Translational radionanomedicine: a clinical perspective
-
Hongyoon Choi
Hongyoon Choi recieved his MD degree (2010) and PhD degree (2014) from Seoul National University. He completed a 4-year residency program at the Department of Nuclear Medicine, Seoul National University Hospital and recieved Board of Nuclear Medicine accreditation in 2015. He currently serves as a public health doctor, a mandatory alternative service. He won the Young Medical Scientist Award of the Seoul Medical Association in 2015. His research is focused on the development of imaging biomarkers and theragnosis for cancer as well as brain disorders. His interests include preclinical and clinical research for innovative diagnostic and therapeutic approaches.
Yun-Sang Lee is the Brain Korea 21 plus (BK21 plus) Associate Professor in the Department of Molecular Medicine and Biopharmaceutical Sciences, Graduate School of Convergence Science and Technology at Seoul National University. He received his BS and MS from the Department of Chemistry, College of Sciences at Kyunghee University, Korea in 1996 and 1998, and his PhD from the Department of Pharmaceutical Manufacturing Chemistry, College of Pharmacy at Seoul National University, Korea in 2006, respectively. He is interested in the field of development and implementation of new methods for radiolabeling chemistry and the development of new diagnostic or therapeutic radiopharmaceuticals, and also, the development of new methods for the surface modification or radiolabeling of nano-materials, especially radionanomedicine, and their uses for diagnosis/therapy or theranostics.
Do Won Hwang recieved his PhD degree in “Program in Neuroscience” in 2009 from Seoul National University. He is currently the Brain Korea 21 plus (BK21 plus) Associate Professor in the Department of Molecular Medicine and Biopharmaceutical Sciences, Graduate School of Convergence Science and Technology at Seoul National University. He recieved an achievement award in the field of radio-nanotechnology in 2015. His research interests focus on the development of multifunctional nanomaterials for disease theranostics, stem cell imaging in regenerative medicine, non-coding RNA monitoring.
Dong Soo Lee is a nuclear medicine physician and Professor in Nuclear Medicine in at Seoul National University (SNU) and SNU Hospital since 1990. He is also Professor and Chairman of Molecular Medicine and Biopharmaceutical Sciences. He is also Director of Bio-MAX/N-Bio which is the Biotechnology Research Institute of SNU. He founded and was the first President of the Korean Society for Nanomedicine in 2012. His major interest is radionanomedicine, which is the combination of nuclear medicine and nanomedicine.


Abstract
Many nanomaterials were developed for the anticipated in vivo theranostic use exploiting their unique characteristics as a multifunctional platform. Nevertheless, only a few nanomaterials are under investigation for human use, most of which have not entered clinical trials yet. Radionanomedicine, a convergent discipline of radiotracer technology and use of nanomaterials in vivo, can facilitate clinical nanomedicine because of its advantages of radionuclide imaging and internal radiation therapy. In this review, we focuse on how radionanomedicine would impact profoundly on clinical translation of nanomaterial theranostics. Up-to-date advances and future challenges are critically reviewed regarding the issues of how to radiolabel and engineer radionanomaterials, in vivo behavior tracing of radionanomaterials and then the desired clinical radiation dosimetry. Radiolabeled extracellular vesicles were further discussed as endogenous nanomaterials radiolabeled for possible clinical use.
Introduction
Medical application has been an emerging field of nanomaterials. Nanomaterials can play a role as a multifunctional platform in medical application due to their unique characteristics as sensors and effectors. As a future medicine, nanomedicine is expected to be widely applied as in vitro nanosensor diagnostics, molecular nanoimaging or targeted nanodelivery for in vivo use and nano-tissue engineering for regenerative medicine. Among them, nanomedicine for diagnostic imaging and targeted therapy is an in vivo technology which is eventually hoped to be used in humans for various purposes. Because nanomaterials are sufficiently small to cross biological barriers including vessel walls and cell membranes, they can interact with biomaterials. Furthermore, they can be designed and modified to exhibit proper physicochemical and biological features for in vivo use. Thus, developing nanomaterials as ‘guided missiles’ which targeted specific cells and deliver drugs efficiently for diagnosis and therapy has received much attention (1). However, due to their possible toxicity and uncertainty of biological behaviors, they have limitations in human application and clinical trials are slowed down (2, 3). Even if an engineered nanomaterial has proper molecular targets and no cytotoxicity in vitro, in vivo distribution, metabolism and excretion is much more complex, which becomes a bottleneck to its entering clinical trials (4). Although more than 200 nanomedicine products have been in clinical trials or even approved (2), eventual success in clinical therapeutics is still uncertain. A feasible breakthrough for future clinical application of nanomaterials may come from radionanomedicine, an approach for clinical translation using radiolabeled nanomaterials (5–7).
The core concept of radionanomedicine lies in using ‘trace’ amounts of multifunctional radiolabeled nanoparticles for in vivo theranostic purposes. Radionanomedicine is one of the clinically feasible theragnostic approaches which combine diagnosis and therapy by a unified material to develop personalized treatment for various diseases (8). From a broad perspective, radiolabeled nanoparticles had already been used in the clinical setting as an established medical practice. For example, radiolabeled nanocolloids were used in liver scans, bone marrow scans as well as lymphoscintigraphy in nuclear medicine (9, 10). These imaging techniques rely only on the size-dependent in vivo distribution or lymphatic clearance of radionanocolloids. On the other hand, recently developed radiolabeled nanoparticles are engineered to target specific molecules of cells or to have specific capability for delivering drugs which enable both diagnosis and therapy. It is radionanomedicine in a narrow sense which includes in vivo application of nanoparticles as a multifunctional platform for monitoring in vivo behavior of nanoparticles and for looking for therapeutic effects on target tissues using therapeutic radionuclides, so-called, internal radiotherapy.
In this review, we explained how radionanomedicine would facilitate clinical application of nanoparticle-based theranostics. As a multifunctional nano-platform, recent advances of modification for radiolabeling are reviewed. In vivo behavior of nanoparticles in the light of radionanomedicine is critically reviewed. For clinical application, radiation internal dosimetry particularly for nanoparticles is discussed. As one of the clinically feasible nanomaterials, endogeneous nanoparticles are further discussed as a specific example.
Radionanomedicine facilitates clinical nanomedicine
Trace amounts of nanomaterials for safety
The safety concern is a critical issue in clinical application of nanomaterials. Although the safety concern is common in other drugs, it is more complex in nanomedicine due to various mechanisms of toxicity and variety of nanoparticles (11). Cellular and subcellular interactions of nanoparticles which can cross biological membranes induce toxic effects. Innate immune responses of cells increase reactive oxygen species (ROS), which resulted in cellular damage (12). Phagocyotosis of metal oxide nanoparticles induces oxidative stress to autocatalzye ROS formation which is followed by cytokine production (12). Oxidative stress induced by nanoparticles can affect DNA damage, cell growth, subcellular signaling and eventually carcinogenesis (13). As another mechanism, nanoparticles are often associated with lysosomal dysfunction. Nanoparticles with positive zeta potential sequester protons which results in excessive activation of the proton pump and osmotic rupture of lysosomes (14). ROS generation followed by cellular signaling cascades associated with inorganic nanomaterials such as quantum dots are dependent on bodily response to toxic materials themselves (15). Biocompatible metallic nanomaterials such as gold also have concerns of cellular and systemic toxicity due to surface ligands and/or the accompanying phagocytic immune responses (16, 17). Moreover, plausible in vivo toxicity of biomaterial nanomaterials such as cationic micelles and liposomes has been addressed in the literature (18). Thus, various nanoparticles could have possible mechanisms of toxicity which are dependent on chemical composition, size, shape and surface molecules of nanoparticles (11). However, one of the most important factors of nanotoxicity is the dose of nanoparticles (13). In vivo toxicity and pharmacologic effects of nanomaterials are dose dependent. Radionanomedicine uses traceable amounts of nanomaterials, much less than pharmacologic amounts. Therefore, in vivo effects of traceable amounts of radiolabeled nanomaterials are not dependent on physicochemical features of nanomaterials themselves. This concept follows the principle of nuclear medicine. Several diagnostic radiopharmaceuticals widely used for patients in nuclear medicine have no pharmacologic effects due to the usual usage of sub-pharmacologic dose of very small amounts. This implies that radiolabeled nanomaterials can even be used in the clinical setting though nanomaterials have concerns of toxicity.
In vivo monitoring of nanoparticles to facilitate clinical trials
Radionanomedicine can elucidate the in vivo fate of nanomaterials. Nuclear imaging of radiolabeled nanomaterials is sensitive to detect the whereabouts of administered nanomaterials in the body. The distribution study of nanomaterials can provide important information for clinical translation of nanomaterials. Firstly, in vivo monitoring elucidates whether engineered nanomaterials properly target the specific tissues such as cancer. Because nuclear imaging modalities are minimally invasive and the allowed quantification even in the deep organs in human, they can be easily translated from small animal experiments to human trials. For instance, silica nanoparticle designed for targeting αvβ3 integrin with 124I and optical probes were experimented in small animal tumor models, which achieved tumor targeting and efficient renal clearance (19). This nanoparticles received U.S. Food and Drug Administration (FDA) approval and a clinical trial was performed, which also showed accumulation of nanoparticles in tumor lesions (20).
Secondly, positron emission tomography (PET) or single photon emission computed tomography (SPECT) provide pharmacokinetics which is a temporal pattern of the whereabouts of nanomaterials in living organisms. This pharmacokinetic information facilitates the development of clinically applicable nanomaterials. Engineering and surface modification of nanomaterials affect in vivo behavior (21, 22), thus, radionanomedicine helps to find optimal modification methods for biomedical application. The most commonly used surface modification is introduction of polyethylene glycol (PEG) to reduce opsonin protein binding in blood. This process could significantly reduce RES sequestration and increased tumor accumulation (21, 23). Size of particles as well as surface modification also affects the pharmacokinetics of nanoparticles. Small sized quantum dots are prone to be excreted by the kidneys which could result in a higher lesion-to-background accumulation ratio (24). PET and SPECT imaging could facilitate selecting clinically appropriate engineered nanoparticles which show high target lesion uptake, minimal accumulation and rapid clearance in critical normal organs.
