Quality of life and reconstructive surgery efforts in severe hand injuries
-
Seyed Arash Alawi
 ,
Dennis Werner
,
Dennis Werner

Abstract
Introduction:
Severe hand trauma, leading to extensive skeletal and tissue defects, requires plastic surgical reconstruction of the highest level aiming at maximizing function and aesthetics. The intention of this study was to investigate clinical parameters and resource consumption connected with severe hand injuries, with specific emphasis on a follow-up evaluation of quality of life after the reconstruction process.
Materials and methods:
In this retrospective study, we evaluated patients with severe hand injuries from 2013 to 2016 who had completed surgical and non-surgical treatment. Measures included total period of therapy (TPT) in days, total duration of operations including anesthesia (TOA), total duration of all operations (TO), and total number of operations (TNO). We also determined total inpatient stay (TIS), total number of clinic presentations with interventions (TNPI), initial hand injury severity score (iHISS), and inpatient proceeds (IPP) in Euros (€). Correlation was assessed between iHISS and TOA, TNO, and TIS. Finally, these patients were reexamined in a follow-up inquiry and the life quality was assessed with the five-level version of the EuroQol five-dimensional (EQ-5D) descriptive system (EQ-5D-5L).
Results:
We analyzed 12 patients with an average age of 44 years (min. 24 years, max. 75 years). Patients receiving reconstructive surgery experienced median (
Conclusion:
Severe hand injuries are related to high efforts for surgical and functional reconstructions, which result in high quality of life measured with the EQ-5D-5L assessment. However, for a defined collective of patients, myoelectric prosthetic functional replacement should be considered. Further studies are necessary to examine functional outcomes and quality of life after bionic prosthetic replacement. Also, a bionic reconstruction score to define hard criteria for taking an acute treatment decision is necessary.
Introduction
Severe hand trauma, leading to extensive skeletal and tissue defects, requires plastic surgical reconstruction of the highest level aiming at maximizing function and aesthetics. However, results sometimes do not fulfill the requirements and expectations of the patient, likely resulting in deficits of function and aesthetics of the upper extremity that warrant sequential operations. Repetitive procedures, which cause both psychological stress and long hospitalization times for the patient, may fail to achieve the degree of functional improvement necessary for optimal patient rehabilitation. In addition to the emotional burden resulting from the injury and the possible functional impairment, severe hand injuries may result in reduced work-place productivity and long return-to-work times [1].
Generally, biological reconstruction should be attempted first to restore function and appearance. However, when critical damage is present, the process of reconstruction should be well considered [2]. An alternative amputation and supply with an advanced prosthesis may be a better option for restoration of a functional hand. However, an emergency score assessing the extent of injury and surgical efforts needed for reconstruction in terms of predicting a reasonable functional and aesthetic outcome is still missing. This score would help decide whether it is worth to reconstruct or to amputate a severely damaged extremity in an emergency setting in the trauma room. Some concepts were established for bionic supply when biological reconstruction failed to regain a satisfactory functional outcome; however, a score for initial decision making is lacking thus far [3].
In light of the current developments and innovations in robotics and bionic prosthetic replacement, improved function and better rehabilitation might be expected. Hereby, the term “bionics” is the application of observed biological functions, which were transferred to designs of engineering systems and modern technologies [4]. These improved results might lead to new and different surgical strategies aiming at definitive prosthetic and bionic rehabilitation rather than frustrating biological reconstruction efforts.
Especially, the psychological burden after mutilation of the hand and the following repetitive reconstruction should be considered [5]. After such damage, the complete psyche is also suffering with a distortion of self-image. This psychological impairment may even have a similar importance as the functional loss and should be considered when biological reconstruction is planned. Severe hand injuries can be associated with pain syndromes like complex regional pain syndrome, major depression, as well as adjustment problems [6]. Not only the mechanics of the hand are an important aspect, but the hand is also an important sensory unit that completes other sensory organs. Symptoms after such a trauma may include nightmares, phantom limb sensations, flashbacks, and thoughts about disfigurement. Especially, post-traumatic stress disorders take an important part in the early stage of processing the injury [7], [8].
Based on current developments, there has been progress in modular prosthetic limb replacement as well as biologic integration, and this path should be considered when a patient with severe hand injury is presented [9]. Bionic prostheses as well as exoskeletons enable a high degree of hand-like function and have a normal extremity appearance. Most of the systems are based on electromyography (EMG) signals through local conscious muscle activation creating a surface potential, which can be used to move the extremity. Further, distant muscle EMG signals can be used by implantable myoelectric sensors to control the device [10]. In addition to these technical developments, pre-bionic training and preparation is needed and is important for appropriate use of the bionic prosthesis [11]. Training is provided with computer-based training systems for prosthetic use and demo bionic prostheses, which are not connected to the body [12]. When considering bionic restoration, an initial review of medical history as well as a thorough clinical examination with identification of EMG signals is necessary. At least two EMG signals are necessary to establish the surface electrodes [13]. For injuries where specific local muscles are deinnervated, surgical procedures, such as neurotization in which the muscle receives a functional nerve or parts of a nerve with a pattern of stimulus allowing reinnervation, are needed. This “targeted muscle reinnervation” restores nerve signals of the muscle through a motor signal [14], [15]. The current negative perceptions of conventional upper-limb prostheses occur mainly due to their low level of functionality as well as discomfort and pain. In some parts of the world, especially Eastern regions, prostheses have a negative stigma. With recent developments, this negative perception might change, and a rethinking of reconstructive procedures may be possible.
