Stability of Ready-to-Administer and Ready-to-Use Epinephrine and Norepinephrine Injection Solutions
-
Rita Marina Heeb
Rita Marina Heeb studied pharmacy at Johann Wolfgang Goethe University in Frankfurt, Germany. Since 2012 she is Head of Quality Control at the Department of Pharmacy of Johannes Gutenberg-University Medical Center Mainz, Germany. She has completed her doctoral thesis in Clinical Pharmacy entitled: “Compliance – and Quality of life measurements at dialysis and liver cirrhosis patients before transplantation” at Johannes-Gutenberg-University Mainz. Her research interests include monitoring of medication adherence and physicochemical stability of pharmaceuticals.
 ,
Bettina Stollhof
,
Bettina Stollhof
Bettina Stollhof studied pharmacy at Johannes Gutenberg-University in Mainz, Germany. She is working at the Pharmacy Department of the Medical Center of Johannes Gutenberg-University Hospital since 2006. She has completed her doctoral thesis in Clinical Pharmacy entitled: “Optimization of Phenprocoumon-dosis by intensive medical-pharmaceutical care” at Johannes-Gutenberg-University Mainz. Her research interests include aseptic drug preparation, infusion management: incompatibilities-reducing infusion schemes and ready-to-use parenteral solutions.
Julia Reichhold is working at the Pharmacy Department of the University Medical Center of Johannes Gutenberg-University Hospital in Mainz since 2010. In 2013 she completed her doctoral thesis entitled: Influence of single units of solid oral medication on drug therapy safety, information and satisfaction of inhouse patients in an open, controlled, prospective, multicenter patient study. The medication of choice in single units was Diovan®, CoDiovan® and Amlodipin. Her special interests and research projects include aseptic drug preparation and drug therapy safety.
Judith Thiesen is working at the Pharmacy Department of the University Medical Center of Johannes Gutenberg-University Hospital in Mainz since 1997. In 2001 she completed her doctoral thesis entitled: Evidence-based optimization of parenteral drug application for oncological patients: incompatibilities-reducing infusion schemes, stability of ready-to-use parenteral solutions of camptothecin-derivatives and taxanes. Her special interests and research projects include aseptic drug preparation, quality control, total quality management as well as physicochemical and microbiological stability of parenteral drug solutions.
Irene Krämer is currently Director of the Pharmacy Department, University Medical Center, Johannes Gutenberg-University Hospital, Mainz and is also a Professor for clinical pharmacy at the Pharmacy School of Johannes Gutenberg-University. She completed her postdoctoral thesis in Pharmaceutical Technology entitled: Development, quality assurance, and optimization of ready-to-use parenteral solutions in the integrated cancer care concept. Her special interests include oncology pharmacy, infectious diseases and aseptic drug preparation. She is doing research projects in the field of physicochemical and microbiological stability of cytotoxic drugs, compatibility of admixtures of nebulizer solutions and monitoring of medication compliance.

Abstract
Background
In the University Medical Centre Mainz, standard concentrations are defined for medicinal products to be administered by continuous injection with syringe pumps in adult intensive care patients. The objective of this study was to evaluate the physicochemical stability of ready-to-use and ready-to-administer preparations containing Epinephrine (E) and Norepinephrine (NE) in standardized concentrations and prepared batch wise in the pharmacy department as basis for assigning shelf-lives.
Methods
E 20 µg/mL and NE 10 µg/mL in disposable syringes and NE 40, 100, 200, 400 µg/ml in 50 ml amber type I glass vials were prepared batch wise and the concentrations were analyzed by stability-indicating, validated reversed-phase HPLC-PDA assays. Test solutions for long-term stability studies were stored under refrigeration (2–8 °C) for 6–12 months or at elevated temperatures (21–27 °C) light protected for up to 6 months or without light protection for up to one month. Osmolality and pH were measured on predefined intervals.
Results
The concentrations of E in 50 mL syringes and NE in 10 mL syringes remained unchanged over a period of 6 months when stored at 2–8 °C. NE preparations of different concentrations prepared in amber glass vials remained stable over a study period of 12 months. At RT the shelf-life decreased to about 6 months and the exposure to mixed daylight at RT caused loss of stability in only few days.
Conclusions
Batch wise preparation of ready-to-administer (RTA) preparations containing 20 µg/mL E or 10 µg/mL NE in disposable syringes as well as ready-to-use (RTU) preparations containing 40, 100, 200 and 400 µg/mL NE was successfully implemented in a pharmacy department. Storage of the preparations at refrigerated temperatures is required to obtain acceptable shelf-lives of 6–12 months. Elevated temperatures and especially exposure to mixed daylight significantly decreased the shelf life.
Introduction
Catecholamines, such as epinephrine (E) or norepinephrine (NE) are potent α-symptomimetic drugs preferably used in emergency cases and intensive care patients for the treatment of hypotension, shock and cardiac arrest. Injection solutions in ampoules or vials marketed in Germany (Suprarenin®, Arterenol®) contain 1 mg/mL (1:1000) of E or NE as active substance. Prior to intravenous administration the products are to be diluted with 5 % glucose infusion solution. E and NE injection solutions are categorized as high alert medication causing significant patient harm when used in error [1]. Medication errors have occurred due to confusion of the appropriate concentrations to be administered and erroneous performance of the dilution process [1]. To lower the error risk it is common sense that standard concentrations should be defined for medicinal products, especially when they are administered by continuous injection with syringe pumps. Patient individual dosing can be achieved by adjusting the injection rate. In order to increase patient safety and decrease the delay caused by dilution of the medicine in emergency cases, the hospital pharmacy can produce ready-to-use and ready-to-administer preparations. A ready-to-administer preparation (RTA) presents the medicinal product at the required concentration and volume in the final container such as syringe. A ready-to-use preparation (RTU) presents the medicinal product at the required concentration and volume in a container. The content has to be transferred to a final administration device such as syringe, infusion bag for administration to the patient. The concept of standard concentrations in pre-filled containers has been successfully implemented in the University Medical Center Mainz for the treatment of adult patients. Various E and NE containing RTA preparations in syringes and RTU preparations in amber glass vials are produced batch wise in the pharmacy department and supplied to the wards. According to the German law batch wise preparation is possible without a manufacturing license if the preparations are exclusively used in the hospital where the pharmacy department is belonging to. However, quality and safety of the preparations must be ensured by following the Good Preparation regulations [2, 3] and using validated procedures and accurate documentation for the process and quality control. The extent to which quality control tests of the finished product are performed should take stability information into account. Stability studies are to be performed to determine shelf-lives and usage periods. Catecholamines degrade rapidly via oxidative reactions which are catalyzed by oxygen, pH>6, heavy metal ions, heat and UV-Vis. Well known degradation products are adrenochrome and noradrenochrome [4, 5]. However, there are no acceptance limits defined for the content of degradation products in the relevant monographies of the Ph. Eur. and the USP [6, 7].
