Developing a European longitudinal and interprofessional curriculum for clinical reasoning
-
Inga Hege
 ,
Martin Adler
,
Martin Adler

Abstract
Clinical reasoning is a complex and crucial ability health professions students need to acquire during their education. Despite its importance, explicit clinical reasoning teaching is not yet implemented in most health professions educational programs. Therefore, we carried out an international and interprofessional project to plan and develop a clinical reasoning curriculum with a train-the-trainer course to support educators in teaching this curriculum to students. We developed a framework and curricular blueprint. Then we created 25 student and 7 train-the-trainer learning units and we piloted 11 of these learning units at our institutions. Learners and faculty reported high satisfaction and they also provided helpful suggestions for improvements. One of the main challenges we faced was the heterogeneous understanding of clinical reasoning within and across professions. However, we learned from each other while discussing these different views and perspectives on clinical reasoning and were able to come to a shared understanding as the basis for developing the curriculum. Our curriculum fills an important gap in the availability of explicit clinical reasoning educational materials both for students and faculty and is unique with having specialists from different countries, schools, and professions. Faculty time and time for teaching clinical reasoning in existing curricula remain important barriers for implementation of clinical reasoning teaching.
Background
Clinical reasoning (CR) is both a complex and core ability that health professions students are expected to learn. Despite the importance of CR, recent studies found that it is not explicitly or longitudinally taught in health professions curricula [1, 2]. However, CR teaching is crucial to improve diagnostic and therapeutic reasoning and reduce errors in patient care [3]. A recent survey among a broad range of international educators (n=313) showed a need for such a longitudinal CR curriculum including a train-the-trainer (TTT) course for educators on how to teach CR. In this investigation, only 28% of participants reported the existence of a longitudinal CR curriculum while 85% expressed the need for such a longitudinal CR curriculum. Participants reported a lack of awareness of the importance of CR teaching, lack of guidelines on how to teach CR, and lack of qualified educators to teach CR as the three most important barriers for implementing explicit CR curricula [2].
To address this shortcoming, we implemented the EU-funded project “Developing, implementing, and disseminating an adaptive clinical reasoning curriculum for healthcare students and educators” (DID-ACT) [4]. In this project we aimed to conceptualize and implement a curriculum on clinical reasoning that is (1) suitable for interprofessional teaching, (2) international, (3) adaptable to different types of instruction and curricula, and (4) supports educators to teach the curriculum through train-the-trainer courses. Our project consortium includes 46 partners from six European countries (Germany, Malta, Poland, Slovenia, Sweden, Switzerland) and the USA, representing 12 healthcare education institutions and three healthcare professions: medicine, nursing, and physiotherapy, as well as healthcare educators and researchers.
Curriculum development
We based our curriculum development process on the six steps of the Kern cycle [5]. This cycle describes the necessary steps from needs assessment to evaluation. The evaluation results obtained in the last step can serve as a starting point for a repeated needs assessment and another cycle. We will describe each step in the following sections and Figure 1 provides an overview about the steps and our implementation.

Overview of the curriculum development process with the six steps of the Kern cycle.
Problem identification and specific needs assessment
Based on the results from the pre-project needs analysis [2], we implemented an in-depth evaluation based on 29 semi-structured interviews to identify potential topics and barriers for implementing such a longitudinal CR curriculum and TTT course. These interviews revealed a variety of barriers, which we grouped into the following categories: Time, Culture, Motivation, Clinical Reasoning as a Concept, Teaching, Assessment, and Infrastructure [6]. We discussed these barriers and developed and prioritized measures to address and overcome them in an (virtual) ideation workshop. For example, the heterogeneous definitions and understanding of clinical reasoning led us to define CR for this project as the following: “Clinical Reasoning encompasses health professionals thinking and acting in assessment, diagnostic, and management processes in clinical situations taking into account the patient‘s specific circumstances and preferences.”
While addressing all these barriers we identified is beyond the scope of our project, we focused on addressing barriers in the Teaching, Assessment, and Concept categories, which include aspects such as a disbelief in explicit CR teaching, lack of awareness of teaching and assessing CR, lack of guidance, and lack of qualified educators. Table 1 provides an overview of the barriers and how we addressed them in our curriculum development process.
