
Effects of virtual reality on fear of birth, length of labor, and fetal well-being: a randomized controlled trial
-
Mine Oruç

 and
Kamile Kabukcuoglu
and
Kamile Kabukcuoglu

Abstract
Objectives
The use of technological methods in childbirth is becoming increasingly common. This study aimed to evaluate the effects of virtual reality (VR) glasses on fear of childbirth, duration of labor, and fetal well-being in women undergoing term vaginal delivery.
Methods
This single-blind randomized controlled trial included 144 pregnant women, equally divided into VR and control groups, stratified by parity. The intervention group watched nature videos via VR glasses in two sessions during the active phase of labor. Data were collected using clinical record forms, a nonstress test (NST) monitoring form, and the Wijma Delivery Expectancy/Experience Questionnaire (W-DEQ-A/B).
Results
The use of VR significantly reduced fear of childbirth and shortened the active phase of labor among both primiparous and multiparous women (p<0.05). No significant differences were found in the total duration of labor or other phases. While significant differences were observed in fetal movements and accelerations between groups, no clinically adverse effects on fetal well-being were reported. No side effects or complications related to the VR intervention were observed.
Conclusions
VR appears to be a safe and effective non-pharmacological method to reduce childbirth fear and shorten the active phase of labor. Further studies are recommended to confirm its effects on labor physiology and neonatal outcomes.
Introduction
With the changing needs of humans and the advancement of technology, digital health services have gained importance in the transformation of healthcare, as in every other field. In line with the Sustainable Development Goals (SDGs) of the United Nations (UN) (2015), the use of digital health applications has accelerated to promote a healthy and quality life for every individual [1]. Digital health services, which have become important for modern health systems worldwide, have expanded to include scientific technologies such as artificial intelligence, wearable technologies, mobile applications, and telemedicine [2]. The most commonly used wearable technology is virtual reality (VR) glasses. VR glasses transport people from their current environment, immersing them in another environment where they can interact with objects within that environment [3], 4]. Because of this feature, VR glasses have emerged as a prominent tool for distraction in the field of healthcare.
The World Health Organization (WHO) advocates for creating a healing environment in health-promotion practices to enhance quality of life and address healthcare challenges. A healing environment can be defined as a physical and emotional setting intentionally designed to promote well-being and recovery by engaging the senses through elements such as natural light, soothing sounds, access to nature, green spaces, and art [5], 6]. Research indicates that one in three women experience psychological trauma during childbirth, even in the absence of physical injury, which can lead to depression, fear of childbirth, reduced breastfeeding, and long-term health issues [7]. Virtual reality (VR) applications have been identified as a tool for cultivating a healing environment by incorporating different layers of sensory experiences such as light and sound, as well as virtual elements including nature, green spaces, and art to enhance overall sensory engagement [3], 5]. Beyond these psychological and sensory benefits, its potential influence on physiological processes during labor has not yet been sufficiently explored. The use of various strategies that focus on the healing environment and relaxation therapy to enhance health, relieving physical symptoms, reduce anxiety, and manage fear plays a significant role in the development of physical birth environments that support the psychological and emotional processes of labor [4], [8], [9], [10], [11], [12], [13], [14].
The focus of SDG-3 – securing healthy lives and promoting well-being at all ages – a new global strategy, has been expanded. This goal goes beyond the survival of women and babies regarding birth, focusing not only on ensuring that they survive birth complications but also on ensuring that they reach and achieve their true strengths and abilities for health and well-being [6], 15]. Women’s birth-related experiences are shaped by subjective, psychological, and physiological processes affected by environmental factors. Prolonged labor, as an important physiological challenge, may negatively affect maternal well-being and neonatal outcomes [16]. Such experiences vary individually: For some women, birth is an exciting and beautiful event, while for others, it is a stressful, tiring, and unpredictable experience [6], 17]. Birth-related experiences are associated with various factors and emotional dimensions of care, affecting the overall maternal condition and fetal health [4]. The WHO has published new recommendations on intrapartum care for all pregnant women and newborns, from pregnancy to birth and the postpartum period. These recommendations go beyond preventing the risk of death and disease and include optimizing the health and well-being of women and babies [6], 18]. In this context, it is important to consider interventions that may positively affect not only maternal experiences but also neonatal outcomes.
The assessment of the fetal health status, severity of contractions, duration of labor, uncertainty of the process, negative birth experiences, and practices implemented after admission to the delivery room can cause stress, fear, and anxiety [4], 19], 20]. Reassuring women and providing supportive care during labor can reduce their fears, ensure the maintenance of fetal well-being, and provide them with a positive birth experience [21], 22]. According to a study conducted among OECD countries, 1 in 10 women who have not given birth prefers cesarean delivery due to the fear of birth [23]. While the fear of birth remains a worldwide problem, there is currently no definitive solution to reduce such fear and foster a positive birth experience. Moreover, although VR has been explored mainly in terms of psychological outcomes, there is a growing need for studies evaluating its impact on labor physiology and neonatal outcomes. The effects of VR applications on the fear of birth and fetal well-being remain unknown. Therefore, the aim of this study was to evaluate the effects of using VR glasses on the fear of birth, duration of labor, and intrapartum fetal well-being.
Subjects and methods
Design
This study adopted a single-blind randomized controlled experimental research design. The Consolidated Standards of Reporting Trials (CONSORT) Statement was followed, and the CONSORT 2010 checklist is provided as supplementary material. The study was registered in the clinicaltrials.gov registry (clinical trial number: NCT05723666).
Participants
The population of the study consisted of pregnant women who sought vaginal birth at the Training and Research Hospital and consented to participate in the study. Data were collected from March to September 2022.
The study included women who (1) could communicate verbally, (2) were aged 18–40 years, (3) had no hearing or vision limitations, (4) had a gestational age of 35–42 weeks, (5) had a singleton pregnancy, (6) planned to have vaginal birth, (7) did not experience any problems during previous pregnancies (e.g., early rupture of membranes, preeclampsia, or gestational diabetes), (8) had no anomalies identified in their fetus, and (9) were in the active phase of labor.
The sample size was calculated using G*Power 3.1 (Heinrich Heine University, Dusseldorf, Germany), based on a power of 80 %, a 5 % margin of error, and a 95 % confidence interval. The required sample size was determined to be 128 women (64 in the intervention [VR] group and 64 in the control group).
