Practical experience using galectin-3 in heart failure
-
Peter A. McCullough
Peter A. McCullough, MD, MPH, FACC, FACP, FCCP, FAHA, FNKF. After receiving a Bachelor’s degree from Baylor University, Dr. McCullough completed his Medical degree as an Alpha Omega Alpha graduate from the University of Texas Southwestern Medical School in Dallas. He went on to complete his Internal Medicine residency at the University of Washington in Seattle, cardiology fellowship including service as Chief Fellow at William Beaumont Hospital, and Master’s degree in public health at the University of Michigan. Dr. McCullough oversees cardiovascular education and research at the Baylor Health System in Dallas, TX, USA. He is an internationally recognized authority on the role of chronic kidney disease as a cardiovascular risk state with over 1000 publications including the “Interface between renal disease and cardiovascular illness” in Braunwald’s Heart Disease Textbook. In 2013, he was honored with the International Vicenza Award for Critical Care Nephrology for his outstanding contribution and dedication to the emerging problem of cardiorenal syndromes.


Abstract
Heart failure is a complex mechanical and neurohormonal syndrome where the left ventricle fails as a pump, resulting in stasis of blood in the lungs and the periphery resulting in the cardial features of effort intolerance, fatigue, and peripheral edema. As part of the neurohormonal and local mechanical strain, tissue macrophages resident in the myocardium secrete galectin-3 which is a paracrine and endocrine factor which stimulates additional macrophages, pericytes, myofibroblasts, and fibroblasts to proliferate and secrete procollagen I which is irreversibly crosslinked resulting in myocardial fibrosis. In the general population, normal plasma concentrations of galectin-3 are <11.0 ng/mL. Galectin-3 measured in blood has been shown to: 1) identify increased risk for new onset heart failure in healthy middle-aged adults; 2) predict cardiac failure in patients after acute coronary syndromes; 3) help establish the diagnosis of heart failure with preserved ejection fraction in patients presenting with exercise intolerance; and 4) aid in the prognosis of heart failure with preserved and reduced left ventricular ejection fraction. This manuscript will present practical real case management in these applications to highlight the importance of this new in vitro diagnostic test.
Introduction
Heart failure (HF) is a complex mechanical and neurohumoral syndrome with symptoms arising from hemodynamic congestion including dyspnea, orthopnea, paroxysmal nocturnal dyspnea or peripheral edema [1, 2]. The functional and histopathologic correlates of cardiac failure include myocyte dysfunction, accelerated apoptosis, and replacement fibrosis [3]. In the failing human heart, considerable quantities of myocardium can be replaced with fibrosis leading to both diastolic and systolic dysfunction as seen on echocardiography. In addition, cardiovascular fibrosis leads to both vascular stiffness and cardiomyopathy, both of which contribute to progressive left ventricular dysfunction (Figure 1). Heterogeneity of depolarization in the myocardium as a result of fibrosis can lead to conduction delay, dyssynchrony, and re-entrant arrhythmias including ventricular tachycardia and ventricular fibrillation. Thus, assessment of the process of cardiovascular fibrosis with a novel in vitro diagnostic assay in plasma can be viewed as a breakthrough for clinicians in case management.

Vascular and left ventricular fibrosis lead to heart failure progression resulting in pump failure or arrhythmic death.
HF is a leading cause of emergency room visits, hospitalizations, and death with five million cases in the US and another 500,000 diagnosed each year resulting in the forecasted prevalence to double by year 2040 [4, 5]. Advancing age is a leading determinant of myocardial fibrosis, and thus, the incidence of HF nearly doubles for patients >85 years of age compared to those <75 years [4].
Approximately two thirds of HF patients have ischemic cardiomyopathy with zones of cardiac fibrosis in the form of a healed infarction [5, 6]. The extent of coronary artery disease and prior infarction is associated with the severity of left ventricular dysfunction and clinical outcomes in those with both preserved and reduced ejection fraction [7, 8].
