Intelligent drug delivery systems for the treatment of solid tumors
-
Triantafyllos Stylianopoulos
Triantafyllos Stylianopoulos is an Assistant Professor of Mechanical Engineering and Head of the Cancer Biophysics Laboratory at the University of Cyprus. He received a diploma in Chemical Engineering from National Technical University of Athens, Greece (2003) and a PhD also in Chemical Engineering from the University of Minnesota, USA (2008). He performed his post-doctoral training at the Department of Radiation Oncology at Harvard Medical School and Massachusetts General Hospital. Dr. Stylianopoulos has co-authored over 50 peer-reviewed articles in the fields of tumor pathophysiology, drug delivery and biomechanics. He is recipient of a highly selective European Research Council (ERC) Starting Grant. Dr. Stylianopoulos is a member of the American Society of Mechanical Engineers, the Biomedical Engineering Society of the US, the European Society for Clinical Nanomedicine and the European Society of Biomechanics.


Abstract
The rationale for the use of nanoparticle formulations to treat cancer is based on the ability of these particles to facilitate selective delivery of drugs to the tumor site, reducing adverse effects and improving therapeutic outcomes. Current clinically approved nanomedicines have managed to reduce adverse effects significantly but the increase in overall survival is modest in many cases. Therefore, even though the goal of a better quality of life for the cancer patients has been achieved in large part, the increase in life expectancy still remains a critical challenge. Abnormalities in the tumor micro-environment prevent homogeneous distribution of nanoparticles to the interior of the tumor, decreasing the efficacy of the drug. Intelligent drug delivery systems offer new hope for overcoming these physiological barriers posed by the tumor and have the potential to provide more effective treatments. This review discusses the barriers to the delivery of nanomedicines to solid tumors, suggests design considerations that could optimize delivery and reviews promising intelligent drug delivery systems that have been developed to date.
Introduction
Development of nanoparticle formulations for tumor detection and treatment has been a field of intense scientific efforts for over two decades. During this period of time tens of thousands of research articles have been published, eight nanoparticle formulations have been already approved for clinical use and many more formulations have entered clinical trials (1–3). Table 1 presents the nanomedicines that have been approved for use in humans along with their indication. Doxil® (or Caelyx®) is a 100 nm PEGylated liposome that contains doxorubicin and it was the first nanoparticle formulation that was granted approval in 1995 and it is currently used for the treatment of HIV-related Kaposi’s sarcoma, metastatic ovarian cancer and metastatic breast cancer; DaunoXome® – a 50 nm liposomal daunorubicin particle – was approved in 1996 for the treatment of HIV-related Kaposi’s sarcoma; Myocet® is a 180 nm liposomal doxorubicin particle approved in 2001 and it is used in Europe and Canada for the treatment of metastatic breast cancer; Abraxane® is a 130 nm albumin-bound paclitaxel that disintegrates in blood plasma to a 10 nm particle, it was approved in 2005 for metastatic breast cancers and recently for pancreatic ductal adenocarcinomas; Lipusu® – a liposomal paclitaxel particle – was approved in 2006 in China for breast and non-small-cell lung cancer; Genexol-PM® – a 20–50 nm micelle of paclitaxel – was approved in South Korea in 2007 for metastatic breast cancer; MM398 – a 100 nm liposomal formulation of irinotecan – was approved in 2014 for pancreatic ductal adenocarcinomas and PICN – a 100–110 nm formulation of paclitaxel stabilized with polymers and lipids – was approved in India in 2014 for metastatic breast cancers.
Clinically approved nanoparticle formulations for treatment of solid tumors.
| Generic name | Trade name(s) | Size | Indication |
|---|---|---|---|
| Pegylated liposomal doxorubicin | Doxil®/Caelyx® | 100 nm | HIV-related Kaposi’s sarcoma |
| Metastatic ovarian cancer | |||
| Metastatic breast cancer | |||
| Liposomal daunorubicin | DaunoXome® | 50 nm | HIV-related Kaposi’s sarcoma |
| Liposomal doxorubicin | Myocet® | 180 nm | Metastatic breast cancer |
| Albumin-bound paclitaxel | Abraxane® | 10 nm (following disintegration in blood) | Metastatic breast cancer Pancreatic ductal adenocarcinoma |
| Liposomal paclitaxel | Lipusu | Not available | Breast and non-small-cell lung cancer |
| Micelle of paclitaxel | Genexol-PM® | 20–50 nm | Metastatic breast cancer |
| Liposomal formulation of irinotecan | MM-398® | 100 nm | Pancreatic ductal adenocarcinoma |
| Paclitaxel injection concentrate for nanodispersion | PICN® | 100 nm | Metastatic breast cancer |
All these clinically approved cancer nanomedicines make use of the enhanced permeability and retention (EPR) effect, i.e. passive accumulation into the tumor. The EPR effect is based on the fact that in many tumors some of their blood vessels have larger vessel wall openings than the vessel wall openings of normal vessels and thus, large nanoparticles will selectively accumulate into the tumor tissue, reducing adverse effects and increasing the efficacy of the drug. Physiological barriers posed by the tumor micro-environment, however, hinder delivery of nanoparticles and result in modest survival benefits (1, 3–5). Inefficient delivery of nanoparticle formulations is also one of the main reasons that despite the vast number of scientific articles published in the field of cancer nanomedicine only few of them managed to reach the market. To overcome these barriers and optimize nanoparticle delivery to solid tumors a careful design of nanoparticle delivery systems is required. Here, we first discuss physiological barriers to the effective delivery of nanomedicines to tumors, subsequently we provide general design considerations and present intelligent drug delivery systems that have been developed to date.