Overview of identified barriers and how we addressed them in our curriculum development process.
| Category | Barrier | Addressed |
|---|---|---|
| Teaching | Disbelief in explicit CR teaching | TTT learning units highlighting the importance of explicit CR teaching & assessment |
| Lack of awareness of methods | TTT learning units on CR teaching & assessment; teaching and assessment methods, resources, and references provided for all learning units | |
| Lack of competency frameworks | Publication of curricular blueprint including themes and overarching learning outcomes and competency levels | |
| No specific guidance | TTT and student learning units with freely available resources, providing an integration guideline | |
| Lack of qualified educators | TTT learning units to qualify educators and facilitate networking | |
| Assessment | Unawareness and implementation issues | TTT learning units on importance of explicit CR teaching & assessment |
| Motivation | Lack of incentives | Provision of a participant certificate for the TTT and student courses |
| Concept | Awareness of importance | TTT learning units on importance of explicit CR teaching & assessment |
| Time | Lack of time in the curriculum | Provision of an integration guideline |
Goals and objectives
As a next step, we constructed overarching learning objectives for the curriculum and the train-the-trainer course and categorized these objectives into themes. We identified these CR-related themes and learning objectives from eight national learning objective catalogs of health professions education from our partner countries (Germany, Poland, Sweden, Switzerland, USA) and a European catalog. In addition, we performed a scoping literature review on CR teaching frameworks [7, 8]. We extracted the relevant learning objectives, translated them into English, and implemented a group consensus process to develop a comprehensive list of learning objectives grouped in themes. We described the details of this process in a previous article [9].
Overall, we defined 35 overarching learning objectives and grouped them into the following 11 themes: (1) Theories of clinical reasoning, (2) Gathering, interpreting, and synthesizing information, (3) Generating differential diagnoses, (4) Developing a treatment/management plan, (5) Patient perspective, (6) (Interprofessional) collaboration (7) Ethical aspects, (8) Self-Reflection & Attitudes, (9) Errors and Biases (10) Teaching clinical reasoning, and (11) Decision making.
Educational strategies
Once we had agreed on the themes and overarching learning objectives, we defined the structure of the DID-ACT curriculum and learning units based on these learning objectives. The DID-ACT curriculum was designed as a series of learning units based on our defined themes that can be implemented longitudinally (i.e. over several years) in undergraduate education. The applied teaching strategies in the learning units include (spaced) repetition, progression of depth and complexity, and opportunities for deliberate practice. Also, the learning units are adaptable to different settings, health profession curricula, and resources available at the schools [10].
Next, we decided on three basic pedagogical principles for the curriculum: learner-centeredness, blended-learning, and case-based learning. (1) A learner-centered approach emphasizes learning as the result of a learner’s active engagement and responsibility in learning activities. It places the learner’s experiences and development of knowledge and meaning in the center of the learning process. The teacher’s role is to support and facilitate the learning process and provide feedback [11]. (2) Blended learning is a meaningful combination of asynchronous/online and synchronous/face-to-face learning activities [12]. This allows teachers and learners to use the synchronous sessions for discussions or knowledge application instead of instructor-led teaching of knowledge. Considering the current COVID-19 pandemic we also include recommendations on how these synchronous sessions can be conducted in a virtual environment. (3) Research has shown that students enjoy case-based learning [13] and virtual patient cases can improve clinical reasoning skills [14]. Therefore, cases and virtual patients are core components especially of the student curriculum and most of the learning and assessment activities are based on them.
Implementation
Based on the 11 themes and learning objectives we planned 25 learning units for undergraduate students (on a novice, intermediate, and advanced levels) and seven TTT units. Figure 2 shows a general overview, and an interactive version is available on our website [4].

Curricular blueprint with the learning units in the four competency levels (columns) and themes (colored circles).
In small interprofessional teams we described the structure and content for each learning unit in a template [4]. This template includes general learning unit aspects such as title, prerequisites, specific (measurable) learning objectives, level of competence (novice, intermediate, and advanced), required time, group size, and description. Depending on the learning objectives each learning unit is then divided into several synchronous and asynchronous sessions and described in detail with instructional methods, required time, and alternative approaches.