Non-ischemic cardiomyopathy accounts for the remaining third of individuals with reduced left ventricular ejection fraction (LVEF). Most forms of non-ischemic cardiomyopathy have an underlying genetic susceptibility (e.g., polymorphisms in sarcomeric proteins, titin), and then a superimposed myocardial insult, such as long-standing hypertension, myocarditis, alcohol, cardiotoxic therapy (e.g., anthracyclines), infiltrative diseases (sarcoid, amyloid), radiation, autoimmune disease, etc. The important aspect of non-ischemic cardiomyopathy epidemiology is that among those discovered to have “idiopathic” dilated cardiomyopathy; approximately 20% of first degree family have subclinical disease [9]. An excess deposition of collagen in the extracellular matrix and tissue fibrosis may be an early finding in patients with subclinical disease and thus blood testing and imaging hold the promise of identifying underlying pathology [10].
Chronic kidney disease (CKD) imposes three important pathophysiologic processes on the heart: 1) pressure overload; 2) volume overload; and 3) cardiomyopathy. When patients with CKD develop myocardial fibrosis and findings of HF, this is termed a type 4 chronic cardiorenal syndrome [11].
Galectin-3-mediated cardiac fibrosis
The evidence base for galectin-3 and its role in the pathogenesis of cardiac fibrosis has been described in detail by McCullough and coworkers [12]. Production of galectin-3 from local pericytes, mast cells, and macrophages, induces resident fibroblasts and myofibroblasts to produce procollagen which is irreversibly crosslinked to collagen generating cardiac fibrosis (Figure 1) [10, 13].
The galectin family of carbohydrate-binding proteins (15 in mammals and 11 in humans) are important proteins in the scarring process. Galectins are carbohydrate-binding proteins involved in the regulation of satellite cell signaling, immunity and cancer. Galectin-3 (aka MAC-2 Ag) is an approximately 30 kDa glycoprotein that has a carbohydrate-recognition-binding domain of approximately 130 amino acids that enables the binding of β-galactosides [14–16]. It is encoded by a single gene (LGALS3) on chromosome 14, locus q21–q22 and expressed in the nucleus and mitochondria [17]. Galectin-3 as a paracrine protein directs cell adhesion, activation, chemoattraction, growth and differentiation, upregulation of the cell cycle, and apoptosis [18]. In the myocardium, galectin-3 assists transforming growth factor β (TGFβ) to increase cell cycle (cyclin D1) and of myofibroblasts which results in their proliferation and synthesis of procollagen 1. Recombinant galectin-3 has been shown to induce cardiac fibroblast proliferation, collagen production, and cyclin D1 expression [19]. In aggregate, the data strongly suggest that galectin-3 is a critical participant in the pathogenesis and progression of HF and therefore, present the following actual cases discussing results and management [20].
Case 1: galectin-3 and the risk of future heart failure
A 55-year-old male is seen in the office with a concern regarding the future risks of myocardial disease. He is asymptomatic but has a longstanding history of well-controlled hypertension and a normal LVEF of 60% and normal renal function. There is a family history of hypertension, HF, and cardiac death. His galectin-3 level is found to be 16.2 ng/mL (normal <11.0 ng/mL) and this prompts repeat echocardiography which reveals mild left ventricular hypertrophy and an LVEF of 45%. His antihypertensive regimen is changed from amlodipine 10 mg p.o. qd to enalapril 20 mg p.o. bid in order to attenuate any further cardiac remodeling and reduce the risks of future HF.
The Framingham Heart Study measured galectin-3 from stored samples of study participants who were free of cardiovascular disease at baseline (single measurement). In this report from Ho and colleagues the mean age of the Framingham cohort was 59 at baseline, and those in the highest galectin-3 tertile (15.4–47.7 ng/mL) had a considerably higher rate (approx. 10% vs. approx. 2%) of incident HF and all-cause mortality when followed over the next 11 years (Figure 2) [21]. These findings have recently been corroborated in the Physicians Health Study where baseline galectin-3 levels also predicted the future risk of HF [22].