To account for a potential data loss rate of up to 15 % due to incomplete or missing data during data collection, the sample size was increased to 72 participants per group (a total of 144 women). Stratified sampling was applied to ensure homogeneity in parity, resulting in 36 primiparous and 36 multiparous women in each group.
Equal distribution by parity was preferred because the duration of labor is known to differ significantly between primiparous and multiparous women, which could influence study outcomes and comparisons between groups [24].
Randomization and blinding
Participants were randomly assigned to either the VR group or the control group. Simple randomization was conducted using the website https://www.random.org to ensure an equal number of participants in both groups. Randomization was not pre-generated; instead, it was performed individually at the time of each participant’s admission to the delivery room, at the beginning of the active phase of labor. This process determined the allocation of primiparous and multiparous women to either group.
Pregnant women (n=144) who agreed to participate in the study and were admitted to the delivery room at the beginning of the active phase of labor were divided into the VR (n=72) and control groups (n=72).
Blinding: Due to the nature of the intervention, neither the participants nor the researcher who conducted the intervention and collected the data were blinded to group allocation. However, the statistician who performed the analyses was blinded throughout the data analysis process.
Research procedures
An informed voluntary consent form and a personal information form were filled out by the VR and control groups. In the VR group, VR glasses were used. In both groups, routine birth monitoring and care were performed by delivery room staff. Both groups were followed up during labor using a clinical record form.
Interventions
VR group
After admission to the delivery room and completion of the informed consent and personal information forms, participants in the VR group received the intervention during the active phase of labor. The intervention involved the use of a virtual reality headset (VR BOX 2.0 model), which is a head-mounted display (HMD) compatible with smartphones. A smartphone was inserted into the headset, and 360-degree nature videos publicly available were displayed. These videos included calming natural scenes such as forests, waterfalls, and oceans. Soothing nature sounds accompanied the videos, and participants wore wired in-ear headphones to enhance immersion. The nature video was chosen because natural environments and sounds are well-documented to reduce stress and anxiety, promote relaxation, and contribute to a healing environment, as highlighted by WHO and recent studies on virtual nature interventions [5], 25].
The VR intervention was administered by the researcher. Before each session, participants were informed about the procedure and guided on how to use the VR headset. The researcher assisted participants with wearing the device and ensured that it was properly adjusted and functioning.
The first VR session lasted approximately 20 min and was conducted concurrently with the non-stress test (NST). This duration was selected because NST monitoring requires a minimum of 20 min of continuous observation to yield reliable results, during which participants were exposed to the VR video.
To evaluate the effects of VR on additional outcomes such as fear of childbirth and labor duration, a second VR session lasting 10 min was scheduled 2 h after the first. The duration of 10 min was chosen to provide additional exposure to VR without inducing fatigue or discomfort for women during the active phase of labor.
Participants who delivered before the second session, declined to participate, or were otherwise unable to complete it were considered as data loss and subsequently excluded from the study.
Only participants who completed both VR sessions were included in the final analysis. Following the second session, the Wijma Delivery Expectancy/Experience Questionnaire-A (W-DEQ-A) was administered. Labor duration was recorded using a clinical record form, and the W-DEQ-B was completed within 4 h postpartum.
Control group
After admission, the control group completed the consent and personal information forms. Following a 20-min NST, they filled out the NST monitoring form and W-DEQ-A. Labor duration was recorded using a clinical record form, and the Wijma Delivery Expectancy/Experience Questionnaire-B (W-DEQ-B) was administered within 4 h after birth.
Measurement tools
The personal information form, covering socio-demographic characteristics and pregnancy history, was completed by both the VR and control groups within the first hour of entering the delivery room. The clinical record form documented labor details, including cervical dilation, contraction patterns, fetal heart sounds, time of birth, and time of placental delivery. The time of placental delivery was recorded as part of routine labor monitoring. The NST monitoring form documented the pregnant women’s emotional state through observational notes during the procedure, as well as the NST results, including fetal heart rate baseline, variability, accelerations, and any decelerations. These parameters were evaluated by the researchers.
Fear of birth was measured using the W-DEQ-A and W-DEQ-B. Developed by Wijma et al. in 1998, the W-DEQ-A has a Cronbach’s alpha of 0.93 [26], 27], and the Turkish version, evaluated by Körükcü et al. in 2012, has an alpha of 0.89. The scale, which assesses women’s expectations about birth, includes 33 items scored on a 6-point Likert scale (0–5), with scores ranging from 0 to 165. Higher scores indicate greater fear, with thresholds for mild (≤37), moderate (38–65), severe (66–84), and clinical (≥85) levels of fear [28].
The W-DEQ-B, developed by Wijma et al. (1998), measures women’s fear of birth with a Cronbach’s alpha of 0.93. The Turkish version, evaluated by Korukcu et al. (2016), has a Cronbach’s alpha of 0.84. The 32-item scale uses a 6-point Likert scale (0–5), with scores ranging from 0 to 160, where higher scores indicate greater fear. It includes six subscales: concerns about contractions, positive behaviors, loneliness, positive emotions, birth, and the baby [29].
Ethical considerations
Approval for the conduct of the study was obtained from the Akdeniz University Clinical Research Ethics Committee (decision number: KAEK-524) (decision date: 07.07.2021) and for the use of the W-DEQ-A and W-DEQ-B from the chief physician of the Akdeniz University Hospital and Assoc. Dr. Öznur Körükcü. In addition, verbal and written consent were obtained from women who agreed to participate in the study.
Data analysis
The data obtained in the study were analyzed using the free trial version of the Statistical Package for the Social Sciences for Windows 25.0. Descriptive statistics (i.e., numbers, percentages, means, and standard deviations [SDs]) were used to present the data. An independent-sample t-test was conducted to test whether the quantitative variables obtained from two unrelated samples differed significantly from each other. The chi-square test was performed to test whether there was a significant difference between the two groups. p-values below 0.05 were considered significant.
Results
The initial study sample consisted of 204 pregnant women. Of them, 60 were excluded because they did not meet the inclusion criteria. The pregnant women were randomly allocated into either the control group (n=72) or the VR group (n=72). Each group comprised 36 primiparous women and 36 multiparous women. Figure 1 shows the CONSORT flow diagram of the study.
