Piriformis muscle injection guided by sciatic nerve stimulation: Quick, simple, and safe technique
-
M. Mayo-Moldes
 ,
A. Carregal
,
A. Carregal

To the Editor,
The Piriformis syndrome (PS) is thought to involve the piriformis muscle because of its proximity to the sciatic nerve. This muscle follows a linear path coinciding with the sciatic nerve which lies beneath the muscle in the parasacral region [1].
PS is associated with buttock, hip and lower limb pain. Medical treatment that has been applied includes therapeutic stretching, ultrasound, massage, oral analgesics and intramuscular local anesthetic with or without steroid injections [2].
There is not a universally accepted technique for injection of the piriformis muscle. Several authors have reported imaging-guided injection techniques with fluoroscopy or CT that may not be available in most pain management centers [3,4]. Nowadays, ultrasound has shown promise for pain. However, the technique requires some experience before it can be performed by one operator also handling the needle [5,6].
We investigated whether local anesthetic nerve-stimulator guided injections are effective in achieving long-lasting pain relief in (PS) because the nerve stimulation is widely available, radiation free and easy to use.
Weprospectively enrolled 100 patients diagnosed of PS. All subjects complained of buttock, hip and lower limb pain for 3 months duration before admission to the study and all of them were refractory to conservative management measures. Pain was aggravated by sitting, stair climbing, and leg crossing. Subjects were excluded if imaging studies demonstrated evidence of a herniated lumbar disk or nerve root impingement, or electromyography examination demonstrated pathology proximal to the sciatic.
We use standard surface landmarks for the posterior approach to sciatic blockade. (After a skin wheal of local anesthetic), a 21G × 100 mm Stimuplex needle (Pajunk) was inserted perpendicular to the skin and advanced with an initial setting of 1.5 mA, 2 Hz. The sciatic nerve is identified by a reduction of frank gluteal contraction and plantar flexion/dorsiflexion response at a current of 1mA. We then retract the needle till extinction of the response.
Two patients did not meet our study criteria, and four patients refused to participate. Thus, 94 patients (70 females and 24 males) were enrolled in the study after applying exclusion criteria. The average age of the patients was 50 years. A perisciatic injection of local anesthetic using a nerve stimulator to locate and inject near the sciatic nerve and into the piriformis muscle was performed. All patients received 10 ml bupivacaine 0.125% without addition of steroids and were clinically evaluated at 1 and 4 weeks after the procedure. The visual analogue scale (VAS) was used to evaluate treatment response (VAS: 0 = no pain; 100 = worst possible pain). Prior to data analysis, improvement greater than 25mmon the VAS score was selected as clinically significant.
Data are shown as the mean ± standard deviations. Data were evaluated using paired t test. P < 0.05 was required for significance. We used SPSS 11 (SPSS Inc., Chicago, IL) for data analysis.
There was a statistically significant reduction in mean VAS scoring for buttock and hip pain at week 1 (84%) and week 4 (70%) (Fig. 1) and the pain was improved from 66.5±16.1mmto 32.8±27.3mm at the 4-week follow-up visit. 70% of patients experienced full recovery and were discharged from the Pain clinic, after 3 months, when pain was mild (VAS <30 mm).
