Rubber Coring of Injectable Medication Vial Stoppers: An Evaluation of Causal Factors
-
Philip Chennell
Philip Chennell is in charge of the Control and Development laboratory unit of the pharmacy department of Clermont-Ferrand’s University Hospital. He obtained his master’s degree in 2012, his PharmD in 2013, and is also currently a PhD candidate. He assumed teaching duties in 2014 at the University d’Auvergne, and is now member of the research team UMR CNRS 6296 “Materials for Health” at Clermont Auvergne University. His current professional interests focus on pharmaceutical preparations, medical devices and content-container interactions.
 ,
Daniel Bourdeaux
,
Daniel Bourdeaux
Daniel Bourdeaux is a pharmacist at the Control and Development laboratory unit of the pharmacy department of Clermont-Ferrand’s University Hospital since 2006 and has teached Clinical Pharmacy at the University d’Auvergne since 2006. He obtained his master’s degree in 2005 and his phD in 2012. Daniel Bourdeaux has been a member of C-BIOSENSS (Characterization and Biological SEcurity of Nano-Structured Surfaces, EA4676) since 2010.
Quentin Citerne studied pharmacy in Clermont-Ferrand from 2009 to 2014. He started his hospital pharmacy internship in November 2014 in Reims, and is currently completing his second year at the University Hospital of Nancy, France.
Catherine Arnaud has been working as a nurse at Clermont-Ferrand’s University Hospital since 1992, and obtained her Health Manager degree in 2002, and has been working in a reanimation ward for the last 14 years. Her daily interests are about healthcare organization and patient care, including the good use of medical devices and clinical problems linked to their use.
Sylvie Cosserant is a nurse with a master’s degree in Management of Health Organizations, and is a Senior Health Manager for several reanimation and anesthetic wards in Clermont-Ferrand’s University Hospital. Her objectives are to develop transversal cooperation between the different clinical wards and to promote paramedical research.
Véra Boiko Alaux obtained her PharmD in 1983, and began to specialize in medical devices in 1992. She is currently in charge of the medical devices unit of the pharmacy department of Clermont-Ferrand’s University Hospital, and is a member of Europharmat’s technical committee. Her main interests are about medical devices’ good use and content-container interactions.
Prof Valerie Sautou is a hospital pharmacist, head of pharmacy department of Clermont-Ferrand’s University Hospital. She is a professor of clinical pharmacy and biotechnology at Clermont Auvergne University. Her research activity is focused on medical devices and content-container interactions. Her research team unit is the UMR CNRS 6296 “Materials for Health”.

Abstract
Purpose:
Coring of a medication vial’s rubber stopper has been reported as a major cause of visible particle presence in injectable preparations. In this study, we investigated and quantified visible particle formation caused by coring associated with four potential causal factors.
Methods:
The factors studied were: nature of the rubber stopper; rubber stopper thickness, type of metal needle bevel used to pierce the stopper, and puncture technique. For each one of 16 different situations, 40 medication vial rubber stoppers were punctured, and the contents filtered. The filters were then examined under optical microscopy and particles present counted and measured.
Results:
The incidence of particle formation ranged from 0 % to 75 %, depending on the situation. Particle length was on average of 0.98±0.39 mm. The situation that gave the most particles (75 %; 30/40) was obtained when using a short bevelled needle, a 4 mm thick chlorobutyl vial stopper and with a puncture angle of 90°. Whilst a puncture technique reduced particle formation by more than 50 % for the most at risk situation, but without eliminating particle formation (residual formation of 22.5 %; 11/40), the use of a blunt bevelled needle totally eliminated the incidence of visible particle creation. The thickness of the rubber and the nature of the elastomer seemed to be linked to coring incidence, but in lesser proportions.
Conclusion:
Puncturing the stoppers using a technique with a 45° puncture angle reduced particle formation, but only the use of a blunt metal needle totally eliminated it.
Introduction
Rubber stoppers allow easy access to drugs contained in glass medication vials, as they can be readily punctured through with a needle or a cannula. In hospitals in general and in intensive care units in particular, the great use of injectable drugs packaged in glass vials with rubber stoppers means that such a practice is very common. For example, in the intensive care units of our hospital, approximately 99,000 rubber stoppers of various medication vials were punctured in 2015. The presence of visible particles of various sizes in medication drug vials, caused by the coring of the vial’s rubber stopper by injection or preparation medical devices, has been regularly reported in scientific literature. Isolated cases have been described [1–4], as well as several studies on particle incidence in used medication vials [5–8]. The incidence of rubber stopper coring, assessed by the presence of visible particles, has been evaluated as ranging overall from 0 to 40 %, depending on the studies and the medical devices used for the piercing of the rubber stopper.
