hours after admittance and was given a prescription for prednisone, 60 mg/d for 14 days, with an anticipated taper over the following 6 weeks. The day after she was discharged, the patient returned to the emergency department with severe diarrhea, intolerance to oral intake, diffuse abdominal pain, and fever. She was readmitted to the hospital and given 2 mg/kg/d of methylprednisolone intravenously. Supplemental parenteral nutrition was also initiated.
The patient underwent GI tract esophagogastroduodenoscopy 24 hours after admission. Results revealed severely inflamed, diffusely erythematous mucosa in the stomach (Figure 1A) and diffusely erythematous, congested mucosa with overlying exudate in the duodenum (Figure 1B). Gastric biopsy specimens demonstrated focally active gastritis without granuloma formation (Figure 2). Giemsa stain results were negative for Helicobacter pylori. Duodenal biopsy specimens showed active duodenitis with acute cryptitis, crypt abscess formation, and mild villous blunting without granulomas or viral inclusions (Figure 3). Results of colonoscopy with examination of the terminal ileum revealed mild colonic inflammation, extending from the rectum to the mid-ascending colon (Figure 4A). The most severe condition appeared to be in a rectosigmoid distribution. The proximal ascending colon and cecum appeared to be spared. The ileal mucosa appeared erythematous and edematous, with overlying exudate (Figure 4B). Biopsy specimens of the rectum, the sigmoid, and descending, transverse, and proximal ascending colon demonstrated mild active colitis with acute cryptitis, crypt abscesses, and neutrophils within the lamina propria (Figure 5). Biopsy specimens of the distal ileum showed moderate active ileitis with acute cryptitis, crypt abscesses, and focal architectural distortion (Figure 6).
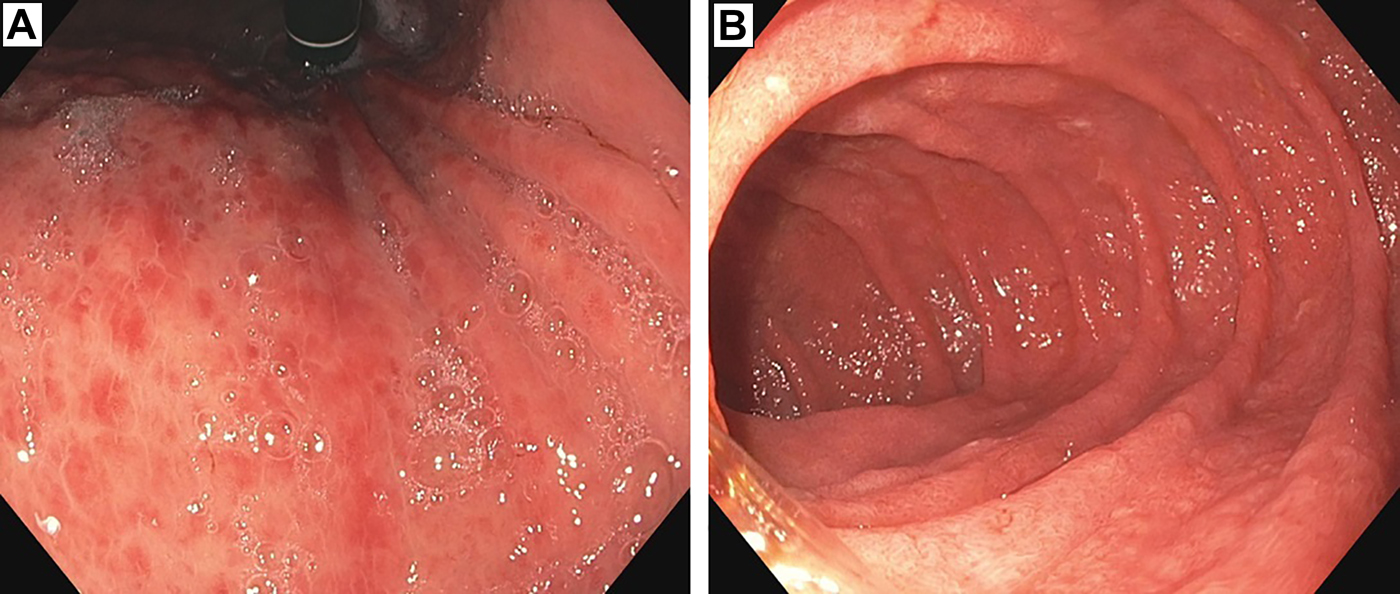
An image taken during esophagogastroduodenoscopy 2 weeks after ipilimumab administration revealed (A) severely inflamed, diffusely erythematous mucosa in the stomach and (B) diffusely erythematous, congested mucosa with overlying exudate in the duodenum.