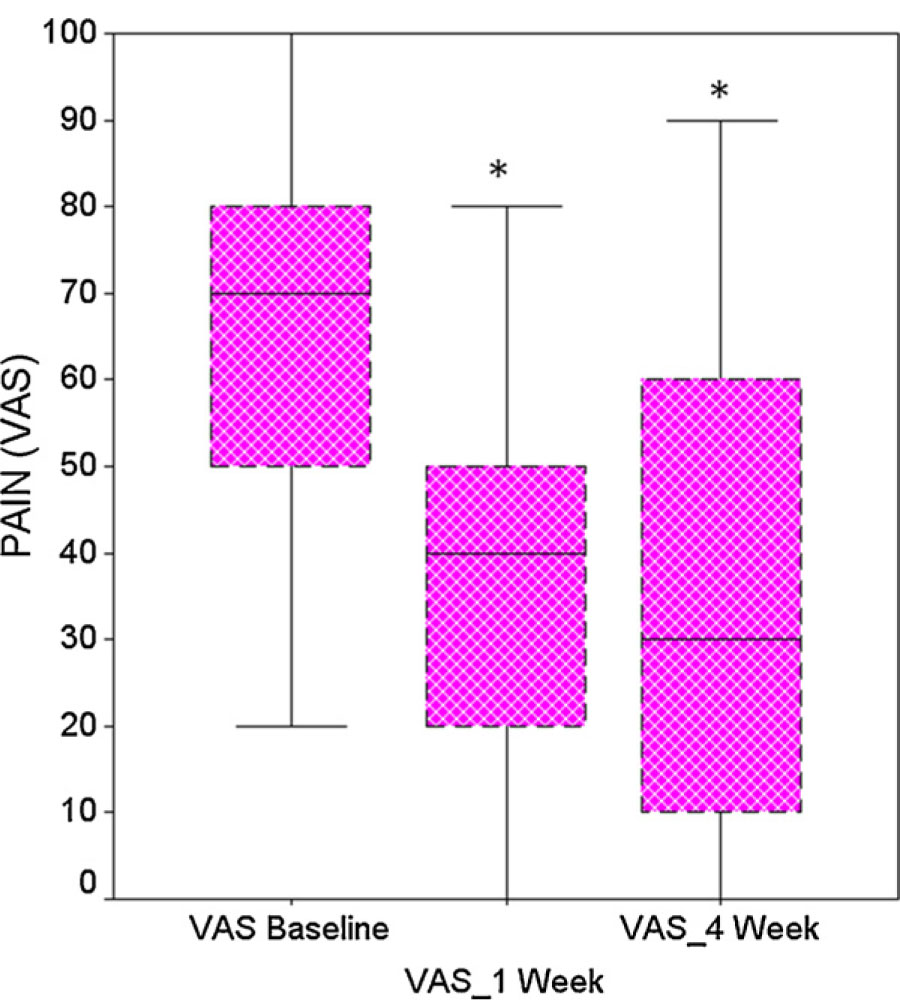
Pain, documented by the visual analogue scale (VAS). Data are presented as median, interquartile range; *P < 0.05, significant difference compared with baseline.
Piriformis muscle depth measured with the needle was a mean of 6.7 ± 1.3 cm.
Our study shows that a perisciatic injection using simple landmarks and utilizing a nerve stimulator to locate and inject near the sciatic nerve and into the piriformis muscle is a quick, simple, economical and effective technique and can be considered an alternative to infiltration guided by fluoroscopy or CT.
DOI of refers to article: http://dx.doi.org/10.1016/j.sjpain.2012.05.072.
-
Conflicts of interest: None of the authors have conflicts of interest to declare.