Clinical risks induced by intravenous administration of visible particulate matter are still incompletely characterised or documented, yet macroscopic particles have been incriminated as being able to cause phlebitis and venous inflammatory reactions [9], reduce tissue capillary perfusion [10], induce the formation of pulmonary embolisms, injection site reactions and granuloma [11], and have even been implicated in a deadly small bowel infarction [12].
The administration safety of injectable drugs is ensured notably by the absence of visible particles in the injected preparation. Regulatory texts worldwide concerning visible particle indicate that parenteral preparations are essentially free from visible particulates [13], clear and practically free from particles [14], or clear and free from readily detectable foreign insoluble matters [15]. However, direct intravenous injections, such as with propofol, remain at risk, as the medication withdrawn from the vial is directly administered to the patient.
Unfortunately, the studies mentioned previously are often lacking in detailed description of medications or medical devices implicated (for example by only referring to generic drug names of the medication vials, without mentioning the drug manufacturer, or without mentioning exact references and manufacturers of the medical devices used), which makes comparisons and possible cause-analysis difficult. Several hypothesises have nevertheless been considered, such as the nature or quality of the rubber constituting the stopper, the type and characteristics of the medical device used for puncturing [8, 16], or the puncturing method used by the nurse or physician [17, 18]. However, no study investigating the relative importance of those factors has been identified in the current literature, and the exact causes of particle creation through coring remain uncertain.
The primary aim of this study was to determine which combination of factors posed the least and the most likelihood of coring and particulate matter creation. Secondary aims were to determine particulate frequency and size, and whether elastomer quality influenced coring frequency or particle size.
Materials and methods
Materials
In order to test two different types of rubber (made from bromobutyl or chlorobutyl elastomer), with two different thicknesses (measured at the centre of the stopper), and two different needle bevels, the following commercially available products were purchased.
Medication vials with stoppers (marketed as single dose vials)
2 mm thick chlorobutyl vial stoppers from Amoxicillin 1 g vials (Panpharma, Fougeres, France), batch 301907, expiry date 01/2017
2 mm thick bromobutyl vial stoppers from Amoxicillin/Clavulanic acid 1 g/200 mg vials (Sandoz, Levallois Perret Cedex, France), batch DW9334, expiry date 12/2015
4 mm thick chlorobutyl vial stoppers from Lidocaine 200 mg/20 mL vials (Aguettant, Lyon Cedex 07, France), batch T-7688C, expiry date 02/2017
4 mm thick bromobutyl vial stoppers from Propofol 500 mg/50 mL vials (Fresenius Kabi France, Louviers, France), batch 16HC0243, expiry date 02/2017
Needles
18 gauge, short bevelled metal hypodermic needles (reference 304622 BD Microlance™, Becton Dickinson France, Le Pont de Claix, France)
18 gauge, blunt bevelled metal hypodermic needles (reference 305180 BD™, Becton Dickinson France, Le Pont de Claix, France)
Other
Sodium chloride 0.9 % saline solution (pourable bottle, Fresenius Kabi France, Louviers, France)
0.45 µm pore size black gridded filter (reference HABG047S6, Merck Millipore, Molsheim, France)
Methods
Study design
In this laboratory study, four different potentially causative factors of 2 levels each were studied together, for a total of 16 (24) different combinations, as presented in the experimental setup (Table 1).
Experimental setup for the study of four different risk factors.
| Causal factors tested | |||||
|---|---|---|---|---|---|
| Needle bevel | Vial stopper thickness (mm) | Vial stopper constitution | Puncture angle | ||
| SITUATIONS | N°1 | Short | 2 | Bromobutyl | 90° |
| N°2 | Short | 4 | Bromobutyl | 90° | |
| N°3 | Short | 2 | Chlorobutyl | 90° | |
| N°4 | Short | 4 | Chlorobutyl | 90° | |
| N°5 | Blunt | 2 | Bromobutyl | 90° | |
| N°6 | Blunt | 4 | Bromobutyl | 90° | |
| N°7 | Blunt | 2 | Chlorobutyl | 90° | |
| N°8 | Blunt | 4 | Chlorobutyl | 90° | |
| N°9 | Short | 2 | Bromobutyl | 45° | |
| N°10 | Short | 4 | Bromobutyl | 45° | |
| N°11 | Short | 2 | Chlorobutyl | 45° | |
| N°12 | Short | 4 | Chlorobutyl | 45° | |
| N°13 | Blunt | 2 | Bromobutyl | 45° | |
| N°14 | Blunt | 4 | Bromobutyl | 45° | |
| N°15 | Blunt | 2 | Chlorobutyl | 45° | |
| N°16 | Blunt | 4 | Chlorobutyl | 45° | |
For each one of the 16 situations, the following protocol was applied by one investigator, who performed solely the manipulations to ensure reproducibility, with n=40 vials per situation: each vial’s stopper was punctured once with a new needle in accordance with the experimental setup, and 3 to 5 mL of saline solution injected into the vial.
