The significance of taking a spiritual history: A randomized controlled study in a sample of German psychotherapists
-
Prof. Dr. rer nat., Professorship for Psychotherapy Research, University-Medical Center Hamburg-Eppendorf, Department for Psychosomatic Medicine and Psychotherapy, Hamburg, Germany; Head of Outpatient Clinic and Training Psychological Psychotherapist.
 ,
,
M.Sc. Psychologie, University-Medical Center Hamburg-Eppendorf, Department for Psychosomatic Medicine and Psychotherapy, Hamburg, Germany.
Prof. Dr. habil., Professorship for Clinical Psychology and Psychotherapy, Medical School Hamburg, Hamburg, Germany.

Abstract
Background: In the past, psychotherapists have neglected religious and spiritual issues compared to other themes like sexuality or somatic experiences.
Objective: We aim to determine if psychotherapists view taking a spiritual history as less important than taking a sexual or somatic history when patients report a spiritual crisis vs. a sexual crisis vs. a somatic crisis as causes for their depressive states.
Method: Using a randomized controlled 3-group-between-subjects design, 117 psychotherapists were randomly assigned to one of three groups and presented with a fictional case vignette of a depressed patient, who reported either a spiritual vs. sexual, vs. somatic crisis as a cause for depression. As dependent variables, we assessed the importance that each group attached to taking a spiritual history, a sexual, or somatic history.
Results: Psychotherapists in the spiritual-crisis condition considered taking a spiritual history significantly less important than psychotherapists in the sexual-crisis condition placed on taking a sexual history (d = 0.47) and psychotherapists in the somatic-crisis condition placed on taking a somatic history (d = 0.57).
Discussion: Our findings show a bias against taking a spiritual history compared to a sexual and a somatic history. This bias could be addressed in the psychotherapy training as the process of taking a spiritual history constitutes a significant component of psychotherapy, one that is particularly sensitive to cultural and religious diversity.
Zusammenfassung
Hintergrund: Studien zur psychotherapeutischen Praxis beobachten, dass Psychotherapeut/-innen religiöse und spirituelle Fragen im Vergleich zu anderen Themen wie Sexualität oder somatische Erfahrungen vernachlässigen.
Zielsetzung: Wir wollen herausfinden, ob Psychotherapeut/-innen die Erhebung einer spirituellen Anamnese für weniger wichtig erachten als die Erhebung einer sexuellen oder somatischen Anamnese, wenn Patient/-innen eine spirituelle Krise vs. eine sexuelle Krise vs. eine somatische Krise als Ursache für ihre depressiven Zustände angeben.
Methode: Unter Verwendung eines randomisierten, kontrollierten 3-Gruppen-Between-Subjects-Designs wurden 117 Psychotherapeuten nach dem Zufallsprinzip einer von drei Gruppen zugeteilt und mit einer fiktiven Fallvignette einer an Depression erkrankten Patientin konfrontiert, die als Ursache für ihre Depression entweder eine spirituelle vs. sexuelle vs. somatische Krise angab. Als abhängige Variablen untersuchten wir die Bedeutung, die jede Gruppe der Erhebung einer spirituellen, einer sexuellen und einer somatischen Anamnese beimaß.
Ergebnisse: Psychotherapeut/-innen in der spirituellen Krisenbedingung hielten die spirituelle Anamnese für signifikant weniger wichtig als Psychotherapeut/-innen eine sexuelle Anamnese in der sexuellen Krisenbedingung (d = 0.47) und Psychotherapeut/-innen in der somatischen Krisenbedingung (d = 0.57), die auf eine somatische Anamnese Wert legten.
Diskussion: Unsere Ergebnisse zeigen eine Voreingenommenheit gegen die spirituelle Anamnese im Vergleich zur sexuellen und somatischen Anamnese. Diese Voreingenommenheit könnte in der Psychotherapieausbildung thematisiert werden, da der Prozess der spirituellen Anamnese eine wichtige Komponente einer kulturell sensiblen und religiöse Vielfältigkeit ermöglichenden Psychotherapie darstellt.
1 Introduction
While early works by William James (James 1890; James 1902; James 1910) explicitly bridge the gap between psychology and religiosity, a potentially critical attitude towards spirituality on the part of the psychotherapeutic community and its intellectual forebears cannot be denied. In early works, Sigmund Freud viewed religion as a ‘collective neurotic illusion’ that was primarily intended to fulfil a psychological function (Freud 1927): From the point of view of human needs, religion can be understood as a need for protection and order that offer comfort and structure, and thus represent a kind of wish fulfilment. According to Freud (1927), projections of desires and conflicts play a decisive role in religious ideas. Freud sees religiosity and spirituality more as an inhibiting antagonist to rational and mature thought processes.
Ironically, sociological descriptions of the development of psychotherapy conclude that psychotherapy and psychoanalysis “should be understood in the structural and functional succession of ecclesiastical-religious meaning” and that “therapeutic institutions modernize and substitute religious patterns of interpretation and practices” (Willems 1999).
