Development of the “KARUNI” (young adolescents community) model to prevent stunting: a phenomenological study on adolescents in Gunungkidul regency, Yogyakarta, Indonesia
-
Benny Karuniawati

 ,
Supriyadi Hari Respati
,
Supriyadi Hari Respati

Abstract
Background
Stunting is a major health problem in developing countries due to chronic malnutrition that impacts physical growth, cognitive ability, and long-term productivity. The focus of stunting prevention is generally aimed at pregnant women and toddlers, while adolescents, especially adolescent girls, are often neglected. In fact, they will be the future mothers who determine the quality of the next generation. Malnutrition and anemia in adolescents increase the risk of giving birth to stunted children. Innovative nutritional intervention programs, such as nutrition education and iron supplements, are needed to break the cycle of stunting, involving adolescents as important targets in prevention. Karuni is a program specifically designed for teenagers aged 12–15 years with the main focus being on empowering teenagers through nutrition education, reproductive health and clean and healthy living behavior as well as involving parents to optimize the program.
Methods
This study used a phenomenological approach to explore the understanding of adolescent girls aged 12–15 years about the stunting prevention program in Gunungkidul Regency, Indonesia. Data were collected through in-depth interviews and FGDs with adolescents, officials running the Adolescent Health Care (PKPR) program, and related agencies. Data validity was guaranteed by triangulation of sources and NVivo was used for analysis.
Results
The identified five themes related to the adolescent intervention program for stunting prevention: program implementation, achievements, barriers, needs, and KARUNI model design. Program monitoring is important, but faces barriers such as the lack of prioritization and motivation. Cross-sectoral collaboration, innovation, and appropriate media are needed in the implementation of the KARUNI model to increase the effectiveness of the stunting prevention program for adolescents.
Conclusions
The importance of the role of adolescents in efforts to reduce the prevalence of stunting, especially through collaboration between health centers (Puskesmas) and schools in implementing the PKPR program, providing iron tablets, and health screening.
Introduction
Stunting or a condition of failure to thrive due to chronic malnutrition is one of the main health problems faced by many developing countries. Its impact is not only seen in height that is lower than the standard for a particular age but also in cognitive development and long-term ability to be productive. A study conducted by the World Bank shows that when stunted children become adults, they are 20 % less productive than those who were healthy children [1]. In addition, long-term effects are also associated with decreased fat oxidation ability, which causes the risk of obesity and degenerative diseases. The results of a multicenter survey conducted by Poh et al. involving 16,700 children in Indonesia, Malaysia, Thailand, and Vietnam showed that stunting was significantly associated with decreased IQ, especially non-verbal, with a value of <89 (OR 1.65 95 % IK: 1.64–1.66) [2].
So far, the main focus of stunting prevention programs has been more directed at pregnant women, toddlers, and children under the age of two (the first 1,000 days of life). However, there is a segment of the population that is crucial in breaking the chain of stunting, but it is often overlooked: adolescents, especially adolescent girls. These girls will become mothers in the future who determine the quality of the next generation. Malnutrition, anemia, and poor reproductive health in adolescent girls have the potential to increase the risk of giving birth to stunted children. Research in India provides evidence that adolescents who experience malnutrition are at risk of giving birth to babies 0.25 standard deviations shorter than the average weight for their age and are five times more likely to experience stunting compared to children born to adult mothers [2].
Innovative stunting prevention programs conducted during adolescence have developed in recent years in various parts of the world including nutrition education, iron supplementation, nutrition interventions and awareness campaigns on the importance of healthy eating patterns [3], [4], [5], [6], [7]. The nutrition intervention program in Ethiopia (called the School Feeding Program) focuses on nutrition education and interventions for adolescent girls. The results of the study explained that the school feeding program has improved nutritional status and academic achievement. However, to ensure the sustainability of the program, the program must be supported by national policies and budget allocation is needed too [7]. Next is the Nutrition-Friendly Schools Initiative program implemented in Latin America and Africa. This program seeks to create a school environment that encourages healthy behaviors, including balanced nutrition. By providing nutritious food at school, this program supports adolescents in obtaining adequate nutrition, which will affect their health and reproductive abilities in the future [8]. In addition, a school-based weekly iron and folic acid supplementation program has been effective in reducing anemia in a group of prospective adolescent girls aged 10–19 years in Ghana [9]. Another program implemented in Delhi, India, namely the provision of weekly iron and folic acid (PIA) supplements accompanied by monthly health education has been effective in reducing the prevalence of anemia in school-age adolescent girls [10] Recent studies emphasize the importance of involving adolescents in stunting prevention efforts. Health education programs targeting teenagers have shown significant improvements in knowledge about stunting and its prevention (Asatuti et al., 2021; [11]). These initiatives can be integrated into school curricula and community activities, focusing on balanced nutrition, family planning, and early childhood care [11]. Forming youth groups dedicated to stunting prevention has proven effective in raising awareness and promoting community engagement [11]. Additionally, monitoring nutritional status and providing nutrition education to adolescents are crucial steps in preventing stunting (Asatuti et al., 2021). By educating teenagers as future parents, these programs aim to reduce stunting rates and improve overall community health. The studies emphasize the need for continued efforts in adolescent education and involvement as a key strategy in the long-term prevention of stunting. Effective stunting prevention measures include providing nutritional education to influential parties such as community health workers, mothers of toddlers, and women of childbearing age (Fristiwi et al., 2023). By educating teenagers as future parents, these programs aim to reduce stunting rates and improve overall community health.
Stunting is one of the pressing public health problems in Indonesia. Various efforts have been made to reduce its prevalence, but the problem remains a serious threat to future generations. The results of the 2023 Indonesian Health Survey showed that the stunting rate was still 21.5 %, down only 0.1 % from 2022 [12]. This challenge is exacerbated by the lack of attention paid to adolescent health in existing stunting prevention programs. Data show that many adolescents in Indonesia experience nutritional problems such as anemia, unbalanced food intake, and minimal knowledge about reproductive health and nutrition. The current prevalence of adolescent anemia is 15.5 % and the prevalence of malnutrition is 15.9 % [12]. Nutritional status, especially in adolescent girls, needs more attention because adolescent girls are prospective mothers who will give birth to the next generation. The lack of early intervention in adolescents’ health causes them to be less prepared to play the role of healthy mothers later in life, meaning that the cycle of stunting continues.