After project members completed the review of a learning unit outline, we implemented it in our learning management system Moodle [15]. This step included providing, and if needed, developing videos, designing activities such as quizzes or assignments with immediate feedback, and developing and/or adapting cases. For the facilitators of the learning unit, we uploaded all required resources, the detailed description of the course outline, and if applicable also sample answers for the assignments and group tasks. With these resources facilitators can prepare their teaching and if needed adapt the course outline.
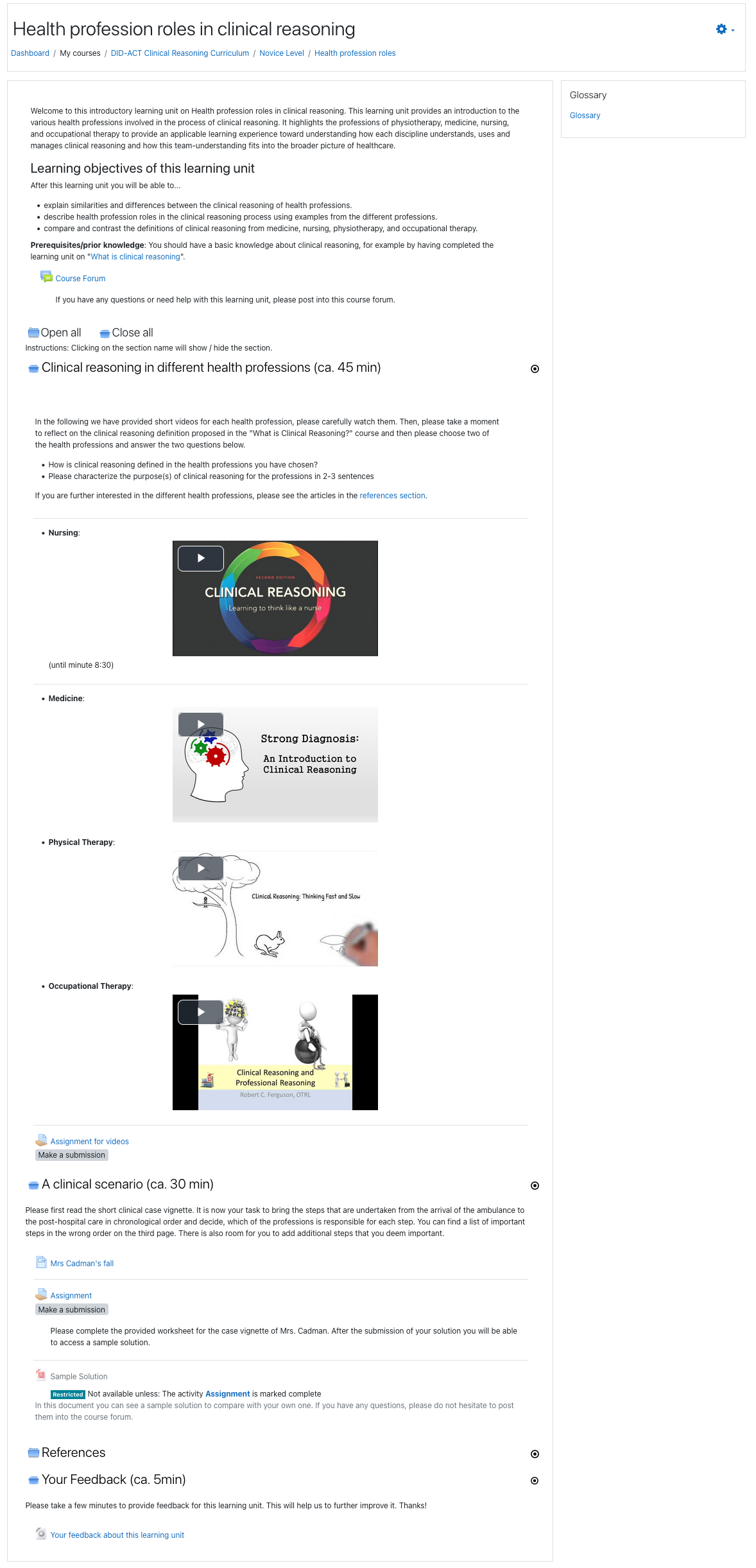
All material is available under a Creative Commons (CC) license, and we used open educational resources (OERs). Access to Moodle is free, but logging in is required using either institutional credentials or self-registration. We have included an example outline of the learning unit for novice students on the health profession roles in CR, which serves as a guide for teachers (see Supplementary File 1). Additionally, this learning unit (as implemented in Moodle), is shown in Supplementary File 2.