But despite past disagreements between spirituality and religiosity on the one hand and reason-emphasizing, rational psychotherapy and psychoanalysis on the other, the way religiosity is dealt with still seems to divide psychotherapists today: In a representative study of Franconian psychotherapists published in 2016, it was shown that psychotherapists have significantly fewer religious ties than the general population (Marquardt & Demling 2016), which replicated observations from the United States (Shafranske & Cummings 2013; Delaney et al. 2007). More relevant than the difference between the confessional ties of the general population and those of psychotherapists, for which there are certainly alternative explanations other than the specific psychological-psychotherapeutic profession, the following circumstance is more relevant for this article. The strong discrepancy between psychotherapists’ claimed importance of the topic of spirituality and religiosity in the context of psychotherapy and the way psychotherapists report of assessing spirituality in psychotherapies. While 2/3 of the psychotherapists surveyed consider religion to be a psychotherapeutically relevant topic for their patients, only 20 % of the psychotherapists surveyed routinely explore this topic in the sense of a spiritual history (Marquardt & Demling 2016). Studies from other secularized countries, such as the U.S. or Norway, also observe similar discrepancies: U.S. doctoral clinical and counseling psychology students (i.e. prospective psychotherapists) mostly aimed at integrating a spiritual history in their work, whereas 75 % reported, that their training programs provided no courses in religion/spirituality (Sanders et al. 2014). This study was replicated in a nationwide study of Norwegian psychology students (i.e. also prospective psychotherapists), observing a high level of interest in addressing religion and spirituality in the sense of a psychotherapeutic professional sensitivity to diversity, which contrasted with the actual way it was addressed in teaching (Mandelkow & Endresen Reme 2022). The American Psychological Association (2017) has also emphasized the importance of addressing religion and spirituality in the context of psychotherapy. This is evident in the Multicultural Guidelines: An Ecological Approach to Context, Identity, and Intersectionality, which identifies both religion and spirituality as aspects of multiculturalism. Rosmarin et al. (2021: 92) describe in their commentary in The Lancet Psychiatry: “Yet, 84 % of the world’s population is religiously affiliated, and 68 % of unaffiliated individuals believe in a higher power. No other social phenomenon is so widespread, yet all but ignored by academic psychiatry”. The present quasi-experimental study is designed to examine whether this ‘ignorance’ described by Rosmarin et al. (2021) has a negative impact on the treatment of people with psychological disorders by neglecting appropriate psychotherapeutic diagnostics and thus treatment.
2 The present study
In the present study, we wanted to examine how important German psychotherapists and psychotherapists in training assess the relevance of assessing a spiritual history (e.g. Frick 2025), a sexual and a somatic history in a specific case example in which a spiritual vs. a sexual vs. a somatic crisis is reported by a patient as the cause of a depressive state. The participants received (randomly assigned) one of three case vignettes. In the first condition, they were presented with a case vignette in which a spiritual crisis was reported by the patient as the cause of her depressive state; in the second condition, a sexual crisis was reported; and in the third condition, a somatic illness was reported by the patient as the cause of her depressive state.
We expected that the participating psychotherapists examined would consider the taking of a spiritual history to be most important if the patient in the case vignette states that a spiritual crisis is the cause of her depressive state. Similarly, we expected that psychotherapists consider the collection of a sexual history or the collection of a somatic history to be most important if the patient in the case vignette reports a sexual or somatic crisis as the cause of her depressive state. This relative importance of taking an appropriate history can be seen from the case vignette. Simply put, if the patient talks about spiritual issues, we expected that participating psychotherapists also ask about the spiritual history, and accordingly regarding sexual and somatic issues.
In line with Rosmarin et al. (2021), however, we also expected that with regard to the cross domain concordant comparison (importance of the respective history-taking per condition) that psychotherapists should differ between conditions in terms of their relative assessment of the importance of case-vignette-compliant history, with a discrimination of spiritual history. Thus, there should be a difference between the conditions in the importance of taking a spiritual history (in the spiritual-crisis condition) and the importance of taking a sexual history (in the sexual-crisis condition) and the importance of a somatic history (in the somatic-crisis condition) in such that between these three variables, psychotherapists should consider a spiritual history to be less important.
3 Method
3.1 Design
We applied a randomized controlled 3-group-between-subjects design by randomly assigning participants either to the spiritual-crisis condition (n = 39), the sexual-crisis condition (n = 38), or to the somatic-crisis condition (n = 34). Our study was approved by the Local Psychological Ethics Committee at the University Medical Center Hamburg-Eppendorf (LPEK-0759).
Procedure of the Study.
3.2 Power analysis
Since, to our knowledge, no study has investigated this research question, the power-analysis was based on the assumption that conditions would exert a large effect (f = 0.4 and d = 0.8) on the dependent variables. The effect-size was then applied to an a-priori power-analysis indicating that 102 participants would be required to achieve 95 % power (α = .05).