To answer this challenge, there needs to be innovation in the form of interventions specifically aimed at adolescents as part of a long-term stunting prevention strategy. Referring to WHO recommendations, it is necessary to strengthen interventions to improve maternal nutrition and health, starting from adolescent girls. The KARUNI (young adolescents community) model is an innovative program designed to improve adolescent health and nutrition as a first step in breaking the chain of stunting. This model is designed to equip adolescents, especially adolescent girls, with the knowledge and skills they need to maintain their health, including education about balanced nutrition, reproductive health, and the importance of early preparation for a healthy pregnancy. The KARUNI program prioritizes a community-based approach, where adolescents are actively involved in educational activities and mentoring related to health and nutrition. In addition, KARUNI groups also play a role in building adolescent awareness about the importance of their role in preventing stunting by improving nutritional status and overall health. Individual compliance in carrying out a behavior will encourage the emergence of self-efficacy towards that behavior [13]. Research indicates that Daily meal tracking tools have been shown to significantly enhance nutrition knowledge and attitudes among teenagers aged 13–16 [14]. Health education programs covering various aspects of healthy living, including nutrition and exercise, can help late adolescents make informed decisions about adopting healthier lifestyles and increase their self-confidence in implementing these changes [15]. Educational and communicative approaches tailored to adolescents’ characteristics and needs can promote healthy behaviors, with studies showing improvements in health knowledge and lifestyle practices after such interventions [16]. Effective nutrition education methods for adolescents include social media, audiovisual tools, and conventional media, with peer educator training playing a key role in successful implementation [17].
Adolescent empowerment plays a crucial role in stunting prevention. Women’s empowerment, particularly in education and knowledge, significantly impacts stunting prevention in children aged 6–59 months [18]. Media-based health education, especially social media platforms like TikTok and Instagram, has proven effective in increasing adolescents’ understanding of stunting prevention [19]. Nursing interventions targeting adolescent mothers can contribute to preventing stunting in their children, focusing on nutrition during pregnancy and breastfeeding [20]. Health education programs aimed at increasing adolescents’ knowledge about proper nutrition and stunting prevention have shown positive results, as evidenced by improved pre- and post-test scores [21]. These studies highlight the importance of empowering adolescents through education, media interventions, and targeted healthcare initiatives to address the global issue of stunting and improve nutritional outcomes for both adolescents and their future children.
This study aims to design a model for an early adolescent group called the KARUNI model as an innovative stunting prevention program that focuses on groups of adolescents. Karuni in this study was conducted to design a new model for empowering teenagers and parents to prevent stunting. By integrating community-based interventions, this program is expected to improve knowledge and healthy behavior among adolescents, as well as strengthen their readiness to support stunting prevention efforts in the future. The results of this study are expected to provide significant contributions to developing a more comprehensive stunting prevention strategy, starting from the adolescent age phase as the foundation of the health of future generations.
Research method
This study uses a phenomenological approach that aims to explore and describe how adolescents understand, experience, and interpret stunting prevention programs in their daily lives. This study uses the perspective of teenagers as the target users of Karuni. The study was conducted in Gunungkidul Regency, Yogyakarta, Indonesia. The main subjects or informants in this study were adolescent girls aged 12–15 years. The supporting informants in this study were officials running the Adolescent Health Care Program (PKPR) at the community health center (Puskesmas), the Health Office, and the Community Empowerment and Village, Population Control and Family Planning (DPMKP2KB) office. The selection criteria for the informants used purposive sampling based on their direct experience in intervention programs for stunting prevention in adolescents and their willingness to share their experiences in depth. The number of informants in this study was 12 adolescent girls, 10 officials from the PKPR program at the Pusksmas, one person from the Health Office, and one person from the DPMKP2KB office.
The data collection method to explore the experiences and perceptions of the subjects was carried out using in-depth interviews and focus group discussions (FGDs). FGD activities for adolescent girls were conducted in the hall of SMP Negeri 2 Karangmojo (junior high school). The FGD activities for the PKPR program holder group at the Puskesmas were conducted in the community hall of the Gunungkidul Health Office. In-depth interviews with the stunting task force at DPMKP2KB were conducted in that office’s meeting room, while interviews with the Health Office were conducted in the room of the head of the family health section. In each group, FGDs and interviews lasted for 1 h. In the data collection process, the researcher acted as the main instrument and was assisted by four research assistants. FGDs and in-depth interviews were conducted using guidelines compiled based on a literature review related to stunting prevention programs for adolescents. These guidelines include open-ended questions so that participants can provide in-depth responses according to their experiences. In addition to the FGD and in-depth interview guidelines, the researcher also used a recorder, camera, and field notes to document the data collection process. This study focuses on the perspective of adolescents for model development, exploring adolescent behavioral problems, exploring adolescent material needs, and identifying appropriate media education for adolescents.
The validation of the data in this study was carried out through the triangulation of sources, namely adolescent girls aged 12–15 years, the head of the DPMKP2KB at the Health Office, officials from the PKPPR program at the Puskesmas, the stunting task force of the DPMKP2KB office in Gunungkidul district, and peer debriefing. All data obtained from the results of FGDs and in-depth interviews were transcribed and coded using NVivo software. In this study, data saturation was achieved after conducting in-depth interviews with the informants. Interviews were conducted repeatedly until no new information or themes were found that were relevant to the study. At this point, the data obtained provided a complete and comprehensive understanding of the experiences of adolescents in the ongoing stunting prevention program. This data saturation is an indicator that the information collected is sufficient and adequate to answer the research questions, and that there are no more significant new variations from the data collected.
This study pays attention to the principles of research ethics, especially those involving adolescents as research subjects. Prior to the study, permission was obtained from the research ethics committee (No.1.538/VI/HREC/2024) issued by RSUD Moewardi (government hospital). In addition, participants and parents or guardians were given an informed consent form explaining the purpose, procedures, and the participant’s right to withdraw at any time during the study. The confidentiality of each participant’s identity was maintained by using anonymous codes in the presentation of the research results.
Results
In this study, the data collection method was interviews conducted with four informants, namely two young women, one stunting task force member from the DPMKP2KB Office, and one Head of Social Welfare from the Gunungkidul Regency Health Office. The focus group discussions (FGDs) were conducted with 10 young women and 10 PKPR officials from the Gunungkidul Regency Health Office. Interviews were conducted at the offices of the DPMKP2KB Office and Gunungkidul Regency Health Office, while focus group discussions with PKPR officials were conducted in the public hall of the Gunungkidul Regency Health Office and the FGDs with adolescents were conducted in the hall of SMP Negeri 2 Karangmojo (junior high school). The interviews and FGDs were conducted by researchers assisted by research assistants (Tables 1 and 2).