The factors analysed were the following:
Needle bevel: standard short bevelled hypodermic needle, customarily used for vial stopper penetration, were compared to blunt needle, marketed as having low coring properties.
A classic puncture technique (needle at 90° to the stopper surface) was compared to an adapted puncture technique (initial puncture angle of 45°, with the needle being straightened up to 90° during insertion into the vial)
Vial stopper elastomer: two rubbers commonly used as constitutive materials of vial stoppers were compared: chlorobutyl versus bromobutyl
Vial stopper thickness: thin 2 mm stoppers were compared with 4 mm thick stoppers
Analyses
Visible particle characterization
The contents of each vial was then emptied (after having manually removed the stopper) and filtered under vacuum through a 0.45 µm filter (10 vials of the same situation per filter, and 4 filters per situation, for a total of 40 vials per situation). The filters were rinsed with a saline solution and were then observed under optical microscopy equipped with a camera and linked to a computer with software allowing images to be taken and the measurement of particles present. Particles present on each filter were counted, photographed and measured.
Infrared spectrophotometric analysis of rubber vials
In order to assess whether the chlorobutyl or bromobutyl samples didn’t present any fundamental chemical differences (between chlorobutyl sample or between bromobutyl samples), one sample of each type of tested vial stopper was submitted to an infrared spectrophotometric analysis using an an Avatar 320 Fourier transform infrared spectrometer (Thermo electron, USA) fitted with a DTGS KBr detector. We used a flat ATR multi-reflection ZnSe crystal to perform the analysis. A thickness of 1 mm lamella was cut with a scalpel in the sample in order to be pressed over the ZnSE crystal. The spectra were then recorded with a resolution of 4, i. e. a digital increment of 1.929 cm−1, and scan number set at 32. The results were processed using Omnic 6.2 software (Thermo electron, USA).
Statistical considerations
For situations where particle formation was observed (categorical dichotomous variables), particle formation percentages were compared using a Pearson’s chi-squared test, or a Fisher’s exact test when applicable. Particle size (length and width) was compared inter-situation using an analysis of variance (ANOVA) test.
Differences were considered statistically significant for a p-value≤0.05.
Results
Particle formation
Results of the initial particle formation assessment are presented in Table 2.
Visible particle formation quantification for the initial assessment, for each analysed situation.
| Causal factors tested | Results | |||||||
|---|---|---|---|---|---|---|---|---|
| Needle bevel | Vial stopper thickness (mm) | Vial stopper constitution | Puncture angle | Particles per 40 vials | Particle formation (%) | 95 % confidence interval (%) | ||
| SITUATIONS | N°1 | Short | 2 | Bromobutyl | 90° | 3 | 7.5 | 0.0–15.7 |
| N°2 | Short | 4 | Bromobutyl | 90° | 2 | 5.0 | 0.0–11.8 | |
| N°3 | Short | 2 | Chlorobutyl | 90° | 0 | 0.0 | 0.0–0.0 | |
| N°4 | Short | 4 | Chlorobutyl | 90° | 30 | 75.0 | 61.6–88.4 | |
| N°5 | Blunt | 2 | Bromobutyl | 90° | 0 | 0.0 | 0.0–0.0 | |
| N°6 | Blunt | 4 | Bromobutyl | 90° | 0 | 0.0 | 0.0–0.0 | |
| N°7 | Blunt | 2 | Chlorobutyl | 90° | 0 | 0.0 | 0.0–0.0 | |
| N°8 | Blunt | 4 | Chlorobutyl | 90° | 0 | 0.0 | 0.0–0.0 | |
| N°9 | Short | 2 | Bromobutyl | 45° | 0 | 0.0 | 0.0–0.0 | |
| N°10 | Short | 4 | Bromobutyl | 45° | 0 | 0.0 | 0.0–0.0 | |
| N°11 | Short | 2 | Chlorobutyl | 45° | 0 | 0.0 | 0.0–0.0 | |
| N°12 | Short | 4 | Chlorobutyl | 45° | 11 | 22.5 | 9.6–35.4 | |
| N°13 | Blunt | 2 | Bromobutyl | 45° | 0 | 0.0 | 0.0–0.0 | |
| N°14 | Blunt | 4 | Bromobutyl | 45° | 0 | 0.0 | 0.0–0.0 | |
| N°15 | Blunt | 2 | Chlorobutyl | 45° | 0 | 0.0 | 0.0–0.0 | |
| N°16 | Blunt | 4 | Chlorobutyl | 45° | 0 | 0.0 | 0.0–0.0 | |
Four situations out of 16 induced particle formation, each one associated with the use of a short bevelled needle (situations N°1, N°2, N°4 and N°12). The situation that gave the most particles (75 %; 30/40) was situation N°4 (short bevelled needle, 4 mm thick chlorobutyl vial stopper, 90° puncture angle).