3.3 Participants
To account for potential study dropouts, we recruited a convenience sample of 129 psychotherapists via snowball-sampling from our institute of psychotherapy. A total of 17 participants were excluded because they had a progress less than 77 % of the total study (i.e. the study was completed by at least 77 %). Thus, our final sample included 112 psychotherapists (M = 33.14 years old, SD = 7.59, 91 female, 20 male, 1 diverse).
4 Procedure
4.1 Informed consent and initial questions
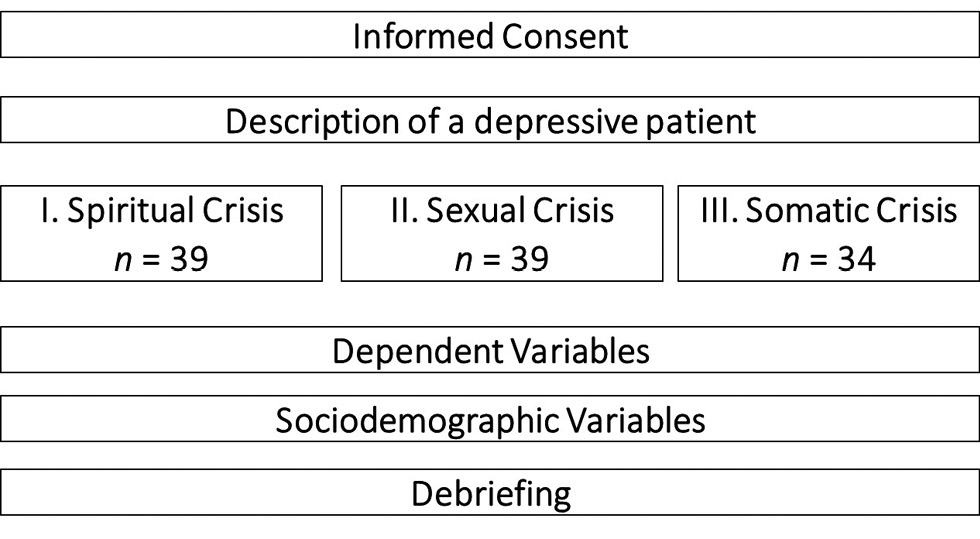
The study was conducted on the online platform Qualtrics. Prior to random assignment to one of three conditions, participants were asked to provide informed consent regarding data assessment and publication. Following each condition’s vignette description, participants were led to the dependent measures (see Fig. 1).
4.2 Description of a depressive patient
Participants in all conditions were given the same vignette read: “Carla, a 22-year-old law student in her 4th semester, has been suffering from a deep lack of motivation and interest for 3 weeks, which is affecting her everyday life and her studies. Because of Carla’s lack of motivation, her flatmate is currently taking on many household tasks and is taking care of most of the everyday requirements, as Carla also has to work at weekends to finance her studies. In the initial interview, Carla reports being quickly exhausted and having difficulty concentrating and paying attention. It was noticeable that she could no longer even enjoy her cat, with whom she had always had a lot of fun. The patient appears depressed in her contact behavior, she seems withdrawn and not very lively.”
4.3 Spiritual-crisis condition
In the spiritual-crisis condition, participants (n = 39) then were presented with the following information: “When asked to explain her current situation, the patient reports her deep disappointment with her religious institution, particularly because of the inconsistencies she has experienced in her community. This and the related frustration with her beliefs and doubts about the existence of God have caused a serious shock to her spirituality. Spirituality, which had been the mainstay of her life, unexpectedly became a source of great doubt.”
4.4 Sexual-crisis condition
In the sexual-crisis condition, participants (n = 39) were presented with the same description as in the spiritual-crisis condition, with the only difference that the words describing her depressive states’ reasons were framed as having a sexual crisis: “When asked to explain her current situation, the patient talks about her deep disappointment at the fact that sexuality is no longer possible in her partnership and the associated collapse of her sexual desire. This has led to a serious impairment of her sexual self-perception; intimacy, which used to be the mainstay of her life, has unexpectedly become a source of great doubt.”
4.5 Somatic-crisis condition
In the somatic-crisis condition, participants (n = 34) were presented with the same description as in the spiritual crisis condition, that the words describing her depressive states’ reasons were framed as having a somatic crisis: “When asked to explain her current situation, the patient reports her deep disappointment at the increasing intensity and frequency of her migraine attacks and the associated frustration at the loss of her physical health, which has been a major shock to her well-being. Well-being, which had been a mainstay of her life, had unexpectedly become a huge burden.”
4.6 Dependent measures
(The questionnaire contained additional measures relevant to other research questions of the larger project. However, all data analyses reported in the article are novel and the findings have not been published elsewhere.)
