The level of unpleasantness of pain influences the choice of home treatment during medical abortion
-
Satu Suhonen


Abstract
Background and aims
Medical abortion is often performed at outpatient clinics or gynaecological wards. Yet, some women may stay at home during medical abortion. Pain has been reported to be one of the main side effects of the procedure.
Methods
We studied whether perceived abortion pain was related to the subjectively evaluated ability to stay at home during medical abortion. The size of the study group was 29 women. We also studied how well these women remembered the intensity and unpleasantness of the abortion pain in a control visit performed 3–6 weeks after abortion.
Results
Especially, the unpleasantness associated with the pain during abortion was an important predictor when women evaluated their ability to stay at home during medical abortion. In those women who might have been able to stay at home in their own view, midwives looking after these women at the outpatient clinic estimated the pain intensity and unpleasantness also about 50% lower than in those who were not able to stay home in their own view. There were no significant differences in intensity, unpleasantness in hindsight of menstruation pain, or the area of this pain in the pain drawings in those women who considered that they might have stayed at home during medical abortion when compared with those who did not. No difference was found in age, gestational age, magnitude of previous pregnancies, miscarriages, vaginal deliveries, induced abortions, Beck’s Depression Index (BDI), Beck’s Anxiety Index (BAI) or AUDIT scores between those who could have stayed at home or those who would not have been able to stay at home during abortion. Components of abortion pain decreased significantly during the second post-abortion day. The more deliveries the subject had experienced the less pain she had during abortion. Multiparous women reported less than a fourth of the pain magnitude of the nulliparous women during abortion. Parity explained both intensity and unpleasantness of abortion pain better than the expected ability to stay at home. The remembrance of the intensity or unpleasantness of abortion pain correlated with actual pain reported at the time of abortion. However, this remembrance did not correlate with the ability to stay at home during the medical abortion.
Conclusions
The unpleasantness of pain during and immediately after abortion was recalled, not as a measure of the pain itself, but as a deciding factor in their judgement of whether or not they would be able to undergo medical abortion at home. Abortion pain is an important factor in enhancing home-based management of medical abortions. Medical staff may be able to detect those women who do not cope at home during the process by observing the intensity of pain. Therefore, proper treatment of pain might reduce the need for hospital-based medical abortions.
Implications
These patients need better care and guidelines for the care of women undergoing medical abortions should include clear recommendations for analgesic treatments, at the least adequate doses of nonopioid analgesics such as paracetamol in combination with NSAIDs like ibuprofen or diclofenac.
1 Introduction
Pain, with all of its components, or rather insufficient treatment of them, has been suggested to be one of the main reasons why many patients might prefer surgical abortion instead of the medical one [1,2]. For example, in Finland, surgical abortion is performed under general anaesthesia which reduces pain related to the abortion procedure. Mifepristone and prostaglandin analogues are widely used to induce medical abortion in early pregnancy [3,4,5]. Pain is one of the main side-effects in this method of abortion [4,5].
Pain sensation consists of two different components, sensory-discriminative (intensity of sensation) and affective-motivational (unpleasantness evoked by sensation), which are differently processed in the central nervous system [6] and which are, therefore, differently sensitive to various pharmacological agents [7,8,9]. Thus, the affective component of pain should be separable from the plain magnitude estimate. The clinical importance of differentiating between the intensity and the unpleasantness of pain is that anxiolytic drugs can specifically decrease the affective component of pain and thus help management of pain [6,7,8,9]. There are reports suggesting that (n) pain during abortion is accompanied and modified by exaggerated mental stress [10,11,12]. Yet, the putative role of affective-motivational pain component on abortion related distress is not well studied.
The present work aimed to answer two main questions. First, we wanted to study if pain during medical abortion correlates with the woman’s subjectively perceived ability to stay at home during medical abortion. Secondly, we wanted to study if memory of the abortion pain correlates with the perceived abortion pain and thereby, also with estimated ability to stay at home during the process.