No particle formation was observed when using a blunt bevelled needle. Indeed, the use of a blunt bevelled needle reduced particle formation to undetectable levels (situations N°5, N°6, N°8 and N°16).
When using a short bevelled needle with a bromobutyl stopper, a puncture angle of 45° reduced particle formation percentages from low (situations N°1 and N°2, 7.5 % and 5 % particle formation with a 90° puncture angle) to undetectable levels (situations N°9 and N°10). However, despite a three-fold reduction in particle formation, changing the puncture angle to 45 °C did not fully prevent particle formation when the initial particle formation level was high (situation N°4 (75 %; 30/40) versus situation N°12 (22.5 %; 11/40) (p<10−4).
When using a short bevelled needle and a puncture angle of 90°, bromobutyl vial stoppers of 2 mm and 4 mm thickness gave similar (statistically non-significant) low particle formation percentages, of respectively 7.5 % (3/40) and 5 % (2/40), for situations N° 1 and N°2. However, in the same conditions, but with chlorobutyl vial stoppers of 2 mm and 4 mm, particle formation went from undetectable (0/40, situation N°3), to 75 %; 30/40 (situation 4).
Overall vial stoppers made from chlorobutyl accounted for 41 particles (situations N°4 and N°12, and bromobutyl only 5 (situations N°1 and N°2).
Particle dimensions
Particles dimensions data is summarized in Table 3, and their distribution is presented in Figure 1.
Observed particle dimensions.
| Particle generating risk situation | Number of particles | Length (mm) | Width (mm) | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Min | Max | Median | Mean | Standard deviation | Min | Max | Median | Mean | Standard deviation | ||
| 2 mm bromobutyl stopper, short bevelled needle, 90° puncture angle | 3 | 0.85 | 0.89 | 0.85 | 0.86 | 0.02 | 0.43 | 0.69 | 0.47 | 0.53 | 0.14 |
| 4 mm bromobutyl stopper, short bevelled needle, 90° puncture angle | 2 | 0.92 | 0.92 | 0.92 | 0.92 | 0.00 | 0.57 | 0.83 | 0.70 | 0.70 | 0.18 |
| 4 mm chlorobutyl stopper, short bevelled needle, 90° puncture angle | 30 | 0.59 | 2.82 | 0.85 | 0.99 | 0.49 | 0.48 | 1.01 | 0.72 | 0.73 | 0.13 |
| 4 mm chlorobutyl stopper, short bevelled needle, 45° puncture angle | 11 | 0.85 | 1.20 | 0.99 | 1.01 | 0.10 | 0.72 | 0.99 | 0.81 | 0.81 | 0.09 |
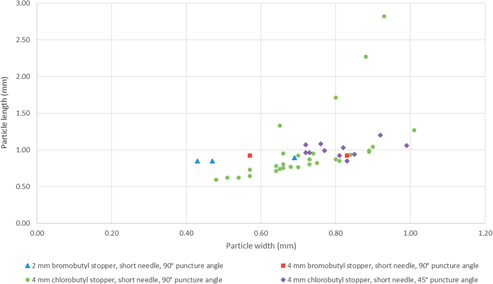
Observed particle dimension distribution.
The observed particle length was not found to be statistically different between the various situations (p=0.94), with an average length of 0.98±0.39 mm (mean±standard deviation). Overall particle width shows statistically significant differences between situations (p=0.015), with particle width being significantly different between particles from situation N°1 (2 mm bromobutyl stopper, blunt bevelled needle, 90° puncture angle) and situations N°4 and 12 (4 mm chlorobutyl stopper, blunt bevelled needle, 90° puncture angle) (p=0.019 and p=0.001, respectively).
Most particles have dimensions inferior to 1 mm, but particles with lengths superior to 1 mm were observed only in situations implicating 4 mm chlorobutyl stoppers. Particle shapes are mostly homogenous and roundish, and look like “cores”, but some other shapes have been noted (Figure 2).
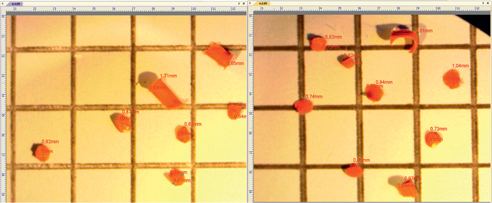
16 particles observed from situation N°4 (short needle bevel, puncture angle of 90°, through a 4 mm chlorobutyl vial stopper), observed through optical microscopy, magnification times 40.
