Toward a New Science of the Clinical Uses of the Arts
-
Steven Brown
 and
Jacob Cameirao
and
Jacob Cameirao

Abstract
The arts are used clinically in a wide variety of applications, spanning from physical therapy to psychotherapy. We present a theoretical analysis of these clinical applications that is grounded in a unified model of the arts. Such an approach is based on an understanding of the relationships among the various art forms and how the arts are able to impact non-art functions via transfer effects. A unified model helps to clarify the distinction between near and far transfer in the clinical uses of the arts. The empirical evidence suggests that art applications for physical therapy tend to be based on near-transfer effects and show high specificity for the employed art forms. By contrast, art applications for psychotherapy tend to be based on far transfer and show less specificity for the employed art forms. We argue that a theory of the clinical uses of the arts has to be predicated on a unified model of the arts themselves. Such a model provides a rational basis for understanding how art forms are able to bring about their clinical effects.
1 Toward a Unified Model of the Clinical Uses of the Arts
Historical analyses indicate that the clinical uses of the arts for healing purposes constitute an ancient feature of human cultural practices, dating back at least to the ancient Greeks in Western culture (Perrot, 2016; Wile, 1926), if not much earlier in indigenous traditions (Winkleman, 2010). In the twentieth century, the clinical uses of the arts became established as professional specializations in the form of various art therapies, including well-known disciplines such as music therapy, dance therapy, drama therapy, and (visual) art therapy (reviewed by Gladding, 2011; Jones, 2021). Such specializations have been propelled by academic training programs and professional accreditation protocols, as well as by professional organizations, journals, and conferences. Our principal claim in the current article is that, while each individual art therapy has matured on its own to become a successful professional discipline, there has been virtually no bridging work attempting to integrate these various disciplines into a unifying framework for the clinical uses of the arts. There are many reasons for this, including a) that the individual art therapies lack unified frameworks for understanding the clinical operations of the arts within their own domains (Robbins, 1997); b) that many training programs for art therapists do not include a research component, thereby creating a divide between research and clinical practice; and c) that there are difficulties in operationalizing the core processes of the art therapies so as to enable their empirical scrutiny (van Westrhenen & Fritz, 2014).
It is important to note that holistic classifications of the branches of the arts hail back more than 2,500 years to the time of Plato and Aristotle and through to the Enlightenment (Aristotle, 335BC/1996; Batteux, 1746/2015; Kristeller, 1952; Malek, 1974; Porter, 2009; Shiner, 2001, 2009; Young, 2015), and yet such thinking has not impacted the collection of disciplines that make up the art therapies. It is critical to bring such unificationist thinking to the realm of the clinical arts in order to understand how art therapies are related to one another.
A central issue that will be addressed in this article is the extent to which the various art therapies are either condition-specific or instead interchangeable. To what extent does a given art therapy show specificity for treating a particular condition? Are certain art therapies more efficacious in treating certain conditions, or do the various therapies simply provide alternative routes for achieving the same clinical outcomes? In order to address such issues, we need a model of the applied arts that not only describes the mechanisms of action of each individual art therapy, but that relates these mechanisms to one another.
Much of the professional practice of the art therapies is characterized by canalization. For example, a dance therapist is not considered to be qualified to do musical interventions, and vice versa for a music therapist. There is a small number of integrative movements that incorporate rich repertoires of art therapies, most notably expressive art therapy (EXAT) (Knill et al., 2004). Such movements succeed at reducing the canalization of individual art therapies by allowing for a more pluralistic application of art forms in a given treatment regimen. However, we believe that even EXAT is plagued by the same absence of an integrative framework of the arts as that which was described above for the individual art therapies. Its approach has been described using the metaphor of a “restaurant menu” (Utigaard, 2022) in which the protocol for selecting among the arts is based on the client’s choice from a range of available options. We contend that, unless one is employing a unified model of the arts as the guiding framework, then even multi-art applications like EXAT become relegated to “restaurant menu” thinking in which the various art forms comprise a toolkit that can be sampled as needed to achieve the same ultimate treatment outcome.
