Avoid Drug Incompatibilities: Clinical Context in Neonatal Intensive Care Unit (NICU)
-
Florence Flamein is a NICU pediatrician at the University Hospital of Lille, France. She obtained her PhD in 2011 at Paris 6 University. Her special interests and research projects include management and follow-up of children with perinatal asphyxia. She also works on the improvement of the quality and safety of neonatal care, particularly on drug prescription and intravenous administration.
 ,
,
Laurent STORME, MD, PhD, is professor of Pediatrics at the University Lille 2 France, and Director of the federative project “1000 days 4 Health”. He is Coordinator of the National Center for Rare Disease “Congenital Diaphragmatic Hernia”. He heads the Neonatal Intensive Care Unit at the University Hospital of Lille.
Aurélie Maiguy-Foinard is a clinical pharmacist at the Wallonie Picarde Hospital in Belgium since November 2016. She was a hospital pharmacist at the Pharmacy Institute of the University Hospital of Lille for two years. She obtained her PharmD in 2013 and her PhD in 2014 at Lille II University. Her special interests and research projects included prevention of adverse drug effects associated with intravenous infusion in anaesthesia and intensive care unit, especially in neonatology. She worked specifically on the assessment of the impact of innovative infusion devices.
Maxime Perez is a hospital and university pharmacist at the Pharmacy Institute of the University Hospital of Lille since November 2015 with special interest in clinical pharmacy. He obtained his PharmD and his PhD in 2015 at Lille II University. His research projects include optimization of medical devices used for the injectable administration of incompatible drugs and the evaluation of particles generated during drugs infusion, especially in pediatric and neonatal cares. He teaches clinical pharmacy at the school of pharmacy of Lille.
Bertrand Décaudin obtained his PharmD in 2003 and his PhD in 2006 at Lille University. He began his career as hospital pharmacist in Dunkerque General Hospital in November 2003 and moved to the Lille University Hospital in January 2009 with special interest in evaluation of medical devices and clinical pharmacy. Since September 2007, he teaches clinical pharmacy at the school of pharmacy of Lille. He manages research projects on drug infusion in anaesthesia and critical care medicine.
Morgane Masse is a hospital and university resident at the Pharmacy Institute of the University Hospital of Lille since November 2012. She obtained her PharmD in 2016 at Lille 2 University. Her research projects focus on interactions between content and container, especially with medical devices containing polyvinylchloride.
Stéphanie Genay is a hospital and university pharmacist at the Pharmacy Institute of the University Hospital of Lille since September 2013 with special interest in clinical pharmacy. She obtained her PharmD in 2013 and her PhD in 2014 at Lille University. Her research projects include optimization of medical devices used for the injectable administration of incompatible drugs, caractérization of interaction container-content, optimization of infusion in anesthesiology. She teaches clinical pharmacy at the school of pharmacy of Lille.
Pascal Odou obtained his PharmD in 1997 and his PhD in 1998 at Lille University. He began his career as hospital pharmacist in the Psychiatric hospital of Armentières in November 1997, moved a first time, to Dunkerque hospital in 1999, and a second time to the University Hospital in January 2009 with special interest in biopharmacy and sterile compounding. Since September 1998, he teaches biopharmacy, drug compounding and hospital pharmacy at the school of pharmacy of Lille. He manages the research unit on drug infusion named GRITA (Group of Research in drug Infusion and Technology associated) and he also manages the Pharmaceutical Department of the University Hospital of Lille.

Abstract
The administration of several intravenous products on the same catheter is a very common situation in neonatology, where the stakes are high and the dangers sometimes unknown to clinicians. A large number of factors are involved in this administration, directly related to the installation of the infusion line. Moreover, the therapeutics used are often limited, and excluding classic “Marketing Authorization”. Some of these products may prove to be incompatible and thus lose their effectiveness, or even generate particles that are likely to be administered to the patient. We must be aware of these risks in order to optimize the prescription and administration of these intravenous products, especially as we treat fragile and immature patients. The aim of this work is to review the literature on the subject for the prescribers of neonatology units.
Introduction
Population
The population of Neonatal Intensive Care Units (NICUs) includes both very immature patients (24 weeks of gestation and 500 g) and often carrying complex pathologies (medical and/or surgical). These children are technically demanding, and the administration of intravenous (IV) therapies is constant.
There are few drugs with a Neonatal Marketing Authorization, so prescriptions are based on recommendations and must be adapted to the gestational age and weight of the newborns [1].
