Pharmaceutical Technology in Practice: A Personal View
-
Alexander T. Florence
Alexander (Sandy) Florence received his BSc (Pharmacy) in 1962 and his PhD in 1965 from the University of Glasgow. From 1976–1988 he was Professor of Pharmaceutical Technology at the University of Strathclyde and from 1988–2006 Dean of The School of Pharmacy, University of London. His research interests have been in surfactant systems, nanoparticle and dendrimer delivery by the oral and intravenous routes and the underlying complexity of drug targeting. With Vincent H. Lee was founding editor of the
Journal of Drug Targeting and for many years until 2016 was Editor-in-Chief of theInternational Journal of Pharmaceutics . He co-authored with David Attwood “Physicochemical Principles of Pharmacy” now in its 6th edition (2015), and has published “An Introduction to Clinical Pharmaceutics” in 2010.

Abstract
This opinion piece argues that the collective knowledge of drugs and medicines, their nature, formulation and manufacture, their delivery and evaluation is unique to pharmacy and it reasserts the fact that science underpins the clinical use of medicines. It argues this from a personal standpoint of an academic pharmaceutical technologist and recounts examples from the author’s own experience.
My first professorial appointment was as a professor of pharmaceutical technology, so I was heartened to discover this journal devoted to this subject with its focus on hospital pharmacy. This was my reaction partly because I have long argued that pharmacists’ clinical activities are dependant on what I deem to be our unique branch of science. In whatever way one perceives and practices pharmacy our collective knowledge of drugs and medicines, their nature, their formulation and manufacture, their delivery and evaluation is surely unique amongst the health care professions. It is vital to assert this, not least as in some circles, in the United Kingdom for example, the mantra is that the “future is clinical.” It is as if science did not underpin the clinical use of medicines! Some clinical pharmacy journals appear to avoid the word “technology” which is part of the known but false dichotomy in science generally between fundamental and applied research. Pierre Joliot [1] the third generation scientist of the Curie-Joliot family, argues that the harmonious development of research implies a continuum of activities spanning fundamental and technological programs and applications.
The activities of hospital pharmacists are less visible to the public than those of other areas of the profession, so it is vital that the work which is carried out in hospitals by pharmacists is recognised. This is one of the imperatives for practitioners to publish their work, that which has been explored both for its intrinsic interest and to underpin best clinical and pharmaceutical practice. As in all disciplines research that is not published is hidden from view; published work which solves problems or explores potential issues alerts others to these topics. New techniques and findings can be shared to stimulate further study. The scope of pharmaceutical technology, as Professor Lagarce [2] has opined, is indeed broad and it is to be hoped that this will be reflected in the pages of this journal.
The community pharmacy sector in the United Kingdom has lost its ability or willingness to make even the simplest of preparations. [1] The increasing complexity of drug entities (such as monoclonal antibodies and proteins) and formulations such as nanosystems, promising technologies like 3D printing and a raft of others, indicates that the technology underlying our profession must address these new challenges. In this way hospital pharmacy will retain its strengths especially as it can act independent of industry, which for all its positive contributions has been acting recently against patient interests by excessive charging of simple generics. [2]
Hence in an attempt to show the circle of hospital pharmacy technology and its links there is perhaps a place for generics pharmaceutical production (Figure 1).