In addition, excretion patterns and physiologic accumulation of nanomaterials explain a plausible toxicity when pharmacologic amounts of nanomaterials are used. For instance, nanomaterials quickly excreted from the body may have less systemic toxicity than those remaining in the body for a long time. A large amount of nanoparticles distributed to normal organs might cause toxicity. A nanoparticle mainly excreted by the hepatobiliary system might increase in serum concentration when hepatic functions are deteriorated (17). Therefore, in vivo kinetics of radiolabeled nanoparticles could explain possible types of toxicity by analogy with preclinical imaging.
The monitoring of in vivo kinetics of very low-dose nanoparticles could enable phase 0 clinical trials. The phase 0 trial is a platform for target modulation and proper target selection for new drug developments in human evaluating biomarkers for drug effects and pharmacokinetics (25). The phase 0 trial eventually reduces costs of the clinical trials and boosts the development. Sub-pharmacologic doses of radiolabeled drugs have been used in phase 0 trials for other drug developments which help in making an early selection of promising candidates for further clinical trials (26, 27). In particular, as biological interactions of nanoparticles are varied according to the engineering and modification of them, they are more complicated and relatively unpredictable compared with macromolecular conventional drugs. Radiolabeled nanoparticles could have an important role in phase 0 trials to facilitate rational drug selection and identify possible toxicity and therapeutic effects eventually to reduce timelines for clinical application. To accelerate phase 0 trials for radionanomedicine, pharmacokinetic modeling based on physiology of nanomaterials will be urgently needed.
Theranostic approach using radiolabeled nanoparticles
Radionanomedicine based on the target-specific delivery of radionuclides for diagnosis and therapy could be a next-generation of molecular theranostics. As radiolabeling can facilitate clinical application of nanomaterials, unique characteristics of nanomaterials may reinforce radionuclide theranostics. The principle of target-specific radionuclide theranostics is derived from nuclear medicine therapy. Classically used 131I for thyroid cancer is the best example, which enables both internal radiotherapy for thyroid cancer tissues and post-therapy scans to find residual thyroid tissues of metastasis (28). Another example is radioimmunotherapy, such as 90Y-ibritumomab tiuxetan (Zevalin) for non-Hodgkin’s lymphoma (29). Therapeutic radionuclides can be combined with a monoclonal antibody and molecular target-specific therapy. These radiolabeled macromolecules are promising theranostic materials though some radionuclides such as 90Y and 177Lu have limitations in image-based monitoring. Another clinically available theranostic approach is radiomicrosphere therapy using 90Y microspheres. As tumor blood supply is mostly derived from the hepatic artery, microspheres labeled with therapeutic radionuclides administered to the hepatic artery could target the tumor tissue with a high tumor-to-normal liver ratio. For a therapeutic plan as a theranostic approach, 99mTc-labeled macroaggregated albumin is clinically used for SPECT imaging as a surrogate for the distribution of microspheres (30). Commercially available products such as resin (SIR-Spheres®, Sirtex Medical Limited, Australia) and glass (TheraSphere®, MDS Nordion, Ottawa, Canada) microspheres have been clinically used in hepatic metastases (31, 32) and hepatocellular carcionoma (33, 34). These clinically available radiolabeled molecules or microspheres might be extended to theranostic approaches of radiolabeled nanoparticles.
The nanoparticles could be labeled with radionuclides according to the purposes, such as for imaging, kinetics or for therapy, by only changing types of radionuclides. For instance, PEGylated liposomes with a chelator, DTPA, could be labeled with 99mTc for SPECT imaging, 68Ga for PET imaging and 177Lu for therapeutic purposes (35). Therapeutic radiolabeled nanoparticles could be not only intravenously injected but also directly delivered to target lesions. The image-guided theranostic approach using radiolabeled nanoparticles achieved by intratumoral administration resulted in high radiation dose delivery to the tumor tissues (36). Furthermore, simultaneous imaging and delivery could be an example of theranostic approach of radiolabeled nanoparticles as nanoparticles loaded drugs rather than therapeutic radionuclides. Nanocarriers for simultaneous drug delivery and imaging such as biocompatible mesoporous silica labeled with 64Cu could be applied to a image-guided drug delivery system (37). Recently developed nanocarriers could selectively release drugs or be activated in accordance with external environments for effective treatment. Such system using a gold nanorod as a multifunctional platform could be labeled with PET agents to realize a combination of chemotherapy, photothermal therapy and PET imaging (38).
Recent evidence of tumor heterogeneity implied that we might need multiple molecular targets and ligands for successful cancer therapy (39, 40). Nanomaterials can provide multifunctional platforms for radiolabeling which enables simultaneous imaging and therapy against the multiplexed targets for proper personalized combined internal radiotherapy. Using the recent one-step surface modification for nanomaterials to have multiple functions, nanomaterials can simultaneously possess multiple targeting ligands and multiple radioisotopes labeled for diagnostic and therapeutic purposes (7, 41). The multifunctionality and flexibility of radiolabeled nanomaterials will promote the radionuclide theranostics.
Approaches for clinical radionanomedicine
Radiolabeling for clinical translation
Exogenous nanomaterials for radionanomedicine generally consist of specific functional nanoparticles, radionuclides combined with or without chelators and surface ligands for specific biological targets. Generally, two different strategies can be considered for radiolabelling. Radionuclides can be extrinsically labeled with chelators on the surfaces or intrinsically labeled within the nanomaterials (42, 43). Intrinsic radiolabeled nanoparticles are limited to the nanoparticles which can be generated by radionuclides. For instance, quantum dots which consist of Cd can have intrinsic radioactivity when they are produced using radioisotopes, 109Cd (44). Also, the integration of 64Cu into CdSe/ZnS quantum dots through cation-exchange reaction yielded self-illuminating quantum dots, and 64Cu-doped quantum dots with intrinsic radioactivity showed effective tumor targeting in an animal xenograft model (45). These types of nanoparticles have advantages in in vivo study because the intrinsically radiolabeled nanoparticles have the same physicochemical properties with unlabeled nanoparticles. Note that only small fractions of nanoparticles are radiolabeled for imaging or therapeutic approaches. However, most of the nanoparticles other than these examples do not allow radiolabeling with intrinsic radioisotopes. Extrinsic radiolabeling is achieved by chemical binding of chelators on the surface of the nanomaterials or by physical encapsulation with lipophilic chelators. Encapsulation of radiotracer has been classically studied, particularly in liposomes, using gamma-emitters of 99mTc or 111In combined with their chelators (46–49) or using positron-emitters of 124I and 18F attached to lipid molecules for membrane labeling (50, 51). Extrinsic radiolabeling on the surfaces of nanomaterials can be used, ranging from inorganic nanomaterials such as gold nanoparticles or quantum dots to organic nanoparticles including liposomes (42, 52). Extrinsic radiolabeling is commonly used for nanoparticles ranged from inorganic to organic nanoparticles. In particular, chelators covalently linked to nanoparticles are flexibly used for various purposes by changing isotopes (42, 53).
For clinical translation of radiolabeled nanoparticles, there are several concerns regarding selection of radioisotopes. In preclinical experiments, in vivo kinetics and imaging of the radiolabeled nanoparticles is studied in small animals. Toxicity of nanoparticles aside, there is a trade-off to choose radionuclides between their imaging capability and their radiation dose for their later human application. Nanoparticles should be matched with proper radionuclides for extrinsic labeling to suit their purpose of further dosimetry as well as imaging capability. One of the most commonly used radiotracer, 99mTc, has a physical 6 h half-life, but the active targeting mediated by functional biomolecules on those engineered nanoparticles can take longer than several hours. To detect actively targeted accumulation in specific tissues, radioisotopes with long half-lives are required. Long-term delayed images shall reveal the excretion pattern and plausible in vivo metabolism of nanoparticles. For example, 141Ce-labeled cerium oxide nanoparticles (half-life 32.5 days) were accumulated in the liver and spleen, but the liver slowly excreted these nanoparticles via intestines in 6 days (54). 111In-labeled HER-2 targeted gold nanoparticles (half-life 2.8 days) were slowly accumulated in the tumor lesions in more than 2 days (55). Because of this delayed target accumulation and excretion, long half-life radiotracers such as 67Ga, 89Zr, or 124I have advantages in distribution studies. Nevertheless, because long half-life increases radiation dose, radionuclides should be selected carefully. If radiolabeled nanoparticles are supposed to be used for diagnostic imaging, radionuclides should be selected considering clinically acceptable radiation doses.
Modification strategy for clinical application
Most nanoparticles in biomedical research have been delivered to the specific targets of cancer and inflammation. The accumulation of nanoparticles was dependent on two different mechanisms, ‘passive targeting’ and ‘active targeting’. Passive targeting is a result of enhanced permeability and retention (EPR). Leakage in inflammation or cancer tissues facilitates the accumulation of nano-sized materials in these lesions (56). Though nanoparticles accumulate effectively in most cancer tissues according to this EPR effect, passive targeting is limited to assure the delivery of therapeutic nanoparticles because tumor is heterogeneous and contains hypoperfused regions where nanoparticles can hardly reach and be accumulated (57). Theranostic nanoparticles have been engineered to have multiplexed targeting ligands on their surfaces to enable active targeting. Most commonly used bioactive molecules are monoclonal antibodies (58). However, antibodies are limited because the relatively large size of antibodies shall increase the diameters of nanoparticles and also the immunogenicity of these nanoparticles (34). Antigen binding proteins, part of monoclonal antibody, and single chain fragments are preferred for surface modification for active targeting due to the higher targeting efficacy with lower immunogenicity (59). And recently, affibodies, aptamers, engineered peptides and small proteins are favored for active targeting. Small molecules are also the favored candidates as the ligands for active targeting because of their ease of conjugation and low immunogenicity (60). Despite the active process of targeting, the real specificity of the uptake of nanoparticles mainly depends on the bioavailability in addition to the ligand-target specificity. As it is difficult for most nanoparticles to escape from the opsonization and the phagocytosis, which is discussed in the later part of this review, nanoparticles should be modified to increase bioavailability for successful active targeting (61).