Physiological barriers to the effective delivery of nanomedicines to solid tumors
Three parameters of the tumor micro-environment determine the accessibility of drugs to solid tumors: the efficiency of the vascular network, the permeability of the tumor blood vessel wall and the composition of the tumor stroma (6). These parameters might vary considerably among tumor types, between a tumor and its metastases and in the same tumor during progression making effective delivery of drugs a tumor- and patient-specific problem. During tumor progression, cancer cells induce an angiogenic process by increasing the levels of pro-angiogenic factors, such as vascular endothelial growth factor (VEGF), platelet derived growth factor (PDGF) and basic fibroblast growth factor (bFGF). Angiogenesis results in the formation of new tumor blood vessels, which are immature and more permeable than normal vessels (7). While in most normal vessels the pores of the vessel wall do not exceed 12 nm, in vivo studies in mice bearing tumors have shown that in tumor vessels the pores can be as large as 2 μm (8). Therefore, nanoparticles with a size larger than 12 nm will selectively cross the wall of tumor vessels. This is the basis of the EPR effect, which led to the use of nanotechnology for cancer treatment. All blood vessels in a tumor, however, are not equally permeable and also the degree of vascular permeability varies among tumor types. Hyper-permeable tumors include but are not limited to a subset of breast cancers, glioblastomas, melanomas and ovarian carcinomas, while pancreatic ductal adenocarcinomas are poorly permeable (9).
The hyper-permeability of tumor blood vessels might allow on one hand the extravasation of nanoparticles from some regions of the tumor but on the other hand results in excessive fluid loss from the vascular to the interstitial space, which reduces perfusion of downstream tumor vessels and thus, the systemic delivery of drugs through these vessels. Another cause of hypo-perfusion is the generation of physical forces due to the growth of the tumor in the confined space of the host tissue. These forces deform and eventually collapse intratumoral blood vessels (10, 11). Vessel compression reduces the effective cross-sectional area for blood flow while vessel collapse results in large avascular regions within the tumor and the formation of necrotic tissue. Therefore, vessel hyper-permeability and compression can render tumors hypo-perfused, which reduces the amount of nanoparticles that reach the tumor site.
Physical forces are determined in large part from the amount of extracellular matrix components (i.e. collagen fibers, proteoglycans, hyaluronic acid) and cancer associated fibroblasts that comprise the tumor micro-environment and constitute in large part the tumor stroma (12). Tumors rich in stroma, such as pancreatic ductal adenocarcinomas and a subset of breast tumors, have abundant collapsed vessels and are hypo-perfused. It is easy to understand that for hypo-perfused tumors with inefficient vascular function, vessel hyper-permeability and the EPR have no effect on the delivery of nanomedicines since drugs will not be able to reach the tumor site. Tumor stroma hinders delivery of drugs with two additional ways: A rich tumor stroma reduces the available space for interstitial transport. The pores in the interstitial space of tumors – through which particles are moving – can be comparable in size with the size of large nanoparticles and thus, these particles are getting trapped. As a result, large nanoparticles cannot effectively penetrate the tumor interstitial space and they are concentrated in the perivascular region, causing an heterogeneous intratumoral distribution (1, 13). The tumor stroma inhibits not only the transport of nanoparticles but also the transport of interstitial fluid. The excessive fluid that enters the tumor interstitial space due to the hyper-permeability of the tumor blood vessels in conjunction with the dysfunction of intratumoral lymphatics results in fluid accumulation in the interstitial space. Fluid accumulation, in turn, causes a uniform elevation of the interstitial fluid pressure (IFP). IFP in tumors can be equal to the micro-vascular pressure, which renders diffusion the only mechanism of transport across the tumor vessel wall and in the tumor interior (14). Diffusion, however, is inversely proportional to the size of the nanoparticles and also depends on its shape, resulting in a size- and shape-dependent delivery.
Apart from vascular structure and stroma composition, other parameters of the tumor micro-environment that have to be considered are the negatively charged glycocalyx of vascular endothelial cells and the negatively charged molecules of hyaluronic acid of the tumor interstitial space. These charged components of the tumor develop electrostatic interactions with charged nanoparticles, which can affect significantly their transport properties.
Design considerations
Particle size, shape and charge are critical design parameters that determine the fate of a nanoparticle (15) (Figure 1). Nanoparticles have to be small enough to be able to travel across the pores of the tumor vessel wall and through the pores of the tumor interstitial space. At the same time, the particles should be large enough so that they will not cross the pores of the vessel wall in normal tissues. The pores in normal vessels are smaller than 12 nm, and thus this can be considered as a low bound for nanoparticle size. In addition, for a particle to be able to extravasate, it needs to have a size of at least 1.5 times smaller than the size of the pores of the vessel wall, and as we discussed in the previous section, this transport is size-dependent (16). Therefore, very large particles (>100 nm in diameter) should be able to cross some of the blood vessels in hyper-permeable tumors but in low amounts. Furthermore, particles larger than 50 nm in diameter cannot penetrate deep into the tumor interstitial space (17), particularly in stroma-rich tumors, and will most likely cause only local effects. Taken together, we conclude that as far as transport is concerned the ideal particle size should be in the range of 12–50 nm. The smaller the particle the more efficient its transport will be but the amount of drug the particle can carry decreases. Therefore, an optimal balance between size and drug load has to be stricken. Apart from the load capacity, the potency of the drug and the drug release kinetics of nanocarriers are another important parameters for their efficacy. For instance, MM-398® even though it is a large – 100 nm – particle, it was recently approved for the treatment of pancreatic cancers, which are considered to be hypo-perfused and have poorly permeable blood vessels. MM-398® contains irinotecan, which is a very potent drug and presumably because of suitable release of the drug from the particle, it has been effective.