The aim of this study was to investigate clinical parameters and resource consumption connected with severe hand injuries. Specific emphasis was placed on evaluation of quality of life after reconstruction to define the validity of surgical reconstruction by a follow-up investigation of the five-level version of the EuroQol five-dimensional (EQ-5D) descriptive system. Additionally, we determined hospital costs, including the duration of surgery, length of stay, and number of operations correlated to the severity of hand injuries.
Materials and methods
In this monocentric, non-randomized, non-blinded, and retrospective study, we included 12 male patients with severe hand injuries from 2013 to 2016, who had completed surgery based on a review of all coded Diagnosis Related Groups (DRGs). The inclusion criteria were severe soft tissue defects; massive injury to the functional structures of the digits, metacarpus, or carpus; and amputation of hand parts. We reviewed the medical records, which included the photographs of the injury upon arrival in the operating room and notes of the findings during the operation. We included all patients who were initially treated at our hospital after trauma and where the treatment was fully documented. We evaluated each patient with injury-related procedures in the electronic Systems Application Product (SAP) system (SAP Deutschland SE&Co. KG, Walldorf, Rhein-Neckar, Version 22.10, Germany), starting at the point of initial trauma care, throughout the indicated operations, and finishing on the final date the patient was treated in our department.
Analysis of images of the physical appearance was facilitated by an internal photography documentation with the image management system (IMS, Imagic Bildverarbeitung AG, Glattbrugg, Switzerland). The initial severity of the hand injury was evaluated based on the initial hand injury severity score (iHISS) from the earliest photographs of the injury. Based on the photographs, we calculated the iHISS using a standard protocol [16]. Our controlling department calculated the inpatient proceeds (IPP) based on the DRG coding. Through the SAP system, we were able to follow every coded operation from the initial trauma date until the last procedure.
We evaluated the following parameters: (1) average age; (2) total period of therapy (TPT) in days, ranging from the initial presentation to the final documented inpatient and outpatient presentation; (3) total duration of all operations including anesthesia (TOA) in hours, calculated by adding 0.5 h for preoperative anesthesia and 0.5 h for ending anesthesia; (4) total duration of all operations (TO); (5) total number of operations (TNO); (6) total inpatient stay (TIS) in days; (7) total number of clinic presentations with interventions (TNPI); and (8) the iHISS. High HISS scores indicate a higher severity and worse functional outcome, and lower scores indicate a lower severity and better functional outcome [16], [17], [18]. An iHISS of 20 points or below is regarded as a “minor” injury, between 21 and 50 as a “moderate” injury, between 51 and 100 as a “severe” injury, and 101 or above as a “major” injury [16]. Proceeds associated with the injury in Euros (€) (9) were calculated from the point of trauma to hospital admission with initial operative treatment up to the latest registered procedure. Correlation was assessed between iHISS and TOA, TNO, and TIS, as well as the proceeds by using Pearson correlation coefficients. The loss of productivity in percent [German=Minderung der Erwerbsfähigkeit (MdE)] was researched through patient files.
The MdE is one of several legal requirements in Germany for the award of an injury pension due to an accident at work, a road accident, or an occupational disease by the statutory accident insurance. Insured persons whose earning capacity is reduced by at least 20% beyond the 26th week as a result of an accident at work or an occupational disease are entitled to such a pension.
Finally, to evaluate the surgical effort, we made a follow-up investigation to evaluate the EQ-5D-5L index value. The EQ-5D-5L is a descriptive system that consists of five dimensions (mobility, self-care, usual activities, pain/discomfort, and anxiety/depression). However, each dimension has five levels: no problems, slight problems, moderate problems, severe problems, and extreme problems. Ethical approval was obtained from the institutional review board (ethical approval no. 7352).
Results
The reconstruction process for each case was unique and highly individualized. Our review recorded the following data about severe hand injuries of 12 male patients: an average age of 44 years (min. 24, max. 75) (1), TPT in days [

Severe hand injury data.