As dependent variables, we assessed in all conditions the importance of assessing this patient’s spiritual, sexual, and somatic histories on a Likert-Scale ranging from -50 (disagree) to +50 (fully agree) by asking three parallel items (“How do you assess the necessity of a comprehensive [spiritual or religious history] [sexual history] [somatic history] in relation to the mental illness of the patient described in the vignette?”, “To what extent do you expect that [spiritual or religious] [sexual] [somatic] issues should be considered in the treatment of this patient?”, “How likely do you think it is that the patient’s suffering from the vignette will increase if a differentiated [spiritual or religious history] [sexual history] [somatic history] is not carried out?”) with an at least acceptable reliability (αs between .73 [somatic] and .94 [spiritual], Hossiep 2022).
4.7 Analytic strategy
In line with the statements from Rosmarin et al. (2021), we wanted to test if psychotherapists have a bias towards not prioritizing the assessment of a spiritual history as important as taking a sexual or somatic history. We hypothesized that psychotherapists in group 1 (the spiritual-crisis-group) would consider taking a spiritual history to be less important than psychotherapists in group 2 (the sexual-crisis-group) consider a sexual history to be important and, in addition, psychotherapists in group 3 (the somatic-crisis-group) consider a somatic history to be important. We conducted an analysis of variance (ANOVA) with condition (spiritual-Crisis condition vs. sexual-crisis condition vs. somatic-crisis condition) as fixed between-subject factor. When the ANOVA showed a significant overall-effect, we calculated the least-significant difference (LSD) as post-hoc analysis.
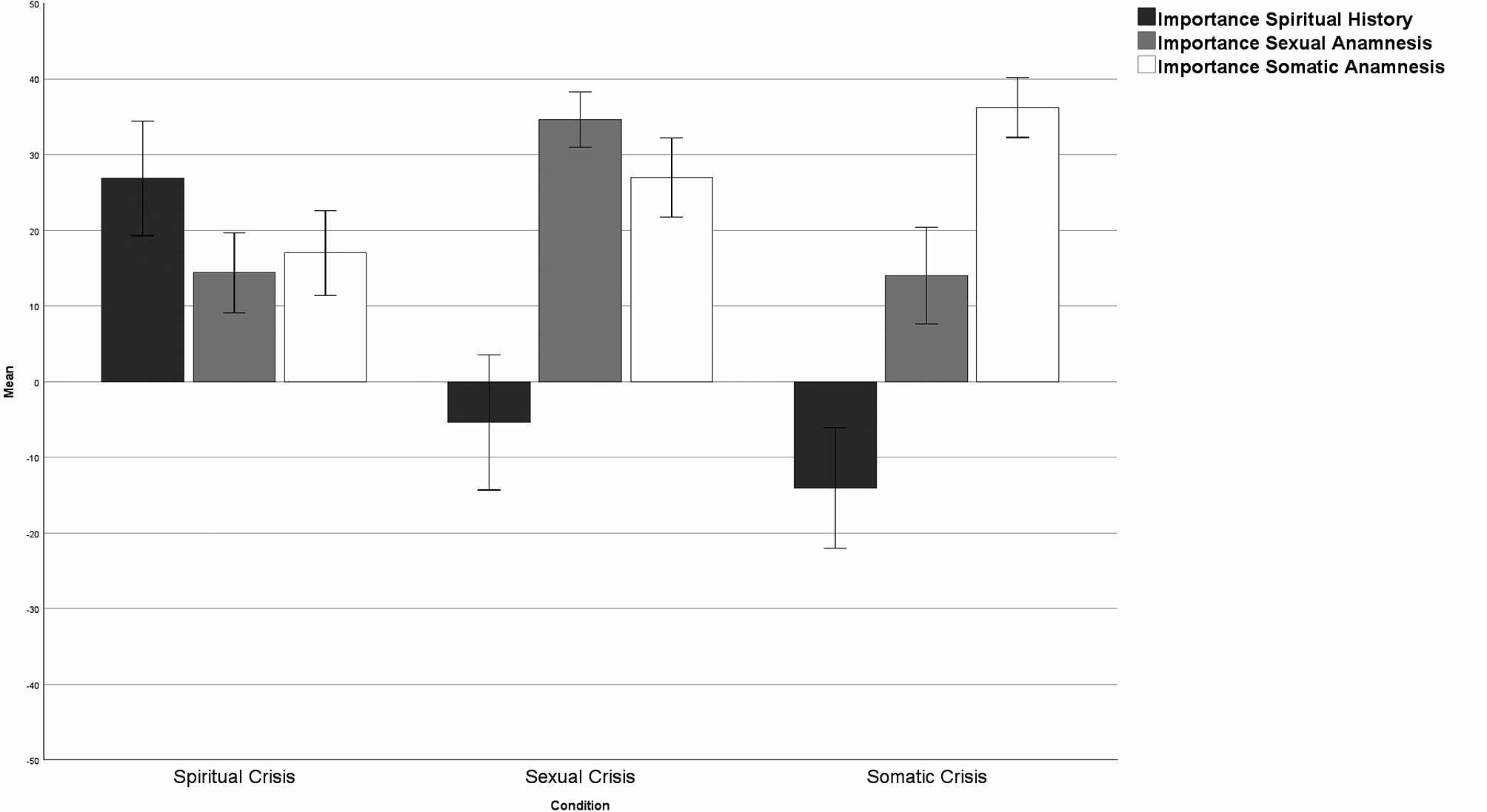
Comparison of psychotherapists’ claimed importance of assessing a spiritual history, sexual history, and somatic history between the conditions (spiritual-crisis condition vs. sexual-crisis condition vs. somatic-crisis condition): Means and 95 % confidence intervals as error bars
5 Results
5.1 Importance of assessing the patient’s spiritual history
