A multivariate Bayesian learning approach for improved detection of doping in athletes using urinary steroid profiles
-
Dimitra Eleftheriou

 ,
Thomas Piper
,
Thomas Piper

Abstract
Biomarker analysis of athletes’ urinary steroid profiles is crucial for the success of anti-doping efforts. Current statistical analysis methods generate personalised limits for each athlete based on univariate modelling of longitudinal biomarker values from the urinary steroid profile. However, simultaneous modelling of multiple biomarkers has the potential to further enhance abnormality detection. In this study, we propose a multivariate Bayesian adaptive model for longitudinal data analysis, which extends the established single-biomarker model in forensic toxicology. The proposed approach employs Markov chain Monte Carlo sampling methods and addresses the scarcity of confirmed abnormal values through a one-class classification algorithm. By adapting decision boundaries as new measurements are obtained, the model provides robust and personalised detection thresholds for each athlete. We tested the proposed approach on a database of 229 athletes, which includes longitudinal steroid profiles containing samples classified as normal, atypical, or confirmed abnormal. Our results demonstrate improved detection performance, highlighting the potential value of a multivariate approach in doping detection.
1 Introduction
Doping has been widely discussed in recent years and remains a challenging topic in the athletic world. In competitive sports, prohibited substances such as anabolic androgenic steroids (AAS), refer to the drugs that are closely associated with the notion of doping [1]. AAS are the most frequent detected class of substances in doping controls [2]. In order to detect the administration of endogenous steroids, i.e. steroids that are produced inside the body such as testosterone, the steroidal module of the Athlete Biological Passport (ABP) was developed [3]. The steroidal module is used to denote a follow-up which is the recording of the concentration of endogenous steroids and their ratios in urine over time. In order to establish the ABP, the World Anti-Doping Agency (WADA) provided harmonised and robust analytical methods for the “steroid profile” which according to their technical document (TD) [4] is composed of the following endogenous anabolic androgenic steroids (EAAS): testosterone (T), epitestosterone (E), androsterone (A), etiocholanolone (Etio), 5α-androstane-3α, 17β-diol (A5), 5β-androstane-3α, 17β-diol (B5), as well as the concentration ratios T/E, A/T, A/Etio, A5/B5 and A5/E (see Table B.1 in the Supplementary Material). As the intra-individual variation of all these markers is much lower than the inter-individual variation in the population of athletes, individual longitudinal monitoring as applied by the ABP increases the sensitivity for the detection of illicit AAS administration. For each athlete an individual reference range is specified for each biomarker as samples are added to the ABP over time. If a new steroid profile enters into the individual ABP and values fall beyond established thresholds, the ABP alerts athlete passport management units (APMUs) that anomalies have been detected that require closer examination [3], [5], [6], [7]. Employing this approach, the ABP mostly aids in revealing the direct and indirect effects of doping with anabolic agents on the individual steroid profile rather than detecting the prohibited substance itself [8], [9]. Therefore, further steps during the closer examination encompass steroid profile confirmation, detection of confounding factors and isotope ratio mass spectrometry (IRMS) based investigations.
By far the most commonly used screening tool in sports drug testing over the last years uses the T/E ratio, as it is considered a stable marker ratio within an athlete’s steroid profile, sensitive to the administration of T itself and T-prohormones [10]. Measuring only the urinary T concentrations has proved inadequate due to the small ratio of intra- to inter-individual variability in the urinary steroid concentrations caused by various factors [10], [11], [12], [13], [14]. Therefore, monitoring the steroid profile at individual level is critical, mostly because the reference values based on the population do not always have the sensitivity to track whether anabolic drugs have been administered [15], [16]. Current approaches receive new measurements of a single biomarker or ratio and, under a Bayesian framework, progressively adapt population-derived limits (when there are no recorded measurements) to individual normal ranges as the number of measurements increases [17]. Multivariate statistical approaches have also been proposed for this purpose, combining population-level information with individual longitudinal monitoring of multiple biomarkers [18], [19], [20]. However, multivariate statistical methods in a Bayesian adaptive framework for analysing urinary steroid profiles have not yet been attempted.
This research focuses on the development of an improved statistical model for classifying each measurement of athletes’ urine samples into suspicious and non-suspicious classes. The classification technique is based on comparisons of sequential measurements of a set of biological variables against previous recordings. For this purpose, we move from the univariate to a multivariate statistical model which considers prior information on inter- and intra-individual variations, and on potential correlation between the EAAS markers. By developing such a multivariate mixed-effects Bayesian model, we aim to leverage three key advantages: (a) incorporating prior knowledge (i.e. historical data from normal steroidal profiles), (b) analysing multiple variables (biomarkers and/or ratios), and (c) handling repeated measurements over time. Multivariate mixed-effects modelling has been used across various applications [21], [22], [23]. A fully validated method using GC-MS analysis and fulfilling all requirements as per TD EAAS [4], [10] determined the six markers and the five ratios which compose the urinary steroid profile of the ABP of 229 athletes. Out of them, 100 were athletes whose samples are considered to be normal (i.e. none of their samples was found beyond the individual limits), 100 were athletes with one or more extreme samples classified as atypical (i.e. samples beyond the individual limits but in none of these a doping offence was detectable), and 29 confirmed dopers, each marked with at least one atypical sample in their longitudinal steroid profile and confirmed to be a real doping offence employing IRMS according to WADA regulation [24]. The latter samples are classified as abnormal. These EAAS concentrations were longitudinally sampled from professional athletes, whereas cross-sectional measurements of the same markers and ratios from a separate baseline population of 164 healthy and non-doped volunteers were used to extract prior information for the normal range of steroid concentrations. It is worth noting that recordings from athletes with normal concentration values are more readily available than from doped athletes. Since the imbalance in size between the two classes is unavoidable, traditional classification methods may not work effectively as they are biased towards the predominant class. Hence, we classify athletes’ samples based on a one-class classification algorithm. The AAS concentrations from non-doped athletes define the “target” class for which adaptive decision boundaries are constructed to separate them from suspicious data points, recognised as outliers or anomalies.
The remaining sections are structured as follows. In Section 2 we introduce the univariate and the multivariate Bayesian adaptive models. The former can be applied to individual biomarkers or ratios within the steroid profile, whereas the latter is proposed as it is specifically engineered to analyse multiple biomarkers and/or ratios simultaneously. Section 3 describes the one-class classification method using the highest posterior predictive density (HPD). In Section 4 we present summaries of real athletes’ data and the 95 % HPD estimation on both models. The inference and computations in the analysis relied on either sampling from a known joint posterior distribution or sampling from a non-closed form distribution employing Markov chain Monte Carlo (MCMC) methods, depending on the model being used. The computer code for the developed models is written in the statistical language R 4.2.2 [25]. We compare the two models with each other but also assess them against a generalised linear mixed effects model (GLMM) and the univariate Bayesian approach introduced by Sottas et al. [17], exclusively designed for the analysis of the T/E ratio. Furthermore, we conduct a comparison with the univariate Bayesian model applied to the Euclidean distance score as outlined in the work of De Figueiredo et al. [26]. Section 5 discusses the main findings and directions for further research.
2 Models
2.1 The univariate Bayesian model
In this section we introduce an expanded version of the univariate Bayesian model for the T/E ratio proposed by Sottas et al. [17] to a univariate Bayesian hierarchical model for any steroidal component or ratio of the ABP. Under a Bayesian framework, the model receives new measurements and progressively adapts population-derived limits, when the number of measurements n is zero, to individual normal ranges, when n is large.