In addition to the medicines to be administered (antibiotics, sedatives, amines, etc.), these patients very often require parenteral (binary or ternary) nutrition (PN), and most of this is done via a single mono-lumen central venous catheter.
All of these therapies result in infusion volumes that can be significant, sometimes with “hidden” intakes such as sodium, and therefore need to be accounted for in total daily intakes.
Since the blood mass is estimated at 80 ml/kg, it is necessary in these low-weight patients to reason in minimum volumes to be infused, while respecting the concentration limits for each drug, as this may lead to water overload.
The hepatic or renal elimination of these drugs is also different in view of their immaturity, and the doses must therefore be appropriate [2, 3]. For example, vancomycin now has a formula for calculating the necessary dose for 24 hours according to the creatinine concentration of the child, which avoids overdosage and therefore nephrotoxicity [4, 5].
Continuous or discontinuous injectable drugs are administered at low volumes and flow rates on the same infusion line as parenteral nutrition (which also often has a low flow rate). This is likely to cause disturbances in administration, and in particular interactions during prolonged contact in the tubing.
In addition, preterm infants are placed in incubators to maintain optimum thermal and hygrometric conditions: an ambient temperature of 35–36 °C and a humidity of up to 80 %. The perfusion line, placed partly inside the incubator, is therefore subjected to these same environmental conditions.
Similarly, during the first week of life, newborns may need phototherapy, which can alter certain photo-sensitive medicines, including vitamins [6]. Moreover, light can create reactive oxygen species that can oxide other chemicals.
Factors
Several factors are involved in the administration of IV treatments, in particular in relation to the devices used.
One consequence is the existence of significant variability in the volumes delivered to the patient.
Thus, in premature babies<1 000 g, it was shown that only 70 % of the expected dose was delivered 75 min after the start of the drug infusion [7].
This is therefore problematic for certain drugs such as catecholamines, aminoglycosides or even insulin.
Studies have shown haemodynamic and oxygenation changes of newborns during the administration of dopamine or noradrenaline [8, 9].
When intravenous treatment is administered, there are 7 factors that can influence this administration:
The height separating the end of the catheter from the syringe pump delivering the drug.
A vertical movement of the syringe pump delivering the drug solution to the patient will result in a bolus (after an upward displacement), a sudden fluid retraction (after a downward movement) and a no-flow time (ranging from a few seconds to several minutes).
These changes are affected by the height of the movement, the type and volume of the syringe, the type and length of the tubing, the pressure exerted or the programmed infusion rate.
It has been demonstrated that there was no correlation between the infusion flow and the no-flow time, and that the delivery rate was inversely proportional to the set infusion rate during vertical movements of the pump [10, 11].
Characteristics of the syringe delivering the drug.
The volume and design of the syringe affect the volumes delivered to the patient, altering the time to reach the steady state of the drug delivery rate, the triggering time of the ratchet occlusion alarm, but also on the time without flow, the suction volume and the volume of the bolus following a vertical movement of the syringe pump [12, 13, 14, 15].
The impact of this factor is amplified with the programming of low flows.
Characteristics of the tubing delivering the drug.
The compliance of the drug delivery tubing affects the variability of its infusion rate, affecting the time to initiate the occlusion alarm, time without flow, suction volume, and bolus volume during vertical movements of the syringe pump [16, 17].
The impact of this factor is further enhanced in combination with high volume syringes (50 mL) and low flow programming.
The use of non-return and anti-siphon valves.
Non-return valves and anti-siphon valves are unidirectional valves, that is, they allow the passage of the solution only in one direction, either to the patient.
They are referred to as non-return valves because they prevent the fluid from rising to the other infusion lines.
Anti-siphon valves are referred to as they prevent a free flow of the contents of the syringe by gravity, resulting from the presence of air in the syringe. They are characterized by a high opening pressure (100–150 mmHg), which is responsible for lengthening the infusion start-up time for low flows and a no-flow time after a lowering of the syringe pump [18, 19].
The use of in-line filters.
The in-line filters are inserted into the infusion sets to prevent deleterious administration of particles to the patient.
These particles can come directly from the preparation (glass or rubber fragments) or be linked to the existence of drug incompatibilities in the context of a multi-infusion [20].
The administration of these particles can have serious consequences for the patient, as endothelial lesions and thrombosis [21, 22], and the use of in-line filters has been shown to reduce the number of general complications and Systemic Inflammatory Response Syndrome (SIRS) [23].
However, a recent meta-analysis did not reveal a significant effect of online filters on overall mortality in pediatrics/neonatology [24].