Evaluation and feedback
We implemented and evaluated nine train-the-trainer and eight novice and intermediate piloted learning units from October 2021 until January 2022 with a total of 198 participating students and 98 educators. The piloted learning units covered five different topics from the student curriculum and five topics from the TTT courses (Table 2). We selected these learning units through a group consensus process during a team meeting where we focused on the following three aspects: (1) local needs assessment (e.g., preference of basic over advanced TTT courses), (2) opportunities for integration of the learning units in local curricula and (3) comparing evaluation outcomes of the same learning units at different institutions.
Overview of pilots.
| Type | Learning unit | Institutions | Profession | n | Comments on implementation |
|---|---|---|---|---|---|
| STU | What is clinical reasoning - an introduction | UAU, UBERN, MFUM | M | 34 | Extracurricular blended-learning for 1st & 2nd year students of medicine with additional participants from Karolinska Institutet, university of porto, university of Zurich. |
| STU | Person-centered approach and the role of the patient | EDU, JU | M | 59 | EDU: 2nd year medical students (“module 6”); JU: 3rd year medical students as part of the “clinical laboratory training of clinical skills 2/4” course. |
| STU | Health professionals roles in clinical reasoning (novice) | UAU, UBERN, MFUM | M | 34 | Extracurricular blended-learning for 1st & 2nd year students of medicine with additional participants from Karolinska Institutet, university of porto, university of Zurich. |
| STU | Generating differential diagnoses and deciding about final diagnoses | UBERN, JU, MFUM | M | 51 | MFUM: Extracurricular pilot for 3rd–5th year students of medicine; UBERN: Pediatric clerkship students in their 4th–5th year; JU: 2nd year medical students as part of the “introduction to clinical sciences” course. |
| STU | Health professionals roles in clinical reasoning (intermediate) | ORU, JU | M, N | 20 | Extracurricular synchronous online event; ORU: 2nd and 3rd year students of nursing. JU: 3rd year nursing and 5th year medicine. Additional participation of 3rd year nursing students from berner bildungszentrum pflege (Switzerland). |
| TTT | What is clinical reasoning & how to put theories into practice | JU, UBERN | M, N, Pa | 32 | JU: Blended learning faculty development at the DPM; UBERN: online course for participants of the MME program. |
| TTT | Information gathering, generating differential diagnoses, decision making, and treatment planning | JU, UBERN, MFUM | M, N | 19 | JU: online faculty development at the DPM; UBERN: Hybrid course for consultants in pediatric emergency medicine; MFUM: online faculty development event. |
| TTT | Person-centered approach and the role of the patient | EDU | M | 7 | Blended learning faculty development event. |
| TTT | Health professionals’ roles in clinical reasoning | UAU, ORU | B, M, N, ph | 18 | UAU: Regular workshop within the faculty development program with; ORU: Synchronous online faculty development event meeting with additional participation of teachers from Karolinska Institutet, mälardalen and sophiahemmet universities in Sweden. |
| TTT | Application of clinical reasoning teaching and assessment methods | UBERN | M | 22 | Online course for participants of the MME program. |
-
Type: STU, student curriculum; TTT, train-the-trainer course; (Partner) Institution: EDU, Malta; MFUM, University of Maribor; JU, Jagiellonian University; ORU, Orebro University; UAU, University of Augsburg; UBERN, University of Bern; Prof, Profession: B, biomedical sciences/analyst; M, medicine, N, nursing; Pa, paramedics; Ph, physical therapy; Implementation: DME, department of medical education; MME, master of medical education.