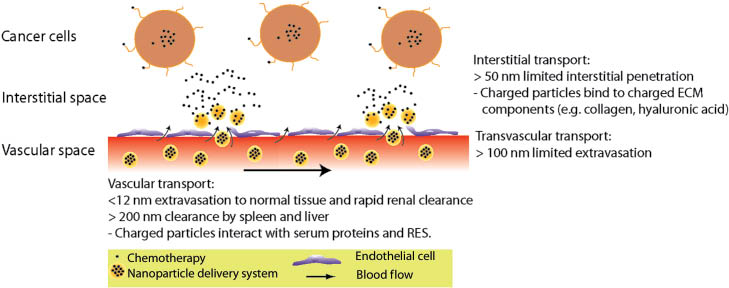
Barriers to nanoparticle delivery. Vascular transport is compromised for nanoparticles smaller than 6 nm in diameter due to rapid renal clearance, while particles less than 12 nm are likely to extravasate in large amounts to normal tissues. Nanoparticle formulations larger than 200 nm are subject to rapid clearance by the liver and spleen and a high surface charge density (either positive or negative) increases interactions with serum proteins and the reticuloendothelial system (RES). Transvascular transport of nanoparticles larger than 100 nm is limited to only the very leaky tumor vessels and to small amounts. Interstitial transport is compromised for nanoparticles larger than 50 nm owing to the limited penetration of the particles into the dense interstitial matrix of many tumors. Negatively charged nanoparticles might develop electrostatic attractive forces with collagen fibers that have a slight positive charge, while positively charged particles can bind to chains of hyaluronic acid that exhibit a high negative charge.
Transvascular and interstitial transport can be enhanced with the use of elongated particles. For nanoparticles of the same volume and structure, elongated particles have superior transport properties compared to their spherical counterparts (15, 18). As far as the surface charge density of the particles is concerned, particles with a small cationic surface charge have superior transvascular flux compared to their anionic or neutral counterparts (19, 20), but neutral particles are ideal for interstitial transport because they do not interact with negatively charged glycosaminoglycans (i.e. hyaluronic acid) or with collagen fibers that carry a slightly positive charge (21, 22).
Other transport steps involved in drug delivery are vascular transport and cellular uptake. Vascular transport is described by the circulation time or blood half life of the particle. Opsonization by serum proteins, renal clearance and clearance from the reticuloendothelial system determine the circulation time of nanoparticles. Particles with sizes less than 6 nm are subject to rapid renal clearance and larger than 200 nm exhibit clearance by the liver and the spleen, while a high surface charge density (either positive or negative) increases interactions with serum proteins and the reticuloendothelial system (3, 23–26). In this respect, particles with neutral surface charge density, spherical or elongated, are ideal for prolong vascular transport. This is achieved in most cases with PEGylation of nanoparticles by surface modification with polyethylene glycols.
Cellular uptake also depends on size, shape and charge. For the size range of our interest (i.e. 12–50 nm) cellular uptake should not depend on the diameter of the nanoparticle. Regarding the effect of the particle shape no conclusive guidelines can be obtained. Experiments have shown that the angle of contact with the cell membrane determines the internalization rate with particles contacting the cells perpendicular to their long axis to be internalized faster (27). These experiments, however, were performed with larger particles, in the micro-meter scale. Finally, cationic particles have shown enhanced cellular uptake compared to neutral or anionic particles (28).
Intelligent design of drug delivery systems
Design of intelligent drug delivery systems has the ability to deal with the abnormalities of the tumor micro-environment. One promising solution is the development of multistage nanoparticles that shrink in size when they enter the interstitial space of the tumor. Particles have been also developed that target not only cancer cells but also the tumor stroma to alleviate physical forces. Another category of intelligent drug delivery systems are stimuli-responsive nanoparticles that respond to parameters of the tumor micro-environment (e.g. enzyme- or pH-responsive particles) or to external sources (e.g. ultrasound, magnetic field, heat, light) to release their therapeutic load.