Infrared spectrophotometric analysis
Obtained infrared spectra are presented Figure 3 (bromobutyl stoppers) and Figure 4 (chlorobutyl stoppers).
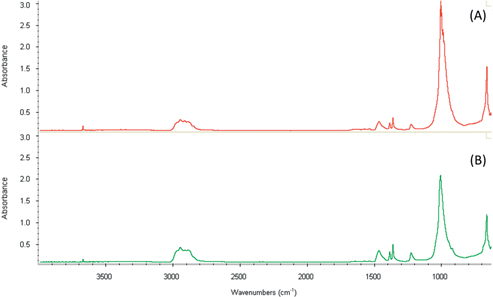
Infrared spectra of the used bromobutyl vial stoppers, (A) from the 2 mm bromobutyl vial stopper and (B) from the 4 mm bromobutyl vial stopper.
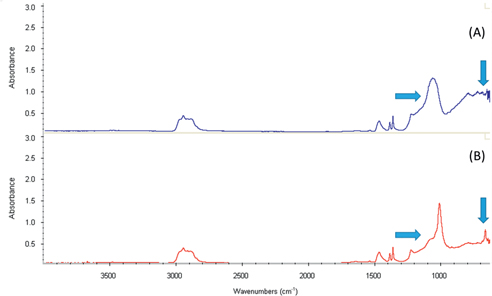
Infrared spectra of the used chlorobutyl vial stoppers, (A) from a 4 mm chlorobutyl vial stopper and (B) from a 2 mm chlorobutyl vial stopper. The arrows indicate differences between (A) and (B).
Infrared spectra show significant differences between chlorobutyl and bromobutyl samples, for wavelengths between 1,200–1,100 cm−1 and around 900–700 cm−1.
Bromobutyl samples present identical spectra, however the chlorobutyl samples’ spectra differ between themselves for wavelengths between 1,100 and 1,000 cm−1 and at 700 cm−1, indicating a clear chemical difference between samples.
Discussion
In our study, we have shown that visible particle formation can be an alarmingly common phenomenon, as visible particle formation was observed in four analysed situations out of 16 using commercially available medication vials, with particle incidence ranging from 0 % to 75 %, depending on the type and thickness of the elastomer, the type of needle, and the needle insertion angle.
Out of the four causal factor studied, the type of needle seems to be of primordial importance, as all of the present particles were detected after use of a standard short bevelled metal needle, and the use of a blunt metal needle totally eliminated particle formation, for all tested situations. Recent data published by Wani et al. also reported the profound impact of the type of medical preparation or administration device used [8]. They compared particle formation after the stopper had been punctured using two different preparation devices, an 18 gauge sharp hypodermic needle and a blunt plastic safety needle, and found an overall frequency of coring incidence of 40.8 % when using blunt plastic safety needles and of 4.2 % when using sharp metal needles. The comparison between their study and our data indicates that the blunt property does not seem in itself sufficient to guaranty minimal coring risks, as two different blunt devices gave opposite coring results. Such a difference could be explained by other intrinsic properties like for example the type of material and quality of the manufacturing (sharpness of the edges, thickness of the needle wall). Data published in 2015 by Eskander et al. [19], who studied the incidence of coring with 3 different access devices, including a blunt plastic safety needle and a metal 18 gauge sharp bevelled needle seems to confirm such a hypothesis. In their trial, the use of a blunt plastic canula cored up to 22 % of propofol medication vial stoppers, whilst the use of the blunt bevelled metal needle reduced the coring incidence ten-fold, without however totally eliminating it.
Also, both Wani et al. and Eskander et al. found that coring rates differed greatly between medications vials, indicating that the quality of the stoppers is probably uneven and manufacturer dependant. However, as batches, brand names and medication manufacturers were not disclosed, no conclusions can be made concerning the type of quality of the rubber vial stopper. In the same way, there is no indication about the puncture method used.
The needle insertion angle also seems to have an important impact on particle incidence, as a 45° initial puncture angle reduced particle formation to un-detectability if the initial particle formation was of less than 7.5 %, and reduced it by more than 50 % when the initial particle formation was of 75 %. The puncture angle is therefore an important factor to help reduce particle formation risk, but in practice it will not be enough to totally eliminate it. In 2001, Shiroyama reported an 18 % incidence rate of coring by 18 gauge injection needles during the use of 100 propofol vials [7], and subsequently proposed what was described as being an advanced puncture technique to reduce coring incidence, by inclining the puncture angle to 45° [18]. Such a technique was also reported by Roth et al. as reducing the risk of coring [17]. In 2013, Campagna et al. studied the occurrence of rubber coring of prednisone acetate vial stoppers. Despite using a needle insertion angle of 45° to 60°, they found an incidence of 10.5 % when using a metal 18 gauge sharp bevelled needle [6], thus confirming our data that a 45° needle insertion angle does help reduce coring incidence but without totally eliminating it. Also, the more elaborate a puncture method, the less likely it is to be fully applied in sometimes urgent clinical situations, thus reducing even further its effectiveness. Therefore, it could be said that such puncture methods are an incomplete safety measure where it comes to reducing visible particle formation.