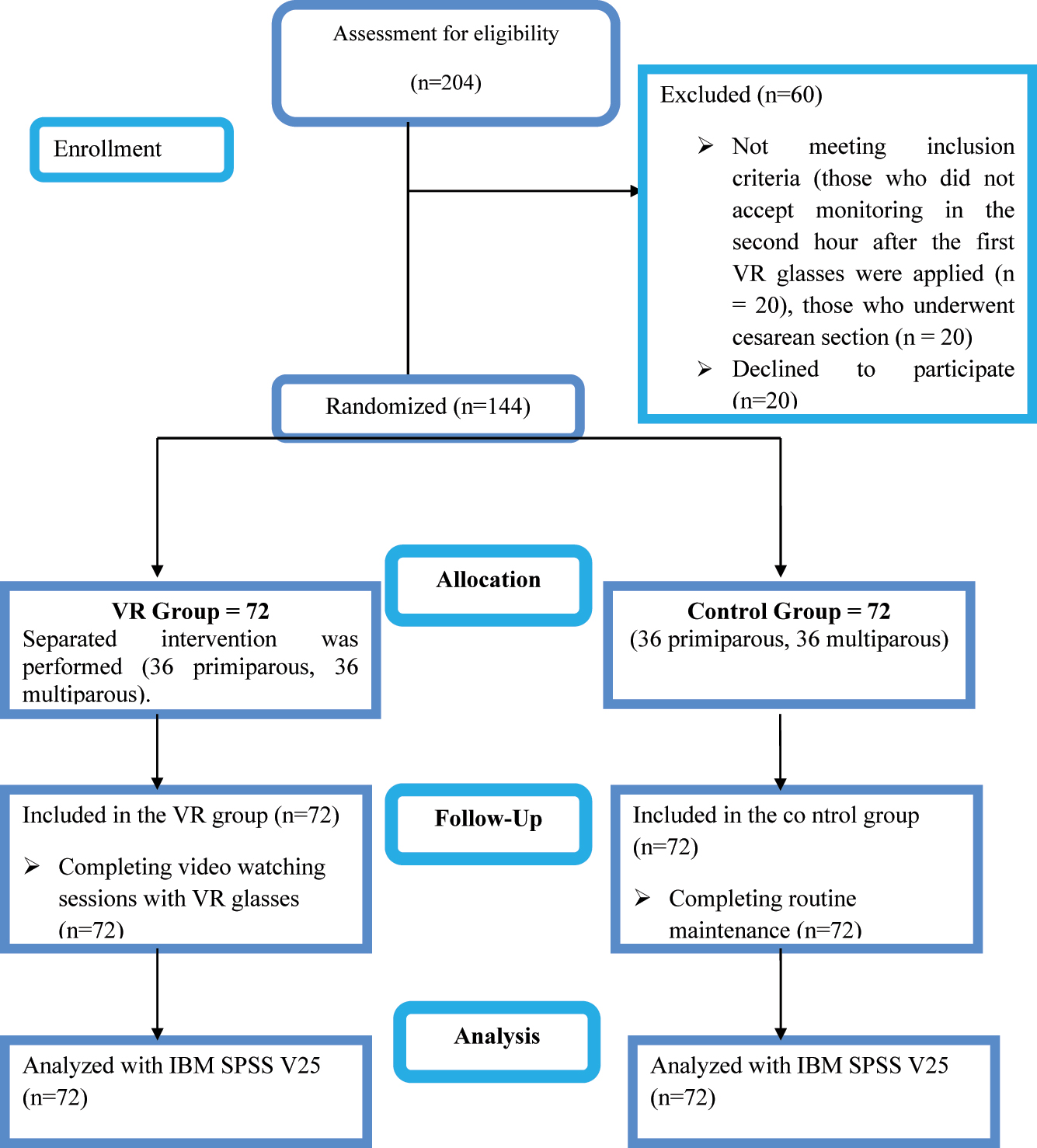
Consort flow chart.
The average age of primiparous women was 24.28 years (VR group) and 23.47 years (control group). For multiparous women, it was 26.50 years (VR group) and 26.69 years (control group). About 38.9 % of primiparous women in the control group and 55.5 % in the VR group were at or beyond 40 weeks of gestation. For multiparous women, 41.7 % in the control group and 36.1 % in the VR group were at or beyond 40 weeks. Approximately 47.2 % of multiparous women in both groups had low educational levels, and 80.6 % of multiparous women in the control group were housewives. Over 80 % of primiparous women in both groups desired their pregnancy (Table 1).
Sociodemographic characteristics of participants (n=144).
| Characteristics | VR group (n=72) | Control group (n=72) | ||
|---|---|---|---|---|
| Age, mean (SD), y | ||||
| Primiparous | 24.28 (3.49) | 23.47 (2.88) | ||
| Multiparous | 26.50 (3.37) | 26.69 (4.41) | ||
|
|
||||
| Primiparous | Multiparous | Primiparous | Multiparous | |
|
|
||||
| Gestational age, n, % | ||||
| 38–39 week | 16 (44.4) | 23 (63.9) | 22 (61.1) | 21 (58.4) |
| 40 and more | 20 (55.5) | 13 (36.1) | 14 (38.9) | 15 (41.7) |
| Level of education, n, % | ||||
| Low | 10 (27.8) | 17 (47.2) | 13 (36.1) | 17 (47.2) |
| Medium | 15 (41.7) | 12 (33.3) | 10 (27.8) | 14 (38.9) |
| High | 11 (30.6) | 7 (19.4) | 13 (36.1) | 5 (13.9) |
| Professional status, n, % | ||||
| Housewife | 16 (44.4) | 22 (61.1) | 18 (50.0) | 29 (80.6) |
| Civil servant | 7 (19.4) | 5 (13.9) | 6 (16.7) | 2 (5.6) |
| Self-employment | 13 (36.1) | 9 (25.0) | 12 (33.3) | 5 (13.9) |
| Desired pregnancy | ||||
| Yes | 30 (83.3) | 29 (80.6) | 34 (94.4) | 26 (72.2) |
| No | 6 (16.7) | 7 (19.4) | 2 (5.6) | 10 (27.8) |
Duration of labor
The total duration of labor (p=0.177), duration of the latent phase of labor (p=0.174), duration of the transition phase of labor (p=0.075), duration of the second stage of labor (p=0.483), and duration of the third stage of labor (p=0.428) among the primiparous women did not significantly differ between the control and VR groups. In contrast, the duration of the active phase of labor (p=0.000) among the primiparous women significantly differed between the groups. The active phase of labor among the primiparous women was longer in the control group than in the VR group (Table 2).