Multistage delivery systems
Multistage drug delivery systems are initially large nanoparticles so that they can ensure long circulation times, high load capacity and selective delivery to the tumor site through the EPR effect (29–31). When the nanoparticles enter the tumor interstitial space, they decrease in size to enable rapid diffusion and uniform distribution in the interior of the tumor. Shrinkage of the nanoparticles is achieved with a proper stimulus from the tumor micro-environment. Proteolytic degradation by matrix metalloproteinases (MMPs) is one such possible mechanism. Many tumors exhibit an overexpression of MMPs, some of which (e.g. MMP-2 and MMP-9) can degrade collagen. Multistage nanoparticles ~100 nm in diameter have been synthesized by gelatin (a type of denatured collagen) and have shown to have the ability to undergo degradation at high MMP levels (Figure 2). Specifically, experiments confirmed a proof-of-principle of the emerging multistage nanoparticle hypothesis using 100 nm gelatin particles containing 10-nm quantum dots as a stand-in for therapeutic or imaging nanocarriers. The gelatin nanoparticles when injected directly in the tumor interior were able to diffuse in a longer distance from the injection point compared to silica, non-degradable particles of the same size, presumably due to the degradation of the gelatin and the release of the smaller, secondary particles.
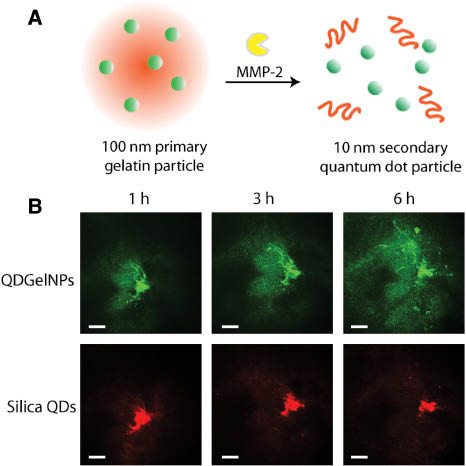
Multistage nanoparticle delivery system. (A) An 100 nm primary nanoparticle made by gelatin is cleaved by enzymes (MMP-2) in the tumor interior and releases secondary 10 nm quantum dot particles. (B) Proof-of-principle of multistage delivery system. Co-injection of gelatin multistage nanoparticles (QDGelNPs) and silica non-degradable particles (Silica QDs) of same size directly to the tumor interior in mice shows the superior penetration of the multistage system (Adapted with permission from (29). Copyright (2011) Proceedings of the National Academy of Science, USA).
Tumor-modifying delivery systems
While multistage drug delivery systems modify the properties of the nanoparticle to optimize intratumoral penetration, tumor-modifying delivery systems alter the tumor micro-environment. Specifically, nanoparticle formulations have been developed that target not only cancer cells but also the tumor stroma, a major barrier to drug delivery (32). Depletion of stromal cells can decompress blood vessels and improve perfusion and nanoparticle delivery to the tumor tissue. Additionally, stromal cells secrete collagen, which along with the cells hinder interstitial diffusion and increase IFP. Therefore, stromal cell depletion can improve the penetration of large nanoparticles in the tumor interior. Indeed, studies have shown that 120 nm particles that target α-smooth muscle actin-expressing stromal cells were able to increase perfusion and delivery and decrease IFP and metastasis in mice bearing tumors (32). Apart from stromal cells other potential targets of the tumor micro-environment are collagen and hyaluronic acid.
Enzyme responsive delivery systems
MMP-2 responsive nanoparticles are covered by a shell of long PEG chains on their surface (e.g. drug loaded liposomes) (33). These chains increase the particle size but protects it from serum proteins. The particles are linked to the PEG chains with MMP-2 sensitive bonds and thus, when the nanoparticle formulation enters the tumor interior the bonds are cleaved decreasing the size of the particle and allowing for better interactions of the particle with cancer cells (Figure 3). Particles might be also functionalized with cancer cell targeting ligands, the ligands after cleavage of the PEG shell become exposed, and this can enhance intracellular delivery. Using this methodology, siRNA-loaded nanoparticles improved by approximately 70% the gene-silencing activity in mice bearing fibrosarcomas (34).
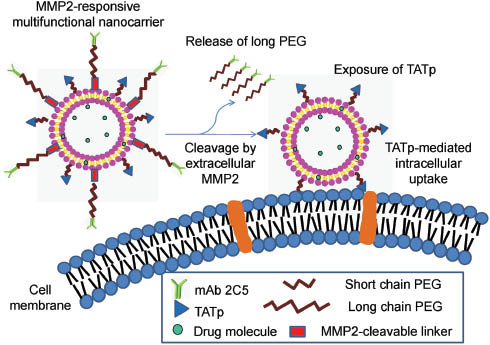
Enzyme responsive delivery system. MMP-2 responsive multifunctional nanocarrier undergoes cleavage of long PEG chains by extracellular MMP-2, reducing in size and exposing its binding ligands. Abbreviations: mAb 2C5: antinucleosome monoclonal antibody, TATp: cell penetrating peptide. Reprinted with permission from (33). Copyright (2012) American Chemical Society).