The degradation rates of individual catecholamines vary and NE is more stable than E. The degradation rates of licensed E and NE injection solutions may vary according to the amount of antioxidative agent (e. g. sodium metabisulfite), pH, and type of container used. Moreover, temperature and the extent of light exposure are to be considered during storage and use of the medicinal products. A review of stability studies regarding E and NE injection solutions and the influence of dilution and concentration of excipients was recently published by Hoellein et al. [5]. The objective of our study was to evaluate the physicochemical stability of RTA and RTU preparations containing E and NE in standardized concentrations and prepared batch wise in the Pharmacy Department of the University Medical Center Mainz as basis for assigning shelf-lives.
Materials and methods
Aseptic preparation of Epinephrine 20 µg/mL and Norepinephrine 10 µg/mL ready-to-administer injection solution
E injection solution 20 µg/mL (i. e. 24 µg/mL E hydrochloride) in 50 mL syringes and NE injection solution 10 µg/mL (i. e. NE hydrochloride 12.2 µg/mL) in 10 mL syringes were aseptically prepared batch wise in the aseptic preparation facility of the Pharmacy Department of the University Medical Center Mainz according to the Good Preparation Guide PIC/S PE 010–4 Annex 1 (Aseptic processing) and the German Pharmacy Ordinance [2, 3]. End product control and release were performed according to the German Pharmacy Ordinance. For further information see Table 1.
Details of the formulation and processing of E and NE products.
| Preparation | Aseptic preparation of Epinephrine 20 µg/mL ready-to-administer injection solution in 50 mL syringes | Aseptic preparation of Norepinephrine 10 µg/mL ready-to-administer injection solution in 10 mL syringes | Manufacture of Norepinephrine injection solution 100 µg/mL, 200 µg/mL, 400 µg/mL in 50 mL glass vials |
|---|---|---|---|
| Batch size | 80 x 50 mL (4000 mL) | 400 x 10 mL (4000 mL) | Test batches of 100×50 mL |
| Ingredients | Suprarenin® injection solution (Sanofi-Aventis Deutschland GmbH, Germany) 25 mL | Arterenol® injection solution (Sanofi-Aventis Deutschland GmbH, Germany) 25 mL | Ph.Eur. NE hydrogentartrate monohydrate powder (Sanofi-Aventis), 40.0 g Ph. Eur. sodium chloride (Fagron GmbH & Co. KG, Barsbüttel, Germany), 5.0 g Ph. Eur. sodium metabisulfite (Caesar & Loretz GmbH, Hilden, Germany) and 0.5 g sodium-EDTA (VWR International GmbH, Darmstadt, Germany) |
| 1 mL contains 1.2 mg E-HCl equal to 1 mg E as active substance and max. 0.5 mg sodium metabisulfite, NaCl, HCl, 4 mg chlorobutanol 0.5H2O, and water for injection as excipients [8, 9]. | 1 ml contains 1.22 mg NE-HCl equal to 1 mg NE as active substance and max. 0.5 mg sodium metabisulfite, NaCl, diluted HCl, 4 mg chlorobutanol 0.5H2O, and water for injection as excipients | ||
| G70 % (B.Braun Melsungen AG, Melsungen, Germany) | G70 % (B.Braun Melsungen AG, Melsungen, Germany) | HCl 10 % (Aug. Hedinger GmbH & Co. KG, Stuttgart, Germany | |
| Water for injection (Aqua ad Inject., B.Braun Melsungen, AG, Melsungen, Germany) | Water for injection (Aqua ad Inject., B.Braun Melsungen, AG, Melsungen, Germany) | Water for injection (AMPUWA, Fresenius SE & Co. KGaA, Bad Homburg, Germany) | |
| Primary container | Infusion bag (Neo Care GmbH, Lüdenscheid, Germany), 4000 mL | Infusion bag (Neo Care GmbH, Lüdenscheid, Germany) | n.a. |
| BD Perfusion 50 ml syringe, BD, Heidelberg, Germany, single-use plastic syringes with photo-resistant barrels for light sensitive drugs | 10 mL 3-piece transparent Baxa Rapid-Fill syringes | Type I amber glass vials (Zscheile & Klinger GmbH, Hamburg, Germany), Chlorobutyl flurotec stoppers and flip off caps (Zscheile & Klinger GmbH, Hamburg, Germany) | |
| Preparation process | 280 mL of G70 % + 3640 mL water for injection were pumped with the Baxa MicroMacro™ Compounder (Baxa Ltd, Aarhus C, Denmark) into an empty 4000 mL infusion bag and mixed. 80 mL of 1 mg/mL E injection concentrate were transferred to the glucose vehicle solution, thoroughly mixed and aseptically filled with the medoc 4xxVMC Compounder (ICU Medical Germany GmbH, Lüdenscheid, Germany) into 50 mL syringes. Two syringes each were packed into a transparent plastic bag and heat sealed. During storage light-tight plastic boxes were used as outer packaging material. | 286 mL of G70 % + 3674 mL water for injection were pumped with the Baxa MicroMacro™ Compounder (Baxa Ltd, Aarhus C, Denmark) into an empty 4000 mL infusion bag and mixed. 40 mL of NE injection concentrate were transferred to the glucose vehicle solution in the infusion bag and thoroughly mixed. The resulting bulk solution containing 10 µg/mL NE was automatically filled, stoppered and labeled with the Baxa Rapid-Fill (Baxa Ltd, Aarhus C, Denmark) into 10 mL syringes. Ten syringes were packed in an aluminium bag and sealed. | The appropriate amounts of Ph. Eur. NE hydrogentartrate monohydrate as active substance and the excipients were weighed. The ingredients were added to about 4800 mL of water for injection which was pre-purged with nitrogen for 30 min. During the dissolution process purging was continued. The pH was adjusted to 3.4 and 3.8 with HCl 10 %, and water added to achieve an exact overall volume of 5000.0 mL bulk solution. The bulk solution was filled in 50 mL Type I amber glass vials using the Plümatex pump (Plümat, Espelkamp, Germany) and the content of the vial purged again with nitrogen to displace the oxygen in the headspace of the vials. Vials were closed with stoppers and caps. Finished products were autoclaved for 15 min at 121 °C, 2 bar. The vials were labeled as test products (not for human use) and specified analytical tests performed. |
Manufacture of Norepinephrine injection solution 40 µg/mL, 100 µg/mL, 200 µg/mL, 400 µg/mL in 50 mL glass vials
Test batches of 100×50 mL NE injection solutions of the concentrations 100 µg/mL, 200 µg/mL, and 400 µg/mL in amber glass vials were manufactured in the sterile production facility of the Pharmacy Department of the University Medical Center Mainz according to the Good Preparation Guide PIC/S PE 010–4 Annex 1 (preparation of terminally sterilized products) and the German Pharmacy Ordinance [2, 3]; see Table 1.