2 Materials and methods
2.1 Subjects
Subjects for this study were drawn from healthy, Finnish-speaking women living in the city of Vantaa seeking abortion at the outpatient clinic of Helsinki University Central Hospital and choosing the medical method (Fig. 1). The local ethics committee (Ethical committee of HUCH) approved the study and the volunteer subjects gave a written informed consent of participation in the study. A questionnaire performed just before and during medical abortion, at the follow up visit 3–6 weeks after abortion, and a pain diary were chosen as methods.
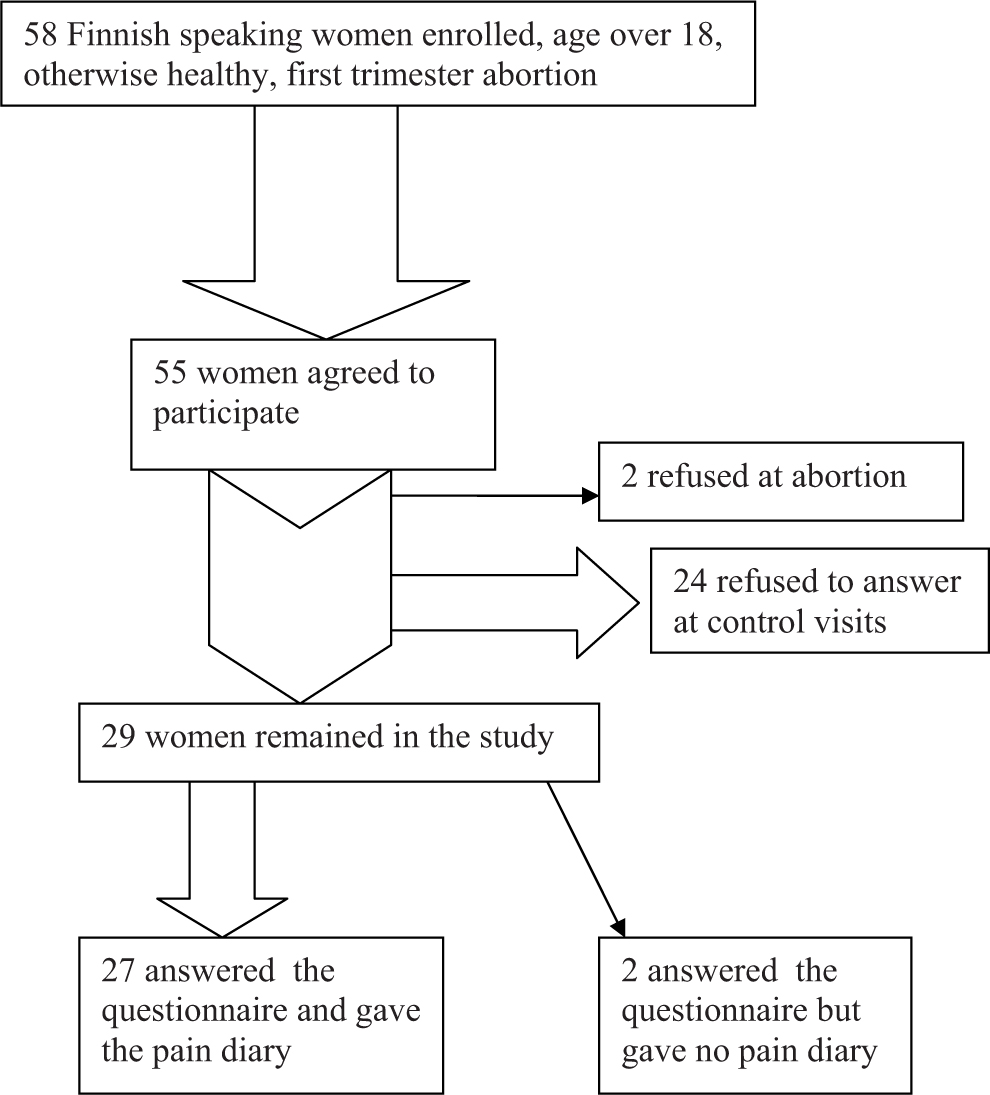
Patient flow in the study.