To overcome the complexity of surface modification and radiolabeling of nanoparticles, we need to develop simple and appropriate procedures. Nanoparticles can be designed for active targeting, radiolabeled for imaging and modified for increased bioavailability. Because of diverse types of modification for nanoparticles, in vivo behavior of them should be tested and favorable candidates would be selected for further clinical translation. As an example of nanoparticles for tumor targeting, nanoparticles should be highly accumulated in the tumor and rapidly excreted from the other organs to reduce the possible toxicity. Nanocarrier systems should effectively deliver and release drugs to the target area (37). Because in vivo kinetics and targeting properties according to such process can be visualized by radiolabeling, various types of engineering such as different active targeting ligands (e.g. RGD peptides) should be tested. Recently, a quick and simple modification method to achieve multifunctionality was developed (41). ‘Jeong’s method’ can make the most metallic or metal-oxide nanoparticles with hydrophobic surface to hydrophilic and give the multifunctionality in one-step (Figure 1). The beauty of Jeong’s method is the simplicity of the procedure, i.e. mixing of the functionalized micelle and hydrophobic nanoparticles followed by gel filtration after vortexing. The total modification time would be <2 h including size exclusion chromatography. In addition, the functionalized nanoparticles modified by this approach can have a monodispersed size-distribution even after the whole modification and radiolabeling step (62). Such a process helps in vivo tests of nanoparticles to select candidates for further clinical translation which show a high lesion-to-normal organ concentration ratio and appropriate targets. We expect the convenience and robustness of this approach will contribute and boost the translational research of nanomedicine.
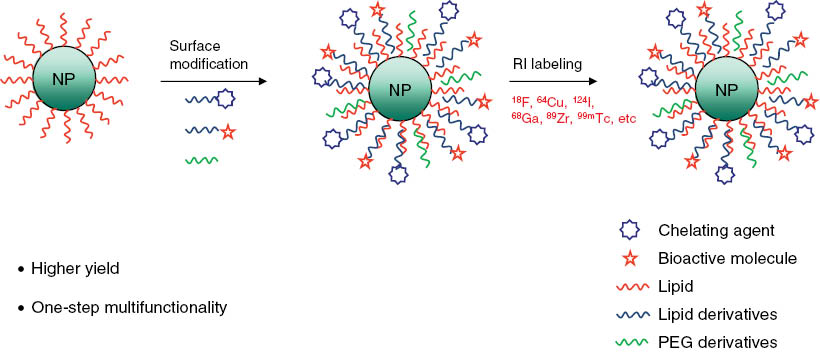
The one-step method for multifunctional nanoparticle.
Clinical translation of radionanomedicine needs quick and simple methods for modification of nanoparticles. Radiolabeled multifunctional nanoparticles can be prepared by simply mixing functionalized micelles and hydrophobic nanoparticles. The modification is followed by radiolabeling. This approach facilitates clinical application as various modified nanoparticles can be tested in vivo and proper candidates for further clinical trial can be selected.
Issues of in vivo behavior investigated by radionanomedicine
A key advantage of radionanomedicine lies in its capability to quantitatively examine in vivo distribution of nanoparticles. In vivo distribution assessed by PET or SPECT imaging provides crucial information of the where-abouts of nanoparticles, prediction of toxicity, dosimetry for specific tissues and excretion patterns (63). Fluorescence imaging of nanoparticles themselves (e.g. quantum dots) or labeled dyes onto the nanoparticles is an easy and simple way to detect in vivo distribution of these nanoparticles. However, this optical imaging is not suitable for human application due to the limited penetration depth as well as the inherent toxicity of the nanoparticles. Serial imaging is possible with radiolabeled nanoparticles even for the organs deep in humans, which allows further quantitative analysis. In spite of the strength of radiolabeled nanoparticles for in vivo tracking, there are several potential pitfalls for clinical translation of radiolabeled nanoparticles.
In vivo distribution and targeting properties are affected by physicochemical factors of radiolabeled nanoparticles. The factors controlling kinetics of nanoparticles were reviewed comprehensively by Moghimi et al. (64). Size and shape of nanoparticles are major factors which influence the clearance, phagocytosis and duration of circulation (64, 65). Particle geometry and surface charge affect the cellular internalization mediated by endocytosis. For instance, non-spherically shaped and positively charged particles let the nanoparticles to be internalized easily (66, 67). Several biological factors as well as these physicochemical properties also affect in vivo distribution. The influence of biological factors on the distribution pattern is so complex that animal studies hardly warrant immediate clinical translation. Several biochemical reactions take place following in vivo administration of nanoparticles, which differ between animals and humans. This is also the case with radiolabeled nanoparticles. Once nanoparticles are administered in body fluids, they will encounter various molecules in our body, which alter the surface of nanoparticles. These biologically-generated collections of proteins on their surfaces are called protein corona. Their composition and patterns change according to the physical characteristics of nanoparticles as well as the nature of human body fluids (68–70). Protein corona are known to significantly affect in vivo distribution and targeted delivery (71, 72). Moreover, the composition of protein corona changes according to the disease status and even shows person-to-person difference (73, 74), which makes inference more difficult about clinical translatability of in vivo application of nanoparticles based on small animal experiments.
Another difficulty in clinical translation of in vivo behavior revealed by radionanomedicine is the fact that radiolabeled nanoparticles are only a small fraction of nanoparticles. Physical properties of nanoparticles rely on preparation steps, which largely affect in vivo behavior of nanoparticles. Even more, size and electrical properties of nanoparticles can be different when the samples are prepared with the same procedures (75). In addition, distribution of properties of nanoparticles means that samples of nanoparticles are inhomogeneous to a certain extent. Radiolabeling procedures could affect the variability of properties of nanoparticles because simple procedures can make aggregated nanoparticles (76). Furthermore, radiolabeled nanoparticles could be slightly different from unlabeled nanoparticles because radiolabelling procedures could alter the nanoparticles to some extent. Nanoparticles with chelators could affect surface areas and shapes of nanoparticles which alter the in vivo behavior compared with unlabeled nanoparticles (77). Characterization procedures of nanoparticles such as electron microscopy, dynamic light scattering and zeta-potential measurements should be critically performed for radiolabeled nanoparticle compared with unlabeled one for clinical translation.
Degradation and metabolism of radiolabeled nanoparticles in vivo should be considered for clinical translation. The serum stability of radiolabeled nanoparticles is confirmed in vitro before in vivo experiments in most cases, however, their clearance in vivo further depends on their interaction with the in vivo biological milieu (59, 78). Clearance from the body of the nanomaterials mostly involves metabolism in the liver followed by intestinal excretion or independent renal excretion. Systemically administered nanoparticles are regarded as foreign materials by the bodily defense system and coated by opsonin proteins. This process is followed by phagocytosis particularly in the mononuclear phagocytic system such as Kupffer cells in liver and macrophages in the spleen and lungs (79). To reduce the opsonization, hydrophilic coating with polyethylene glycol (PEG) has been tried as a popular surface modification. However, opsonization takes also place with these hydrophilized PEGylated nanoparticles. Though the inorganic nanoparticles coated with organic compounds are generally stable in vitro, they could easily be degraded in vivo (80). This degradation of radiolabeled nanoparticles makes in vivo distribution of nanoparticles more unpredictable. If the degradation of radiolabeled nanoparticles occurs in vivo before they reach the target, nuclear imaging might yield incorrect information regarding the in vivo distribution of nanoparticles (80). To clarify these issues, distribution and excretion of radioisotopes themselves or the radioisotope-chelator complex should be studied simultaneously with radiolabeled nanoparticles in preclinical models (5, 81). Figure 2 summarizes the pitfalls of interpretation of the distribution of systemically administered radiolabeled nanoparticles using radioactivity detection.
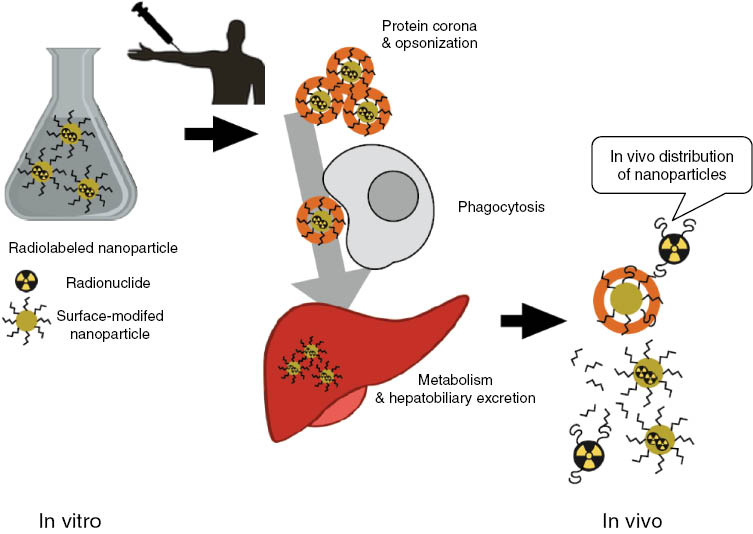
Pitfalls in tracking radiolabeled nanoparticles.
Systemically administered nanoparticles encounter various biological molecules and several reactions take place. Protein corona is generated around the nanoparticles and opsonized. After this immediate reaction, injected nanoparticles could induce phagocytosis particularly in mononuclear phagocyte systems. Radiolabeled nanoparticles could be degraded and nuclear imaging might delineate only the radioactivity and yield inaccurately the distribution of nanoparticles.
