Buerger Test for Erythromelalgia Revisited
-
William F. Wright

Abstract
Leo Buerger, MD, was the first to describe dependent rubor associated with marked atherosclerosis. Historically, dependent rubor has been described as erythromelalgia (or erythromelia), and terms such as chronic rubor, reactionary rubor, induced rubor, and hyperemic response have also been used to describe this sign associated with peripheral vascular disease. This brief review will reacquaint physicians with the Buerger test, which is used to assess arterial sufficiency, as well as erythromelalgia, and the proposed mechanisms responsible for erythromelalgia. The Buerger test is an important consideration when examining patients for erythromelalgia, which remains distinct from erythema associated with skin and soft-tissue infections.
Keywords: Buerger test, dependent rubor, erythromelalgia, rubor
In this 1924 publication, The Circulatory Disturbances of the Extremities: Including Gangrene, Vasomotor and Trophic Disorders,1 Leo Buerger, MD, was the first to describe dependent rubor associated with marked atherosclerosis.2,3 Buerger introduced several new physical signs for vascular conditions, including gangrene and peripheral vascular disease.1,3 Buerger emphasized the importance of recognizing potential symptoms associated with chronic atherosclerosis before gangrene is apparent, such as absent pulses, extremity coldness, foot and toe ulcers, impaired nail growth, poor capillary refill, foot pallor with limb elevation, and redness of the limb in the dependent position.1,3
Rubor involving the toes, sometimes the dorsal (Figure 1) and plantar (Figure 2) aspects of the foot at varying distances on a limb (to the ankle or higher) in the dependent or horizontal position, is a phenomenon Buerger termed erythromelalgia (Greek. erythrós, red; melia, limb).1,3 Terms such as dependent rubor, chronic rubor, reactionary rubor, induced rubor, and hyperemic response have also been used to describe erythromelalgia (or erythromelia).1,3 Although Buerger stated that erythromelalgia was most characteristic of thromboangiitis obliterans, it was also found with marked atherosclerotic occlusions of larger arteries in patients with or without diabetes mellitus.1

Erythromelalgia, or dependent rubor, with the dorsal foot in the dependent position (A) or at 60° in the horizontal position for 2 minutes (B).
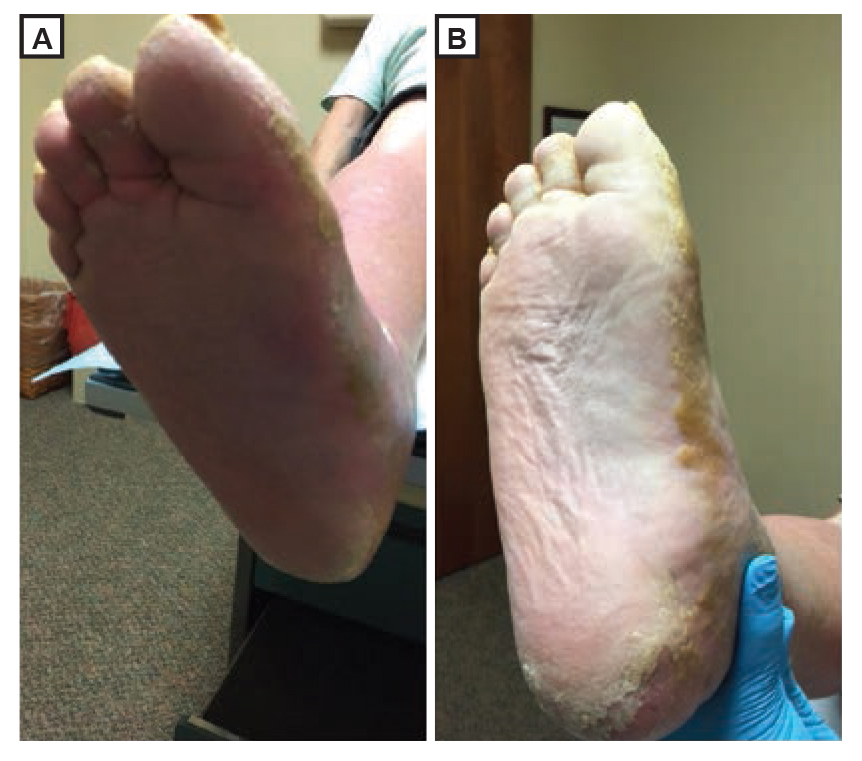
Erythromelalgia, or dependent rubor, with the plantar foot in the dependent position (A) or at 60° in the horizontal position for 2 minutes (B).