Let y = (y 1, …, y n ) represent the vector with the n log-transformed recorded values of the biomarker Y collected from the same athlete. It is important to mention that the period among two sequential samples of an athlete is long enough for them to be considered independent, a standard assumption also employed in the ABP approach. Hence, we assume the logarithm of EAAS values to be a vector of n independent and identically distributed draws from a Gaussian distribution with mean μ and variance σ 2, that is
We focus on modelling the logarithm of these EAAS concentrations due to the fact that there are physical constraints on the measurement values (i.e. all markers are positive) and taking the logarithm allows us to use the Gaussian distribution in our models. To describe prior knowledge about the unknown parameters, i.e. the mean μ and the precision τ = 1/σ 2, we specify the joint prior distribution as the product of a conditional and a marginal distribution expressed as p(μ, τ) = p(μ|τ)p(τ). Given our limited prior information on the parameters of the model regarding the six available biomarkers and their five ratios with the exception of the T/E ratio, we propose specifying weakly informative conditionally conjugate priors on these model parameters. Therefore, a Gaussian distribution is assigned to the mean conditional on the precision as
with hyper-parameters μ 0 (prior mean) and κ 0 (prior sample size, which determines the tightness of the prior). The inverse of the variance is assumed to follow a conjugate Gamma prior distribution expressed as
where α 0 and β 0 determine the shape and rate hyper-parameters, respectively. The T/E ratio is excluded from the semi-informative prior setting because there is adequate population information regarding its characteristics given by Sottas et al. [17]. However, we present the analysis results of T/E using both informative and weakly informative priors for comparison purposes. As a conjugate family, the joint posterior distribution for the pair of parameters (μ, τ) is also a Gaussian-Gamma distribution, a combination of a Gaussian distribution for the mean parameter μ and a Gamma distribution for the precision parameter τ, denoted as
where the index n on the hyper-parameters indicates the updated values after seeing the n observations from the sample data, that is
2.2 Proposed multivariate Bayesian adaptive model
In Sottas et al. [17], the T/E marker is modelled by a univariate Gaussian distribution in a Bayesian context. In this section, we present a multivariate Bayesian adaptive model (MBA), which can deal with a wide variety of markers in their logarithmic scale as a generalisation of the univariate model of Ref. [17]. The MBA is expressed as
where y
ijk
denotes the logarithm of the ith observation of the kth marker for the jth athlete, μ
k
is the fixed effect for the overall mean of all observations of kth response marker, b
jk
is the random effect of athlete j for the kth marker, and e
ijk
is the random term for other variation in its ith measurement, while i = 1, …, n
j
, j = 1, …, J and k = 1, …, K. The assumptions here are that for a certain marker k, the random effects b
jk
are independent, identically and normally distributed between subjects and the error terms e
ijk
are also independent, identically and normally distributed between and within subjects. Shorthand notation for the overall mean is
where the overall mean
μ
and the random effects
μ
j
have conjugate multivariate Gaussian priors, while the precision matrices Ω
e
, Ω
μ
and Ω
b
have conjugate Wishart priors. Historical prior information about all response variables is captured by the prior mean vector
μ
0
. Moreover, d
e
, d
μ
and d
b
denote the degrees of freedom, and S
e
, S
μ
and S
b
are the prior covariance matrices which are selected such that their corresponding prior distributions will be non-informative. The degrees of freedom of the Wishart distribution need to be greater than the data dimension minus one, i.e. d
e
> K − 1, so a non-informative value for this parameter is chosen to be equal to K [27]. The prior covariance matrices S
e
, S
μ
and S
b
are all set equal to
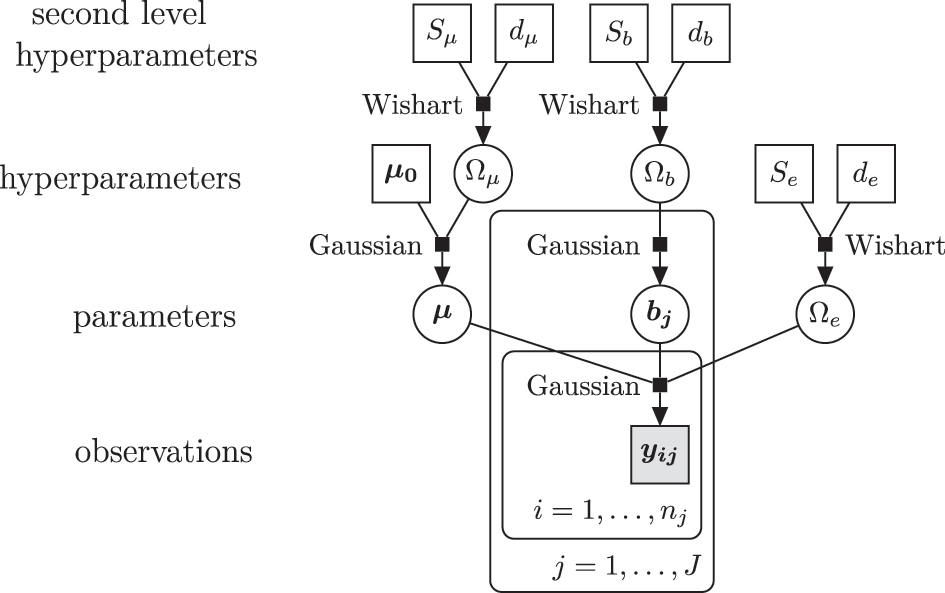
A graphical representation of the MBA with conjugate priors. The overall mean, μ , and the precision matrix, Ω e , are assumed to be independent.
We approximate the posterior parameters by using Gibbs sampling [28], [29]. To apply the Gibbs sampler (see Algorithm 1), the full conditional posterior distributions for each of the unknown parameters of
where in this section y is an n j × J × K data matrix and
Algorithm 1.
Gibbs algorithm
|
Precondition: Generate an initial state
|
| 1: for t ← 1 to T do |
| 2: draw
|
| 3: for j ← 1 to J do |
| 4: draw
|
| 5: end for |
| 6: draw
|
| 7: draw
|
| 8: draw
|
| 9: end for |
3 Methodology
3.1 One-class classification
One-class classification (OCC) algorithms are used in classification when only one class, called the “target” class, is fully known and the others are either absent or poorly sampled [30], [31], [32]. Doping detection constitutes a challenging topic in forensic toxicology, as standard binary classification procedures, such as the Naive Bayes classifier, are unsuitable due to the severe class imbalance. Consequently, doping detection can be framed as a one-class classification problem since measurements from doped athletes can be difficult to obtain, either due to the elaborated techniques that athletes use to avoid testing, or due to the undetectable use of banned substances.
For doping analysis, full information is provided on non-doped athletes who have been voluntarily tested, but limited knowledge is available for athletes who have received doping regimens. Thus, the samples from athletes with normal concentration values are treated as the “target” class. The focus is on studying whether there is evidence that new samples from athletes, whose doping status is unknown, are compatible with the known normal class of samples, or whether they show an abnormal pattern and should be considered as outliers. A classifier, that is a function which assigns each input data point to a class, accounting for other confounding factors such as sex, cannot be constructed with known standard rules in the case of imbalanced classes. In a machine learning context, the main purpose is to infer a classifier from a limited set of training data noting that, in addition to the complexity of unbalanced data, the classifier should also have the capability to deal with longitudinal data, their updating nature as well as potential confounders. We approach the one-class classification problem using a density estimation method applied to the multivariate Bayesian adaptive model introduced in Section 2.2. This model is trained exclusively on the majority class; i.e. normal values from non-doped athletes, as described in the following section.