(1) Age in years (median
We also recorded the TNO (median
We also assessed the IPP (Figure 2, graph 9), finding a median cost of 14,595 €. The majority (>50%) of patients had iHISS up to 150, which correlated with proceeds with a correlation coefficient of 0.871 (Figure 2, graph 10). We further determined whether the initial injury severity (iHISS) correlated with TOA (Figure 2, graph 11a), TNO (Figure 2, graph 11b), and TIS (Figure 2, graph 11c); iHISS was positively correlated with each of these factors (Pearson correlation coefficient TIS=0.817, TOA=0.857, TNO=0.871). The loss of productivity (MdE) was not defined in four cases that did not stem from a work-related accident. In two cases, the patients did not incur any loss of productivity (MdE). In four cases, the MdE was 15%, 5%, 40%, and 50%. In two patients, the evaluation was in progress at the time this paper was prepared. Based on the follow-up inquiry, the EQ-5D-5L index value resulted in a high level of life quality with a median score of 0.898 (min. 0.8, max. 1) (Figure 3). An overview of the analyzed patients is shown in Table 1.

iHISS correlation with procedure parameters.
(9) IPP (
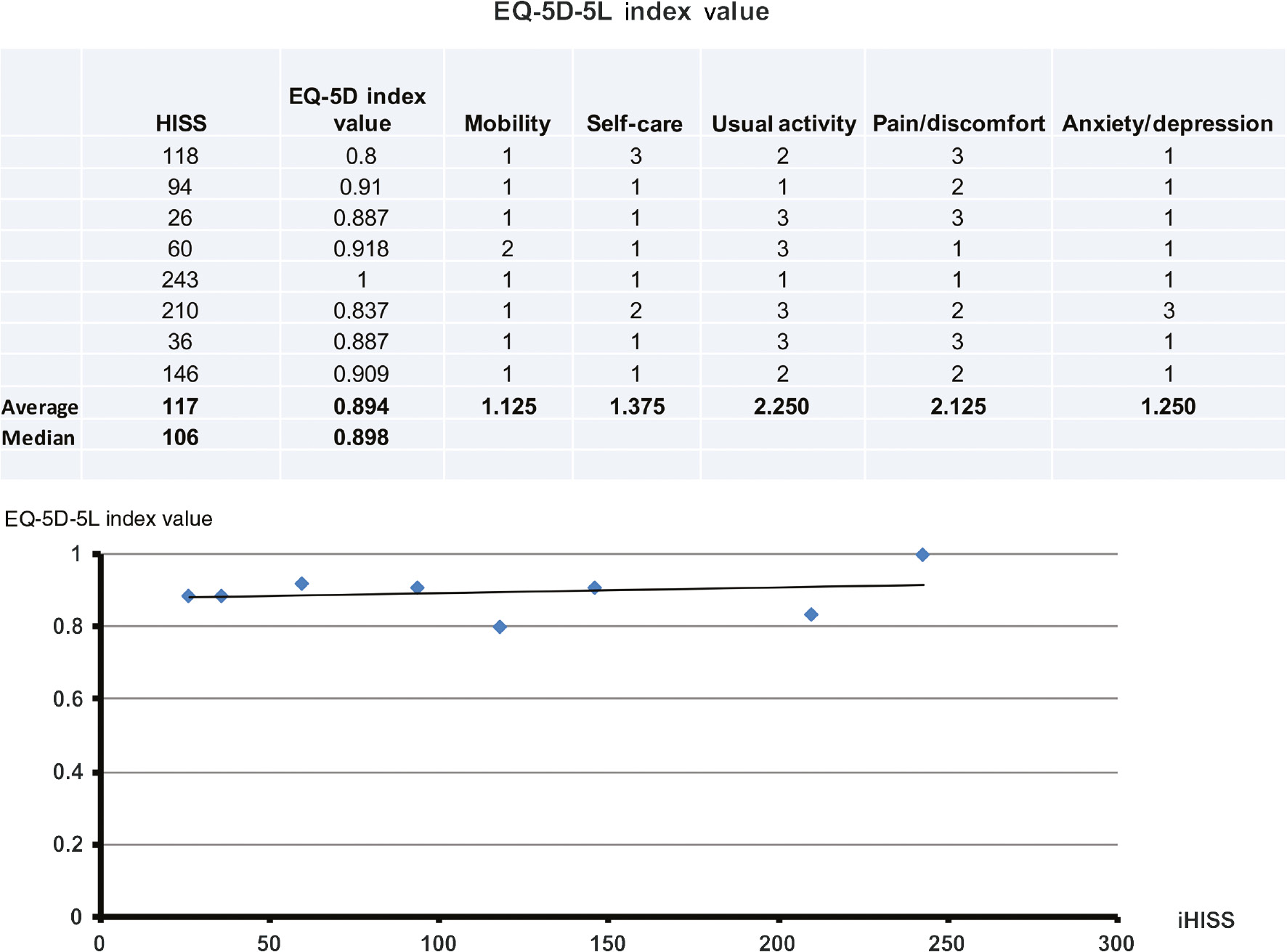
Life quality EQ-5D-5L.