![Figure 2 Rates of de novo heart failure according to galectin-3 level in the Framingham Heart Study. Adapted from reference [21].](/document/doi/10.1515/cclm-2014-0278/asset/graphic/cclm-2014-0278_fig2.jpg)
Rates of de novo heart failure according to galectin-3 level in the Framingham Heart Study. Adapted from reference [21].
Thus our patient with hypertension and an elevated galectin-3 level has higher risks of CKD with rapid progression as well as incidence HF and death. He should be considered to have stage A HF and in addition to the angiotensin converting enzyme inhibitor, consider β-adrenergic blockade if tolerated from a blood pressure and exercise perspective. In addition, surveillance for HF signs and symptoms is warranted.
Case 2: acute coronary syndrome with measurement of galectin-3
A 60-year-old man presents with a non-ST-segment elevation myocardial infarction. Coronary angiography reveals a severe lesion in the LAD treated with PCI and stenting and a moderate lesion in the proximal left circumflex which was not treated. The baseline galectin-3 was 22.1 ng/mL, B-type natriuretic peptide (BNP) was 151 pg/mL, and LVEF=55%. The patient developed pulmonary edema and was transferred to the intensive care unit on hospital day 3 after prompt recognition and treatment. In this case both the galectin-3 and BNP anticipated acute decompensation and were prompts for careful observation in the hospital. Grandin et al. in the PROVE IT-TIMI 22 (Pravastatin or Atorvastatin Evaluation and Infection Therapy-Thrombolysis In Myocardial Infarction 22) trial found that a galectin-3 value >16.7 ng/mL was associated with a 2.1-fold risk (95% CI 1.2–3.6) for developing HF, p=0.010 (Figure 3) [23]. Thus in addition to assessment of the degree of coronary disease, LVEF, and BNP, galectin-3 is helpful in the management of ACS. It is likely the galectin-3 level reflects the circulating levels before the myocardial infarction occurred since acute ischemia or infarction does not rapidly simulate macrophage production of galectin-3.
![Figure 3 Development of heart failure (HF) in patients after acute coronary syndrome (ACS) in the Thrombolysis in Myocardial Infarction PROVE-IT 22 trial. Adapted from reference [23].](/document/doi/10.1515/cclm-2014-0278/asset/graphic/cclm-2014-0278_fig3.jpg)
Development of heart failure (HF) in patients after acute coronary syndrome (ACS) in the Thrombolysis in Myocardial Infarction PROVE-IT 22 trial. Adapted from reference [23].
Case 3: establishing an office diagnosis of heart failure
An obese 55-year-old female is seen for dyspnea on exertion (functional class II) and pedal edema. She has a history of hypertension treated with chlorthalidone. She has a normal cardiac exam. Electrocardiogram reveals normal sinus rhythm with left ventricular hypertrophy and no Q-waves. Persantine cardiac nuclear scintigraphy revealed normal myocardial perfusion. Echocardiography revealed LVH and LVEF=65% with a pseudonormal (grade II) pattern of diastolic dysfunction. The BNP was 94 pg/mL and the galectin-3 was elevated at 20.4 ng/mL confirming a diagnosis of HF with preserved ejection fraction (HFPEF). Enalapril 5 mg p.o. bid and spironolactone 25 mg p.o. qd were started and chlorthalidone were discontinued. This case highlights how galectin-3 is useful in the obese dyspneic patient in sorting out multiple source of exercise intolerance and revealing significant myocardial disease.