References
[1] Benzon HT, Katz JA, Benzon HA, Iqbal MS. Piriformis syndrome: anatomic considerations, a new injection technique, and a review of the literature. Anesthesiology 2003;98:1442–8.Search in Google Scholar
[2] Fishman LM, Anderson C, Rosner B. Botox and physical therapy in the treatment of piriformis syndrome. Am J Phys Med Rehabil 2002;81: 936–42.Search in Google Scholar
[3] Fishman SM, Caneris OA, Bandman TB, Audette JF, Borsook D. Injection of the piriformis muscle by fluoroscopic and electromyographic guidance. Reg Anesth Pain Med 1998;23:554–9.Search in Google Scholar
[4] Betts A. Combined fluoroscopic and nerve stimulator technique for injection of the piriformis muscle. Pain Phys 2004;7: 279–81.Search in Google Scholar
[5] Smith J, Hurdle MF, Locketz AJ, Wisniewski SJ. Ultrasound-guided piriformis injection: technique description and verification. Arch Phys Med Rehabil 2006;87:1664–7.Search in Google Scholar
[6] Peng PW, Narouze S. Ultrasound-guided interventional procedures in pain medicine: a review of anatomy, sonoanatomy, and procedures: part I: nonaxial structures. Reg Anesth Pain Med 2009;34: 458–74.Search in Google Scholar
© 2012 Scandinavian Association for the Study of Pain
Articles in the same Issue
- Editorial comment
- Spontaneous pain is reduced by conditioning pain modulation in peripheral neuropathy but not in fibromyalgia—Implications for different pain mechanisms
- Clinical pain research
- Differential pain modulation in patients with peripheral neuropathic pain and fibromyalgia
- Editorial comment
- Pulsed radiofrequency—Time for a clinical pause and more science
- Clinical pain research
- Pulsed radiofrequency in peripheral posttraumatic neuropathic pain: A double blind sham controlled randomized clinical trial
- Editorial comment
- Phantom pains and sensations – how does it feel? Only the patient really knows
- Clinical pain research
- Phantom phenomena – Their perceived qualities and consequences from the patient’s perspective
- Editorial comment
- Impact of mental stressor on conditioned pain modulation
- Original experimental
- The effect of a mental stressor on conditioned pain modulation in healthy subjects
- Editorial comment
- Pharmacological modulation of chronic pain after whiplash injury
- Clinical pain research
- Whiplash Associated Disorders (WAD): Responses to pharmacological challenges and psychometric tests
- Editorial comment
- Why are autonomic responses to pressure pain different from those to heat pain and ischaemic pain?
- Original experimental
- Cardiovascular responses to and modulation of pressure pain sensitivity in normotensive, pain-free women
- Correspondence
- Piriformis muscle injection guided by sciatic nerve stimulation: Quick, simple, and safe technique
- Correspondence
- Musculus piriformis syndrome: Localization and injection therapy—Comment to letter from Mayo-Moldes M et al. [1]
- Abstracts
- The “pain matrix” reloaded
- Abstracts
- Endpoints in animal pain models
- Abstracts
- Evaluating pain-related behavior in spinal cord injury
- Abstracts
- The role of the amygdala in sensory and emotional-like pain behavior in neuropathic animals
- Abstracts
- Peripheral and central pain mechanisms—From animal models to clinical research
- Abstracts
- Human experimental models of central sensitization—Do they bridge the gap between animal models and clinical observations?
- Abstracts
- Assessment of central sensitization in the clinic. Is it possible?
- Abstracts
- Migraine neurobiology and treatment
- Abstracts
- Chronic headaches–Goals and obstacles
- Abstracts
- Trigeminal neuralgia and other cranial neuralgias
- Abstracts
- Temporomandibular disorders: Pathophysiology and diagnosis
- Abstracts
- HIV-associated painful polyneuropathy
- Abstracts
- Keynote: Neuronal and glial signalling in pain neuroplasticity
- Abstracts
- Neuropathic pain—From guidelines to clinical practice
- Abstracts
- Postoperative pain treatment. What’s the evidence—And how to use it?
- Abstracts
- NSAIDs in postoperative pain
- Abstracts
- How should we prevent persistent postoperative pain?
- Abstracts
- Opioids: Genetics and receptors
- Abstracts
- Chronic pain and sleep disorders
- Abstracts
- Population-based studies on chronic pain: The role of opioids
- Abstracts
- Living beyond pain: Acceptance and commitment therapy
- Abstracts
- Modality specific alterations of esophageal sensitivity caused by longstanding diabetes mellitus
- Abstracts
- Validation of a porcine behavioural model of UVB induced inflammatory pain
- Abstracts
- Recovery after a lumbar disc herniation is dependent on a gender and OPRM1 Asn40Asp genotype interaction
- Abstracts
- Pain sensitivity changes in chronic pain patients with and without spinal cord stimulation assessed by nociceptive withdrawal reflex thresholds and electrical pain thresholds
- Abstracts
- Acceptance and commitment therapy for fibromyalgia: A randomized controlled trial
- Abstracts
- Sortilins in neuropathic pain
- Abstracts
- Systematic review of neuropathic component in persistent post-surgical pain
- Abstracts
- Pain prevalence in a university hospital in Iceland
- Abstracts
- The effect of tail-docking neonate piglets on ATF-3 and NR2B immunoreactivity in coccygeal dorsal root ganglia and spinal cord dorsal horn neurons: Preliminary data
- Abstracts
- Na+/K+-ATPase dependent regulation of astrocyte Ca2+ signalling: A novel mechanism for modulation of long-term pain?