To evaluate selected pilot learning units, we developed two questionnaires to capture student and facilitator experience and satisfaction with a learning unit. The questionnaires are based on the “Evaluation of Technology-Enhanced Learning Materials” (ETELM) tool [16] and are available on the DID-ACT website.
Overall, we received 199 completed questionnaires from students and facilitators. Table 3 shows a summary of the most relevant results.
Summary of mean (standard deviation) values of selected responses from participants and facilitators of the student and educator learning units (7-item Likert scale, 1=strongly disagree, 7=strongly agree).
| Student course | Train-the-trainer course | |||
|---|---|---|---|---|
| Participants | Facilitators | Participants | Facilitators | |
| Responses (response rate). | 125 (63%) | 6 (33%) | 56 (57%) | 12 (86%) |
| This learning unit will improve my clinical reasoning (teaching) skills. | 5.8 (1.5) | – | 5.9 (1.5) | – |
| The educational activities encouraged engagement with learning unit materials/content. | 5.8 (1.2) | 6.0 (1.3) | 6.0 (1.2) | 5.5 (1.2) |
| The learning unit effectively blended online and face-to-face elements. | 5.8 (1.4) | 5.3 (1.5) | 5.9 (1.4) | 6.0 (0.6) |
| The learning unit technologies and media supported the learning objectives. | 5.9 (1.1) | 4.8 (1.6) | 5.6 (1.3) | 5.6 (1.2) |
| The overall quality of this learning unit was excellent. | 5.5 (1.4) | 5.0 (1.3) | 5.5 (1.5) | 5.6 (0.9) |
In open-ended questions students endorsed the virtual patients, cases, the engagement of the facilitators, and the small-group group discussions (often conducted in multinational and interprofessional teams) which broadened their views on clinical reasoning. Students also identified challenges (both technical and navigation issues) with the learning management system Moodle. Additionally, some participants suggested modifications of the content for a better representativeness of the diverse array of health professions. Facilitators commented that the TTT pilots sometimes required a high workload which resulted in challenges with their limited time for faculty development.
Based on the evaluation results, we identified, discussed, and implemented several areas for technical and content improvements. These improvements included more technical guidance on how to navigate on the learning platform Moodle, more detailed instructions and examples for facilitators, and more elaborate feedback for users with the asynchronous learning activities. Moreover, we developed and published an integration guideline on our website, describing how the learning units can be integrated into existing health profession curricula and faculty development programs.
The evaluation was exempted from a detailed ethical review by the Institutional Review Board of the University of Bern, Switzerland (decision Req-2020-00074).
Challenges
One of our initial challenges was the heterogeneous terminology within and across professions [17]. Therefore, we dedicated several meetings to discussing our perspectives and developing our CR definition as a foundation for the DID-ACT curriculum. Our definition resonated with professions present on our team and in the needs analysis as well as contemporary CR literature including diagnostic, management, caring and rehabilitation perspectives [18, 19].
Another initial challenge was an emphasis on physician perspectives in our curriculum development process. Despite being a multiprofessional project team, including physicians, nurses, and physiotherapists, the number of physicians was higher, resulting in some of the small group curriculum development teams being unequally staffed. In such groups, we may have missed opportunities for more in-depth interprofessionality, although all partners were open-minded and deeply interested in interprofessional clinical reasoning.
Lastly, integrating the new themes into existing curricula is a long-term process that requires several years for completion. Our developed learning units are available for immediate use, however, considering already overloaded healthcare curricula we anticipate gradual replacement of old content with new content over time will likely occur. Another important and sometimes overlooked need is aligning curricular assessment with newly integrated content to facilitate the evaluation of learning outcomes beyond the level of satisfaction and self-efficacy.
As part of the project, we also developed plans for sustainability. However, the realization of those plans will be an ongoing mission for the upcoming years. We believe that the need for explicit and longitudinal clinical reasoning curricula to include a TTT course will facilitate a sustained integration and further dissemination of the DID-ACT curriculum.