3.2 Highest posterior predictive density
The Bayesian model specification contributes to hierarchically shift from the prior evidence about population parameters θ to the revised knowledge, expressed in the posterior density p( θ | y ), as new data become available. Using MCMC sampling methods, we can estimate the posterior density function and then approximate the K-variate predictive density function of a 1 × K new observable vector y n+1 given the data y of dimensionality n j′ × J′ × K, where J′ = J + 1. Therefore, the predictive density function is calculated as
which is formed by weighting the possible values of
θ
in the future observation f(
y
n+1
|
θ
) by how likely we believe they are to occur, p(
θ
|
y
). Note that
y
consists of both data from the baseline longitudinal population,
where γ is the largest constant such that Pr(
Y
n+1
∈ C
α
|
y
) ≥ 1 − α [33], which serves as the criterion for classifying new recordings. A new test result
y
n+1
is considered to be an outlier if, for at least one biomarker k, the corresponding observable
Based on the decision rule in (9) the lower and upper limits of the HPD are obtained, which define the most credible normal boundaries of future EAAS concentrations or ratios. HPD intervals are robust to the shape of the posterior distribution and are not affected by outliers or skewness. These sample-specific boundaries can be used in detecting potential steroid misuse that may cause abnormally high or low concentration values of biomarkers or ratios, as well as in revealing urine sample replacement or the impact of other confounding factors. It is worth mentioning that there is the usual trade-off in choosing an appropriate α, since lower α values give wider intervals. High α values give narrower intervals implying that an extreme new measurement has a low probability of lying in the interval. Furthermore, note that testing the first measurement of a new athlete is based only on the population thresholds, since n = 0. Population thresholds are presented in Table B.6 of the Supplementary Material and were obtained by Van Renterghem et al. [16]. Further information about population thresholds was derived by Rauth [34] and Kicman et al. [35].
3.3 Continuity assumption
In this one-class classification process, we assume that the continuity assumption holds. This is a general assumption in pattern recognition, according to which points that are close to each other are more likely to share a label. For this purpose, when the model suggests an outlier, then this observation is automatically excluded from the set of recordings that are used to compute the HPD intervals for normal samples. If we do not discard the observations flagged up as outliers, we should expect to learn the noise, and any noise measurements which are considered as normal measurements have a significant impact on the personalised accepted limits. Hence, we cannot expect to infer a good classification in such a case.
4 Results
4.1 Data summary
The proposed method was applied to athletes’ longitudinal steroid profile data extracted from their ABP. The datasets have been collected by following all the appropriate ethical approval procedures. Individual steroid profiles were analysed according to established methods including gas chromatography-mass spectrometry (GC-MS). Figure 2 represents a real GC-MS multiple reaction monitoring chromatogram produced by an unsuspicious urine sample. The longitudinal dataset includes six endogenous androgenic steroid concentrations and five concentration ratios proposed by WADA (i.e. T, E, A, Etio, A5, B5, T/E, A/T, A/Etio, A5/B5 and A5/E), which were repeatedly collected from each athlete in or out-of-competition.
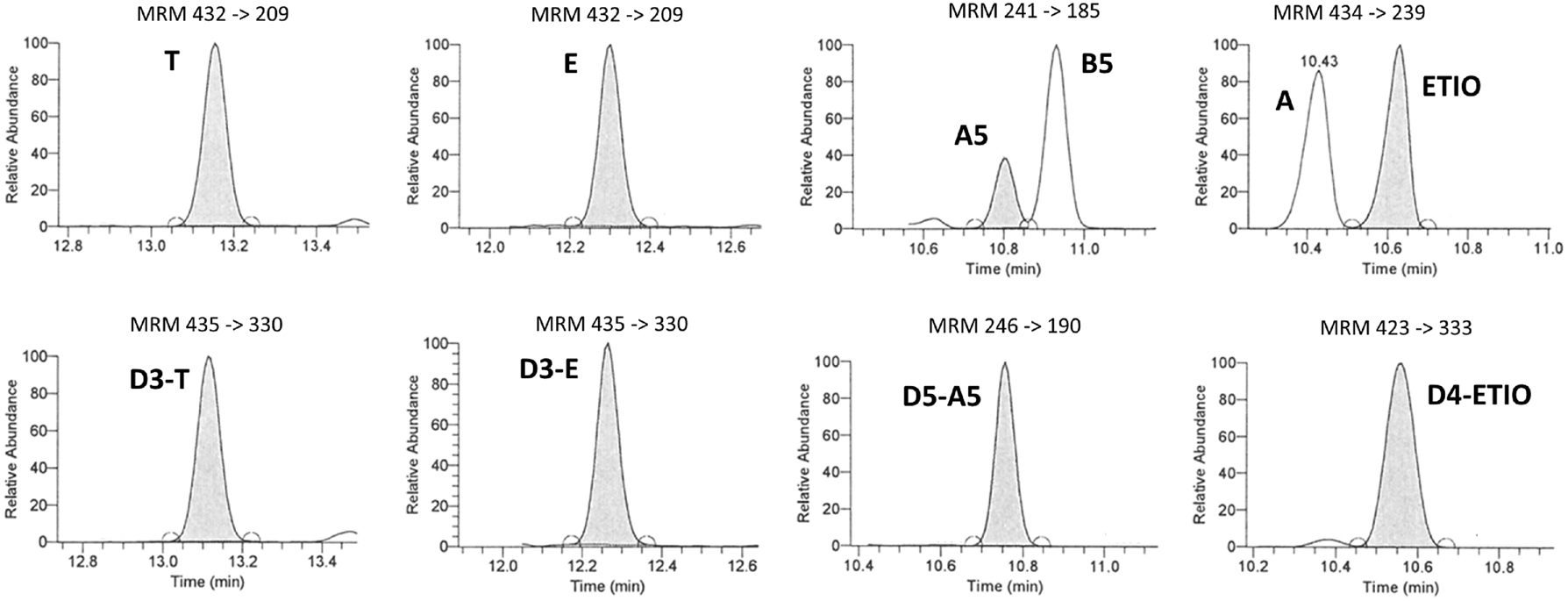
Extracted chromatograms obtained for an unsuspicious urine sample. Shown are the multiple reaction monitoring (MRM) ion transitions employed for the quantification of endogenous steroids (upper part) and their deuterated analogues (lower part).
A total of 1,433 normal urine samples were obtained from 100 athletes (50 males and 50 females), 2,504 samples were obtained from 100 athletes (50 males and 50 females) whose longitudinal steroid profiles contain values classified as atypical, and 462 samples from 29 athletes (15 males and 14 females) with at least one confirmed abnormal value in their steroid profile (Table 1), employing IRMS in line with WADA regulation [24]. Figure A.1 in the Supplementary Material shows that there is severe imbalance between normal (grey) and non-normal (black) samples with the former specifying the majority class. Specifically, out of 4,399 urine samples across all athletes, only 327 (7.43 %) were non-normal values (275 from athletes with atypical samples, and 52 from athletes with abnormal samples). Sample calibration was carried out prior to the analysis according to the estimated real limits of the applied methodology. Limit of detection (LOD) values and limit of quantification (LOQ) values within the steroid profiles of the athletes have been replaced by commonly accepted minimum cut-off values for all markers; i.e. all
Summary of urine samples collected from athletes in the longitudinal dataset. Of the total 4,399 samples, 1,433 samples from 100 normal athletes were used to train the MBA model, while the remaining 2,966 samples from non-normal athletes were utilized as a test set.
| Athletes class | Normal | Non-normal | |||
| Dopers class | Non-dopers (N = 100) | Non-confirmed (N = 100) | Confirmed (N = 29) | ||
| Sample class | Normal | Normal | Atypical | Normal | Abnormal |
| Urine samples, n | 1,433 | 2,229 | 275 | 410 | 52 |
Furthermore, single EAAS and ratio measurements of 164 healthy individuals have been provided as part of a separate cross-sectional study, representing a baseline population of which 91 were men and 73 women of age between 18 and 54 [19]. Figure A.2 in the Supplementary Material presents the scatter and density plots for men (black) and women (grey) for all available markers and ratios. The concentrations of markers seem to be slightly separable between men and women. However, this does not apply to the ratios, where the distributions of both sexes seem similar, except for the A/T ratio. The correlation between the various markers and ratios shows that plain markers are more highly correlated compared to the ratios (Figure A.2).
