The effects of modal value and imperative mood on self-predicted compliance to health guidance: the case of COVID-19
-
Sara Vilar-Lluch
Sara Vilar-Lluch is a Lecturer in Language and Linguistics at Cardiff University, UK. Her main research interests are in the areas of discourse analysis, Systemic Functional Linguistics, the expression of evaluation and emotion, and metaphor analysis, with a particular focus on health communication. Prior to Cardiff, she held research and teaching positions at the University of Nottingham.
 ,
Emma McClaughlin
,
Emma McClaughlin
Emma McClaughlin is a Research Fellow in Corpus Linguistics at the University of Nottingham. With research interests in corpus linguistics and discourse analysis, her research at the University of Nottingham has focused on health communication. She has worked on projects examining the discourses surrounding Coronavirus, menstrual health, avian influenza, and misinformation. Prior to Nottingham, she held a research position at Queen Margaret University in Edinburgh working on the topic of trust in public communication of COVID-19 in Scotland.
 ,
Svenja Adolphs
,
Svenja Adolphs
Svenja Adolphs is Professor of English Language and Linguistics at the University of Nottingham, UK. Her research interests are in the areas of corpus linguistics (in particular, multimodal spoken corpus linguistics), pragmatics and discourse analysis. She has published widely in these areas, including
Introducing Electronic Text Analysis (2006, Routledge),Corpus and Context: Investigating Pragmatics Functions in Spoken Discourse (2008, John Benjamins),Introducing Pragmatics in Use (1st ed. 2011, 2nd ed. 2020, Routledge, with Anne O’Keeffe and Brian Clancy),Spoken Corpus Linguistics: From Monomodal to Multimodal (2013, Routledge, with Ronald Carter) and theRoutledge Handbook of English Language and Digital Humanities (2020, Routledge, edited with Dawn Knight).Dawn Knight is Professor of Applied Linguistics at Cardiff University. Her research interests and expertise lie in the areas of corpus linguistics, discourse analysis, digital and online communication and non-verbal communication. She has led and/or contributed to a wide range of UK Research and Innovation (UKRI) and Welsh Government-funded multi-disciplinary and cross-institutional projects and has a sustained output of research publications, including two co-authored Palgrave books in 2020. Recent projects include the National Corpus of Contemporary Welsh (
CorCenCC ),FreeTxt and Interactional Variation Online (IVO ).Elena Nichele is a Lecturer in International Business Management at the University of Lincoln. Previously, she was a Research Fellow at the School of Computer Science, University of Nottingham (UK), where she was a member of the Horizon Digital Economy Research Institute and the Trustworthy Autonomous Systems Hub. Her expertise combines linguistics and marketing. She has been investigating perceptions, frequently expressed with the aid of technology and artificial intelligence, whilst focusing on the impact of identity and culture, with particular regard to the concept of authenticity. Her main research area is the complementary and interdependent relationship between global and local factors.

Abstract
Health messaging is effective if it achieves audience adherence to guidance. Through the lens of Systemic Functional Linguistics, we examine the expression of obligation in poster-based health campaigns (4 posters) employed during the COVID-19 pandemic in the UK by considering whether differences in grammatical mood and modality values impact on public compliance toward the message content. Effects of mood and modality variations are examined through a quantitative-cum-qualitative analysis of results from a representative survey (N = 1,089), which included closed questions on self-predicted compliance to health guidance and open questions on the respondents’ understanding of messaging. The quantitative results favour medium values of obligation (“should” vis-à-vis “must”) and directives in declarative mood for self-efficacy messages, and expressions of certainty when the need to take action to prevent negative outcomes is conveyed. The qualitative results show that, communication context and linguistic features being equal, message types (i.e., self-efficacy, moralising, fear appeals) and visual cues prevail in conditioning public reception. Moreover, since directives employing modality allow for speakers’ inclusion among the targeted addressees, they appear to offer more favourable outcomes than those in the imperative mood. This study provides empirical insights into the effects of modality and mood on health guidance compliance.
1 Introduction
The COVID-19 pandemic evidenced the importance of health communication for behavioural change and public adherence to health-promoting behaviours. The need for effective messaging addressing national audiences on a global scale motivated research on the importance of cultural values in achieving guidance support (e.g., Liu and Yang 2023), the communication affordances of social media (e.g., Love et al. 2023), governmental communications (e.g., Jaworska 2021; Vincent et al. 2023), and the reception of public health messages (e.g., McClaughlin et al. 2023). The social interest in effective health communication, however, expands beyond global health emergencies. Health-promoting behaviours, treatment seeking and adherence are essential for improving people’s lives (DiMatteo et al. 2012).
This study considers the linguistic strategies adopted in social media posters to promote health measures. Responding to the need to tailor messages’ content and form to target audiences (Salmon and Atkin 2003: 453), we examine whether expressions of obligation differing in strength and directness are associated with differences in self-predicted compliance. We consider message effectiveness for COVID-19 official communications in the United Kingdom, notably fear appeals, self-efficacy and moralising messages. We adopt a mixed-methods approach, combining insights from a Public Involvement Panel, a public survey, and a quantitative-cum-qualitative examination of responses to survey questions.
2 Literature review
2.1 Posters as a form of health communication
Social media interventions can be effective communicative strategies, also promoting behavioural change among populations with health disparities (in higher risk of incidence, prevalence and mortality) (Vereen et al. 2023). Poster communications present limitations derived from design constraints, such as providing simplified and eye-catching information (Ward and Hawthorne 1994), and have been associated with low credibility values (Salmon and Atkin 2003: 462). However, posters can effectively communicate health information to different communities, proving to be highly successful in reaching the target audiences (Salmon and Atkin 2003: 462). Posters are inexpensive and can reach large audiences over sustained periods of time, achieving a more continuous effect than other interventions (Barik et al. 2019; Hasanica et al. 2020; Naikoba and Hayward 2001; Pittet et al. 2000; Ward and Hawthorne 1994).
Successful poster communications have been used in handwashing and vaccination campaigns (Pittet et al. 2000; Qureshi et al. 2004; Thomas et al. 2005), to inform patients about health conditions, increasing awareness and encouraging learning (Ward and Hawthorne 1994), and as health-educational materials in schools (Hasanica et al. 2020). Poster campaigns used to promote handwashing in hospitals have been found to be more effective when posters promote the required action than when they only present the rationale behind the measure, which, despite raising awareness, have a lower impact on behavioural change (Thomas et al. 2005: 372). Effective handwashing campaigns have attested the need to accompany visual reminders with other measures, such as on-site surveillance and providing the required equipment (Pittet et al. 2000: 1311). Contrary to exclusively online-based health communications, posters can be adopted in offline settings, making them particularly valuable among communities with restricted Internet access (e.g., Fajri et al. 2022).
The studies reviewed show the appropriateness of keeping posters as part of nationwide health campaigns, highlighting the interest of understanding whether certain linguistic choices are more effective than others in conveying obligation. We consider official posters from the following UK Government campaigns – “Stay Home, Protect the NHS, Save Lives” and “Stay Alert, Control the Virus, Save Lives” – and examine (1) how differences in mood and modality affect self-predicted compliance with COVID-19 health messages in Britain; (2) how linguistic and compliance variations relate to health message type, notably fear appeals (emphasis of harmful physical or social consequences, Berry 2006: 109), moralising messages (reliance on moral values, Täuber 2018) and self-efficacy messages (provision of harm-reducing instructions, Seeger 2006); and (3) whether those linguistic alterations can be associated with different levels of audience engagement with the guidance.
2.2 Directives and advice-giving in health communication
Directives are traditionally defined as “attempts of varying degrees […] by the speaker to get the hearer to do something”, and include speech acts such as invites, advice, requests, or commands (Searle 1979: 13–14). Health-related interactions ordinarily involve some advice or guidance given by health professionals to the general public, and part of the body of research in directives has considered health communication contexts, both in face-to-face interactions, such as Heritage and Sefi’s (1992) pioneering study of the interactions between health visitors and first-time mothers, and written interactions, such as Locher’s (2010) study of health advice columns. In the context of the COVID-19 pandemic, use of directives has been examined in official communications such as COVID-19 briefings (Vincent et al. 2023) and advice letters issued by governments and health authorities (Yang 2021).