Length of childbirth results of VR group and control group.
| Variables | Control group | VR group | ||||
|---|---|---|---|---|---|---|
| Primiparous |
|
SS |
|
SS | t | p-Value |
| Total duration of labor, hour | 7.08 | 2.94 | 6.25 | 2.18 | 1.365 | 0.177 |
| Duration of the latent phase, hour | 6.22 | 1.42 | 6.89 | 2.54 | −1.376 | 0.174 |
| Duration of the active phase, hour | 5.86 | 2.26 | 2.11 | 0.89 | 9.277 | 0.000a |
| Duration of the transition phase, hour | 2.00 | 0.96 | 1.64 | 0.72 | 1.807 | 0.075 |
| Duration of the second stage, minute | 23.89 | 9.23 | 22.39 | 8.80 | 0.706 | 0.483 |
| Duration of the third stage, minute | 12.61 | 5.15 | 11.56 | 6.06 | 0.797 | 0.428 |
| Multiparous | ||||||
| Total duration of labor, hour | 5.25 | 2.35 | 5.39 | 1.92 | −0.275 | 0.784 |
| Duration of the latent phase, hour | 5.25 | 2.32 | 5.25 | 2.49 | 0.000 | 1.000 |
| Duration of the active phase, hour | 3.75 | 1.81 | 2.69 | 1.12 | 2.977 | 0.004a |
| Duration of the transition phase, hour | 1.33 | 0.59 | 1.67 | 0.86 | −1.919 | 0.060 |
| Duration of the second stage, minute | 15.86 | 6.26 | 16.03 | 4.74 | −0.127 | 0.899 |
| Duration of the third stage, minute | 9.42 | 4.03 | 10.17 | 3.75 | −0.817 | 0.417 |
The total duration of labor (p=0.784), duration of the latent phase of labor (p=1.000), duration of the transition phase of labor (p=0.060), duration of the second stage of labor (p=0.899), and duration of the third stage of labor (p=0.417) among the multiparous women did not significantly differ between the control and VR groups. Conversely, there was a significant difference in the duration of the active phase of labor among the multiparous women between the groups (p=0.004). The active phase of labor among the multiparous women was shorter in the VR group (2.69 h) than in the control group (3.75 h) (Table 2). This is because the calculation of total labor duration includes the latent, active, second, and third stages. Since no significant differences were observed in the latent, second, or third stages, the reduction in the active phase alone did not lead to a significant difference in the total labor duration.
NST results
Among primiparous women, fetal movements (p=0.000) and accelerations (p=0.001) significantly differed between the VR and control groups. Both parameters were higher in the control group. No significant difference was found in the number of decelerations between the groups (p=0.874) (Table 3).
NST results of VR group and control group.
| Variables | Control group | VR group | ||||
|---|---|---|---|---|---|---|
| Primiparous |
|
SS |
|
SS | t | p-Value |
| The numbers of fetal movements | 5.69 | 2.30 | 8.22 | 2.86 | −4.131 | 0.000a |
| The numbers of accelerations | 7.50 | 1.89 | 6.17 | 1.30 | 3.489 | 0.001a |
| Multiparous | ||||||
| The numbers of fetal movements | 6.75 | 2.12 | 8.42 | 2.33 | −3.174 | 0.002a |
| The numbers of accelerations | 7.06 | 2.30 | 5.94 | 1.91 | 2.227 | 0.029a |
Among multiparous women, there were significant differences in fetal movements (p=0.002) and accelerations (p=0.029) between the groups. Accelerations were more frequent in the control group, whereas fetal movements were higher in the VR group (Table 3).
W-DEQ-A scores
The W-DEQ-A scores of the primiparous and multiparous women significantly differed between the VR and control groups. Based on the W-DEQ-A scores, the primiparous women in the VR and control groups had moderate and severe fear of birth, respectively. Similarly, the multiparous women in the VR and control groups were found to have moderate (40.69) and severe (77.81) fear of birth, respectively (Table 4).
Wijma birth expectation/experience scale/version A (W-DEQ-A) results of VR group and control.
| W-DEQ.A | Control group | VR group | ||||
|---|---|---|---|---|---|---|
|
|
SS |
|
SS | t | p-Value | |
| Primiparous | 77.50 | 18.70 | 55.33 | 9.61 | 6.326 | 0.000a |
| Multiparous | 77.81 | 21.12 | 40.69 | 6.95 | 10.015 | 0.000a |
W-DEQ-B scores
Among multiparous women, the overall W-DEQ-B score was significantly lower in the VR group (49.43) compared to the control group (91.50). Additionally, all six W-DEQ-B subscale scores were significantly lower in the VR group than in the control group (p<0.05), as shown in Table 5.
Wijma birth expectation/experience scale/version B (W-DEQ-B) results of VR group and control group.
| Variables | Control group | VR group | ||||
|---|---|---|---|---|---|---|
| Primiparous |
|
SS |
|
SS | t | p-Value |
| Anxiety about labor pain | 28.83 | 5.69 | 15.75 | 4.30 | 11.002 | 0.000a |
| Lack of positive behaviors | 11.36 | 3.15 | 8.14 | 3.11 | 4.371 | 0.000a |
| Loneliness | 17.94 | 5.24 | 12.00 | 4.07 | 5.374 | 0.000a |
| Lack of positive emotions | 21.97 | 5.20 | 11.31 | 3.50 | 10.205 | 0.000a |
| Anxiety about birth | 7.39 | 2.63 | 4.00 | 1.84 | 6.335 | 0.000a |
| Anxiety about the baby | 5.00 | 2.98 | 2.25 | 1.87 | 4.692 | 0.000a |
| W-DEQ.B | 92.50 | 17.83 | 53.44 | 8.13 | 11.957 | 0.000a |
| Multiparous | ||||||
| Anxiety about labor pain | 26.92 | 4.24 | 15.28 | 3.68 | 12.434 | 0.000a |
| Lack of positive behaviors | 11.17 | 2.91 | 5.67 | 2.38 | 8.775 | 0.000a |
| Loneliness | 18.25 | 4.12 | 9.14 | 2.54 | 11.287 | 0.000a |
| Lack of positive emotions | 23.17 | 3.51 | 10.69 | 2.78 | 16.726 | 0.000a |
| Anxiety about birth | 6.78 | 2.23 | 3.33 | 1.55 | 7.609 | 0.000a |
| Anxiety about the baby | 4.22 | 2.51 | 1.31 | 1.45 | 6.040 | 0.000a |
| W-DEQ.B | 90.50 | 10.70 | 45.42 | 5.87 | 22.167 | 0.000a |
Among primiparous women, similar results were observed, with the VR group scoring lower on all W-DEQ-B subscales compared to the control group, indicating a lower level of fear following childbirth.