Case 4: galectin-3 and prognosis of heart failure with reduced ejection fraction
A 68-year-old female with ischemic cardiomyopathy, LVEF=30% and class 3 HF was seen for routine office visit. Past history included an anterior wall myocardial infarction several years ago confirmed by troponin testing and standard clinical criteria, dyslipidemia, and stroke. She has fatigue, dyspnea on exertion, orthopnea, S3, and 3+ edema on exam. Cardiac magnetic resonance imaging demonstrated a large area of anterior fibrosis in the zone of a prior infarction (Figure 4). The galectin-3 level was found to be 28.8 ng/mL. The patient was changed from quarterly to monthly visits. Spironolactone 25 mg p.o. qd was started, enalapril was doubled in dose to 10.0 mg p.o. bid, and the remainder of the medical regiment was unchanged (carvedilol 12.5 mg p.o. bid, bumetanide 2 mg p.o. qd, warfarin 2.0 mg p.o. qd, aspirin 81 mg p.o. qd). In addition, she was referred for an implantable cardio defibrillator. The very elevated galectin-3 level indicates progressive cardiac and vascular fibrosis which can lead to the progression of HF by creating tissue heterogeneity which is the substrate for arrhythmias and cardiac death.
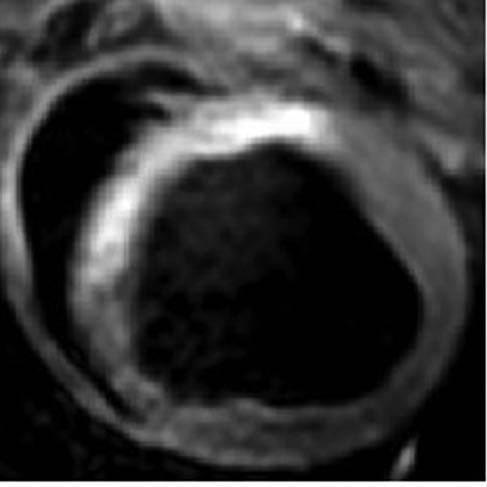
Cardiac magnetic resonance imaging showing a large area of anterior left ventricular fibrosis as a result of a previous myocardial infarction.
Among unselected HF patients, the median galectin-3 level is 17.7 ng/mL. Lin and coworkers measured blood galectin-3 in 106 patients with stable class 2 HF and mean LVEF of 35% and found significant relationships between galectin-3 and measures of cardiac fibrosis and extracellular matrix formation using multivariate analysis [24]. Log-transformed values of galectin-3 was significantly correlated with type 3 aminoterminal propeptide of procollagen (p=0.006), tissue inhibitor of metalloproteinase-1 (p=0.025), and metalloproteinase-2 (p=0.016).
Approximately 90% of patients with HF experience death that is either attributable to pump failure or arrhythmias [4]. Progression of HF is characterized by frequent hospitalizations, symptomatic arrhythmias, and complications from other illnesses, such as infection, renal failure, and electrolyte imbalances including hyponatremia. As progressive cardiac fibrosis contributes to both systolic and diastolic impairment and creates opportunities for lethal arrhythmias, it is intuitive that a blood marker of cardiac fibrosis would be independently associated with HF hospitalization and death. In the Pro-BNP Investigation of Dyspnea in the Emergency Department (PRIDE) study, among those patients with acute dyspnea in the emergency department, log galectin-3 was associated with death, odds ratio (OR)=10.3 (p=0.007) and the composite of death or hospitalization, OR=14.3 (p<0.001) for death and the combination of death or hospitalization [24, 25].
Galectin-3 was measured in 592 subjects in the Counseling in Heart failure (COACH) trial prior to hospital discharge and 6 months later in the office [24]. A two-fold rise in galectin-3 from baseline independently predicted HF rehospitalization and death after adjustment for age, gender, and natriuretic peptide levels with adjusted hazard ratio of 1.77, 95% CI 1.42–2.20, p<0.001. Data combined from the COACH and CORONA (Controlled Rosuvastatin Multinational Study in Heart Failure) revealed that as little as a 15% change in outpatients can predict a worse (increase) or better (decrease) prognosis [26]. However, when evaluated individually in a smaller sample in CORONA, Gullestad and coworkers failed to find an independent relationship between the change in galectin-3 and HF outcomes when NT-proBNP was included in the final model [27]. Thus, galectin-3 has a more narrow range of biological variability (±15%) than the natriuretic peptides where in general, a doubling of the baseline indicates worsening and a 50% decrease over time signals improvement [28]. In COACH, galectin-3 had prognostic values in both HFREF and HFPEF.