Since advice-giving, and directives more generally, involve forwarding “a preferred course of future action” (Heritage and Sefi 1992: 368), it is associated with normativity (the action is presented as standard or appropriate) and epistemic asymmetry (the audience is in need of the information) (Shaw et al. 2015: 319). The power asymmetry between advice givers and receivers carries interactional complexity, turning advice-giving into a potentially face-threatening act (Locher 2010: 45). Directives frequently involve a difference in the status of speakers and hearers. The authority of the speaker makes the directive valid and the hearer’s compliance necessary; in certain contexts, such as medical consultations, it may allow for utterances presented as information to be attributed “advice potential” (Sarangi and Clarke 2002: 298). This is the case for the frequent use of ‘hints’ (Ervin-Tripp 1976: 40) observed by Vincent et al. (2023) in the governmental briefings, and the indirect directive noted in Table 1.
Directives considered.
| Speech function | Mood | Lexicalisation obligation | Examples | Message type |
|---|---|---|---|---|
| Directive: suggestion/command | Declarative | Modulation: Subjective: Implicit | 1) “You should/must wear a face covering (over mouth and nose) if you are visiting hospital” | Self-efficacy |
| Direct | 2) “I wear this to protect you. Please wear yours to protect me. You should/must wear a face covering to keep your nose and mouth covered at all times on public transport, unless you have good reasons not to.” | Moralising | ||
| Directive: command | Imperative | Mood system | 3) “Stay at home. Save lives” | Self-efficacy |
| Direct | 4) “We’re all at risk. Follow the rules to keep everyone safe” | Fear appeal | ||
| 5) “Look her in the eyes and tell her you never bend the rules” | Moralising | |||
| Directive | Declarative | Inferred from information given (modalisation of certainty) | 6) “If you go out, you can spread it. People will/could die.” | Fear appeal |
| Indirect | 7) “Staying at home saves lives” | Self-efficacy |
All the directives considered in this study (Table 1) were displayed in health posters attributed to the UK Government and/or the National Health Service (NHS). Table 1 distinguishes directives according to directness (how literally we say what we mean, Ervin-Tripp 1976: 26), and suggestion and command types as realised by modulation strength variations. Ability to comply has been identified as a central feature of requests (Curl and Drew 2008); while requests acknowledge hearers’ willingness or capacity to comply, allowing for some degree of contingency, commands do not observe non-compliance (Craven and Potter 2010: 419, 426). These observations suggest that directives formulated as advice (“should” in Table 1) would trigger lower degrees of compliance than strong commands (“must” and imperative in Table 1), despite conveying the same information or health threat.
Effects of frame changes on decision-making are well-recognised in prospect theory (Tversky and Kahneman 1981), which has shown that people’s preferences about the same choices may be reversed depending on how the problem is formulated (e.g., “78 % of people will survive”, “22 % of people will die”). Acknowledging the lack of consistency in decision-making across frame changes, this study considers the effects of linguistic variation (directness and degree of obligation) in directives and health message variation (fear appeals, self-efficacy and moralising messages) upon people’s compliance.
3 Data and methods
This study combines quantitative and qualitative analyses of closed and open questions of a public survey to examine the effects of linguistic framing into respondents’ self-predicted compliance with health guidance. A Public Involvement Panel was integrated from conception of the project to finish. Panel members offered insights on message reception, sources consulted, and provided feedback to study materials, including the tailoring of survey questions and selection and adaptation of poster images used as stimuli, which all originated between April and July 2020 (Table 2, Section 3.1.1). This study received the approval of the Ethics Committee at the University of Nottingham (CS-2020-R77). The participants gave informed consent to participate in the study before taking part.
Health messages displayed in closed-questions to test effects of modality and mood.
| Message | Group A | Group B |
|---|---|---|
|
1–
Modulation: Obligation in self-efficacy messages |
 “You should wear a face covering (over mouth and nose) if you are visiting hospital” Contrived example |
 “You must wear a face covering (over mouth and nose) if you are visiting hospital” Original version, June 2020 |
|
2–
Modulation: Obligation in moralising messages |
 “You should wear a face covering to keep your nose and mouth covered at all times on public transport, unless you have good reasons not to.” Contrived example. Original reads “Wear a face covering to keep your nose and mouth covered …”, July 2020 |
 “You must wear a face covering to keep your nose and mouth covered at all times on public transport, unless you have good reasons not to.” Contrived example. |
|
3–
Modalisation: Probability in fear appeals |
 “If you go out, you can spread it. People will die.” Original version, April 2020 |
 “If you go out, you can spread it. People could die.” Contrived example. |
|
4–
Imperative versus indicative mood in directives |
 “Staying at home saves lives” Contrived example. |
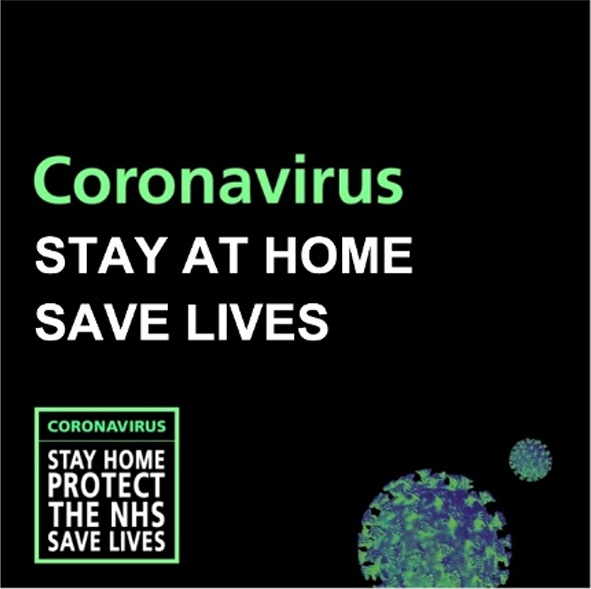 “Stay at home Save lives” Original wording, Welsh Government logo and affiliation removed for survey, April 2020 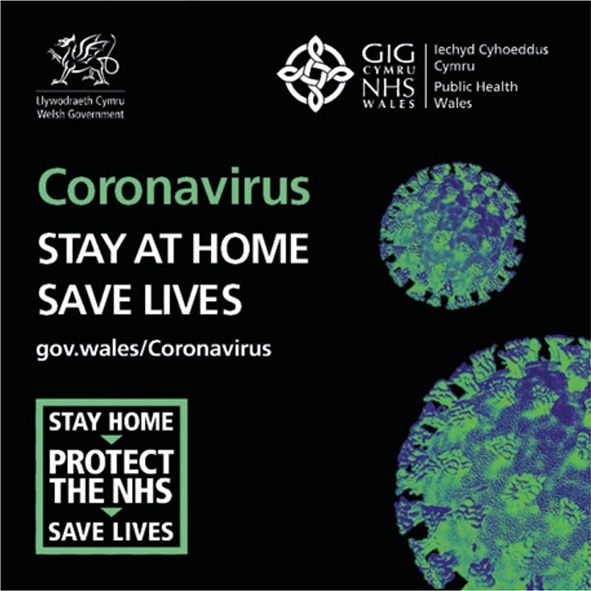 |
3.1 Survey
We commissioned Ipsos UK to survey a nationally representative sample of 1,089 adults aged 16–75 in Great Britain. The surveys took place on the online Omnibus between 1st and 3rd March 2022. Quotas were set on age, gender, region, social grade and working status. The data were weighted following the Random Iterative Model (RIM) (Sharot 1986) to the known offline population for age, working status and social grade within gender and region to correct small scale imbalances in the profile achieved (the demographic breakdown is available at McClaughlin et al. 2023, Appendix 2).