Discussion
This study demonstrated that the use of VR glasses during labor shortened the duration of the active phase of labor, and reduced the fear of birth among the pregnant women. It is reasonable to expect that VR-based distraction will be most beneficial during the active phase, when pain, stress, and anxiety are most intense. However, no improvement was observed in NST parameters such as fetal movements and accelerations in the VR group. On the contrary, both parameters were significantly higher in the control group, suggesting that VR did not have a positive impact on fetal activity during labor. Fetal reactivity during NST may be governed by physiological processes that are less directly influenced by brief, intrapartum VR exposure, whereas maternal affect (stress/anxiety) is more amenable to modulation in the active phase.
There was no significant difference noted in the total duration of labor of the primiparous and multiparous women between the control and VR groups in the present study. In the study by Akin et al. (2021), it was found that VR application was ineffective in shortening the duration of the first and second stages of labor [27]. In the study by Ebrahimian et al. (2021), the first and second stages of labor were shorter in the VR group than in the control group. Conversely, Gökduman Keleş and Altinkaya (2022) found no significant difference in the duration of labor of primigravida women between the control group and the group that used VR glasses. In our trial, total labor time did not differ despite a shorter active phase, because total duration aggregates the latent, active, second, and third stages; in the absence of changes in the other stages, a reduction confined to the active phase alone is unlikely to yield a statistically significant difference in total labor time.
In the present study, the active phase of labor was shorter in the VR group than in the control group. Similarly, in a randomized controlled study using VR during labor, the active phase was found to be shorter in the VR group than in the control group [8]. In the study by Estrella-Juarez et al. (2023), the first stage of labor among mothers who received VR application and music therapy was shorter than that among mothers who received the control intervention [30]. Karacan and Akköz Çevik (2022) also reported congruent findings in their study conducted among 114 primiparous pregnant women who used VR glasses and applied breathing exercises [31]. The authors found that the active phase of labor was shorter for mothers who used VR glasses than for those who received the control treatment. This resulted in a reduction in the level of stress hormones due to the increased comfort experienced by pregnant women during labor. The shortened duration of the active phase of labor observed in the VR group may be related to improved maternal comfort and reduced stress, which are known to promote endogenous oxytocin release during labor [6]. Although oxytocin levels were not measured in this study, previous literature suggests that psychological well-being and relaxation can positively influence labor progression through hormonal pathways. Taken together, these data support a stage-specific effect: VR appears most beneficial when pain and anxiety peak (active phase), whereas effects in other stages may be limited. This stage-specific effect may be attributed to the fact that stress, pain, and anxiety peak during the active phase of labor. As the need for distraction and psychological support is greatest in this critical period, the impact of VR becomes more pronounced. This mechanism may explain why VR is particularly effective in the active phase, while its influence appears limited in the earlier or later stages of labor.
Factors such as psychological well-being, anxiety, and stress can affect the NST results of pregnant women [32], 33]. In this study, significant differences were found in the numbers of fetal movements and accelerations between the VR and control groups. Previous studies have shown that reduced anxiety and increased maternal relaxation may lead to more frequent fetal movements and accelerations during NST [32], 34]. However, in the present study, fetal movements and accelerations were not consistently higher in the VR group. In fact, in primiparous women, both parameters were higher in the control group. These findings suggest that while VR may reduce anxiety and fear of birth, its effects on fetal reactivity during labor may not follow a predictable pattern and could be influenced by additional physiological or contextual factors. Accordingly, VR’s psychological benefits may not uniformly translate into changes in fetal activity indices recorded during intrapartum monitoring.
The fear and stress experienced by women during labor cause the level of cortisol secreted to increase [35]. In the present study, the primiparous and multiparous women in the VR group experienced less fear of birth than did those in the control group. Although no study using VR was found in the literature review to report reduced fear of birth, the results are consistent with those of studies examining the effects of distraction and relaxation techniques on the fear of birth. In their study, Klabbers et al. (2019) found that the level of fear of birth decreased after haptotherapy compared with that after the control intervention [36]. Conversely, Koyuncu and Bülbül (2021) discovered that women who did yoga had lower levels of fear of birth [37]. Additionally, in a study examining the effects of hypnosis during and after pregnancy, it was found that the W-DEQ-A scores were lower in spontaneous vaginal birth [38].
The main purpose of managing the fear of birth among women is to either eliminate their uncertainties about birth or help them accept these uncertainties and reduce their concerns about birth [21]. In this study, the women’s concerns about labor pain were fewer in the VR group than in the control group. In the study by Akin et al. (2021), the perceived labor pain and anxiety levels were found to be lower in the intervention group where ultrasound images of babies were shown using VR glasses than in the control group. Other studies have also shown that watching videos using VR devices during birth reduces pain and anxiety [10], 11], 19]. Numerous non-pharmacological techniques, including breathing exercises, massage, aromatherapy, music therapy, and hypnobirthing, have been shown to reduce labor-related pain and anxiety [8], 22]. These methods work primarily by promoting relaxation and diverting attention away from pain. Virtual reality (VR), as a modern distraction technique, combines immersive visual and auditory stimuli to create a multi-sensory experience. This approach may enhance the effectiveness of traditional methods by fully engaging the user’s attention and altering pain perception through cognitive distraction [11]. The concentration of benefit during the active phase aligns with this mechanism, as cognitive load and nociceptive input are highest and thus most modifiable at that time.