Tables B.2–B.5 in the Supplementary Material summarise the statistics (minimum, 1st quartile; Q1 and 3rd quartile; Q3, mean, median, maximum EAAS values and standard deviation) of the baseline cross-sectional population and the longitudinally-monitored athletes. The boxplots of the mean values of the available longitudinal metabolites and ratios are reported in Figure 3. When available, the WADA limits (lower and/or upper) are denoted by the solid lines based on Table B.6 of the Supplementary Material. Androsterone and Etiocholanolone share the same population thresholds among females and males. When population-specific information is unavailable for certain ratios, the Q3 values derived from the cross-sectional dataset are used as initial population thresholds for the respective ratios.
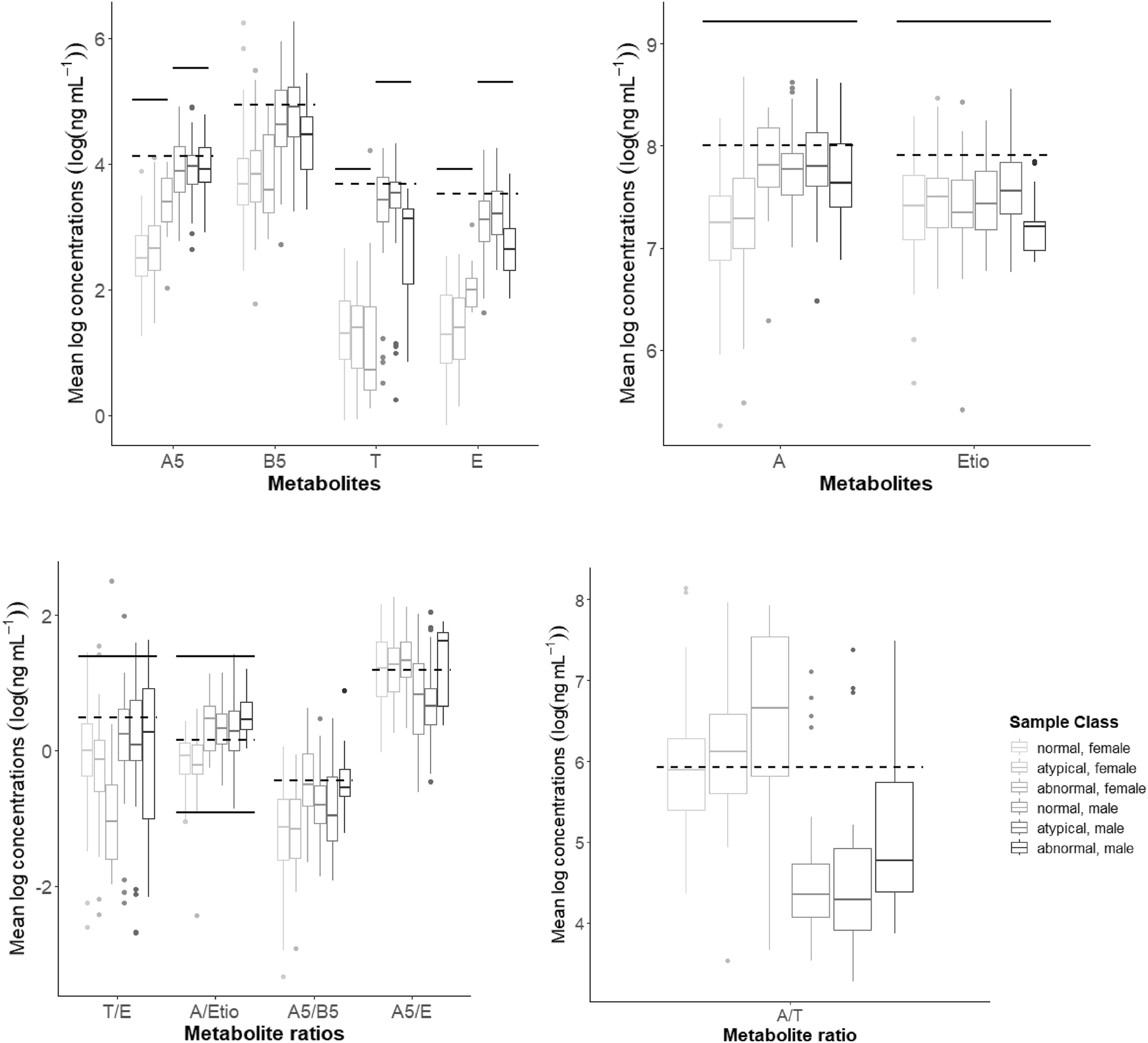
Boxplots for the mean logarithmic values of the metabolite concentrations (ng mL−1) and their ratios from the longitudinal steroid profiles of the 229 athletes by sex and sample class. WADA log-limits are denoted by the solid lines. Dashed lines represent the mean log-concentrations of the metabolites obtained from the baseline cross-sectional population.
4.2 Estimation of highest posterior predictive density
4.2.1 Univariate HPD estimation
Here we fit the univariate Bayesian model to each athlete and each biomarker in the ABP separately. To implement the model, we initially specified the prior distributions for the model parameters as described in Equations (2) and (3). While the correlation between the empirical mean and precision of log-transformed concentration values across all markers was relatively weak, ranging from −0.33 to 0.32, we consider a prior dependency between the parameters μ and τ. We set the hyperparameters κ
0 = 1, α
0 = 10, and β
0 = 1, while we control for possible confounding due to sex differences by setting
where n ≥ 0, and (μ (t), τ (t)) is the parameter pair of the tth draw obtained through the sampler with total number of iterations T = 5,000. In practice, the integration averaging is performed using an empirical average based on samples from the posterior distribution. At first, we simulate replicates of new data, y n+1, from the posterior predictive distribution. Then we derive the 95 % HPD interval, using it as a criterion to classify a real data point as either a normal value or an outlier. Unlike the multivariate mixed-effects model in Section 2.2, this model cannot be applied to longitudinal data. Therefore, the available baseline longitudinal population cannot serve as a training set in this case. The univariate model constitutes an unsupervised learning approach, where the sample class is considered unknown. However, in our dataset, the true class for each of the 4,399 EAAS concentrations and ratios of 229 athletes is known, allowing us to estimate the predictive accuracy of the method.
In Figure 4, the A5 and T/E series of a doped athlete are depicted with the blue-solid lines. The red dotted lines are the 95 % HPD intervals of the predictive distribution, which serve as the posterior normal boundaries at each specific time point. Before observing any data, the upper limits are defined by WADA’s population thresholds, when they are available (see Table B.6 in the Supplementary Material). For marker B5, we used the maximum value obtained by the Caucasian population in Van Renterghem et al. [16], while for the remaining ratios (A5/B5, A5/E and A/T) we chose the Q3 values 4, 10 and 10,000, respectively, as reasonable starting thresholds derived from the cross-sectional dataset. The purple dashed lines indicate the usual Z-score upper limits as presented in Sottas et al. [17]. The gold diamonds symbolise the abnormal values in the athlete’s profile, which the model considers as suspicious values that need further investigation. For the T/E ratio in Figure 4(b), there are two additional green dashed-dotted lines that indicate the upper and lower limits of the T/E model with informative priors introduced by Sottas et al. [17]. For example, in Figure 4(a), there are two androsterone samples which are higher than the upper limits, and in Figure 4(b), Sottas’ model identifies four abnormal T/E tests, out of which three are in common with those suggested by the general univariate model.
