A Case of Idiopathic Colonic Varices
-

Abstract
Colonic varices, usually detected by means of colonoscopy, are extremely rare and typically indicative of portal hypertension or chronic hepatopathology. Even more rare are those cases with no underlying disease, or idiopathic colonic varices. The authors report a case of these unexplained varices found during colonoscopy of a 30-year-old man with a 10-year history of diarrhea and occasional bloody stool. A thorough workup was performed, revealing no underlying abnormalities for his varices. Additionally, the authors review the literature of this rare diagnosis. Physicians must rule out hepatic, vascular, and cardiac causes before classifying a case of varices as idiopathic.
Colonic varices are a source of rectal bleeding in which attempts should always be made to find an underlying etiologic pattern. Physicians should rule out a hepatic cause—including portal hypertension, fibrosis, cirrhosis, necrosis, and thrombosis, as well as vascular anomalies and cardiac conditions—before classifying a case of varices as idiopathic.
Idiopathic colonic varices are extremely rare, with 38 cases reported in the literature, to our knowledge.1-31 Bright red blood in the rectum with or without pain is often the presenting sign. Typical etiologic factors of a colonic varix are liver disease with portal hypertension or portal or mesenteric thrombosis. Less common causes are vascular malformations, heart failure, and abdominal adhesions. When these causes have been ruled out, the colonic varices are considered idiopathic. In the present report, we describe a case of idiopathic colonic varices.
Report of Case
A 30-year-old man presented to a community emergency department because of intense abdominal discomfort, distention, and diarrhea. His past medical history was notable for a 10-year history of chronic diarrhea, bloating, occasional bloody stool, and no family history of gastrointestinal disease or complications. A computed tomographic (CT) scan of the abdomen revealed a possible partial obstruction in the terminal ileum. The patient was discharged to home with analgesics and instructed to follow up with a gastroenterologist.
Five days later, the patient presented to our office with continued mild to moderate abdominal discomfort and diarrhea. Family history, social history, and physical examination findings were unremarkable. After a review of the CT scan, which showed contrast material and some evidence of bowel wall thickening, an inflammatory process was suspected. Laboratory tests were ordered, and a colonoscopy was scheduled for the next day.
The colonoscopy revealed diffuse erythema and congestion in the terminal ileum and throughout the colon. Markedly dilated, tortuous veins were appreciated throughout the colon (Figure 1) and rectum. From biopsies obtained throughout the colon, pathologic results revealed dilated thin-walled vessels in the lamina propria with vascular congestion and hemorrhage (Figure 2) but did not reveal colitis. Because of the finding of varices throughout the colon, portal hypertension or liver disease was suspected.

Colonoscopic images of varices revealed markedly dilated, tortuous veins that were appreciated throughout the colon of a 30-year-old man with abdominal discomfort and diarrhea.