Based on the follow-up inquiry, the EQ-5D-5L index value resulted in a high level of life quality with a median score of 0.898 (min. 0.8, max. 1).
Overview of analyzed severe hand injuries.
| Patient | Age (years) | HISS | Type of trauma | TPT (days) | TIS (days) | TOA (h) | TNO | EQ-5D-5L index value | Mobility | Self-care | Usual activity | Pain/discomfort | Anxiety/depression |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 75 | 118 | Circular saw injury | 164 | 15 | 12 | 4 | 1 | 1 | 3 | 2 | 3 | 1 |
| 2 | 38 | 16 | Circular saw injury | 56 | 5 | 4 | 1 | ||||||
| 3 | 53 | 94 | Rotating steel brush | 185 | 8 | 6 | 1 | 1 | 1 | 1 | 1 | 2 | 1 |
| 4 | 49 | 26 | Explosion injury | 52 | 9 | 6 | 3 | 1 | 1 | 1 | 3 | 3 | 1 |
| 5 | 60 | 46 | Circular saw injury | 48 | 41 | 14 | 4 | ||||||
| 6 | 46 | 60 | Contusion injury/laceration | 861 | 85 | 37 | 10 | 1 | 2 | 1 | 3 | 1 | 1 |
| 7 | 48 | 243 | Contusion injury/laceration | 483 | 103 | 59 | 21 | 1 | 1 | 1 | 1 | 1 | 1 |
| 8 | 31 | 210 | Contusion injury/laceration | 356 | 87 | 38 | 14 | 1 | 1 | 2 | 3 | 2 | 3 |
| 9 | 27 | 36 | Motorcycle accident | 28 | 14 | 13 | 5 | 1 | 1 | 1 | 3 | 3 | 1 |
| 10 | 24 | 47 | Circular saw injury | 26 | 7 | 4 | 2 | ||||||
| 11 | 50 | 146 | Circular saw injury | 733 | 29 | 22 | 5 | 1 | 1 | 1 | 2 | 2 | 1 |
| 12 | 31 | 284 | Contusion injury/laceration | 547 | 140 | 56 | 20 | ||||||
| Min | 24 | 16 | 26 | 5 | 4 | 1 | |||||||
| Median | 47 | 77 | 175 | 22 | 13 | 5 | |||||||
| Max | 75 | 284 | 861 | 140 | 58.8 | 21 |
Figure 4 shows a representative image of severe injuries in both hands seen in a 29-year-old patient with complete soft tissue avulsion and partial amputation of digits I–IV of the left hand and digits I, II, and IV of the right hand, as well as multiple fractures of the hands on both sides.
![Figure 4: Compilation of severe hand injuries – initial trauma and results.Example of a severe hand injury of both hands with complete soft tissue avulsion and partial amputation of digits I–IV of the left hand and digits I, II, and IV of the right hand in a 29-year-old patient. Multiple fractures of the hands on both sides were noted (A). Initially, we carried out a debridement and a restoration of the skin, i.e. a full skin graft of the residual tissue on both sides. Additionally, we prepared stump formation of digits I–IV of the left hand and digits I, II, and IV of the right hand. On the right hand (B), an amputation of the distal finger of the interphalangeal (IP) joint of digit I, an amputation of the distal IP joint (DIP) of digit II, and an exarticulation of the distal phalanx of digit IV followed. Multiple debridements and the installation of a vacuum system followed. After initial skin necrosis, we temporarily covered the defect with Epigard on the right hand [B(6)]. On the left hand (C), we initially performed an amputation of the distal phalanx in the IP joint of digit I. Amputation was done on the intermediate phalanx of digit II as well as the intermediate phalanx of digit III. The skin defect was temporary covered with xenograft on the left hand [C(2)]. For saving the position of the fingers, K-wire fixation of the stumps was done [B(9) and C(5)]. Subsequently, Matriderm and split-thickness skin transplantation on both hands was carried out. After the initial skin healing [B(8) and C(3)], we processed an extensive scar release in combination with arterio- and neurolysis and creation of a new first intermediate finger fold on the left hand. On the right hand, a detachment of the adductor pollicis as well as the interosseus dorsalis was carried out, and the defect was reconstructed with a groin flap [B(9)]. A reconstruction was done with a free groin flap for the right side and a pedicled groin flap from the left side. Flap thinning and repositioning of the flaps was carried out for improving the aesthetic appearance [C(9)]. Patient data: age 29 years, TPT=547 days, TOA=56 h, TO=36 h, TNO=20, TIS=140 days, TNPI=9, iHISS=284, and IPP=66,534 €.](/document/doi/10.1515/iss-2018-0002/asset/graphic/j_iss-2018-0002_fig_004.jpg)
Compilation of severe hand injuries – initial trauma and results.