Not all drugs are filterable, such as suspensions, micellar solutions, liposomes, having a high viscosity or a risk of adsorption on the filter membrane.
In addition, a recent study showed that the presence of an in-line filter on the infusion line reduced flow irregularities, as well as the start-up time of the syringe pumps at low flow rates [25].
The use of multi-access devices.
As several medications (including PN and IV lipids) are administered simultaneously, the infusion line set comports multi-access devices. Thus, stopcocks or octopusses are often added to the infusion line.
The factors affecting the mass flow of medications administered to the patient are:
the internal volume, compliance and design of the multi-access device,
the sum of the infusion rates (also called total flow rate), including the flow rate of the drug and that of the carrier fluid (usually PN),
the conditions for mixing the administered drug integrating the carrier fluid,
the delivery of bolus upstream in the case of stopping, then the resumption of an infusion,
a change in flow during infusion, which is responsible for a delay in returning to steady state, which will be dependent of the flow rate of the carrier fluid as well as on the internal volume of the delivery system.
The catheter.
There are several catheters available for NICU patients.
The first vascular access usually used in NICU is the umbilical one, which is a short-term and emergency access.
Umbilical venous catheters (UVCs) are commonly used in NICUs to provide intravenous fluids and nutrition, to provide intravenous medications, and for blood sampling.
UVCs are used from birth to 5 days of life and are replaced by a Peripherally Inserted Central Catheter (PICC).
A PICC is a venous silicon catheter used for a medium or long-term access. The ideal position for the tip of the PICC is in the inferior or superior vena cava. PICC allows drug administration, parenteral nutrition, fluid therapy and infusions.
The choice of the catheter will depend on the chosen venous approach, the duration of the infusion, the desired flow rate, the type of drug administered, or the weight of the patient.
In addition, there are specific constraints related to the diameter of the catheters and the number of accesses available [26, 27].
The catheter characteristics, in particular the type of material which compose it [28] and the internal volume of the device [29, 30], have an effect on the volumes delivered to the patient.
These characteristics are amplified with the programming of low infusion rates.
Risks
There are a number of risks associated with prescribing and administering IV treatments, especially in NICU.
The first risk is the risk of error [31].
Errors may occur at every stage between the decision to administer a therapy to the patient and the actual delivery to the patient.
Here are different steps, each of which involves a risk of error:
medical prescription (dose, interval, incompatibilities …) [32]
preparation of the treatment (reconstitution, dilution …)
administration to the patient (patient identity, flow, rinsing, traceability).
Following a finding in our NICU concerning vancomycin administration, we were able to show great disparities during the preparation of this antibiotic and which were related to the use of the needle [33].
Moreover, it was also demonstrated that the preparation of small volumes was a source of error, and that it was not desirable to inject volumes<0.3 mL. In this case, a double dilution must be provided in order to obtain sufficient volumes.
Various tools now allow us to limit these risks of errors: prescribing software, drug incompatibilities cross-tables (Figure 1), absence of transcription of prescriptions, compliance with protocols for preparation, verification at the patient’s bed …
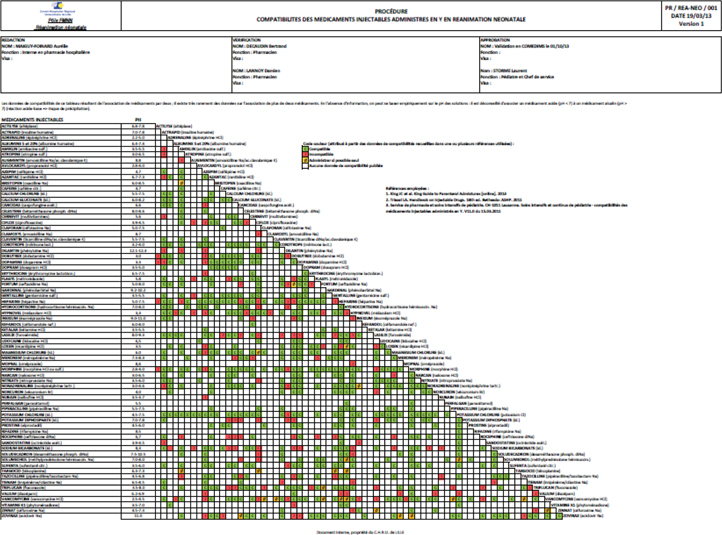
Illustration of the cross-table used in our NICU to avoid drug incompatibilities.
The second risk is the infectious risk, since these infusion lines are manipulated several times a day, especially during access to multi-access devices, and remain in place for several days to several weeks.