Characteristics of informants in FGDs.
| No | Participant | Age | Education | Employment |
|---|---|---|---|---|
| 1 | S | 52 | Diploma III | Puskesmas midwife |
| 2 | Sw | 49 | Diploma III | Puskesmas midwife |
| 3 | Sn | 54 | Diploma III | Puskesmas midwife |
| 4 | Lr | 50 | Diploma III | Puskesmas midwife |
| 5 | Ki | 36 | Diploma III | Puskesmas midwife |
| 6 | Fnh | 33 | Diploma III | Puskesmas midwife |
| 7 | Wr | 38 | Diploma III | Puskesmas midwife |
| 8 | Yn | 39 | Diploma III | Puskesmas midwife |
| 9 | Mnk | 25 | Diploma III | Puskesmas midwife |
| 10 | Ddt | 32 | Diploma III | Puskesmas midwife |
| 11 | Pna | 14 | Junior high | Student |
| 12 | K | 14 | Junior high | Student |
| 13 | D | 14 | Junior high | Student |
| 14 | Ea | 14 | Junior high | Student |
| 15 | Ca | 13 | Junior high | Student |
| 16 | Vr | 13 | Junior high | Student |
| 17 | Ta | 14 | Junior high | Student |
| 18 | Rds | 13 | Junior high | Student |
| 19 | Mrp | 14 | Junior high | Student |
| 20 | Js | 14 | Junior high | Student |
Characteristics of participants in IDI activities.
| No | Participant | Age | Education | Employment |
|---|---|---|---|---|
| 1 | E | 36 | Master’s | DPMKP2KB stunting task force |
| 2 | Tyn | 41 | Bachelor’s | Head of social welfare |
| 3 | Eac | 14 | Junior high | Student |
| 4 | Vra | 14 | Junior high | Student |
There were 20 participants in the FGD activity, consisting of two large groups, namely midwives working at the Puskesmas and students. The ages of the participants varied from 13 to 54 years. The Puskesmas midwives had an age range of 25–54 years, while the students were between 13 and 14 years. All of the Puskesmas midwives had a Diploma III educational background, indicating that they had completed higher education in midwifery and the students were at the junior high school level (Tables 1 and 2).
There were four participants, two of whom were professionals, and two others were junior high school students. The ages of the professional participants were 36 and 41 years, while the age of the junior high school student participants was 14 years. The first participant had a master’s degree and the second participant had a bachelor’s degree and the other two participants were currently still at junior high school. After data collection was conducted. The research data was analyzed using content analysis. The interview results were transcribed, then codes were determined and combined into categories and find the thems as follows (Figure 1).
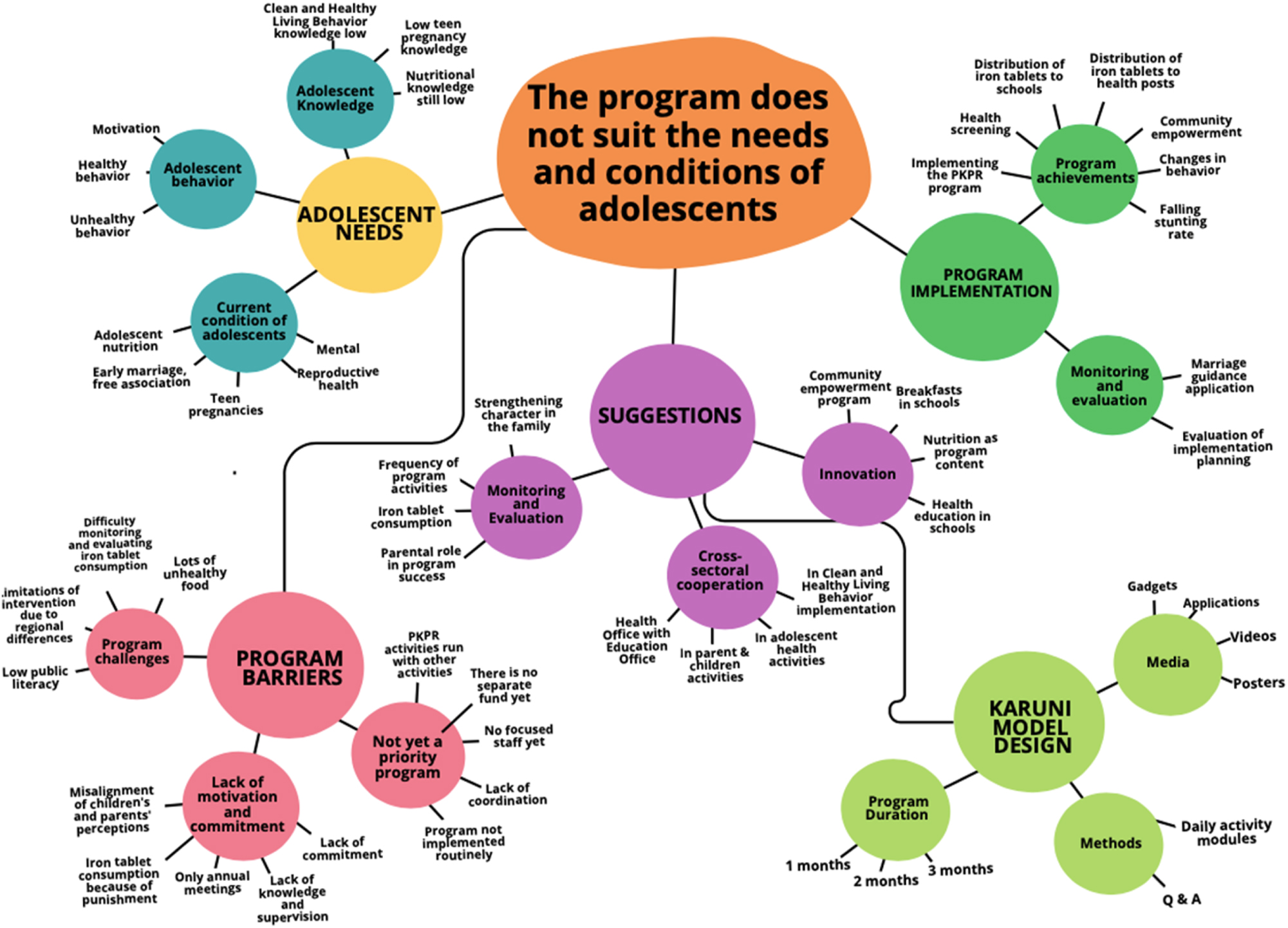
Research overview.
