Cullen Sign and Grey Turner Sign Revisited
-
William F. Wright

Abstract
Cullen sign and Grey Turner sign, named after Thomas Stephen Cullen, MB, and George Grey Turner, MBBS, respectively, are signs of abdominal wall hemorrhage and are generally associated with acute pancreatitis. However, the research from which these signs arose was documented long before Cullen and Grey Turner made their contributions. The present article examines the history, pathologic mechanisms, and clinical application of these signs in relation to acute pancreatitis and ectopic pregnancy.
Given the prominence of Thomas Stephen Cullen, MB, and George Grey Turner, MBBS, in the history of clinical medicine, one is inclined to believe that the 2 principal physical examination signs (Figure 1) that bear their names—periumbilical ecchymosis (Cullen sign) and flank ecchymosis (Grey Turner sign)—were identified solely by these 2 men. However, the ideas from which these signs arose were documented by others long before Cullen and Grey Turner made their contributions. Cullen and Grey Turner are names for common physical examination signs of abdominal wall hemorrhage, also known as rectus abdominis subfascial bleeding. To provide appropriate and timely interventions, it is important that health care providers—particularly primary care and emergency physicians, general and colorectal surgeons, obstetricians, and gastroenterologists—have a thorough, evidenced-based understanding of these signs in terms of historical evolution, anatomy, pathophysiologic and epidemiologic processes, and associated medical conditions.

(A) Periumbilical ecchymosis (Cullen sign) and
(B) flank ecchymosis (Grey Turner sign). Published with permission from Chung and Chuang.1
Early Historical Concepts of Abdominal Wall Hemorrhage
One might assume that Cullen sign and Grey Turner sign emerged not long after clinicians recognized that physical examination findings could be used to ferret out disease among the many aches and minor perturbations of otherwise healthy existence. But, in fact, such observations seem to have been used as a means of distinguishing health from disease for as long as humans have committed thoughts to writing. There are, for example, written accounts of spontaneous rectus abdominis subfascial bleeding traced as far back as the writings of Hippocrates, Claudius Galen, and Leonardo da Vinci.2-4 The earliest published account of this condition in the United States was written by Samuel Bainbridge Richardson4 in 1857 in his description of a healthy 28-year-old man. In 1882, Czechoslovakian surgeon Karl Maydl provided accurate descriptions of this condition, as well as an extensive review of literature covering 14 cases between 1809 and 1880.6
Since that time, many cases of abdominal wall bleeding have been described using terms such as spontaneous hematoma of the abdominal wall, spontaneous hematoma of the rectus sheath, and spontaneous rupture of the epigastric artery.7 Spontaneous abdominal wall hemorrhage offers the best example of early notions of abdominal wall bleeding; however, this clinical finding is distinct from Cullen sign and Grey Turner sign, which also indicate abdominal wall bleeding. An important distinction is that neither Cullen nor Grey Turner intended these signs to be indicators of intra-abdominal pathology.
Abdominal Wall Hemorrhage Associated With Intra-abdominal Pathology
Abdominal wall hemorrhage has been reported after trauma, subcutaneous drug injection, and paracentesis, and it has been reported to occur spontaneously during pregnancy and biliary tract disease. However, the first description of isolated periumbilical discoloration as a result of intra-abdominal pathology was made by American surgeon Joseph Louis Ransohoff in 1906 in his account of a 53-year-old man with a ruptured common bile duct and bile peritonitis.8 Ransohoff wrote,
On inspection of the abdomen, attention was called to a marked jaundice of the umbilicus. The navel was of distinct saffron-yellow color in strong contrast with the rest of the skin over the abdomen.8
Six years later, Grey Turner reported the observation of “a bluish color appearance of the abdominal wall surrounding the umbilicus” in a 54-year-old woman with acute pancreatitis.9 He later described abdominal wall discoloration of the flanks in a 53-year-old man with acute pancreatitis, as follows9:
The tenderness over the gall-bladder region was very marked, and I now noticed two large discolored areas in the loins. They were about the size of the palm of the hand, slightly raised above the surface, and of a dirty-greenish color. There was a little edema, with pitting on pressure, but there was no pain or tenderness.
In 1918, Cullen presented a paper entitled, “A new sign in ruptured extrauterine pregnancy,”10 in which he reported periumbilical “bluish-black” discoloration in a 38-year-old woman in association with a ruptured ectopic pregnancy. Although it is historically associated with ruptured ectopic pregnancy, Cullen sign has also been described in association with acute pancreatitis and other clinical conditions such as rectus sheath hematoma,11 splenic rupture in infectious mononucleosis,12 portal hypertension,13 amoebic liver abscess,14 metastatic thyroid cancer,15 metastatic esophageal cancer,16 and non-Hodgkin lymphoma.17 Current prominent clinical manuals such as Harrison’s Principles of Internal Medicine and Cecil’s Textbook of Internal Medicine describe both Cullen sign and Grey Turner sign in association with severe acute pancreatitis, and it is now customary for medical students, resident physicians, and attending physicians to associate one with the other.