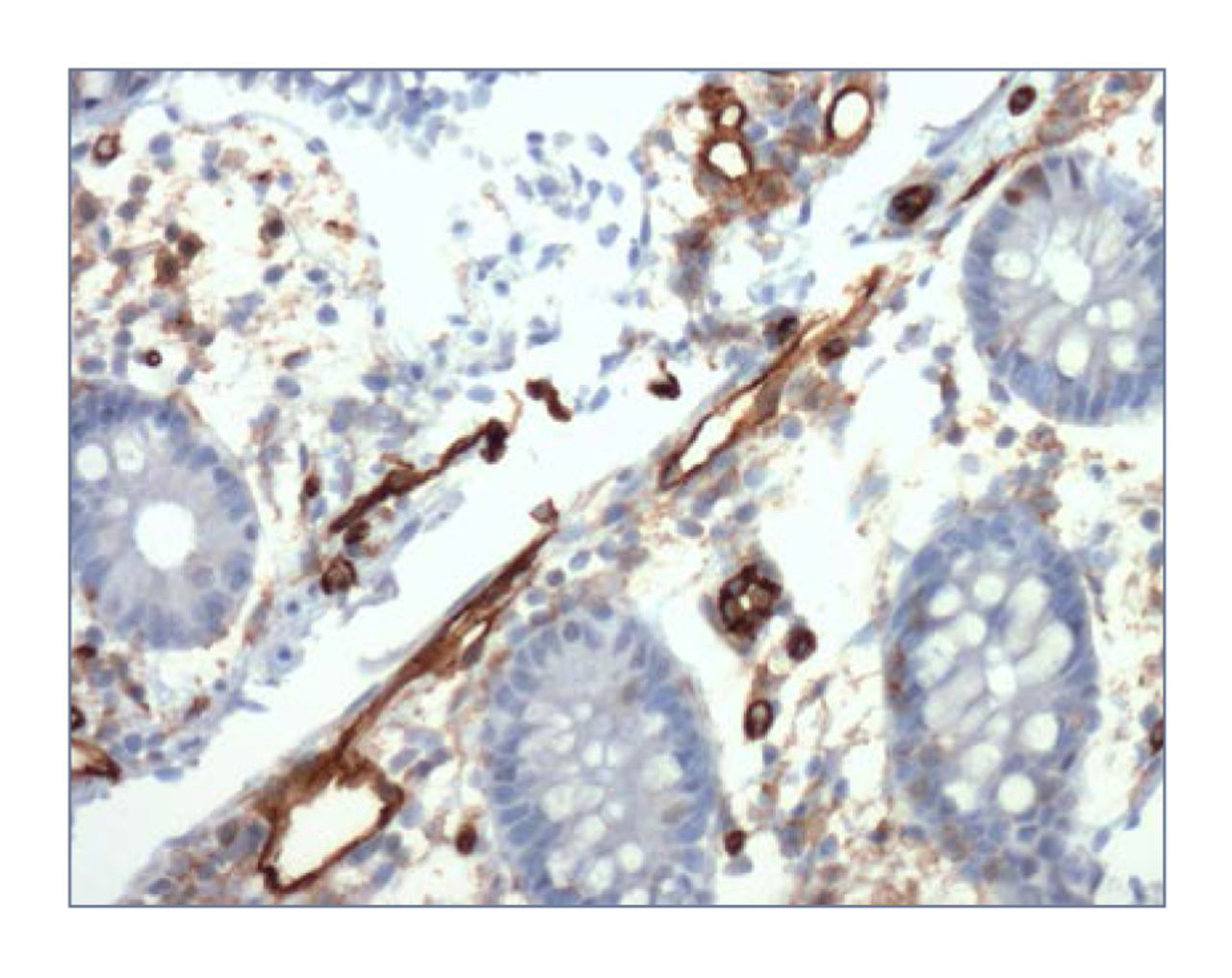
A 20X CD31 stain (mouse monoclonal JC/70A) of a sample taken from the colon of a 30-year-old man with abdominal discomfort and diarrhea, revealing dilated, thin-walled vessels in the lamina propria with vascular congestion and hemorrhage.
The CT scan was reviewed again and discussed with the original reading radiologist, and it was determined that there was no sign of liver disease and that mesenteric arteries and veins appeared normal. All results from other laboratory tests, including liver enzyme levels, were also unremarkable.
Two weeks after initial presentation, Doppler ultrasonography was performed and results revealed normal flow in the hepatic and portal veins, as well as in the inferior vena cava. Ultrasonographic image showed diffusely increased echogenicity consistent with diffuse fatty change. A core liver biopsy was ordered to investigate a hepatic etiologic process in the varices.
Six weeks after initial presentation, an upper endoscopy was performed and revealed no esophageal varices or signs of venous congestion.