2.2 Questionnaire
After agreeing to participate in the study, the women were interviewed by midwives of the department. The information about the age of the women, number of former pregnancies, deliveries, abortions and miscarriages were recorded. Remembrance of the intensity of the menstruation pain, e.g. sensory-discriminative component of pain, was recorded with the common 100 mm visual analogue scale (VAS) [6,9,13]. Remembrance of the affective motivational component (unpleasantness) of the menstruation pain was separately determined by using VAS, too [6,7,8,9]. The subject made a pain drawing. The area of pain in the drawing is also suggested to be a reliable system to detect severity of pain in chronic pain patients [14]. The size of the remembrance of pain area was recorded with a transparent planimeter (mm2). The medications the patients most often used to relieve pain during menstruation were recorded. The number and dosage of different preparations of pain relieving drugs was the measured variable.
2.3 Medical abortion
The length of the pregnancy (days) was evaluated by ultrasound before choosing the method of abortion. During the study period, medical abortion was an alternative to surgical evacuation if the gestational age was ≤63 days by ultrasound. The medical abortion at this hospital included at the time of the study, 200mg mifepristone followed by 400 μg misoprostol administered vaginally. In the case of heavier bleeding after mifepristone, misoprostol was given orally. The women stayed at the out-patient clinic usually for 3–4 h. The maximum magnitude of pain sensation and maximum unpleasantness evoked by the pain was recorded with the VAS-method and each woman made a pain drawing, too, just before deciding to leave the ward. Without knowing the estimates made by the woman, the midwife observing the woman undergoing medical abortion also made an evaluation of the maximum intensity of pain sensation and maximum unpleasantness evoked by the pain with the VAS-method. The medication used for pain relief during abortion was recorded, too. Types and dosages, and number of times analgesics were given were scored separately. As a rule paracetamol (500 mg) and a combination of paracetamol (500 mg) + codeine (30 mg) was routinely administrated when suitable as pain prophylaxis at the same time misoprostol was given [15,16].When this combination was not suitable ibuprofen 600mg was used.
A pain diary with daily questions concerning greatest intensity and unpleasantness of daily pain after abortion was given to the patients. Every day when they felt pain, the patients marked in the diary the intensity and unpleasantness of pain (VAS) and the medications they used to relieve pain. They were also advised to draw a pain drawing every day for 1 week.
In the control visit to the public-health nurse, the patients returned the pain diaries, and answered a questionnaire. They were asked to try to remember the intensity and unpleasantness of pain (VAS). They were asked to try to redraw the pain picture of the abortion pain by memory. The nurse asked the question “Would you now think that you could have stayed at home during the medical abortion?”. The patient was allowed to answer only “yes” or “no”. BDI, BAI and AUDIT-questionnaire for detection of substance abuse were performed at the follow-up visit.
2.4 Statistical analysis
Data are expressed as mean ± SD, or median and range or inter-quartile range (IQR). Differences between two groups were analyzed using Student’s t-test or Mann–Whitney U-test and, when appropriate, paired t-test or Wilcoxon signed rank test. To determine the consistency of the assessments in the pain intensity tests for each patient, and correlations between the evaluations provided by the nurses and the different recorded factors, the Pearson rank correlation was used [17,18]. Analyzing differences between several groups was performed with one and two way ANOVA. Both nonparametric and parametric versions were used when needed. Repeated measurements with multi-group comparisons were analyzed with repeated measures (RM) one or two way ANOVA. Statistical analyses were performed with PC and Sigma Stat for Windows (Systat Software Inc., Point Richmond, CA, USA). Statistical significance was set at P-value < 0.05.