Example of a severe hand injury of both hands with complete soft tissue avulsion and partial amputation of digits I–IV of the left hand and digits I, II, and IV of the right hand in a 29-year-old patient. Multiple fractures of the hands on both sides were noted (A). Initially, we carried out a debridement and a restoration of the skin, i.e. a full skin graft of the residual tissue on both sides. Additionally, we prepared stump formation of digits I–IV of the left hand and digits I, II, and IV of the right hand. On the right hand (B), an amputation of the distal finger of the interphalangeal (IP) joint of digit I, an amputation of the distal IP joint (DIP) of digit II, and an exarticulation of the distal phalanx of digit IV followed. Multiple debridements and the installation of a vacuum system followed. After initial skin necrosis, we temporarily covered the defect with Epigard on the right hand [B(6)]. On the left hand (C), we initially performed an amputation of the distal phalanx in the IP joint of digit I. Amputation was done on the intermediate phalanx of digit II as well as the intermediate phalanx of digit III. The skin defect was temporary covered with xenograft on the left hand [C(2)]. For saving the position of the fingers, K-wire fixation of the stumps was done [B(9) and C(5)]. Subsequently, Matriderm and split-thickness skin transplantation on both hands was carried out. After the initial skin healing [B(8) and C(3)], we processed an extensive scar release in combination with arterio- and neurolysis and creation of a new first intermediate finger fold on the left hand. On the right hand, a detachment of the adductor pollicis as well as the interosseus dorsalis was carried out, and the defect was reconstructed with a groin flap [B(9)]. A reconstruction was done with a free groin flap for the right side and a pedicled groin flap from the left side. Flap thinning and repositioning of the flaps was carried out for improving the aesthetic appearance [C(9)]. Patient data: age 29 years, TPT=547 days, TOA=56 h, TO=36 h, TNO=20, TIS=140 days, TNPI=9, iHISS=284, and IPP=66,534 €.
Discussion
Our results show that severe hand injuries with a high iHISS are correlated with repetitive operations and are connected with long operation times, high numbers of total operations, and long therapy intervals. On average, the TPT was 175 days, which shows the long process of therapy and surgical treatment to restore the best possible function and aesthetics. In addition, the TO in hours with an average of 9 h and an accumulated average of TIS of 22 days emphasize the consequences of severe hand injuries with repeated interventions and reconstructions. However, our investigations emphasize the good outcomes in life quality based on the EQ-5D-5L assessment although the high psychological burden after mutilation of the hand [5]. The initial injury severity (iHISS) is positively correlated with TOA (Figure 2, graph 11a), TNO (Figure 2, graph 11b), and TIS in days (Figure 2, graph 11c) with a Pearson correlation coefficient of TIS=0.817, TOA=0.857, and TNO=0.871. A final evaluation of functional outcome after surgical reconstruction must be done in a follow-up survey. Based on investigations, a replantation is indicated after combined and complex macroamputations of the upper extremity [19], [20]. In cases with sharp wound edges, for example, specialists agree on an absolute indication for replantation. For cases with additional soft tissue damage including avulsion and multilevel injury, an early amputation should be considered even if authors report that there might be psychological benefits. However, even if the functional outcome is poor, the reintegration and partial recovery seem to be important for the patients’ self-perception [19], [20], [21]. Under the aspect of current developments and possibilities of bionic reconstruction, it may be a good alternative to aim for initial amputation and for prosthetic supply thereafter. In addition, bionic prostheses are superior to amputation stumps from the aesthetic point of view.
Costs for the health-care system arise mainly from direct, indirect, and intangible costs like repetitive operations, intensive physiotherapy, and occupational therapy as well as inadequate reintegration in the working place. As we only could account for proceeds based on the DRGs, the complete costs could not be quantified like indirect costs due to all concluded therapies. Based on different methodologies, the costs for the health-care system are estimated to be about 10,000 €–40,000 € per case [22], [23], [24] compared to our results with a median IPP of 14,595 €. Initially, due to disability and post-traumatic disorder, quality of life suffers [25], [26]; however, it seems to reach good values after a complete reconstruction process. Factors that improve long-term outcome after severe hand injuries are not only the anatomical reconstruction but also a multidisciplinary approach with pain management, early psychotherapeutic treatment, occupational therapy, as well as early rehabilitation programs. In addition, individual factors like social and financial support [27], perception of disability, motivation of rehabilitation, and coping from trauma take an essential part of rehabilitation and return to work after severe hand trauma [28]. Based on the medical history as well as social and cultural background, the treatment should be adapted by early involvement of the patient to optimize the outcome and life quality [29].