At 8 weeks from initial presentation, the core liver biopsy was performed and confirmed mild to moderate steatosis but no significant cirrhosis, necrosis, or bridging fibrosis. At the time of the biopsy, hepatic and portal vein pressure measurements were obtained and revealed a mean right atrial pressure of 10 mm Hg, a mean free hepatic vein pressure of 10 mm Hg, and a mean wedged hepatic vein pressure of 11 mm Hg. These measurements yield a hepatic vein pressure gradient of 1 mm Hg (normal, 1-5 mm Hg) and allowed us to rule out hepatic outflow obstruction and portal hypertension.
At the completion of the 8-week visit, the patient had already experienced a moderate improvement of symptoms, with 2 soft bowel movements per day and no associated pain. After an extensive workup, no clear explanation for his colonic varices emerged. We continue to follow up this patient for possible recurrence and monitor for signs of liver disease.
Discussion
Even in the presence of advanced liver disease, colonic varices are relatively rare. Bresci et al32 detected colonic varices in 31% of patients with cirrhosis of the liver. The prevalence of colonic varices is virtually unattainable because the condition could remain subclinical for a life-time. In an autopsy-based study that explored the prevalence of the condition, Feldman et al33 found colonic varices in 2 of 2912 cadavers (0.0007%).
Idiopathic colonic varices are extremely rare, with 38 cases to our knowledge being reported in the literature to date.1-31 Age at diagnosis varied from 14 to 81 years with a mean, median, and mode of 41, 37, and 33 years, respectively. The male-to-female ratio of reported cases of idiopathic colonic varices is 25:13. Most cases presented with a history of blood in the stool. Due to the idiopathic nature of the disease and the associated blood loss, at least 13 cases required at least a partial resection of the bowel.1-13 However, conservative management was deemed prudent in most cases.12,14-27
Most colonic varices of known origin were found along either the distribution of the superior or inferior mesenteric vein, but idiopathic varices tended to occur throughout the colon. Gudjonsson et al34 reviewed 69 cases of colonic varices and found 66% of instances distributed along the inferior mesenteric vein, 26% along that of the superior mesenteric vein, and 8% throughout the colon. Adding in the present case, there are currently 26 of 39 cases (67%) of documented idiopathic colonic varices that involved the entire colon.1-6,10,12-19,21-23,25-30
There have been several cases of colonic varices without portal hypertension in which an alternate etiologic process was identified. Three instances of vascular malformations leading to colonic varices,35-37 with 2 including a hereditary component,35,36 have been documented. At least 15 cases of idiopathic colonic varices in the literature have a familial component.12,14,19,22,28,29,31 Our patient, however, has no family history of gastrointestinal disease or complications.
Adhesions have been documented as a cause of colonic varices without portal hypertension,38 but the varices were localized to an area of the colon in the vicinity of the site of the adhesion. The varices in our patient were throughout the colon and rectum and do not follow the localized profile that would be expected with adhesions.
Congestive heart failure has also been implicated in colonic varices.33 This condition can lead to venous congestion, such as that seen in colonic varices. Nevertheless, our patient showed no signs of venous congestion anywhere else in the body and no indications of heart disease.
Conclusion
Idiopathic colonic varices generally manifest with active, or a history of, rectal bleeding.4 In cases of idiopathic colonic varices with multiple recurrences or refractory bleeding, surgical colectomy may be considered. However, in many patients, including ours, conservative management was indicated.
-
Financial Disclosures: None reported.