![Figure 4:
A series of 29 longitudinal values of (a) A5 and (b) T/E (blue solid-dotted line) obtained from a doped athlete; the upper and lower limits (red dotted lines) are the 95 % HPD intervals from the univariate Bayesian model; upper limits based on a usual Z-score (purple dashed line); abnormal values are marked with gold diamonds. For (b), upper and lower limits (green dashed-dotted lines) are the 95 % HPD interval from the T/E model of Sottas et al. [17], with its suggested abnormal values indicated by green stars.](/document/doi/10.1515/ijb-2024-0019/asset/graphic/j_ijb-2024-0019_fig_004.jpg)
A series of 29 longitudinal values of (a) A5 and (b) T/E (blue solid-dotted line) obtained from a doped athlete; the upper and lower limits (red dotted lines) are the 95 % HPD intervals from the univariate Bayesian model; upper limits based on a usual Z-score (purple dashed line); abnormal values are marked with gold diamonds. For (b), upper and lower limits (green dashed-dotted lines) are the 95 % HPD interval from the T/E model of Sottas et al. [17], with its suggested abnormal values indicated by green stars.
Figure A.3(a)–(k) in the Supplementary Material displays the series of the six EAAS along with their five corresponding ratios for the same athlete. Given that the 21st, 22nd and 23rd sample tests of that athlete are confirmed as abnormal, only E, T/E and A5/E were sensitive enough to detect these anomalies within the athlete’s steroid profile. Note that if the model suggests a sample as an outlier, we automatically exclude it from the set of recordings which are used to compute the HPD intervals, because it might have an impact on the validity of the following personalised normal limits.
4.2.2 Multivariate HPD estimation
To apply the multivariate Bayesian adaptive model, we initially specified the prior distributions for the model parameters
We first simulate from the posterior predictive distribution many replicates of the new data, y n+1 , and thus we derive the 95 % HPD interval to classify a real data point into either a normal value or an outlier. Data from athletes with exclusively normal samples were used for model training (i.e. the 1,433 samples from the baseline longitudinal population of 100 athletes), whereas normal, atypical and abnormal samples from the 129 non-normal athletes comprised the test set (Table 1). The concept behind this one-class classification approach is to train the model exclusively using normal data from non-doped athletes, by estimating p( θ normal| y normal), and then evaluating the likelihood of a future unlabelled observation to be generated by this model. Multiple parameters were estimated via the Gibbs sampler for this model. Due to their large number, we provide a selection of diagnostic plots to evaluate MCMC convergence in Chapter 3 of the PhD thesis by Eleftheriou [36]. The complete set of diagnostic plots are available in the supplementary folder titled “Diagnostics” on GitHub.
4.3 Classification performance
In forensic toxicology, high specificity is important, thus a very low false positive rate is required in order to prevent the accusation of an innocent athlete. However, classification accuracy values and measures regarding the majority class such as the overall accuracy, tend to be pretty high because they are computed under the assumption of balanced class distributions. Consequently, we use appropriate metrics for evaluating the classification performance of the models which can deal with the imbalance of the dataset, such as the F1 score and G-mean (Geometric mean) defined as
and
Tables 2 and 3 present the classification performance of the univariate model and the MBA model in comparison with the univariate T/E model proposed by Sottas et al. [17], the univariate Euclidean distance (ED) score model of De Figueiredo et al. [26] and a generalised linear mixed-effects model (GLMM) using a false positive rate α = 0.05. The GLMM model is implemented via the glmer() function from the lme4 package in R [37] to fit a mixed effects logistic regression model with a binomial distribution for the response variable “Class ij ”, which is a binary variable that represents the class of each observation i of athlete j including the biomarkers and/or ratios as individual level continuous predictors, and a random intercept by athlete ID. The problem of unreliable overall accuracy in binary class classification with imbalanced data through the GLMM has been alleviated by the application of oversampling, as evidenced by the now equivalent values of balanced accuracy and overall accuracy (see Table 3).
Predictive performance of univariate and multivariate models trained on longitudinal profiles of 100 non-doped athletes and tested on profiles from the remaining 129 athletes, evaluated based on the 95 % HPD interval.
| Classification model | Variable | G-mean | F 1 | Precision | Sensitivity | Specificity | Balanced | Overall |
|---|---|---|---|---|---|---|---|---|
| accuracy | accuracy (95 % CI) | |||||||
| Univariate | A5 | 0.46 | 0.15 | 0.11 | 0.25 | 0.84 | 0.55 | 0.80 (0.79, 0.81) |
| B5 | 0.50 | 0.17 | 0.12 | 0.30 | 0.83 | 0.56 | 0.79 (0.78, 0.80) | |
| A | 0.38 | 0.13 | 0.11 | 0.17 | 0.86 | 0.53 | 0.83 (0.82, 0.84) | |
| ETIO | 0.38 | 0.12 | 0.10 | 0.16 | 0.89 | 0.52 | 0.84 (0.82, 0.85) | |
| T | 0.50 | 0.18 | 0.13 | 0.30 | 0.83 | 0.57 | 0.79 (0.78, 0.81) | |
| E | 0.52 | 0.17 | 0.11 | 0.34 | 0.78 | 0.56 | 0.75 (0.73, 0.76) | |
| T/E a | 0.48 | 0.19 | 0.15 | 0.26 | 0.88 | 0.57 | 0.84 (0.82, 0.85) | |
| A/ETIO | 0.41 | 0.24 | 0.39 | 0.17 | 0.98 | 0.58 | 0.92 (0.91, 0.93) | |
| A/T | 0.39 | 0.15 | 0.13 | 0.17 | 0.91 | 0.54 | 0.86 (0.85, 0.87) | |
| A5/B5 | 0.47 | 0.18 | 0.14 | 0.25 | 0.88 | 0.57 | 0.84 (0.82, 0.85) | |
| A5/E | 0.55 | 0.23 | 0.17 | 0.35 | 0.86 | 0.61 | 0.82 (0.81, 0.83) | |
| Sottas et al. [17] | T/E b | 0.52 | 0.20 | 0.15 | 0.32 | 0.85 | 0.59 | 0.81 (0.80, 0.82) |
| MBA | EAAS | 0.55 | 0.24 | 0.18 | 0.38 | 0.78 | 0.58 | 0.74 (0.72, 0.75) |
| Ratios | 0.62 | 0.35 | 0.29 | 0.44 | 0.87 | 0.65 | 0.82 (0.80, 0.83) | |
| All | 0.63 | 0.30 | 0.20 | 0.55 | 0.73 | 0.64 | 0.71 (0.70, 0.73) | |
| Univariate ED score | EAAS | 0.22 | 0.20 | 0.11 | 0.98 | 0.05 | 0.52 | 0.15 (0.14, 0.17) |
| Ratios | 0.22 | 0.20 | 0.11 | 0.99 | 0.05 | 0.52 | 0.15 (0.14, 0.16) | |
| All | 0.20 | 0.20 | 0.11 | 0.99 | 0.04 | 0.52 | 0.15 (0.14, 0.16) |
-
aThis model specifies weakly informative priors. bFor Sottas’ model the priors are set to be strongly informative. Metrics used are defined as Precision =
Predictive performance of univariate and multivariate models trained and tested on longitudinal profiles of 229 athletes, using a 50 % training and 50 % testing split, evaluated based on the 95 % HPD interval.