Pathophysiologic Process of Cullen Sign and Grey Turner Sign
The notion of blood within the abdominal wall as a result of pancreatic inflammatory products has been promulgated to account for the development of Cullen sign and Grey Turner sign. In 1953, surgeons Elbert T. Phelps and Richard A. Lemmer described a case of hemorrhagic pancreatitis in a 34-year-old man who developed Grey Turner sign on the left flank.18 A biopsy of the left flank lesion demonstrating the greatest discoloration was taken on hospital day 7 and revealed…
… edema of the subcutaneous tissue with a moderate amount of perivascular infiltration of lymphocytes around some of the smaller vessels, but there was no evidence of vascular lesions or tissue necrosis.18
In 1958, nationally known academic obstetrician James A. Merrill reported the histologic findings of a 43-year-old woman with Cullen sign.19 Microscopic examination of the biopsy demonstrated intact erythrocytes within all tissue planes and most pronounced in the striated muscles, superficial adipose tissue, and surrounding dermal sweat glands. Erythrocytes were not found filling lymphatics. While hemosiderin deposition occurred within the dermis, vascular endothelial components were intact.
In another case report, Meyers et al20 used computed tomographic images of 4 patients presenting with acute pancreatitis to posit pathways leading to the development of Cullen sign and Grey Turner sign in 1989. According to their findings, Grey Turner sign may result from anatomical defects of the transversalis fascia, which may serve as a structural predisposition allowing direct extension of hemorrhagic fluid from the anterior pararenal space (via the 2 leaves of the posterior renal fascia) to the lateral edge of the quadratus lumborum muscle. Cullen sign may develop secondary to an inflamed gastrohepatic ligament allowing direct extension of hemorrhagic fluid across the falciform ligament to the periumbilical anterior abdominal wall.
Based on these findings, it is thought that both signs occur as a result of hemorrhagic fluid tracking from retroperitoneal regions along fascial planes, thus permitting access to the abdominal wall musculature and subsequent periumbilical or flank tissues.18-20 Skin discoloration results from the accumulation of blood within the subcutaneous fascial planes.18-20 Variation of color between green, yellow, and purple is based on the stage of red blood cell breakdown.18-20
Evidence of The Accuracy of Cullen Sign and Grey Turner Sign
Despite their long history, Cullen sign and Grey Turner sign are considered to be relatively uncommon. In a collective review of 6063 patients with ectopic pregnancy between 1941 and 1955, Merrill19 reported Cullen sign was observed in only 4 patients (0.06%). In a retrospective study to examine the clinical spectrum of acute pancreatitis and identify factors related to life-threatening complications, Jacobs et al21 reported that of 519 patients from December 1963 through April 1969, Grey Turner sign occurred in 5 (0.96%) and Cullen sign occurred in 4 (0.77%). The associated mortality rate of patients presenting with these signs was reported between 50% to 60%. In a randomized, double-blinded trial involving 257 patients evaluating the effects of aprotinin and glucagon on the course of acute pancreatitis, it was reported that Grey Turner sign was observed in only 2 patients (0.78%).22 Finally, in a prospective evaluation of 770 patients admitted to the Glasgow Royal Infirmary for acute pancreatitis between January 1971 and March 1983, Dickson and Imrie23 reported 9 patients (1.17%) with Grey Turner sign, 9 patients (1.17%) with Cullen sign, and 5 patients (0.65%) with both signs. In this cohort, these signs most commonly appeared on hospital day 4 and had a female to male ratio of 3:1, with an associated mortality rate of 37%.23