The survey design and the analysis was conducted by the project team. The survey questions discussed in this paper consider the effects that strength of obligation and directness of commands as realized by modality and mood choices may have on audience self-predicted compliance to health messages (Table 2, Figures 1 and 2); the full survey is available from McClaughlin et al. (2023, Appendix 3). Specifically, we consider the overall self-predicted compliance per message examined and differences by age group, the demographic variable that showed the most variation for the questions examined.

We’re all at risk (fear appeal).
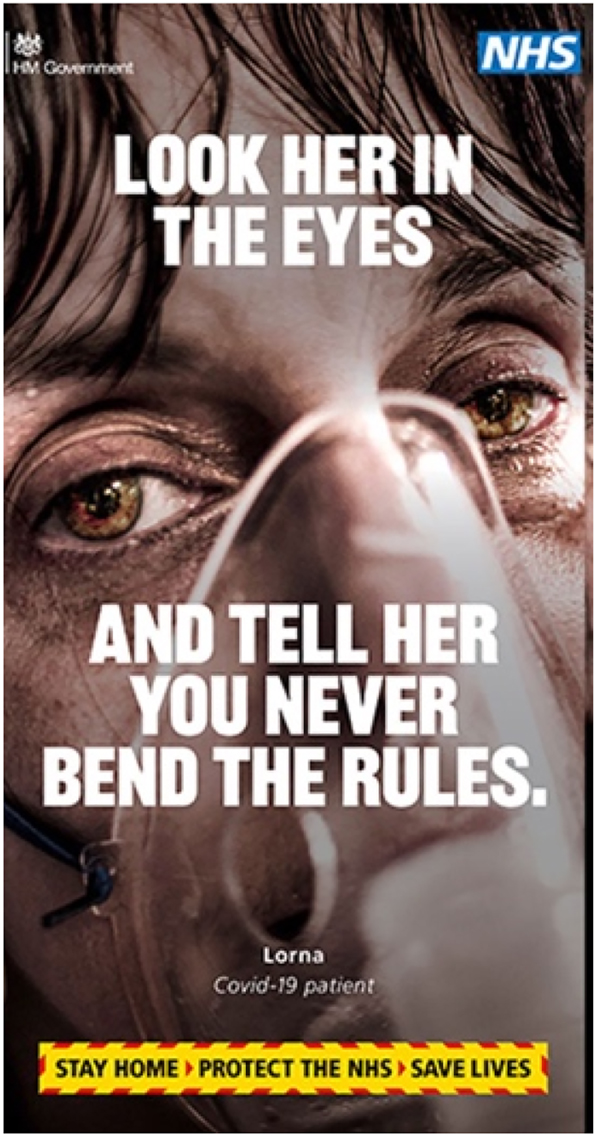
Look her in the eyes (moralising message).
3.1.1 Closed-questions
The participants were presented with either “Group A” or “Group B” images (Table 2), and were asked “How likely or unlikely would you be to follow the guidance in this public health message if such measures were re-introduced as a result of a new COVID-19 variant?”. They responded through a seven-point Likert scale: “extremely likely”, “very likely”, “fairly likely”, “neither likely nor unlikely”, “fairly unlikely”, “very unlikely”, “extremely unlikely” (presented at random in either forward or reverse order); a further “don’t know” response was anchored at the end. The images were selected at random per sample group and were identical except for the changes in modality or mood.
Modality was expressed through modal verbs and varied in value only (see analytical framework, Section 3.2.1): for each pair of images, one message would show a medium modality value of obligation or probability (“should”, “could”), and the other a high value, connoting strong imposition or certainty (“must”, “will”) (posters 1–3, Table 2, corresponding to fear appeals, moralising and self-efficacy messages, three message types employed in UK official campaigns). The effects of mood were examined by displaying the same directive in indicative and imperative mood (poster 4, Table 2, corresponding to a self-efficacy message).
3.1.2 Open-questions
The participants were presented with Figures 1 and 2 and asked “Looking at the public health communication below, what do you think it is trying to say or get across? And what is your reaction to this? Please write in below.” Both posters formulate the command in imperative mood, but differ in message type: Figure 1 is a fear appeal (the course of action is justified by evoking fear, “we’re all at risk”); Figure 2 is moralising (the course of action is evoked by appealing to moral values) – two message types with mixed-assessments in the literature (Berry 2006; Täuber 2018).
The interaction between message type and formulation of directive (imperative) was examined considering the participants’ engagement with the directive, exploring the inclusion of the course of action advised in the participants’ responses, and comparing the wording used by the participants in reporting the health guidance with the original formulation. The analysis assumed that, the more references the participants make to the guidance, the easier it is for them to focus on the behaviour promoted, thus increasing the likelihood of compliance.
3.2 Analytical framework
The qualitative analysis of open responses is based on the description of modality and mood offered in Systemic Functional Linguistics (SFL), which understand them as the clause elements that construe the social relationships between the actors involved, in order to examine how health message writers ask the audience to comply with the measures.
3.2.1 Modality
Modality encodes speakers’ judgements or requests. SFL distinguishes “Modalisation” and “Modulation”, depending on whether what is expressed constitutes a proposition (a description, Modalisation), or a proposal (Modulation). Modalisation involves expressions of Probability (“You can get ill”) and Usuality (“He usually gets travel-sick”) (Halliday and Matthiessen 2004: 147). Modulation involves Obligation (“You should wash your hands”), in command speech function, and Inclination (“I will wash my hands”), in offer speech function (Halliday and Matthiessen 2004: 147). Modality evaluations have polarity (positive or negative) and may show high, medium or low values (e.g., must, should, can) (Halliday and Matthiessen 2004: 143–149). Depending on the speaker’s viewpoint, modality has a subjective orientation, if the speaker stands as the source of the evaluation (“I oblige you to wash your hands”), or an objective orientation (“It is compulsory …”), if the evaluation source is presented as objective (Halliday and Matthiessen 2004: 149–150). The source of the evaluation can be explicit (i.e., “I oblige …” [subjective:explicit], “It is certain …” [objective:explicit]), or implicit (“You must wash …”, [subjective:implicit], “Certainly …”, [objective:implicit]) (2004: 149–150). See Figure 3 for a summary.

Modality as understood in SFL (adapted from Halliday and Matthiessen 2004: 150, Figure 4.25).
3.2.2 Mood
The mood system is the most basic grammatical encoding of the interpersonal function and defines the grammaticalization of the primary speech functions (statements, questions, offers and commands) (Halliday and Matthiessen 2004: 107–108). As a clause element, the Mood is composed of the Finite and the Subject elements. The Finite is part of a verbal group and it expresses tense (e.g., do, has) or modality (e.g., can, might); the Subject is a nominal group or personal pronoun and corresponds to the grammatical subject (Halliday and Matthiessen 2004: 111–112). Realisation variations in the inclusion and ordering of the Finite and Subject (Figure 4, represented by the arrows) define two main mood types: the imperative and the indicative, the latter further subdivided into declarative and interrogative (Halliday and Matthiessen 2004: 114).

Overview of the mood system as understood in SFG (adapted from Halliday and Matthiessen 2004: 23, Figure 1.9).
The indicative mood is typically used in information exchanges and presents both elements: SubjectˆFinite for declaratives (“He [S] must [F] be ill”), the unmarked[1] structure of statements; FiniteˆSubject for yes/no interrogatives (“Is [F] he [S] ill?”), and Wh-ˆFinite for Wh- interrogatives (Who is [F] ill?), the unmarked structures of questions.
The imperative mood is typically used for commands; its unmarked positive realisation does not present any mood element (“Wash your hands”), but we can find the Finite in negative imperatives (“Don’t …!) or to add emphasis (“Do wash …”), and sometimes also the Subject (“You wash …!”) (Halliday and Matthiessen 2004: 138). Besides these congruent realisations of speech functions, these can also be realised noncongruently (interpersonal metaphors) – e.g., commands realised as yes/no interrogatives (“Can you wash …?”) or declaratives (“you should wash …”), which offer more potential for negotiation (2004: 628, 632).