In the present study, the loneliness subscale score of both primiparous and multiparous women was found to be lower in the VR group than in the control group. In the literature review, no study was found to use a distraction method to reduce mothers’ feelings of loneliness during labor. However, in some studies, motivational interviews, education, and psychological interventions such as counseling reduced feelings of loneliness [39], 40]. These findings indicate the need for more studies using technological methods such as VR applications aimed at reducing feelings of loneliness. Reducing perceived loneliness may also be one pathway through which VR improves comfort and contributes to a shorter active phase, although this requires confirmation in future research.
In this study, the anxiety level of the primiparous and multiparous women regarding birth and their baby was found to be lower in the VR group than in the control group. In a previous study where VR was used as a distraction method, the birth-related anxiety levels were observed to be lower in the VR group [8]. In their study, Akin et al. (2021) reported that the anxiety level of pregnant women who watched videos using VR glasses was lower. While several non-pharmacological interventions aim to reduce fear and anxiety during labor, not all are equally effective across different subdimensions. For example, in a study by Vural and Aslan (2019), emotional freedom techniques and breathing awareness did not significantly affect the subdimension related to fear about the baby [41]. This highlights that certain interventions may have limited effects on specific aspects of childbirth fear. In contrast, the use of VR in the present study was associated with lower levels of fear related to both labor and the baby, suggesting that immersive distraction techniques may have broader psychological benefits.
While the fear of birth of the primiparous women in the VR group was at a moderate level (53.44), that of the primiparous women in the control group was at a clinical level (92.50) (Table 5). In the present study, both W-DEQ-A and W-DEQ-B scores were significantly lower in the VR group compared to the control group, among both primiparous and multiparous women. These findings indicate that the use of VR during labor may help reduce both anticipatory fear and the actual experience of childbirth-related fear. Although no previous study was identified that used the W-DEQ-B in evaluating VR interventions, other distraction-based methods such as cognitive behavioral therapy or yoga have been shown to reduce childbirth fear [20], 37]. These results support the potential of immersive technologies like VR in addressing psychological aspects of childbirth.
Beyond statistical significance, the findings of this trial may have important implications for clinical practice. Reducing childbirth fear and shortening the active phase of labor can enhance maternal comfort and potentially decrease the need for pharmacological interventions such as analgesics or anxiolytics. The absence of adverse effects further supports VR as a safe, acceptable, and easily implementable adjunct to routine intrapartum care. Given that the active phase is the most stressful stage for both women and healthcare providers, VR could serve as a practical, non-pharmacological tool to improve the birth experience and contribute to more positive maternal outcomes. Future research should also investigate implementation strategies and cost-effectiveness to guide integration of VR into standard practice.
Limitations and strengths
This study has several limitations. First, the sample included only women who experienced spontaneous vaginal births, which limits the generalizability of the results to women who undergo cesarean sections or assisted births. Second, data loss occurred due to 20 participants in the VR group refusing further monitoring after the first session, 10 experiencing rapid labor progression, and 30 requiring cesarean delivery due to negative NST results. These exclusions were accurately represented in the CONSORT flow diagram (Figure 1), where the data loss due to withdrawal, rapid labor, and cesarean deliveries was documented. Third, although the W-DEQ-A is a widely validated instrument, its application during the active phase of labor may have been cognitively burdensome for some participants. Administering the questionnaire before labor onset could have provided a more stable baseline for anticipatory fear. Fourth, the VR intervention involved only two short sessions (20 and 10 min), and the video content was not personalized. These factors may have affected the depth and duration of the VR’s psychological impact.
Despite these limitations, the study has several strengths. It is among the few randomized controlled trials exploring immersive VR use during labor. Stratified randomization by parity ensured balanced group allocation, and both primiparous and multiparous women were included. The use of validated instruments (W-DEQ-A and B) and standardized clinical documentation strengthened the study’s methodological integrity. Furthermore, the real-time implementation of VR in an actual clinical setting supports its practical applicability.
Conclusions
Based on the findings of this randomized controlled trial, the use of VR glasses during labor significantly reduced the duration of the active phase and decreased the fear of childbirth among both primiparous and multiparous women. However, VR did not shorten the total duration of labor, which is an important outcome that highlights the need to interpret its benefits with caution. Although there were significant differences in NST parameters between the groups, the clinical implications of these differences remain uncertain, and no direct negative impact on fetal well-being was observed. No side effects or adverse reactions related to the VR intervention were reported by participants or observed by clinical staff. Taken together, these results suggest that VR may serve as a safe and effective non-pharmacological method to support maternal comfort during labor, primarily by reducing childbirth fear and facilitating a shorter active phase, rather than by shortening the overall labor process. Further studies with larger and more diverse populations are recommended to explore long-term effects, optimize content and duration of VR exposure, and examine potential physiological impacts more comprehensively.
Acknowledgment
We would like to thank all participants and the clinical staff who supported this study.
-
Research ethics: The authors confirm that the data utilized in this manuscript have been lawfully acquired. Approval for this study was obtained from the Akdeniz University Clinical Research Ethics Committee (decision number: KAEK-524) (decision date: 07.07.2021). The study was conducted in accordance with the Declaration of Helsinki (as revised in 2013).
-
Informed consent: Informed consent was obtained from all individuals included in the study.
-
Author contributions: All authors have accepted responsibility for the entire content of this manuscript and approved its submission. CRediT authorship contribution statement. Mine Oruc: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Project administration, Validation, Writing – original draft, Writing – review & editing. Kamile Kabukcuoglu: Project administration, Supervision, Writing – review & editing.
-
Use of Large Language Models, AI and Machine Learning Tools: None declared.
-
Conflict of interest: The authors state no conflict of interest.
-
Research funding: None declared.
-
Data availability: The datasets generated and/or analyzed during the current study are available from the corresponding author on reasonable request.
-
Clinical trial registration: Clinical trial number: NCT05723666.