With regard to the claimed need to assess the patient’s spiritual history, we observed a difference between the three conditions, F(2, 109) = 28.51, p ≤ .001, η2 = .34 (see figure 2). Participants in the spiritual-crisis condition, M = 26.84, SD = 23.29, were significantly more likely to regard the assessment of the patient’s spiritual history as important than participants in the sexual-crisis condition, M = -5.40, SD = 27.47, t(76) = 5.76, p ≤ .001, 95 % CI [21.15; 43.32], d = 1.31, and those in the somatic-crisis condition, M = -14.06, SD = 22.86, t(71) = 7.06, p ≤ .001, 95 % CI [29.41; 52.39], d = 1.66. With regard to the claimed need to assess the patient’s spiritual history, we observed no difference between participants in the sexual-crisis condition and those in the somatic-crisis Condition, p = .138.
5.2 Importance of assessing the patient’s sexual history
With regard to the claimed need to assess the patient’s sexual history, we observed a difference between the three conditions, F(2, 109) = 22.13, p ≤ .001, η2 = .29 (see figure 2). Participants in the sexual-crisis condition, M = 26.84, SD = 23.29, were significantly more likely to regard the assessment of the patient’s sexual history as important than participants in the spiritual-crisis condition, M = 14.38, SD = 16.37, t(36) = 5.78, p ≤ .001, 95 % CI [13.30; 27.18], d = 1.31 and those in the somatic-crisis condition, M = 14.00, SD = 18.29, t(34) = 5.70, p ≤ .001, 95 % CI [13.42; 27.81], d = 1.33. With regard to the claimed need to assess the patient’s sexual history, we observed no difference between participants in the spiritual-crisis condition and those in the somatic-crisis condition, p = .918.
5.3 Importance of assessing the patient’s somatic history
With regard to the claimed need to assess the patient’s somatic history, we observed a difference between the three conditions, F(2, 109) = 14.37, p ≤ .001, η2 = .21 (see figure 2). Participants in the somatic-crisis condition, M = 36.23, SD = 11.33, were significantly more likely to regard the assessment of the patient’s somatic history as important than participants in the spiritual-crisis condition, M = 16.98, SD = 17.31, t(36) = 5.35, p ≤ .001, 95 % CI [12.12; 26.37], d = 1.26 and those in the sexual-crisis condition, M = 26.97, SD = 16.21, t(34) = 2.58, p = .011, 95 % CI [2.13; 16.39], d = 0.60. With regard to the claimed need to assess the patient’s somatic history, participants in the spiritual-crisis condition considered the assessment of the patient’s somatic history to be significantly less important than participants in the sexual-crisis condition, t(36) = 2.88, p = .005, 95 % CI [3.10; 16.86], d = 0.65.