3 Results
Characterization of the patients is presented in Table 1. The number of previous deliveries was higher in those women who considered that they might have stayed at home during medical abortion (median 1 vs. 0, P = 0.032, U-test). Intensity (one way ANOVA, F{Df 2,26} = 4.432, P = 0.022) and unpleasantness (Kruskall–Wallis ANOVA on ranks: H{Df 2} = 8.456, P = 0.015) of pain at the time of abortion was also milder the more previous deliveries the women had (Fig. 2). Midwives’ estimation of pain intensity (mean ± SD: 26 ± 27mm vs. 51± 30mm, P = 0.029, t-test) and unpleasantness (median 12 vs. 39, P = 0.031, U-test) was lower in those women who stated that they might have been able to stay at home. There were no significant differences in intensity, and unpleasantness of the remembrance of menstruation pain, or the area of this pain in the pain drawings of those women who considered that they might have stayed home during medical abortion when compared with those who did not consider home treatment an option. No differences were found in age, gestational age, number of previous pregnancies, miscarriages, vaginal deliveries, induced abortions, BDI, BAI or AUDIT scores between those who could have stayed at home or those who would not have been able to stay at home during abortion, either. Parity explained both intensity (two way ANOVA: F{Df 1,26} = 5.461, P = 0.029) and unpleasantness (F{Df 1,26} = 5.462, P = 0.029) of abortion pain better than the expected ability to stay at home (intensity: F{Df 1,26} = 1.055, P = 0.315; unpleasantness F{Df 1,26} = 2.242, P = 0.148). There was no interaction between parity and expected ability to stay at home (intensity: F{Df 1,26} = 0.0686, P = 0.796; unpleasantness: F{Df 1,26} = 0.441, P = 0.513) in the effect on pain.

Effect of parity on different components of abortion pain. Mean (bars) and SD (brackets) are shown.
Descriptive data of the subjects.
| Parameter | Mean | SD | ||
|---|---|---|---|---|
| Age | 26.6 years | 6.1 years | ||
| Duration of pregnancy | 47 days | 8 days | ||
| Magnitude of menstruation pain (VAS) | 40 mm | 32 mm | ||
| Unpleasantness of menstruation pain (VAS) | 42 mm | 32 mm | ||
| Area of pain in drawing, menstruation, planimeter | 206 mm2 | 257 mm2 | ||
| Magnitude of abortion pain (VAS) | 44 mm | 34 mm | ||
| Unpleasantness of abortion pain (VAS) | 44 mm | 35 mm | ||
| Area of pain in drawing, abortion, planimeter | 212mm2 | 235 mm2 | ||
| Parameter | Range | Median | Inter quartile range 25% | Inter quartile range 75% |
|
|
||||
| Number of pregnancies | 0–7 | 2 | 1 | 2 |
| Number of induced abortions | 0–3 | 0 | 0 | 1 |
| Number of miscarriages | 0–4 | 0 | 0 | 0 |
| Number of deliveries | 0–3 | 0 | 0 | 2 |
| Number of vaginal deliveries | 0–2 | 0 | 0 | 1 |
The remembrance of abortion pain correlated with the pain at the time of medical abortion (intensity: r = 0.370, P = 0.0485; unpleasantness r = 0.517, P = 0.004). Both components of pain during medical abortion were clearly more severe in those patients who estimated that they could not have been at home during medical abortion. However, no such difference existed in their pain memories (Fig. 3). The intensity of pain during and after medical abortion was higher (two way RM-ANOVA: F{Df 1} = 4.334, P = 0.047) in those who thought they would not be able to stay at home during abortion. The pain intensity relieved significantly two days after abortion (F{Df 3} = 9.339, P < 0.001) but there was no interaction between time and expected ability to stay at home (Fig. 4). Unpleasantness of abortion pain tended to be significantly higher in women who thought they would not be able to stay at home (F{Df 1} = 3.688, P = 0.065) and in these patients the unpleasantness relieved significantly within two days, too (F{Df 3} = 9.140, P < 0.001). There was a significant interaction between time and expected ability to stay at home (F{Df 3} = 2.752, P = 0.049) suggesting that the difference in unpleasantness of pain separating those Women who thought they would be able to stay at home from those who did not, took place at the time of abortion (Fig. 4).