References
1. United nations, department of economic and social affairs. 17 goals. Available from: https://sdgs.un.org/goals [Accessed 18 July 2025].Search in Google Scholar
2. Mathews, SC, McShea, M, Hanley, CL, Ravitz, A, Labrique, AB, Cohen, AB, et al.. Digital health: a path to validation. NPJ Digit Med 2019;2:38. https://doi.org/10.1038/s41746-019-0111-3.Search in Google Scholar PubMed PubMed Central
3. Bevilacqua, R, Maranesi, E, Riccardi, GR, Di Donna, V, Pelliccioni, P, Luzi, R, et al.. Non-immersive virtual reality for rehabilitation of the older people: a systematic review into efficacy and effectiveness. J Clin Med 2019;8:1882. https://doi.org/10.3390/jcm8111882.Search in Google Scholar PubMed PubMed Central
4. Hansen, ML, Lorentzen, IP, Andersen, CS, Jensen, HS, Fogsgaard, A, Foureur, M, et al.. The effect on the birth experience of women and partners of giving birth in a “birth environment room”: a secondary analysis of a randomised controlled trial. Midwifery 2022;112:103424. https://doi.org/10.1016/j.midw.2022.103424.Search in Google Scholar PubMed
5. Boz, İ. Healing caring environment. Balıkesir Health Sci J 2018;7:56–61. https://doi.org/10.5505/bsbd.2018.88579.Search in Google Scholar
6. World Health Organization. WHO recommendations: intrapartum care for a positive childbirth experience. Geneva: World Health Organization; 2019. Available from: [Accessed 18 July 2025].Search in Google Scholar
7. Mucuk, Ö, Özkan, H. Travmatik doğum eylemi ve ebelik bakımı. Arch Curr Med Res 2021;30:218–25. https://doi.org/10.17827/aktd.938148.Search in Google Scholar
8. Ebrahimian, A, Bilandi, RR, Bilandī, MRR, Sabzeh, Z. Comparison of the effectiveness of virtual reality and chewing mint gum on labor pain and anxiety: a randomized controlled trial. BMC Pregnancy Childbirth 2022;22:49. https://doi.org/10.1186/s12884-021-04359-3.Search in Google Scholar PubMed PubMed Central
9. Gökduman, KM. The effect of virtual reality glasses played with music during episiotomy repair on women’s perceived pain, vital signs and postpartum comfort. Aydın: Aydın Adnan Menderes University, Institute of Health Sciences; 2022. Available from: National Thesis Center of the Council of Higher Education (Turkey) [doctoral thesis]: https://tez.yok.gov.tr.Search in Google Scholar
10. Massov, L, Robinson, B, Rodriguez-Ramirez, E, Maude, R. Virtual reality is beneficial in decreasing pain in labouring women: a preliminary study. Aust N Z J Obstet Gynaecol 2023;63:193–7. https://doi.org/10.1111/ajo.13591.Search in Google Scholar PubMed
11. Mohammad, EB, Ahmad, M. Virtual reality as a distraction technique for pain and anxiety among patients with breast cancer: a randomized control trial. Palliat Support Care 2019;17:29–34. https://doi.org/10.1017/S1478951518000639.Search in Google Scholar PubMed
12. Mohamed, H, Sweelam, M, Mohamed, HM, Mohamed, A, Elkhalek, N, Mohamed, N, et al.. Effect of virtual reality application on pain and anxiety among primiparous women with episiotomy. Egypt J Health Care 2022;13:625–39. https://doi.org/10.21608/ejhc.2022.233172.Search in Google Scholar
13. Tan, XYJ, Choong, SYX, Cheng, LJ, Lau, Y. Relaxation interventions for improving sleep outcomes in perinatal women: a systematic review and meta-analysis of randomized controlled trials. Midwifery 2021;103:103151. https://doi.org/10.1016/j.midw.2021.103151.Search in Google Scholar PubMed
14. Tian, Q, Xu, M, Yu, L, Yang, S, Zhang, W. The efficacy of virtual reality–based interventions in breast cancer–related symptom management: a systematic review and meta-analysis. Cancer Nurs 2023;46:E276–87. https://doi.org/10.1097/NCC.0000000000001099.Search in Google Scholar PubMed
15. United Nations. The sustainable development goals report 2017. New York: United Nations; 2017:20–4 pp.Search in Google Scholar
16. Girault, A, Lepelletier, M, Le Ray, C, ENP2021 Study Group. Maternal and neonatal outcomes of prolonged second stage of labor with delayed pushing: a study of French perinatal practices before and after guideline changes. Eur J Obstet Gynecol Reprod Biol 2025;304:63–9. https://doi.org/10.1016/j.ejogrb.2024.11.010.Search in Google Scholar PubMed
17. Namujju, J, Muhindo, R, Mselle, LT, Waiswa, P, Nankumbi, J, Muwanguzi, P, et al.. Childbirth experiences and their derived meaning: a qualitative study among postnatal mothers in Mbale regional referral hospital, Uganda. Reprod Health 2018;15:1–11. https://doi.org/10.1186/s12978-018-0628-y.Search in Google Scholar PubMed PubMed Central
18. Yıldız, H. Intrapartum care model for a positive childbirth experience: world health organization’s recommendations. J Health Sci Kocaeli Univ 2019;5:98–105. Available from: https://dergipark.org.tr/en/download/article-file/719906.10.30934/kusbed.546900Search in Google Scholar
19. McCauley, E, Rood, K, Benedict, J, Koenig, N, Schaffir, J. Maternal mood and anxiety effects on the fetal nonstress test: voluntary submission. Am J Obstet Gynecol MFM 2023;5:101053. https://doi.org/10.1016/j.ajogmf.2023.101053.Search in Google Scholar PubMed
20. Najafi, TF, Dashti, S, Bolghanabadi, N, Rezvanifard, M, Andaroon, N, Abadibavil, D, et al.. Evaluation of the effect of cognitive behavioral therapy on tocophobia: a systematic review and meta-analysis. Arch Psychiatr Nurs 2021;35:255–60. https://doi.org/10.1016/j.apnu.2021.03.009.Search in Google Scholar PubMed
21. Häggsgård, C, Nilsson, C, Teleman, P, Rubertsson, C, Edqvist, M. Women’s experiences of the second stage of labour. Women Birth 2021;35:e464–70. https://doi.org/10.1016/j.wombi.2021.11.005.Search in Google Scholar PubMed
22. Smith, CA, Levett, KM, Collins, CT, Jones, L, Dahlen, HG, Suganuma, M, et al.. Massage, reflexology and other manual methods for pain management in labour. Cochrane Database Syst Rev 2018;3:CD009290. https://doi.org/10.1002/14651858.CD009290.pub3.Search in Google Scholar PubMed PubMed Central