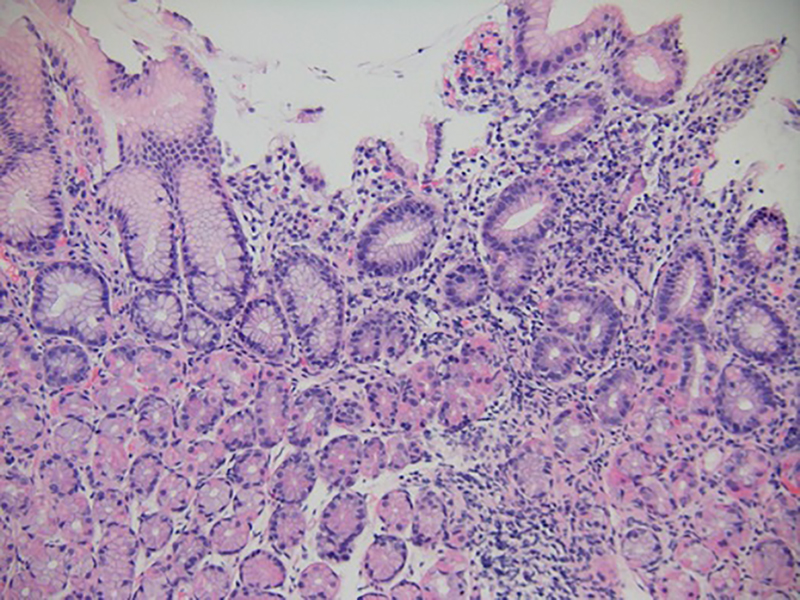
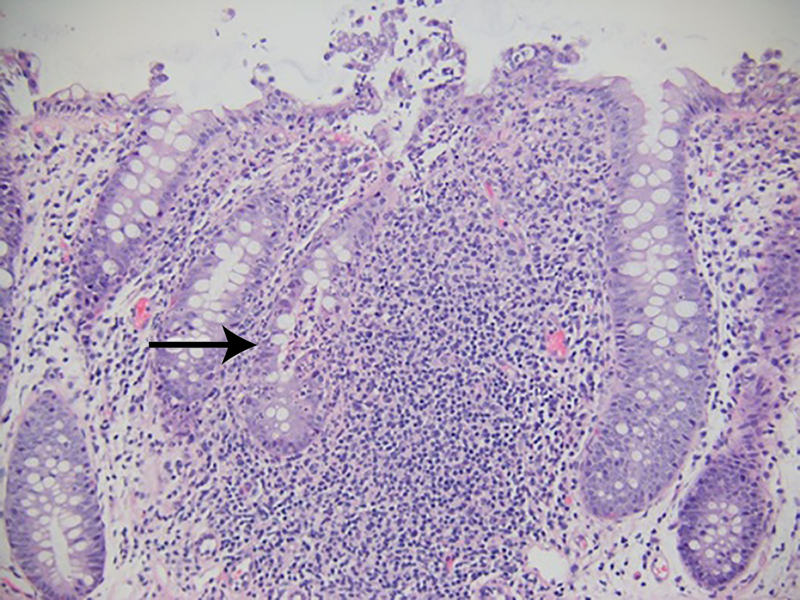
Gastric biopsy specimen taken 2 weeks after ipilimumab administration demonstrated focally active gastritis without granuloma formation (hematoxylin-eosin, original magnification ×100).