Comparison of intensity and unpleasantness of abortion pain with the remembrance of the respective pain components. Mean (bars) and SD (brackets) are shown.

Development of pain components after abortion (0-point) in patients who by self-estimation would or would not have been able to stay at home during the process. Mean (dots) and SD (brackets) are shown.
4 Discussion
Both components of abortion pain were more severe in women who did not feel fit enough to stay at home during medical abortion. Patients’ estimates of sensory-discriminative (intensity) and affective-motivational (unpleasantness) components of abortion pain correlated well with each other and their magnitudes matched well. Our results support the evidence that pain is one of the main side effects to be treated in medical abortion [1,2,4,5].
The affective-motivational component of abortion pain (unpleasantness) seemed to predict how the subjects estimated their ability to stay at home during medical abortion. Although unpleasantness of pain is known to be separable from plain intensity estimate [6,7,8,9], no significant difference between the magnitude of these components was found during the medical abortion process itself. However, considerably later (at the visit to the public-health nurse) the unpleasantness, but not the intensity of pain at the time of the abortion process, seemed to have an impact on the subject’s estimate of her ability to stay at home during medical abortion. Significant unpleasantness due to pain reduced the subject’s self-estimated ability to undergo medical abortion at home. Thus, memory of unpleasant pain existed but the women failed to recall it clearly as a VAS-measure at the visit to the public-health nurse. Instead, they obviously recalled the unpleasant memory about pain by formulating their judgement how they might have coped with medical abortion process at home. Thus, the unpleasantness of pain during and immediately after abortion was recalled, not as a measure of the pain itself, but as a deciding factor in their judgement of whether or not they would be able to undergo medical abortion at home.
Our results are only partially in line with former studies. Memory of experimental acute pain has been reported to be enhanced by the recall of unpleasant affection towards the original painful event [19]. The affective state at the time of the procedure has been reported to be related just to the recall of the long term affective component of pain [20]. We failed to observe enhanced recall of measurable painful memory but we observed increased aversion or feeling of helplessness towards the procedure that induced unpleasant pain. Nevertheless, our findings support reports suggesting that the affective burden of abortion modifies pain perception [10,11,12] and should also be managed during the procedure.
The more previous deliveries the subject had the less she suffered from pain. Parity was more important in determining the severity of pain than, for example, perceived ability to stay at home during abortion. The strong role of parity in predetermining the magnitude of abortion pain in the present study is in line with the former studies [12,21].
Midwives who took care of women during medical abortion were able to detect those subjects who were in severe pain, thereby identifying the women who would not have been able to stay at home during medical abortion. Thus, their opinion about the severity of pain might be useful when considering which woman can undergo medical abortion at home if this situation would happen again.
The main shortcoming of the present study was the small number of patients. We are sure that this difficulty in recruiting patients had a major impact on our results. Women were not eager to participate in this kind of questionnaire study during an abortion process. This has hampered other attempts to study medical abortion and has led to small numbers of patients in experimental groups, too [1].
A combination of per oral paracetamol (1000 mg) and codeine (30 mg) [15,16] was routinely administrated when applicable as pain prophylaxis for medical abortion at the time misoprostol was given. Whether this is an adequate dosage remains controversial. According to Bjørge et al. [22], most of the women (85%) required more than 800mg paracetamol and 60mg codeine via rectum to relieve their pain during the first hours in the ward. There is room for future work to determine optimal prophylactic dosage of nonopioid and opioid analgesics to relieve pain induced by medical abortion [23].