Late onset infections due to the catheter are most often related to coagulase-negative staphylococci, but sometimes the catheter can be colonized with yeast (Candida) [34]. These infections can have serious consequences, and increase the morbidity of NICU patients [35].
The last risk, sometimes unknown, is that of Systemic Inflammatory Response Syndrome (SIRS).
The SIRS is related to the particle administration during infusion, and has already been well demonstrated for adult patients of intensive care units [22], and more recently in the pediatric population [36].
Drug interactions
Incompatibility is an undesirable reaction that occurs between the drug and the solution, container or another drug.
The two types of incompatibilities associated with IV administration are physical and chemical.
A drug interaction describes the alteration of a drug effect due to the influence of another substance resulting in a solution that is no longer optimal for the patient after the substances are mixed.
Physical reactions of drugs usually refer to either phase separation or precipitation due to a change of the relation between ionization and nonionization and solubility. The pH-value and the buffer capacity of the IV solutions and the drugs used are major factors responsible for physical interactions.
Repeated blackening of in-line filters had also been observed with particle formation upstream of the device during infusion of binary PN mixtures prepared in bags and delivered in our NICU [37].
To avoid this, we use a cross-table to check drug incompatibilities before prescribing and/or administering them. Unfortunately, there is still missing datas for several drugs (Figure 1).
For example, ceftriaxone is contraindicated in neonates if they require (or are expected to require) treatment with calcium-containing IV solutions, including continuous calcium-containing infusions such as PN because of the risk of precipitation of ceftriaxone-calcium [38].
Injection or infusion of drugs and fluids releases micro particles into the bloodstream.
Various studies have demonstrated the contamination of infusion solutions with glass particles from opening glass ampoules, particles from rubber stoppers or conglomerates of the PN components. These particles may stimulate the immune system and cause organ damage [39].
Particulate matter are “mobile undissolved particles, other than gas bubbles, unintentionally present in the solutions”.
Injectable drug particulate matter are divided into two classes based on the source of the particulate matter: intrinsic particles, defined as those originally associated with the solution, and extrinsic particles, defined as those that enter the container or solution during manufacturing.
Particles may harm the pulmonary endothelium either directly or through activation of complement, platelets and/or neutrophils, leading to the formation of occlusive micro thrombi [40].
Boehne and al. hypothesis was that infused particles act directly on the microcirculation of several organ systems such as the kidney and lung and induce a systemic hypercoagulability and inflammation [36].
Their study demonstrate potential beneficial effects of in-line filtration on the preservation of various organ systems, even if further experimental and clinical investigations are necessary to clarify the exact impact of infused particles [36].
Solutions
Considering all these elements, it seems essential to design the infusion line set with the prescribing habits of the NICU and the needs of the patients.
We also adapt the volume of the syringes according to the perfused flow rates.
We designed our actual infusion line set with NICU nurses and hospital pharmacists.
It was then tested in vitro with solutions of different colors, at the flows prescribed in NICU. This allowed us to highlight the importance of the use of non-return valves because in their absence there was a rise of colored product in the tubings.
The use of in-line filters is now recommended in our NICUs in France and Europe [41, 42].
We use 2 types of in-line filters: 0.22 µm for PN and filterable drugs and 1.2 µm for IV lipids.
In our NICU the entire line set is changed each 96 hours (and each 24 hours for IV lipids line) (Figure 2).

Example of an infusion line set used in our NICU for PN, IV lipids, drug infusion and medications with octopuses and autoflushes. There are two parts in the line set: one used for IV lipids which comports a 1.2 µm in-line filter and is removed each 24 hours; and one used for PN, filterable drugs and continuous infusions which comports a 0.22 µm in-line filter and is removed each 96 hours. There is also a special access for non-filterable drugs and/or IV bolus.
Some medical devices are also being developed and evaluated for the NICU patients, such as multi-lumen devices, allowing the separation of the different treatments administered in the tubing, which could avoid drug incompatibilities [43].
Finally, it is also certain that the risk of a prescription error can be limited by the use of a prescription software [44]. We use in our NICU the prescribing software “LOGIPREN®”, whose drug thesaurus and the dilution and administration protocols have been completely reviewed with the help of referring pharmacists. This software should soon integrate the known drug incompatibilities, and thus further limit the risk of error when prescribing.
Conclusion
The management of prescriptions in NICU patients is a daily and challenging issue.
It requires taking into account the volumes, the devices used and the possible drug incompatibilities in these immature and low weight patients.