An advantage of enzyme responsive systems is that MMPs and particularly MMP-2 and MMP-9 play a crucial role in angiogenesis and cancer cell invasion and metastasis by cleaving away the extracellular matrix and creating space for formation of new vessels and movement of cells. Therefore, levels of MMP-2 and MMP-9 are high at perivascular regions and at the tumor margin where high vascular density is observed and these are also the regions where nanoparticles are most likely to extravasate. It should be noticed, however, that MMPs are also present, in lower amounts, in the blood plasma and in normal tissues. This can cause disintegration of the nanoparticles either in the plasma, decreasing the circulation time or in normal tissues causing adverse effects. The kinetics of nanoparticle degradation must be carefully adjusted so that the system to be responsive only in the tumor.
pH responsive delivery systems
The irregular tumor micro-vasculature creates an acidic micro-environment, which affects the normal pH values of the tissue (35, 36). As a result, pH values in the tumor vary from physiological levels (~7.4) at perivascular regions to values as low as 6.5 away from the vessels. Drug loaded, pH-sensitive nanoparticles have been developed, which are able to release their therapeutic load triggered by subtle changes of the pH. Chemotherapeutic molecules are very small (<1 nm) and diffuse rapidly in the tumor interior once they have been released. PH-sensitive liposomes have been synthesized and their efficacy was tested in mice bearing tumors, exhibiting improved anti-tumor activity (37) and reduced toxicity (38). However, acidic regions are usually far from tumor blood vessels – in a distance larger than 300 μm – and heterogeneously distributed (1, 35). Therefore, interstitial transport still remains an issue for this type of delivery systems because the nanoparticles should be able to travel through the pores of the interstitial matrix from the blood vessels to the acidic regions of the tumor.
External stimuli-responsive delivery systems
Nanoparticle formulations are being developed to respond to an external source and particularly to a magnetic field, ultrasound, heat or light (36, 39, 40). The external source is used either to increase the concentration of the nanoparticles to the tumor site or to locally activate the particles in order to release the drug. Nanoparticle delivery systems made by magnetite, which due to their superior magnetic properties are also referred to as superparamagnetic iron oxide nanoparticles, are guided by a magnetic field applied externally to the tumor region, increasing their concentration. These particles can be also incorporated into liposomes, micelles and other nanoparticle systems and undergo functionalization with moieties for cancer cell targeting (36, 39). Concentration of magnetic nanoparticles to the tumor site, however, is not necessarily related to increased intratumoral distribution. Barriers to transvascular and interstitial transport can still be a challenge and careful design is required. Ultrasound is a non-invasive imaging modality with a wide range of safe clinical applications. The rationale for the use of ultrasound in cancer nanomedicine is the fact that sound waves can destroy the nanoparticles and cause the release of the drug, referred to as sonoporation. In another methodology, when micro-bubbles are co-injected with nanoparticles, the sound waves break the bubbles disrupting locally the blood flow and altering transiently the size of the pores of the vessel wall. These effects can increase the probability of the nanoparticles to extravasate into the tumor.
Finally, local controlled release of drugs can be also achieved with heat or light. Thermo-sensitive and light-sensitive nanoparticles have been developed with perhaps the most promising strategy being photo-sensitive particles that respond to photo-dynamic treatments (41, 42).
From the above methodologies for the use of an external stimulus to improve efficacy of nanomedicines, two formulations have managed to reach clinical trials: the thermosensitive liposome containing doxorubicin, ThermoDox, for the treatment of breast cancers and hepatocellular carcinomas and the magnetic nanoparticle, NanoTherm, for the treatment of glioblastomas (39).
Conclusions
Intelligent drug delivery systems have the potential to provide fresh hope to the use of nanomedicine for the selective treatment of solid tumors, utilizing both the abnormal tumor micro-environment and advances in nanotechnology. To date design strategies are taking advantage of the size-dependence of nanoparticle delivery and also endogenous and exogenous stimuli. Utilization of the shape- and charge-dependence could potentially lead to better results and it is a promising area of research. Nanoparticle targeting to cancer cells and the rate of release of the drug from the nanoparticles are other important design parameters (3). We have to consider, however, that cancer is a continuously evolving disease with mechanisms to protect itself from the action of nanoparticles by developing drug resistance. Optimizing delivery of nanomedicines even though might not lead to complete cure due to therapy resistance, is a pre-requisite for better treatments. Additionally, solid tumors vary significantly from one type to the other, between the primary tumor and its metastases and within the same tumor during progression. Design criteria for nanoparticles are different for any of these cases and for that reason drug delivery systems should be cancer- and patient-specific. Biomarkers to provide information for the state of a tumor micro-environment would be beneficial for the selection of the proper nanoparticle properties. Therefore, another promising area of research is the development of biomarkers and imaging techniques to characterize the state of a tumor and also to image the drug delivery system. Emerging imaging approaches have the potential to help in this direction (43).
Review summary
Current nanomedicines have succeeded in improving quality of life but increase in overall survival still remains a critical challenge.
Tumor abnormal micro-environment hinders effective delivery of large nanoparticles, which reduces treatment efficacy.
Particle size, shape and charge determine in large part the delivery of nanomedicines; proper particle size is in the range of 12–50 nm, elongated particles have better transport properties and neutral particles have longer circulation time and better interstitial transport.
Multistage nanoparticle delivery systems are initially large in order to enable long circulation times, contain high doses of drug, and ensure selective delivery to tumors. These particles shrink in size when they reach the tumor interior for optimal intratumoral penetration.
Tumor-modifying delivery systems target not only cancer cells, but also components of the tumor stroma to improve perfusion and interstitial penetration.
Stimuli-responsive delivery systems respond to parameters of the tumor micro-environment (e.g. enzyme- or pH-responsive particles) or to external sources (e.g. ultrasound, magnetic field, heat, light) to release their therapeutic load.