- Abstracts
- Glutamate attenuates nitric oxide release from isolated trigeminal ganglion satellite glial cells
- Abstracts
- Acute behavioural responses to tail docking in piglets – Effects of increasing docking length?
- Abstracts
- Dose and administration-period play a key role in the effect of ceftriaxone on neuropathic pain in CCI-operated rats
- Abstracts
- Translational aspects of rectal evoked potentials: A comparative study in rats and humans
- Abstracts
- Time-course of analgesic effects of botulinum neurotoxin type A (BoNTA) on human experimental model of pain induced by injection of glutamate into temporalis muscle
- Abstracts
- The effect of nerve compression and capsaicin on contact heat evoked potentials (CHEPs) related to Aδ and C fibers
- Abstracts
- Effect of specific trapezius exercises vs. coordination training on corticomotor control of neck muscles
- Abstracts
- SNP in TNFα T308G is predictive for persistent postoperative pain following inguinal hernia surgery
- Abstracts
- Chronic pain in thoracotomy
- Abstracts
- The variability in thermal threshold-assessments in post-thoracotomy pain syndrome
- Abstracts
- Persistent pain, sensory disturbances and functional impairment after adjuvant chemotherapy for breast cancer
- Abstracts
- Neuroplastic alterations in brain responses to painful visceral stimulations reflects individual neuropathic symptoms in diabetes mellitus patients
- Abstracts
- Exercise and conditioned pain modulation have different effects on cuff pressure pain tolerance in humans
- Abstracts
- Hyperalgesia in human skin and deep-tissues inside and outside of a UVB irradiated area
- Abstracts
- Effect of experimental jaw muscle pain on bite force during mastication
- Abstracts
- Reflex threshold assessment methodology for evaluation of central sensitisation is vulnerable to EMG crosstalk
- Abstracts
- Cognitive modulation of experimental pain at spinal and cortical levels
- Abstracts
- Influence of emotionally loaded visual and gustatory stimuli on pain perception
- Abstracts
- Modulating pain with augmented reality
- Abstracts
- Offset analgesia: A reproducibility study
- Abstracts
- Visualization of painful process in peripheral tissue using positron emission tomography and [11C]-D-deprenyl
- Abstracts
- Mirror-image sensory dysfunction in the post-thoracotomy pain syndrome
- Abstracts
- Genetic variation in opioid receptor genes and sensitivity to experimental pain in male and female healthy volunteers
- Abstracts
- Mechanical sensitivity in migraine patients during attack, remission, and pain-free periods:A preliminary study
- Abstracts
- Multivariate pattern analysis of evoked brain potentials by temporal matching pursuit and support vector machine
- Abstracts
- Pain following stroke: A prospective study
- Abstracts
- Chronic thoracic pain in children after cardiac surgery
- Abstracts
- Chronic pain after breast augmentation is associated with both signs of peripheral nerve injury and central nervous mechanisms
- Abstracts
- Sensory phenotypes in patients with peripheral neuropathic pain evaluated with quantitative sensory testing
- Abstracts
- Is health related quality of life related to the pattern of chronic pain?