The design of the infusion line seems essential and should be carried out in partnership with our pharmacist colleagues, or even tested it in vitro if possible, as we did in our department.
Although this may appear complex, there are now technological solutions adapted to this particular population of NICUs, and new devices are also being developed and tested.
There are still missing data on the various possible drug interactions, but the use of in-line filters may partially limit their consequences.
The real complexity of these administrations in NICUs necessitates close collaboration between neonatologists and the pharmacists in order to optimize each infusion line.
About the authors

Florence Flamein is a NICU pediatrician at the University Hospital of Lille, France. She obtained her PhD in 2011 at Paris 6 University. Her special interests and research projects include management and follow-up of children with perinatal asphyxia. She also works on the improvement of the quality and safety of neonatal care, particularly on drug prescription and intravenous administration.

Laurent STORME, MD, PhD, is professor of Pediatrics at the University Lille 2 France, and Director of the federative project “1000 days 4 Health”. He is Coordinator of the National Center for Rare Disease “Congenital Diaphragmatic Hernia”. He heads the Neonatal Intensive Care Unit at the University Hospital of Lille.

Aurélie Maiguy-Foinard is a clinical pharmacist at the Wallonie Picarde Hospital in Belgium since November 2016. She was a hospital pharmacist at the Pharmacy Institute of the University Hospital of Lille for two years. She obtained her PharmD in 2013 and her PhD in 2014 at Lille II University. Her special interests and research projects included prevention of adverse drug effects associated with intravenous infusion in anaesthesia and intensive care unit, especially in neonatology. She worked specifically on the assessment of the impact of innovative infusion devices.

Maxime Perez is a hospital and university pharmacist at the Pharmacy Institute of the University Hospital of Lille since November 2015 with special interest in clinical pharmacy. He obtained his PharmD and his PhD in 2015 at Lille II University. His research projects include optimization of medical devices used for the injectable administration of incompatible drugs and the evaluation of particles generated during drugs infusion, especially in pediatric and neonatal cares. He teaches clinical pharmacy at the school of pharmacy of Lille.

Bertrand Décaudin obtained his PharmD in 2003 and his PhD in 2006 at Lille University. He began his career as hospital pharmacist in Dunkerque General Hospital in November 2003 and moved to the Lille University Hospital in January 2009 with special interest in evaluation of medical devices and clinical pharmacy. Since September 2007, he teaches clinical pharmacy at the school of pharmacy of Lille. He manages research projects on drug infusion in anaesthesia and critical care medicine.

Morgane Masse is a hospital and university resident at the Pharmacy Institute of the University Hospital of Lille since November 2012. She obtained her PharmD in 2016 at Lille 2 University. Her research projects focus on interactions between content and container, especially with medical devices containing polyvinylchloride.

Stéphanie Genay is a hospital and university pharmacist at the Pharmacy Institute of the University Hospital of Lille since September 2013 with special interest in clinical pharmacy. She obtained her PharmD in 2013 and her PhD in 2014 at Lille University. Her research projects include optimization of medical devices used for the injectable administration of incompatible drugs, caractérization of interaction container-content, optimization of infusion in anesthesiology. She teaches clinical pharmacy at the school of pharmacy of Lille.

Pascal Odou obtained his PharmD in 1997 and his PhD in 1998 at Lille University. He began his career as hospital pharmacist in the Psychiatric hospital of Armentières in November 1997, moved a first time, to Dunkerque hospital in 1999, and a second time to the University Hospital in January 2009 with special interest in biopharmacy and sterile compounding. Since September 1998, he teaches biopharmacy, drug compounding and hospital pharmacy at the school of pharmacy of Lille. He manages the research unit on drug infusion named GRITA (Group of Research in drug Infusion and Technology associated) and he also manages the Pharmaceutical Department of the University Hospital of Lille.
Conflict of interest statement: Authors state no conflict of interest. All authors have read the journal’s Publication ethics and publication malpractice statement available at the journal’s website and hereby confirm that they comply with all its parts applicable to the present scientific work.