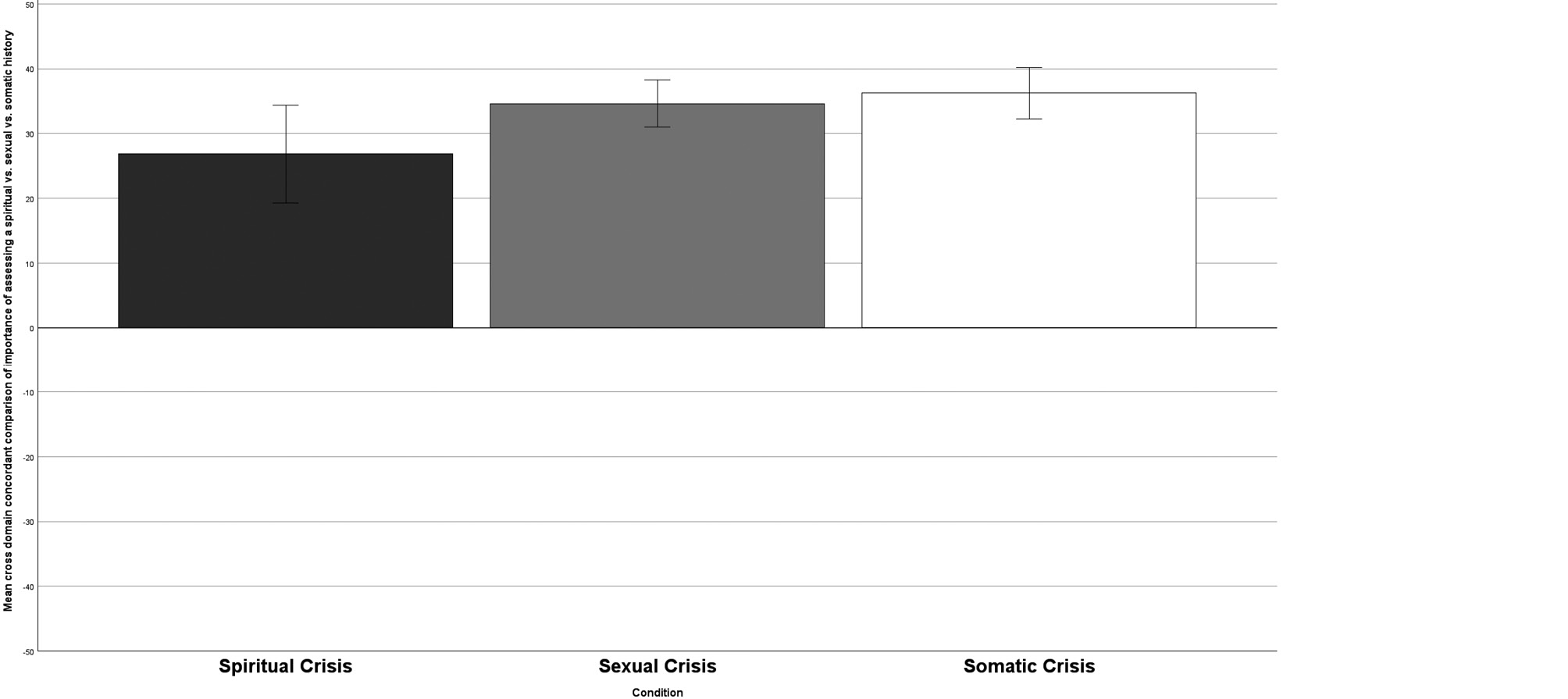
Cross domain concordant comparison of psychotherapists’ claimed importance of assessing a spiritual history in the spiritual-crisis condition vs. psychotherapists’ claimed importance of assessing a sexual history in the sexual-crisis condition vs. psychotherapists’ claimed importance of assessing a somatic history in the somatic-crisis condition: Means and 95 % confidence intervals as error bars
5.4 Importance of history assessment in accordance with condition
With regard to the claimed importance to assess the patient’s history in accordance with the condition (i.e. importance of assessing patient’s spiritual history in the spiritual-crisis condition, importance of assessing patient’s sexual history in the sexual-crisis condition, and importance of assessing patient’s somatic history in the somatic-crisis condition) we observed a difference between the three conditions, F(2, 109) = 3.48, p = .034, η2 = .06 (see figure 3). Participants in the spiritual-crisis condition, M = 26.84, SD = 23.29, considered the assessment of the patient’s spiritual history to be significantly less important than participants in the sexual-crisis condition with regard to the sexual history, M = -34.62, SD = 11.32, t(76) = 2.08, p = .040, 95 % CI [0.37; 15.19], d = 0.47. Similarly, participants in the spiritual-crisis condition considered the assessment of the patient’s spiritual history to be significantly less important than participants in the somatic-crisis condition with regard to the somatic history, M = 36.23, SD = 11.33, t(71) = 2.42, p = .017, 95 % CI [1.71; 17.07], d = 0.57. We observed no difference between participants in the sexual-crisis condition and those in the somatic-crisis condition, p = .679.
6 Discussion
Our study addresses a phenomenon that has been observed by religious psychologists: While psychotherapists acknowledge the importance of spirituality, there appears to be a bias against evaluating spiritual histories, but to our knowledge this has not yet been experimentally investigated.
Research among general practitioners has indicated that taking a spiritual history can serve as a “possible door opener for a trusting doctor-patient relationship” (Mächler et al. 2022). In our pilot study, we observed that psychotherapists acknowledged within the spiritual-crisis condition the necessity of assessing a spiritual history (vs. a sexual vs. a somatic history) when patients reported a spiritual crisis as the cause of a depressive state. Interestingly, groups 2 and 3 (the sexual and somatic groups) rated a spiritual history as not important at all (in contrast to the sexual somatic history, which is considered important in all conditions, i.e. in the mean positive scale range). However, compared to the other conditions, the psychotherapists in the spiritual-crisis condition placed significantly less importance on the assessment of a spiritual history than psychotherapists in the sexual-crisis condition or the somatic-crisis condition with regard to the assessment of sexual or somatic anamneses when those were cited in the respective conditions as causes of depressive states. Thus, our hypotheses could be confirmed. There may be a variety of possible reasons for this. One plausible reason, in our view, could be seen in the long and difficult tradition between psychotherapy and spirituality, or, to repeat it in the words of Rosmarin et al. (2021: 92): “No other social phenomenon is so widespread, yet all but ignored by academic psychiatry.”