- Abstracts
- Comparison between ropivacaine local infiltration analgesia with ketorolac or placebo for total knee replacement surgery
- Abstracts
- Treatment with topical capsaicin: Experience from a pain clinic
- Abstracts
- Distribution of concussion related symptoms after whiplash injury in risk strata
- Abstracts
- HIV/AIDS in different cultures
- Abstracts
- Pain perception is altered in patients with medication-overuse headache but can improve after detoxification
- Abstracts
- Detoxification in a structured programme is effective for medication-overuse headache
Articles in the same Issue
- Editorial comment
- Spontaneous pain is reduced by conditioning pain modulation in peripheral neuropathy but not in fibromyalgia—Implications for different pain mechanisms
- Clinical pain research
- Differential pain modulation in patients with peripheral neuropathic pain and fibromyalgia
- Editorial comment
- Pulsed radiofrequency—Time for a clinical pause and more science
- Clinical pain research
- Pulsed radiofrequency in peripheral posttraumatic neuropathic pain: A double blind sham controlled randomized clinical trial
- Editorial comment
- Phantom pains and sensations – how does it feel? Only the patient really knows
- Clinical pain research
- Phantom phenomena – Their perceived qualities and consequences from the patient’s perspective
- Editorial comment
- Impact of mental stressor on conditioned pain modulation
- Original experimental
- The effect of a mental stressor on conditioned pain modulation in healthy subjects
- Editorial comment
- Pharmacological modulation of chronic pain after whiplash injury
- Clinical pain research
- Whiplash Associated Disorders (WAD): Responses to pharmacological challenges and psychometric tests
- Editorial comment
- Why are autonomic responses to pressure pain different from those to heat pain and ischaemic pain?
- Original experimental
- Cardiovascular responses to and modulation of pressure pain sensitivity in normotensive, pain-free women
- Correspondence
- Piriformis muscle injection guided by sciatic nerve stimulation: Quick, simple, and safe technique
- Correspondence
- Musculus piriformis syndrome: Localization and injection therapy—Comment to letter from Mayo-Moldes M et al. [1]
- Abstracts
- The “pain matrix” reloaded
- Abstracts
- Endpoints in animal pain models
- Abstracts
- Evaluating pain-related behavior in spinal cord injury
- Abstracts
- The role of the amygdala in sensory and emotional-like pain behavior in neuropathic animals
- Abstracts
- Peripheral and central pain mechanisms—From animal models to clinical research
- Abstracts
- Human experimental models of central sensitization—Do they bridge the gap between animal models and clinical observations?
- Abstracts
- Assessment of central sensitization in the clinic. Is it possible?
- Abstracts
- Migraine neurobiology and treatment
- Abstracts
- Chronic headaches–Goals and obstacles
- Abstracts
- Trigeminal neuralgia and other cranial neuralgias
- Abstracts
- Temporomandibular disorders: Pathophysiology and diagnosis
- Abstracts
- HIV-associated painful polyneuropathy
- Abstracts
- Keynote: Neuronal and glial signalling in pain neuroplasticity
- Abstracts
- Neuropathic pain—From guidelines to clinical practice
- Abstracts
- Postoperative pain treatment. What’s the evidence—And how to use it?
- Abstracts
- NSAIDs in postoperative pain
- Abstracts
- How should we prevent persistent postoperative pain?
- Abstracts
- Opioids: Genetics and receptors
- Abstracts
- Chronic pain and sleep disorders
- Abstracts
- Population-based studies on chronic pain: The role of opioids
- Abstracts
- Living beyond pain: Acceptance and commitment therapy
- Abstracts
- Modality specific alterations of esophageal sensitivity caused by longstanding diabetes mellitus
- Abstracts
- Validation of a porcine behavioural model of UVB induced inflammatory pain
- Abstracts
- Recovery after a lumbar disc herniation is dependent on a gender and OPRM1 Asn40Asp genotype interaction
- Abstracts
- Pain sensitivity changes in chronic pain patients with and without spinal cord stimulation assessed by nociceptive withdrawal reflex thresholds and electrical pain thresholds
- Abstracts
- Acceptance and commitment therapy for fibromyalgia: A randomized controlled trial
- Abstracts
- Sortilins in neuropathic pain
- Abstracts
- Systematic review of neuropathic component in persistent post-surgical pain
- Abstracts
- Pain prevalence in a university hospital in Iceland
- Abstracts
- The effect of tail-docking neonate piglets on ATF-3 and NR2B immunoreactivity in coccygeal dorsal root ganglia and spinal cord dorsal horn neurons: Preliminary data
- Abstracts
- Na+/K+-ATPase dependent regulation of astrocyte Ca2+ signalling: A novel mechanism for modulation of long-term pain?