According to the results of the FGDs and in-depth interviews conducted on the four target groups, five main themes were obtained related to the adolescent intervention program as an effort to prevent stunting in Gunungkidul Regency. These five themes are program implementation, obstacles to program implementation, adolescent needs, suggestions and design of the KARUNI model.
Program implementation
The intervention program for adolescents in preventing stunting in Gunungkidul Regency has been implemented in terms of program achievements where in its implementation monitoring and evaluation have been carried out to measure the impact of the program. According to the findings, several intervention programs targeting adolescents, such as the Adolescent Health Care Service (PKPR), education for adolescents, provision of Fe tablets, health screening. Monitoring has also been carried out routinely monthly, quarterly, semi-annually, annually.
Program achievements
According to the FGDs and interviews, the informant explained that Gunungkidul has implemented several adolescent intervention programs to prevent stunting, namely starting from the implementation of the PKPR program by the Puskesmas in collaboration with schools, providing iron tablets to adolescent girls both through schools and posyandu (integrated health posts), implementing health screening packaged in a community empowerment program with the main goal of changing behavior to reduce the prevalence of stunting, especially in Gunungkidul.
“The PKPR program, namely at the adolescent posyandu, Hb health screening for women, fish, nutritious rice, blood-boosting tablets, and HIV screening, from the laboratory with the HIV program holder together” (Yn, 39 years old, FGD for PKPR officials at the Puskesmas)
“The decline in stunting rates automatically means we know that most people’s education is low, so sometimes, for example, from the results of stunting habitats when they have been referred, my child is still fine” (E, 36 years old, in-depth interview with the DPMKP2KB)
Monitoring and evaluation
Monitoring and evaluation are important aspects in ensuring that the stunting prevention program runs according to its targets. The informants said that monitoring and evaluation activities are carried out to monitor compliance with iron tablet consumption, changes in adolescent behavior, and the effectiveness of educational activities carried out. Periodic evaluations are also important to identify barriers faced during program implementation and to find the right solutions to overcome these challenges.
“Yes, usually we do the program for three months, there is quarterly monitoring, then there is semester monitoring, then including evaluation of reporting records and there is also annual reporting. If the routine report is per month, so one month, three months, six months and one year” (TYN, 41 years old, in-depth interview with the Health Office).
The informants added that evaluation also helps in measuring the impact of the program on reducing stunting rates in the community, meaning that the program can continue to be adjusted and improved to achieve optimal results.
“So if the program evaluation is certain, the coverage of stunted adolescent health must be there every month, so in the reporting there is a measurement, yeah? Before we intervene in the initial measurement, the initial measurement we do the intervention for six months then we repeat the intervention” (TYN, 41 years old, in-depth interview with the Health Office).
Barriers to implementation
The results of the FGD and in-depth interviews show that several barriers to the implementation of the adolescent health intervention program as an effort to prevent stunting, namely the adolescent health intervention program has not been a priority program, there is still a lack of motivation and commitment from related parties meaning that there are still challenges in the implementation of the next program.
Not yet a priority program
The stunting prevention program for adolescents has not been a priority in national or local health policies. The informants said that, in the implementation of the adolescent health intervention program in the form of the PKPR program, there are no human resources that focus on adolescent health, meaning that PKPR activities are carried out simultaneously with other activities, the program cannot be implemented routinely, and there is a lack of coordination in program implementation. In addition, the informant said that in this activity there are no special funds to finance the adolescent health program.
“Human resources and funds because for the implementation of adolescent posyandu, the posyandu are during working hours, for example on holidays, we cannot monitor during holidays” (KI, 36 years old, FGD for puskesmas PKPR officials)
“Not routinely, if possible the puskesmas needs data”, “Only twice” (J, 14 years old, FGD for adolescents).
Lack of motivation and commitment
One of the biggest challenges to implementing adolescent health intervention programs – especially those related to stunting prevention – is the lack of motivation and commitment on the part of adolescents themselves, parents, health workers, and other stakeholders. The informants said that the high rate of stunting is due to the lack of parental knowledge, which causes a lack of integration in maintaining a healthy lifestyle between children and parents. Then the lack of adolescent knowledge about reproductive health results in adolescents’ non-compliance in consuming iron tablets and if they consume iron tablets because of punishment. In addition, the lack of knowledge among adolescents about reproductive health makes it difficult to increase adolescent motivation to consume iron tablets and participate in adolescent health post activities.
“The method is that the puskesmas will send the tablets, then they will be divided into one box per class, and if they have taken it, they will be asked to sign” (J, 14 years old, FGD for adolescents)
“It is mandatory to take it, if you don’t, it will be recorded and reported to the Karangmojo Puskesmas official” (SM, 56th, in-depth school interview)
“The meeting is only held once a year for new students” (J, 14 years old, FGD for adolescents)
Program challenges
Health intervention programs for adolescents in preventing stunting face various challenges that can affect their effectiveness and sustainability. The informants conveyed that one of the challenges in implementing the stunting prevention program for adolescents is the large number of unhealthy foods currently available which can result in a lack of nutritional intake in adolescents. In addition, the challenges that must be faced by health workers and the government are the difficulty in monitoring and evaluating the implementation of iron tablet consumption due to the lack of literacy related to health among the public. Furthermore, the difference in the work area of the Puskesmas and the adolescents’ homes makes it difficult for health workers to intervene in different areas.
“Currently, many people sell jumbo ice, that is also a challenge for us because excessive sugar consumption interferes with iron absorption” (DDT, 32 years old, PKPR official at the Puskesmas)
“Compliance in taking iron tablets because we have to control it is a bit difficult” (50 years old, PKPR official at the Puskesmas)
Needs of adolescents
Currently, adolescents are faced with various conditions that affect their health and well-being. Limited access to information about nutrition and health, as well as unhealthy behavior patterns, can contribute to an increased risk of stunting. Adolescent knowledge about the importance of balanced nutrition and a healthy lifestyle is crucial in preventing this problem. In addition, adolescent behavior which is often influenced by their social and cultural environment can also affect eating habits and lifestyle.
Conditions of adolescents
In an effort to reduce stunting rates, we need to pay attention to the conditions of adolescents because adolescence is a critical phase in individual development that can impact future health outcomes. The results of the FGDs and in-depth interviews conducted showed that the conditions of adolescents that need attention and can affect future health outcomes are mental health, adolescent nutrition, free association which can lead to adolescent pregnancy and early marriage as well as reproductive disorders in the future.