Physicians should be aware that erythromelalgia is a sign of clinically significant peripheral vascular disease and is independent of skin and soft-tissue infections. The purpose of this brief review is to reacquaint physicians with the Buerger test (which is used to assess arterial sufficiency), erythromelalgia, and the proposed mechanisms responsible for erythromelalgia, and also to describe the evidence-based foundation for their clinical reliability.
Pathophysiologic Process
Buerger stated that erythromelalgia is caused by a compensatory dilatation of superficial capillaries resulting from substantial luminal narrowing of larger arteries.1 In a prospective single-center trial, Schwartz et al4 used noninvasive video microscopy to document qualitative morphologic characteristics of lower-extremity nutritional skin microcirculation in patients with atherosclerosis. Fourteen study participants with artherosclerosis and 11 age-matched control participants were assessed for capillary blood flow velocity, capillary diameter, and number of flow-active capillaries. The study participants were found to have a capillary blood flow velocity of 0.16 mm/s, capillary diameter of 10.5 µm, and 6.8 capillaries per field, whereas the control participants had a capillary blood flow velocity of 0.10 mm/s, capillary diameter of 8.7 µm, and 5.3 capillaries per field. These data support erythromelalgia as the clinical manifestation of a compensatory dilatation of superficial capillaries and of an increased number of flow-active capillaries.
The Buerger Test
Placement of the healthy foot in the dependent position below heart level decreases capillary blood flow, and elevation produces no changes in flow.4 However, the same maneuver in patients with foot pain at rest and clinically significant atherosclerosis results in increased capillary blood flow with pedal dependency (ie, the patient is seated on an examination table with the foot in the down position) and decreased capillary blood flow on pedal elevation.4 The Buerger test should be used to evaluate patients suspected of having reduced circulation due to vascular obturation.1 When administering this test, physicians should elevate the limb to be perpendicular to the horizontal plane, which would cause pallor in patients with clinically significant peripheral vascular disease.1 On gradual lowering of the limb, the angle at which the color returns (ie, the angle of circulatory sufficiency) should be recorded.1 In a variation of the Buerger test, the affected limb should be elevated to 60º from the horizontal plane for 2 minutes, and then the limb should be placed in the dependent position for another 2 minutes.5 Limb pallor during this test indicates peripheral artery disease, as does rubor in the dependent position. Although Buerger noted that the angle of the leg that results in pallor is a valuable adjunct in the recognition of the extent of circulatory disturbance and prognosis, no studies have been published, to the authors’ knowledge, that correlate specific angles to the degree of arterial occlusion.
Sensitivity and Specificity of the Buerger Test
To better understand the diagnostic value of the Buerger test, Insall et al5 collected data among 55 patients (30 of whom had positive results using a variation of the Buerger test) with disabling claudication. The authors5 reported erythromelalgia in 43% of patients with a positive test result. Although 73% of patients who had a positive test result had palpable femoral pulses, popliteal and posterior tibial pulses were palpable in 7% of patients (no palpable dorsalis pedis pulses were detected). Arteriography demonstrated that 93% of arterial occlusions occurred below the inguinal ligament, and occlusions below the adductor hiatus were reported to be statistically significant among these patients (31% Buerger positive, 0% Buerger negative; P<.01).5 In a critical review of patients with suspected chronic ischemia of the lower extremities, McGee and Boyko3 reported a sensitivity of 100% and specificity of 54% of the Buerger test (positive likelihood ratio, 2.2; negative likelihood ratio, 0).
The cumulative evidence from these studies suggests that the Buerger test may be highly sensitive for detecting arterial occlusions below the popliteal fossa but is not specific for arterial occlusion above the popliteal fossa. Although the specificity is low, the high sensitivity suggests that a positive Buerger test result indicates probable occlusive peripheral vascular disease.
Conclusion
Physicians should consider using the Buerger test when peripheral vascular disease is suspected.3,6 The finding of erythromelalgia remains distinct from erythema associated with skin and soft-tissue infections. When infection is present, tenderness, edema, and cutaneous warmth over the affected region will often be elicited, indicating necrosis or purulence complicating a gangrenous limb.7 Patients with skin and soft-tissue infections usually have a predisposing condition such as ulcers, wounds, cutaneous fissuring, or toe-web intertrigo, as well as a history of saphenous vein removal, radiation therapy, or venous stasis disease.7 Erythema due to infection will remain on elevation of the affected limb.7 The Buerger test emphasizes the continued importance of a meticulous bedside examination, which remains the touchstone of clinical medicine, even in an era of growing overreliance on expensive and often deleterious dye-based imaging studies.