4 Results
4.1 Effects of modality and mood on self-predicted compliance
4.1.1 Direct commands with modal expressions of obligation
Messages 1 and 2 (posters 1 and 2, Table 2) constitute self-efficacy and moralising messages respectively:
| “You should /must wear a face covering (over mouth and nose) if you are visiting hospital” |
| “I wear this to protect you. Please wear yours to protect me. You should / must wear a face covering to keep your nose and mouth covered at all times on public transport, unless you have good reasons not to.” |
The messages indicate the guidance with direct commands and where it is to be followed (hospitals, public transport). Message 2 includes the rationale for following the guidance (protection). The modal auxiliaries “should” and “must” involve an implicit subjective orientation, and only differ in value (medium, high).
Figures 5 and 6[2] show that self-predicted compliance is high for both modal values in the two message types, thus challenging the expectation of obligation strength (modal value) functioning as a determining factor of public adherence to guidance.

Overall self-predicted compliance for high and medium values of Modulation:Obligation in message 1 (self-efficacy).

Overall self-predicted compliance for high and medium values of Modulation:Obligation in message 2 (moralising).
For message 1 (self-efficacy), there is a slightly significant difference in self-predicted compliance per Group A (“should”) (M = 5.40, SD = 1.712)[3] and Group B (“must”) (M = 5.13, SD = 1.860); t (1,061) = 2.201, p = 0.028. Overall compliance for the self-efficacy message (Figure 5) is somewhat higher for directives with medium value modality (“should”). While these results would indicate a disinclination for high values of obligation, suggesting a general reluctance towards directives that may appear more face-threatening, for message 2 (moralising) the difference in self-predicted compliance per Group A (“should”) (M = 5.27, SD = 1.761) and Group B (“must”) (M = 5.22, SD = 1.808) is not significant; t (1,063) = 0.511, p = 0.610 (see also Figure 6).
These results could be partly affected by the composition of message 2 poster: the modalised command is presented in smaller print, allowing the participants to read it as an elaboration of the visually salient guidance in imperative, displayed in larger yellow fonts (Kress and van Leeuwen 2021: 210–211).
Tables 3 and 4 below report the overall self-predicted compliance per age group for the two message types, and identify the older groups (55–75 and 45–54 years) as those who show the highest compliance for both messages in the four variations. However, preference for higher or medium modality values varies by age group and message type. For the self-efficacy message (Table 3), the participants favour medium modality values (“should”) regardless of age. While differences in modality preferences are minimal for the older groups, the younger participants, particularly the 25–34 age group, report a strong disinclination for high values of obligation (“must”), alongside the lowest levels of self-predicted compliance (Table 3).
Overall self-predicted compliance per age group for high and medium values of Modulation:Obligation in message 1 (self-efficacy).
| Age groups | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| 16–24 | 25–34 | 35–44 | 45–54 | 55–75 | ||||||
| Unweighted base | 160 | 202 | 192 | 210 | 325 | |||||
| Should* | Must* | Should* | Must | Should* | Must* | Should* | Must | Should* | Must*a | |
| Likely | 77 % | 53 % | 59 % | 45 % | 68 % | 73 % | 79 % | 74 % | 79 % | 78 % |
| Neither likely nor unlikely | 11 % | 13 % | 14 % | 14 % | 15 % | 8 % | 7 % | 11 % | 8 % | 7 % |
| Unlikely | 8 % | 25 % | 25 % | 36 % | 14 % | 16 % | 11 % | 14 % | 13 % | 16 % |
| Don’t know | 1 % | 6 % | 3 % | 5 % | 2 % | 2 % | 2 % | 1 % | 3 % | 2 % |
-
aPercentages marked with an asterisk (*) do not add up to 100 % due to rounding. Applicable to all the tables.
Overall self-predicted compliance per age group for high and medium values of Modulation:Obligation in message 2 (moralising).
| Age groups | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| 16–24 | 25–34 | 35–44 | 45–54 | 55–75 | ||||||
| Unweighted base | 160 | 202 | 192 | 210 | 325 | |||||
| Should | Must* | Should* | Must | Should | Must | Should* | Must* | Should* | Must | |
| Likely | 61 % | 51 % | 53 % | 64 % | 72 % | 67 % | 71 % | 79 % | 78 % | 81 % |
| Neither likely nor unlikely | 19 % | 17 % | 19 % | 17 % | 16 % | 12 % | 11 % | 7 % | 6 % | 8 % |
| Unlikely | 18 % | 21 % | 25 % | 18 % | 8 % | 21 % | 16 % | 12 % | 16 % | 11 % |
| Don’t know | 2 % | 10 % | 2 % | 1 % | 4 % | * | 1 % | 1 % | 1 % | * |
Instead, for message 2 (moralising), the older populations (age groups 45–54 and 55–75) and the 25–34 age group favour the high imposition of “must” (Table 4), while the youngest age group (16–24) shows the highest rejection for strong obligation (see Appendix, Figure 9, for diagram with significant mean differences of self-predicted compliance per group and framing variation).
The self-efficacy message triggered high levels of self-predicted compliance across all age groups except the 25–34 group; instead, the moralising message worked better for the older audiences, with the younger populations showing medium degrees of compliance (Table 4). The tenor clash observed in message 2b, with the directive in imperative formulated as a request (“please wear …”) and the command connoting strong obligation (“You must …”), could contribute to the resistance of the young respondents.
4.1.2 Indirect commands: compliance conveyed from the consequences of the health risk
Fear appeals, like message 3, are common health messages (Berry 2006: 109). In message 3, the need to follow the guidance is inferred from the negative consequences of non-compliance, and the likelihood of risk is modalised. The visuals accompanying the text further emphasise the severity of the virus (poster 3, Table 2): a long shot of an elderly man in bed receiving assistance acquires visual salience through colours (bright orange and yellow), the absence of gaze contact with the viewer contributes to offer the represented scene, in impersonal distance, as factual information (Kress and van Leeuwen 2021: 118).
| “If you go out, you can spread it. People will/could die.” |
Although compliance values are high for both variations of the message (Figure 7), there is a significant difference in self-predicted compliance per Group A (“will”) (M = 5.40, SD = 1.684) and Group B (“could”) (M = 5.13, SD = 1.810); t (1,058) = 2.532, p = 0.011.

Overall self-reported compliance for high and medium values of Modalisation:Probability in fear appeals (message 3).
The association of stronger modality (“will”) with greater compliance suggests that conveying certainty when reporting the outcomes of a health risk promotes the audience’s inclination to engage in preventive actions, and reflect previous studies, which stress the importance of informing the audience of the magnitude of the health threat in promoting guidance (e.g., Berry 2006: 109; Hale and Dillard 1995).
Contrary to the modulation of obligation in self-efficacy or moralising messages, Table 5 shows that all age groups reported a preference for high modality values for the fear appeal.
Overall self-reported compliance per age group for high and medium values of Modalisation:Probability in fear appeals (message 3).
| Age groups | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| 16–24 | 25–34 | 35–44 | 45–54 | 55–75 | ||||||
| Unweighted base | 160 | 202 | 192 | 210 | 325 | |||||
| Will | Could* | Will* | Could* | Will | Could | Will | Could | Will | Could | |
| Likely | 61 % | 54 % | 63 % | 46 % | 72 % | 67 % | 79 % | 75 % | 79 % | 77 % |
| Neither likely nor unlikely | 24 % | 21 % | 18 % | 29 % | 15 % | 10 % | 8 % | 13 % | 5 % | 10 % |
| Unlikely | 12 % | 19 % | 15 % | 22 % | 10 % | 21 % | 11 % | 10 % | 13 % | 14 % |
| Don’t know | 3 % | 7 % | 3 % | 2 % | 3 % | 2 % | 2 % | 2 % | 3 % | – |
The 25–34 age group showed the lowest compliance for medium probability (“could”), and the youngest population (16–24) showed the greatest refusal of high probability values (“will”) (see Appendix, Figure 9). As for the other message types, the older audiences reported higher compliance, regardless of the wording. Previous studies have also identified age as a determining factor for fear appeals’ success (Berry 2006: 109; Hale and Dillard 1995; Institute of Medicine 2015).