Conclusion
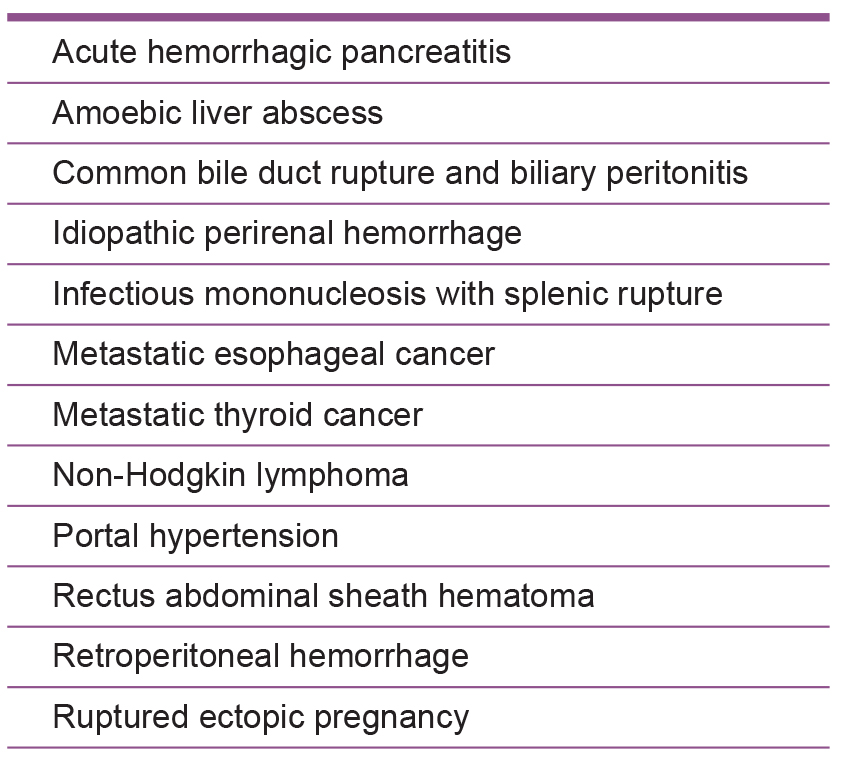
Based on the review of the literature, it is evident that Cullen sign and Grey Turner sign are neither sensitive nor specific for acute pancreatitis. Further, Cullen sign is neither sensitive nor specific for ectopic pregnancy, for which it was originally ascribed. Therefore, it may be best to revise the teaching of these signs from cardinal manifestations of acute pancreatitis and ectopic pregnancy to conditions associated with abdominal pathology and retroperitoneal hemorrhage (Figure 2). This revised teaching would be best given with continued emphasis on the bedside examination of patients through all years of training and beyond. The medical profession should continue to refine its understanding of Cullen sign and Grey Turner sign, along with other physical signs, and carefully examine their operating characteristics. Medical educators must also urge their trainees to do the same.
References
1. Chung KM ,ChuangSS.Cullen and Grey Turner signs in idiopathic perirenal hemorrhage.CMAJ. 2011;183(16):E1221. doi:10.1503/cmaj.101548.10.1503/cmaj.101548Search in Google Scholar PubMed PubMed Central
2. Payne RL. Spontaneous rupture of the superior and inferior epigastric arteries within the abdominis sheath. Ann Surg . 1938;108(4):757-68.10.1097/00000658-193810000-00019Search in Google Scholar PubMed PubMed Central
3. Cohn H ,HoffmanW,GoldnerMG. Spontaneous hemorrhage within the rectus sheath; report of a case. N Engl J Med . 1953;249(27):1115-1116.10.1056/NEJM195312312492706Search in Google Scholar PubMed
4. Parker WS ,ChristiansenKH. Rupture of the rectus abdominis muscle with hematoma. Arch Surg . 1960;81:655-659.10.1001/archsurg.1960.01300040139027Search in Google Scholar PubMed
5. Richardson SB. Rupture of the right rectus abdominis muscle from muscular efforts: operation and recovery, with remarks. Am J Med Sci . 1857;33:41-45.10.1097/00000441-185701000-00004Search in Google Scholar
6. Maydl K. Ueber subcutane Muskel- und Sehnenzerreissungen, sowie Rissfracturen. Deutsche Zeitschr f Chir . 1882;17:306.10.1007/BF02794061Search in Google Scholar
7. Jackson PP, GrayEJ. Abdominal-wall hematomas. Arch Surg . 1966;92(2):194-197.10.1001/archsurg.1966.01320200034006Search in Google Scholar PubMed
8. Ransohoff J. Gangrene of the gall bladder: rupture of the common bile duct, with a new sign. JAMA. 1906;46(6):395-397.10.1001/jama.1906.62510330001001Search in Google Scholar
9. G rey-Turner G. Local discoloration of the abdominal wall as a sign of acute pancreatitis. Br J Surg. 1919;394-395.10.1002/bjs.1800072711Search in Google Scholar
10. Cullen TS. A new sign in ruptured extrauterine pregnancy. Am J Obstet Gynecol. 1918;78:457-460.Search in Google Scholar
11. Guthrie CM , StanfeyHA. Rectus sheath haematoma presenting with Cullen’s sign and Grey-Turner’s sign. Scott Med J. 1996;41(2):54-55.10.1177/003693309604100207Search in Google Scholar PubMed
12. Warwick RJ , WeeB, KirkpatrickD, FinneganOC. Infectious mononucleosis, ruptured spleen and Cullen’s sign. Ulster Med J. 2003;72(2):111-113.Search in Google Scholar
13. Chauhan S , GuptaM, SachdevA, D’CruzS, KaurI. Cullen’s and Turner’s sign associated with portal hypertension. Lancet. 2008;372(9632):54. doi:10.1016/S0140-6736(08)60993-9.10.1016/S0140-6736(08)60993-9Search in Google Scholar
14. Misra A , AgrahariD, GuptaR. Cullen’s sign in amoebic liver abscess. Postgrad Med J. 2002;78(921):427-428.10.1136/pmj.78.921.427Search in Google Scholar PubMed PubMed Central
15. Marinella MA. Cullen’s sign associated with metastatic thyroid cancer. N Engl J Med. 1999;340(2):149-150.10.1056/NEJM199901143400214Search in Google Scholar PubMed