About the author

Triantafyllos Stylianopoulos is an Assistant Professor of Mechanical Engineering and Head of the Cancer Biophysics Laboratory at the University of Cyprus. He received a diploma in Chemical Engineering from National Technical University of Athens, Greece (2003) and a PhD also in Chemical Engineering from the University of Minnesota, USA (2008). He performed his post-doctoral training at the Department of Radiation Oncology at Harvard Medical School and Massachusetts General Hospital. Dr. Stylianopoulos has co-authored over 50 peer-reviewed articles in the fields of tumor pathophysiology, drug delivery and biomechanics. He is recipient of a highly selective European Research Council (ERC) Starting Grant. Dr. Stylianopoulos is a member of the American Society of Mechanical Engineers, the Biomedical Engineering Society of the US, the European Society for Clinical Nanomedicine and the European Society of Biomechanics.
Acknowledgments
The manuscript is based on the reviews: Jain RK and Stylianopoulos T, Nat Rev Clin Oncol, 7, 653–664, 2010, and Stylianopoulos T and Jain RK, Nanomedicine J, 2015. This work was supported by the European Commission, Marie-Curie Reintegration grant Cancer Nanomedicine (No. PIRG08-GA-2010-276894).
Conflict of interest statement: The author states no conflict of interest. He has read the journal’s Publication ethics and publication malpractice statement available at the journal’s website and hereby confirms that he complies with all its parts applicable to the present scientific work.
References
1. Jain RK, Stylianopoulos T. Delivering nanomedicine to solid tumors. Nat Rev Clin Oncol 2010;7:653–64.10.1038/nrclinonc.2010.139Suche in Google Scholar PubMed PubMed Central
2. Bourzac K. Nanotechnology: carrying drugs. Nature 2012;491:S58–60.10.1038/491S58aSuche in Google Scholar PubMed
3. Stylianopoulos T, Jain RK. Design considerations for nanotherapeutics in oncology. Nanomedicine 2015;11:1893–1907.10.1016/j.nano.2015.07.015Suche in Google Scholar PubMed PubMed Central
4. O’Brien ME, Wigler N, Inbar M, Rosso R, Grischke E, Santoro A, et al. Reduced cardiotoxicity and comparable efficacy in a phase III trial of pegylated liposomal doxorubicin HCl (CAELYX/Doxil) versus conventional doxorubicin for first-line treatment of metastatic breast cancer. Ann Oncol 2004;15:440–9.10.1093/annonc/mdh097Suche in Google Scholar PubMed
5. Gill PS, Wernz J, Scadden DT, Cohen P, Mukwaya GM, von Roenn JH, et al. Randomized phase III trial of liposomal daunorubicin versus doxorubicin, bleomycin, and vincristine in AIDS-related Kaposi’s sarcoma. J Clin Oncol 1996;14:2353–64.10.1200/JCO.1996.14.8.2353Suche in Google Scholar PubMed
6. Chauhan VP, Stylianopoulos T, Boucher Y, Jain RK. Delivery of molecular and nanomedicine to tumors: Transport barriers and strategies. Annu Rev Chem Biomol Eng 2011;2:281–98.10.1146/annurev-chembioeng-061010-114300Suche in Google Scholar PubMed
7. Carmeliet P, Jain RK. Molecular mechanisms and clinical applications of angiogenesis. Nature 2011;473:298–307.10.1038/nature10144Suche in Google Scholar PubMed PubMed Central
8. Hobbs SK, Monsky WL, Yuan F, Roberts WG, Griffith L, Torchilin VP, et al. Regulation of transport pathways in tumor vessels: role of tumor type and microenvironment. Proc Natl Acad Sci USA 1998;95:4607–12.10.1073/pnas.95.8.4607Suche in Google Scholar PubMed PubMed Central
9. Stylianopoulos T, Jain RK. Combining two strategies to improve perfusion and drug delivery in solid tumors. Proc Natl Acad Sci USA 2013;110:18632–7.10.1073/pnas.1318415110Suche in Google Scholar PubMed PubMed Central
10. Stylianopoulos T, Martin JD, Snuderl M, Mpekris F, Jain SR, Jain RK. Coevolution of solid stress and interstitial fluid pressure in tumors during progression: implications for vascular collapse. Cancer Res 2013;73:3833–41.10.1158/0008-5472.CAN-12-4521Suche in Google Scholar PubMed PubMed Central
11. Jain RK, Martin JD, Stylianopoulos T. The role of mechanical forces in tumor progression and therapy. Annu Rev Biomed Eng 2014;16:321–46.10.1146/annurev-bioeng-071813-105259Suche in Google Scholar PubMed PubMed Central
12. Stylianopoulos T, Martin JD, Chauhan VP, Jain SR, Diop-Frimpong B, Bardeesy N, et al. Causes, consequences, and remedies for growth-induced solid stress in murine and human tumors. Proc Natl Acad Sci USA 2012;109:15101–8.10.1073/pnas.1213353109Suche in Google Scholar PubMed PubMed Central
13. Yuan F, Leunig M, Huang SK, Berk DA, Papahadjopoulos D, Jain RK. Microvascular permeability and interstitial penetration of sterically stabilized (stealth) liposomes in a human tumor xenograft. Cancer Res 1994;54:3352–6.Suche in Google Scholar