References
1. Ward RM, Benjamin D, Barrett JS, Allegaert K, Portman R, Davis JM et al. Safety, dosing, and pharmaceutical quality for studies that evaluate medicinal products (including biological products) in neonates. Pediatr Res 2017;81:692–711.10.1038/pr.2016.221Suche in Google Scholar PubMed
2. Kearns GL, Abdel-Rahman SM, Alander SW, Blowey DL, Leeder JS, Kauffman RE. Developmental pharmacology–drug disposition, action, and therapy in infants and children. N Engl J Med 2003 18;349:1157–1167.10.1056/NEJMra035092Suche in Google Scholar PubMed
3. Oni L, Hawcutt DB, Turner MA, Beresford MW, McWilliam S, Barton C et al. Optimising the use of medicines to reduce acute kidney injury in children and babies. Pharmacol Ther 2017;174:55–62.10.1016/j.pharmthera.2017.02.018Suche in Google Scholar PubMed
4. Irikura M, Fujiyama A, Saita F, Fukushima S, Kitaoka H, Fukuda T et al. Evaluation of the vancomycin dosage regimen based on serum creatinine used in the neonatal intensive care unit. Pediatr Int 2011;53:1038–1044.10.1111/j.1442-200X.2011.03441.xSuche in Google Scholar PubMed
5. Zhao W, Lopez E, Biran V, Durrmeyer X, Fakhoury M, Jacqz-Aigrain E. Vancomycin continuous infusion in neonates: Dosing optimisation and therapeutic drug monitoring. Arch Dis Child 2013;98:449–453.10.1136/archdischild-2012-302765Suche in Google Scholar PubMed
6. Chessex P, Laborie S, Lavoie JC, Rouleau T. Photoprotection of solutions of parenteral nutrition decreases the infused load as well as the urinary excretion of peroxides in premature infants. Semin Perinatol 2001;25:55–59.10.1053/sper.2001.23188Suche in Google Scholar PubMed
7. Sherwin CMT, McCaffrey F, Broadbent RS, Reith DM, Medlicott NJ. Discrepancies between predicted and observed rates of intravenous gentamicin delivery for neonates. J Pharm Pharmacol 2009;61:465–471.10.1211/jpp.61.04.0008Suche in Google Scholar
8. Stowe CD, Storgion SA, Lee KR, Phelps SJ. Hemodynamic response to intentionally altered flow continuity of dobutamine and dopamine by an infusion pump in infants. Pharmacotherapy 1996;16:1018–1023.Suche in Google Scholar
9. Cunningham S, Deere S, McIntosh N. Cyclical variation of blood pressure and heart rate in neonates. Arch Dis Child 1993;69:64–67.10.1136/adc.69.1_Spec_No.64Suche in Google Scholar
10. Donald AI, Chinthamuneedi MP, Spearritt D. Effect of changes in syringe driver height on flow: A small quantitative study. Crit Care Resusc 2007;9:143–147.Suche in Google Scholar
11. Neff TA, Fischer JE, Schulz G, Baenziger O, Weiss M. Infusion pump performance with vertical displacement: Effect of syringe pump and assembly type. Intensive Care Med 2001;27:287–291.10.1007/s001340000784Suche in Google Scholar PubMed
12. Kim DW, Steward DJ. The effect of syringe size on the performance of an infusion pump. Pediatr Anesth 1999;9:335–337.10.1046/j.1460-9592.1999.00402.xSuche in Google Scholar PubMed
13. Capes DF, Dunster KR, Sunderland VB, McMillan D, Colditz PB, McDonald C. Fluctuations in syringe-pump infusions: association with blood pressure variations in infants. Am J Health Syst Pharm 1995;52:1646–1653.10.1093/ajhp/52.15.1646Suche in Google Scholar PubMed
14. Weiss M, Fischer J, Neff BO. The effects of syringe plunger design on drug delivery during vertical displacement of syringe pumps. Anaesthesia 2000a;55:1094–1098.10.1046/j.1365-2044.2000.01550.xSuche in Google Scholar PubMed
15. Weiss M, Hug MI, Neff T, Fischer J. Syringe size and flow rate affect drug delivery from syringe pumps. Can J Anesth 2000b;47:1031–1035.10.1007/BF03024878Suche in Google Scholar PubMed
16. Weiss M, Neff T, Gerber A, Fischer J. Impact of infusion line compliance on syringe pump performance. Pediatr Anesth 2000c;10:595–599.10.1111/j.1460-9592.2000.566ab.xSuche in Google Scholar PubMed
17. Weiss M, Bänziger O, Neff T, Fanconi S. Influence of infusion line compliance on drug delivery rate during acute line loop formation. Intensive Care Med 2000d;26:776–779.10.1007/s001340051246Suche in Google Scholar PubMed