23. Stoll, KH, Hauck, YL, Downe, S, Payne, D, Hall, W, ICAPP Study Team. Preference for cesarean section in young nulligravid women in eight OECD countries and implications for reproductive health education. Reprod Health 2017;14:116. https://doi.org/10.1186/s12978-017-0354-x.Search in Google Scholar PubMed PubMed Central
24. Rosenbloom, JI, Rottenstreich, A, Yagel, S, Sompolinsky, Y, Levin, G. The length of the second stage of labor in nulliparous, multiparous, grand-multiparous, and grand-grand multiparous women in a large modern cohort. Eur J Obstet Gynecol Reprod Biol 2020;253:273–7. https://doi.org/10.1016/j.ejogrb.2020.08.029.Search in Google Scholar PubMed
25. Chan, SHM, Qiu, L, Esposito, G, Mai, KP, Tam, KP, Cui, J, et al.. Nature in virtual reality improves mood and reduces stress: evidence from young adults and senior citizens. Virtual Real 2023;27:3285–300. https://doi.org/10.1007/s10055-021-00604-4.Search in Google Scholar PubMed PubMed Central
26. Wijma, K, Wijma, B, Zar, M. Psychometric aspects of the WDEQ: a new questionnaire for the measurement of fear of childbirth. J Psychosom Obstet Gynaecol 1998;19:84–97. https://doi.org/10.3109/01674829809048501.Search in Google Scholar PubMed
27. Akin, B, Yilmaz Kocak, M, Küçükaydın, Z, Güzel, K. The effect of showing images of the foetus with the virtual reality glass during labour process on labour pain, birth perception and anxiety. J Clin Nurs 2021;30:2301–8. https://doi.org/10.1111/jocn.15768.Search in Google Scholar PubMed
28. Korukcu, O, Kukulu, K, Firat, MZ. The reliability and validity of the Turkish version of the wijma delivery expectancy/experience questionnaire (W-DEQ) with pregnant women. J Psychiatr Ment Health Nurs 2012;19:193–202. https://doi.org/10.1111/j.1365-2850.2011.01694.x.Search in Google Scholar PubMed
29. Korukcu, O, Bulut, O, Kukulu, K. Psychometric evaluation of the wijma delivery expectancy/experience questionnaire version B. Health Care Women Int 2016;37:550–67. https://doi.org/10.1080/07399332.2014.943838.Search in Google Scholar PubMed
30. Estrella-Juarez, F, Requena-Mullor, M, Garcia-Gonzalez, J, Lopez-Villen, A, Alarcon-Rodriguez, R. Effect of virtual reality and music therapy on the physiologic parameters of pregnant women and fetuses and on anxiety levels: a randomized controlled trial. J Midwifery Womens Health 2023;68:35–43. https://doi.org/10.1111/jmwh.13413.Search in Google Scholar PubMed
31. Karacan, E, Akkoz Cevik, S. The effect of breathing exercises using a breathing exercise device and virtual reality applications during pregnancy and labor on labor. CIN Comput Inform Nurs 2024;42:780–7. https://doi.org/10.1097/CIN.0000000000001178.Search in Google Scholar PubMed
32. Khodakarami, B, Janesari Ladani, M, Kazemi, F, Aghababaei, S. The effect of music on fetus movement during non-stress test. Avicenna J Nurs Midwifery Care 2020;28:1–8. https://doi.org/10.30699/ajnmc.28.4.1.Search in Google Scholar
33. Timur, TS, İnci Coşkun, E, Nacar, G, Erci, B. The effect of motivational video and nutrition on the non-stress test: a randomized controlled clinical trial. J Obstet Gynaecol 2022;43:1–7. https://doi.org/10.1080/01443615.2022.2034765.Search in Google Scholar PubMed
34. Gebuza, G, Zaleska, M, Kaźmierczak, M, Mieczkowska, E, Gierszewska, M. The effect of music on the cardiac activity of a fetus in a cardiotocographic examination. Adv Clin Exp Med 2018;27:615–21. https://doi.org/10.17219/acem/68847.Search in Google Scholar
35. Amiri, P, Mirghafourvand, M, Esmaeilpour, K, Kamalifard, M, Ivanbagha, R. The effect of distraction techniques on pain and stress during labor: a randomized controlled clinical trial. BMC Pregnancy Childbirth 2019;19:534. https://doi.org/10.1186/s12884-019-2683-y.Search in Google Scholar PubMed PubMed Central
36. Klabbers, GA, Wijma, K, Paarlberg, KM, Emons, WH, Vingerhoets, AJ. Haptotherapy as a new intervention for treating fear of childbirth: a randomized controlled trial. J Psychosom Obstet Gynaecol 2019;40:38–47. https://doi.org/10.1080/0167482X.2017.1398230.Search in Google Scholar PubMed
37. Koyuncu, SB, Bülbül, M. The impact of yoga on fear of childbirth and childbirth self-efficacy among third trimester pregnants. Complement Ther Clin Pract 2021;44:101438. https://doi.org/10.1016/j.ctcp.2021.101438.Search in Google Scholar PubMed
38. Babbar, S, Oyarzabal, AJ. The application of hypnosis in obstetrics. Clin Obstet Gynecol 2021;64:635–47. https://doi.org/10.1097/GRF.0000000000000635.Search in Google Scholar PubMed
39. Calpbinici, P, Özçirpan, ÇY. The effect of the training program provided to primiparous pregnant women through the motivational interview method on their fear of childbirth, childbirth self-efficacy, and delivery mode: a randomized controlled trial. Curr Psychol 2023;42:21609–23. https://doi.org/10.1007/s12144-022-03285-7.Search in Google Scholar
40. Mortazavi, F, Mehrabadi, M, karrabi, R. Effectiveness of solution-focused counseling therapy on pregnancy anxiety and fear of childbirth: a randomized clinical trial. Nurs Pract Today 2021;8:244–54. https://doi.org/10.21203/rs.3.rs-137775/v1.Search in Google Scholar
41. Vural, PI, Aslan, E. Emotional freedom techniques and breathing awareness to reduce childbirth fear: a randomized controlled study. Complement Ther Clin Pract 2019;35:224–31. https://doi.org/10.1016/j.ctcp.2019.02.011.Search in Google Scholar PubMed
Supplementary Material
This article contains supplementary material (https://doi.org/10.1515/jpm-2025-0462).
© 2025 the author(s), published by De Gruyter, Berlin/Boston
This work is licensed under the Creative Commons Attribution 4.0 International License.