“Pregnancy first” (PNA, 14 years old, FGD for adolescents)
“Malnutrition” (K, 14 years old, FGD for adolescents)
Adolescent knowledge
Adolescent knowledge related to stunting prevention programs is very important, considering that they are at an age where understanding health and nutrition can affect their behavior and future generations. The informants said that adolescents do not yet have good knowledge related to adolescent nutritional needs and balanced nutrition. Adolescents also do not yet have good knowledge about reproductive health, even though with good knowledge they can prevent stunting in the future. In addition, informants said that adolescent knowledge is still low related to clean and healthy living practices, such as hand hygiene, sanitation, engaging in sports activities, and the importance of avoiding bad habits where they only wash their hands if they feel their hands are dirty. Related to adolescent pregnancy, the informants said that adolescent pregnancy occurs because of curiosity and thinking that getting married is fun.
“No need to work, the husband works” (J, 14 years old, FGD for adolescents)
“…because of pregnancy, and also because of the economy” (K, 14 years old, FGD for adolescents)
Adolescent behavior
Adolescent behavior plays a very important role in stunting prevention programs because this behavior can affect their own health and well-being, as well as the next generation. Adolescent behavior in choosing food has a major influence on nutritional intake. The results of the FGDs and in-depth interviews show that most adolescents do not practice healthy behaviors such as having breakfast every morning for various reasons, and they wash their hands only if they feel dirty. Related to balanced nutrition, they consume foods that they like but do not meet the nutritional needs of adolescents. Furthermore, the informant said that a motivation to be able to get used to healthy behavior is having a boyfriend.
“Sometimes I have breakfast, sometimes I don’t” (D, 14 years old, FGD for adolescents GD).
“No, I’m afraid of pooping” (T, 14 years old, FGD for adolescents)
“Reminder to eat, don’t forget to eat, honey ha ha …” (J, 14 years old, FGD for adolescents D)
Suggestions
As an effort to increase the effectiveness of the program, especially preventing stunting through interventions with adolescents, the government – as policymakers – and health workers – as program implementers – need to make various efforts, including innovating, conducting cross-sectoral collaboration in specific interventions, and conducting periodic and continuous program monitoring and evaluation.
Innovation
The needs and challenges faced by adolescents continue to develop along with social, economic, and technological changes. Innovation in stunting prevention programs can help adjust interventions to current conditions experienced by adolescents. Informants said that innovation can be carried out by including nutrition programs in community empowerment programs where programs that involve adolescents as agents of change can create a sense of ownership and responsibility for their own health, and inspire them to contribute to the health and well-being of the community. Informants also said that it is necessary to include a joint breakfast program to improve focus, concentration, and cognitive abilities. Informants said that adolescents who eat breakfast tend to have better academic performance.
“After exercising, we eat together but in our respective classes” (J, 14 years old, FGD for adolescents).
“If it is specifically related to nutritional intake, it is a community empowerment program that is related to nutrition” (E, 36 years old, in-depth interview with the DPMKP2KB)
“When these adolescents cannot cope, it is difficult to overcome it… we can train these teachers from us from the puskesmas, also for adolescent health interventions through educational institutions, usually teachers, because most of the time these adolescents spend is at school, so we empower them within the school environment” (TYN, 41 years old, in-depth interview with the Health Office).
Cross-sectoral cooperation
In the FGD and interviews, the informants stated that cross-sectoral cooperation is very important in improving the achievement of stunting prevention programs for adolescents because stunting is a complex issue and is influenced by various factors, including health, nutrition, education, economy, and environment. In addition, cross-sectoral cooperation allows stunting prevention programs to reach a larger proportion of the population and increase program effectiveness by combining various resources, skills, and expertise.
“All partners work hard, there are no assistants, there are also none, yes, so the concept is that from the central script, the target must be committed to these three main points, then from the assistant when there are obstacles, selection, assistance, action” (E, 36 years old, in-depth interview with the DPMKP2KB)
“Well, there must also be sacrifices from health workers outside their working hours, so then a commitment also from the government and in institutions also facilitating posyandu activities for adolescents” (TYN, 41 years old, in-depth interview with the Health Office).
Monitoring and evaluation
Monitoring and evaluation need to be carried out periodically to find out whether the program is running according to plan or requires adjustments; this is to ensure that the interventions provided are truly effective in reducing stunting rates in adolescents. According to the results of FGDs and in-depth interviews, informants conveyed the need to monitor adolescent iron consumption in schools in order to take corrective actions on the program being run. Furthermore, to increase adolescent compliance in consuming iron tablets, monitoring and evaluation can be carried out by parents, so it is considered very important to strengthen the role of parents in the success of the adolescent program and the need for character strengthening to optimize the program that is already running.
“One of the monitors that was there was a companion to drink iron tablets, this is also included in the innovation strategy” (TYN, 41 years old, in-depth interview with the Health Office).
“For example, if the puskesmas gives out iron tablets but they don’t take them but their blood increases. They are told to drink them but their parents are not there, no one reminds them” (LR, 50 years old, PKPR official at the Puskesmas)
KARUNI model design
The KARUNI model is an innovative approach to stunting prevention specifically designed for adolescents aged 12–15 years. The main focus of this model is empowering adolescents through education about nutrition, reproductive health, and clean and healthy living behavior (PHBS). This study revealed that the formulation of KARUNI model included program duration, media and sources of health information for adolescents, and methods for improving adolescent health.
Program duration
The duration of the program is very important in ensuring the effectiveness of the stunting prevention program; this is particularly so with adolescents because behavioral changes do not occur instantly, especially when related to habits that are already ingrained in everyday life. Informants said that changing or starting new habits takes between one and three months.
“One to three months” (K, 14 years old, FGD for adolescents)
Media and sources of health information for adolescents
The selection of the right media and sources of health information for adolescents is very important because what is selected will affect how adolescents understand, receive, and apply health information. The results of the study show that informants explained that media that are easily accepted by adolescents are videos and illustrated posters because they are considered more relevant and interesting to them, so they are more likely to pay attention to them. In addition, informants said that to make it easier for adolescents to access information whenever they need it, the media used should be an application.