4.1.3 Health guidance as imperative or declarative
The impact of directness in commands was examined with message 4 (poster 4, Table 2), considering differences in mood. Like message 1, message 4 is a self-efficacy message, but instead of employing modulation of obligation, the directive is either inferred from an information-giving declarative (indirect), or formulated in imperative (direct).
| “Staying at home saves lives”/“Stay at home Save lives” |
The responses show a significant difference in self-predicted compliance per Group A (declarative) (M = 5.23, SD = 1.819) and Group B (imperative) (M = 5.21, SD = 1.857); t (1,061) = 0.160, p = 0.018 (see Figure 8 for percentages), with higher self-predicted compliance reported for the declarative.

Overall self-predicted compliance for directives in declarative and imperative mood.
The disinclination for directness is consistent with the preference for medium values of Modulation:Obligation reported for message 1.
Self-predicted compliance for mood variation is conditioned, to a point, by age (Table 6, see also Appendix Figure 9).
Overall self-predicted compliance per age group for directives in declarative (decl.) and imperative (imp.) mood.
| Age groups | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| 16–24 | 25–34 | 35–44 | 45–54 | 55–75 | ||||||
| Unweighted base | 160 | 202 | 192 | 210 | 325 | |||||
| Decl.* | Imp. | Decl. | Imp. | Decl. | Imp. | Decl.* | Imp. | Decl.* | Imp. | |
| Likely | 60 % | 52 % | 53 % | 40 % | 66 % | 64 % | 76 % | 78 % | 79 % | 80 % |
| Neither likely nor unlikely | 12 % | 20 % | 17 % | 28 % | 13 % | 15 % | 9 % | 7 % | 6 % | 8 % |
| Unlikely | 26 % | 21 % | 22 % | 28 % | 18 % | 20 % | 14 % | 14 % | 13 % | 12 % |
| Don’t know | 1 % | 7 % | 8 % | 4 % | 3 % | 1 % | 2 % | 1 % | 3 % | – |
While the two oldest age groups reported slightly higher values of compliance for the imperative, the younger audiences, especially the 25–34 age group, reported lower levels for the imperative, supporting the results obtained for Modulation: Obligation in message 1 (Table 3).
4.2 Engagement with health guidance
4.2.1 Engaging with directives
The effect of direct commands in message reception was examined considering the open question responses for the posters displayed in Figures 1 (fear appeal) and 2 (moralising). Figure 1 precedes the directive (“Follow the rules …”) with the rationale to comply (“We’re all at risk”), attributes salience in the poster (large fonts in yellow) and promotes adherence by emphasising the audience’s lack of immunity. Figure 2 only includes the directive in imperative (“Look her in the eyes and tell …”), and the need to comply with the guidance is inferred from the appeal to the audience’s moral values, triggered by the combination of the textual and the visual messages: an extremely close-up shot of a woman severely ill, explicitly described as “Covid-19 patient” and individuated (“Lorna”). The poster invites engagement and attributes visual salience to the ventilator and the indirect gaze of the patient; the absence of direct eye contact contributes to promote empathy, and the high angle connotes powerlessness (Kress and van Leeuwen 2021: 62, 143).
The responses were coded following the categories noted below. Broadly, we distinguished between those responses that were merely descriptive, of the poster or the respondents’ evaluations, and those responses that included references to the directive.
Descriptive
Description: personal evaluation: the participants offer evaluations about the message (“I feel very positive to see this ad.”, “Getting bored with it”). Message fatigue was identified for both posters, especially for Figure 1. The references to the political scandal Partygate[4] were also coded as evaluations (“This makes me think that there is one rule for the population and one for the prime minister and the MPs […]”).
Description: poster: the participants describe the poster, either commenting on how it looks or the intentions attributed to the messaging (“this poster gets to the point clearly”, “Trying to scare people”).
Description: poster & personal evaluation: the participants provide descriptions of the poster including evaluations (“Pretty clear. Just a great pity that the ones that made the rules didn’t apply them to the,selves (sic) […]”, “Nobody is safe but I don’t think it is necessarily correct”, “Trying to spread alarm. I scoff at such fear porn”). These responses frequently express disagreement, either with the poster or with the government in power at the time.
Engagement with the directive
Description: poster & explicit directive: the participants describe the poster and include a directive restating or paraphrasing the guidance (underlined), (“Good visual representation of 2 m social distancing. Tells people that no one is immune from catching covid. Everyone needs to help prevent its spread […]”).
Directive: information: the participants unpack the meaning of the textual or visual information of the poster, but do not explicitly report the directive (“Social distancing helps”, “That ‘bending’ the rules can have serious effects on people’s lives”).
Directive: information & personal evaluation: the participants convey the information provided in the message and expand on it with evaluations, without engaging with the directive (“Telling everyone we (sic) at risk. I don’t care”).
Directive: information & explicit directive: the participants paraphrase the information provided and formulate the directive, either by employing the imperative mood or Modulation:Obligation; “Covid does not discriminate so people need to follow the rules to help keep everyone safe” [Modulation:Obligation:Objective:Implicit],[5] “everyone is at risk so we must protect each other” [Modulation:Obligation:Subjective:Implicit], “Anyone can catch and spread the illness. Take necessary precautions” [imperative].
Directive: explicit directive: the participants formulate the command, either using the imperative mood or Modulation:Obligation, without reporting information backing the guidance (“Keep your distance […]” [imperative], “Everyone needs to follow the rules […]” [Modulation: Obligation:Objective:Implicit]). The directives formulated as non-finite clauses, with the finite elided, were also coded as “explicit” (“To keep our distance to keep safe”, which stands for “[The health communication is trying to say that we have/need ] to keep our distance to keep safe” [Modulation:Obligation:Objective:Implicit]).
Absence of engagement with the health message or the poster
“Don’t know”
No answer
Table 7 provides a summary.
Engagement with directives in health message reception.
| Coding | We’re all at risk | Total Figure 1 | Look her in the eyes | Total Figure 2 | Total | |
|---|---|---|---|---|---|---|
| (Figure 1) | (Figure 2) | |||||
| Absence of engagement | “Don’t know” | 54 | 141 | 50 | 133 | 104 |
| No answer | 87 | 83 | 170 | |||
| Descriptive | Description: personal evaluation | 79 | 313 | 72 | 547 | 151 |
| Description: poster | 215 | 451 | 666 | |||
| Description: poster & personal evaluation | 19 | 24 | 43 | |||
| Engagement with the directive | Description: poster & explicit directive (modulation: obligation/imperative mood) | 1 | 635 | 3 | 409 | 4 |
| Directive: information | 176 | 110 | 286 | |||
| Directive: information & explicit directive (modulation: obligation/imperative mood) | 47 | 15 | 62 | |||
| Directive: explicit directive (modulation: obligation) | 89 | 45 | 134 | |||
| Directive: explicit directive (imperative mood) | 308 | 230 | 538 | |||
| Directive: declarative (formulated as declarative) | 11 | 4 | 15 | |||
| Directive: information & personal evaluation | 3 | 2 | 5 | |||
The participants showed reasonable engagement with the directive of the posters. A total of 1,044 responses included some engagement, in contrast to 860 purely descriptive responses, which presented more references to the poster and intentions attributed to message writers than evaluations (Table 7). However, the level of engagement with the directives differed across the messages. Figure 1 provoked a higher engagement, with 635 responses referring to the directive and 313 descriptive responses (Table 7). Instead, Figure 2 is associated with lower engagement, with 409 responses referring to the directive and 547 descriptive responses. Of those participants who engaged with the directive of Figure 2, 110 paraphrased the information provided in the visual format (e.g., “Breaking the rules has serious medical effects”), without including further reference to the guidance. The different engagement with the directives suggests that the participants paid more attention to the guidance promoted in Figure 1 than in Figure 2, which would make Figure 1 a more effective health message. The higher number of descriptive responses triggered by Figure 2 suggests that the visuals and message type (moralising) divert the audience’s attention from the actual guidance; instead, Figure 1 presents a long shot offering the action to be adopted (though the distance is not specified, and the picture is inconsistent with the slogan, “stay at home”).