Excretion and degradation of systemically administered nanoparticles are also complex. The excretion and degradation of nanoparticles are generally mediated by opsonization and phagocytosis. After these clearance processes, nanoparticles and their metabolites are excreted via hepatobiliary or urinary tract (82). The excretion of multiple metabolites of engineered nanoparticles should take place via both routes, however, nanoparticle excretion is varied between phagocytosis, hepatobiliary and/or renal excretion according the characteristics of each radiolabeled nanoparticle. In an example of a radiolabeled upconversion nanoparticle (UCNP), radiolabeled UCNPs gathered in hepatic vascular sinusoids, were taken up by hepatocytes and finally excreted via bile canaliculi in their integral form rather than been taken up in Kupffer cells (83). This study of the excretion pathway using radioactivity and upconversion-luminescence imaging using 64Cu-labeled UCNP confirmed the excretion in the integral form. This was different from excretion of another radiolabeled nanoparticle after the capsular detachment from the nanoparticles (83). As a different excretion pathway, direct excretion from intestines mediated by goblet cells was also reported, not mediated by hepatobiliary excretion (84). Due to this complexity of in vivo distribution and excretion of nanoparticles which might even vary between individuals according to the types of nanoparticles, an individualized distribution study is required to consider the future clinical application.
To sum up, in vivo distribution is affected by several individual factors as well as physical characteristics of nanoparticles. In vitro stability cannot be translated directly to in vivo situations because of various biochemical reactions occur immediately after administration. In addition, excretion and metabolism of radiolabeled nanoparticles make biodistribution study harder to interpret. The complexity and uncertainty of distribution, metabolism and excretion of nanoparticles suggest that all nanoparticles need individualized human biodistribution study based on radionanomedicine.
Dosimetry of radionanomedicine
Radiation dosimetry is crucial for the clinical use of radiolabeled nanoparticles for therapy as well as diagnosis. Dosimetry data are required for radiation safety as well as measurement of effective radiation doses for internal radiotherapy. Radiation doses absorbed in specific tissues are determined by kinetics of radiopharmaceuticals, physical characteristics of radionuclides such as half-life, emission types and retention time (85). To calculate radiation doses to the specific target organs, total cumulated radioactivity calculated by integration of time radioactivity curve is obtained first. Absorbed radiation doses to the target organs consist of radiation from the radioactivity of target organs themselves and radiation from the neighboring organs. This calculation process is standardized in the open-source softwares such as OLINDA/EXM (86). Pharmacokinetics of radiolabeled nanoparticles and anatomical distribution are key points to calculate dosimetry.
Although radiation dosimetry of radiolabeled nanoparticles is the essential for clinical application, few preclinical studies have been reported. Preclinical dosimetry study using therapeutic radiolabeled nanoparticles can provide the information for basic treatment planning with regard to the administration dose for successful clinical trials. Delivery of the highest absorbed dose to the target tissues satisfying safety dose which limits to the critical organs including bone marrow, liver and kidneys are the key issues in designing therapeutic application of radiolabeled nanoparticles. They depend upon the types of radionuclides given and their pharmacokinetics varying with modified surface characteristics. In preclinical studies, dosimetry using radiolabeled liposomes was performed to determine which types of liposomes were the most effective for delivering optimal dose and least radiation to bone marrow (87–89). Furthermore, radiation dosimetry of nanoparticles for diagnostic imaging should be performed to predict safety in humans. In a recent report of first-in-human study using 124I-labeled silica nanoparticles (20), radiation doses were reported as the fundamental safety data for further clinical trial. Because radioiodine-labeled nanoparticles increase concerns of free iodine-related thyroid damage, this study focused on radiation doses to the thyroid as a critical organ.
Radiation dosimetry has been routinely performed in developments of new radiopharmaceutics. It should be also performed before clinical application of radiolabeled nanoparticles. Even though radiation dosimetry of nanoparticles is almost similar to that of conventional radiopharmaceutics, there are some points that need to be carefully considered. Firstly, nanoparticles for internal radiotherapy can be labeled with multiple radionuclides, which can make it harder to estimate radiation dosimetry. Recent reports suggest that the combination of different types of beta-emitters could be effective for internal radiotherapy according to the tumor size and uptake of nanoparticles (90, 91). Various therapeutic radionuclides with different beta-ray energy such as 90Y and 177Lu can be combined for a personalized optimal ratio according to the tumor properties (90). Therefore, radiation dosimetry of multiple radionuclides might be considered the future for radiolabeled nanoparticles particularly for internal radiation therapy to tumors. In addition, because of multifunctionality, radiolabeled nanoparticles can deliver chemical drugs as well as therapeutic radionuclides. In vivo kinetics obtained by radiolabeled nanoparticles can provide radiation dosimetry as well as estimated concentration of chemical drugs in the target tissue. For example, 186re-labeled liposomal doxorubicin could be applied to simultaneous local radiation and chemotherapy for tumor tissues (92). Dosimetry calculated by accumulation of the radiolabeled liposomes helps determine both radiation and chemotherapy doses for the treatment.
In the future, every clinical trial using radiolabeled nanoparticles should be accompanied by appropriate dosimetry studies. Considering that the internal dosimetry is done by using the kinetic data of radiotracer administered in vivo, the preclinical kinetic modeling and the precise quantification of radiolabeled nanoparticles must precede the ensuing dose-optimization studies.
Radionanomedicine of endogenous nanoparticles
Inorganic exogenous nanoparticles have been studied for biomedical application with the due concerns about in vivo safety. As we do not use a pharmacologic amount but a trace amount of radiolabeled nanoparticles, we are not worried about the possible toxicity of these nanoparticles. Nevertheless, we still need to care about substantial biocompatibility of these nanoparticles for facilitating clinical nanomedicine. In this aspect, endogenous nanoparticles recently received great attention. Most living things ranging from unicellular organisms to complex multicellular organisms exploit extracellular vesicles for intercellular communication (93). We can consider these extracellular vesicles as endogeneous nanomaterials, and in contrast, liposomes can be considered as exogenous organic nanomaterials which are extracellular vesicle-mimetic. Because they can be engineered for diagnostic and therapeutic purposes as exogenous nanomaterials, we expect that we could avoid the concerns about toxicity and possibly the immune responses and thus facilitated clinical application is expected.
Extracellular vesicles are a broad spectrum of vesicles excreted by various types of cells. They can be found in most types of body fluids including serum, urine and saliva. Recently, as biological nanomaterials, they have been used as emerging therapeutics for oncology (94, 95) and regenerative medicine (96). Extracellular vesicles basically consist of a lipid bilayer and contain the proteins, the cytosolic components and the nucleic acids which carry biological information for intercellular communication (97). Thus, they can be used as nanocarriers which transport genetic materials and proteins as well as drugs (94, 98). Simple loading ability of both lipophilic drugs (doxolubicin or curcumin) and hydrophilic molecules (therapeutic nucleic acids) highlights the potential attributes of exosome (extracellular vesicles) as delivery vehicle. Another example of therapeutic use of extracelluar vesicles for cancer therapy was exosome-based cancer immunotherapy. Given that exosomes deliver tumor-antigens to elicit immune responses, exosome-derived anti-tumor immune response was proposed as cancer therapeutics. Exosome-based cancer immunotherapy derived from dendritic cells was already performed as a phase I clinical trial (99–101).
Even though biomedical application of extracellular vesicles is promising, in vivo behavior and distribution of administered extracellular vesicles are still unknown. In spite of advantages in biocompatibility of extracellular vesicles for in vivo administration, in vivo kinetics and behavior have not been fully understood. Thus, radiolabeled extracellular vesicles for quantification of systemic distribution could facilitate clinical translation of them because they have less concern about safety than other nanoparticles (102, 103). Recently, radiolabeled extracellular vesicles disclosed biodistribution of systemically administered extracellular vesicles, either natural exosomes or exosome-mimetic nanovesicles. Using reporter systems expressed in exosomes to have membrane-bound streptavidin, 125I was successfully labeled to exosomes by conjugation of norbiotinamide and biodistribution could be elucidated (104). 111In-oxine (105) or 99mTc-HMPAO (76) was used for radiolabeling which used the principle of entrapment of radiotracers converted in the cytosol from hydrophobic to hydrophilic compounds. These radiolabeling with entrapment could be a biocompatible option as the entrapment procedures could be performed in physiologic condition only mixing extracellular vesicles with the radiotracers. SPECT images were successfully acquired in animals using 99mTc-HMPAO-labeled extracellular vesicles (76). So far, most studies of exosomes presumed that they have target-specific homing effect (106, 107). Several studies which used exosomes for therapeutics focused on therapeutic effects on target tissues without in vivo distribution study. The radiolabeled exosomes can elucidate whether they target the specific tissues as well as disclose the distribution, i.e. physiologic behaviors of exosomes in the body.
For clinical application of extracellular vesicles of radionanomedicine, a lot of further studies are warranted. Firstly, low yield of exosomes produced from cultured cells limits the evaluation of therapeutic usability of extracellular vesicles as well as imaging studies with radiolabeling. Vesicles secreted from cells are isolated and purified by various methods including ultracentrifugation, filtration and immunoaffinity isolation from culture media or biological fluids (108). However, large-scale production for in vivo application is difficult. A recently developed method which collects exosome-mimetic nanovesicles from whole cells can be an alternative (109). Radionanomedicine with high detection sensitivity can contribute to overcome this problem of low yield of radiolabeled exosomes. Secondly, just as exogeneous nanoparticles are metabolized and degraded in the body, extracellular vesicles are also degraded rapidly (104, 110). Thus, whereabouts of radionuclides might not reflect the accurate distribution of the vesicles themselves. Simple measurement by thin layer chromatography capable of distinguishing the radiolabeled extracellular vesicles from the degraded extracellular vesicles would be helpful to better understand in vivo stability and distribution of the radiolabeled extracellular vesicles. Furthermore, as extracellular vesicles are derived from a variety of cells or found in any body fluids, their composition also varies a lot according to the condition of the cells (111). Recent evidence on in vivo behavior of extracellular vesicles clearly demonstrated that their in vivo distribution varies depending on the cell sources or the administration routes (112). For examples, bone marrow dendritic cell-derived exosomes were inclined to splenic tissue, but muscle cell-derived exosomes or melanoma-derived exosomes accumulated more in the liver and the lungs, respectively. Their differential intrinsic homing ability will help guide the design of in vivo therapeutic extracellular vesicles as carriers to deliver the drug to the tissue of interest. Interestingly, the same group documented there were no differences of cross-species distribution of extracellular vesicles between human and mouse-originated extracellular vesicles in a mouse xenograft model despite different cell origin-dependent tissue tropism (112). This complexity and diversity of extracellular vesicles suggest that the imaging of radiolabeled extracellular vesicles should be routinely performed if they are further considered for their usefulness for clinical theranostics.