18. McCarroll C, McAtamney D, Taylor R. Alteration in flow delivery with antisyphon devices. Anaesthesia 2000;55:355–357.10.1046/j.1365-2044.2000.01282.xSuche in Google Scholar PubMed
19. Weiss M, Fischer J, Neff T, Schulz G, Bänziger O. Do antisiphon valves reduce flow irregularities during vertical displacement of infusion pump systems? Anaesth Intensive Care 2000;28:680–683.10.1177/0310057X0002800613Suche in Google Scholar PubMed
20. Oie S, Kamiya A. Particulate and microbial contamination in in-use admixed parenteral nutrition solutions. Biol Pharm Bull 2005;28:2268–2270.10.1248/bpb.28.2268Suche in Google Scholar PubMed
21. Puntis J, Wilkins K, Ball PA, Rushton DI, Booth IW. Hazards of parenteral treatment: Do particles count? Arch Dis Child 1992;67:1475–1477.10.1136/adc.67.12.1475Suche in Google Scholar PubMed PubMed Central
22. Lehr HA, Brunner J, Rangoonwala R, Kirkpatrick CJ. Particulate matter contamination of intravenous antibiotics aggravates loss of functional capillary density in postischemic striated muscle. Am J Respir Crit Care Med 2002;165:514–520.10.1164/ajrccm.165.4.2108033Suche in Google Scholar PubMed
23. Jack T, Boehne M, Brent BE, Hoy L, Köditz H, Wessel A, et al. In-line filtration reduces severe complications and length of stay on pediatric intensive care unit: A prospective, randomized, controlled trial. Intensive Care Med 2012;38:1008–1016.10.1007/s00134-012-2539-7Suche in Google Scholar
24. Foster JP, Richards R, Showell MG, Jones LJ. Intravenous in-line filters for preventing morbidity and mortality in neonates. Cochrane Database Syst Rev 2015;6:CD005248.10.1002/14651858.CD005248.pub3Suche in Google Scholar
25. Brotschi B, Grass B, Weiss M, Doell C, Bernet V. In-line filter included into the syringe infusion pump assembly reduces flow irregularities. Intensive Care Med 2012;38:518–522.10.1007/s00134-011-2452-5Suche in Google Scholar
26. Stovroff M, Teague WG. Intravenous access in infants and children. Pediatr Clin North Am 1998;45:1373–1393.10.1016/S0031-3955(05)70095-XSuche in Google Scholar
27. Ramasethu J. Complications of vascular catheters in the neonatal intensive care unit. Clin Perinatol 2008;35:199–222.10.1016/j.clp.2007.11.007Suche in Google Scholar
28. Angle JF, Matsumoto AH, Skalak TC, O’Brien RF, Hartwell GD, Tegtmeyer CJ. Flow characteristics of peripherally inserted central catheters. J Vasc Interv Radiol 1997;8:569–577.10.1016/S1051-0443(97)70611-0Suche in Google Scholar
29. Lovich MA, Peterfreund GL, Sims NM, Peterfreund RA. Central venous catheter infusions: A laboratory model shows large differences in drug delivery dynamics related to catheter dead volume. Crit Care Med 2007;35:2792–2798.Suche in Google Scholar
30. Bartels K, Moss DR, Peterfreund RA. An analysis of drug delivery dynamics via a pediatric central venous infusion system: Quantification of delays in achieving intended doses. Anesth Analg 2009;109:1156–1161.10.1213/ane.0b013e3181b220c9Suche in Google Scholar PubMed
31. De Giorgi I, Fonzo-Christe C, Cingria L, Caredda B, Meyer V, Pfister RE, et al. Risk and pharmacoeconomic analyses of the injectable medication process in the paediatric and neonatal intensive care units. Int J Qual Health Care 2010;22:170–178.10.1093/intqhc/mzq015Suche in Google Scholar PubMed
32. Machado AP, Tomich CS, Osme SF, Ferreira DM, Mendonça MA, Pinto RM, et al. Prescribing errors in a Brazilian neonatal intensive care unit. Cad Saude Publica 2015;31:2610–2620.10.1590/0102-311X00194714Suche in Google Scholar PubMed
33. Foinard A, Décaudin B, Simon N, Barthélémy C, Storme L, Odou P. Vancomycin syringe study shows significant reduction in dosing variability after introducing a revised protocol. Acta Paediatr 2014;103:e93–e94.10.1111/apa.12484Suche in Google Scholar PubMed
34. Kaufman DA. Challenging issues in neonatal candidiasis. Curr Med Res Opin 2010;26:1769–1778. DOI:10.1185/03007995.2010.487799.Suche in Google Scholar PubMed