Integration of galectin-3 in heart failure management
An algorithm for patients with established HF confirmed by BNP or NT-proBNP is shown in Figure 5. For patients in the ≤17.8 ng/mL range, good clinical practice and usual care are reasonable with periodic outpatient follow-up visits. For those in the 17.9–25.9 ng/mL range, more intensified care management is suggested by galectin-3 with possibly more frequent visits, medication monitoring and device monitoring/adjustment. In HF cases with galectin-3 >25.9 ng/mL, there a markedly elevated risk of HF hospitalization and an even greater chance of death. In this group the most aggressive management could be considered including dedicated HF nurses and allied health professionals, home care, monthly or more frequent office visits, and possibly referral for transplantation. Optimization of medical and device therapy is also indicated by clinical parameters, such as functional class, congestion, edema, QRS duration, and other parameters on the intracardiac electrocardiogram [29]. Importantly, a galectin-3 level >25.9 ng/mL predicts a 28% chance of hospitalization and a 43% risk of death over 18 months; signaling an opportunity for counseling and in appropriate situations, measures appropriate for end-of-life care.
![Figure 5 Evidence-based algorithm for the measurement of galectin-3 in patients after hospitalization or in the office with established heart failure.Mgt, management. Adapted from reference [12].](/document/doi/10.1515/cclm-2014-0278/asset/graphic/cclm-2014-0278_fig5.jpg)
Evidence-based algorithm for the measurement of galectin-3 in patients after hospitalization or in the office with established heart failure.
Mgt, management. Adapted from reference [12].
Summary
Galectin-3 is a paracrine factor that reflects cardiac fibroblast proliferation, collagen deposition, and progression of left ventricular dysfunction. In the general population, elevations of galectin-3 above the normal range relate a higher risk for the de novo development of HF. In the evaluation of dyspnea and fatigue, galectin-3 in conjunction with the natriuretic peptides, may help establish or rule out a diagnosis of HF. In established, chronic HF patients, galectin-3 levels >25.9 pg/mL, or increasing levels over 6 months portend high rates of hospitalization and death. Practical case summaries and the literature to date indicate galectin-3 is a valuable tool for HF risk prediction, diagnosis, prognosis, and management. Future research is needed to understand how galectin-3 levels integrate with established biomarkers such as troponin I or T and BNP or NT-proBNP.
Conflict of interest statement
Authors’ conflict of interest disclosure: The authors stated that there are no conflicts of interest regarding the publication of this article.
Research funding: None declared.
Employment or leadership: None declared.
Honorarium: None declared.
About the author

Peter A. McCullough, MD, MPH, FACC, FACP, FCCP, FAHA, FNKF. After receiving a Bachelor’s degree from Baylor University, Dr. McCullough completed his Medical degree as an Alpha Omega Alpha graduate from the University of Texas Southwestern Medical School in Dallas. He went on to complete his Internal Medicine residency at the University of Washington in Seattle, cardiology fellowship including service as Chief Fellow at William Beaumont Hospital, and Master’s degree in public health at the University of Michigan. Dr. McCullough oversees cardiovascular education and research at the Baylor Health System in Dallas, TX, USA. He is an internationally recognized authority on the role of chronic kidney disease as a cardiovascular risk state with over 1000 publications including the “Interface between renal disease and cardiovascular illness” in Braunwald’s Heart Disease Textbook. In 2013, he was honored with the International Vicenza Award for Critical Care Nephrology for his outstanding contribution and dedication to the emerging problem of cardiorenal syndromes.