Parallel to the progress of current surgical reconstruction methods, there have been vast improvements in modern bionic prosthesis, including sensory feedback of the prosthesis through implementation of nerve connections. This allows the perception of natural sensations when touching and gripping an object. Initial results are promising for artificial sensors for hand prostheses, which stimulate the median and ulnar nerve by multichannel, intra-fascicular electrodes. These sensors can allow for a differentiation between stiffness and shape [30], [31]. More research is necessary to implement modern techniques such as osseous integration or connection between muscles and nerves into biologic systems [31], [32], [33]. The sensory feedback mechanism is fundamental for the complete range of function of an extremity and may allow patients to manipulate objects gradually. For example, a patient with tetraplegia recovered extremity functionality by undergoing reconstruction using neuro-prosthetic limbs, as shown by Collinger et al. [34]. Aszmann et al. [3] showed that bionic prostheses could yield good functional outcomes in severe hand injuries. Recent developments also allow partial hand prostheses, which improve the functionality for patients with partial hand and digit amputations. In addition to this new focus on technical replacement, normal human function may also be enhanced [14].
The methodological shortcoming of the study is the cross-sectional nature of the investigation as well as the snapshot of the current EQ-5D-5L. The adaption process is not measured. The retrospective nature of the HISS calculation and the lack of a standardized homogeneous control group for all questionnaires limit the study. Based on the investigation, the quality of life was little affected by the hand injury in the majority of patients.
Conclusion
The value of surgical reconstruction is certainly present due to the good quality of life assessed; however, the development of prosthetic-engineering disciplines will profoundly alter the goals of plastic and reconstructive surgery. The use of these technologies will continue to grow, enabling advances in the replacement of damaged tissue. A shared decision making by the patient and physician at an appropriate time point on which treatment to take, gaining the best possible functional and aesthetic results, is essential. An emergency score assessing the extent of injury and surgical efforts needed for reconstruction in terms of predicting a reasonable functional and aesthetic outcome should be established. This score would help decide whether it is worth to reconstruct or to amputate a severely damaged extremity in an emergency setting in the trauma room.
A comparison between surgical restoration and early bionic prostheses supply, in terms of functionality, patient satisfaction, and price, is recommended for future studies. Related thereto, a bionic reconstruction score has to be defined even if investigations show that the iHISS can adequately predict for a functional outcome [17], [18]. However, there is no established scoring system for mutilating hand injuries and validated method to predict functional recovery compared to bionic supply. Early amputation and temporary coverage of defects with the intention to restore hand function with a bionic prosthesis should be investigated in pilot studies. For patients, we must compare established surgical procedures with modern limb prosthetic devices and define hard criteria for taking a treatment decision [35].
Author Statement
Research funding: The authors received no financial support for the research, authorship, and/or publication of this article. Conflict of interest: The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. Informed consent: Informed consent was taken from all included patients. Ethical approval: The research related to human use complied with all the relevant national regulations and institutional policies, was performed in accordance to the tenets of the Helsinki Declaration and approval was obtained from the institutional review board (ethical approval no. 7352).
Author Contributions
Seyed Arash Alawi: conceptualization; data curation; formal analysis; investigation; methodology; project administration; resources; supervision; validation; visualization; writing – original draft; writing – review and editing. Dennis Werner: data curation; writing – review and editing. Sören Könneker: formal analysis; writing – review and editing. Peter M. Vogt: conceptualization; formal analysis; methodology; project administration; writing – review and editing. Andreas Jokuszies: data curation; formal analysis; methodology; supervision; writing – review and editing.
Publication Funding
The German Society of Surgery funded the article processing charges of this article.
References