In conclusion, we report that the high affective component of pain during medical abortion modifies subsequent perceived ability to stay at home during the process. Parity also has an impact on that ability. The more deliveries the subject had the less there was pain during medical abortion and the easier it would have been to stay at home during the abortion. Medical staff may be able to detect those women who do not cope at home during the process by observing the intensity of pain.
DOI of refers to article: 10.1016/j.sjpain.2010.11.004.
References
[1] Grimes DA, Susan Smith MS, Witham AD. Mifepristone and misoprostol versus dilation and evacuation for midtrimester abortion: a pilot randomised controlled trial. BJOG 2004;111:148–53.Search in Google Scholar
[2] Rørbye C, Nørgaard M, Nilas L. Medical versus surgical abortion: comparing satisfaction and potential confounders in a partly randomized study. Hum Reprod 2005;20:834–8.Search in Google Scholar
[3] Cameron IT, Michie AF, Baird DT. Therapeutic abortion in early pregnancy with antiprogestogen RU486 alone or in combination with prostaglandin analogue (gemeprost). Contraception 1986;34:459–68.Search in Google Scholar
[4] Silvestre L, Dubois C, Renault M, Rezvani Y, Baulieu EE, Ulmann A. Voluntary interruption of pregnancy with mifepristone (RU 486) and a prostaglandin analogue. A large-scale French experience. NEJM 1990;322:645–8.Search in Google Scholar
[5] Spitz IM, Bardin CW, Benton L, Robbins A. Early pregnancy termination with mifepristone and misoprostol in the United States. NEJM 1998;338: 1241–7.Search in Google Scholar
[6] Price DD. Psychological and neural mechanisms of the affective dimension of pain. Science 2000;288:1769–72.Search in Google Scholar
[7] Gracely RH, McGrath P, Dubner R. Validity and sensitivity of ratio scales of sensory and affective verbal pain descriptors: manipulation of affect by diazepam. Pain 1978;5:19–29.Search in Google Scholar
[8] Gracely RH, McGrath P, Dubner R. Narcotic analgesia: fentanyl reduces the intensity but not the unpleasantness of painful tooth pulp sensations. Science 1979;203:1261–3.Search in Google Scholar
[9] Kauppila T, Kemppainen P, Tanila H, Pertovaara A. Effect of systemic medetomidine, an alpha2 adrenoceptor agonist, on experimental pain in humans. Anesthesiology 1992;74:3–8.Search in Google Scholar
[10] Belanger E, Melzack R, Lauzon P. Pain on first-trimester abortion: a study of psychosocial and material predictors. Pain 1989;36:339–50.Search in Google Scholar
[11] Wells N. Pain and distress during abortion. Health Care Women Int 1991;12:293–302.Search in Google Scholar
[12] Wiebe E. Pain control in medical abortion. Int J Gynaecol Obstet 2001;74:275–80.Search in Google Scholar
[13] Bond MR, Pilowsky I. Subjective assessment of pain and its relationship to the administration of analgesics in patients with advanced cancer. J Psychosomatic Res 1966;10:203–8.Search in Google Scholar
[14] Margolis RB, Tait RC, Krause SJ. A rating system for use with patient pain drawings. Pain 1986;24:57–65.Search in Google Scholar
[15] Niinimaki M, Jouppila P, Martikainen H, Talvensaari-Mattila A. A randomized study comparing efficacy and patient satisfaction in medical or surgical treatment of miscarriage. Fertil Steril 2006;86:367–72.Search in Google Scholar
[16] Fiala C, Swahn ML, Stephansson O, Gemzell-Danielsson K. The effect of non-steroidal anti-inflammatory drugs on medical abortion with mifepristone and misoprostol at 13-22 weeks gestation. Hum Reprod 2005;20:3072–7.Search in Google Scholar
[17] Redelmeier DA, Kahneman D. Patients’ memories of painful medical treatments: real-time and retrospective evaluations of two minimally invasive procedures. Pain 1996;66:3–8.Search in Google Scholar