References
1. Raghava V, Ramachandran V. Epidemiology of heart failure. In: Mann DL, editor. Heart failure: a companion to Braunwald’s heart disease, 2nd ed. Saint Louis, Missouri: Elsevier Saunders, 2011.Search in Google Scholar
2. McMurray, J. What is heart failure? In: Abraham W, Krum H, editors. Heart failure: a practical approach to treatment. New York, New York: McGraw Hill, 2007.Search in Google Scholar
3. Vasquez C, Benamer N, Morley GE. The cardiac fibroblast: functional and electrophysiological considerations in healthy and diseased heart. J Cardiovasc Pharmacol 2011;57:380–8.10.1097/FJC.0b013e31820cda19Search in Google Scholar
4. McCullough PA, Philbin EF, Spertus JA, Kaatz S, Sandberg KR, Weaver WD. Confirmation of a heart failure epidemic: findings from the Resource Utilization Among Congestive Heart Failure (REACH) study. J Am Coll Cardiol 2002;39:60–9.10.1016/S0735-1097(01)01700-4Search in Google Scholar
5. Soman P, Lahiri A, Mieres JH, Calnon DA, Wolinsky D, Beller GA, et al. Etiology and pathophysiology of new-onset heart failure: evaluation by myocardial perfusion imaging. J Nucl Cardiol 2009;16:82–91.10.1007/s12350-008-9010-8Search in Google Scholar
6. van den Borne SW, Diez J, Blankesteijn WM, Verjans J, Hofstra L, Narula J. Myocardial remodeling after infarction: the role of myofibroblasts. Nat Rev Cardiol 2010;7:30–7.10.1038/nrcardio.2009.199Search in Google Scholar
7. Vanhecke TE, Kim R, Raheem SZ, McCullough PA. Myocardial ischemia in patients with diastolic dysfunction and heart failure. Curr Cardiol Rep 2010;12:216–22.10.1007/s11886-010-0101-1Search in Google Scholar
8. Vanhecke TE, Franklin BA, Soman P, Lahiri A, Mieres JH, Sias T, et al. Influence of myocardial ischemia on outcomes in patients with systolic versus non-systolic heart failure. Am J Cardiovasc Dis 2011;1:167–75.10.1016/S0735-1097(11)62015-9Search in Google Scholar
9. Michels VV, Moll PP, Miller FA, Tajik AJ, Chu JS, Driscoll DJ, et al. The frequency of familial dilated cardiomyopathy in a series of patients with idiopathic dilated cardiomyopathy. N Engl J Med 1992;326:77–82.10.1056/NEJM199201093260201Search in Google Scholar PubMed
10. Hutchinson KR, Stewart JA Jr, Lucchesi PA. Extracellular matrix remodeling during the progression of volume overload-induced heart failure. J Mol Cell Cardiol 2010;48:564–9.10.1016/j.yjmcc.2009.06.001Search in Google Scholar PubMed PubMed Central
11. Tumlin JA, Costanzo MR, Chawla LS, Herzog CA, Kellum JA, McCullough PA, et al. Cardiorenal syndrome type 4: insights on clinical presentation and pathophysiology from the eleventh consensus conference of the Acute Dialysis Quality Initiative (ADQI). Contrib Nephrol 2013;182:158–73.10.1159/000349972Search in Google Scholar PubMed
12. McCullough PA, Olobatoke A, Vanhecke TE. Galectin-3: a novel blood test for the evaluation and management of patients with heart failure. Rev Cardiovasc Med 2011;12:200–10.10.3909/ricm0624Search in Google Scholar PubMed
13. Creemers EE, Pinto YM. Molecular mechanisms that control interstitial fibrosis in the pressure-overloaded heart. Cardiovasc Res 2011;89:265–72.10.1093/cvr/cvq308Search in Google Scholar
14. Cooper DN. Galectinomics: finding themes in complexity. Biochim Biophys Acta 2002;1572:209–31.10.1016/S0304-4165(02)00310-0Search in Google Scholar
15. Dumic J, Dabelic S, Flögel M. Galectin-3: an open-ended story. Biochim Biophys Acta 2006;1760:616–35.10.1016/j.bbagen.2005.12.020Search in Google Scholar PubMed