14. Boucher Y, Baxter LT, Jain RK. Interstitial pressure gradients in tissue-isolated and subcutaneous tumors: implications for therapy. Cancer Res 1990;50:4478–84.Suche in Google Scholar
15. Chauhan VP, Jain RK. Strategies for advancing cancer nanomedicine. Nat Mater 2013;12:958–62.10.1038/nmat3792Suche in Google Scholar PubMed PubMed Central
16. Chauhan VP, Stylianopoulos T, Martin JD, Popović Z, Chen O, Kamoun WS, et al. Normalization of tumour blood vessels improves the delivery of nanomedicines in a size-dependent manner. Nat Nanotechnol 2012;7:383–388.10.1038/nnano.2012.45Suche in Google Scholar PubMed PubMed Central
17. Popovic Z, Liu W, Chauhan VP, Lee J, Wong C, Greytak AB, et al. A nanoparticle size series for in vivo fluorescence imaging. Angew Chem Int Ed Engl 2010;49:8649–52.10.1002/anie.201003142Suche in Google Scholar PubMed PubMed Central
18. Chauhan VP, Popovic Z, Chen O, Cui J, Fukumura D, Bawendi MG, et al. Fluorescent nanorods and nanospheresfor real-time in vivo probing of nanoparticle shape-dependent tumor penetration. Angew Chem Int Ed Engl 2011;50:11417–20.10.1002/anie.201104449Suche in Google Scholar PubMed PubMed Central
19. Stylianopoulos T, Soteriou K, Fukumura D, Jain RK. Cationic nanoparticles have superior transvascular flux into solid tumors: Insights from a mathematical model. Ann Biomed Eng 2013;41:68–77.10.1007/s10439-012-0630-4Suche in Google Scholar PubMed PubMed Central
20. Dellian M, Yuan F, Trubetskoy VS, Torchilin VP, Jain RK. Vascular permeability in a human tumour xenograft: molecular charge dependence. Br J Cancer 2000;82:1513–8.Suche in Google Scholar
21. Lieleg O, Baumgartel RM, Bausch AR. Selective filtering of particles by the extracellular matrix: an electrostatic bandpass. Biophys J 2009;97:1569–77.10.1016/j.bpj.2009.07.009Suche in Google Scholar PubMed PubMed Central
22. Stylianopoulos T, Poh MZ, Insin N, Bawendi MG, Fukumura D, Munn LL, et al. Diffusion of particles in the extracellular matrix: The effect of repulsive electrostatic interactions. Biophys J 2010;99:1342–9.10.1016/j.bpj.2010.06.016Suche in Google Scholar PubMed PubMed Central
23. Longmire M, Choyke PL, Kobayashi H. Clearance properties of nano-sized particles and molecules as imaging agents: considerations and caveats. Nanomedicine (Lond) 2008;3: 703–17.10.2217/17435889.3.5.703Suche in Google Scholar PubMed PubMed Central
24. Choi HS, Liu W, Misra P, Tanaka E, Zimmer JP, Ipe BT, et al. Renal clearance of quantum dots. Nat Biotechnol 2007;25:1165–70.10.1038/nbt1340Suche in Google Scholar PubMed PubMed Central
25. Choi HS, Liu W, Liu F, Nasr K, Misra P, Bawendi MG, et al. Design considerations for tumour-targeted nanoparticles. Nat Nanotechnol 2010;5:42–7.10.1038/nnano.2009.314Suche in Google Scholar PubMed PubMed Central
26. Zamboni WC, Torchilin V, Patri AK, Hrkach J, Stern S, Lee R, et al. Best practices in cancer nanotechnology: perspective from NCI nanotechnology alliance. Clin Cancer Res 2012;18:3229–41.10.1158/1078-0432.CCR-11-2938Suche in Google Scholar PubMed PubMed Central
27. Gratton SE, Ropp PA, Pohlhaus PD, Luft JC, Madden VJ, Napier ME, et al. The effect of particle design on cellular internalization pathways. Proc Natl Acad Sci USA 2008;105:11613–8.10.1073/pnas.0801763105Suche in Google Scholar PubMed PubMed Central
28. Agarwal R, Roy K. Intracellular delivery of polymeric nanocarriers: a matter of size, shape, charge, elasticity and surface composition. Ther Deliv 2013;4:705–23.10.4155/tde.13.37Suche in Google Scholar PubMed
29. Wong C, Stylianopoulos T, Cui J, Martin J, Chauhan VP, Jiang W, et al. Multistage nanoparticle delivery system for deep penetration into tumor tissue. Proc Natl Acad Sci USA 2011;108:2426–31.10.1073/pnas.1018382108Suche in Google Scholar PubMed PubMed Central
30. Stylianopoulos T, Wong C, Bawendi MG, Jain RK, Fukumura D. Multistage nanoparticles for improved delivery into tumor tissue. Methods Enzymol 2012;508:109–30.10.1016/B978-0-12-391860-4.00006-9Suche in Google Scholar PubMed PubMed Central
31. Stylianopoulos T, Economides EA, Baish JW, Fukumura D, Jain RK. Towards optimal design of cancer nanomedicines: multi-stage nanoparticles for the treatment of solid tumors. Ann Biomed Eng 2015;43:2291–300.10.1007/s10439-015-1276-9Suche in Google Scholar PubMed PubMed Central
32. Murakami M, Ernsting MJ, Undzys E, Holwell N, Foltz WD, Li SD. Docetaxel conjugate nanoparticles that target alpha-smooth muscle actin-expressing stromal cells suppress breast cancer metastasis. Cancer Res 2013;73:4862–71.10.1158/0008-5472.CAN-13-0062Suche in Google Scholar PubMed