16. Marinella MA , BaumannM. Cullen’s sign associated with metastatic esophageal carcinoma. J Hosp Med. 2008;3(3):277-278.10.1002/jhm.300Search in Google Scholar PubMed
17. Silvestre JF , JoverR, BetllochI, CarnicerF, BanulsJ, Perez-MateoM. Cullen’s sign secondary to intra-abdominal non-Hodgkin’s lymphoma. Am J Gastroenterology. 1996;91(5):1040-1041.Search in Google Scholar
18. Phelps ET , LemmerRA. Acute hemorrhagic pancreatitis with Grey-Turner’s sign and elevated urinary amylase; a case report. Bull Georgetown Univ Med Cent. 1953;6(3):64-70.Search in Google Scholar
19. Merrill JA. Cullen’s sign: a historical review and report of histologic observations. Obstet Gynecol. 1958;12(3):317-324.Search in Google Scholar
20. Meyers MA , FeldbergMA, OliphantM. Grey Turner’s sign and Cullen’s sign in acute pancreatitis. Gastrointest Radiol. 1989;14(1):31-37.10.1007/BF01889150Search in Google Scholar PubMed
21. Jacobs ML , DaggettWM, CivetteJM, et al.. Acute pancreatitis: analysis of factors influencing survival. Ann Surg. 1977;185(1):43-51.10.1097/00000658-197701000-00007Search in Google Scholar PubMed PubMed Central
22. Morbidity of acute pancreatitis: the effects of aprotinin and glucagon. Gut. 1980;21(4):334-339.10.1136/gut.21.4.334Search in Google Scholar PubMed PubMed Central
23. Dickson AP , I mrieCW. The incidence and prognosis of body wall ecchymosis in acute pancreatitis. Surg Gynecol Obstet. 1984;159(4):343-347.Search in Google Scholar
© 2016 American Osteopathic Association
This work is licensed under the Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
Articles in the same Issue
- AOA COMMUNICATION
- Official Call: 2016 Annual Business Meeting of the American Osteopathic Association
- Proposed Amendments to the AOA Constitution, Bylaws, and Code of Ethics
- ORIGINAL CONTRIBUTION
- Glycated Hemoglobin Testing to Identify Undiagnosed Diabetes Mellitus in the Inpatient Setting
- Correlation of Somatic Dysfunction With Gastrointestinal Endoscopic Findings: An Observational Study
- BRIEF REPORT
- Cancer Mortality Trends in Medically Underserved Counties in Virginia
- REVIEW
- Comprehensive Evaluation for Obesity: Beyond Body Mass Index
- MEDICAL EDUCATION
- Ten Tips for Maximizing the Effectiveness of Emergency Medicine Procedure Laboratories
- Osteopathic Manipulative Treatment Technique Scores on the COMLEX-USA Level 2-PE: An Analysis of the Skills Assessed
- SPECIAL COMMUNICATION
- Cullen Sign and Grey Turner Sign Revisited
- CASE REPORT
- Disseminated Varicella-Zoster Virus After Vaccination in an Immunocompetent Patient
- CLINICAL IMAGES
- Gout Flare With a Draining Tophus
Articles in the same Issue
- AOA COMMUNICATION
- Official Call: 2016 Annual Business Meeting of the American Osteopathic Association
- Proposed Amendments to the AOA Constitution, Bylaws, and Code of Ethics
- ORIGINAL CONTRIBUTION
- Glycated Hemoglobin Testing to Identify Undiagnosed Diabetes Mellitus in the Inpatient Setting
- Correlation of Somatic Dysfunction With Gastrointestinal Endoscopic Findings: An Observational Study
- BRIEF REPORT
- Cancer Mortality Trends in Medically Underserved Counties in Virginia
- REVIEW
- Comprehensive Evaluation for Obesity: Beyond Body Mass Index
- MEDICAL EDUCATION
- Ten Tips for Maximizing the Effectiveness of Emergency Medicine Procedure Laboratories
- Osteopathic Manipulative Treatment Technique Scores on the COMLEX-USA Level 2-PE: An Analysis of the Skills Assessed
- SPECIAL COMMUNICATION
- Cullen Sign and Grey Turner Sign Revisited
- CASE REPORT
- Disseminated Varicella-Zoster Virus After Vaccination in an Immunocompetent Patient
- CLINICAL IMAGES
- Gout Flare With a Draining Tophus