Sarcoidosis Presenting as an Epididymal Mass
-
Wayne D. Hey

Abstract
Sarcoidosis is a multisystem inflammatory disease that characteristically involves the lungs and lymph nodes. Involvement of the genitourinary system is rare. We report the case of a 39-year-old African American man who presented with an asymptomatic right-sided epididymal mass and underwent partial epididymectomy. Pathologic analysis revealed numerous noncaseating granulomas. Results from computed tomography imaging of the chest and lung biopsy were consistent with sarcoidosis.
Sarcoidosis is a systemic, multiorgan, granulomatous disorder of idiopathic etiologic process characterized by epithelioid, noncaseating granulomas. It most frequently involves the lungs, skin, eyes, or liver. In the United States, lifetime risk of sarcoidosis is up to 2.4%, with disease risk higher in women and African Americans.1
The disease is localized to the chest in 84% of patients2 and causes common pulmonary symptoms such as cough, dyspnea, and pleuritic chest pain. Involvement of the genitourinary system is extremely rare, accounting for only 0.2% of all clinically diagnosed cases of sarcoidosis—5% of which are diagnosed at autopsy.3
In the present report, we describe an African American patient who presented with a right epididymal mass. Pathologic evaluation of the excised mass and results from imaging studies confirmed the diagnosis of sarcoidosis.
Report of Case
A 39-year-old African American man presented to our office for evaluation of an asymptomatic right-sided epididymal mass. He noticed the lesion during a self-examination 2 months earlier. The patient denied any systemic symptoms or recent exposure to toxins or pathogens. His family history was clinically significant for a brother with a history of sarcoidosis.
Physical examination revealed a 2-cm, well-circumscribed, painless mass in the superior portion of the right epididymis. Findings from the remainder of the physical examination were normal (blood pressure, 113/67 mm Hg; body temperature, 97.8°F; pulse rate, 71 beats per min). Results from scrotal ultrasonography revealed a hypoechoic lesion on the right epididymis. Preoperative laboratory work of α-fetoprotein, β-human chorionic gonadotropin, and lactate dehydrogenase did not reveal abnormalities.
As a result of patient concern and for diagnostic purposes, scrotal exploration occurred with excision of the right epididymal mass via a median-raphe scrotal incision. Gross findings revealed a 2.3 × 1.6 × 1.1 cm gray-tan, firm oval epididymal mass (Figure 1). Pathologic evaluation exposed noncaseating granulomas. Acid-fast and hematoxylin and eosin stains were negative for acid-fast and fungal micro-organisms (Figure 2), suggesting the presence of sarcoidosis.
After surgical removal of the mass, the patient had a computed tomography scan of the chest and lung biopsy, which revealed bilateral hilar lymphadenopathy consistent with sarcoidosis. These findings concurred with the diagnosis of sarcoidosis.
The patient had an uneventful postoperative recovery and was treated with nonsteroidal anti-inflammatory medications.
Comment
As previously stated, involvement of the genitourinary system with sarcoidosis is rare. In 1936, Schaumann4 published the first case of testicular sarcoidosis. Since then, sarcoid granulomas have been reported in the prostate,5,6 testes,7,8 and epididymis,3,9 with the latter being most common.10 Involvement of the penis, scrotum, and spermatic cord are rare.10 According to a 2005 report, and including the present report, 62 cases of histologically proven sarcoidosis involving the male reproductive tract (including the epididymis, testes, spermatic cord, tunica albuginea, and prostate) have been reported.11
Urogenital sarcoidosis is 10 times more common in African American men than in white men.12 Genitourinary manifestations of sarcoidosis include kidney disease with nephrocalcinosis, painless testicular masses (as discussed in the present report), and epididymo-orchitis with associated testicular swelling. Lesions are typically unilateral—bilateral lesions account for less than one-third of patients with epididymal sarcoidosis.9

Median-raphe scrotal incision used to excise an epididymal mass in a 39-year-old African American man. The mass was 2.3 × 1.6 × 1.1 cm, oval shaped, and firm.
Other systemic inflammatory conditions such as tuberculosis can also affect the epididymis. The genitourinary tract is involved in 20% of patients with extrapulmonary tuberculosis, with the epididymis being the most common site of genital organ involvement.13 Because epididymal tuberculosis can cause infertility, men with a history of chronic epididymitis should be monitored. In patients with epididymal masses, physicians should have a high index of suspicion for the presence of epididymal tuberculosis and sarcoidosis. Physicians should also document the differential diagnosis so that systemic treatment can be provided. Underlying masses in the epididymis may represent systemic illness and must be treated as such.