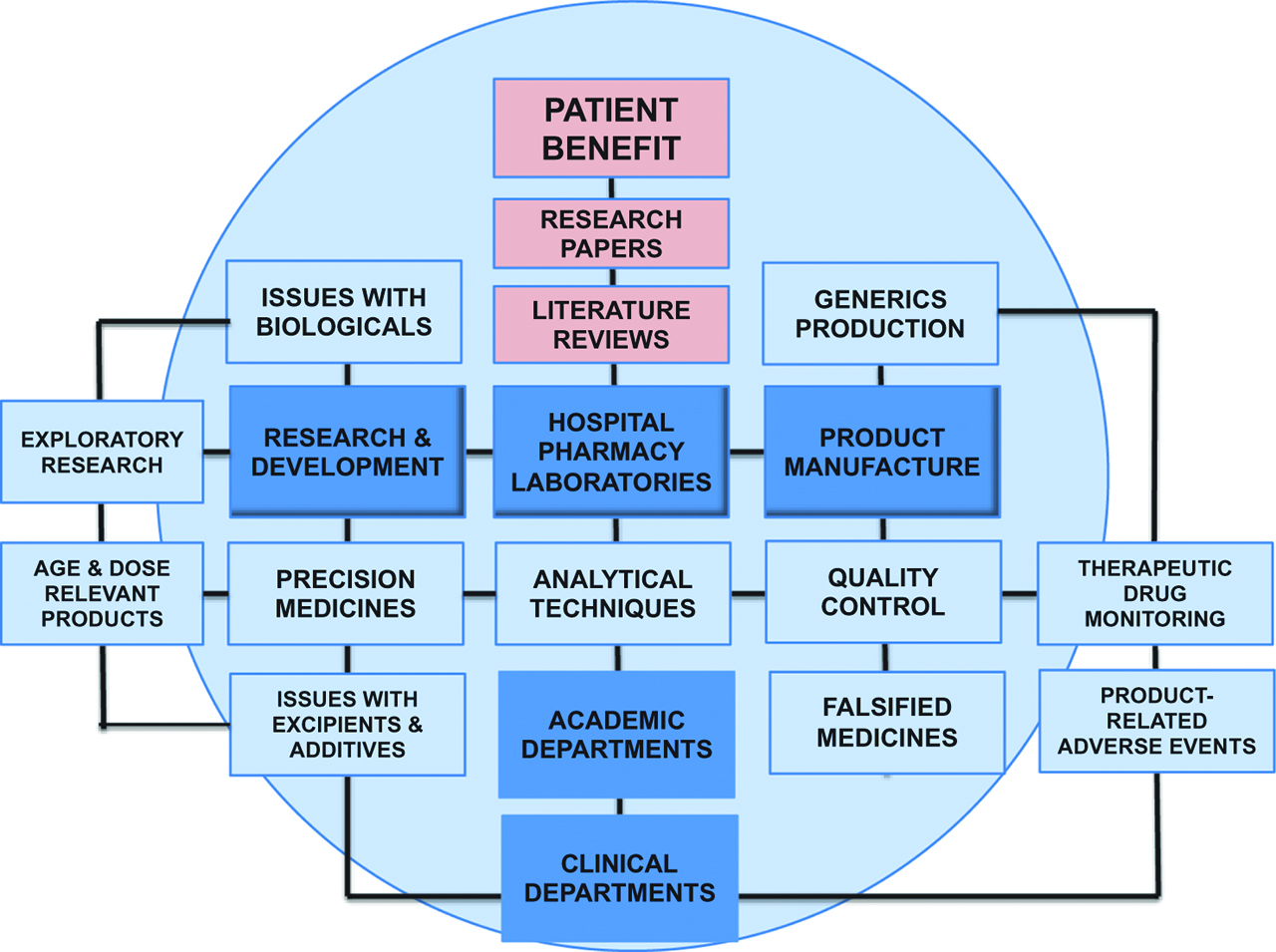
The circle of present and possible activities centered on hospital pharmacy laboratories and associated departments, highlighting the importance of exploratory research, investigating for example excipient properties and potential dose forms for precision medicine and the importance of disseminating investigative work as discussed in the text.
Our capability and knowledge is especially relevant in the promise of personalised medicine, which requires not only in some cases genetic profiling, but having delivery systems able to be tailored for each individual or like group such as children [3]. Indubitably our clinical future is entwined with the technological. In the UK there has been considerable investment in and development of pharmaceutical manufacturing units (PMUs) and many have sophisticated facilities, but I feel that their research and development activities have yet to receive more widespread dissemination.
Reading papers published so far in the journal I have learned of the complexities of topics of which I had only a passing knowledge. This is exactly the purpose of the literature! In these days of overwhelming information in electronic databases, reviews published by experienced pharmacists which may be based on literature research brings together information from a wide variety of sources and makes sense of it. Review articles are often the most cited. I endeavored using past experience to extract the essentials for students and new graduates in the short volume entitled An Introduction to Clinical Pharmaceutics [4] aiming to link aspects of technology with clinical aspirations.