“For example, there is an LC that can access health materials, which is interesting, so it was done in class, so it could be a healthy class for teenagers driven by the guidance and counseling teacher with the Red Cross, for example, the office provides a joint application. Just download it” (SW, 49 y.o., PKPR official at the Puskesmas)
“Using video media” (J, 14 years old, FGD for adolescents)
Methods for improving adolescent health
The selection of the right method in the stunting prevention program for adolescents is very important because the method will affect the effectiveness of the program in achieving its main goals, namely increasing knowledge, awareness, and the healthy behavior of adolescents that contribute to stunting prevention. The informants said that the method used to change behavior was using a daily activity module to guide them every time they engaged in stunting prevention behavior. Meanwhile, to increase knowledge, the method used was counseling accompanied by interactive discussions.
K: “Yes, it was given in the form of a novel”.
B: “Oh, a module,”
B: “So, if you get used to checking, it will often become a routine?”
J: “Yes”.
“Counseling” (D, 14 years old, FGD for adolescents)
Discussion
This study reveals various important aspects of the efforts to reduce the prevalence of stunting through an adolescent health approach. This study describes the active role of puskesmas (community health centers) and schools in implementing the Adolescent Health Care (PKPR) program, providing iron tablets, and various health screening activities aimed at changing adolescent behavior. The PKPR is implemented at the puskesmas level as the spearhead of adolescent health services [22], 23]. This program includes various services such as reproductive health education and health screening [23]. In addition, the formation of adolescent cadres who care about stunting is also an important strategy in efforts to prevent stunting and improve child health [11]. Various studies have shown that collaboration between puskesmas and schools is very important to implement these programs [24], 25]. However, challenges remain, including inconsistent implementation and limited resources. Routine health services for adolescents can help prevent new health problems and reduce the incidence of existing problems, such as anemia [25].
Other findings indicate that monitoring and evaluation are key elements in the success of stunting prevention programs. Evaluations are conducted regularly to monitor behavioral changes and the effectiveness of interventions, such as compliance with iron tablet consumption. However, several obstacles such as a lack of health literacy among the public and coordination between institutions are obstacles to carrying out optimal evaluations. Monitoring and evaluation are crucial elements in the success of stunting prevention programs. Routine evaluations are conducted to monitor behavioral changes and the effectiveness of interventions, such as compliance with iron tablet consumption [26]. However, several obstacles hinder optimal evaluation, including the low health literacy among the public and a lack of coordination between institutions [27], 28].
Research shows that adolescent health interventions face significant implementation challenges, including limited financial resources, lack of coordination between sectors, and inadequate human resources [29], 30]. In Ghana and India, studies have shown that many planned strategies for adolescent health are only partially implemented or not implemented at all [30], 31]. A lack of engagement with adolescent perspectives and cultural contexts also hinders effective implementation [30]. In addition, standardized measurement instruments and long-term follow-up studies are needed, especially in low- and middle-income countries [32]. To improve adolescent health programs, experts recommend a multisectoral approach, increased funding, better training for health service providers, and greater involvement of young people in policy development and implementation [29], 31].
Recent studies highlight the importance of targeted interventions for adolescents in stunting prevention programs. Media-based health education, particularly social media platforms like TikTok and Instagram, has shown effectiveness in increasing adolescents’ knowledge about stunting prevention [19]. However, addressing stunting requires a comprehensive approach that considers factors such as dietary patterns, eating disorders, and body image among adolescent girls in high-prevalence countries [33]. A multi-site Indonesian cohort study is ongoing to better understand the developmental trajectories of stunted and non-stunted adolescents, examining growth, nutrition, psychosocial wellbeing, and pubertal development [34]. These findings underscore the need for holistic, adolescent-focued strategies to combat stunting and improve overall health outcomes.
This study highlights the importance of involving adolescents in stunting prevention efforts. Adolescents can act as effective agents of change and peer educators if equipped with the appropriate knowledge and skills [35], 36]. Community service approaches involving adolescents have shown promising results in increasing awareness and commitment to reducing stunting rates [11]. Educational interventions, such as nutrition counseling training for adolescents, have shown significant improvements in their knowledge of stunting and their ability to counsel peers and mothers of young children [37].
Conclusions
This study emphasizes the importance of the approach to adolescent health in efforts to reduce the prevalence of stunting through collaboration between puskesmas and schools. The Adolescent Health Care Program (PKPR), provision of iron tablets, and health screening are key strategies in increasing awareness of nutrition and reproductive health for adolescents, especially girls. However, the implementation of this program still faces challenges, including limited resources, the need for coordination between institutions, and low health literacy among the public. Involving adolescents as agents of change – such as through training and their role as peer educators – is an important step in strengthening the effectiveness of stunting interventions and expanding their impact in the community.
Acknowledgments
Our sincere gratitude goes to Universitas Sebelas Maret for their support with the facilities and resources that made this research possible. We also thank Politeknik Kesehatan Karya Husada Yogyakarta for their cooperation and valuable contribution in providing data and guidance during the research process. Support from both institutions has been essential to the successful completion of this research manuscript.
-
Research ethics: This study adheres to the principles of research ethics, especially those involving adolescents as research subjects. Before the study was conducted, permission was obtained from the research ethics committee (No.1.538/VI/HREC/2024). In addition, the participants and parents or guardians were given a written consent form explaining the purpose, procedures, and the participant’s right to withdraw at any time during the study. The confidentiality of each participant’s identity was maintained by using an anonymous code in presenting the research results.
-
Informed consent: Informed consent was obtained from all individuals included in this study, or their legal guardians or wards.
-
Author contributions: Conception and design: BK, FB, DU. Data analysis and interpretation: BK. Drafting of the article: BK, FB. Critical revision of the article for important intellectual content: SHR, SM. Final approval of the article: BK, FB, SHR, SM. Data collection and assembly: BK. The authors have accepted responsibility for the entire content of this manuscript and approved its submission.
-
Use of Large Language Models, AI and Machine Learning Tools: None declared.
-
Conflict of interest: The authors declare that there is no conflict of interest.
-
Research funding: None declared.
-
Data availability: Not applicable.