4.2.2 Reporting the health guidance
The qualitative analysis of the open-questions has identified the imperative mood as the preferred form to report a directive, all directed to a second person addressee which does not include the speaker (Table 7). This preference for the imperative contrasts with the higher self-predicted compliance for the self-efficacy message in declarative mood observed in the quantitative analysis (Figure 8). Such a contrast could be partly influenced by the original adoption of the imperative in the messages considered.
In what follows, we consider the participants’ use of modulation in reporting commands in their answers, observing whether these uses reflect the preferences reported for the closed-questions, and how the participants position themselves towards the guidance. The responses that engage with the directives employing modality are comparatively more prominent for Figure 1 and show a preference for objective implicit forms of modulation, followed by subjective implicit forms (Table 8).
Use of modality in reporting directives of health messages.
| Formulating obligation | We’re all at risk (Figure 1) | Look her in the eyes (Figure 2) | ||
|---|---|---|---|---|
| Modulation: obligation | Linguistic form | Addressee of directive | Linguistic form | Addressee of directive |
| Objective: implicit | Total: 43 | Total: 11 | ||
| “need to” (35) | 1 plural (17) | “need to” (8) | 1 plural (4) | |
| 3 plural (13) | 1 singular (1) | |||
| 1 singular (1) | 2 singular (1) | |||
| 2 singular (3) | 3 plural (2) | |||
| Impersonal passive (1) | ||||
| “have [a responsibility/a duty]” (4) | 1 plural (2) | “have [a duty]” (2) | 1 plural (2) | |
| 3 plural (2) | ||||
| “have to” (2) | 1 plural (1) | Elision of finite (15) | 1 plural (2) | |
| 3 plural (1) | Indefinite (speaker included) (13) | |||
| Elision of finite (29) | 1 plural (3) | |||
| 2 plural (1) | ||||
| 2 singular (4) | ||||
| Indefinite (21) | ||||
| Objective: explicit | Total: 5 | |||
| “it’s (very) important …” (4) | 1 plural (1) | |||
| 3 plural (1) | It is important … (1) | Indefinite (speaker included) | ||
| Impersonal (2) | ||||
| “it is required” (1) | Impersonal-passive (1) | |||
| Subjective: implicit | Total: 34 | Total: 22 | ||
| “must” (6) | 1 plural (4) | “will” (1) | 2 singular (1) | |
| 3 plural (2) | “should” (21) | 1 plural (4) | ||
| “shall” (1) | 1 plural (1) | 2 singular (9) | ||
| “should” (27) | 1 plural (3) | 3 plural (7) | ||
| 3 plural (10) | Impersonal passive (1) | |||
| 2 singular (3) | ||||
| Impersonal-passive (1) | ||||
| Subjective: explicit | Total: 1 | – | ||
| (elision: “[the ad is] asking people …”) | 3 plural (1) | |||
Objective implicit expressions of obligation include “need to”, most commonly (“[…] people need to follow the rules to help keep everyone safe”), “have to” (“Everyone has to follow the rules”), and the relational process “have” with “responsibility” or “duty” as usual attributes (“WE all have responsibility to protect each other”). “Need to” is the expression of obligation most often used to refer to an addressee including the speaker (first person plural) (Table 8). Occasionally, the Subject and the Finite are elided and the participants directly report the hypotactic clause, focusing on the action that needs to be accomplished (“[we have/need] To keep our distance to keep safe”). In these cases, the addressees of the directive have been retrieved from the personal pronouns or possessive determiners included in the response (first person plural determiner “our” in the previous example); when referents were not available, the addressee was noted as “indefinite”. Expressions of obligation with an objective explicit orientation are, in contrast, scarce and only given for Figure 1. The objective explicit orientation construes the obligation as a projection (“It doesn’t matter if you’re relatively young […] therefore it’s important to maintain a safe distance”), and the addressee is often left unspecified, inferred to include both the speaker and third parties.
The most recurrent expression of obligation with a subjective implicit orientation is the medium value modal auxiliary “should”, especially for third person plural addressees (“Everyone is at risk and so everyone should be careful”). References to third person plural addresses may implicitly include the speaker (“everyone” in the example) or not (references to “people”). The high value modal “must” has also been observed, especially when targeting a group of addressees inclusive of the speaker (“We must continue to maintain social distancing.”), but it is comparatively infrequent (Table 8). These findings adhere to the preference for “should” over “must” in message 1 (self-efficacy) observed in the closed-questions. Other modal auxiliaries employed to express obligation are “shall” (“[…] we’re all in the same boat therefore shall we all follow the rules”) and “will” (“you will stick to the rules so […]”), though both are rare in this data.
Although the figures are too small to establish any statistically significant association, Table 8 shows that different modulation types involve different positionings of the speakers towards the obligations conveyed, explicitly construing the obligation as concerning them or others only. In contrast, all directives formulated in imperative mood were addressed to second person addressees.
5 Discussion and conclusion
The recurrent references to the socio-political milieu observed in the open question responses illustrate that health message reception is conditioned by a variety of factors that are difficult to disaggregate, thus making it challenging to determine the actual influence of linguistic variables such as mood or modality on the audience’s compliance. Comparing the participants’ engagement with the directives of Figures 1 and 2 (Section 4.2), and examining the compliance reported for the posters with grammatical variations (Section 4.1), suggests that the framing of the command can affect message reception. However, our survey design does not allow us to completely disentangle the framing effects achieved by linguistic variation from those derived from message type (moralising, fear appeal, self-efficacy). The visual features were not explicitly examined, yet multimodal studies on health communication have highlighted their importance for message effectiveness (Jones et al. 2023).
The closed-question responses have shown some relatively significant but overall modest differences in self-predicted compliance (0.05 > p > 0.01) by modality and mood variations. With the exception of the 24–35 age group, the participants reported high levels of compliance overall. These results suggest a ceiling effect for self-predicted compliance for all message types, since the majority of participants scored high values for both variables of mood and modality tested. It is therefore difficult, if not impossible, to relate the compliance score to such variables exclusively. This observation could either suggest that the participants exhibited reservations in providing authentic reports, or that in a health crisis, individuals tend to show high levels of compliance regardless of the message they are exposed to due to factors external to the health communications, such as the experience of the pandemic itself.
Further factors to consider include the official sources displayed in the posters (NHS, UK Government), and the two-year exposure to similar health guidance that the participants had had by the time of participating in the survey. The responses for the open questions relating to Figures 1 and 2 included repeated references to the extensive exposure to health messaging (e.g., “Heard it all before”); these responses reveal message fatigue and confirm that it may have conditioned closed-question responses.
Previous studies on governmental communication during the COVID-19 pandemic highlight the importance of the relationship between the audience and the advice-givers in promoting adherence to the guidelines – e.g., Yang’s (2021) study on advice letters issued by the Chinese government and health authorities; Jaworska’s (2021) examination of Angela Merkel’s effective communicative strategies; and Love et al. (2023) study of engagement strategies in tweets published by local government organisations in England. Scientific and medical sources, such as the NHS in the posters considered, are attributed higher levels of public trust than political authorities (Coleman et al. 2020). These studies would suggest that message source positively affected compliance. In addition to information source, the communication context referenced in some messages (e.g., the hospital, message 1, Table 2) is likely to have played a role in motivating the high levels of self-predicted compliance. Communication context is a key factor determining compliance, as revealed by open text responses to self-efficacy messaging not examined in this paper (e.g., “If this was in hospitals, I think people would still be sensitive to it, but anywhere else it will be ignored”) (McClaughlin et al. 2023).