[1] Rosberg HE, Carlsson KS, Cederlund RI, Ramel E, Dahlin LB. Costs and outcome for serious hand and arm injuries during the first year after trauma – a prospective study. BMC Public Health 2013;13:501.10.1186/1471-2458-13-501Search in Google Scholar PubMed
[2] Sherman R. To reconstruct or not to reconstruct? N Engl J Med 2002;347:1906–7.10.1056/NEJMp020150Search in Google Scholar PubMed
[3] Aszmann OC, Vujaklija I, Roche AD, Salminger S, Herceg M, Sturma A, et al. Elective amputation and bionic substitution restore functional hand use after critical soft tissue injuries. Sci Rep 2016;6:34960.10.1038/srep34960Search in Google Scholar PubMed
[4] Lipetz LE. Bionics. Science 1963;140:1419–26.10.1126/science.140.3574.1419Search in Google Scholar PubMed
[5] Grob M, Papadopulos NA, Zimmermann A, Biemer E, Kovacs L. The psychological impact of severe hand injury. J Hand Surg Eur Vol 2008;33:358–62.10.1177/1753193407087026Search in Google Scholar PubMed
[6] Mendelson RL, Burech JG, Polack EP, Kappel DA. The psychological impact of traumatic amputations. A team approach: physician, therapist, and psychologist. Hand Clinics 1986;2:577–83.10.1016/S0749-0712(21)00564-3Search in Google Scholar PubMed
[7] Cohen RI. Post-traumatic stress disorder: does it clear up when the litigation is settled? Br J Hosp Med 1987;37:485.Search in Google Scholar PubMed
[8] Johnson RK. Psychologic assessment of patients with industrial hand injuries. Hand Clinics 1993;9:221–9.10.1016/S0749-0712(21)00963-XSearch in Google Scholar PubMed
[9] Cipriani C, Controzzi M, Carrozza MC. The SmartHand transradial prosthesis. J Neuroeng Rehabil 2011;8:29.10.1186/1743-0003-8-29Search in Google Scholar PubMed
[10] Weir RF, Troyk PR, DeMichele GA, Kerns DA, Schorsch JF, Maas H. Implantable myoelectric sensors (IMESs) for intramuscular electromyogram recording. IEEE Trans Bio-Med Eng 2009;56:159–71.10.1109/TBME.2008.2005942Search in Google Scholar
[11] Aszmann OC, Roche AD, Salminger S, Paternostro-Sluga T, Herceg M, Sturma A, et al. Bionic reconstruction to restore hand function after brachial plexus injury: a case series of three patients. Lancet 2015;385:2183–9.10.1016/S0140-6736(14)61776-1Search in Google Scholar PubMed
[12] Mattioli FE, Lamounier EA Jr, Cardoso A, Soares AB, Andrade AO. Classification of EMG signals using artificial neural networks for virtual hand prosthesis control. In: Conference Proceedings: Annual International Conference of the IEEE Engineering in Medicine and Biology Society. IEEE Engineering in Medicine and Biology Society Annual Conference. 2011;2011:7254–7.Search in Google Scholar
[13] Salminger S, Roche AD, Hruby LA, Sturma A, Riedl O, Bergmeister KD, et al. Prosthetic reconstruction to restore function in transcarpal amputees. J Plast Reconstr Aesthet Surg 2016;69:305–10.10.1016/j.bjps.2015.10.029Search in Google Scholar PubMed
[14] Farina D, Aszmann O. Bionic limbs: clinical reality and academic promises. Sci Transl Med 2014;6:257ps12.10.1126/scitranslmed.3010453Search in Google Scholar PubMed
[15] Cheesborough JE, Smith LH, Kuiken TA, Dumanian GA. Targeted muscle reinnervation and advanced prosthetic arms. Semin Plast Surg 2015;29:62–72.10.1055/s-0035-1544166Search in Google Scholar PubMed
[16] Campbell DA, Kay SPJ. The hand injury severity scoring system. J Hand Surg Br Eur Vol 1996;21:295–8.10.1016/S0266-7681(05)80187-1Search in Google Scholar
[17] Saxena P, Cutler L, Feldberg L. Assessment of the severity of hand injuries using ‘hand injury severity score’, and its correlation with the functional outcome. Injury 2004;35:511–6.10.1016/S0020-1383(03)00211-0Search in Google Scholar
[18] Matsuzaki H, Narisawa H, Miwa H, Toishi S. Predicting functional recovery and return to work after mutilating hand injuries: usefulness of Campbell’s Hand Injury Severity Score. J Hand Surg Am 2009;34:880–5.10.1016/j.jhsa.2009.02.009Search in Google Scholar PubMed
[19] Stanger K, Horch RE, Dragu A. Severe mutilating injuries with complex macroamputations of the upper extremity – is it worth the effort? World J Emerg Surg 2015;10:30.10.1186/s13017-015-0025-6Search in Google Scholar PubMed PubMed Central
[20] Sugun TS, Ozaksar K, Ada S, Kul F, Ozerkan F, Kaplan I, et al. [Long-term results of major upper extremity replantations]. Acta Orthop Traumatol Turc 2009;43:206–13.10.3944/AOTT.2009.206Search in Google Scholar PubMed
[21] Gulgonen A, Ozer K. Long-term results of major upper extremity replantations. J Hand Surg Eur Vol 2012;37:225–32.10.1177/1753193411427228Search in Google Scholar PubMed
[22] Lotze M, Grodd W, Birbaumer N, Erb M, Huse E, Flor H. Does use of a myoelectric prosthesis prevent cortical reorganization and phantom limb pain? Nat Neurosci 1999;2:501–2.10.1038/9145Search in Google Scholar PubMed
[23] Robinson LS, Sarkies M, Brown T, O’Brien L. Direct, indirect and intangible costs of acute hand and wrist injuries: a systematic review. Injury 2016;47:2614–26.10.1016/j.injury.2016.09.041Search in Google Scholar PubMed