16. Krześlak A, Lipińska A. Galectin-3 as a multifunctional protein. Cell Mol Biol Lett 2004;9:305–28.Search in Google Scholar
17. Raimond J, Zimonjic DB, Mignon C, Mattei M, Popescu NC, Monsigny M, et al. Mapping of the galectin-3 gene (LGALS3) to human chromosome 14 at region 14q21-22. Mamm Genome 1997;8:706–7.10.1007/s003359900548Search in Google Scholar PubMed
18. Henderson NC, Sethi T. The regulation of inflammation by galectin-3. Immunol Rev 2009;230:160–71.10.1111/j.1600-065X.2009.00794.xSearch in Google Scholar PubMed
19. Liu YH, D’Ambrosio M, Liao TD, Peng H, Rhaleb NE, Sharma U, et al. N-acetyl-seryl-aspartyl-lysyl-proline prevents cardiac remodeling and dysfunction induced by galectin-3, a mammalian adhesion/growth-regulatory lectin. Am J Physiol Heart Circ Physiol 2009;296:H404–12.10.1152/ajpheart.00747.2008Search in Google Scholar PubMed PubMed Central
20. Sharma UC, Pokharel S, van Brakel TJ, van Berlo JH, Cleutjens JP, Schroen B, et al. Galectin-3 marks activated macrophages in failure-prone hypertrophied hearts and contributes to cardiac dysfunction. Circulation 2004;110:3121–8.10.1161/01.CIR.0000147181.65298.4DSearch in Google Scholar PubMed
21. Ho JE, Liu C, Lyass A, Courchesne P, Pencina MJ, Vasan RS, et al. Galectin-3, a marker of cardiac fibrosis, predicts incident heart failure in the community. J Am Coll Cardiol 2012;60:1249–56.10.1016/j.jacc.2012.04.053Search in Google Scholar PubMed PubMed Central
22. Djoussé L, Matsumoto C, Petrone A, Weir NL, Tsai MY, Gaziano JM. Plasma galectin 3 and heart failure risk in the Physicians’ Health Study. Eur J Heart Fail 2014;16:350–4.10.1002/ejhf.21Search in Google Scholar PubMed PubMed Central
23. Grandin EW, Jarolim P, Murphy SA, Ritterova L, Cannon CP, Braunwald E, et al. Galectin-3 and the development of heart failure after acute coronary syndrome: pilot experience from PROVE IT-TIMI 22. Clin Chem 2012;58:267–73.10.1373/clinchem.2011.174359Search in Google Scholar PubMed
24. Lin YH, Lin LY, Wu YW, Chien KL, Lee CM, Hsu RB, et al. The relationship between serum galectin-3 and serum markers of cardiac extracellular matrix turnover in heart failure patients. Clin Chim Acta 2009;409:96–9.10.1016/j.cca.2009.09.001Search in Google Scholar PubMed
25. van Kimmenade RR, Januzzi JL Jr, Ellinor PT, Sharma UC, Bakker JA, Low AF, et al. Utility of amino-terminal pro-brain natriuretic peptide, galectin-3, and apelin for the evaluation of patients with acute heart failure. J Am Coll Cardiol 2006;48:1217–24.10.1016/j.jacc.2006.03.061Search in Google Scholar PubMed
26. van der Velde AR, Gullestad L, Ueland T, Aukrust P, Guo Y, Adourian A, et al. Prognostic value of changes in galectin-3 levels over time in patients with heart failure: data from CORONA and COACH. Circ Heart Fail 2013;6:219–26.10.1161/CIRCHEARTFAILURE.112.000129Search in Google Scholar PubMed
27. Gullestad L, Ueland T, Kjekshus J, Nymo SH, Hulthe J, Muntendam P, et al. The predictive value of galectin-3 for mortality and cardiovascular events in the Controlled Rosuvastatin Multinational Trial in Heart Failure (CORONA). Am Heart J 2012;164:878–83.10.1016/j.ahj.2012.08.021Search in Google Scholar PubMed
28. Wu AH, Smith A. Biological variation of the natriuretic peptides and their role in monitoring patients with heart failure. Eur J Heart Fail 2004;6:355–8.10.1016/j.ejheart.2003.12.011Search in Google Scholar PubMed
29. Shenkman HJ, Pampati V, Khandelwal AK, McKinnon J, Nori D, Kaatz S, et al. Congestive heart failure and QRS duration: establishing prognosis study. Chest 2002;122:528–34.10.1378/chest.122.2.528Search in Google Scholar PubMed