Routine batches of the NE injections solutions 40 µg/mL and 400 µg/mL (60 L bulk solution) were manufactured as described in Table 1. After sterilization in the final container each vial was inspected for defects and presence of visible particles. The vials were labeled corresponding to the legal requirements and packed into cardboard packages of 20×50 mL (Iphas Pharma Verpackung GmbH, Würselen, Germany). End product control and release were performed according to the German Pharmacy Ordinance.
Storage of test solutions
Epinephrine 20 µg/mL injection solution in 50 mL syringes
Stability tests were performed with 30 syringes randomly picked from a routine batch. The syringes with photo resistant barrels were stored at 2–8 °C in the refrigerator or at RT (21 °C or 27 °C) on a shelf without additional light protection. In order to study the influence of daylight, 3 syringes were picked and 20 mL of the content were transferred to 20 mL disposable BD Discardit® syringes with transparent barrels and stored on a shelf without additional light protection.
Norepinephrine 10 µg/mL injection solution in 10 mL syringes
Stability tests were performed with 30 syringes randomly picked from a routine batch. The syringes with transparent barrels were either stored at 2–8 °C or at RT without additional light-protection.
Norepinephrine injection solution 100 µg/mL, 200 µg/mL, 400 µg/mL in 50 mL glass vials
All test batches were stored refrigerated at 2–8 °C. At the predefined intervals 3 vials were randomly picked for stability tests.
Norepinephrine injection solution 40 µg/mL, 400 µg/mL in 50 mL glass vials
From routine batches of each concentration 18 vials were randomly picked and used for stability testing. 15 vials were stored at RT with a light-tight secondary packaging. The content of 3 vials was withdrawn into three disposable 50 mL syringes with transparent barrels (Original-Perfusor®-Spritzen, B.Braun Melsungen AG, Melsungen, Germany) and stored on a shelf without additional light protection.
Temperature was monitored with temperature loggers throughout the storage periods.
Sample preparation
Samples were withdrawn from 3 vials or syringes at each predefined time point as seen in Table 2 and assayed without (E 20 µg/mL, NE 10 µg/mL, 40 µg/mL) or with further dilution (NE 100 µg/mL, 200 µg/mL, 400 µg/mL). Dilution was performed with water HPLC grade in order to achieve a concentration of 40 µg/mL NE.
Each sample was assayed in triplicate (n=9 concentrations, i. e. one sample taken from each of 3 test products per timepoint). Additional samples were withdrawn for testing the physicochemical stability. Osmolality and pH were determined once in one sample of 3 test products (n=3).
Determination of chemical stability
HPLC Assay
E and NE concentrations were determined by a stability-indicating reversed-phase high-performance liquid chromatography (RP-HPLC) assay with photodiode array-detection (PDA).
The HPLC system consisted of a Waters Alliance 2695 with a Waters 996 PDA. Data were acquired and integrated by using Waters Empower Pro, Empower Build 1154 Software, version 5.00.00.00 (Waters Eschborn, Germany).
For quantitave analysis of E in the injection solutions a specific HPLC-assay was developed. For quantitave analysis of NE in the injection solutions a known HPLC-assay was adapted [10, 11]. The characteristics are given in Table 3.
Storage conditions and timepoints of sampling of the E and NE injection solutions.
| Days | Months | Days | ||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Storage Temperature 2–8 °C | 0 | 7 | 14 | 28 | 2 | 3 | 6 | 7 | 9 | 12 | Storage Temperature>21 °C | 0 | 1 | 3 | 6 | 7 | 14 | 28 |
| E | x | x | x | x | x | x | x | x | – | – | E | x | x | x | x | x | x | – |
| NE | x | x | x | x | x | x | xb | x | xa | xb | NE | x | x | – | – | x | x | x |
NE 400 µg/mL was additionally determined at month 9,
NE 10 µg/mL was measured after 4 and 10 month instead of 6 and 12 months.
Characteristics of the RP-HPLC assays established for quantitative analysis of E and NE injections solutions.
| Parameter | E hydrochloride | NE hydrochloride/tartrate |
|---|---|---|
| Column (MZ-Analysentechnik, Mainz, Germany) | Nucleodur HILIC® 5 µm, 250×4.6 mm (stationay phase: silica gel type B with ammonium sulfonyl groups) | µBondapak C18, 300×3.9 mm |
| Flow rate | 1.5 mL/min | 1 mL/min |
| Injection Volume | 100 µl | 20 µl |
| Runtime | 10 min | 15 min |
| Detection Wavelength | 280 nm (adrenochrome 480 nm) | 230 nm (adrenochrome 480 nm) |
| Mobile phase | 25 % ammonium acetate buffer 0.96 mg/mL, pH 4.5 (PanReac AppliChem GmBH, Darmstadt, Germany), and 75 % acetonitrile HPLC grade | 70 % potassium dihydrogen phosphate (PanReac AppliChem GmBH, Darmstadt, Germany) buffer 3.4 mg/mL, pH 3, containing 0.06 mg/mL SDS (Sigma-Aldrich) and 30 % methanol (Fisher Scientific GmbH, Schwerte, Germany) |
Validation of the RP-HPLC assays
The assays were validated following the ICH Q2 (R1) guidelines for stability studies [12].
Suitability
Suitability of the HPLC method was evaluated by analyzing forced degraded solutions. Aliquots of the commercially available E injection solution were alkalized to pH 8 and 11 with 1 N NaOH and heated. Aliquots of the commercially available NE injection solution were diluted to 10 µg/mL and either alkalized to pH 14 with 1 N NaOH or acidified to pH 1 with 1 N HCl or purely heat degraded. Alkalized and acidified aliquots were analysed prior to and after heating. Additional experiments were performed with the commercially available medicinal products which were used as educts in order to detect possible interferences of the peaks of the active substances with the peaks of excipients.
Linearity
Linearity of the method was proven by analyzing seven different concentrations of E and NE. Calibration standards containing E hydrochloride (Suprarenin® 25 mg/25 mL, Sanofi-Aventis Deutschland GmbH, Germany, linearity range: 5 µg/mL-15 µg/mL), NE hydrochloride (Arterenol® 1 mg/mL, Sanofi-Aventis Deutschland GmbH, Germany, linearity range: 10 µg/mL-30 µg/mL), NE tartrate (Norepinephrine hydrogen tartrate powder (Sanofi-Aventis Deutschland GmbH, Germany) in Water HPLC grade (1 mg/mL norepinephrine), linearity range: 20 µg/mL-60 µg/mL) were prepared by diluting commercially available injection concentrates with HPLC water or dissolving in HPLC water. Each calibration standard was injected in triplicate.
Accuracy and precision
Intraday accuracy and precision were validated with 10 quality control standards of E 20 µg/mL, NE (hydrochloride) 10 µg/mL and NE (tartrate) 40 µg/mL with 28-fold-injection. Interday accuracy and precision were validated by analyzing the quality control standards on five or three different days for E hydrochloride and NE tartrate.