Conclusions
Our curriculum development process followed a similar approach described by Singh et al. in which they embedded CR into a medical curriculum in the UK as a monoprofessional longitudinal theme including TTT learning units [20]. In both approaches, the strongest enabler of implementing a CR curriculum is the investment in faculty development to train educators motivated to implement explicit CR teaching techniques. However, one of the main identified barriers in implementing CR teaching [6] and noticed also in the feedback we received during our piloting of learning units was the limited time and availability of educators. Overcoming this requires institutional changes, such as protected time for educators and incentives to facilitate and prioritize their participation in faculty development courses. For example, creating recognizable certificates for professional development in this area and/or participation in the training as part of one’s regular hours could mitigate this barrier.
A strength of the DID-ACT curriculum in comparison to other longitudinal CR curricula [20], [21], [22] is the international and interprofessional approach and the pilot implementation of the curriculum at several universities across five European countries. The emphasis on interprofessional collaboration and the recognition of patient participation in clinical reasoning of all health professions enabled us to have a broad perspective on clinical reasoning [7].
The challenges we encountered during our curriculum development process led to many fruitful and inspiring discussions which enabled us to learn from each other and develop a joint understanding of CR and the different goals of involved health professionals. Therefore, we recommend establishing a multiprofessional team and dedicating as much time as possible for sharing and discussing the different perspectives if one is planning to implement interprofessional (CR) teaching. This requires an open and respectful atmosphere that promotes equal contribution of knowledge and experience by all professionals to the discussion, and a sustainable curriculum implementation plan.
Funding source: Erasmus+Knowledge Alliance
Award Identifier / Grant number: 612454-EPP-1-2019-1-DE-EPPKA2-KA
Acknowledgments
We would like to thank all our colleagues who are part of the project and contributed significantly to the project’s success. Also, we want to thank all students, educators, and healthcare professionals for their valuable and meaningful feedback on our work.
-
Research funding: This work is part of the Erasmus + Knowledge Alliance DID-ACT (612454-EPP-1-2019-1-DE-EPPKA2-KA).
-
Author contributions: All authors have accepted responsibility for the entire content of this manuscript and approved its submission.
-
Competing interests: Authors state no conflict of interest.
-
Informed consent: Informed consent was obtained from all individuals included in this study.
-
Ethical approval: The evaluation was exempted from a detailed ethical review by the Institutional Review Board of the University of Bern, Switzerland (decision Req-2020-00074).
References
1. Rencic, J, Trowbridge, RLJr, Fagan, M, Szauter, K, Durning, S. Clinical reasoning education at US medical schools: results from a national survey of internal medicine clerkship directors. J Gen Intern Med 2017;32:1242–6. https://doi.org/10.1007/s11606-017-4159-y.Search in Google Scholar PubMed PubMed Central
2. Kononowicz, AA, Hege, I, Edelbring, S, Sobocan, M, Huwendiek, S, Durning, SJ. The need for longitudinal clinical reasoning teaching and assessment: results of an international survey. Med Teach 2020;42:457–62. https://doi.org/10.1080/0142159x.2019.1708293.Search in Google Scholar PubMed
3. World Health Organization (WHO). Diagnostic errors – technical series on safer primary care; 2016. Available from: https://apps.who.int/iris/bitstream/handle/10665/252410/9789241511636-eng.pdf [Accessed 2 Dec 2022].Search in Google Scholar
4. DID-ACT. Project website [Online]. Available from: http://www.did-act.eu [Accessed 2 Dec 2022].Search in Google Scholar
5. Thomas, PA, Kern, DE, Hughes, MT, Chen, BY, editors. Curriculum development for medical education: a six-step approach, 3rd ed. Baltimore. MD: Johns Hopkins University Press; 2016.Search in Google Scholar