Identical infrared spectra were obtained with both bromobutyl samples, indicating that there is no fundamental chemical difference between bromobutyl samples. As bromobutyl elastomer was implicated in particle formation when using a short bevelled needle with a 90° puncture angle, with a incidence irrespective of thickness (7.5 % and 5 %, for 2 mm and 4 mm respectively), it seems plausible that the stopper thickness does not significantly affect visible particle incidence. The huge difference in particle incidence observed between situations N°3 and N°4 (0 % versus 75 %, when using a short bevelled needle, 90° puncture angle, with respectively a 2 mm or 4 mm thick chlorobutyl stopper) could be explained by the chlorobutyl thickness (2 mm versus 4 mm). However, as infrared spectrophotometric analysis of the chlorobutyl rubber showed a clear chemical difference between chlorobutyl samples, and with regard to the absence of influence of elastomer thickness for bromobutyl samples, it also seems plausible that the observed difference be linked to the chemical quality of the elastomer, and not to the thickness of the stopper. However, as it is possible to have variations of the chemical composition of the stopper from different suppliers (who employ various additives such as vulcanisers, accelerators, stabilizers, pigments), it is difficult to extrapolate the results of the present study to all stoppers.
The particles observed had on average dimensions of around a millimetre, yet some particles were more than 50 % bigger, with lengths greater than 1.5 mm. Qualitatively the particles look mostly like cores, but the variation in size as well as the presence of other shapes suggests that there may be multiples ways in which the particles are formed (tearing, shearing or shredding of the vial stopper). The dimensions we observed are consistent with those reported in other studies. Riess and Strong reported a particle having dimensions of 0.4 mm by 1.5 mm [2], and the particles observed from prednisone acetate vial stopper coring had sizes ranging from 0.6 mm to 1.1 mm [6]. When it comes to risk assessment, larger particles, despite plausibly being able to cause more clinical damage, are more easily noticed once created, due to their larger size. Smaller particles, on the other hand, can be much harder to detect, and may be more easily aspirated through the needle into the syringe used for parenteral administration. In our study, 18 gauge needles were used, with an interior diameter of 0.927 mm, and as such many of the particles created could have been aspirated up through it (although not the bigger ones). Particle colour can also aid or hamper detection, as it is generally easier to detect an orange particle than a grey one. In any case, vigilance and systematic visual inspection of the solution to be administered is of great importance.
This work has investigated potential risk factors impacting visible particle formation. The use of puncture-free medication vials as the source of the rubber vial stoppers is a guarantee that the results were not affected by a previous puncture of the elastomer, and is also close to real clinical situations. However, the analysis of particles formed was realised before aspirating the contents into a syringe (which is the next step in clinical contexts), in order to avoid particles adhering to the syringe’s piston, rendering their analysis difficult. The formation of visible particles is clearly a not uncommon situation, with incidence varying with the quality of the products available (injection or preparation medical devices, medication rubber stoppers), and puncture technique. The number of samples tested for each situation (n=40) is high enough for correct statistical analysis between situations; however it is not high enough to identify systematically very low particle incidence (less than 2.5 %).
In our establishment, adult and neonate intensive care units are especially aware of problem, and in those units, blunt bevelled metal needles are used for direct intravenous administrations. However, visible particles are probably only the tip of the particle iceberg, as the clinical impact of sub-visible particles has also been increasingly investigated [3, 20, 21], as well as their potential relevance to latex allergies [22, 23], and the only way to simultaneously reduce risks linked to both visible and subvisible particles would be to promote the systematic use of appropriate medical devices, such as terminal online filters for all parenteral administrations, and not just for infusions, and/or the use of filter needles.
In conclusion to this work, we have shown that rubber coring can be partially reduced by the use of an adapted puncture technique, and totally eliminated by using blunt metal needles.
About the authors

Philip Chennell is in charge of the Control and Development laboratory unit of the pharmacy department of Clermont-Ferrand’s University Hospital. He obtained his master’s degree in 2012, his PharmD in 2013, and is also currently a PhD candidate. He assumed teaching duties in 2014 at the University d’Auvergne, and is now member of the research team UMR CNRS 6296 “Materials for Health” at Clermont Auvergne University. His current professional interests focus on pharmaceutical preparations, medical devices and content-container interactions.