Although it is impossible to disaggregate the impact of linguistic choices from the communication and socio-political related factors discussed, the differences in self-reported compliance observed in the closed-questions allow us to report some tendencies among the British public: (i) fear appeals are preferred when they display certainty over the outcomes (high values of Modalisation:Probability); (ii) self-efficacy messages are better accepted if imposition is mitigated with medium values of obligation; (iii) the audience favours directives in declarative mood vis-à-vis imperative (though declaratives with Modulation:Obligation were not compared with imperatives in this survey); and (iv) moralising messages do not seem to show any difference between medium or high values of obligation.
The analysis of the responses to the messaging in Figures 1 and 2 has revealed that, given an equal communication context (e.g., the same health campaign for the same health crisis) and the same linguistic formulation within the message (imperative mood), message type and visual cues prevail in conditioning the public reception of health messaging. This was particularly obvious for Figure 2 (moralising), where most of the participants did not engage with the directive, but provided personal assessments of the poster instead. Objective and, to a lesser extent, subjective modulation expressions can be associated with a varied positioning of the speaker towards the directive, which may or may not include the speaker among the addressees. These forms of modulation contrast with the imperative mood, which was always directed to a second person addressee, implicitly distancing the speaker from the directive. These findings suggest that avoiding the imperative mood and employing declaratives with medium modulation values, either with subjective or objective orientations, and referring to a first-person plural subject may be a more productive way of conveying obligation in health campaigns.
Funding source: Arts and Humanities Research Council
Award Identifier / Grant number: AH/V015125/1
Funding source: Engineering and Physical Sciences Research Council
Award Identifier / Grant number: EP/T022493/1
About the authors
Sara Vilar-Lluch is a Lecturer in Language and Linguistics at Cardiff University, UK. Her main research interests are in the areas of discourse analysis, Systemic Functional Linguistics, the expression of evaluation and emotion, and metaphor analysis, with a particular focus on health communication. Prior to Cardiff, she held research and teaching positions at the University of Nottingham.
Emma McClaughlin is a Research Fellow in Corpus Linguistics at the University of Nottingham. With research interests in corpus linguistics and discourse analysis, her research at the University of Nottingham has focused on health communication. She has worked on projects examining the discourses surrounding Coronavirus, menstrual health, avian influenza, and misinformation. Prior to Nottingham, she held a research position at Queen Margaret University in Edinburgh working on the topic of trust in public communication of COVID-19 in Scotland.
Svenja Adolphs is Professor of English Language and Linguistics at the University of Nottingham, UK. Her research interests are in the areas of corpus linguistics (in particular, multimodal spoken corpus linguistics), pragmatics and discourse analysis. She has published widely in these areas, including Introducing Electronic Text Analysis (2006, Routledge), Corpus and Context: Investigating Pragmatics Functions in Spoken Discourse (2008, John Benjamins), Introducing Pragmatics in Use (1st ed. 2011, 2nd ed. 2020, Routledge, with Anne O’Keeffe and Brian Clancy), Spoken Corpus Linguistics: From Monomodal to Multimodal (2013, Routledge, with Ronald Carter) and the Routledge Handbook of English Language and Digital Humanities (2020, Routledge, edited with Dawn Knight).
Dawn Knight is Professor of Applied Linguistics at Cardiff University. Her research interests and expertise lie in the areas of corpus linguistics, discourse analysis, digital and online communication and non-verbal communication. She has led and/or contributed to a wide range of UK Research and Innovation (UKRI) and Welsh Government-funded multi-disciplinary and cross-institutional projects and has a sustained output of research publications, including two co-authored Palgrave books in 2020. Recent projects include the National Corpus of Contemporary Welsh (CorCenCC), FreeTxt and Interactional Variation Online (IVO).
Elena Nichele is a Lecturer in International Business Management at the University of Lincoln. Previously, she was a Research Fellow at the School of Computer Science, University of Nottingham (UK), where she was a member of the Horizon Digital Economy Research Institute and the Trustworthy Autonomous Systems Hub. Her expertise combines linguistics and marketing. She has been investigating perceptions, frequently expressed with the aid of technology and artificial intelligence, whilst focusing on the impact of identity and culture, with particular regard to the concept of authenticity. Her main research area is the complementary and interdependent relationship between global and local factors.
Acknowledgments
We are grateful to the other members of the project team Pepita Barnard, Derek McAuley and Alexandra Lang at the University of Nottingham and to Ipsos UK, in particular Flora Meisl. We are also thankful to the three anonymous reviewers and the editor of the journal for their helpful comments and suggestions.
-
Research funding: The project Coronavirus Discourses: linguistic evidence for effective public health messaging was funded by the Arts and Humanities Research Council (AHRC): AH/V015125/1 and the Engineering and Physical Sciences Research Council ‘Trusted Data Driven Products’: EP/T022493/1.
-
Data availability: Data are available on reasonable request.

Mean difference (MD) per message type and age group with significant mean differences marked (MD ≥ 1).
References
Barik, Ardila L., Rizki A. Purwaningtyas & Dwi Astuti. 2019. The effectiveness of traditional media (leaflet and poster) to promote health in a community setting in the digital era: A systematic review. Jurnal NERS 14(3). 76–80. https://doi.org/10.20473/jn.v14i3.16988.Search in Google Scholar
Bartlett, Tom. 2014. Analysing power in language: A practical guide. Oxon/New York: Routledge.10.4324/9781315851938Search in Google Scholar
Berry, Dianne. 2006. Health communication: Theory and practice. UK: McGraw-Hill Education.Search in Google Scholar
Coleman, Stephen, Nely Konstantinova & Giles Moss. 2020. The pandemic and its publics: How people receive, interpret and act upon official guidance. https://eprints.whiterose.ac.uk/170636/1/The_pandemic_and_its_publics_011220.pdf (accessed 25 April 2022).Search in Google Scholar
Craven, Alexandra & Jonathan Potter. 2010. Directives: Entitlement and contingency in action. Discourse Studies 12(4). 419–442. https://doi.org/10.1177/1461445610370126.Search in Google Scholar
Curl, Traci S. & Paul Drew. 2008. Contingency and action: A comparison of two forms of requesting. Research on Language and Social Interaction 41(2). 129–153. https://doi.org/10.1080/08351810802028613.Search in Google Scholar
DiMatteo, M. Robin, Kelly B. Haskard-Zolnierek & Leslie R. Martin. 2012. Improving patient adherence: A three-factor model to guide practice. Health Psychology Review 6(1). 74–91. https://doi.org/10.1080/17437199.2010.537592.Search in Google Scholar
Ervin-Tripp, Susan. 1976. Is Sybil there? The structure of some American English directives. Language in Society 5(1). 25–66. https://doi.org/10.1017/s0047404500006849.Search in Google Scholar
Fajri, Nurul, Said Usman, Sofia Sofia, Irwan Saputra & Marthoenis Marthoenis. 2022. Media effectiveness health promotion video and poster on Covid-19 vaccination on improving knowledge and attitude of Cadres in Banda Aceh City. Budapest International Research and Critics Institute (BIRCI-Journal): Humanities and Social Sciences 5(2).Search in Google Scholar
Hale, Jerold L. & James P. Dillard. 1995. Fear appeals in health promotion campaigns: Too much, too little, or just right? In Edward Maibach & Roxanne L. Parrott (eds.), Designing health messages: Approaches from communication theory and public health practice, 65–80. London/New Delhi: SAGE.10.4135/9781452233451.n4Search in Google Scholar