The review in the journal by Flamein et al. [5] details the multiple factors in the administration of IV preparations – from flow behaviour and drug interactions to particulate contamination. These topics are linked to other disciplines and pursuits. In my own case both the nature of flow of particulates in blood and their behaviour in vivo have been an interest for many years in determining the fate of administered nanoparticles for drug delivery. This single example of a paper demonstrates the links between our various disciplines and the need to read outside one’s own field to discover and share new perspectives. Facing up to complex realities is the role of the researcher. The review’s bibliography led me to two papers, one on extravasation [6] and the other on incompatibilities in parenteral nutrition [7]. It is this aspect of publications that assists us all navigating the maze of information available on each topic. Serendipity and chance play their part in research as well as in our careers. A recent paper on inkjet printing was in a physics journal [8]. The physics of cancer and technological and physicochemical approaches to treatment are the areas that Niederhuber and Baker [9] of the US National Cancer Institute have said have too long been thought of as “tangential to the endeavour”. So the clinical pharmacy-technology-science dichotomy is not new. It is vital that some of the invention and expertise in matters of pharmaceutical technology are embedded in our hospitals. Hospitals are surely seen to be the true clinical centres.
Collaboration between academic pharmacy groups and hospital units can, in my own experience stimulate both. While my interests have been mainly in the field of surfactants and nanosystems it has been difficult to resist what might be thought of as tangential interests. The following examples are, by their nature, personal “historical” accounts which by necessity are UK-biased. Two colleagues (Allan Baillie and Anne Mendelow) and I in Strathclyde had contact with a dermatologist in a local hospital and we became interested in contact dermatitis and its evaluation by patch testing. We were first surprised to find an absence of quality control of the skin test formulations prepared in the hospital, and this led to a short paper on the influence of formulation optimisation. Reactions to test patch application were routinely estimated visually (e.g. +++/++/+/-). Technological approaches were applied to achieve greater quantitative data, using both skin-reflectance techniques [10] and infra-red thermography [11]. A typical result is shown in Figure 2.
![Figure 2: A thermographic image after application of four patches to the back of a patient. The quantitative colour image chart is not shown here. (For details see reference [11]).](/document/doi/10.1515/pthp-2018-0013/asset/graphic/j_pthp-2018-0013_fig_002.jpg)
A thermographic image after application of four patches to the back of a patient. The quantitative colour image chart is not shown here. (For details see reference [11]).
For many years my “education” continued not only through my postgraduate students and postdoctoral fellows or in the library, but at the table of the UK Committee on Safety of Medicines and its Sub-Committee on Chemistry Pharmacy and Standards (CPS). Overall a fascinating time that led me to examine back in our laboratory some of the issues that arose. One of the first (circa 1973) at the very start of my regulatory apprenticeship was a technological matter concerning digoxin tablets. A milling problem at Wellcome Laboratories resulted in a long period during which Lanoxin® digoxin tablets contained larger drug particles: their bioavailability was thus compromised. Patients stabilised on doses of these had serious toxicity problems following on the reintroduction of the normal milling process. Our study of a range of the UK and other National Standard digoxin samples, showed that even these varied widely in their dissolution rates because of their different particle characteristics. This so-called “digoxin affair” led to the first dissolution tests introduced in the British Pharmacopoeia.
In 1983–4 the much vaunted and indeed ingenious osmotic pump formulation of sodium indomethacin (Osmosin®) caused in some patients not only pain but perforation of the gastro-intestinal tract. The single exit for the release of drug resulted in localised high concentrations of drug and the osmotic salt. The tablets had an adhesive tendency and this led us to measure this aspect of a large range of coated tablets to (porcine) oesophageal tissue using a simple apparatus. A second case was with emepronium bromide used for nocturnal enuresis was different: it caused oesophageal ulceration. The drug molecule has surfactant properties which would have been a contributing factor. We found that the coated tablets literally exploded releasing the core of pure drug as seen in Figure 3 (a,b) along with results on a range of tablets. Such simple experiments should not be dismissed: they might nowadays be used to quickly identify counterfeit products with similar appearance but different surface and bulk properties.