[24] de Putter CE, van Beeck EF, Polinder S, Panneman MJ, Burdorf A, Hovius SE, et al. Healthcare costs and productivity costs of hand and wrist injuries by external cause: a population-based study in working-age adults in the period 2008–12. Injury 2016;47:1478–82.10.1016/j.injury.2016.04.041Search in Google Scholar PubMed
[25] McFarland LV, Hubbard Winkler SL, Heinemann AW, Jones M, Esquenazi A. Unilateral upper-limb loss: satisfaction and prosthetic-device use in veterans and service members from Vietnam and OIF/OEF conflicts. J Rehabil Res Dev 2010;47:299–316.10.1682/JRRD.2009.03.0027Search in Google Scholar
[26] Pezzin LE, Dillingham TR, Mackenzie EJ, Ephraim P, Rossbach P. Use and satisfaction with prosthetic limb devices and related services. Arch Phys Med Rehabil 2004;85:723–9.10.1016/j.apmr.2003.06.002Search in Google Scholar PubMed
[27] Hu J, Jiang Y, Liang Y, Yu IT, Leng H, He Y. Predictors of return to work and duration of absence following work-related hand injury. Int J Injury Contr Saf Promot 2014;21:216–23.10.1080/17457300.2013.792280Search in Google Scholar PubMed
[28] Ramel E, Rosberg HE, Dahlin LB, Cederlund RI. Return to work after a serious hand injury. Work 2013;44:459–69.10.3233/WOR-2012-1373Search in Google Scholar PubMed
[29] Engel GL. The need for a new medical model: a challenge for biomedicine. Science 1977;196:129–36.10.1126/science.847460Search in Google Scholar PubMed
[30] Muridan N, Chappell PH, Cranny A, White NM. Texture sensor for a prosthetic hand. Proc Eng 2010;5:605–8.10.1016/j.proeng.2010.09.182Search in Google Scholar
[31] Raspopovic S, Capogrosso M, Petrini FM, Bonizzato M, Rigosa J, Di Pino G, et al. Restoring natural sensory feedback in real-time bidirectional hand prostheses. Sci Transl Med 2014;6:222ra19.10.1126/scitranslmed.3006820Search in Google Scholar PubMed
[32] Tan DW, Schiefer MA, Keith MW, Anderson JR, Tyler J, Tyler DJ. A neural interface provides long-term stable natural touch perception. Sci Transl Med 2014;6:257ra138.10.1126/scitranslmed.3008669Search in Google Scholar PubMed PubMed Central
[33] Ortiz-Catalan M, Hakansson B, Branemark R. An osseointegrated human-machine gateway for long-term sensory feedback and motor control of artificial limbs. Sci Transl Med 2014;6:257re6.10.1126/scitranslmed.3008933Search in Google Scholar PubMed
[34] Collinger JL, Wodlinger B, Downey JE, Wang W, Tyler-Kabara EC, Weber DJ, et al. High-performance neuroprosthetic control by an individual with tetraplegia. Lancet 2013;381:557–64.10.1016/S0140-6736(12)61816-9Search in Google Scholar PubMed
[35] Hutchinson DT. The quest for the bionic arm. J Am Acad Orthop Surg 2014;22:346–51.10.5435/JAAOS-22-06-346Search in Google Scholar PubMed
Supplementary Material:
The article (https://doi.org/10.1515/iss-2018-0002) offers reviewer assessments as supplementary material.
©2018 Alawi S.A., et al., published by De Gruyter, Berlin/Boston
This work is licensed under the Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 License.
Articles in the same Issue
- Highlight: Basic Research in Pediatric Surgery
- Editorial
- Basic research in pediatric surgery
- Reviews
- Animal models of necrotizing enterocolitis: review of the literature and state of the art
- Recent developments in cell-based ENS regeneration – a short review
- Role of viruses in biliary atresia: news from mice and men
- Tissue engineering in pediatric urology – a critical appraisal
- Resorbable implants in pediatric fracture treatment
- General Research
- Review
- First-line molecular therapies in the treatment of metastatic colorectal cancer – a literature-based review of phases II and III trials
- Original Articles
- Effect of cryopreservation on lymph node fragment regeneration after autologous transplantation in the minipig model
- Quality of life and reconstructive surgery efforts in severe hand injuries
- Case Report
- IgG4-related sclerosing cholangitis mimicking hilar cholangiocarcinoma (Klatskin tumor): a case report of a challenging disease and review of the literature
Articles in the same Issue
- Highlight: Basic Research in Pediatric Surgery
- Editorial
- Basic research in pediatric surgery
- Reviews
- Animal models of necrotizing enterocolitis: review of the literature and state of the art
- Recent developments in cell-based ENS regeneration – a short review
- Role of viruses in biliary atresia: news from mice and men
- Tissue engineering in pediatric urology – a critical appraisal
- Resorbable implants in pediatric fracture treatment
- General Research
- Review
- First-line molecular therapies in the treatment of metastatic colorectal cancer – a literature-based review of phases II and III trials
- Original Articles
- Effect of cryopreservation on lymph node fragment regeneration after autologous transplantation in the minipig model
- Quality of life and reconstructive surgery efforts in severe hand injuries
- Case Report
- IgG4-related sclerosing cholangitis mimicking hilar cholangiocarcinoma (Klatskin tumor): a case report of a challenging disease and review of the literature