Robustness
Robustness of the assay was evaluated by using different batches of mobile phase and different temperatures during the validation assays.
Stability
Test and routine batches were released when the actual concentrations of E and NE were not less than 95.0 % and not more than 105.0 % of the nominal value. A product was declared as stable when the measured concentration was ≥90 % of the initial concentration designated as 100 %.
pH, osmolality
pH measurements were performed with a pH 210 Microprocessor pH-Meter (Hanna Instruments, Kehl am Rhein, Germany) equipped with a pH glass electrode (Mettler Toledo, Gießen, Germany). Calibration was performed with calibration standards (pH 4.01 and 10.01) from Hanna Instruments.
Osmolality measurements were performed with Osmometer M30 (Gonotec GmbH, Berlin, Germany). Calibration was performed with calibration standard 1 mL
300 mosmol/kg NaCl/H2O (Gonotec GmbH, Berlin, Germany) according to chapter 2.2.35 Ph.Eur.
Visual inspection, visible particles
Test solutions were visually inspected for particulate matter and changes in color whenever test solutions were picked and samples were withdrawn. Solutions without changes were defined as physically stable.
Results
Chemical stability
Suitability of the assays was shown by forced degradation tests. Alkalization of E and
NE solutions with NaOH resulted in reduced parent peaks, a peak corresponding to adrenochrome (480 nm) and additional peaks of not identified degradation products with rel. Rt<1 (s. Figure 1). None of the degradation peaks interfered with the parent peak of E and NE. Corresponding to the methyl group in the aminoalkyl sidechain E revealed to be less stable than NE.

HPLC-Chromatogram of alkalized epinephrine 20 µg/ml RTA 50 mL, detection wavelength 480 nm.
The HPLC methods developed for the E and NE containing injection solutions were robust and the validation parameters met the ICH Q2 (R1) criteria (compare Table 4 and Figure 2–3).

HPLC chromatogram of epinephrine 20 µg/ml RTA 50 mL syringe, PDA at 280 nm and after alkalization (3D Plot).
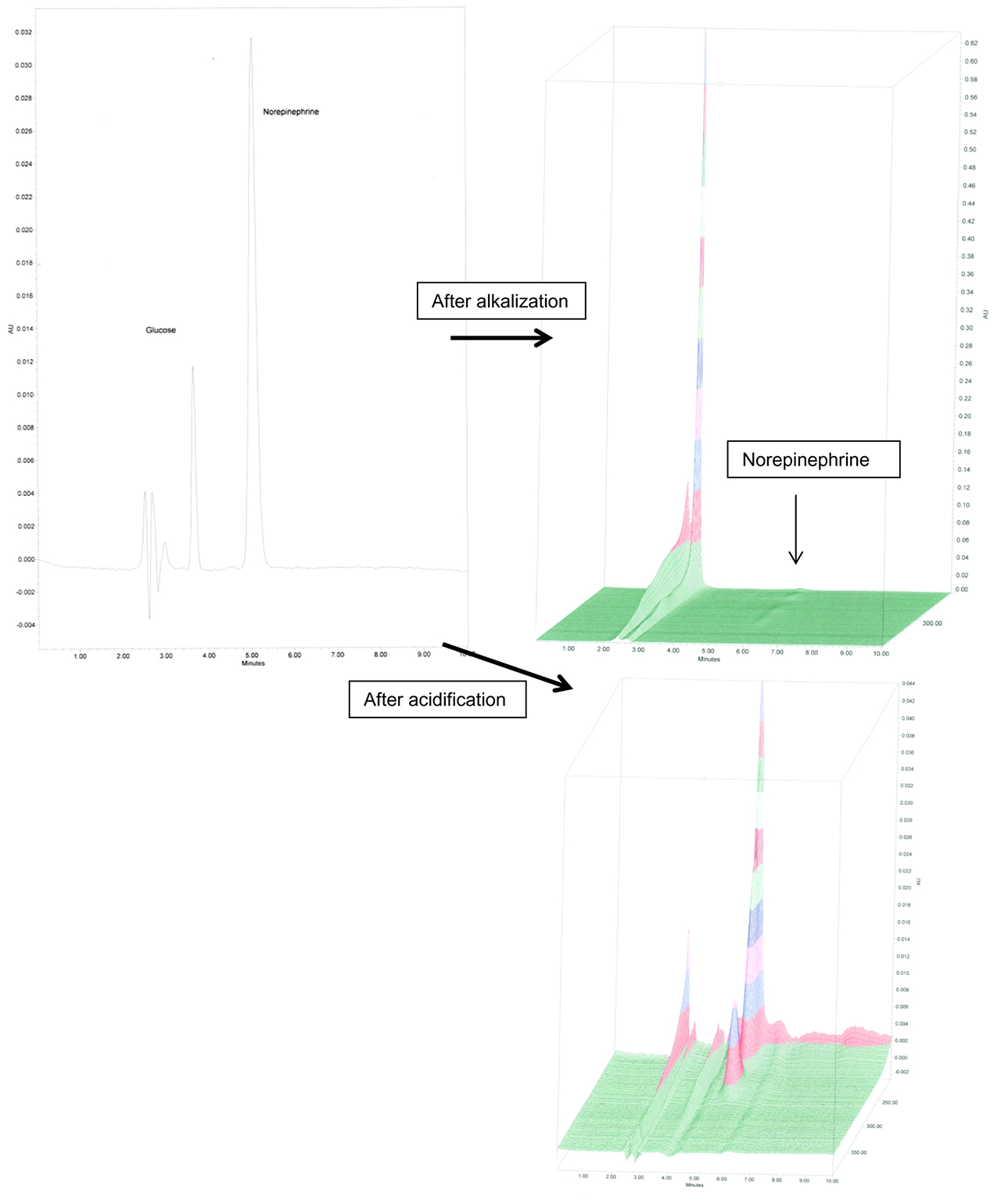
Exemplary HPLC chromatogram of norepinephrine 10 µg/ml RTA syringe, PDA at 230 nm, after alkalization (PDA PLOT on the top) and after acidification (PDA PLOT on the bottom).
Validation parameters of the RP-HPLC assays.
| Validation Parameter | E hydrochloride | NE hydrochloride | NE tartrate |
|---|---|---|---|
| Linearity | 0.9996 | 0.9997 | 0.9993 |
| Intraday RSDra [%] | 0.96 | 0.75 | 2.52 |
| Interday RSDta[%] | 2.46 | 1.53 | 2.92 |
RSDr: Intraday repeatability, RSDt: Interday repeatability.
Epinephrine 20 µg/mL injection solution in 50 mL syringes
The epinephrine concentration decreased in the E 20 µg/mL RTA injection solution to about 97 % of the initial concentration over a period of 6 months under refrigerated storage conditions (2–8 °C). Detailed results are given in Table 5. When stored at a temperature of 21 °C the injection solutions were stable for 14 days. When stored at 27 °C the injection solutions were only stable for 3 days irrespective of light exposure (compare Table 6).