References
1. Mursalins, l, Siahaan, AHI, Saputera, Wahid, A, Dermawan, Z, Bassa, N, et al.. Pelaksanaan program investing in nutrition and early years (INEY) dalam mendukung percepatan penurunan stunting Tahun 2018–2023. Laporan Akhir 2024.Suche in Google Scholar
2. Bhan, N. Preventing teenage pregnancy in India to end the cycle of undernutrition. Lancet Child Adolesc Health 2019;3:439–40. https://doi.org/10.1016/S2352-4642(19)30111-7.Suche in Google Scholar PubMed
3. Nugraheni, R. Program edukasi gizi pada remaja putri untuk mencegah stunting: tinjauan literatur nutrition education program for adolescent girls to prevent stunting: literature review. Jurnal Promotif Preventif 2024;7:569–77.Suche in Google Scholar
4. Onis, D, BrancMercedesa, F. Childhood stunting: a global perspective. Matern Child Nutr 2016;12:12–26. https://doi.org/10.1111/mcn.12231.Suche in Google Scholar PubMed PubMed Central
5. Mistry, SK, Hossain, MB, Arora, A. Maternal nutrition counselling is associated with reduced stunting prevalence and improved feeding practices in early childhood: a post-program comparison study. Nutr J 2019;18:1–9. https://doi.org/10.1186/s12937-019-0473-z.Suche in Google Scholar PubMed PubMed Central
6. Jusliani, J, Syamsuddin, S. Tinjauan efektivitas intervensi gizi terhadap stunting dan masalah gizi pada anak balita. Jurnal Riset Sains dan Kesehatan Indonesia 2024;1:124–9. https://doi.org/10.69930/jrski.v1i3.156.Suche in Google Scholar
7. Mideksa, S, Getachew, T, Bogale, F, Woldie, E, Ararso, D, Samuel, A, et al.. School feeding in Ethiopia: a scoping review. BMC Publ Health 2024;24:1–13. https://doi.org/10.1186/s12889-023-17613-4.Suche in Google Scholar PubMed PubMed Central
8. WHO. Nutrition action in schools: a review of the evidence related to the nutrition-friendly schools initiative. Switzerland: © World Health Organization 2020; 2020.Suche in Google Scholar
9. Gosdin, L, Sharma, AJ, Tripp, K, Amoaful, EF, Mahama, AB, Selenje, L, et al.. A school-based weekly iron and folic acid supplementation program effectively reduces anemia in a prospective cohort of ghanaian adolescent girls. J Nutr 2021;151:1646–55. https://doi.org/10.1093/jn/nxab024.Suche in Google Scholar PubMed PubMed Central
10. Davoudi-Kiakalayeh, A, Mohammadi, R, Pourfathollah, AA, Siery, Z, Davoudi-Kiakalayeh, S. Alloimmunization in thalassemia patients: new insight for healthcare. Int J Prev Med 2017;8:66–9. https://doi.org/10.4103/ijpvm.IJPVM.Suche in Google Scholar
11. Amalia, L, Mokodompis, Y, Hiola, F. Pembentukan kader remaja peduli stunting dalam upaya penanggulangan masalah gizi pada balita. Jurnal Pengabdian Masyarakat Farmasi: Pharmacare Society 2023;2:178–83. https://doi.org/10.37905/phar.soc.v2i3.22011.Suche in Google Scholar
12. Badan Kebijakan Pembangunan Kesehatan. Survei Kesehatan Indonesia (SKI) dalam Angka: Data akurat Kebijakan Tepat. Survei Kesehatan Indonesia Tahun 2023 2023;235.Suche in Google Scholar
13. van Leer, E. Enhancing adherence to voice therapy via social cognitive strategies. Semin Speech Lang 2021;42:019–31. https://doi.org/10.1055/s-0040-1722755.Suche in Google Scholar PubMed
14. Sulastiyo, A. Pengaruh edukasi dengan daily meal tracker terhadap perubahan pengetahuan & sikap remaja usia 13–16 tahun. Jurnal Riset Gizi 2022;10. https://doi.org/10.31983/jrg.v10i1.8091.Suche in Google Scholar
15. Sumarwati, M, Mulyono, WA, Nani, D, Swasti, KG, Abdilah, HA. Pendidikan kesehatan tentang gaya hidup sehat pada remaja tahap akhir. Jurnal Abdimas BSI: Jurnal Pengabdian Kepada Masyarakat 2022;5:36–48. https://doi.org/10.31294/jabdimas.v5i1.11354.Suche in Google Scholar
16. Hikmah, H, Musa, SM. Gaya hidup sehat remaja dengan pendekatan edukatif dan komunikatif. Prosiding Simposium Nasional Multidisiplin (SinaMu) 2022;3. https://doi.org/10.31000/sinamu.v3i0.6001.Suche in Google Scholar
17. Murdiningrum, S, Handayani, H. Efektifitas media edukasi gizi untuk peningkatan pengetahuan gizi remaja. Jurnal Mahasiswa BK An-Nur: Berbeda, Bermakna, Mulia 2021;7:53. https://doi.org/10.31602/jmbkan.v7i3.5759.Suche in Google Scholar
18. Margatot, DI, Huriah, T. The effectiveness of women empowerment in preventing stunting in children aged 6–59 months. Bali Med J 2021;10:1230–4. https://doi.org/10.15562/bmj.v10i3.2852.Suche in Google Scholar
19. Marlinawati, DA, Rahfiludin, MZ, Mustofa, SB. Effectiveness of media-based health education on stunting prevention in adolescents: a systematic review. AgriHealth: J Agri-food, Nutr Public Health 2023;4:102. https://doi.org/10.20961/agrihealth.v4i2.71357.Suche in Google Scholar
20. Erfina, E, Hariati, S, Tawali, S. Development and evaluation of nursing intervention in preventing stunting in children of adolescent mothers: a mixed-methods research protocol. Nutr Health 2023;29:369–75. https://doi.org/10.1177/02601060231181712.Suche in Google Scholar PubMed
21. Baroroh, I. Peningkatan pengetahuan tentang pemenuhan gizi remaja dan edukasi pencegahan stunting. Jurnal ABDIMAS-HIP Pengabdian Kepada Masyarakat 2022;3:60–4. https://doi.org/10.37402/abdimaship.vol3.iss2.194.Suche in Google Scholar
22. Agustini, NNM, Arsani, NLKA. Remaja sehat melalui pelayanan kesehatan peduli remaja di tingkat puskesmas. Jurnal Kesehatan Masyarakat [Internet] 2013;9:66–73.Suche in Google Scholar
23. Kadek Alit Arsani, NL. Peranan program pkpr (pelayanan kesehatan peduli remaja) terhadap kesehatan reproduksi remaja di kecamatan buleleng. Jurnal Ilmu Sosial dan Humaniora 2013;2. https://doi.org/10.23887/jish-undiksha.v2i1.1289.Suche in Google Scholar
24. Fitriani, L, Wahyuni, S. Peningkatan pengetahuan dan kepatuhan remaja putri melalui pemberian pendidikan kesehatan tentang mengkomsumsi tablet Fe. SIPISSANGNGI. Jurnal Pengabdian Kepada Masyarakat 2022;2:54. https://doi.org/10.35329/sipissangngi.v2i1.2783.Suche in Google Scholar