References
1 Gentilli S Aronici M Portigliotti L Pretato T Garavoglia M . Idiopathic ileo-colonic varices in a young patient[published online September 11, 2011]. Updates Surg.2012;64(3):235-238. doi:10.1007/s13304-011-0101-8.10.1007/s13304-011-0101-8Search in Google Scholar PubMed
2 Grasso E Sciolli L Ravetta F Pelloni A . A rare case of idiopathic colonic varices: case report and review of the literature. Chirurgia. 2012;25(2):111-114.Search in Google Scholar
3 Krishna RP Singh RK Ghoshal UC . Recurrent lower gastrointestinal bleeding from idiopathic ileocolonic varices: a case report. J Med Case Rep.2010;4:257. doi:10.1186/1752-1947-4-257.10.1186/1752-1947-4-257Search in Google Scholar PubMed PubMed Central
4 Abraham-Igwe C Patel R . Idiopathic colonic varices: a case report. Endoscopy. 2002;34(8):680.10.1055/s-2002-33235Search in Google Scholar PubMed
5 Lopes LM Ramada JM Certo MG et al. . Massive lower gastrointestinal bleeding from idiopathic ileocolonic varix: report of a case. Dis Colon Rectum.2006;49(4):524-526.10.1007/s10350-005-0279-2Search in Google Scholar PubMed
6 Keren D Rainis T Stermer E Goldstein O Lavy A . Extensive idiopathic colonic varices in a young patient. Dig Dis Sci.2005;50(6):1175-1176.10.1007/s10620-005-2729-zSearch in Google Scholar PubMed
7 Han JH Jeon WJ Chae HB et al. . A case of idiopathic colonic varices: a rare cause of hematochezia misconceived as tumor. World J Gastroenterol.2006;12(16):2629-2632.10.3748/wjg.v12.i16.2629Search in Google Scholar PubMed PubMed Central
8 Detry RJ Kartheuser A Moisse R et al. . Idiopathic non-familial rectal and colonic varices requiring sigmoidorectal resection and coloanal anastomosis [case report]. Eur J Gastroenterol Hepatol.1996;8(10):1023-1026.10.1097/00042737-199610000-00018Search in Google Scholar PubMed
9 Villarreal HA Marts BC Longo WE Ure T Vernava AM Joshi S . Congenital colonic varices in the adult: report of a case. Dis Colon Rectum.1995;38(9):990-992.10.1007/BF02049739Search in Google Scholar PubMed
10 Mehta R Deepak S John A Balakrishnan V . Idiopathic colonic varices. Indian J Gastroenterol.2004;23(1):30-31.Search in Google Scholar
11 Isbister WH Pease CW Delahunt B . Colonic varices: report of a case. Dis Colon Rectum.1989;32(6):524-527.10.1007/BF02554511Search in Google Scholar PubMed
12 Hawkey CJ Amar SS Daintith HA Toghill PJ . Familial varices of the colon occurring without evidence of portal hypertension. Br J Radiol.1985;58(691):677-679.10.1259/0007-1285-58-691-677Search in Google Scholar PubMed
13 Wagner M Kiselow MC Keats WL Jan ML . Varices of the colon. Arch Surg.1970;100(6):718-720.10.1001/archsurg.100.6.718Search in Google Scholar
14 Zaman L Bebb JR Dunlop SP Jobling JC Teahon K . Familial colonic varices—a cause of “polyposis” on barium enema. Br J Radiol.2008;81(961):e17-e19. doi:10.1259/bjr/66055283.10.1259/bjr/66055283Search in Google Scholar
15 Simvoulakis E Viazis N Pipis P Stefanidis G Avgerinos A . Diffuse idiopathic colonic varices presenting with lower gastrointestinal bleeding in an elderly patient: a case report and review of the literature. Acta Gastroenterol Belg.2006;69(1):15-19.Search in Google Scholar
16 Nikolopoulos N Xynos E Datsakis K Kasapidis P Vassilakis JS . Varicosis coli totalis: report of a case of idiopathic aetiology. Digestion. 1990;47(4):232-235.10.1159/000200502Search in Google Scholar
17 Tang SJ Zanati S Dubcenco E et al. . Diagnosis of small-bowel varices by capsule endoscopy. Gastrointest Endosc.2004;60(1):129-135.10.1016/S0016-5107(04)01458-0Search in Google Scholar