Treatment for patients with genitourinary sarcoidosis is controversial. Although corticosteroid therapy can cause sarcoidosis to regress,1,7 spontaneous resolution has occurred.14 In most cases of epididymal sarcoidosis, excisional biopsy is required for diagnostic and therapeutic purposes. In addition, these lesions can often be difficult to differentiate from malignancy based on ultrasonography findings. Therefore, resection should be favored in any equivocal cases. In patients with known sarcoidosis, a trial of corticosteroids may resolve the condition.1 In patients with fertility concerns, excisional or needle biopsy may also be considered.
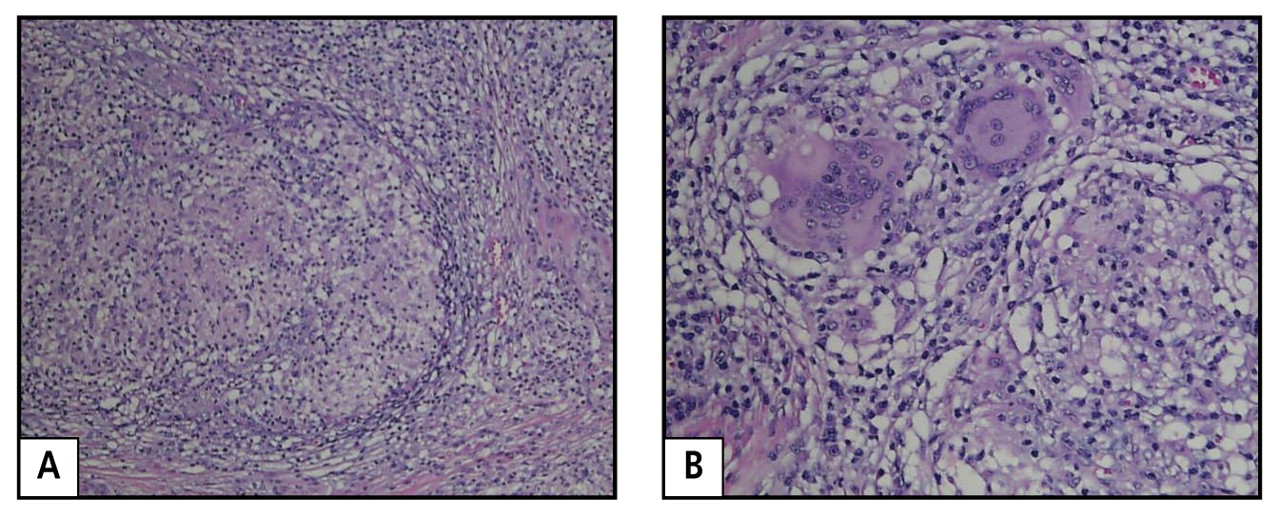
Pathologic evaluation of the epididymal mass from a 39-year-old African American man revealed noncaseating granuloma (A; hematoxylin and eosin stain ×10). Higher power view (B; hematoxylin and eosin stain ×40) exposed multinucleated giant cells seen within a noncaseating granuloma. These findings, in addition to those from a computed tomography scan of the chest and lung biopsy, confirmed a diagnosis of sarcoidosis.
Conclusion
For patients—particularly African American men—presenting with an epididymal or genitourinary mass, physicians must remember to include sarcoidosis in the differential diagnosis.