6. Sudacka, M, Adler, M, Durning, SJ, Edelbring, S, Frankowska, A, Hartmann, D, et al.. Why is it so difficult to implement a longitudinal clinical reasoning curriculum? A multicenter interview study on the barriers perceived by European health professions educators. BMC Med Educ 2021;21:575. https://doi.org/10.1186/s12909-021-02960-w.Search in Google Scholar PubMed PubMed Central
7. Elvén, M, Welin, E, Wiegleb Edström, D, Petreski, T, Szopa, M, Durning, SJ, et al.. Clinical reasoning curricula in health professions education: a scoping review. J Med Educ Curric Dev [Manuscript submitted for publication].Search in Google Scholar
8. Elvén, M, Welin, E, Edström, DW, Petreski, T, Szopa, M, Durning, SJ, et al.. How can clinical reasoning teaching change from a ‘black-box phenomenon’ to a structured clinical reasoning curriculum? Insights from a scoping review. In: 5th montreal international conference on clinical reasoning. Montreal: Canada; 2022.Search in Google Scholar
9. Parodis, I, Andersson, L, Durning, SJ, Hege, I, Knez, J, Kononowicz, AA, et al.. Clinical reasoning needs to be explicitly addressed in health professions curricula: recommendations from a European consortium. Int J Environ Res Publ Health 2021;18:11202. https://doi.org/10.3390/ijerph182111202.Search in Google Scholar PubMed PubMed Central
10. Quirk, M, Chumley, H. The adaptive medical curriculum: a model for continuous improvement. Med Teach 2018;40:786–90. https://doi.org/10.1080/0142159x.2018.1484896.Search in Google Scholar
11. Wright, GB. Student-centered learning in higher education. Int J Learn High Educ 2011;23:92–7.Search in Google Scholar
12. Rowe, M, Frantz, J, Bozalek, V. The role of blended learning in the clinical education of healthcare students: a systematic review. Med Teach 2012;34:e216–21. https://doi.org/10.3109/0142159x.2012.642831.Search in Google Scholar
13. Thistlethwaite, JE, Davies, D, Ekeocha, S, Kidd, JM, MacDougall, C, Matthews, P, et al.. The effectiveness of case-based learning in health professional education. A BEME systematic review: BEME guide no. 23. Med Teach 2012;34:e421–44. https://doi.org/10.3109/0142159x.2012.680939.Search in Google Scholar PubMed
14. Kononowicz, AA, Woodham, LA, Edelbring, S, Stathakarou, N, Davies, D, Saxena, N, et al.. Virtual patient simulations in health professions education: systematic review and meta-analysis by the digital health education collaboration. J Med Internet Res 2019;21:e14676. https://doi.org/10.2196/14676.Search in Google Scholar PubMed PubMed Central
15. DID-ACT project consortium. DID-ACT learning management system moodle [Online]. Available from: https://did-act.instruct.eu [Accessed 2 Dec 2022].Search in Google Scholar
16. Cook, DA, Ellaway, RH. Evaluating technology-enhanced learning: a comprehensive framework. Med Teach 2015;37:961–70. https://doi.org/10.3109/0142159x.2015.1009024.Search in Google Scholar
17. Young, M, Thomas, A, Gordon, D, Gruppen, L, Lubarsky, S, Rencic, J, et al.. The terminology of clinical reasoning in health professions education: implications and considerations. Med Teach 2019;41:1277–84. https://doi.org/10.1080/0142159x.2019.1635686.Search in Google Scholar PubMed
18. Higgs, J, Jensen, GM, Loftus, S, Christensen, N. Clinical reasoning in the health professions, 4th ed. Edinburgh, UK: Elsevier; 2019.Search in Google Scholar
19. Cook, DA, Sherbino, J, Durning, SJ. Management reasoning: beyond the diagnosis. JAMA 2018;319:2267–8. https://doi.org/10.1001/jama.2018.4385.Search in Google Scholar PubMed
20. Singh, M, Collins, L, Farrington, R, Jones, M, Thampy, H, Watson, P, et al.. From principles to practice: embedding clinical reasoning as a longitudinal curriculum theme in a medical school programme. Diagnosis 2021;92:184–94. https://doi.org/10.1515/dx-2021-0031.Search in Google Scholar PubMed
21. Connor, DM, Narayana, S, Dhaliwal, G. A clinical reasoning curriculum for medical students: an interim analysis. Diagnosis 2021;9:265–73. https://doi.org/10.1515/dx-2021-0112.Search in Google Scholar PubMed
22. Rowat, J, Suneja, M. Longitudinal clinical reasoning theme embedded across four years of a medical school curriculum. Diagnosis 2022;9:468–75. https://doi.org/10.1515/dx-2022-0046.Search in Google Scholar PubMed
Supplementary Material
This article contains supplementary material (https://doi.org/10.1515/dx-2022-0103).