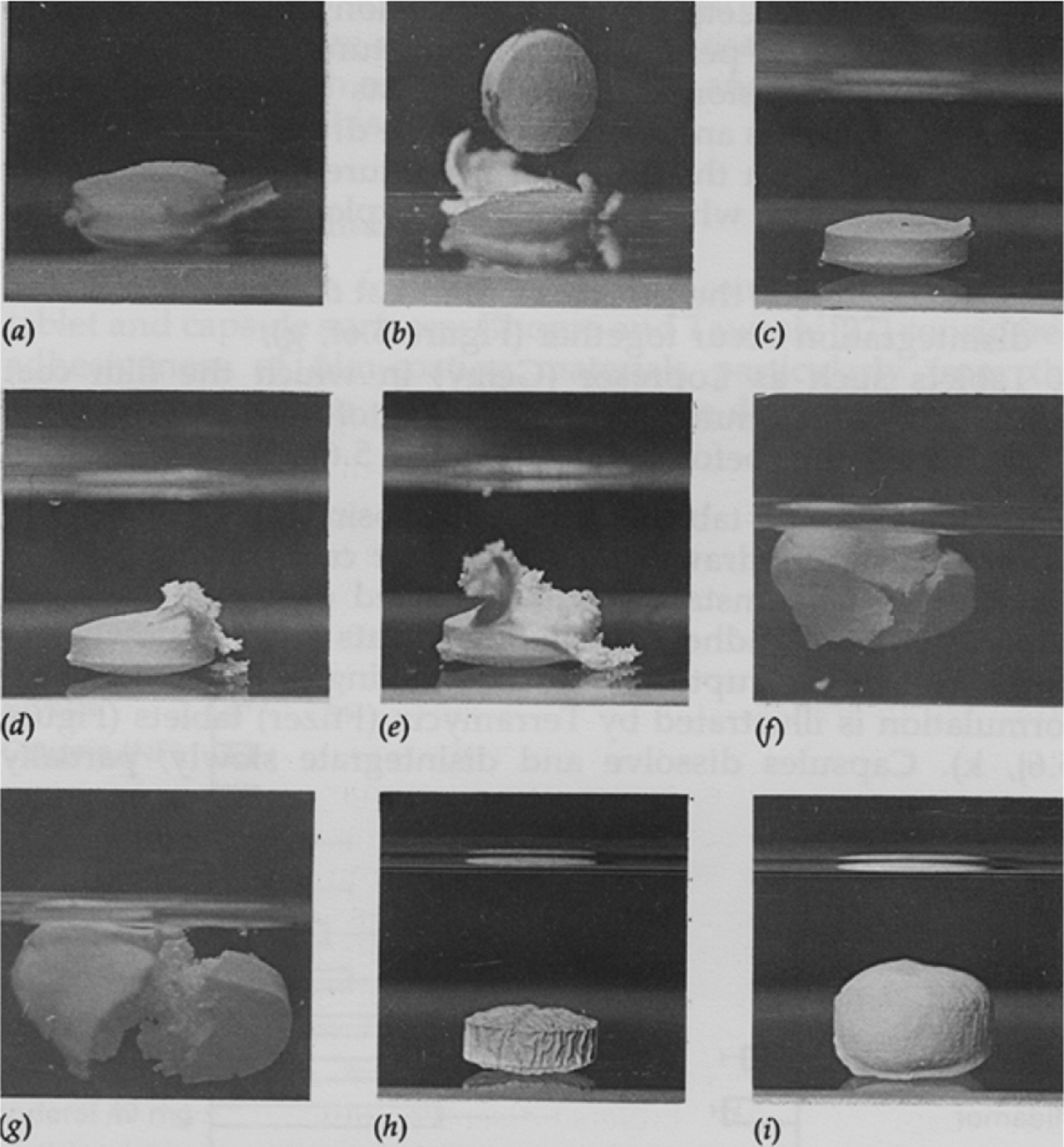
Photographic records of various disintegration patterns of oral tablets in vitro(a,b): the Cetiprin formulation illustrating the emepromium drug core being expelled. (c,d,e) shows gradual rupture of a film coat and release of contents; (f,g) simultaneous coat rupture and disintegration (h,i): swelling of a tablet without rupture. From A. T. Florence and E. G. Salole, Formulation Factors in Adverse Reactions. Wright: London, 1990. (pp 96–102).