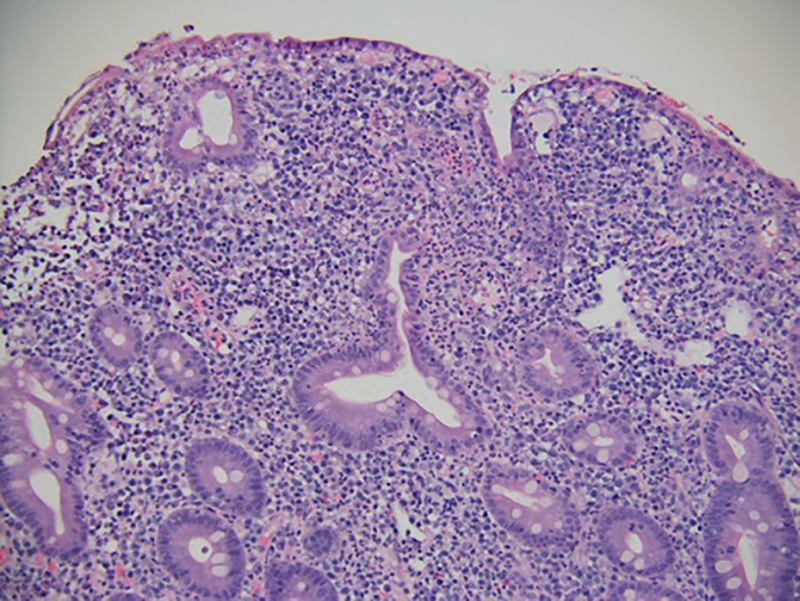
Duodenal biopsy specimens taken 2 weeks after ipilimumab administration demonstrated active duodenitis with acute cryptitis, crypt abscess formation, and mild villous blunting (hematoxylin-eosin, original magnification ×100).
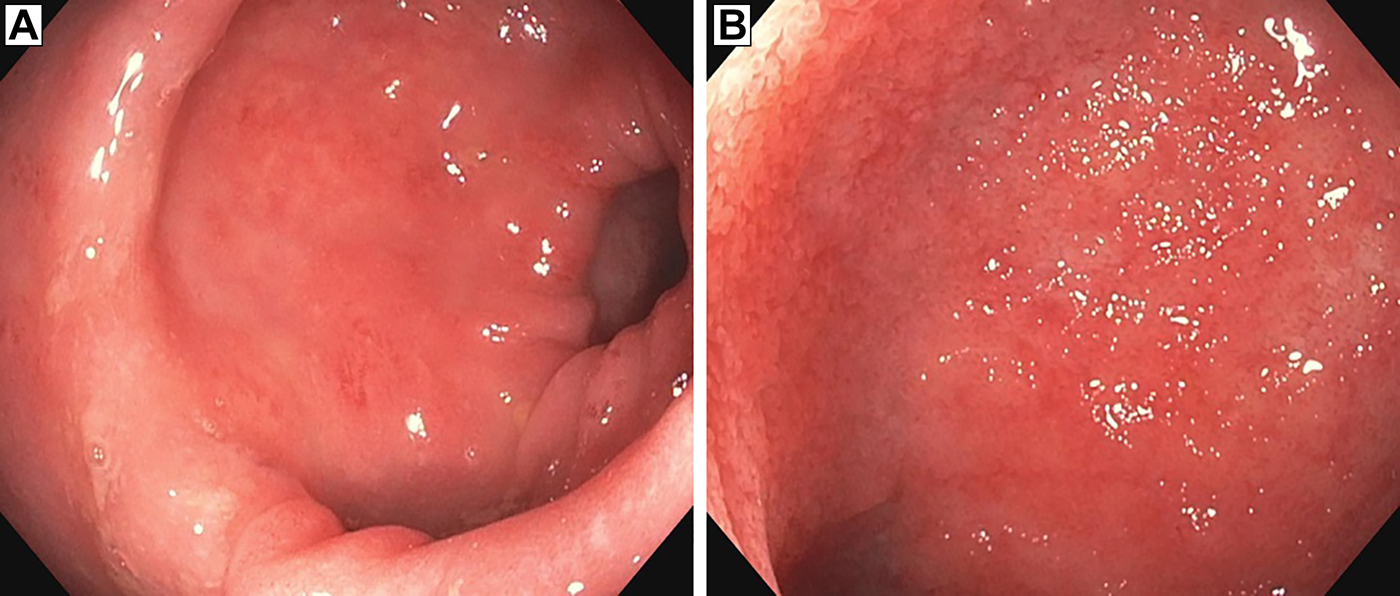
Colonoscopy with examination of the terminal ileum taken 2 weeks after ipilimumab administration showed (A) mild colonic inflammation, extending from the rectum to the mid-ascending colon and (B) erythematous and edematous ileal mucosa.