- Abstracts
- Glutamate attenuates nitric oxide release from isolated trigeminal ganglion satellite glial cells
- Abstracts
- Acute behavioural responses to tail docking in piglets – Effects of increasing docking length?
- Abstracts
- Dose and administration-period play a key role in the effect of ceftriaxone on neuropathic pain in CCI-operated rats
- Abstracts
- Translational aspects of rectal evoked potentials: A comparative study in rats and humans
- Abstracts
- Time-course of analgesic effects of botulinum neurotoxin type A (BoNTA) on human experimental model of pain induced by injection of glutamate into temporalis muscle
- Abstracts
- The effect of nerve compression and capsaicin on contact heat evoked potentials (CHEPs) related to Aδ and C fibers
- Abstracts
- Effect of specific trapezius exercises vs. coordination training on corticomotor control of neck muscles
- Abstracts
- SNP in TNFα T308G is predictive for persistent postoperative pain following inguinal hernia surgery
- Abstracts
- Chronic pain in thoracotomy
- Abstracts
- The variability in thermal threshold-assessments in post-thoracotomy pain syndrome
- Abstracts
- Persistent pain, sensory disturbances and functional impairment after adjuvant chemotherapy for breast cancer
- Abstracts
- Neuroplastic alterations in brain responses to painful visceral stimulations reflects individual neuropathic symptoms in diabetes mellitus patients
- Abstracts
- Exercise and conditioned pain modulation have different effects on cuff pressure pain tolerance in humans
- Abstracts
- Hyperalgesia in human skin and deep-tissues inside and outside of a UVB irradiated area
- Abstracts
- Effect of experimental jaw muscle pain on bite force during mastication
- Abstracts
- Reflex threshold assessment methodology for evaluation of central sensitisation is vulnerable to EMG crosstalk
- Abstracts
- Cognitive modulation of experimental pain at spinal and cortical levels
- Abstracts
- Influence of emotionally loaded visual and gustatory stimuli on pain perception
- Abstracts
- Modulating pain with augmented reality
- Abstracts
- Offset analgesia: A reproducibility study
- Abstracts
- Visualization of painful process in peripheral tissue using positron emission tomography and [11C]-D-deprenyl
- Abstracts
- Mirror-image sensory dysfunction in the post-thoracotomy pain syndrome
- Abstracts
- Genetic variation in opioid receptor genes and sensitivity to experimental pain in male and female healthy volunteers
- Abstracts
- Mechanical sensitivity in migraine patients during attack, remission, and pain-free periods:A preliminary study
- Abstracts
- Multivariate pattern analysis of evoked brain potentials by temporal matching pursuit and support vector machine
- Abstracts
- Pain following stroke: A prospective study
- Abstracts
- Chronic thoracic pain in children after cardiac surgery
- Abstracts
- Chronic pain after breast augmentation is associated with both signs of peripheral nerve injury and central nervous mechanisms
- Abstracts
- Sensory phenotypes in patients with peripheral neuropathic pain evaluated with quantitative sensory testing
- Abstracts
- Is health related quality of life related to the pattern of chronic pain?
- Abstracts
- Comparison between ropivacaine local infiltration analgesia with ketorolac or placebo for total knee replacement surgery
- Abstracts
- Treatment with topical capsaicin: Experience from a pain clinic
- Abstracts
- Distribution of concussion related symptoms after whiplash injury in risk strata
- Abstracts
- HIV/AIDS in different cultures
- Abstracts
- Pain perception is altered in patients with medication-overuse headache but can improve after detoxification
- Abstracts
- Detoxification in a structured programme is effective for medication-overuse headache