[18] Krulewitch H, London MR, Skakel VJ, Lundstedt GJ, Thomason H, Brummel-Smith K. Assessment of pain in cognitively impaired older adults: a comparison of pain assessment tools and their use by non-professional caregivers. J Am Geriatr Soc 2000;48:1607–11.Search in Google Scholar
[19] Gedney JJ, Logan H. Memory for stress-associated acute pain. J Pain 2004;5(March (2)):83–91.Search in Google Scholar
[20] Gedney JJ, Logan H, Baron RS. Predictors of short-term and long-term memory of sensory and affective dimensions of pain. J Pain 2003;4:47–55.Search in Google Scholar
[21] Hamoda H, Ashok PW, Flett GMM, Templeton A. Analgesia requirements and predictors of analgesia use for women undergoing medical abortion up to 22 weeks of gestation. BJOG 2004;111:996–1000.Search in Google Scholar
[22] Bjørge L, Johnsen SL, Midbøe G, Augestad G, Økland I, Helland H, Stray-Pedersen S, Iversen OE. Early pregnancy termination with mifepristone and misoprostol in Norway. Acta Obstet Gynecol Scand 2001;80:1056–61.Search in Google Scholar
[23] Livshits A, Machtinger R, David LB, Spira M, Moshe-Zahav A, Seidman DS. Ibuprofen and paracetamol for pain relief during medical abortion: a double-blind randomized controlled study. Fertil Steril 2009;91: 1877–80.Search in Google Scholar
© 2010 Scandinavian Association for the Study of Pain
Articles in the same Issue
- Editorial comment and review
- Redheads, pain mechanisms and genetics: Lessons learned from inconclusive studies
- Clinical pain research
- Pain sensitivity and experimentally induced sensitisation in red haired females
- Editorial comment
- Assessment and mechanisms of mechanical allodynia
- Clinical pain research
- The perception threshold counterpart to dynamic and static mechanical allodynia assessed using von Frey filaments in peripheral neuropathic pain patients
- Editorial comment
- Pain during pharmacologically induced termination of pregnancy
- Clinical pain research
- The level of unpleasantness of pain influences the choice of home treatment during medical abortion
- Editorial comment
- Botulinum toxin for the treatment of pain?
- Original experimental
- Dysport® for the treatment of myofascial back pain: Results from an open-label, Phase II, randomized, multicenter, dose-ranging study
- Editorial comment
- Trends in analgesic drug use evaluated by national prescription data bases: Differences between immigrants and native citizens of Norway
- Observational studies
- Dispensing of prescribed analgesics in Norway among young people with foreign-or Norwegian-born parents
Articles in the same Issue
- Editorial comment and review
- Redheads, pain mechanisms and genetics: Lessons learned from inconclusive studies
- Clinical pain research
- Pain sensitivity and experimentally induced sensitisation in red haired females
- Editorial comment
- Assessment and mechanisms of mechanical allodynia
- Clinical pain research
- The perception threshold counterpart to dynamic and static mechanical allodynia assessed using von Frey filaments in peripheral neuropathic pain patients
- Editorial comment
- Pain during pharmacologically induced termination of pregnancy
- Clinical pain research
- The level of unpleasantness of pain influences the choice of home treatment during medical abortion
- Editorial comment
- Botulinum toxin for the treatment of pain?
- Original experimental
- Dysport® for the treatment of myofascial back pain: Results from an open-label, Phase II, randomized, multicenter, dose-ranging study
- Editorial comment
- Trends in analgesic drug use evaluated by national prescription data bases: Differences between immigrants and native citizens of Norway
- Observational studies
- Dispensing of prescribed analgesics in Norway among young people with foreign-or Norwegian-born parents