Stability of E 20 µg/mL injection solution in 50 mL syringes stored at 2–8 °C. Concentration expressed as mean±realative standard deviation of triplicate assays of three test solutions (n=9). Drug concentrations in samples taken at time zero were designated as 100 %.
| E 20 µg/mL injection solution stored in plastic syringes, n=9 | ||
|---|---|---|
| Storage condition 2–8 °C | ||
| Storage period | Measured concentration | Initial concentration remaining±RSD |
| Day | [µg/ml] | [%] |
| 0 | 20.12 | 100.00±0.24 |
| 7 | 20.38 | 101.28±0.53 |
| 14 | 20.40 | 101.38±0.24 |
| 28 | 20.11 | 99.96±1.00 |
| Month | ||
| 2 | 20.22 | 100.49±1.37 |
| 3 | 20.13 | 100.08±0.92 |
| 6 | 19.64 | 97.60±1.39 |
| 7 | 18.56 | 92.23±1.67 |
| 12 | 18.59 | 91.25±3.27 |
Stability of E 20 µg/mL injection solution in 50 mL syringes stored at 21 °C and 27 °C with/without light-protection. Concentration expressed as mean±realative standard deviation of triplicate assays of three test solutions (n=9). Drug concentrations in samples taken at time zero were designated as 100 %.
| E 20 µg/mL injection solution stored in plastic syringes at T>21 °C, n=9 | ||||||
|---|---|---|---|---|---|---|
| Storage condition | Syringes with photoresistant barrel T=Ø21°C | Syringes with photoresistant barrel T=Ø26.6 °C | Syringes with transparent barrels T=Ø26.6 °C | |||
| Storage period | Measured concentration | Initial concentration remaining±RSD | Measured concentration | Initial concentration remaining±RSD | Measured concentration | Initial concentration remaining±RSD |
| Day | [µg/mL] | [%] | [µg/mL] | [%] | [µg/mL] | [%] |
| 0 | 20.25 | 100.00±0.75 | 19.76 | 100.00±1.84 | 19.86 | 100.00±0.61 |
| 1 | 19.97 | 98.89±0.90 | 18.93 | 96.19±1.89 | 18.85 | 94.25±0.82 |
| 3 | n.d. | n.d. | 19.81 | 100.61±1.37 | 19.54 | 97.88±1.93 |
| 6 | n.d. | n.d. | 17.46 | 88.38±3.26 | 17.38 | 86.80±0.71 |
| 7 | 19.64 | 96.97±1.43 | 17.50 | 88.55±3.05 | 17.80 | 89.02±1.18 |
| 14 | 18.48 | 91.24±3.27 | n.d. | n.d. | n.d. | n.d. |
Norepinephrine 10 µg/mL injection solution in 10 mL syringes
NE injection solutions 10 µg/mL in 10 mL syringes revealed to be stable over a period of 6 months when stored refrigerated and 28 days when stored at RT (compare Table 7).
Stability of NE 10 µg/mL injection solution in 10 mL syringes stored at 2–8 °C or RT without light-protection. Concentration expressed as mean±realative standard deviation of triplicate assays of three test solutions (n=9). Drug concentrations in samples taken at time zero were designated as 100 %.
| NE 10 µg/mL injection solution stored in plastic syringes at 2–8 °C and RT, n=9 | ||||
|---|---|---|---|---|
| Storage condition | 2–8 °C | Syringes with transparent barrels RT | ||
| Storage Period | Measured concentration | Initial Concentration remaining±RSD | Measured Concentration | Initial concentration remaining±RSD |
| Day | [µ/mL] | [%] | [µ/mL] | [%] |
| 0 | 9.23 | 100.00±0.50 | 10.38 | 100.00±1.60 |
| 1 | n.d. | n.d. | 9.88 | 95.15±1.08 |
| 7 | 9.18 | 99.52±0.59 | 9.80 | 94.40±1.50 |
| 14 | 9.18 | 99.54±0.66 | 9.72 | 93.60±1.19 |
| 21 | n.d. | n.d. | 9.67 | 93.17±0.57 |
| 28 | 9.17 | 99.33±0.48 | 9.49 | 91.44±0.96 |
| 35 | n.d. | n.d. | 9.27 | 89.31±1.24 |
| Month | ||||
| 3 | 9.17 | 99.35±0.47 | 9.25 | 89.16±1.23 |
| 4 | 8,89 | 96.38±1.11 | n.d. | n.d. |
| 10 | 8,92 | 96.67±0.98 | n.d. | n.d. |
Norepinephrine injection solution 40, 100, 200, 400 µg/mL in 50 mL vials
NE injections solutions 100, 200, 400 µg/mL in 50 ml vials remained stable over a period of 12 months when stored refrigerated (compare Table 8). NE injection solutions 40 µg/mL and 400 µg/mL were stable over a period of 28 days when stored at RT and light-protected. When NE 400 µg/mL injection solution was transferred to disposable syringes with transparent barrels NE concentration decreased to 94 % in a period of 14 days. For the NE 40 µg/mL injection solution the exposure to light was deleterious (Table 9).
Stability of NE injection solutions stored in 50 mL vials at 2–8 °C. Concentration expressed as mean±realative standard deviation of triplicate assays of three test solutions (n=9). Drug concentrations in samples taken at time zero were designated as 100 %.
| NE injection solution in 50 mL vials stored at 2–8 °C, n=9 | ||||||
|---|---|---|---|---|---|---|
| Storage condition | 100 µg/mL | 200 µg/mL | 400 µg/mL | |||
| 2–8 °C | 2–8 °C | 2–8 °C | ||||
| Storage period | Measured Concentration | Initial concentration remaining±RSD | Measured concentration | Initial concentration remaining±RSD | Measured Concentration | Initial concentration remaining±RSD |
| Day | [µg/mL] | [%] | [µg/mL] | [%] | [µg/mL] | [%] |
| 0 | 97.10 | 100.00±0.54 | 197.45 | 100.00±0.23 | 389.93 | 100.00±0.40 |
| 7 | 97.33 | 100.23±0.58 | 195.45 | 98.98±0.37 | 392.37 | 100.63±0.31 |
| 14 | 97.25 | 100.16±1.09 | 195.45 | 98.98±0.28 | 393.53 (day 19) | 100.92±0.47 |
| 28 | 97.00 | 99.90±0.34 | 196.75 | 99.64±0.31 | 396.07 | 101.57±0.39 |
| Month | ||||||
| 2 | 96.15 | 99.04±0.91 | 196.20 | 99.37±0.18 | n.d. | n.d. |
| 3 | 95.35 | 97.97±0.95 | 194.00 | 98.25±1.01 | 389.47 | 99.88±0.31 |
| 6 | 97.60 | 100.52±0.48 | 197.65 | 100.08±0.64 | 387.98 | 99.50±0.40 |
| 7 | 95.03 (8 months) | 97.88±0.32 | n.d. | n.d. | 408.11 | 104.66±1.22 |
| 12 | 94.43 | 97.25±0.53 | 186.85 | 94.63±0.96 | 391.53 | 100.41±0.77 |
Stability of NE injection solutions stored in 50 mL at RT with or without light-protection. Concentration expressed as mean±realative standard deviation of triplicate assays of three test solutions (n=9). Drug concentrations in samples taken at time zero were designated as 100 %.