How do we ensure more effectively that pharmacy graduates see and recognise in this complex mix of drugs, medicines, systems that function optimally and sub-optimally, the multitude of issues of modern formulations, biosimilars, monoclonal antibodies, interactions, “targeting” nanotechnologies, the toxicity and bioactivity of some excipients, such as the multiple actions of surfactants? Would they readily see the connections between the fact that Suggamadex terminates the pharmacological action of rocuronium [12] and that 2-hydroxypropyl-β-cyclodextrin is valuable in Niemann-Pick disease [13]. Would the use of simple capsules of insulin crystals used in a clinical trial reported recently in a study of the oral absorption of insulin [14] seem to them to be somehow odd, as I thought it was. We know that the cyclodextrin Suggamadex by enveloping the neuromuscular blocking agent ends its action at the close of a procedure. It has also has been found to reduce the incidence of anaphylactic reactions to the anaesthetic. We know that 2-hydropropryl-β-cyclodextrin binds cholesterol and thus reduces the abnormal cholesterol levels in the disease in question. Both are examples of excipients as actives, a field full of promise.
The value of research is not measured by its cost. Literature research itself can unravel many mysteries of drug treatment. It alerts us to analogies and links to our basic knowledge. It assists us all in teaching the next generation of practitioners. The educational role of hospital pharmacists will be strengthened by research and publication and being at the interface of technology and clinical practice. We complete the circle when this combines to optimise patient care. No one can seriously doubt that the pharmaceutical and analytical technologies at our disposal are fundamental enablers of clinical excellence and progress. I trust that Pharmaceutical Technology in Hospital Pharmacy will be an important vehicle to realise this ambition.
About the author

Alexander (Sandy) Florence received his BSc (Pharmacy) in 1962 and his PhD in 1965 from the University of Glasgow. From 1976–1988 he was Professor of Pharmaceutical Technology at the University of Strathclyde and from 1988–2006 Dean of The School of Pharmacy, University of London. His research interests have been in surfactant systems, nanoparticle and dendrimer delivery by the oral and intravenous routes and the underlying complexity of drug targeting. With Vincent H. Lee was founding editor of the Journal of Drug Targeting and for many years until 2016 was Editor-in-Chief of the International Journal of Pharmaceutics. He co-authored with David Attwood “Physicochemical Principles of Pharmacy” now in its 6th edition (2015), and has published “An Introduction to Clinical Pharmaceutics” in 2010.
Acknowledgements
I must thank the all research students, postdoctoral researchers and colleagues who over 50 years have contributed to my appreciation of the science of pharmacy, and I thank Professor Lagarce for having invited me to write this piece for the journal.
References
1. Joliot P. “La Recherche Passionnément”. Paris: Éditions Odile Jacob; 2001.Search in Google Scholar
2. Lagarce F. The field of pharmaceutical technology in hospitals is broad. Pharm Tech Hosp Pharm 2016;1:55–56.10.1515/pthp-2016-0014Search in Google Scholar
3. Florence AT, Lee VHL. Personalised medicines: more tailored drugs, more tailored delivery. Int J Pharm 2011;415:29–33.10.1016/j.ijpharm.2011.04.047Search in Google Scholar
4. Florence AT. “An Introduction to Clinical Pharmaceutics”. London: Pharmaceutical Press; 2010.Search in Google Scholar
5. Flamein, F., Storme, L., Maiguy-Foinard, A, Perez, M, Decaudin, B, Masse, M, et al. Avoid drug incompatibilities: clinical context in neonatal intensive care units (NICU). Pharm Tech Hosp Pharm 2017;2:71–78.10.1515/pthp-2017-0009Search in Google Scholar