Daniel Bourdeaux is a pharmacist at the Control and Development laboratory unit of the pharmacy department of Clermont-Ferrand’s University Hospital since 2006 and has teached Clinical Pharmacy at the University d’Auvergne since 2006. He obtained his master’s degree in 2005 and his phD in 2012. Daniel Bourdeaux has been a member of C-BIOSENSS (Characterization and Biological SEcurity of Nano-Structured Surfaces, EA4676) since 2010.

Quentin Citerne studied pharmacy in Clermont-Ferrand from 2009 to 2014. He started his hospital pharmacy internship in November 2014 in Reims, and is currently completing his second year at the University Hospital of Nancy, France.

Catherine Arnaud has been working as a nurse at Clermont-Ferrand’s University Hospital since 1992, and obtained her Health Manager degree in 2002, and has been working in a reanimation ward for the last 14 years. Her daily interests are about healthcare organization and patient care, including the good use of medical devices and clinical problems linked to their use.

Sylvie Cosserant is a nurse with a master’s degree in Management of Health Organizations, and is a Senior Health Manager for several reanimation and anesthetic wards in Clermont-Ferrand’s University Hospital. Her objectives are to develop transversal cooperation between the different clinical wards and to promote paramedical research.

Véra Boiko Alaux obtained her PharmD in 1983, and began to specialize in medical devices in 1992. She is currently in charge of the medical devices unit of the pharmacy department of Clermont-Ferrand’s University Hospital, and is a member of Europharmat’s technical committee. Her main interests are about medical devices’ good use and content-container interactions.

Prof Valerie Sautou is a hospital pharmacist, head of pharmacy department of Clermont-Ferrand’s University Hospital. She is a professor of clinical pharmacy and biotechnology at Clermont Auvergne University. Her research activity is focused on medical devices and content-container interactions. Her research team unit is the UMR CNRS 6296 “Materials for Health”.
Conflict of interest statement: Authors state no conflict of interest. All authors have read the journal’s Publication ethics and publication malpractice statement available at the journal’s website and hereby confirm that they comply with all its parts applicable to the present scientific work.
References
Beer K. Potential foreign body emboli associated with botulinum toxin A injections. J Drugs Dermatol 2007 févr;6(2):220–1.Search in Google Scholar
2. Riess ML, Strong T. Near-embolization of a rubber core from a propofol vial. Anesth Analg 2008 mars;106(3):1020–1.10.1213/ane.0b013e31816323b4Search in Google Scholar
3. Singhal SK. particulate contamination in intravenous drugs: coring from syringe plunger. J Anaesthesiol Clin Pharmacol 2010 déc;26(4):564.10.4103/0970-9185.74621Search in Google Scholar
4. Stein HA, Vu BL. Coring: a potential problem in eye surgery. J Cataract Refract Surg 1994 mars;20(2):169–71.10.1016/S0886-3350(13)80159-9Search in Google Scholar
5. Asakura T, Seino H, Nozaki S, Abe R. Occurrence of coring in insulin vials and possibility of rubber piece contamination by self-injection. Yakugaku Zasshi 2001;121(6):459–63.10.1248/yakushi.121.459Search in Google Scholar PubMed
6. Campagna R, Pessis E, Guerini H, Feydy A, Drapé J-L. Occurrence of coring after needle insertion through a rubber stopper: study with prednisolone acetate. Eur Radiol 2013 févr 1;23(2):424–7.10.1007/s00330-012-2602-3Search in Google Scholar PubMed
7. Shiroyama K. The incidence of « coring » during aspiration of propofol from a 50-ml vial. J Anesth 2001;15(2):120.10.1007/s005400170042Search in Google Scholar PubMed
8. Wani T, Wadhwa A, Tobias JD. The incidence of coring with blunt versus sharp needles. J Clin Anesth 2014 mars;26(2):152–4.10.1016/j.jclinane.2013.10.007Search in Google Scholar PubMed
9. Dorris GG, Bivins BA, Rapp RP, Weiss DL, DeLuca PP, Ravin MB. Inflammatory potential of foreign particulates in parenteral drugs. Anesth Analg 1977 juin;56(3):422–8.10.1213/00000539-197705000-00022Search in Google Scholar PubMed
10. Lehr H-A, Brunner J, Rangoonwala R, Kirkpatrick CJ. Particulate matter contamination of intravenous antibiotics aggravates loss of functional capillary density in postischemic striated muscle. Am J Respir Crit Care Med 2002 févr 15;165(4):514–20.10.1164/ajrccm.165.4.2108033Search in Google Scholar PubMed