©2014 by De Gruyter
Articles in the same Issue
- Frontmatter
- Preface
- Biomarkers in the emergency department. Handle with care
- Editorial
- Copeptin in critical illness
- Reviews and Mini Reviews
- Role of presepsin for the evaluation of sepsis in the emergency department
- Opinion paper on utility of point-of-care biomarkers in the emergency department pathways decision making
- How galectin-3 changes acute heart failure decision making in the emergency department
- Galectin-3 in diabetic patients
- Practical experience using galectin-3 in heart failure
- Novel biomarkers in acute heart failure: MR-pro-adrenomedullin
- The role of glycemia in acute heart failure patients
- Copeptin (CTproAVP), a new tool for understanding the role of vasopressin in pathophysiology
- Original Articles
- Copeptin decrease from admission to discharge has favorable prognostic value for 90-day events in patients admitted with dyspnea
- Comparison between white blood cell count, procalcitonin and C reactive protein as diagnostic and prognostic biomarkers of infection or sepsis in patients presenting to emergency department
- Procalcitonin in early rule-in/rule-out of sepsis in SIRS patients admitted to a medical ward
- May thrombopoietin be a useful marker of sepsis severity assessment in patients with SIRS entering the emergency department?
- Bleeding prevalence and transfusion requirement in patients with thrombocytopenia in the emergency department
- Acute metformin intoxication: 2012 experience of Emergency Departement of Lodi, Italy
- Structural myocardial alterations in diabetes and hypertension: the role of galectin-3
- A new device for the prompt diagnosis of urinary tract infections
Articles in the same Issue
- Frontmatter
- Preface
- Biomarkers in the emergency department. Handle with care
- Editorial
- Copeptin in critical illness
- Reviews and Mini Reviews
- Role of presepsin for the evaluation of sepsis in the emergency department
- Opinion paper on utility of point-of-care biomarkers in the emergency department pathways decision making
- How galectin-3 changes acute heart failure decision making in the emergency department
- Galectin-3 in diabetic patients
- Practical experience using galectin-3 in heart failure
- Novel biomarkers in acute heart failure: MR-pro-adrenomedullin
- The role of glycemia in acute heart failure patients
- Copeptin (CTproAVP), a new tool for understanding the role of vasopressin in pathophysiology
- Original Articles
- Copeptin decrease from admission to discharge has favorable prognostic value for 90-day events in patients admitted with dyspnea
- Comparison between white blood cell count, procalcitonin and C reactive protein as diagnostic and prognostic biomarkers of infection or sepsis in patients presenting to emergency department
- Procalcitonin in early rule-in/rule-out of sepsis in SIRS patients admitted to a medical ward
- May thrombopoietin be a useful marker of sepsis severity assessment in patients with SIRS entering the emergency department?
- Bleeding prevalence and transfusion requirement in patients with thrombocytopenia in the emergency department
- Acute metformin intoxication: 2012 experience of Emergency Departement of Lodi, Italy
- Structural myocardial alterations in diabetes and hypertension: the role of galectin-3
- A new device for the prompt diagnosis of urinary tract infections