Conclusion: future perspectives of radionanomedicine
Targeted delivery of nanoparticles for theranostic purpose is promising for future clinical application due to their multifunctionality and flexibility. However, the clinical translation is limited due to the concerns of toxicity and uncertainty of in vivo physiology. Radionanomedicine provides in vivo behavior of nanoparticles using traceable amounts of nanomaterials which would avoid any predicted pharmacologic effects. In principle, this principle of radiotracer technology and noninvasive nuclear imaging could facilitate clinical trials. Furthermore, using therapeutic radioisotopes, internal radiotherapy based on radiation dosimetry can be achieved with image-based monitoring.
For clinical translation of nanoparticles initiated from radionanomedicine, several issues related with radiation and interpretation of results should be carefully considered. In particular, in vivo behavior of radiolabeled nanoparticles is too complex to be simply interpreted by tracer amounts of them, because it is affected by physicochemical and biological characteristics of nanoparticles. Variability of nanoparticles and alteration in a biological milieu that might be associated with individual-to-individual difference make it harder to interpret biological behavior of nanoparticles. Therefore, development of a procedure of simple and appropriate radiolabeling and surface modification is urgently warranted because demands are great for the characterization of in vivo behaviors of various types of nanoparticles. The fact that in vivo distribution and excretion of nanoparticles are varied between individuals suggests that clinically applicable nanoparticles should be routinely examined for their biodistribution using radionanomedicine discipline. In addition, for the clinical application of radiolabeled nanoparticles, internal radiation dosimetry is required as an essential safety assurance using quantitation of expected dose for internal radiotherapy. As the dosimetry is also based on the kinetics of radiolabeled nanoparticles, kinetic modeling and distribution revealing the contribution of physicochemical and biological aspects of nanoparticles should be comprehensively studied. The periodic table of nanoparticle physiology according to the types of nanoparticles in various biological milieu will eventually be constructed using radiolabeled nanoparticles (5).
Funding source: Ministry of Health and Welfare
Award Identifier / Grant number: HI14C0466
Award Identifier / Grant number: HI14C3344
Award Identifier / Grant number: HI14C1277
Funding source: National Research Foundation of Korea
Award Identifier / Grant number: NRF-2015M3C7A1028926
Funding statement: This research was supported by a grant from the Korea Health Technology R&D Project through the Korea Health Industry Development Institute (KHIDI), funded by the Ministry of Health and Welfare, Republic of Korea (HI14C0466), and funded by the Ministry of Health and Welfare, Republic of Korea (HI14C3344), and funded by the Ministry of Health and Welfare, Republic of Korea (HI14C1277), and supported by the Technology Innovation Program (10052749) funded by the Ministry of Trade, Industry and Energy (MOTIE), Republic of Korea, and supported by the original of technology research program for brain science through the national research foundation of Korea (NRF-2015M3C7A1028926).
About the authors

Hongyoon Choi recieved his MD degree (2010) and PhD degree (2014) from Seoul National University. He completed a 4-year residency program at the Department of Nuclear Medicine, Seoul National University Hospital and recieved Board of Nuclear Medicine accreditation in 2015. He currently serves as a public health doctor, a mandatory alternative service. He won the Young Medical Scientist Award of the Seoul Medical Association in 2015. His research is focused on the development of imaging biomarkers and theragnosis for cancer as well as brain disorders. His interests include preclinical and clinical research for innovative diagnostic and therapeutic approaches.
Yun-Sang Lee is the Brain Korea 21 plus (BK21 plus) Associate Professor in the Department of Molecular Medicine and Biopharmaceutical Sciences, Graduate School of Convergence Science and Technology at Seoul National University. He received his BS and MS from the Department of Chemistry, College of Sciences at Kyunghee University, Korea in 1996 and 1998, and his PhD from the Department of Pharmaceutical Manufacturing Chemistry, College of Pharmacy at Seoul National University, Korea in 2006, respectively. He is interested in the field of development and implementation of new methods for radiolabeling chemistry and the development of new diagnostic or therapeutic radiopharmaceuticals, and also, the development of new methods for the surface modification or radiolabeling of nano-materials, especially radionanomedicine, and their uses for diagnosis/therapy or theranostics.

Do Won Hwang recieved his PhD degree in “Program in Neuroscience” in 2009 from Seoul National University. He is currently the Brain Korea 21 plus (BK21 plus) Associate Professor in the Department of Molecular Medicine and Biopharmaceutical Sciences, Graduate School of Convergence Science and Technology at Seoul National University. He recieved an achievement award in the field of radio-nanotechnology in 2015. His research interests focus on the development of multifunctional nanomaterials for disease theranostics, stem cell imaging in regenerative medicine, non-coding RNA monitoring.
Dong Soo Lee is a nuclear medicine physician and Professor in Nuclear Medicine in at Seoul National University (SNU) and SNU Hospital since 1990. He is also Professor and Chairman of Molecular Medicine and Biopharmaceutical Sciences. He is also Director of Bio-MAX/N-Bio which is the Biotechnology Research Institute of SNU. He founded and was the first President of the Korean Society for Nanomedicine in 2012. His major interest is radionanomedicine, which is the combination of nuclear medicine and nanomedicine.
Acknowledgments:
This research was supported by a grant from the Korea Health Technology R&D Project through the Korea Health Industry Development Institute (KHIDI), funded by the Ministry of Health and Welfare, Republic of Korea (HI14C0466), and funded by the Ministry of Health and Welfare, Republic of Korea (HI14C3344), and funded by the Ministry of Health and Welfare, Republic of Korea (HI14C1277), and supported by the Technology Innovation Program (10052749) funded by the Ministry of Trade, Industry and Energy (MOTIE), Republic of Korea, and supported by the original of technology research program for brain science through the national research foundation of Korea (NRF-2015M3C7A1028926).
Conflict of interest statement: Authors state no conflict of interest. All authors have read the journal’s publication ethics and publication malpractice statement available at the journal’s website and hereby confirm that they comply with all its parts applicable to the present scientific work.
References
1. Lehner R, Wang X, Marsch S, Hunziker P. Intelligent nanomaterials for medicine: carrier platforms and targeting strategies in the context of clinical application. Nanomedicine 2013;9:742–57.10.1016/j.nano.2013.01.012Search in Google Scholar
2. Etheridge ML, Campbell SA, Erdman AG, Haynes CL, Wolf SM, McCullough J. The big picture on nanomedicine: the state of investigational and approved nanomedicine products. Nanomedicine 2013;9:1–14.10.1016/j.nano.2012.05.013Search in Google Scholar
3. Wicki A, Witzigmann D, Balasubramanian V, Huwyler J. Nanomedicine in cancer therapy: challenges, opportunities, and clinical applications. J Control Release 2015;200:138–57.10.1016/j.jconrel.2014.12.030Search in Google Scholar
4. Allen TM, Cullis PR. Drug delivery systems: entering the mainstream. Science 2004;303:1818–22.10.1126/science.1095833Search in Google Scholar
5. Lee DS, Im HJ, Lee YS. Radionanomedicine: widened perspectives of molecular theragnosis. Nanomedicine 2015;11:795–810.10.1016/j.nano.2014.12.010Search in Google Scholar
6. Muthu MS, Wilson B. Multifunctional radionanomedicine: a novel nanoplatform for cancer imaging and therapy. Nanomedicine (Lond) 2010;5:169–71.10.2217/nnm.09.107Search in Google Scholar
7. Lee YS, Kim YI, Lee DS. Future perspectives of radionanomedicine using the novel micelle-encapsulation method for surface modification. Nucl Med Mol Imaging 2015;49:170–3.10.1007/s13139-015-0358-9Search in Google Scholar
8. Lee DE, Koo H, Sun IC, Ryu JH, Kim K, Kwon IC. Multifunctional nanoparticles for multimodal imaging and theragnosis. Chem Soc Rev 2012;41:2656–72.10.1039/C2CS15261DSearch in Google Scholar