| NE injection solution in 50 mL vials stored light-protected or in transparent plastic syringes at RT, n=9 | ||||||||
|---|---|---|---|---|---|---|---|---|
| Storage condition | 40 µg/mL | 400 µg/mL | 40 µg/mL | 400 µg/mL | ||||
| Vials with photoresistant barrel RT | Vials with photoresistant barrel RT | Syringes with transparent barrels RT | Syringes with transparent barrels RT | |||||
| Storage period | Measured concentration | Initial concentration remaining±RSD | Measured concentration | Initial concentration remaining±RSD | Measured Concentration | Initial concentration remaining±RSD | Measured concentration | Initial concentration remaining±RSD |
| Day | [µg/mL] | [%] | [µg/mL] | [%] | [µg/mL] | [%] | [µg/mL] | [%] |
| 0 | 40.40 | 100.00±0.88 | 407.67 | 100.00±0.81 | 39.89 | 100.00±0.94 | 411.56 | 100.00±0.88 |
| 1 | n.d. | n.d. | 408.29 | 100.15±0.47 | n.d. | n.d. | n.d. | n.d. |
| 7 | 39.08 | 96.74±0.91 | 407.68 | 100.00±0.94 | 30.63 | 76.78±9.85 | 396.06 | 96.23±0.75 |
| 14 | 39.30 | 97.30±0.86 | 407.30 | 99.91±2.65 | 25.06 | 62.83±14.92 | 385.72 | 93.72±0.78 |
| 21 | n.d. | n.d. | n.d. | n.d. | 20.29 | 50.86±22.73 | 359.87 | 87.44±1.09 |
| 28 | 39.23 | 97.11±0.64 | 409.19 | 100.37±0.54 | 18.66 | 46.77±27.37 | 353.29 | 85.84±0.79 |
| Month | ||||||||
| 6 | 35.55 | 88.01±1.35 | 372.44 | 91.36±0.82 | n.d. | n.d. | n.d. | n.d. |
pH measurement, osmolality
Only slight changes of pH and osmolality became obvious when the test products were stored refrigerated up to 12 months (data not shown in a table). pH values decreased in test solutions stored at RT over time as shown in Table 10. In test solutions stored at RT with light protection the pH values also varied only slightly over a storage period of 28 days. However, when the test solutions were exposed to light the pH values decreased significantly over time. In parallel, osmolality increased over time, especially when the test solutions were exposed to mixed daylight.
pH values and osmolality of E and NE injection solutions stored at RT with or without light-protection.
| pH+/–RSD [%], n=3 | ||||||||
|---|---|---|---|---|---|---|---|---|
| Storage period | E | NE | NE | |||||
| 20 µg/mL | 20 µg/mL | 10 µg/mL | 40 µg/mL | 400 µg/mL | ||||
| Day | light-protected 21°C | light-protected 27 °C | without light-protecting 27 °C | without light-protecting RT | light-protected RT | without light-protecting RT | light-protected RT | without light-protected RTg |
| 0 | n.d. | 5.2±0.02 | 5.2±0.02 | 5.3±5.17 | 4.4±2.37 | 4.5±3.29 | 3.8±0.94 | 3.9±3.84 |
| 1 | 5.4±3.22 | 5.4±0.02 | 5.3±0.03 | 5.3±1.70 | 4.2±7.32 | 4.3±2.15 | 3.6±2.06 | 3.8±0.66 |
| 3 | n.d. | 5.6±0.03 | 5.0±0.01 | n.d. | n.d. | n.d. | n.d. | n.d. |
| 6 | n.d. | 5.1±0.01 | 4.5±0.07 | n.d. | n.d. | n.d. | n.d. | n.d. |
| 7 | 5.8±1.74 | 5.3±0.03 | 4.7±0.04 | 4.9±3.43 | 4.4±1.13 | 4.6±1.41 | 3.9±1.90 | 4.0±0.99 |
| 14 | 5.4±3.43 | n.d. | n.d. | 5.5±7.56 | 3.7±4.89 | 3.1±8.25 | 3.5±1.35 | 3.5±1.61 |
| 21 | n.d. | n.d. | n.d. | 6.1±9.10 | n.d. | 2.9±14.58 | n.d. | 3.0±0.19 |
| 28 | n.d. | n.d. | n.d. | 5.3±3.95 | 4.2±4.79 | 2.9±15.94 | 3.8±2.51 | 2.8±4.09 |
| Osmolality [mosmol/kg]+/–RSD [%], n=3 | ||||||||
| Day | ||||||||
| 0 | n.d. | 258±0.00 | 258±0.00 | 296±0.00 | 260±0.00 | 260±0.00 | 263±0.00 | 263±0.00 |
| 1 | 293±1.48 | 288±0.01 | 290±0.00 | 295±0.00 | 254±0.00 | 254±0.00 | 257±0.00 | 261±0.00 |
| 3 | n.d. | 307±0.01 | 305±0.01 | n.d. | n.d. | n.d. | n.d. | n.d. |
| 6 | n.d. | 288±0.03 | 282±0.01 | n.d. | n.d. | n.d. | n.d. | n.d. |
| 7 | 292±4.94 | 283±0.01 | 284±0.00 | 305±0.00 | 265±0.00 | 266±0.00 | 268±0.00 | 269±0.00 |
| 14 | 291±5.25 | n.d. | n.d. | 298±0.00 | 266±0.00 | 265±0.00 | 271±0.00 | 274±0.00 |
| 21 | n.d. | n.d. | n.d. | 306±0.00 | n.d. | 274±0.00 | n.d. | 276±0.00 |
| 28 | n.d. | n.d. | n.d. | 309±0.00 | 276±0.00 | 284±0.00 | 288±0.00 | 289±0.00 |
Discussion
As epinephrine and norepinephrine are categorized as high alert medication, RTA injection solutions in syringes and RTU injection solutions in glass vials should be prepared in standardized concentrations in the pharmacy departments of hospitals. The batch wise processed products are subject to analytical tests, e. g. determination of the active substance content prior to release of the batch. Stability testing is essential for assigning shelf lives and in-use storage periods. The concentrations of E and NE are in general determined by RP-HPLC assays according to the Pharmacopoeia [Ph. Eur].