| Classification model | Variable | G-mean | F 1 | Precision | Sensitivity | Specificity | Balanced | Overall |
|---|---|---|---|---|---|---|---|---|
| accuracy | accuracy (95 % CI) | |||||||
| GLMM | EAAS | 0.10 | 0.02 | 1 | 0.01 | 1 | 0.51 | 0.88 (0.87, 0.90) |
| Ratios | 0.25 | 0.11 | 0.82 | 0.06 | 1 | 0.53 | 0.89 (0.87, 0.90) | |
| All | 0.25 | 0.12 | 0.83 | 0.06 | 1 | 0.53 | 0.89 (0.87, 0.90) | |
| GLMM (after oversampling) | EAAS | 0.20 | 0.08 | 0.79 | 0.04 | 0.99 | 0.51 | 0.51 (0.49, 0.53) |
| Ratios | 0.38 | 0.26 | 0.89 | 0.15 | 0.98 | 0.57 | 0.57 (0.55, 0.59) | |
| All | 0.39 | 0.27 | 0.81 | 0.16 | 0.96 | 0.56 | 0.56 (0.54, 0.58) |
-
Metrics used are defined as Precision =
The classification using the univariate models suggest the T/E, A/ETIO and A5/E ratios as the most sensitive variables for detecting anomalies in the steroidal profile with higher F1 scores (
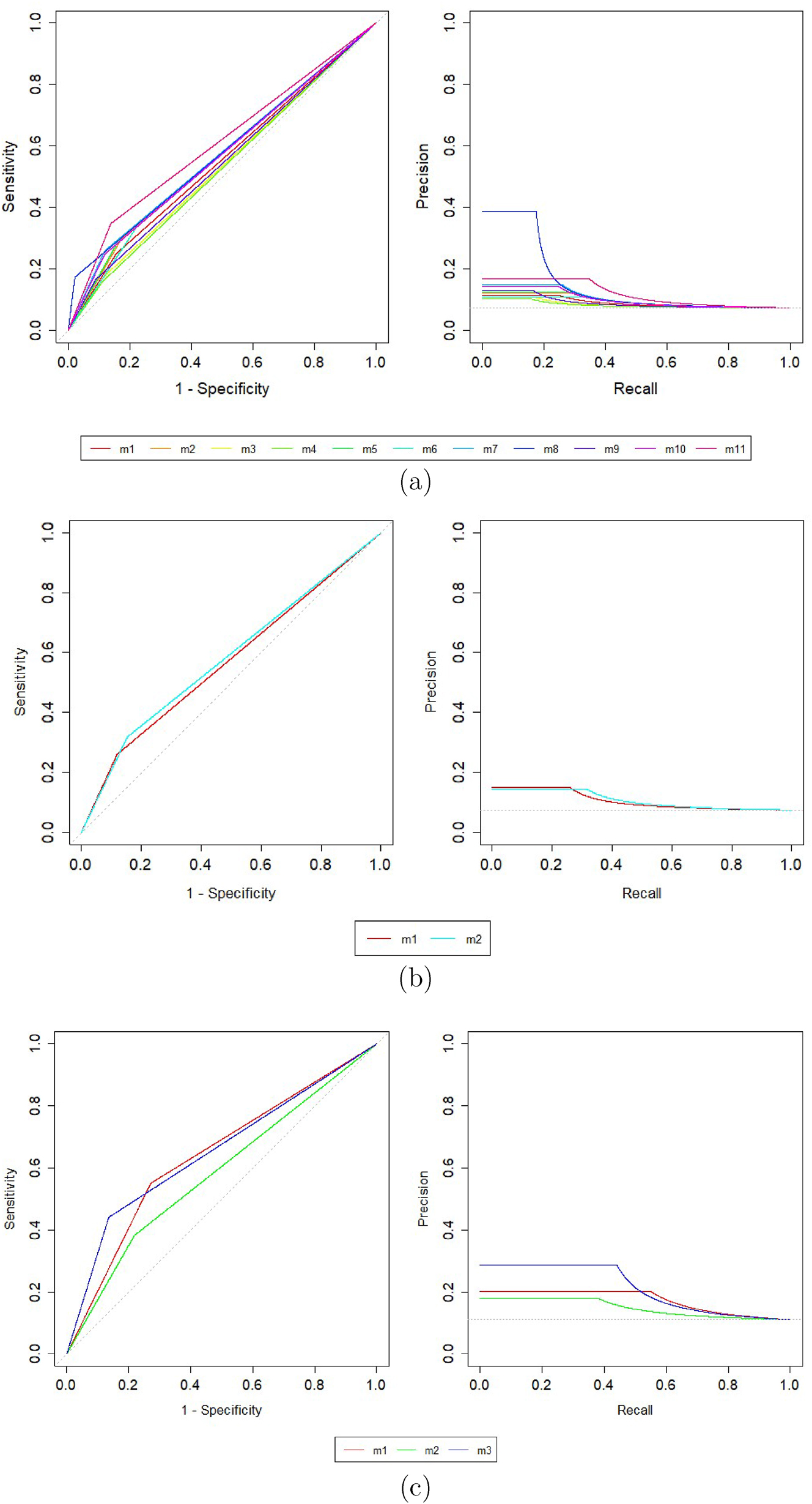
ROC curves obtained from (a) the univariate models (m1: A5, m2: B5, m3: A, m4: ETIO, m5: T, m6: E, m7: T/E, m8: A/ETIO, m9: A/T, m10: A5/B5, m11: A5/E), (b) m1: T/E model versus m2: Sottas’ model for T/E, and (c) the multivariate models (m1: all EAAS markers and ratios, m2: EAAS only, m3: ratios only) applied to the longitudinal test set.
The proposed multivariate Bayesian adaptive (MBA) model has been applied to: (a) EAAS markers only; (b) ratios only; and (c) all EAAS markers and ratios. Evaluating the F1 scores of MBA in Table 2, it appears that MBA achieves an improved classification performance across all models. Further, we observe that the univariate ED score model exhibits considerably higher sensitivity and lower specificity values, indicating a tendency to classify normal values as abnormal. Conversely, in Table 3, the GLMM performance is characterised by significantly higher specificity and lower sensitivity, suggesting a tendency to classify abnormal values as normal. Therefore, their F1 score values are biased towards either very high or very low sensitivity. To address this, we employ the G-mean metric to compare all models, which is the harmonic mean of sensitivity and specificity, as defined in Equation (13). The highest G-mean values are consistently achieved by the multivariate Bayesian adaptive models, which overall outperform univariate (e.g. A5, B5, A) and multivariate models (univariate ED score and GLMM).
As shown in Table 2, between the applications of the MBA model the G-mean and F1 metrics exhibit consistently higher values when compared to their counterparts in the univariate models. Comparing further between the performance of the MBAs, the five available ratios were found to be the most powerful set of variables with the highest metric values
![Figure 6:
Classification metrics per component; i.e. markers and ratios separately, only EAAS, only ratios, all EAAS markers and ratios. T/E1 corresponds to the T/E model from Section 2.1, while T/E2 corresponds to the T/E model by Sottas et al. [17]. Subscripts “pre”, “post”, denote pre-oversampling and post-oversampling, respectively.](/document/doi/10.1515/ijb-2024-0019/asset/graphic/j_ijb-2024-0019_fig_006.jpg)
Classification metrics per component; i.e. markers and ratios separately, only EAAS, only ratios, all EAAS markers and ratios. T/E1 corresponds to the T/E model from Section 2.1, while T/E2 corresponds to the T/E model by Sottas et al. [17]. Subscripts “pre”, “post”, denote pre-oversampling and post-oversampling, respectively.