25. Agustina, AN, Dewi, SU, Rahayu, HS, Mahardika, P. Upaya menurunkan kejadian anemia melalui program pelayanan kesehatan peduli remaja. GEMAKES: Jurnal Pengabdian Kepada Masyarakat 2024;4:120–8. https://doi.org/10.36082/gemakes.v4i1.1513.Suche in Google Scholar
26. Rustiawan, A, Pratiwi, A. Evaluasi program pemberian tablet tambah darah pada ibu hamil di puskesmas gedongtengen. Abdi Geomedisains 2022:61–71. https://doi.org/10.23917/abdigeomedisains.v2i2.313.Suche in Google Scholar
27. Sari, DP, Yusran, R. Evaluasi kebijakan pencegahan stunting di nagari pulakek koto baru kecamatan sungai pagu kabupaten solok selatan. J Civic Edu 2022;5:90–100. https://doi.org/10.24036/jce.v5i1.661.Suche in Google Scholar
28. Putra, A, Fitri, Y. Studi meta analisis: efektifitas pencegahan stunting melalui program literasi gizi menggunakan pendekatan pendidikan keluarga. Jurnal Obor Penmas: Pendidikan Luar Sekolah 2021;4:1–10. https://doi.org/10.32832/oborpenmas.v4i1.4727.Suche in Google Scholar
29. Roy, K, Shinde, S, Sarkar, BK, Malik, K, Parikh, R, Patel, V. India’s response to adolescent mental health: a policy review and stakeholder analysis. Soc Psychiatr Psychiatr Epidemiol 2019;54:405–14. https://doi.org/10.1007/s00127-018-1647-2.Suche in Google Scholar PubMed PubMed Central
30. Agblevor, EA, Darko, NA, Acquah, PA, Addom, S, Mirzoev, T, Agyepong, IA. “We have nice policies but…”: implementation gaps in the Ghana adolescent health service policy and strategy (2016–2020). Front Public Health 2023;11. https://doi.org/10.3389/fpubh.2023.1198150.Suche in Google Scholar PubMed PubMed Central
31. Barua, A, Watson, K, Plesons, M, Chandra-Mouli, V, Sharma, K. Adolescent health programming in India: a rapid review. Reprod Health 2020;17:87. https://doi.org/10.1186/s12978-020-00929-4.Suche in Google Scholar PubMed PubMed Central
32. Salam, RA, Das, JK, Lassi, ZS, Bhutta, ZA. Adolescent health interventions: conclusions, evidence gaps, and research priorities. J Adolesc Health 2016;59:S88–92. https://doi.org/10.1016/j.jadohealth.2016.05.006.Suche in Google Scholar PubMed PubMed Central
33. Setiawan, AS, Budiarto, A, Indriyanti, R. Eating behavior of adolescent girls in countries with a high prevalence of stunting under five: a systematic review. Front Psychol 2023;14. https://doi.org/10.3389/fpsyg.2023.1228413.Suche in Google Scholar PubMed PubMed Central
34. Medise, BE, Julia, M, Devaera, Y, Sitaresmi, MN, Asmarinah, WNA, Kalalo, RT, et al.. Understanding the pubertal, psychosocial, and cognitive developmental trajectories of stunted and non-stunted adolescents: protocol of a multi-site Indonesian cohort study. Front Pediatr 2024;12. https://doi.org/10.3389/fped.2024.1296128.Suche in Google Scholar PubMed PubMed Central
35. Wandini, K, Angesti, AN. Peran remaja dalam pencegahan stunting (kepedulian remaja investasi generasi). Jurnal Pemberdayaan Komunitas MH Thamrin 2023;5:15–21. https://doi.org/10.37012/jpkmht.v5i1.1368.Suche in Google Scholar
36. Mitra, N, Rahmalisa, U. Program kemitraaan masyarakat pembinaan satuan tugas peduli stunting remaja sebagai agen perubahan melalui informasi digital. J-ABDI: Jurnal Pengabdian kepada Masyarakat 2022;2:5045–52. https://doi.org/10.53625/jabdi.v2i5.3595.Suche in Google Scholar
37. Wagustina, S, Arnisam, A, Mulyani, NS, Hadi, A, Fitriyaningsih, E. Penguatan percepatan penurunan stunting melalui pemberdayaan remaja peduli stunting. Jurnal PADE: Pengabdian & Edukasi 2024;6:39. https://doi.org/10.30867/pade.v6i1.1788.Suche in Google Scholar
© 2025 the author(s), published by De Gruyter, Berlin/Boston
This work is licensed under the Creative Commons Attribution 4.0 International License.
Artikel in diesem Heft
- Frontmatter
- Original Articles
- Evaluating the relationship between marijuana use, aggressive behaviors, and victimization: an epidemiological study in colombian adolescents
- Enhancing adolescent health awareness: impact of online training on medical and community health officers in Andhra Pradesh, India
- Development of the “KARUNI” (young adolescents community) model to prevent stunting: a phenomenological study on adolescents in Gunungkidul regency, Yogyakarta, Indonesia
- Energy drinks, depression, insomnia, and stress in palestinian adolescents: a cross-sectional study
- Characterization of the most common diagnoses in a population of adolescents and young adults attended by a Healthcare Service Provider (HSP) in Bogotá, Colombia
- Association of chronotype pattern on the quality of sleep and anxiety among medical undergraduates – a cross-sectional study
- Addressing emotional aggression in Thai adolescents: evaluating the P-positive program using EQ metric
Artikel in diesem Heft
- Frontmatter
- Original Articles
- Evaluating the relationship between marijuana use, aggressive behaviors, and victimization: an epidemiological study in colombian adolescents
- Enhancing adolescent health awareness: impact of online training on medical and community health officers in Andhra Pradesh, India
- Development of the “KARUNI” (young adolescents community) model to prevent stunting: a phenomenological study on adolescents in Gunungkidul regency, Yogyakarta, Indonesia
- Energy drinks, depression, insomnia, and stress in palestinian adolescents: a cross-sectional study
- Characterization of the most common diagnoses in a population of adolescents and young adults attended by a Healthcare Service Provider (HSP) in Bogotá, Colombia
- Association of chronotype pattern on the quality of sleep and anxiety among medical undergraduates – a cross-sectional study
- Addressing emotional aggression in Thai adolescents: evaluating the P-positive program using EQ metric