33. Zhu L, Kate P, Torchilin VP. Matrix metalloprotease 2-responsive multifunctional liposomal nanocarrier for enhanced tumor targeting. ACS Nano 2012;6:3491–8.10.1021/nn300524fSuche in Google Scholar PubMed PubMed Central
34. Hatakeyama H, Akita H, Ito E, Hayashi Y, Oishi M, Nagasaki Y, et al. Systemic delivery of siRNA to tumors using a lipid nanoparticle containing a tumor-specific cleavable PEG-lipid. Biomaterials 2011;32:4306–16.10.1016/j.biomaterials.2011.02.045Suche in Google Scholar PubMed
35. Helmlinger G, Yuan F, Dellian M, Jain RK. Interstitial pH and pO2 gradients in solid tumors in vivo: high-resolution measurements reveal a lack of correlation. Nat Med 1997;3:177–82.10.1038/nm0297-177Suche in Google Scholar PubMed
36. Zhu L, Torchilin VP. Stimulus-responsive nanopreparations for tumor targeting. Integr Biol (Camb) 2013;5:96–107.10.1039/c2ib20135fSuche in Google Scholar PubMed PubMed Central
37. Kim IY, Kang YS, Lee DS, Park HJ, Choi EK, Oh YK, et al. Antitumor activity of EGFR targeted pH-sensitive immunoliposomes encapsulating gemcitabine in A549 xenograft nude mice. J Control Release 2009;140:55–60.10.1016/j.jconrel.2009.07.005Suche in Google Scholar PubMed
38. Han S, Liu Y, Nie X, Xu Q, Jiao F, Li W, et al. Efficient delivery of antitumor drug to the nuclei of tumor cells by amphiphilic biodegradable poly(L-aspartic acid-co-lactic acid)/DPPE co-polymer nanoparticles. Small 2012;8:1596–606.10.1002/smll.201102280Suche in Google Scholar PubMed
39. Mura S, Nicolas J, Couvreur P. Stimuli-responsive nanocarriers for drug delivery. Nat Mater 2013;12:991–1003.10.1038/nmat3776Suche in Google Scholar PubMed
40. Blum AP, Kammeyer JK, Rush AM, Callmann CE, Hahn ME, Gianneschi NC. Stimuli-responsive nanomaterials for biomedical applications. J Am Chem Soc 2015;137:2140–54.10.1021/ja510147nSuche in Google Scholar PubMed PubMed Central
41. von Maltzahn G, Park JH, Agrawal A, Bandaru NK, Das SK, Sailor MJ, et al. Computationally guided photothermal tumor therapy using long-circulating gold nanorod antennas. Cancer Res 2009;69:3892–900.10.1158/0008-5472.CAN-08-4242Suche in Google Scholar PubMed PubMed Central
42. Fomina N, Sankaranarayanan J, Almutairi A. Photochemical mechanisms of light-triggered release from nanocarriers. Adv Drug Deliv Rev 2012;64:1005–20.10.1016/j.addr.2012.02.006Suche in Google Scholar PubMed PubMed Central
43. Emblem KE, Mouridsen K, Bjornerud A, Farrar CT, Jennings D, Borra RJ, et al. Vascular architecture imaging identifies patient responders to anti-angiogenic therapy. Nat Med 2013;19:1178–83.10.1038/nm.3289Suche in Google Scholar PubMed PubMed Central
©2016 by De Gruyter
Artikel in diesem Heft
- Frontmatter
- In this issue
- Guest Editorial
- Nanotheranostics: is integrating therapeutics with diagnostics enough?
- What’s Up?
- What’s up in nanomedicine?
- Special section Nanotheranostics
- Review
- Intelligent drug delivery systems for the treatment of solid tumors
- Original Articles
- Ultrasound-induced doxorubicin release from folate-targeted and non-targeted P105 micelles: a modeling study
- Effect of pH, ultrasound frequency and power density on the release of calcein from stealth liposomes
- Meeting Report
- Nanotheranostics: realizing the great promise?
- Regular contributions
- Original Article
- Delivery and cytotoxicity of doxorubicin and temozolomide to primary glioblastoma cells using gold nanospheres and gold nanorods
- Opinion Paper
- How organizers of scientific meetings and journal editors could facilitate transfer of nanomedicine into the clinic
Artikel in diesem Heft
- Frontmatter
- In this issue
- Guest Editorial
- Nanotheranostics: is integrating therapeutics with diagnostics enough?
- What’s Up?
- What’s up in nanomedicine?
- Special section Nanotheranostics
- Review
- Intelligent drug delivery systems for the treatment of solid tumors
- Original Articles
- Ultrasound-induced doxorubicin release from folate-targeted and non-targeted P105 micelles: a modeling study
- Effect of pH, ultrasound frequency and power density on the release of calcein from stealth liposomes
- Meeting Report
- Nanotheranostics: realizing the great promise?
- Regular contributions
- Original Article
- Delivery and cytotoxicity of doxorubicin and temozolomide to primary glioblastoma cells using gold nanospheres and gold nanorods
- Opinion Paper
- How organizers of scientific meetings and journal editors could facilitate transfer of nanomedicine into the clinic