35. Stoll BJ, Hansen N, Fanaroff AA, Wright LL, Carlo WA, Ehrenkranz RA et al. Late-onset sepsis in very low birth weight neonates: The experience of the NICHD Neonatal Research Network. Pediatrics 2002;110:285–291.10.1542/peds.110.2.285Suche in Google Scholar PubMed
36. Boehne M, Jack T, Köditz H, Seidemann K, Schmidt F, Abura M et al. In-line filtration minimizes organ dysfunction: New aspects from a prospective, randomized, controlled trial. BMC Pediatr 2013;13:21.10.1186/1471-2431-13-21Suche in Google Scholar PubMed PubMed Central
37. Foinard A, Perez M, Barthélémy C, Lannoy D, Flamein F, Storme L et al. In Vitro Assessment of Interaction Between Amino Acids and Copper in Neonatal Parenteral Nutrition. J Parenter Enteral Nutr 2016;40:827–834.10.1177/0148607115571967Suche in Google Scholar PubMed
38. Nakai Y, Tokuyama E, Yoshida M, Uchida T. Incompatibility of ceftriaxone sodium with calcium-containing products. Yakugaku Zasshi 2009;129:1385–1392.10.1248/yakushi.129.1385Suche in Google Scholar PubMed
39. Jack T, Brent BE, Boehne M, Müller M, Sewald K, Braun A et al. Analysis of particulate contaminations of infusion solutions in a pediatric intensive care unit. Intensive Care Med 2010;36:707–711.10.1007/s00134-010-1775-ySuche in Google Scholar PubMed PubMed Central
40. Brent BE, Jack T, Sasse M. In-line filtration of intravenous fluids retains ‘spearhead’-shaped particles from the vascular system after open-heart surgery. Eur Heart J 2007;28:1192.10.1093/eurheartj/ehl398Suche in Google Scholar PubMed
41. IGAS, RAPPORT N°2014-168RSuche in Google Scholar
42. Koletzko B, Goulet O, Hunt J, Krohn K, Shamir R, Parenteral Nutrition Guidelines Working Group et al. 1. Guidelines on Paediatric Parenteral Nutrition of the European Society of Paediatric Gastroenterology, Hepatology and Nutrition (ESPGHAN) and the European Society for Clinical Nutrition and Metabolism (ESPEN), Supported by the European Society of Paediatric Research (ESPR). J Pediatr Gastroenterol Nutr 2005;41:S1–87.Suche in Google Scholar
43. Horri et al. Frequency of dosage prescribing medication errors associated with manual prescriptions for very preterm infants. J Clin Pharm Ther 2014;39:637–641.10.1111/jcpt.12194Suche in Google Scholar PubMed
44. Perez M, Décaudin B, Foinard A, Barthélémy C, Debaene B, Lebuffe G, et al. Compatibility of medications during multi-infusion therapy: A controlled in vitro study on a multilumen infusion device. Anaesth Crit Care Pain Med 2015;34:83–88.10.1016/j.accpm.2014.06.003Suche in Google Scholar PubMed
© 2017 Walter de Gruyter GmbH, Berlin/Boston
Artikel in diesem Heft
- Frontmatter
- graphical-abstract
- Editorial
- The infusion, not so simple …
- Conference Report
- Challenges and Opportunities in Drug Administration: The Twelve Tasks of Infusorix!
- Reviews
- Drug Flow Through Clinical Infusion Systems: How Modeling of the Common-volume Helps Explain Clinical Events
- Closed-loop Administration of General Anaesthesia: From Sensor to Medical Device
- Avoid Drug Incompatibilities: Clinical Context in Neonatal Intensive Care Unit (NICU)
- Criteria for Judging the Quality of a Publication on Physicochemical Stability of Ready to Use Injectable Drugs
- Research Article
- Impact of Physical Parameters on Dosing Errors due to a Syringe Exchange in Multi-Infusion Therapy
Artikel in diesem Heft
- Frontmatter
- graphical-abstract
- Editorial
- The infusion, not so simple …
- Conference Report
- Challenges and Opportunities in Drug Administration: The Twelve Tasks of Infusorix!
- Reviews
- Drug Flow Through Clinical Infusion Systems: How Modeling of the Common-volume Helps Explain Clinical Events
- Closed-loop Administration of General Anaesthesia: From Sensor to Medical Device
- Avoid Drug Incompatibilities: Clinical Context in Neonatal Intensive Care Unit (NICU)
- Criteria for Judging the Quality of a Publication on Physicochemical Stability of Ready to Use Injectable Drugs
- Research Article
- Impact of Physical Parameters on Dosing Errors due to a Syringe Exchange in Multi-Infusion Therapy