9. Alazraki NP, Eshima D, Eshima LA, Herda SC, Murray DR, Vansant JP, et al. Lymphoscintigraphy, the sentinel node concept, and the intraoperative gamma probe in melanoma, breast cancer, and other potential cancers. Semin Nucl Med 1997;27:55–67.10.1016/S0001-2998(97)80036-0Search in Google Scholar
10. Strand SE, Bergqvist L. Radiolabeled colloids and macromolecules in the lymphatic system. Crit Rev Ther Drug Carrier Syst 1989;6:211–38.Search in Google Scholar
11. Nel A, Xia T, Madler L, Li N. Toxic potential of materials at the nanolevel. Science 2006;311:622–7.10.1126/science.1114397Search in Google Scholar PubMed
12. Xia T, Kovochich M, Brant J, Hotze M, Sempf J, Oberley T, et al. Comparison of the abilities of ambient and manufactured nanoparticles to induce cellular toxicity according to an oxidative stress paradigm. Nano Lett 2006;6:1794–807.10.1021/nl061025kSearch in Google Scholar
13. Buzea C, Pacheco II, Robbie K. Nanomaterials and nanoparticles: sources and toxicity. Biointerphases 2007;2:MR17–71.10.1116/1.2815690Search in Google Scholar
14. Nel AE, Mädler L, Velegol D, Xia T, Hoek EMV, Somasundaran P, et al. Understanding biophysicochemical interactions at the nano-bio interface. Nat Mater 2009;8:543–57.10.1038/nmat2442Search in Google Scholar
15. Kirchner C, Liedl T, Kudera S, Pellegrino T, Muñoz Javier A, Gaub HE, et al. Cytotoxicity of colloidal CdSe and CdSe/ZnS nanoparticles. Nano Lett 2005;5:331–8.10.1021/nl047996mSearch in Google Scholar
16. Boisselier E, Astruc D. Gold nanoparticles in nanomedicine: preparations, imaging, diagnostics, therapies and toxicity. Chem Soc Rev 2009;38:1759–82.10.1039/b806051gSearch in Google Scholar
17. Khlebtsov N, Dykman L. Biodistribution and toxicity of engineered gold nanoparticles: a review of in vitro and in vivo studies. Chem Soc Rev 2011;40:1647–71.10.1039/C0CS00018CSearch in Google Scholar
18. Knudsen KB, Northeved H, Kumar PE, Permin A, Gjetting T, Andresen TL, et al. In vivo toxicity of cationic micelles and liposomes. Nanomedicine 2015;11:467–77.10.1016/j.nano.2014.08.004Search in Google Scholar
19. Benezra M, Penate-Medina O, Zanzonico PB, Schaer D, Ow H, Burns A, et al. Multimodal silica nanoparticles are effective cancer-targeted probes in a model of human melanoma. J Clin Invest 2011;121:2768–80.10.1172/JCI45600Search in Google Scholar
20. Phillips E, Penate-Medina O, Zanzonico PB, Carvajal RD, Mohan P, Ye Y, et al. Clinical translation of an ultrasmall inorganic optical-PET imaging nanoparticle probe. Sci Transl Med 2014;6:260ra149.10.1126/scitranslmed.3009524Search in Google Scholar
21. Storm G, Belliot SO, Daemen T, Lasic DD. Surface modification of nanoparticles to oppose uptake by the mononuclear phagocyte system. Adv Drug Deliver Rev 1995;17:31–48.10.1016/0169-409X(95)00039-ASearch in Google Scholar
22. Roser M, Fischer D, Kissel T. Surface-modified biodegradable albumin nano- and microspheres. II: effect of surface charges on in vitro phagocytosis and biodistribution in rats. Eur J Pharm Biopharm 1998;46:255–63.10.1016/S0939-6411(98)00038-1Search in Google Scholar
23. Otsuka H, Nagasaki Y, Kataoka K. PEGylated nanoparticles for biological and pharmaceutical applications. Adv Drug Deliv Rev 2003;55:403–19.10.1002/9781118135440.ch47Search in Google Scholar
24. Schipper ML, Iyer G, Koh AL, Cheng Z, Ebenstein Y, Aharoni A, et al. Particle size, surface coating, and PEGylation influence the biodistribution of quantum dots in living mice. Small 2009;5:126–34.10.1002/smll.200800003Search in Google Scholar PubMed PubMed Central
25. Kummar S, Kinders R, Rubinstein L, Parchment RE, Murgo AJ, Collins J, et al. Compressing drug development timelines in oncology using phase ‘0’ trials. Nat Rev Cancer 2007;7:131–9.10.1038/nrc2066Search in Google Scholar PubMed
26. Marchetti S, Schellens JH. The impact of FDA and EMEA guidelines on drug development in relation to Phase 0 trials. Br J Cancer 2007;97:577–81.10.1038/sj.bjc.6603925Search in Google Scholar PubMed PubMed Central
27. LoRusso PM. Phase 0 clinical trials: an answer to drug development stagnation? J Clin Oncol 2009;27:2586–8.10.1200/JCO.2008.21.5798Search in Google Scholar PubMed
28. Aktolun C, Goldsmith SJ. Nuclear medicine therapy: principles and clinical applications. New York, USA: Springer Science and Business Media, 2012.Search in Google Scholar
29. Goldsmith SJ. Radioimmunotherapy of lymphoma: Bexxar and Zevalin. Semin Nucl Med 2010;40:122–35.10.1053/j.semnuclmed.2009.11.002Search in Google Scholar PubMed
30. Garin E, Lenoir L, Rolland Y, Edeline J, Mesbah H, Laffont S, et al. Dosimetry based on 99mTc-macroaggregated albumin SPECT/CT accurately predicts tumor response and survival in hepatocellular carcinoma patients treated with 90Y-loaded glass microspheres: preliminary results. J Nucl Med 2012;53:255–63.10.2967/jnumed.111.094235Search in Google Scholar PubMed
31. Saxena A, Bester L, Shan L, Perera M, Gibbs P, Meteling B, et al. A systematic review on the safety and efficacy of yttrium-90 radioembolization for unresectable, chemorefractory colorectal cancer liver metastases. J Cancer Res Clin Oncol 2014;140: 537–47.10.1007/s00432-013-1564-4Search in Google Scholar PubMed
32. Sharma RA, Van Hazel GA, Morgan B, Berry DP, Blanshard K, Price D, et al. Radioembolization of liver metastases from colorectal cancer using yttrium-90 microspheres with concomitant systemic oxaliplatin, fluorouracil, and leucovorin chemotherapy. J Clin Oncol 2007;25:1099–106.10.1200/JCO.2006.08.7916Search in Google Scholar PubMed
33. Geschwind JFH, Salem R, Carr BI, Soulen MC, Thurston KG, Goin KA, et al. Yttrium-90 microspheres for the treatment of hepatocellular carcinoma. Gastroenterology 2004;127:S194–205.10.1053/j.gastro.2004.09.034Search in Google Scholar PubMed
34. Salem R, Lewandowski RJ, Mulcahy MF, Riaz A, Ryu RK, Ibrahim S, et al. Radioembolization for hepatocellular carcinoma using Yttrium-90 microspheres: a comprehensive report of long-term outcomes. Gastroenterology 2010;138:52–64.10.1053/j.gastro.2009.09.006Search in Google Scholar PubMed
35. Helbok A, Decristoforo C, Dobrozemsky G, Rangger C, Diederen E, Stark B, et al. Radiolabeling of lipid-based nanoparticles for diagnostics and therapeutic applications: a comparison using different radiometals. J Lipos Res 2010;20:219–27.10.3109/08982100903311812Search in Google Scholar PubMed
36. Phillips WT, Bao A, Brenner AJ, Goins BA. Image-guided interventional therapy for cancer with radiotherapeutic nanoparticles. Adv Drug Deliver Rev 2014;76:39–59.10.1016/j.addr.2014.07.001Search in Google Scholar PubMed PubMed Central
37. Chen F, Hong H, Zhang Y, Valdovinos HF, Shi S, Kwon GS, et al. In vivo tumor targeting and image-guided drug delivery with antibody-conjugated, radiolabeled mesoporous silica nanoparticles. ACS Nano 2013;7:9027–39.10.1021/nn403617jSearch in Google Scholar PubMed PubMed Central
38. Xiao Y, Hong H, Matson VZ, Javadi A, Xu W, Yang Y, et al. Gold nanorods conjugated with doxorubicin and cRGD for combined anticancer drug delivery and PET imaging. Theranostics 2012;2:757–68.10.7150/thno.4756Search in Google Scholar PubMed PubMed Central
39. Gerlinger M, Rowan AJ, Horswell S, Larkin J, Endesfelder D, Gronroos E, et al. Intratumor heterogeneity and branched evolution revealed by multiregion sequencing. N Engl J Med 2012;366:883–92.10.1056/NEJMoa1113205Search in Google Scholar PubMed PubMed Central
40. Fahey F, Zukotynski K, Capala J, Knight N; Organizing Committee C, Participants of NCISJWoTRT. Targeted radionuclide therapy: proceedings of a joint workshop hosted by the National Cancer Institute and the Society of Nuclear Medicine and Molecular Imaging. J Nucl Med 2014;55:337–48.10.2967/jnumed.113.135178Search in Google Scholar PubMed
41. Lee YK, Jeong JM, Hoigebazar L, Yang BY, Lee YS, Lee BC, et al. Nanoparticles modified by encapsulation of ligands with a long alkyl chain to affect multispecific and multimodal imaging. J Nucl Med 2012;53:1462–70.10.2967/jnumed.111.092759Search in Google Scholar PubMed
42. Xing Y, Zhao J, Conti PS, Chen K. Radiolabeled nanoparticles for multimodality tumor imaging. Theranostics 2014;4:290–306.10.7150/thno.7341Search in Google Scholar PubMed PubMed Central
43. Goel S, Chen F, Ehlerding EB, Cai W. Intrinsically radiolabeled nanoparticles: an emerging paradigm. Small 2014;10:3825–30.10.1002/smll.201401048Search in Google Scholar
44. Sun M, Hoffman D, Sundaresan G, Yang L, Lamichhane N, Zweit J. Synthesis and characterization of intrinsically radiolabeled quantum dots for bimodal detection. Am J Nucl Med Mol Imaging 2012;2:122–35.Search in Google Scholar
45. Sun X, Huang X, Guo J, Zhu W, Ding Y, Niu G, et al. Self-illuminating 64Cu-doped CdSe/ZnS nanocrystals for in vivo tumor imaging. J Am Chem Soc 2014;136:1706–9.10.1021/ja410438nSearch in Google Scholar
46. Suresh M, Cao Y. A simple and efficient method for radiolabeling of preformed liposomes. J Pharm Pharm Sci 1998;1:31–7.Search in Google Scholar