Our study does not address the origins of psychotherapists’ bias, nor does it address whether the findings reflect a localized phenomenon specific to Northern German therapists, who tend to be relatively young (with a mean age of 33 years). Nonetheless, these findings encourage a need for enhanced training in psychotherapy to improve the assessment of spiritual histories. If the field of psychotherapy is to be integrative and sensitive to cultural and personal resources and challenges, spiritual crises, which are cited by patients as a contributory cause of their depressive disorders, must be taken at least as seriously as sexual or somatic crises.
Über die Autoren
Prof. Dr. rer nat., Professorship for Psychotherapy Research, University-Medical Center Hamburg-Eppendorf, Department for Psychosomatic Medicine and Psychotherapy, Hamburg, Germany; Head of Outpatient Clinic and Training Psychological Psychotherapist.
M.Sc. Psychologie, University-Medical Center Hamburg-Eppendorf, Department for Psychosomatic Medicine and Psychotherapy, Hamburg, Germany.
Prof. Dr. habil., Professorship for Clinical Psychology and Psychotherapy, Medical School Hamburg, Hamburg, Germany.
Author contributions: All the authors have accepted responsibility for the entire content of this manuscript and approved its submission.
Research funding: None declared.
Competing interests: Authors state no conflict of interest.
Informed consent: Informed consent was obtained from all individuals included in this study.
Ethical approval: The research related to human use complied with all the relevant national regulations, institutional policies, is in accordance the tenets of the Helsinki Declaration, and has been approved by the authors’ institutional review board or equivalent committee (LPEK-0759).
References
American Psychological Association (2017) Multicultural guidelines: an ecological approach to context, identity, and intersectionality (Zitierdatum: 11.01.2025), available at http://www.apa.org/about/policy/multicultural-guidelines.pdf.Search in Google Scholar
Delaney HD, Miller WR, Bisonó AM (2007) Religiosity and spirituality among psychologists: a survey of clinician members of the American psychological association. Professional Psychology, Research and Practice 38:538–546.10.1037/0735-7028.38.5.538Search in Google Scholar
Freud S (1964) The future of an illusion. New York: Doubleday.Search in Google Scholar
Frick E (2025) Spirituelle Anamnese. In: Frick E, Roser T, Stotz-Ingenlath G (eds.) Spiritualität und Medizin. Gemeinsame Sorge für den kranken Menschen (3. Auflage). Stuttgart: Kohlhammer. [ahead of print].Search in Google Scholar
James W (1890) The principles of psychology. New York: Holt.10.1037/10538-000Search in Google Scholar
James W (1902) The varieties of religious experience: A study in human nature. New York: Longmans, Green, and Co.10.1037/10004-000Search in Google Scholar
James W (1910) A pluralistic universe. New York: Longmans, Green, and Co.10.2307/1412963Search in Google Scholar
Hossiep R (2022) Cronbachs Alpha. In: Wirtz MA (Hg.) Dorsch Lexikon der Psychologie. Bern: Hogrefe (Zitierdatum: 11.01.2025), abrufbar unter: https://dorsch.hogrefe.com/stichwort/cronbachs-alpha.Search in Google Scholar
Mächler R, Sturm N, Frick E, Schalhorn F, Stolz R, Valentini J, Krisam J, Straßner C (2022) Evaluation of a spiritual history with elderly multi-morbid patients in general practice – a mixed-methods study within the project HoPES3. International journal of environmental research and public health 19:538.10.3390/ijerph19010538Search in Google Scholar PubMed PubMed Central
Mandelkow L, Endresen Reme S (2022) Religious sensitivity at secular universities -A cross-sectional replication study among Norwegian psychology students. Nordic Journal of Religion and Society(1):4–19.10.18261/njrs.35.1.1Search in Google Scholar
Marquardt M, Demling JH (2016) Psychotherapie und Religion: Eine repräsentative Umfrage unter Psychotherapeuten in Süddeutschland. PPmP-Psychotherapie· Psychosomatik· Medizinische Psychologie 66:473–480.10.1055/s-0042-117457Search in Google Scholar PubMed
Rosmarin DH, Pargament KI, Koenig HG (2021) Spirituality and mental health: challenges and opportunities. The lancet. Psychiatry 8:92–93.10.1016/S2215-0366(20)30048-1Search in Google Scholar PubMed
Shafranske EP, Cummings JP (2013) Religious and spiritual beliefs, affiliations, and practices of psychologists. In: Pargament KI, Mahoney A, Shafranske EP (eds.) APA handbooks in psychology. APA handbook of psychology, religion, and spirituality (Vol. 2): An applied psychology of religion and spirituality. 23–41.10.1037/14046-002Search in Google Scholar
Willems H (1999) Modernisierung institutioneller Selbstthematisierung: Von der Beichte über die Psychoanalyse zur Gruppentherapie. In: von Graevenitz G (Hg.) Konzepte der Moderne. Germanistische Symposien Berichtsbände. Stuttgart: J. B. Metzler. 120–146.10.1007/978-3-476-05565-1_7Search in Google Scholar
© 2025 Walter de Gruyter GmbH, Berlin/Boston
Articles in the same Issue
- Titelseiten
- Editorial
- Spiritual Care in Caring Communities
- Spiritueller Impuls
- Einsamer Tod
- Originalia
- Seelsorglich wirksam.