18 Vuillemin E Croquet V Coumeau D Ouali L . Idiopathic ileocolonic varices: a rare cause of lower gastrointestinal bleeding [in French]. Gastroentérologie Clinique et Biologique. 2004;28(11):1183-1184.10.1016/S0399-8320(04)95205-0Search in Google Scholar
19 López-Cepero Andrada JM López Silva M Ferr Álamo A Salado Fuentes M Benítez Roldán A . Varices colónicas familiares: presentación de dos casos. Gastroenterología y Hepatología. 2000;23(7):341-343.Search in Google Scholar
20 Place RJ . Idiopathic colonic varices as a cause of lower gastrointestinal bleeding. South Med J.2000;93(11):1112-1114.10.1097/00007611-200011000-00016Search in Google Scholar
21 Van Gossum M Reuss K Moussaoui M Bourgeois V . Idiopathic colonic varices: an unusual cause of massive lower gastrointestinal hemorrhage [case report]. Acta Gastroenterol Belg.2000;63(4):397-399.Search in Google Scholar
22 Bernardini D Barthet M Castellani P Sahel J Gauthier A Botta-Fridlund D . Familial varices of the colon: report of four cases [in French]. Gastroentérologie Clinique et Biologique. 1998;22(10):827-830.Search in Google Scholar
23 Schilling D Maier M Kohler B Würmel W Jakob P Riemann JF . Idiopathic mesenteric varices causing lower gastrointestinal bleeding. Eur J Gastroenterol Hepatol.1996;8(2):177-179.10.1097/00042737-199602000-00016Search in Google Scholar
24 Loffeld RJ van Bochove A de Graaf JC . Colonic varices: an unusual cause of occult blood loss [in Dutch]. Nederlands Tijdschrift voor Geneeskunde. 1996;140(49):2467-2469.Search in Google Scholar
25 Shrestha R Dunkelberg JC Schaefer JW . Idiopathic colonic varices: an unusual cause of massive lower gastrointestinal hemorrhage [case report]. Am J Gastroenterol.1995;90(3):496-497.Search in Google Scholar
26 Vella-Camilleri FC Friedrich R Vento AO . Diffuse colonic varices: an uncommon cause of intestinal bleeding. Am J Gastroenterol.1986;81(6):492-494.Search in Google Scholar
27 Weingart J Höchter W Ottenjann R . Varices of the entire colon—an unusual cause of recurrent intestinal bleeding. Endoscopy. 1982;14(2):69-70.10.1055/s-2007-1021582Search in Google Scholar
28 el-Dosoky MM Reeders JW Dol JA Tytgat GN . Familial intestinal varices without portal hypertension: a case report. Eur J Radiol.1994;18(2):140-141.10.1016/0720-048X(94)90283-6Search in Google Scholar
29 Morini S Caruso F De Angelis P . Familial varices of the small and large bowel. Endoscopy. 1993;25(2):188-190.10.1055/s-2007-1010283Search in Google Scholar PubMed
30 Iredale JP Ridings P McGinn FP Arthur MJ . Familial and idiopathic colonic varices: an unusual cause of lower gastrointestinal haemorrhage [case report]. Gut. 1992;33(9):1285-1288.10.1136/gut.33.9.1285Search in Google Scholar
31 Solis-Herruzo JA . Familial varices of the colon diagnosed by colonscopy. Gastrointest Endosc.1977;24(2):85-86.10.1016/S0016-5107(77)73461-3Search in Google Scholar
32 Bresci G Parisi G Capria A . Clinical relevance of colonic lesions in cirrhotic patients with portal hypertension. Endoscopy. 2006;38(8):830-835.10.1055/s-2006-944629Search in Google Scholar
33 Feldman M Sr Smith VM Warner CG . Varices of the colon: report of three cases. JAMA. 1962;179:729-730.10.1001/jama.1962.03050090057014bSearch in Google Scholar
34 Gudjonsson H Zeiler D Gamelli RL Kaye MD . Colonic varices: report of an unusual case diagnosed by radionuclide scanning, with review of the literature. Gastroenterology. 1986;91(6):1543-1547.10.1016/0016-5085(86)90213-1Search in Google Scholar