1 Statement on sarcoidosis. Joint Statement of the American Thoracic Society (ATS), the European Respiratory Society (ERS) and the World Association of Sarcoidosis and Other Granulomatous Disorders (WASOG) adopted by the ATS Board of Directors and by the ERS Executive Committee, February 1999. Am J Respir Crit Care Med. 1999;160:736-755. http://ajrccm.atsjournals.org/cgi/content/full/160/2/736. Accessed October 14, 2009.Search in Google Scholar
2 Roos N, Bick U, Vassallo P, Diederich S, Müller-Miny H, Auffermann W, et al. Thoracic sarcoidosis [review] [in German]. Radiologe. 1990;30:581-590.Search in Google Scholar
3 Svetec DA, Waguespack RL, Sabanegh ES Jr. Intermittent azoospermia associated with epididymal sarcoidosis. Fertil Steril. 1998;70:777-779.10.1016/S0015-0282(98)00272-6Search in Google Scholar
4 Schaumann J. Lymphogranulomatosis benigna in the light of prolonged clinical observations and autopsy findings. Br J Dermatol. 1936;48:399 .10.1111/j.1365-2133.1936.tb10366.xSearch in Google Scholar
5 Mulpuru SK, Gujja K, Pai VM, Chen CY, Levey RL. A rare and unusual cause of PSA (prostate-specific antigen) elevation: sarcoidosis of the prostate [case report]. Am J Med Sci. 2008;335:246-248.10.1097/MAJ.0b013e31811eba71Search in Google Scholar
6 Furusato B, Koff S, McLeod DG, Sesterhenn IA. Sarcoidosis of the prostate [case report]. J Clin Pathol. 2007;60:325-326.10.1136/jcp.2006.039222Search in Google Scholar
7 Datta SN, Freeman A, Amerasinghe CN, Rosenbaum TP. A case of scrotal sarcoidosis that mimicked tuberculosis. Nat Clin Pract Urol. 2007;4:227-230. http://www.nature.com/nrurol/journal/v4/n4/full/ncpuro0777.html. Accessed October 12, 2009.Search in Google Scholar
8 Wong JA, Grantmyre J. Sarcoid of the testis. Can J Urol. 2006;13:3201-3203.Search in Google Scholar
9 Gerstenhaber BJ, Green R, Sachs FL. Epididymal sarcoidosis: a report of two cases and a review of the literature. Yale J Biol Med. 1977;50:669-675. http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2595577/?tool=pubmed. Accessed October 7, 2009.Search in Google Scholar
10 Vasu TS, Lai RS, Amzuta IG, Nasr MR, Lenox RJ. Sarcoidosis presenting as intrascrotal mass: case report and review. South Med J. 2006;99:995-997.10.1097/01.smj.0000224127.65377.07Search in Google Scholar
11 Rehman J, Rizkala ER, Chughtai B, Khan SA. Hypoechoic testicular mass: a case of testicular and epididymal sarcoidosis. Urology. 2005;66:657 .10.1016/j.urology.2005.03.008Search in Google Scholar
12 Ricker W, Clark M. Sarcoidosis: a clinical pathologic review of 300 cases, including 22 autopsies. Am J Clin Pathol. 1949;19:725 .10.1093/ajcp/19.8.725Search in Google Scholar
13 Porter MP, Eubank WB, Krieger JN. Genitourinary tuberculosis: a focused update for the practicing urologist. Contemp Urol. 2001;13:34-48.Search in Google Scholar
14 Ryan DM, Lesser BA, Crumley LA, Diederich S, Müller-Miny H, Auffermann W, et al. Epididymal sarcoidosis [review]. J Urol. 1993;149:134-136.10.1016/S0022-5347(17)36023-8Search in Google Scholar
The American Osteopathic Association
This work is licensed under the Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
Articles in the same Issue
- LETTERS
- Billing and Coding for OMT
- BOOK REVIEWS
- Manipulation in Motion: A Video Companion to A Pocket Manual of OMT [DVD]
- Medicare for Baby Boomers & Beyond
- CORRECTIONS
- Corrections
- EDITORIALS
- Realigning the JAOA to Sharpen Our Focus
- MEDICAL EDUCATION
- Clearly Distinct: Outcomes of Initiative to Increase Integration of Osteopathic Principles and Practice at West Virginia School of Osteopathic Medicine
- Student Performance on Levels 1 and 2-CE of COMLEX-USA: Do Elective Upper-Level Undergraduate Science Courses Matter?
- REVIEWS
- Nutritional Deficiencies After Gastric Bypass Surgery
- CASE REPORTS
- Osteopathic Manipulative Treatment in the Management of Notalgia Paresthetica
- Sarcoidosis Presenting as an Epididymal Mass
Articles in the same Issue
- LETTERS
- Billing and Coding for OMT
- BOOK REVIEWS
- Manipulation in Motion: A Video Companion to A Pocket Manual of OMT [DVD]
- Medicare for Baby Boomers & Beyond
- CORRECTIONS
- Corrections
- EDITORIALS
- Realigning the JAOA to Sharpen Our Focus
- MEDICAL EDUCATION
- Clearly Distinct: Outcomes of Initiative to Increase Integration of Osteopathic Principles and Practice at West Virginia School of Osteopathic Medicine
- Student Performance on Levels 1 and 2-CE of COMLEX-USA: Do Elective Upper-Level Undergraduate Science Courses Matter?
- REVIEWS
- Nutritional Deficiencies After Gastric Bypass Surgery
- CASE REPORTS
- Osteopathic Manipulative Treatment in the Management of Notalgia Paresthetica
- Sarcoidosis Presenting as an Epididymal Mass