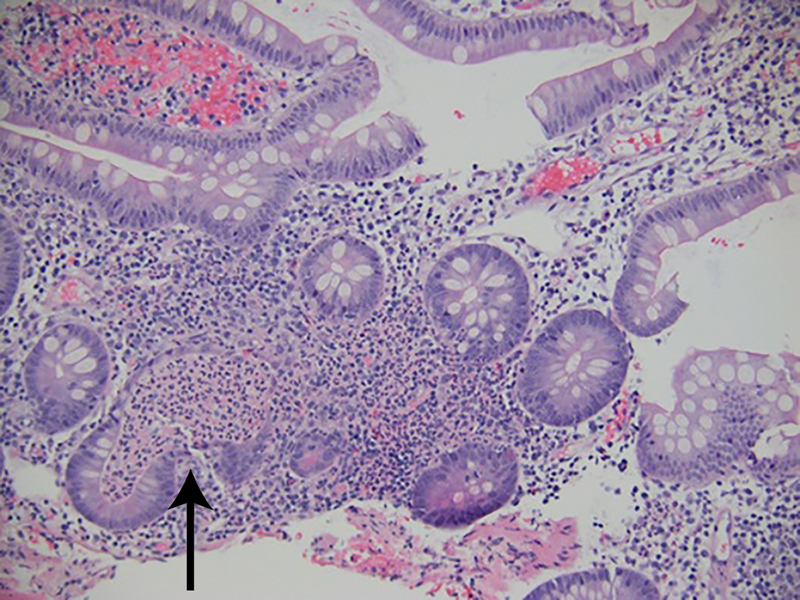
Biopsy specimens of the rectum, sigmoid, and descending, transverse, and proximal ascending colon taken 2 weeks after ipilimumab administration showed active colitis with acute cryptitis, crypt abscesses, and neutrophils within the lamina propria (hematoxylin-eosin, original magnification ×100).
Biopsy specimen of the distal ileum taken 2 weeks after ipilimumab administration showed active ileitis with acute cryptitis, crypt abscesses, and focal architectural distortion (hematoxylin-eosin, original magnification ×100).
After administration of 2 mg/kg/d of methylprednisolone for 72 hours, the patient's symptoms slightly improved, but abdominal pain and diarrhea continued. Stool, urine, and blood cultures were negative for concomitant infectious diseases. Given the diffuse nature of GI tract involvement and continued symptoms, the patient was given an intravenous infusion of infliximab, 5 mg/kg. Four days after infliximab administration, the patient reported an improvement in her symptoms, with near resolution of diarrhea and tolerance of small meals. Intravenous steroids and parenteral nutrition supplementation were discontinued, and a prednisone taper was initiated, starting at 60 mg/d and tapering by 10 mg/wk. The patient was discharged 9 days after admittance. A 2-week follow-up appointment revealed continued improvement in abdominal pain with occasional diarrhea, and the patient was given 5 mg/kg of infliximab intravenously. Within a week, the patient's diarrhea and abdominal pain resolved. Because of the severity of her GI tract irAEs, it was determined that ipilimumab would be contraindicated.