11. Doessegger L, Mahler H-C, Szczesny P, Rockstroh H, Kallmeyer G, Langenkamp A, et al. The potential clinical relevance of visible particles in parenteral drugs. J Pharm Sci 2012 août;101(8):2635–44.10.1002/jps.23217Search in Google Scholar PubMed
12. Cant AJ, Lenney W, Kirkham N. Plastic material from a syringe causing fatal bowel necrosis in a neonate. Br Med J Clin Res Ed 1988 avr 2;296(6627):968–9.10.1136/bmj.296.6627.968-aSearch in Google Scholar PubMed PubMed Central
13. United States Pharmacopoeia – National Formulary (USP-NF). (2015). Chapter <788>, Particulate Matter for Injections, USP 35–NF 30 reissueSearch in Google Scholar
14. European Pharmacopeia, 8th edition. (2015). Particulate contamination: visible particles. Method 2.9.20 2008Search in Google Scholar
15. Japanese Pharmacopoeia, 16th edition, (2010). Foreign Insoluble Matter Test for Injections, Chapter 6.06.Search in Google Scholar
16. Nicol G. Preventing rubber stopper coring. Anaesthesia 2002 févr;57(2):207.10.1046/j.1365-2044.2002.2470_41.xSearch in Google Scholar PubMed
17. Roth JV. How to enter a medication vial without coring. Anesth Analg 2007 juin;104(6):1615.10.1213/01.ane.0000260552.76585.53Search in Google Scholar PubMed
18. Shiroyama K, Izumi H, Kubo T. An advanced puncture technique decreases the incidence of coring during the use of 50-ml propofol vials. J Anesth 2002;16(2):181–2.10.1007/s005400200019Search in Google Scholar PubMed
19. Eskander J, Cotte J, Glenn E, Friedman S, Rosinia F. The incidence of coring and fragmentation of medication vial rubber stoppers. J Clin Anesth 2015 août;27(5):442–4.10.1016/j.jclinane.2015.01.009Search in Google Scholar PubMed
20. Boehne M, Jack T, Köditz H, Seidemann K, Schmidt F, Abura M, et al. In-line filtration minimizes organ dysfunction: new aspects from a prospective, randomized, controlled trial. BMC Pediatr 2013;13:21.10.1186/1471-2431-13-21Search in Google Scholar PubMed PubMed Central
21. Jack T, Boehne M, Brent BE, Hoy L, Köditz H, Wessel A, et al. In-line filtration reduces severe complications and length of stay on pediatric intensive care unit: a prospective, randomized, controlled trial. Intensive Care Med 2012 juin;38(6):1008–16.10.1007/s00134-012-2539-7Search in Google Scholar PubMed PubMed Central
22. Primeau M-N, Adkinson Jr NF, Hamilton RG. Natural rubber pharmaceutical vial closures release latex allergens that produce skin reactions. J Allergy Clin Immunol 2001 juin;107(6):958–s62.10.1067/mai.2001.115630Search in Google Scholar PubMed
23. Heitz JW, Bader SO. An evidence-based approach to medication preparation for the surgical patient at risk for latex allergy: is it time to stop being stopper poppers? J Clin Anesth 2010 Sept;22(6):477–83.10.1016/j.jclinane.2009.12.006Search in Google Scholar PubMed
©2016 Walter de Gruyter GmbH, Berlin/Boston
Articles in the same Issue
- Frontmatter
- graphical-abstract
- Editorial
- Quality and Safety in the Hospital: The Pharmacist is the Key Person
- Research Articles
- Rubber Coring of Injectable Medication Vial Stoppers: An Evaluation of Causal Factors
- Prospective Descriptive Study of RFID Tag Detection Rates based on Various Exploratory Scenarios Aimed at Identifying Optimal Conditions of Use
- Surface Contamination in a Teaching Hospital: A 6 Year Perspective
- Short Communications
- Evaluation of the Surface Contamination by Cytotoxic Agents of a Chemotherapy Reconstitution Unit: From Analysing Work Practices to Preventive and Corrective Actions
- Simultaneous Determination of Sufentanil and Ziconotide in Combination for Intrathecal Analgesia by UPLC-UV
- Reviewer Acknowledgment
Articles in the same Issue
- Frontmatter
- graphical-abstract
- Editorial
- Quality and Safety in the Hospital: The Pharmacist is the Key Person
- Research Articles
- Rubber Coring of Injectable Medication Vial Stoppers: An Evaluation of Causal Factors
- Prospective Descriptive Study of RFID Tag Detection Rates based on Various Exploratory Scenarios Aimed at Identifying Optimal Conditions of Use
- Surface Contamination in a Teaching Hospital: A 6 Year Perspective
- Short Communications
- Evaluation of the Surface Contamination by Cytotoxic Agents of a Chemotherapy Reconstitution Unit: From Analysing Work Practices to Preventive and Corrective Actions
- Simultaneous Determination of Sufentanil and Ziconotide in Combination for Intrathecal Analgesia by UPLC-UV
- Reviewer Acknowledgment