47. Phillips WT, Rudolph AS, Goins B, Timmons JH, Klipper R, Blumhardt R. A simple method for producing a technetium-99m-labeled liposome which is stable in vivo. Int J Rad Appl Instrum B 1992;19:539–47.10.1016/0883-2897(92)90149-SSearch in Google Scholar
48. Awasthi VD, Goins B, Klipper R, Phillips WT. Dual radiolabeled liposomes: biodistribution studies and localization of focal sites of infection in rats. Nucl Med Biol 1998;25:155–60.10.1016/S0969-8051(97)00162-5Search in Google Scholar
49. Bao A, Goins B, Klipper R, Negrete G, Phillips WT. Direct 99mTc labeling of pegylated liposomal doxorubicin (Doxil) for pharmacokinetic and non-invasive imaging studies. J Pharmacol Exp Ther 2004;308:419–25.10.1124/jpet.103.059535Search in Google Scholar PubMed
50. Mougin-Degraef M, Jestin E, Bruel D, Remaud-Le Saëc P, Morandeau L, Faivre-Chauvet A, et al. High-activity radio-iodine labeling of conventional and stealth liposomes. J Liposome Res 2006;16:91–102.10.1080/08982100500528941Search in Google Scholar PubMed
51. Marik J, Tartis MS, Zhang H, Fung JY, Kheirolomoom A, Sutcliffe JL, et al. Long-circulating liposomes radiolabeled with [18F]fluorodipalmitin ([18F]FDP). Nucl Med Biol 2007;34:165–71.10.1016/j.nucmedbio.2006.12.004Search in Google Scholar PubMed PubMed Central
52. Morales-Avila E, Ferro-Flores G, Ocampo-García BE, de María Ramírez F. Radiolabeled nanoparticles for molecular imaging, Molecular Imaging, Prof. Bernhard Schaller (Ed.). 2012; InTech, DOI: 10.5772/31109. Available from: http://www.intechopen.com/books/molecular-imaging/radiolabeled-nanoparticles-for-molecular-imaging.10.5772/31109Search in Google Scholar
53. Locatelli E, Gil L, Israel LL, Passoni L, Naddaka M, Pucci A, et al. Biocompatible nanocomposite for PET/MRI hybrid imaging. Int J Nanomedicine 2012;7:6021–33.10.2147/IJN.S38107Search in Google Scholar PubMed PubMed Central
54. Yang L, Sundaresan G, Sun M, Jose P, Hoffman D, McDonagh PR, et al. Intrinsically radiolabeled multifunctional cerium oxide nanoparticles for in vivo studies. J Mater Chem B 2013;1:1421–31.10.1039/c2tb00404fSearch in Google Scholar PubMed
55. Chattopadhyay N, Fonge H, Cai Z, Scollard D, Lechtman E, Done SJ, et al. Role of antibody-mediated tumor targeting and route of administration in nanoparticle tumor accumulation in vivo. Mol Pharm 2012;9:2168–79.10.1021/mp300016pSearch in Google Scholar PubMed
56. Jain RK, Stylianopoulos T. Delivering nanomedicine to solid tumors. Nat Rev Clin Oncol 2010;7:653–64.10.1038/nrclinonc.2010.139Search in Google Scholar PubMed PubMed Central
57. Smith BR, Kempen P, Bouley D, Xu A, Liu Z, Melosh N, et al. Shape matters: intravital microscopy reveals surprising geometrical dependence for nanoparticles in tumor models of extravasation. Nano Lett 2012;12:3369–77.10.1021/nl204175tSearch in Google Scholar PubMed PubMed Central
58. Brannon-Peppas L, Blanchette JO. Nanoparticle and targeted systems for cancer therapy. Adv Drug Deliv Rev 2004;56: 1649–59.10.1016/j.addr.2004.02.014Search in Google Scholar PubMed
59. Alexis F, Pridgen E, Molnar LK, Farokhzad OC. Factors affecting the clearance and biodistribution of polymeric nanoparticles. Mol Pharm 2008;5:505–15.10.1021/mp800051mSearch in Google Scholar PubMed PubMed Central
60. Kamaly N, Xiao Z, Valencia PM, Radovic-Moreno AF, Farokhzad OC. Targeted polymeric therapeutic nanoparticles: design, development and clinical translation. Chem Soc Rev 2012;41:2971–3010.10.1039/c2cs15344kSearch in Google Scholar PubMed PubMed Central
61. Bertrand N, Wu J, Xu X, Kamaly N, Farokhzad OC. Cancer nanotechnology: the impact of passive and active targeting in the era of modern cancer biology. Adv Drug Deliv Rev 2014;66:2–25.10.1016/j.addr.2013.11.009Search in Google Scholar PubMed PubMed Central
62. Yang BY, Moon SH, Seelam SR, Jeon MJ, Lee YS, Lee DS, et al. Development of a multimodal imaging probe by encapsulating iron oxide nanoparticles with functionalized amphiphiles for lymph node imaging. Nanomedicine (Lond) 2015;10:1899–910.10.2217/nnm.15.41Search in Google Scholar PubMed
63. Almeida JP, Chen AL, Foster A, Drezek R. In vivo biodistribution of nanoparticles. Nanomedicine (Lond) 2011;6:815–35.10.2217/nnm.11.79Search in Google Scholar PubMed
64. Moghimi SM, Hunter AC, Andresen TL. Factors controlling nanoparticle pharmacokinetics: an integrated analysis and perspective. Annu Rev Pharmacol Toxicol 2012;52:481–503.10.1146/annurev-pharmtox-010611-134623Search in Google Scholar PubMed
65. Cerqueira BB, Lasham A, Shelling AN, Al-Kassas R. Nanoparticle therapeutics: Technologies and methods for overcoming cancer. Eur J Pharm Biopharm 2015;97:140–51.10.1016/j.ejpb.2015.10.007Search in Google Scholar PubMed
66. Gratton SE, Ropp PA, Pohlhaus PD, Luft JC, Madden VJ, Napier ME, et al. The effect of particle design on cellular internalization pathways. Proc Natl Acad Sci USA 2008;105:11613–8.10.1073/pnas.0801763105Search in Google Scholar PubMed PubMed Central
67. Nangia S, Sureshkumar R. Effects of nanoparticle charge and shape anisotropy on translocation through cell membranes. Langmuir 2012;28:17666–71.10.1021/la303449dSearch in Google Scholar PubMed
68. Ge C, Tian J, Zhao Y, Chen C, Zhou R, Chai Z. Towards understanding of nanoparticle-protein corona. Arch Toxicol 2015;89:519–39.10.1007/s00204-015-1458-0Search in Google Scholar PubMed
69. Lundqvist M, Stigler J, Elia G, Lynch I, Cedervall T, Dawson KA. Nanoparticle size and surface properties determine the protein corona with possible implications for biological impacts. Proc Natl Acad Sci USA 2008;105:14265–70.10.1073/pnas.0805135105Search in Google Scholar PubMed PubMed Central
70. Casals E, Pfaller T, Duschl A, Oostingh GJ, Puntes V. Time evolution of the nanoparticle protein corona. ACS Nano 2010;4:3623–32.10.1021/nn901372tSearch in Google Scholar PubMed
71. Sahneh FD, Scoglio CM, Monteiro-Riviere NA, Riviere JE. Predicting the impact of biocorona formation kinetics on interspecies extrapolations of nanoparticle biodistribution modeling. Nanomedicine (Lond) 2015;10:25–33.10.2217/nnm.14.60Search in Google Scholar PubMed
72. Wolfram J, Yang Y, Shen J, Moten A, Chen C, Shen H, et al. The nano-plasma interface: implications of the protein corona. Colloids Surf B Biointerfaces 2014;124:17–24.10.1016/j.colsurfb.2014.02.035Search in Google Scholar PubMed PubMed Central
73. Hajipour MJ, Raheb J, Akhavan O, Arjmand S, Mashinchian O, Rahman M, et al. Personalized disease-specific protein corona influences the therapeutic impact of graphene oxide. Nanoscale 2015;7:8978–94.10.1039/C5NR00520ESearch in Google Scholar PubMed
74. Hajipour MJ, Laurent S, Aghaie A, Rezaee F, Mahmoudi M. Personalized protein coronas: a “key” factor at the nanobiointerface. Biomater Sci 2014;2:1210–21.10.1039/C4BM00131ASearch in Google Scholar PubMed
75. Cho EJ, Holback H, Liu KC, Abouelmagd SA, Park J, Yeo Y. Nanoparticle characterization: state of the art, challenges, and emerging technologies. Mol Pharmaceutics 2013;10:2093–110.10.1021/mp300697hSearch in Google Scholar
76. Hwang do W, Choi H, Jang SC, Yoo MY, Park JY, Choi NE, et al. Noninvasive imaging of radiolabeled exosome-mimetic nanovesicle using (99m)Tc-HMPAO. Sci Rep 2015;5:15636.10.1038/srep15636Search in Google Scholar
77. Llop J, Gómez-Vallejo V, Gibson N. Quantitative determination of the biodistribution of nanoparticles: could radiolabeling be the answer? Nanomedicine 2013;8:1035–8.10.2217/nnm.13.91Search in Google Scholar
78. Jain TK, Reddy MK, Morales MA, Leslie-Pelecky DL, Labhasetwar V. Biodistribution, clearance, and biocompatibility of iron oxide magnetic nanoparticles in rats. Mol Pharm 2008;5:316–27.10.1021/mp7001285Search in Google Scholar
79. Owens DE, 3rd, Peppas NA. Opsonization, biodistribution, and pharmacokinetics of polymeric nanoparticles. Int J Pharm 2006;307:93–102.10.1016/j.ijpharm.2005.10.010Search in Google Scholar
80. Kreyling WG, Abdelmonem AM, Ali Z, Alves F, Geiser M, Haberl N, et al. In vivo integrity of polymer-coated gold nanoparticles. Nat Nanotechnol 2015;10:619–23.10.1038/nnano.2015.111Search in Google Scholar
81. de Barros AB, Tsourkas A, Saboury B, Cardoso VN, Alavi A. Emerging role of radiolabeled nanoparticles as an effective diagnostic technique. EJNMMI Res 2012;2:39.10.1186/2191-219X-2-39Search in Google Scholar
82. Ding XY, Hong CJ, Liu Y, Gu ZL, Xing KL, Zhu AJ, et al. Pharmacokinetics, tissue distribution, and metabolites of a polyvinylpyrrolidone-coated norcantharidin chitosan nanoparticle formulation in rats and mice, using LC-MS/MS. Int J Nanomedicine 2012;7:1723–35.10.2147/IJN.S29696Search in Google Scholar
83. Seo HJ, Nam SH, Im HJ, Park JY, Lee JY, Yoo B, et al. Rapid hepatobiliary excretion of micelle-encapsulated/radiolabeled upconverting nanoparticles as an integrated form. Sci Rep 2015;5:15685.10.1038/srep15685Search in Google Scholar
84. Zhao B, Sun L, Zhang W, Wang Y, Zhu J, Zhu X, et al. Secretion of intestinal goblet cells: a novel excretion pathway of nanoparticles. Nanomedicine 2014;10:839–49.10.1016/j.nano.2013.10.004Search in Google Scholar