6. Devaud, J-C., Sigrist, T., Zaug, C., Guignard B, et al. Proposition d’une marche à suivre pour la gestion et la prevention d’extravasation d’agents non-cytotoxiques. Pharmactuel 2012;45:132–36.Search in Google Scholar
7. Fonzo-Christe C, Bouchoud L, Pfister R. Incompatibilités médiamenteuses et nutrition parentérale en néonatologie. Nutr Clin Métab 2017:31:24–27.10.1016/j.nupar.2016.10.001Search in Google Scholar
8. Martin GD, Hoath SD, Hutchings IF. Inkjet printing – the physics of manipulating liquid jets and drops. J Phys Conf Ser 2008;105:012001.10.1088/1742-6596/105/1/012001Search in Google Scholar
9. Niederhuber JE, Barker AD. Integrity and leveraging the physical sciences to open a new frontier in oncology. 2008. See physics.cancer.gov/report/psl.aspxSearch in Google Scholar
10. Mendelow AY, Forsyth A, Feather JW, Baillie AJ, Florence AT. Skin reflectance measurements of patch responses. Contact Dermatitis 1986;15:73–78.10.1111/j.1600-0536.1986.tb01280.xSearch in Google Scholar
11. Baillie AJ, Biagioni PA, Forsyth A, Garioch JJ, McPherson D. Thermographic assessment of patch test responses. Br J Dermatol 1990;122:351–60.10.1111/j.1365-2133.1990.tb08283.xSearch in Google Scholar
12. Gijsenbergh F, Ramael S, Houwing N, Van Iersel T. First human exposure of Org 25969, a novel agent to reverse the action of rocuronium bromide. Anesthesiology 2005;103:695–703.10.1097/00000542-200510000-00007Search in Google Scholar
13. Ory. D.S., Ottinger, E.A., Farhat, N.Y., King, K.A., Jiang, X, Weissfeld, L, et al. Intrathecal 2-hydroxy-β-cyclodextrin decreases neurological disease progression in Niemann-Pick disease, type C1. Lancet 2017;390:1758–68.10.1016/S0140-6736(17)31465-4Search in Google Scholar
14. Krishner JP, Schatz DA, Bundy B, Skyler JS, Greenbaum CJ. Effect or oral insulin on prevention of diabetes in relatives of patients with Type 1 diabetes. J Amer Med Assoc 2017;318:1891–1902.10.1001/jama.2017.17070Search in Google Scholar PubMed PubMed Central
© 2018 Walter de Gruyter GmbH, Berlin/Boston
Articles in the same Issue
- Frontmatter
- Editorial
- After Ten Issues Our Journal Has Found Its Audience and Main Topics
- Research Articles
- HPLC – Quality by Design Approach for Simultaneous Detection of Torsemide, Spironolactone and Their Degradant Impurities
- Physico-Chemical Stability of Sodium Thiosulfate Infusion Solutions in Polyolefin Bags at Room Temperature over a Period of 24 Hours
- Long-Term Stability Comparison between an Original and a Generic Version of Piperacillin/Tazobactam in Dextrose 5 % Infusion Polyolefin Bags at 5 ± 3 °C after Microwave Freeze-Thaw Treatment
- Environmental and Product Contamination during the Preparation of Antineoplastic Drugs with Robotic Systems
- Qualification and Performance Evaluation of an Automated System for Compounding Injectable Cytotoxic Drugs
- Short Communication
- Feedback on the Centralization of Intrathecal Analgesic Preparations in Hospital Pharmacy
- Opinion Paper
- Pharmaceutical Technology in Practice: A Personal View
Articles in the same Issue
- Frontmatter
- Editorial
- After Ten Issues Our Journal Has Found Its Audience and Main Topics
- Research Articles
- HPLC – Quality by Design Approach for Simultaneous Detection of Torsemide, Spironolactone and Their Degradant Impurities
- Physico-Chemical Stability of Sodium Thiosulfate Infusion Solutions in Polyolefin Bags at Room Temperature over a Period of 24 Hours
- Long-Term Stability Comparison between an Original and a Generic Version of Piperacillin/Tazobactam in Dextrose 5 % Infusion Polyolefin Bags at 5 ± 3 °C after Microwave Freeze-Thaw Treatment
- Environmental and Product Contamination during the Preparation of Antineoplastic Drugs with Robotic Systems
- Qualification and Performance Evaluation of an Automated System for Compounding Injectable Cytotoxic Drugs
- Short Communication
- Feedback on the Centralization of Intrathecal Analgesic Preparations in Hospital Pharmacy
- Opinion Paper
- Pharmaceutical Technology in Practice: A Personal View