© 2023 the author(s), published by De Gruyter, Berlin/Boston
This work is licensed under the Creative Commons Attribution 4.0 International License.
{kind=link}
Articles in the same Issue
- Frontmatter
- Review
- Cognitive biases in internal medicine: a scoping review
- Opinion Papers
- “Pivot and Cluster Strategy” in the light of Kahneman’s “Decision Hygiene” template
- Developing a European longitudinal and interprofessional curriculum for clinical reasoning
- Optimizing measurement of misdiagnosis-related harms using symptom-disease pair analysis of diagnostic error (SPADE): comparison groups to maximize SPADE validity
- Reframing context specificity in team diagnosis using the theory of distributed cognition
- Original Articles
- Promoting clinical reasoning with meta-memory techniques to teach broad differential diagnosis generation in a pediatric core clerkship
- Semantic competence and prototypical verbalizations are associated with higher OSCE and global medical degree scores: a multi-theory pilot study on year 6 medical student verbalizations
- Influence of comorbid depression and diagnostic workup on diagnosis of physical illness: a randomized experiment
- Recognition, diagnostic practices, and cancer outcomes among patients with unintentional weight loss (UWL) in primary care
- Quantitation of neurofilament light chain protein in serum and cerebrospinal fluid from patients with multiple sclerosis using the MSD R-PLEX NfL assay
- Analysis of common biomarkers in capillary blood in routine clinical laboratory. Preanalytical and analytical comparison with venous blood
- Comparison between cerebrospinal fluid biomarkers for differential diagnosis of acute meningitis
- Short Communications
- Exploring relationships between physician stress, burnout, and diagnostic elements in clinician notes
- Development of a student-created internal medicine frameworks website for healthcare trainees
- Case Report - Lessons in Clinical Reasoning
- Lessons in clinical reasoning – pitfalls, myths, and pearls: a case of crushing, substernal chest pain
- Letters to the Editor
- Ample room for cognitive bias in diagnosing accidental hypothermia
- Auscultation order of lung and heart sounds and autonomous noise cancellation
- Reliability of a single-nostril nasopharyngeal swab for diagnosing SARS-CoV-2 infection
Articles in the same Issue
- Frontmatter
- Review
- Cognitive biases in internal medicine: a scoping review
- Opinion Papers
- “Pivot and Cluster Strategy” in the light of Kahneman’s “Decision Hygiene” template
- Developing a European longitudinal and interprofessional curriculum for clinical reasoning
- Optimizing measurement of misdiagnosis-related harms using symptom-disease pair analysis of diagnostic error (SPADE): comparison groups to maximize SPADE validity
- Reframing context specificity in team diagnosis using the theory of distributed cognition
- Original Articles
- Promoting clinical reasoning with meta-memory techniques to teach broad differential diagnosis generation in a pediatric core clerkship
- Semantic competence and prototypical verbalizations are associated with higher OSCE and global medical degree scores: a multi-theory pilot study on year 6 medical student verbalizations
- Influence of comorbid depression and diagnostic workup on diagnosis of physical illness: a randomized experiment
- Recognition, diagnostic practices, and cancer outcomes among patients with unintentional weight loss (UWL) in primary care
- Quantitation of neurofilament light chain protein in serum and cerebrospinal fluid from patients with multiple sclerosis using the MSD R-PLEX NfL assay
- Analysis of common biomarkers in capillary blood in routine clinical laboratory. Preanalytical and analytical comparison with venous blood
- Comparison between cerebrospinal fluid biomarkers for differential diagnosis of acute meningitis
- Short Communications
- Exploring relationships between physician stress, burnout, and diagnostic elements in clinician notes
- Development of a student-created internal medicine frameworks website for healthcare trainees
- Case Report - Lessons in Clinical Reasoning
- Lessons in clinical reasoning – pitfalls, myths, and pearls: a case of crushing, substernal chest pain
- Letters to the Editor
- Ample room for cognitive bias in diagnosing accidental hypothermia
- Auscultation order of lung and heart sounds and autonomous noise cancellation
- Reliability of a single-nostril nasopharyngeal swab for diagnosing SARS-CoV-2 infection