85. Fisher DR. Internal dosimetry for systemic radiation therapy. Semin Radiat Oncol 2000;10:123–32.10.1016/S1053-4296(00)80049-1Search in Google Scholar
86. Stabin MG, Sparks RB, Crowe E. OLINDA/EXM: the second-generation personal computer software for internal dose assessment in nuclear medicine. J Nucl Med 2005;46:1023–7.Search in Google Scholar
87. Emfietzoglou D, Kostarelos K, Sgouros G. An analytic dosimetry study for the use of radionuclide-liposome conjugates in internal radiotherapy. J Nucl Med 2001;42:499–504.Search in Google Scholar
88. Kostarelos K, Emfietzoglou D. Tissue dosimetry of liposome-radionuclide complexes for internal radiotherapy: toward liposome-targeted therapeutic radiopharmaceuticals. Anticancer Res 2000;20:3339–45.Search in Google Scholar
89. Chen LC, Wu YH, Liu IH, Ho CL, Lee WC, Chang CH, et al. Pharmacokinetics, dosimetry and comparative efficacy of 188Re-liposome and 5-FU in a CT26-luc lung-metastatic mice model. Nucl Med Biol 2012;39:35–43.10.1016/j.nucmedbio.2011.06.010Search in Google Scholar PubMed
90. Walrand S, Hanin F-X, Pauwels S, Jamar F. Tumour control probability derived from dose distribution in homogeneous and heterogeneous models: assuming similar pharmacokinetics, 125Sn–177Lu is superior to 90Y–177Lu in peptide receptor radiotherapy. Phys Med Biol 2012;57:4263.10.1088/0031-9155/57/13/4263Search in Google Scholar PubMed
91. Lucas S, Feron O, Gallez B, Masereel B, Michiels C, Vander Borght T. Monte Carlo Calculation of radioimmunotherapy with 90 Y-, 177 Lu-, 131 I-, 124 I-, and 188 re-nanoobjects: choice of the best radionuclide for solid tumour treatment by using TCP and NTCP concepts. Comput Math Methods Med 2015;2015:284–360.10.1155/2015/284360Search in Google Scholar PubMed PubMed Central
92. Soundararajan A, Dodd III GD, Bao A, Phillips WT, McManus LM, Prihoda TJ, et al. Chemoradionuclide therapy with 186Re-labeled liposomal doxorubicin in combination with radiofrequency ablation for effective treatment of head and neck cancer in a nude rat tumor xenograft model. Radiology 2011;261:813–23.10.1148/radiol.11110361Search in Google Scholar PubMed PubMed Central
93. Kim DK, Kang B, Kim OY, Choi DS, Lee J, Kim SR, et al. EVpedia: an integrated database of high-throughput data for systemic analyses of extracellular vesicles. J Extracell Vesicles 2013;2:20384.10.3402/jev.v2i0.20384Search in Google Scholar PubMed PubMed Central
94. van Dommelen SM, Vader P, Lakhal S, Kooijmans SA, van Solinge WW, Wood MJ, et al. Microvesicles and exosomes: opportunities for cell-derived membrane vesicles in drug delivery. J Control Release 2012;161:635–44.10.1016/j.jconrel.2011.11.021Search in Google Scholar PubMed
95. Ohno S, Takanashi M, Sudo K, Ueda S, Ishikawa A, Matsuyama N, et al. Systemically injected exosomes targeted to EGFR deliver antitumor microRNA to breast cancer cells. Mol Ther 2013;21:185–91.10.1038/mt.2012.180Search in Google Scholar PubMed PubMed Central
96. Biancone L, Bruno S, Deregibus MC, Tetta C, Camussi G. Therapeutic potential of mesenchymal stem cell-derived microvesicles. Nephrol Dial Transplant 2012;27:3037–42.10.1093/ndt/gfs168Search in Google Scholar PubMed
97. Kowal J, Tkach M, Thery C. Biogenesis and secretion of exosomes. Curr Opin Cell Biol 2014;29:116–25.10.1016/j.ceb.2014.05.004Search in Google Scholar PubMed
98. Sun D, Zhuang X, Xiang X, Liu Y, Zhang S, Liu C, et al. A novel nanoparticle drug delivery system: the anti-inflammatory activity of curcumin is enhanced when encapsulated in exosomes. Mol Ther 2010;18:1606–14.10.1038/mt.2010.105Search in Google Scholar PubMed PubMed Central
99. Escudier B, Dorval T, Chaput N, André F, Caby MP, Novault S, et al. Vaccination of metastatic melanoma patients with autologous dendritic cell (DC) derived-exosomes: results of thefirst phase I clinical trial. J Transl Med 2005;3:10.10.1186/1479-5876-3-10Search in Google Scholar PubMed PubMed Central
100. Morse MA, Garst J, Osada T, Khan S, Hobeika A, Clay TM, et al. A phase I study of dexosome immunotherapy in patients with advanced non-small cell lung cancer. J Transl Med 2005;3:9.10.1186/1479-5876-3-9Search in Google Scholar PubMed PubMed Central
101. Dai S, Wei D, Wu Z, Zhou X, Wei X, Huang H, et al. Phase I clinical trial of autologous ascites-derived exosomes combined with GM-CSF for colorectal cancer. Mol Ther 2008;16:782–90.10.1038/mt.2008.1Search in Google Scholar PubMed PubMed Central
102. Mignot G, Roux S, Thery C, Segura E, Zitvogel L. Prospects for exosomes in immunotherapy of cancer. J Cell Mol Med 2006;10:376–88.10.1111/j.1582-4934.2006.tb00406.xSearch in Google Scholar PubMed PubMed Central
103. Gyorgy B, Hung ME, Breakefield XO, Leonard JN. Therapeutic applications of extracellular vesicles: clinical promise and open questions. Annu Rev Pharmacol Toxicol 2015;55:439–64.10.1146/annurev-pharmtox-010814-124630Search in Google Scholar PubMed PubMed Central
104. Morishita M, Takahashi Y, Nishikawa M, Sano K, Kato K, Yamashita T, et al. Quantitative analysis of tissue distribution of the B16BL6-derived exosomes using a streptavidin-lactadherin fusion protein and iodine-125-labeled biotin derivative after intravenous injection in mice. J Pharm Sci 2015;104:705–13.10.1002/jps.24251Search in Google Scholar PubMed
105. Smyth T, Kullberg M, Malik N, Smith-Jones P, Graner MW, Anchordoquy TJ. Biodistribution and delivery efficiency of unmodified tumor-derived exosomes. J Control Release 2015;199:145–55.10.1016/j.jconrel.2014.12.013Search in Google Scholar PubMed PubMed Central
106. Hood JL, San RS, Wickline SA. Exosomes released by melanoma cells prepare sentinel lymph nodes for tumor metastasis. Cancer Res 2011;71:3792–801.10.1158/0008-5472.CAN-10-4455Search in Google Scholar PubMed
107. Zhuang X, Xiang X, Grizzle W, Sun D, Zhang S, Axtell RC, et al. Treatment of brain inflammatory diseases by delivering exosome encapsulated anti-inflammatory drugs from the nasal region to the brain. Mol Ther 2011;19:1769–79.10.1038/mt.2011.164Search in Google Scholar PubMed PubMed Central
108. Witwer KW, Buzas EI, Bemis LT, Bora A, Lässer C, Lötvall J, et al. Standardization of sample collection, isolation and analysis methods in extracellular vesicle research. J Extracell Vesicles 2013;2:20360.10.3402/jev.v2i0.20360Search in Google Scholar PubMed PubMed Central
109. Jang SC, Kim OY, Yoon CM, Choi DS, Roh TY, Park J, et al. Bioinspired exosome-mimetic nanovesicles for targeted delivery of chemotherapeutics to malignant tumors. ACS Nano 2013;7:7698–710.10.1021/nn402232gSearch in Google Scholar PubMed
110. Takahashi Y, Nishikawa M, Shinotsuka H, Matsui Y, Ohara S, Imai T, et al. Visualization and in vivo tracking of the exosomes of murine melanoma B16-BL6 cells in mice after intravenous injection. J Biotechnol 2013;165:77–84.10.1016/j.jbiotec.2013.03.013Search in Google Scholar PubMed
111. Colombo M, Moita C, van Niel G, Kowal J, Vigneron J, Benaroch P, et al. Analysis of ESCRT functions in exosome biogenesis, composition and secretion highlights the heterogeneity of extracellular vesicles. J Cell Sci 2013;126:5553–65.10.1242/jcs.128868Search in Google Scholar PubMed
112. Wiklander OP, Nordin JZ, O’Loughlin A, Gustafsson Y, Corso G, Mäger I, et al. Extracellular vesicle in vivo biodistribution is determined by cell source, route of administration and targeting. J Extracell Vesicles 2015;4:26316.10.3402/jev.v4.26316Search in Google Scholar PubMed PubMed Central
©2016, Dong Soo Lee et al., published by De Gruyter
This work is licensed under the Creative Commons Attribution-NonCommercial-NoDerivatives 3.0 License.
Articles in the same Issue
- Frontmatter
- In this issue
- What’s Up?
- What’s up in nanomedicine?
- Special section Radionanomedicine
- Guest Editorial
- Radionanomedicine
- Review
- Translational radionanomedicine: a clinical perspective
- Perspective
- A potentially versatile nano-platform
- Regular contributions
- Original Articles
- Preparation and characterization of nanoparticles composed of methylated N-(4-N,N-dimethyl aminobenzyl) chitosan for oral delivery of cyclosporine A
- Formulation of gentamicin as surface modified self-nanoemulsifying formulations (SNEFs) improves its anti-pneumococcal activity
Articles in the same Issue
- Frontmatter
- In this issue
- What’s Up?
- What’s up in nanomedicine?
- Special section Radionanomedicine
- Guest Editorial
- Radionanomedicine
- Review
- Translational radionanomedicine: a clinical perspective
- Perspective
- A potentially versatile nano-platform
- Regular contributions
- Original Articles
- Preparation and characterization of nanoparticles composed of methylated N-(4-N,N-dimethyl aminobenzyl) chitosan for oral delivery of cyclosporine A
- Formulation of gentamicin as surface modified self-nanoemulsifying formulations (SNEFs) improves its anti-pneumococcal activity