5 Discussion
Our primary objective in this research was to develop a multivariate Bayesian adaptive (MBA) model for repeated measurements of various urinary biomarkers and their ratios, as a generalisation of a widely used univariate model [17] which also uses urinary steroid profile data for doping detection. Similar to the univariate model, the proposed methodology considers the population distribution of these biomarkers and the individual’s own history; i.e. previous measurements of the athlete’s biomarkers. Additionally, the MBA model can incorporate other relevant demographic characteristics, such sex and age, as covariates, when examining their effects is a primary objective. The method simultaneously models multiple measurements of endogenous substances that are able to reveal the presence of doping agents, and utilises a one-class classification rule to improve detection performance in the presence of class imbalance. The resulting personalised normal ranges for athletes’ longitudinal steroid profiles show improved detection performance in a dataset of professional athletes, as compared to the performance of the existing univariate model. The proposed method thus appears promising as an additional monitoring tool in the anti-doping toolkit. One of the method’s advantages is that it relies on the urinary steroid profile, which produces easily accessible, reliable, quickly quantifiable and reproducible data from samples that are obtained in a non-invasive way and with a low financial cost. In addition, a user-friendly software implementing the multivariate Bayesian adaptive model has been specifically designed for doping control analyses in anti-doping laboratories.
A challenging aspect of this work was the presence of class imbalance due to the scarcity of data from confirmed doping cases. To alleviate this problem, the technique of one-class classification was applied to the proposed multivariate Bayesian adaptive model. For GLMM, oversampling was utilised, although other techniques such as undersampling, a combination of undersampling and oversampling or boosting algorithms that are able to convert weak learners to strong learners could also be explored [38], [39].
Building on this strong performance, our proposed multivariate Gaussian adaptive model, also provides the foundation and flexibility for further research to generalise the MBA model. Future development could include incorporating non-linear effects to capture more complex relationships or extending the Gaussian framework to a mixture of Gaussians for greater flexibility. Applications on additional markers and ratios is another direction which is worth investigating. An illustrative example of this concept can be found in the work of Wilkes et al. [40]. Lastly, this research examines the predictive performance of the Bayesian adaptive model when applied to six biomarkers and five ratios. It would be of interest to explore whether a subset of these variables could further improve performance. Further testing on additional datasets is needed to produce robust recommendations as to the optimal implementation of the model.
Funding source: Engineering and Physical Sciences Research Council (EPSRC)
Award Identifier / Grant number: 00339974
Acknowledgments
We are grateful to Dr Eugenio Alladio of the Department of Chemistry at the University of Torino for generously providing access to their laboratory dataset, which enriched the outcomes of this study. We would also like to thank Dr Ludger Evers for helpful discussions throughout this research work.
-
Research ethics: The datasets have been collected by following all the appropriate ethical approval procedures.
-
Informed consent: Not applicable.
-
Author contributions: The authors have accepted responsibility for the entire content of this manuscript and approved its submission.
-
Use of Large Language Models, AI and Machine Learning Tools: None declared.
-
Conflict of interest: The authors declare that there are no conflicts of interest.
-
Research funding: DE is supported by a doctoral scholarship awarded by the Engineering and Physical Sciences Research Council (EPSRC).
-
Data availability: Summary data are provided.
References
1. Kanayama, G, Pope Jr, HG. History and epidemiology of anabolic androgens in athletes and non-athletes. Mol Cell Endocrinol 2018;464:4–13. https://doi.org/10.1016/j.mce.2017.02.039.Search in Google Scholar PubMed
2. World Anti-Doping Agency. 2021 Anti-doping testing figures [Online]. https://www.wada-ama.org/sites/default/files/2023-01/2021_anti-doping_testing_figures_en.pdf [Accessed 19 Feb 2024].Search in Google Scholar
3. Sottas, PE, Saugy, M, Saudan, C. Endogenous steroid profiling in the athlete biological passport. Endocrinol Metabol Clin 2010;39:59–73. https://doi.org/10.1016/j.ecl.2009.11.003.Search in Google Scholar PubMed
4. World Anti-Doping Agency. Technical document – TD2021EAAS [Online]. https://www.wada-ama.org/sites/default/files/2022-01/td2021eaas_final_eng_v_2.0.pdf [Accessed 19 Feb 2024].Search in Google Scholar
5. Sottas, PE, Robinson, N, Rabin, O, Saugy, M. The athlete biological passport. Clin Chem 2011;57:969–76. https://doi.org/10.1373/clinchem.2011.162271.Search in Google Scholar PubMed
6. Vernec, AR. The athlete biological passport: an integral element of innovative strategies in antidoping. Br J Sports Med 2014;48:817–19. https://doi.org/10.1136/bjsports-2014-093560.Search in Google Scholar PubMed
7. World Anti-Doping Agency. WADA technical document – TD2021APMU [Online]. https://www.wada-ama.org/sites/default/files/resources/files/td2021apmu_final_eng_0.pdf [Accessed 19 Feb 2024].Search in Google Scholar
8. Kuuranne, T, Saugy, M, Baume, N. Confounding factors and genetic polymorphism in the evaluation of individual steroid profiling. Br J Sports Med 2014;48:848–55. https://doi.org/10.1136/bjsports-2014-093510.Search in Google Scholar PubMed PubMed Central
9. Piper, T, Geyer, H, Haenelt, N, Huelsemann, F, Schaenzer, W, Thevis, M. Current insights into the steroidal module of the athlete biological passport. Int J Sports Med 2021;42:863–78. https://doi.org/10.1055/a-1481-8683.Search in Google Scholar PubMed PubMed Central
10. Mareck, U, Geyer, H, Opfermann, G, Thevis, M, Schänzer, W. Factors influencing the steroid profile in doping control analysis. J Mass Spectrom 2008;43:877–91. https://doi.org/10.1002/jms.1457.Search in Google Scholar PubMed
11. Harris, EK. Effects of intra-and interindividual variation on the appropriate use of normal ranges. Clin Chem 1974;20:1535–42. https://doi.org/10.1093/clinchem/20.12.1535.Search in Google Scholar
12. Brooks, RV, Jeremiah, G, Webb, WA, Wheeler, M. Detection of anabolic steroid administration to athletes. J Steroid Biochem 1979;11:913–17. https://doi.org/10.1016/b978-0-08-023796-1.50129-8.Search in Google Scholar
13. Donike, M, Barwald, K, Klostermann, KR, Schanzer, W, Zimmermann, J. Nachweis von exogenem testosteron [detection of exogenous testosterone]. Sport: Leistung und Gesundheit 1983;293–8.Search in Google Scholar
14. Sottas, PE, Robinson, N, Giraud, S, Taroni, F, Kamber, M, Mangin, P, et al.. Statistical classification of abnormal blood profiles in athletes. Int J Biostat 2006;2. https://doi.org/10.2202/1557-4679.1011.Search in Google Scholar
15. Sottas, P-E, Saudan, C, Schweizer, C, Baume, N, Mangin, P, Saugy, M. From population-to subject-based limits of T/E ratio to detect testosterone abuse in elite sports. Forensic Sci Int 2008;174:166–72. https://doi.org/10.1016/j.forsciint.2007.04.001.Search in Google Scholar PubMed
16. Van Renterghem, P, Van Eenoo, P, Geyer, H, Schänzer, W, Delbeke, FT. Reference ranges for urinary concentrations and ratios of endogenous steroids, which can be used as markers for steroid misuse, in a Caucasian population of athletes. Steroids 2010;75:154–63. https://doi.org/10.1016/j.steroids.2009.11.008.Search in Google Scholar PubMed