HPLC assay and physicochemical stability
Variations of the HPLC assays are used for stability testing of diluted E and NE injection solutions [5, 13, 14]. Based on the known methods [10, 11] we established an HPLC assay for quantitative analysis of NE using the µBondapak C18 column and SDS containing mobile phase. The assay revealed to be robust and met the validation criteria of the relevant ICH Guideline. However in daily practice we observed that the retention time of the NE peak increased over time. To avoid this phenomenon after 12 injections the column is to be flushed by an admixture of 95 % water HPLC grade and 5 % acetonitrile for a period of 20 min. Because of this additional effort we decided to develop an alternative assay for the quantification of E based on the cation exchange principle and installed the Nucleodur HILIC column. The mobile phase consists of ammonium acetate buffer and acetonitrile. The column and the mobile phase revealed to be fragile. However the assay met the validation criteria of the relevant ICH Guideline and was used for stability testing. Suitability of the assay was shown by forced degradation under acidic and alkalized conditions with and without heat. Most degradation peaks were registered after alkalization, since higher pH values enforce the degradation process and the formation of red colored adrenochromes. Hence, the suitability of the HPLC assay for E was solely tested by alkaline induced degradation and pure heat. Peaks of the resulting adrenochrome did not interfere with the parent peak. For the calibration of the HPLC assay, in general standard solutions prepared from reference substance of the active ingredients are used. In this case, dilutions of the commercially available injection concentrates were used, because these are applied as source solutions in aseptic preparation. No matrix effects and interference between active ingredients and excipients were found during HPLC analysis.
Another limitation of our study is the lacking determination of subvisible particles. These tests are only run for batch release of the RTU products and were never out of specification.
RTA preparations
When the decision was made to use standardized concentrations of E (20 µg/mL) and NE (10, 40, 100, 200, 400 µg/mL) in emergency cases and intensive care units in our hospital, the pharmacy department developed formulations and aseptic preparation processes. The most convenient way to prepare RTA injection solutions in syringes is to dilute commercially available injection concentrate with vehicle solution and to fill the required volume in suitable primary containers. Because of the pH-dependent stability of E and NE, weakly acidic 5 % glucose solution was used as vehicle for RTA preparations resulting in pH values of about 5. However sterility is to be ensured by aseptic preparation and terminal sterilization processes are not applicable. Shelf life of these preparations is limited by the microbiological stability. RTA preparations containing 20 µg/mL E or 10 µg/mL NE in disposable syringes revealed to be physicochemically stable at refrigerated temperatures for more than 6 months, which is longer than the designated shelf life based on microbiological stability. According to our quality controls and environmental monitoring program we limit the shelf-life for RTA preparations in disposable syringes to a maximum of 3 months. Long-term stability of similar preparations regarding the concentrations of E and NE and syringes as primary containers are not yet published. The decreased stability of these preparations at elevated temperatures (21 °C, 26 °C) and light exposure corresponds to the known stability determining factors. Adams et al. reported that concentrations of E 50 µg/mL RTA preparations (vehicle solution G5 %) stored at 20–25 °C remained unchanged for 4 days (max. test period) [15]. Commercially available E 1 mg/mL injection solution filled into 1 mL syringes with a pH range of 3.17–3.23 remained stable when stored at RT for 3 months (after 1 month: E=101.4 %, after 3 months: E=101.2 % of the nominal concentration) [16]. To our best knowledge no further studies of similar RTA preparations are available. Administration of the RTA preparations over a period of 24 hours does not affect stability.
RTU preparations
Extended shelf lives are applicable when terminally sterilized RTU preparations are produced in glass vials. Moreover, the preparation is more efficient, less time consuming and larger batch sizes are feasible.
For NE RTU preparations we designed a formulation based on the formulation of the licensed medicinal product. We omitted the preservative because of single use and increased the sulfite concentration to reduce oxidation. Degradation of NE was further decelerated by adjusting the pH to 3.4–3.8, addition of EDTA as excipient, purging the bulk solution with nitrogen, using amber Type I glass vials and flurotec stoppers as primary packaging material. The formulation revealed to be sterilizable by moist heat without loss of content. RTU preparations containing NE in the concentration range of 40 to 400 µg/mL remained stable for more than 12 months. At RT the shelf-life decreased to about 6 months and the exposure to mixed daylight at RT caused loss of stability in only a few days.
The results regarding mixed daylight exposure are not reliable because of lack of standardization of the stability influencing factors. The content of the 10 µg/mL NE syringes was protected from light by the labels while the content of 400 µg/ml NE syringes was not protected. The influence of the NE concentration and the type of preparation (RTA in syringes, RTU in glass vials) did not become evident by our study design.
Peaks corresponding to adrenochromes were not detected in any of the HPLC-PDA chromatograms at the detection wavelength of 480 nm. During visual inspection of the test solutions color changes were not obvious.
Conclusion
Batch wise preparation of RTA preparations containing 20 µg/mL E or 10 µg/mL NE in disposable syringes as well as RTU preparations containing 40, 100, 200 and 400 µg/mL NE was successfully implemented in a pharmacy department. Storage of the preparations at refrigerated temperatures is required to obtain acceptable shelf-lives of 6–12 months. Elevated temperatures and especially exposure to mixed daylight significantly decreased the shelf life.
About the authors

Rita Marina Heeb studied pharmacy at Johann Wolfgang Goethe University in Frankfurt, Germany. Since 2012 she is Head of Quality Control at the Department of Pharmacy of Johannes Gutenberg-University Medical Center Mainz, Germany. She has completed her doctoral thesis in Clinical Pharmacy entitled: “Compliance – and Quality of life measurements at dialysis and liver cirrhosis patients before transplantation” at Johannes-Gutenberg-University Mainz. Her research interests include monitoring of medication adherence and physicochemical stability of pharmaceuticals.

Bettina Stollhof studied pharmacy at Johannes Gutenberg-University in Mainz, Germany. She is working at the Pharmacy Department of the Medical Center of Johannes Gutenberg-University Hospital since 2006. She has completed her doctoral thesis in Clinical Pharmacy entitled: “Optimization of Phenprocoumon-dosis by intensive medical-pharmaceutical care” at Johannes-Gutenberg-University Mainz. Her research interests include aseptic drug preparation, infusion management: incompatibilities-reducing infusion schemes and ready-to-use parenteral solutions.

Julia Reichhold is working at the Pharmacy Department of the University Medical Center of Johannes Gutenberg-University Hospital in Mainz since 2010. In 2013 she completed her doctoral thesis entitled: Influence of single units of solid oral medication on drug therapy safety, information and satisfaction of inhouse patients in an open, controlled, prospective, multicenter patient study. The medication of choice in single units was Diovan®, CoDiovan® and Amlodipin. Her special interests and research projects include aseptic drug preparation and drug therapy safety.