- Freiwilliges Engagement in sozialen Organisationen im Hinblick auf die Motive des Engagements, Erleben emotionaler Distanzierung (Cool Down) und Lebenszufriedenheit bei Menschen mit unterschiedlichen Indikatoren der Spiritualität
- Research article
- The significance of taking a spiritual history: A randomized controlled study in a sample of German psychotherapists
- Leserbrief
- Leserbrief zu: Reininger et al. (2025)
- Research article
- Adaptation of Spiritual Intelligence Scale for Turkish: a validity and reliability study
- Interview
- Gut umsorgt: Spiritualität in sorgenden Gemeinschaften. Eine Perspektive der Praxis.
- Essay
- Sorgende Gemeinschaften – leibhaftige Spiritualität
- Hilfe – um Himmelswillen!
- Erfahrungsbericht
- Spiritual Care – etwas Selbstverständliches in meinem Leben?
- Interview
- „Da bedeutet die Caring Community, man guckt aufeinander“
- Zusammen ist man weniger allein – Einblicke in eine Caring Community. Perspektiven und Herausforderungen
- Tagungsbericht
- „Digitale Sorge für die Seele – Anthropologie, Digitalisierung und Seelsorge“
- „Religion, seelische Gesundheit und Integration nach Migration und Flucht“
- Rezension
- Karl-Josef Kuschel (2024) Weihnachten und der Koran. Ostfildern: Patmos. ISBN 978-3-8436-1437-5; 224 Seiten; Preis: 24,– € (D); 25,50 € (A); 28,80 CHF; 18,99 € (E-Book)
- Robert Sempach, Christoph Steinebach und Peter Zängl (Hg.) (2023) Care schafft Community – Community braucht Care. Wiesbaden: Springer VS. ISBN: 978-3-658-32553-4; 297 Seiten, Preis: D 74,99 €; A 87,50 €; CH 89,90 CHF; E-Book 59,99 €
- Stichwort
- Sorge
- Mitteilungen
- Mitteilungen
Articles in the same Issue
- Titelseiten
- Editorial
- Spiritual Care in Caring Communities
- Spiritueller Impuls
- Einsamer Tod
- Originalia
- Seelsorglich wirksam.
- Freiwilliges Engagement in sozialen Organisationen im Hinblick auf die Motive des Engagements, Erleben emotionaler Distanzierung (Cool Down) und Lebenszufriedenheit bei Menschen mit unterschiedlichen Indikatoren der Spiritualität
- Research article
- The significance of taking a spiritual history: A randomized controlled study in a sample of German psychotherapists
- Leserbrief
- Leserbrief zu: Reininger et al. (2025)
- Research article
- Adaptation of Spiritual Intelligence Scale for Turkish: a validity and reliability study
- Interview
- Gut umsorgt: Spiritualität in sorgenden Gemeinschaften. Eine Perspektive der Praxis.
- Essay
- Sorgende Gemeinschaften – leibhaftige Spiritualität
- Hilfe – um Himmelswillen!
- Erfahrungsbericht
- Spiritual Care – etwas Selbstverständliches in meinem Leben?
- Interview
- „Da bedeutet die Caring Community, man guckt aufeinander“
- Zusammen ist man weniger allein – Einblicke in eine Caring Community. Perspektiven und Herausforderungen
- Tagungsbericht
- „Digitale Sorge für die Seele – Anthropologie, Digitalisierung und Seelsorge“
- „Religion, seelische Gesundheit und Integration nach Migration und Flucht“
- Rezension
- Karl-Josef Kuschel (2024) Weihnachten und der Koran. Ostfildern: Patmos. ISBN 978-3-8436-1437-5; 224 Seiten; Preis: 24,– € (D); 25,50 € (A); 28,80 CHF; 18,99 € (E-Book)
- Robert Sempach, Christoph Steinebach und Peter Zängl (Hg.) (2023) Care schafft Community – Community braucht Care. Wiesbaden: Springer VS. ISBN: 978-3-658-32553-4; 297 Seiten, Preis: D 74,99 €; A 87,50 €; CH 89,90 CHF; E-Book 59,99 €
- Stichwort
- Sorge
- Mitteilungen
- Mitteilungen