17. Sottas, P-E, Baume, N, Saudan, C, Schweizer, C, Kamber, M, Saugy, M. Bayesian detection of abnormal values in longitudinal biomarkers with an application to T/E ratio. Biostatistics 2007;8:285–96. https://doi.org/10.1093/biostatistics/kxl009.Search in Google Scholar PubMed
18. Brown, PJ, Kenward, MG, Bassett, EE. Bayesian discrimination with longitudinal data. Biostatistics 2001;2:417–32. https://doi.org/10.1093/biostatistics/2.4.417.Search in Google Scholar PubMed
19. Alladio, E, Caruso, R, Gerace, E, Amante, E, Salomone, A, Vincenti, M. Application of multivariate statistics to the steroidal module of the athlete biological passport: a proof of concept study. Anal Chim Acta 2016;922:19–29. https://doi.org/10.1016/j.aca.2016.03.051.Search in Google Scholar PubMed
20. Amante, E, Pruner, S, Alladio, E, Salomone, A, Vincenti, M, Bro, R. Multivariate interpretation of the urinary steroid profile and training-induced modifications. The case study of a marathon runner. Drug Test Anal 2019;11:1556–65. https://doi.org/10.1002/dta.2676.Search in Google Scholar PubMed
21. Wang, M, Li, Z, Lee, EY, Lewis, MM, Zhang, L, Sterling, NW, et al.. Predicting the multi-domain progression of Parkinson’s disease: a Bayesian multivariate generalized linear mixed-effect model. BMC Med Res Methodol 2017;17:1–10. https://doi.org/10.1186/s12874-017-0415-4.Search in Google Scholar PubMed PubMed Central
22. Xia, YM, Tang, NS. Bayesian analysis for mixture of latent variable hidden Markov models with multivariate longitudinal data. Comput Stat Data Anal 2019;132:190–211. https://doi.org/10.1016/j.csda.2018.08.004.Search in Google Scholar
23. Shamshoian, J, Şentürk, D, Jeste, S, Telesca, D. Bayesian analysis of longitudinal and multidimensional functional data. Biostatistics 2022;23:558–73. https://doi.org/10.1093/biostatistics/kxaa041.Search in Google Scholar PubMed PubMed Central
24. World Anti-Doping Agency. WADA technical document – TD2021IRMS [Online]. https://www.wada-ama.org/sites/default/files/resources/files/td2021irms_final_eng_0.pdf [Accessed 19 Feb 2024].Search in Google Scholar
25. R Core Team. The R project for statistical computing [Online]https://www.r-project.org/ [Accessed 20 Oct 2023].Search in Google Scholar
26. De Figueiredo, M, Saugy, J, Saugy, M, Faiss, R, Salamin, O, Nicoli, R, et al.. A new multimodal paradigm for biomarkers longitudinal monitoring: a clinical application to women steroid profiles in urine and blood. Anal Chim Acta 2023;1267:341389. https://doi.org/10.1016/j.aca.2023.341389.Search in Google Scholar PubMed
27. DeGroot, MH. Optimal statistical decisions. Hoboken, New Jersey, United States: John Wiley & Sons; 2005, 82.Search in Google Scholar
28. Casella, G, George, EI. Explaining the Gibbs sampler. Am Statistician 1992;46:167–74. https://doi.org/10.1080/00031305.1992.10475878.Search in Google Scholar
29. Gelman, A, Carlin, JB, Stern, HS, Dunson, DB, Vehtari, A, Rubin, DB. Bayesian data analysis. Boca Raton, Florida, United States: CRC Press; 2013.10.1201/b16018Search in Google Scholar
30. Minter, T. Single-class classification. In: LARS symposia; 1975:54 p.10.5179/benthos1970.1975.54Search in Google Scholar
31. Bishop, CM. Novelty detection and neural network validation. IEE Proc Vis Image Signal Process 1994;141:217–22. https://doi.org/10.1049/ip-vis:19941330.10.1049/ip-vis:19941330Search in Google Scholar
32. Khan, SS, Madden, MG. One-class classification: taxonomy of study and review of techniques. Knowl Eng Rev 2014;29:345–74. https://doi.org/10.1017/s026988891300043x.Search in Google Scholar
33. Hyndman, RJ. Computing and graphing highest density regions. Am Statistician 1996;50:120–6. https://doi.org/10.1080/00031305.1996.10474359.Search in Google Scholar
34. Rauth, S. Referenzbereiche von urinären Steroidkonzentrationen und Steroidquotienten: ein Beitrag zur Interpretation des Steroidprofils in der Routinedopinganalytik [Ph.D. thesis]. Deutsche Sporthochschule Köln; 1994.Search in Google Scholar
35. Kicman, AT, Coutts, SB, Walker, CJ, Cowan, DA. Proposed confirmatory procedure for detecting 5 alpha-dihydrotestosterone doping in male athletes. Clin Chem 1995;41:1617–27. https://doi.org/10.1093/clinchem/41.11.1617.Search in Google Scholar
36. Eleftheriou, D. Bayesian hierarchical modelling for biomarkers with applications to doping detection and prostate cancer prediction [Ph.D. thesis]. University of Glasgow; 2022.Search in Google Scholar
37. Bates, D, Mächler, M, Bolker, B, Walker, S. Fitting linear mixed-effects models using lme4. J Stat Software 2015;67:1–48. https://doi.org/10.18637/jss.v067.i01.Search in Google Scholar
38. Kotsiantis, S, Kanellopoulos, D, Pintelas, P. Handling imbalanced datasets: a review. GESTS Int Trans Comput Sci Eng 2006;30:25–36.Search in Google Scholar
39. Schapire, RE. Empirical inference. Berlin, Germany: Springer; 2013:37–52 pp.10.1007/978-3-642-41136-6_5Search in Google Scholar
40. Wilkes, EH, Rumsby, G, Woodward, GM. Using machine learning to aid the interpretation of urine steroid profiles. Clin Chem 2018;64:1586–95. https://doi.org/10.1373/clinchem.2018.292201.Search in Google Scholar PubMed
Supplementary Material
This article contains supplementary material (https://doi.org/10.1515/ijb-2024-0019).
© 2025 the author(s), published by De Gruyter, Berlin/Boston
This work is licensed under the Creative Commons Attribution 4.0 International License.
Articles in the same Issue
- Frontmatter
- Research Articles
- Prognostic adjustment with efficient estimators to unbiasedly leverage historical data in randomized trials
- Homogeneity test and sample size of response rates for AC 1 in a stratified evaluation design
- A review of survival stacking: a method to cast survival regression analysis as a classification problem
- DsubCox: a fast subsampling algorithm for Cox model with distributed and massive survival data
- A hybrid hazard-based model using two-piece distributions
- Regression analysis of clustered current status data with informative cluster size under a transformed survival model
- Bayesian covariance regression in functional data analysis with applications to functional brain imaging
- Risk estimation and boundary detection in Bayesian disease mapping
- An improved estimator of the logarithmic odds ratio for small sample sizes using a Bayesian approach
- Short Communication
- A multivariate Bayesian learning approach for improved detection of doping in athletes using urinary steroid profiles
- Research Articles
- Guidance on individualized treatment rule estimation in high dimensions
- Weighted Euclidean balancing for a matrix exposure in estimating causal effect
- Penalized regression splines in Mixture Density Networks
Articles in the same Issue
- Frontmatter
- Research Articles
- Prognostic adjustment with efficient estimators to unbiasedly leverage historical data in randomized trials
- Homogeneity test and sample size of response rates for AC 1 in a stratified evaluation design
- A review of survival stacking: a method to cast survival regression analysis as a classification problem
- DsubCox: a fast subsampling algorithm for Cox model with distributed and massive survival data
- A hybrid hazard-based model using two-piece distributions
- Regression analysis of clustered current status data with informative cluster size under a transformed survival model
- Bayesian covariance regression in functional data analysis with applications to functional brain imaging
- Risk estimation and boundary detection in Bayesian disease mapping
- An improved estimator of the logarithmic odds ratio for small sample sizes using a Bayesian approach
- Short Communication
- A multivariate Bayesian learning approach for improved detection of doping in athletes using urinary steroid profiles
- Research Articles
- Guidance on individualized treatment rule estimation in high dimensions
- Weighted Euclidean balancing for a matrix exposure in estimating causal effect
- Penalized regression splines in Mixture Density Networks