35 Hardy M Barbin JY Caroli J . Familial mesenteric hypertension [in French]. Revue Médico-chirurgicale des Maladies du Foie. 1967;42(6):237-246.Search in Google Scholar
36 Atin V Sabas JA Cotano JR Madariaga M Galan D . Familial varices of the colon and small bowel. Int J Colorectal Dis.1993;8(1):4-8.10.1007/BF00341268Search in Google Scholar PubMed
37 Sugiyama S Yashiro K Nagasako K et al. . Extensive varices of ileocecum: report of a case. Dis Colon Rectum.1992;35(11):1089-1091.10.1007/BF02253001Search in Google Scholar PubMed
38 Manzi D Samanta AK . Adhesion-related colonic varices. J Clin Gastroenterol.1985;7(1):71-75.10.1097/00004836-198502000-00012Search in Google Scholar PubMed
© 2014 The American Osteopathic Association
This work is licensed under the Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
Articles in the same Issue
- Abstracts
- 2013 SOMA Abstracts and Poster Competition
- 2013 BIOM Abstracts and Poster Competition
- Editorial
- Our Past, Present, and Future Are in Our Hands
- Letters
- Osteopathic Manual Treatment and Ultrasound Therapy for Chronic Low Back Pain: An Illustration of Osteopathic Semantic Confusion
- Original Contribution
- The Persistence of Lumbar Somatic Dysfunction and Its Association With Bone Mineral Density
- Medical Education
- Patterns of Misrepresentation of Clinical Findings on Patient Notes During the COMLEX-USA Level 2-PE
- Special Communication
- A Degree of Difference: The Origins of Osteopathy and First Use of the “DO” Designation
- A Research Primer, Part 2: Guidelines for Developing a Research Project
- Case Report
- A Case of Seasonal Recurrent Myopericarditis
- A Case of Idiopathic Colonic Varices
- The Somatic Connection
- OMT Relieves Severe Chronic Low Back Pain
- Abdominal Muscles Are the Front Side of the Low Back
- Systematic Review Paints Incomplete Picture of OMT Research
- Manual Therapy or Exercise Effective for Hip or Knee Osteoarthritis
- Review of Severe Adverse Events From Spinal Manipulative Therapy of the Lumbopelvic Area
- A Chiropractic Perspective: Spinal Manipulative Therapy Is Not Causally Related to Stroke
- Clinical Images
- Abducens Palsy
- In Your Words
- No Place Like HOME
Articles in the same Issue
- Abstracts
- 2013 SOMA Abstracts and Poster Competition
- 2013 BIOM Abstracts and Poster Competition
- Editorial
- Our Past, Present, and Future Are in Our Hands
- Letters
- Osteopathic Manual Treatment and Ultrasound Therapy for Chronic Low Back Pain: An Illustration of Osteopathic Semantic Confusion
- Original Contribution
- The Persistence of Lumbar Somatic Dysfunction and Its Association With Bone Mineral Density
- Medical Education
- Patterns of Misrepresentation of Clinical Findings on Patient Notes During the COMLEX-USA Level 2-PE
- Special Communication
- A Degree of Difference: The Origins of Osteopathy and First Use of the “DO” Designation
- A Research Primer, Part 2: Guidelines for Developing a Research Project
- Case Report
- A Case of Seasonal Recurrent Myopericarditis
- A Case of Idiopathic Colonic Varices
- The Somatic Connection
- OMT Relieves Severe Chronic Low Back Pain
- Abdominal Muscles Are the Front Side of the Low Back
- Systematic Review Paints Incomplete Picture of OMT Research
- Manual Therapy or Exercise Effective for Hip or Knee Osteoarthritis
- Review of Severe Adverse Events From Spinal Manipulative Therapy of the Lumbopelvic Area
- A Chiropractic Perspective: Spinal Manipulative Therapy Is Not Causally Related to Stroke
- Clinical Images
- Abducens Palsy
- In Your Words
- No Place Like HOME