Halliday, Michael A. K. & Christian M. I. M. Matthiessen. 2004. Introduction to functional grammar. London: Routledge.Search in Google Scholar
Hasanica, Nino, Aida Ramic-Catak, Adnan Mujezinovic, Saed Begagic, Kenan Galijasevic & Mirza Oruc. 2020. The effectiveness of leaflets and posters as a health education method. Materia Socio Medica 32(2). 135. https://doi.org/10.5455/msm.2020.32.135-139.Search in Google Scholar
Heritage, John & Sue Sefi. 1992. Dilemmas of advice: Aspects of the delivery and reception of advice in interactions between health visitors and first-time mothers. In Paul Drew & John Heritage (eds.), Talk at work. Interaction in institutional settings, 359–417. Cambridge: Cambridge University Press.Search in Google Scholar
Institute of Medicine. 2015. Communicating to advance the public’s health: Workshop summary. Washington, DC: The National Academies Press.Search in Google Scholar
Jaworska, Sylvia. 2021. Competence and collectivity: The discourse of Angela Merkel’s media communications during the first wave of the pandemic. Discourse, Context & Media 42. 100506. https://doi.org/10.1016/j.dcm.2021.100506.Search in Google Scholar
Jones, Christian, David Oakey & Kay O’Halloran. 2023. “I will say the picture of the background is not related to the words”: Using corpus linguistics and focus groups to reveal how speakers of English as an additional language perceive the effectiveness of the phraseology and imagery in UK public health tweets during COVID-19. Applied Corpus Linguistics 3(2). 100053. https://doi.org/10.1016/j.acorp.2023.100053.Search in Google Scholar
Kress, Gunther & Theo van Leeuwen. 2021. Reading images. The grammar of visual design. London: Routledge.10.4324/9781003099857Search in Google Scholar
Liu, Zhuling & Janet Yang. 2023. Public support for COVID-19 responses: Cultural cognition, risk perception, and emotions. Health Communication 38(4). 648–658. https://doi.org/10.1080/10410236.2021.1965710.Search in Google Scholar
Locher, Miriam. 2010. Health internet sites: A linguistic perspective on health advice columns. Social Semiotics 20(1). 43–59. https://doi.org/10.1080/10350330903438402.Search in Google Scholar
Love, Robbie, Erika Darics & Rudi Palmieri. 2023. Engaging the public: English local government organisations’ social media communications during the COVID-19 pandemic. Applied Corpus Linguistics 3(3). 100060. https://doi.org/10.1016/j.acorp.2023.100060.Search in Google Scholar
McClaughlin, Emma, Sara Vilar-Lluch, Tamsin Parnell, Dawn Knight, Elena Nichele, Svenja Adolphs, Jérémie Clos & Giovanni Schiazza. 2023. The reception of public health messages during the COVID-19 pandemic. Applied Corpus Linguistics 3(1). 100037. https://doi.org/10.1016/j.acorp.2022.100037.Search in Google Scholar
Naikoba, Sarah & Andrew Hayward. 2001. The effectiveness of interventions aimed at increasing handwashing in healthcare workers-a systematic review. Journal of Hospital Infection 47(3). 173–180. https://doi.org/10.1053/jhin.2000.0882.Search in Google Scholar
Pittet, Didier, Stéphane Hugonnet, Stephan Harbarth, Philippe Mourouga, Valérie Sauvan, Sylvie Touveneau & Thomas V. Perneger. 2000. Effectiveness of a hospital-wide programme to improve compliance with hand hygiene. The Lancet 356(9238). 1307–1312. https://doi.org/10.1016/s0140-6736(00)02814-2.Search in Google Scholar
Qureshi, Aamir M., Niall Hughes, Elizabeth Murphy & William R. Primrose. 2004. Factors influencing uptake of influenza vaccination among hospital-based health care workers. Occupational Medicine 54(3). 197–201. https://doi.org/10.1093/occmed/kqg087.Search in Google Scholar
Salmon, Charles & Charles Atkin. 2003. Using media campaigns for health promotion. In Teresa L. Thompson, Alicia M. Dorsey, Katherine Miller & Roxanne Parrot (eds.), Handbook of health communication, 449–472. Mahwah: Lawrence Erlbaum Associates.Search in Google Scholar
Sarangi, Srikant & Angus Clarke. 2002. Constructing an account by contrast in counselling for childhood genetic testing. Social Science & Medicine 54(2). 295–308. https://doi.org/10.1016/s0277-9536(01)00029-6.Search in Google Scholar
Searle, John R. 1979. Expression and meaning. Studies in the theory of speech acts. Cambridge: Cambridge University Press.10.1017/CBO9780511609213Search in Google Scholar
Seeger, Matthew W. 2006. Best practices in crisis communication: An expert panel process. Journal of Applied Communication Research 34(3). 232–244. https://doi.org/10.1080/00909880600769944.Search in Google Scholar
Sharot, Trevor. 1986. Weighting survey results. Journal of the Market Research Society 28(3). 269–284.Search in Google Scholar
Shaw, Chloe, Jonathan Potter & Alexa Hepburn. 2015. Advice-implicative actions: Using interrogatives and assessments to deliver advice in mundane conversation. Discourse Studies 17(3). 317–342. https://doi.org/10.1177/1461445615571199.Search in Google Scholar
Täuber, Susanne. 2018. Moralized health-related persuasion undermines social cohesion. Frontiers in Psychology 9. 909. https://doi.org/10.3389/fpsyg.2018.00909.Search in Google Scholar
Thomas, McKinley, Wanda Gillespie, Janis Krauss, Steve Harrison, Regina Medeiros, Michael Hawkins, Ross Maclean & Keith F. Woeltje. 2005. Focus group data as a tool in assessing effectiveness of a hand hygiene campaign. American Journal of Infection Control 33(6). 368–373. https://doi.org/10.1016/j.ajic.2005.03.011.Search in Google Scholar
Tversky, Amos & Daniel Kahneman. 1981. The framing of decisions and the psychology of choice. Science 211(4481). 453–458. https://doi.org/10.1126/science.7455683.Search in Google Scholar
Vereen, Rhyan N., Rachel Kurtzman & Seth M. Noar. 2023. Are social media interventions for health behavior change efficacious among populations with health disparities? A meta-analytic review. Health Communication 38(1). 133–140. https://doi.org/10.1080/10410236.2021.1937830.Search in Google Scholar
Vincent, Benet, Kate Power, Peter Crosthwaite & Sheena Gardner. 2023. Directives in Covid-19 government guidance: An international comparison. Applied Corpus Linguistics 3(3). 100063. https://doi.org/10.1016/j.acorp.2023.100063.Search in Google Scholar
Ward, Kim & Kamila Hawthorne. 1994. Do patients read health promotion posters in the waiting room? A study in one general practice. British Journal of General Practice 44(389). 583–585.Search in Google Scholar
Yang, Na. 2021. Engaging readers across participants: A cross-interactant analysis of metadiscourse in letters of advice during the COVID-19 pandemic. Journal of Pragmatics 186. 181–193. https://doi.org/10.1016/j.pragma.2021.10.017.Search in Google Scholar
© 2024 the author(s), published by De Gruyter, Berlin/Boston
This work is licensed under the Creative Commons Attribution 4.0 International License.
Articles in the same Issue
- Frontmatter
- Editorial
- Announcement
- Research Articles
- Narratives about epistemic trespassing
- Damned if feminists do, damned if feminists don’t? Political significance of institutional inclusive writing guidelines in a Belgian francophone university
- Evaluative language in Chinese online food discourse: overall distribution, local patterning, and readers’ involvement
- Metaphorical language in the discourse of Yasser Arafat
- The effects of modal value and imperative mood on self-predicted compliance to health guidance: the case of COVID-19
- Embodied movement as a stratified semiotic mode: how movement, gaze and speech mean together in the classroom
Articles in the same Issue
- Frontmatter
- Editorial
- Announcement
- Research Articles
- Narratives about epistemic trespassing
- Damned if feminists do, damned if feminists don’t? Political significance of institutional inclusive writing guidelines in a Belgian francophone university
- Evaluative language in Chinese online food discourse: overall distribution, local patterning, and readers’ involvement
- Metaphorical language in the discourse of Yasser Arafat
- The effects of modal value and imperative mood on self-predicted compliance to health guidance: the case of COVID-19
- Embodied movement as a stratified semiotic mode: how movement, gaze and speech mean together in the classroom