Discussion
Gastrointestinal tract toxic injury caused by ipilimumab is thought to arise from the dysregulation of GI tract mucosal immunity, evidenced by increased antibody titers to the enteric flora and levels of neutrophil-derived fecal calprotectin.7 A thorough review of the literature revealed a rare but undefined incidence of histologically proven diffuse upper and lower GI tract toxic injury from ipilimumab, with the esophagus and duodenum being the most commonly affected regions of the upper GI tract.8 Disease that is not confined to the large intestine may represent a more severe variant and portend a higher risk of complications.4 We postulate that in this case, diffuse toxic injury likely does not represent a separate clinicopathologic entity from confined toxic injury but, rather, a stronger intolerance to self-antigens of the GI tract mucosa. In light of the similarity between the distribution of GI tract mucosal injury in toxic injury caused by ipiliumamab and in GI tract graft-vs-host disease, predilection for inflammation of the lower GI tract and the relative infrequency of upper GI tract involvement could indicate a contribution from intestinal microflora and proportionate antigen exposure.9,10
Assessment of the severity of irAEs should be performed according to the National Cancer Institute's Common Terminology Criteria for Adverse Events, version 4.0,11 and upper and lower endoscopic evaluation should be considered in patients with toxic injury classified as grade 2 or higher.12 In patients with severe GI tract irAEs who do not experience clinical improvement from intravenous corticosteroids within 5 to 7 days or who relapse during treatment, a single dose of infliximab, 5 mg/kg, should be considered.5,13 Such treatment failure has been demonstrated in approximately 35% of patients with grade 3 to 4 GI tract toxic injury.9 Contraindications to antitumor necrosis factor α therapy, such as serious infections, sepsis, and perforation, should be excluded before consideration. Additional administration of infliximab can be performed if symptomatic response is insufficient after 2 weeks.13
Conclusion
Ipilimumab is a fully human, monoclonal antibody that inhibits CTLA-4 to promote antitumor activity against advanced melanoma.1,2 This inhibition of CTLA-4 can also potentiate T-cell activation and proliferation and produce irAEs.3 Consequent to the antitumor benefits of immune checkpoint therapy and its increasing role in cancer management, it is important and relevant for physicians in various specialties to become familiar with this classification of medication and to understand its potential for toxic injury.
References
1. Ratuapli SK , DepetrisG, ShepardB, NguyenCC. Severe colitis caused by biologics: what an endoscopist needs to know.Minerva Gastroenterol Dietol. 2014;60:287-290.Search in Google Scholar
2. Weber J. Review: anti-CTLA-4 antibody ipilimumab: case studies of clinical response and immune-related adverse events. Oncologist . 2007;12(7):864-872.10.1634/theoncologist.12-7-864Search in Google Scholar PubMed
3. Sznol M , CallahanM, YuanJ, WolchokJ. Key issues in the management of gastrointestinal immune-related adverse events associated with ipilimumab administration. Commun Oncol . 2013;10(12):351-358. doi:10.12788/j.cmonc.0055Search in Google Scholar
4. Ipilimumab [package insert]. New York, NY: Bristol-Myers Squibb; 2011.Search in Google Scholar
5. Tarhini A. Immune-mediated adverse events associated with ipilimumab CTLA-4 blockade therapy: the underlying mechanisms and clinical management. Scientifica (Cairo) . 2013;2013:857519. doi:10.1155/2013/857519Search in Google Scholar PubMed PubMed Central
6. Fecher L , AgarwalaS, HodiFS, WeberJ. Ipilimumab and its toxicities: a multidisciplinary approach. Oncologist . 2013;18(6):733-743. doi:10.1634/theoncologist.2012-0483Search in Google Scholar PubMed PubMed Central
7. Berman D , ParkerSM, SiegelJ, et al. Blockade of cytotoxic T-lymphocyte antigen-4 by ipilimumab results in dysregulation of gastrointestinal immunity in patients with advanced melanoma. Cancer Immun. 2010;10:11.Search in Google Scholar
8. Boasberg P , HamidO, O’DayS. Ipilimumab: unleashing the power of the immune system through CTLA-4 blockade. Semin Oncol . 2010;37:440-449. doi:10.1053/j.seminoncol.2010.09.004Search in Google Scholar PubMed
9. Beck KE , BlansfieldJA, TranKQ, et al. Enterocolitis in patients with cancer after antibody blockade of cytotoxic T-lymphocyte-associated antigen 4. J Clin Oncol. 2006;24(15):2283-2289.10.1200/JCO.2005.04.5716Search in Google Scholar PubMed PubMed Central