Judith Thiesen is working at the Pharmacy Department of the University Medical Center of Johannes Gutenberg-University Hospital in Mainz since 1997. In 2001 she completed her doctoral thesis entitled: Evidence-based optimization of parenteral drug application for oncological patients: incompatibilities-reducing infusion schemes, stability of ready-to-use parenteral solutions of camptothecin-derivatives and taxanes. Her special interests and research projects include aseptic drug preparation, quality control, total quality management as well as physicochemical and microbiological stability of parenteral drug solutions.

Irene Krämer is currently Director of the Pharmacy Department, University Medical Center, Johannes Gutenberg-University Hospital, Mainz and is also a Professor for clinical pharmacy at the Pharmacy School of Johannes Gutenberg-University. She completed her postdoctoral thesis in Pharmaceutical Technology entitled: Development, quality assurance, and optimization of ready-to-use parenteral solutions in the integrated cancer care concept. Her special interests include oncology pharmacy, infectious diseases and aseptic drug preparation. She is doing research projects in the field of physicochemical and microbiological stability of cytotoxic drugs, compatibility of admixtures of nebulizer solutions and monitoring of medication compliance.
Acknowledgement
We would like to thank A. Klein, C. John, A. Orth, A. Semar, J. Gehring for performing the analytical tests.
Conflict of interest statement: Authors state no conflict of interest. All authors have read the journal’s Publication ethics and publication malpractice statement available at the journal’s website and hereby confirm that they comply with all its parts applicable to the present scientific work.
References
1. Institute for Safe Medication Practices. ISMP list of high alert medications in communty/ambulatory healthcare [Internet] 2011 [cited 2017 Jul 20]. Available at: https://www.ismp org/communityRx/tools/ambulatoryhighalert asp. Accessed 30 January 2011Search in Google Scholar
2. PIC/S Guide to good practices for the preparation of medicinal products in healthcare establishments PE 010-4, 1 March 2014Search in Google Scholar
3. Ordinance on the Operation of Pharmacies https://www.abda.de/fileadmin/assets/Gesetze/ApBetrO_engl_Stand-2016-12.pdf. Accessed July 2017Search in Google Scholar
4. Grunert R, Wollmann H. Effect of ultraviolet and visible light on drugs of the phenylalkylamine series with a view toward their stability in plastic containers. 17. Stability of drugs and preparations. 83. Problems of the use of plastic containers for liquid pharmaceuticals. Pharmazie 1982;37:798–99.Search in Google Scholar
5. Hoellein L, Holzgrabe U. Ficts and facts of epinephrine and norepinephrine stability in injectable solutions. Int J Pharm 2012;434:468–80.10.1016/j.ijpharm.2012.05.017Search in Google Scholar PubMed
6. Council of Europe. European pharmacopoeia. 9th ed. Strasbourg: Council of Europe; 2016.Search in Google Scholar
7. Council of Experts and its Expert Committees. U.S. Pharmacopoeia-National Formulary [USP 40 NF 35]. Volume 2. Rockville, Md: United States Pharmacopeial Convention, Inc; 2017.Search in Google Scholar
8. SmPC. Suprarenin®. 2015. Available at: https://mein.sanofi.de/produkte/Suprarenin/Downloads?id=77f451d1-172d-4ea0-9f6a-16e8488292bf. Accessed 20 Jul 2017.Search in Google Scholar
9. SmPC. Arterenol®. Available at: https://mein.sanofi.de/produkte/Arterenol/Downloads?id=fb251295-cc9b-4f0a-92db-1e697943ffe6. Accessed 20 Jul 2017.Search in Google Scholar
10. Höllein L, Bennack E, Holzgrabe U. Individual dilutions from commercial norepinephrine injectables (Arterenol®)- stability, quality and analytic. Krankenhauspharmazie 2012;33:427–31.Search in Google Scholar
11. Ghanayem NS, Yee L, Nelson T, Wong S, Gordon SJB, Marcdante K, et al. Stability of dopamine and epinephrine solutions up to 84 hours. Pediatr Crit Care Med 2001;2:315–17.10.1097/00130478-200110000-00005Search in Google Scholar PubMed
12. ICH Q2 (R1) Guideline. 2005. Available at: http://www.ich.org/fileadmin/Public_Web_Site/ICH_Products/Guidelines/Quality/Q2_R1/Step4/Q2_R1__Guideline.pdf. Accessed Apr 2012.Search in Google Scholar
13. Walker SE, Law S, Garland J, Fung E, Iazzetta J. Stability of Norepinephrine solutions in normal saline and 5 % dextrose in water. Can J Hosp Pharm 2010;63:113–18.10.4212/cjhp.v63i2.896Search in Google Scholar PubMed
14. Bonhomme L, Benhamou D, Comoy E, Preaux N. Stability of adrenaline pH-adjusted solutions of local anaesthetics. Prog Ph Bio Anal 1991;6:497–99.10.1016/0731-7085(91)80252-5Search in Google Scholar
15. Adams HA, Borner U, Hempelmann G. Untersuchungen zur Stabilität klinisch gebräuchlicher Katecholaminlösungen. Wehrmed Mschr 1985;12:547–49.Search in Google Scholar
16. Kerddonfak S, Manuyakorn W, Kamchaisatian W, Sasisakulporn C, Teawsomboonkit W, Benjaponpitak S. The stability and sterility of epinephrine prefilled syringe. Asian Pac J Allergy Immunol 2010;28:53–57.Search in Google Scholar PubMed
© 2017 Walter de Gruyter GmbH, Berlin/Boston
Articles in the same Issue
- graphical-abstract
- Frontmatter
- Guest Editorial
- Stability Studies: A Scientific Mission of the Hospital Pharmacist
- Research Articles
- Physicochemical Stability of Reconstituted Decitabine (Dacogen®) Solutions and Ready-to-Administer Infusion Bags when Stored Refrigerated or Frozen
- Stability of Ready-to-Administer and Ready-to-Use Epinephrine and Norepinephrine Injection Solutions
- Stability Study of Morphine and Baclofen Solution in Polypropylene Syringes
- A Sorption Study between Ophthalmic Drugs and Multi Dose Eyedroppers in Simulated Use Conditions
- Preparation and Physico-Chemical Stability of Dexamethasone Oral Suspension
Articles in the same Issue
- graphical-abstract
- Frontmatter
- Guest Editorial
- Stability Studies: A Scientific Mission of the Hospital Pharmacist
- Research Articles
- Physicochemical Stability of Reconstituted Decitabine (Dacogen®) Solutions and Ready-to-Administer Infusion Bags when Stored Refrigerated or Frozen
- Stability of Ready-to-Administer and Ready-to-Use Epinephrine and Norepinephrine Injection Solutions
- Stability Study of Morphine and Baclofen Solution in Polypropylene Syringes
- A Sorption Study between Ophthalmic Drugs and Multi Dose Eyedroppers in Simulated Use Conditions
- Preparation and Physico-Chemical Stability of Dexamethasone Oral Suspension