References
1. Buerger L. The Circulatory Disturbances of the Extremities: Including Gangrene, Vasomotor and Trophic Disorders . Philadelphia, PA: WB Saunders Company; 1924:128-129,162-165,214-215,390.Search in Google Scholar
2. Luft FC. Leo Buerger (1879-1943) revisited. Am J Med Sci. 2009;337(4):287. doi:10.1097/MAJ.0b013e318198d03010.1097/MAJ.0b013e318198d030Search in Google Scholar
3. McGee SR , BoykoEJ. Physical examination and chronic lower-extremity ischemia: a critical review. Arch Intern Med. 1998;158(12):1357-1364.10.1001/archinte.158.12.1357Search in Google Scholar
4. Schwartz RW , FreedmanAM, RichardsonDR, et al. Capillary blood flow: videodensitometry in the atherosclerotic patient. J Vasc Surg. 1984;1(6):800-808.10.1016/0741-5214(84)90012-0Search in Google Scholar
5. Insall RL , DaviesRJ, ProutWG. Significance of Buerger’s test in the assessment of lower limb ischaemia. J R Soc Med. 1989;82(12):729-731.10.1177/014107688908201209Search in Google Scholar
6. Endean ED , SloanDA, VeldenzHC, DonnellyMB, SchwarczTH. Performance of the vascular physical examination by residents and medical students. J Vasc Surg. 1994;19(1):149-154.10.1016/S0741-5214(94)70129-6Search in Google Scholar
7. Hirschmann JV , RaugiGJ. Lower limb cellulitis and its mimics: part II: conditions that simulate lower limb cellulitis. J Am Acad Dermatol. 2012;67(2):177,e1-e9. doi:10.1016/j.jaad.2012.03.02310.1016/j.jaad.2012.03.023Search in Google Scholar PubMed
© 2017 American Osteopathic Association
This work is licensed under the Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
Articles in the same Issue
- LETTERS TO THE EDITOR
- Landmark Article Transforms Traditional View of the Autonomic Nervous System
- AOA COMMUNICATION
- JAOA Peer Reviewers, 2016
- ORIGINAL CONTRIBUTION
- Use of Patient-Authored Prehistory to Improve Patient Experiences and Accommodate Federal Law
- BRIEF REPORT
- Somatic Dysfunction in the Diagnosis of Uncommon Ectopic Pregnancies: Surgical Correlation and Comparison With Related Pathologic Findings
- REVIEW
- Common Foot and Ankle Injuries: What Not to Miss and How Best to Manage
- CLINICAL PRACTICE
- Pectus Excavatum: A Review of Diagnosis and Current Treatment Options
- MEDICAL EDUCATION
- Comparison of Basic Science Knowledge Between DO and MD Students
- SPECIAL COMMUNICATION
- Buerger Test for Erythromelalgia Revisited
- CASE REPORT
- Ruptured Primary Omental Pregnancy Mimicking Adnexal Implantation
- Long Thoracic Nerve Injury Caused by Overhead Weight Lifting Leading to Scapular Dyskinesis and Medial Scapular Winging
- CLINICAL IMAGES
- Diffuse Idiopathic Skeletal Hyperostosis
Articles in the same Issue
- LETTERS TO THE EDITOR
- Landmark Article Transforms Traditional View of the Autonomic Nervous System
- AOA COMMUNICATION
- JAOA Peer Reviewers, 2016
- ORIGINAL CONTRIBUTION
- Use of Patient-Authored Prehistory to Improve Patient Experiences and Accommodate Federal Law
- BRIEF REPORT
- Somatic Dysfunction in the Diagnosis of Uncommon Ectopic Pregnancies: Surgical Correlation and Comparison With Related Pathologic Findings
- REVIEW
- Common Foot and Ankle Injuries: What Not to Miss and How Best to Manage
- CLINICAL PRACTICE
- Pectus Excavatum: A Review of Diagnosis and Current Treatment Options
- MEDICAL EDUCATION
- Comparison of Basic Science Knowledge Between DO and MD Students
- SPECIAL COMMUNICATION
- Buerger Test for Erythromelalgia Revisited
- CASE REPORT
- Ruptured Primary Omental Pregnancy Mimicking Adnexal Implantation
- Long Thoracic Nerve Injury Caused by Overhead Weight Lifting Leading to Scapular Dyskinesis and Medial Scapular Winging
- CLINICAL IMAGES
- Diffuse Idiopathic Skeletal Hyperostosis