10. Beelen DW , ElmaaqacliA, MullerKD, HircheH, SchaeferUW. Influence of intestinal bacterial decontamination using metronidazole and ciprofloxacin or ciprofloxacin alone on the development of acute graft-versus-host disease after marrow transplantation in patients with hematologic malignancies: final results and long-term follow-up of an open-label prospective randomized trial.Blood. 1999;93(10):3267-3275.10.1182/blood.V93.10.3267.410k22_3267_3275Search in Google Scholar
11. The National Cancer Institute. Common Terminology Criteria for Adverse Events (CTCAE). Version 4.0. Washington, DC: US Dept of Health and Human Services; 2009.Search in Google Scholar
12. Della Vittoria Scarpati G , FuscielloC, PerriF, et al. Ipilimumab in the treatment of metastatic melanoma: management of adverse events. Onco Targets Ther . 2014;7:203-209. doi:10.2147/OTT.S57335Search in Google Scholar PubMed PubMed Central
13. Lemech C , ArkenauHT. Novel treatments for metastatic cutaneous melanoma and the management of emergent toxicities.Clin Med Insights Oncol. 2012;6:53-66. doi:10.4137/CMO.S5855Search in Google Scholar PubMed PubMed Central
© 2018 American Osteopathic Association
This work is licensed under the Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
Articles in the same Issue
- THE SOMATIC CONNECTION
- Stand Up and Climb Out of Ankle Spasticity
- OMT MINUTE
- OMT for Cancer Patients After Bowel Resection
- STILL RELEVANT
- Discovering Osteopathic Antiquity in Historical Osteopathic Pamphlets
- LETTERS TO THE EDITOR
- Chronic Pain Management: Perspective of an Osteopathic Medical Student in New Mexico
- ORIGINAL CONTRIBUTION
- Variations in Progression and Regression of Precancerous Lesions of the Uterine Cervix on Cytology Testing Among Women of Different Races
- Medical Student Decision-Making: Standard Surgical Excision or Mohs Micrographic Surgery to Manage Basal Cell Carcinoma
- BRIEF REPORT
- Evaluating the Effectiveness of One-on-One Conversations to Increase Colorectal Cancer Screening in a Community-Based Clinical Setting
- JAOA/AACOM MEDICAL EDUCATION
- Effect of Ultrasonography on Student Learning of Shoulder Anatomy and Landmarks
- CASE REPORT
- Toxic Injury to the Gastrointestinal Tract After Ipilimumab Therapy for Advanced Melanoma
- Nephroblastoma Arising in a Primary Testicular Teratoma in a Nonatrophic Testis of a 50-Year-Old Man
- THE SOMATIC CONNECTION
- It Makes a Difference What You Are Thinking When You Touch Someone Clinically
- OMT May Be Helpful in the Management of Benign Paroxysmal Positional Vertigo
- CSF Flow Has a Significant Respiratory Component
- Lymphatic Vessels Found in the Brain—Osteopathic Considerations, Part 2: Now in Humans and Monkeys
- CLINICAL IMAGES
- Pott Puffy Tumor
- IN YOUR WORDS
- Gratitude: Reflections and Belonging in the Osteopathic Family
Articles in the same Issue
- THE SOMATIC CONNECTION
- Stand Up and Climb Out of Ankle Spasticity
- OMT MINUTE
- OMT for Cancer Patients After Bowel Resection
- STILL RELEVANT
- Discovering Osteopathic Antiquity in Historical Osteopathic Pamphlets
- LETTERS TO THE EDITOR
- Chronic Pain Management: Perspective of an Osteopathic Medical Student in New Mexico
- ORIGINAL CONTRIBUTION
- Variations in Progression and Regression of Precancerous Lesions of the Uterine Cervix on Cytology Testing Among Women of Different Races
- Medical Student Decision-Making: Standard Surgical Excision or Mohs Micrographic Surgery to Manage Basal Cell Carcinoma
- BRIEF REPORT
- Evaluating the Effectiveness of One-on-One Conversations to Increase Colorectal Cancer Screening in a Community-Based Clinical Setting
- JAOA/AACOM MEDICAL EDUCATION
- Effect of Ultrasonography on Student Learning of Shoulder Anatomy and Landmarks
- CASE REPORT
- Toxic Injury to the Gastrointestinal Tract After Ipilimumab Therapy for Advanced Melanoma
- Nephroblastoma Arising in a Primary Testicular Teratoma in a Nonatrophic Testis of a 50-Year-Old Man
- THE SOMATIC CONNECTION
- It Makes a Difference What You Are Thinking When You Touch Someone Clinically
- OMT May Be Helpful in the Management of Benign Paroxysmal Positional Vertigo
- CSF Flow Has a Significant Respiratory Component
- Lymphatic Vessels Found in the Brain—Osteopathic Considerations, Part 2: Now in Humans and Monkeys
- CLINICAL IMAGES
- Pott Puffy Tumor
- IN YOUR WORDS
- Gratitude: Reflections and Belonging in the Osteopathic Family