The principal objective of the current article is to apply a unified model of the arts to the therapeutic uses of the arts in order to identify mechanisms of action by which the arts produce their clinical effects. We will apply these ideas to both physical therapy and psychotherapy in order to reveal how contrastive these applications tend to be in practice. Our general approach in evaluating the clinical efficacy of the art therapies will occur along two dimensions, as shown in Figure 1. (1) We will consider the efficacy of the art therapies in comparison to that of non-art therapies. In doing so, we will only consider evidence-based non-art therapies that are standards for treatment. (2) Instead of examining the therapeutic value of each art form singularly, we will take a highly comparative approach that considers the treatment efficacy of the various art forms relative to one another, including as a function of which disorders or symptoms they are used to treat. Intuition tells us that we would not send a patient with a gait disturbance to a voice therapist, and yet when it comes to the treatment of depression, it may be the case that movement- and singing-based psychotherapies produce very similar outcomes. We will thus use a comparative approach in order to examine the condition-specificity vs. interchangeability of the various art therapies as a function of the conditions that they may treat, with a principal focus on the contrast between physical therapy and psychotherapy. Ultimately, we believe that a unified model of the arts can inform a new science of the applied arts, one that provides a rational basis for understanding how art forms are able to bring about their clinical effects.
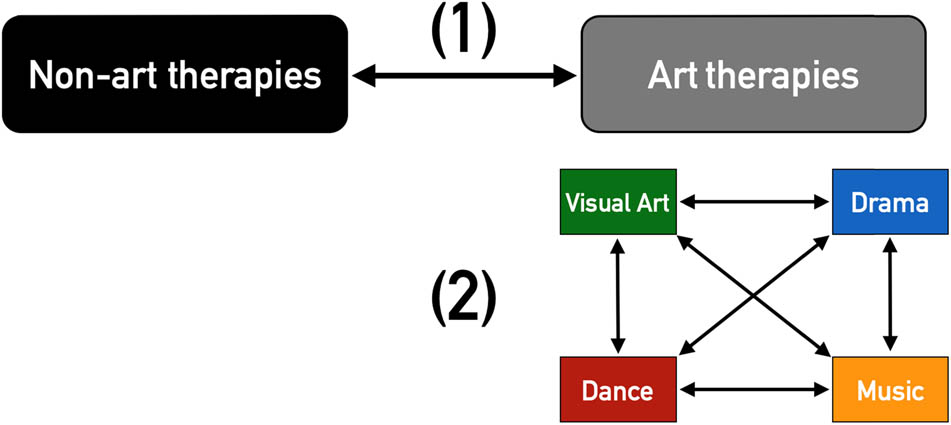
Two levels of analysis of the efficacy of the art therapies, whether for physical therapy or psychotherapy: (1) comparison of the art therapies with conventional non-art therapies, and (2) comparison of the art therapies among themselves. Note that the color-coding of the art forms in this figure is maintained throughout all of the figures.
It is important to note that the majority of the empirical clinical studies about the art therapies that are examined in this article are found in Tables S1–S4, not in the References section. A compilation of 45 meta-analyses is described there, as discussed in Section 6. The current article takes the form of a narrative review – rather than a quantitative analysis – of the published literature on art therapies. Our principal aim is to provide a theoretical framework for unifying the clinical applications of the arts where no such framework exists. The objective is to present a cross-arts model that can serve as a null hypothesis against which future work can be tested.
2 A classification of the Arts and, by Extension, of the Applied Arts
Space limitations prevent us from presenting a detailed functional and evolutionary account of the arts, which is described by the first author in Brown (2022). What is clear is that the arts did not evolve primarily to function as therapeutic aides. The clinical uses of the arts, despite their importance in human life and their antiquity in human cultures, are unquestionably ancillary functions for all of the branches of the arts. Given this, what are the primary functions of the arts? The arts are principally about the social communication of ideas, including the group-wide expression of emotions through collective rituals. Brown (2018, 2019, 2022) has argued that the two fundamental functions of the arts are narrative re-creation and interpersonal coordination. These functions will serve as the basis for the classification scheme of the art therapies shown in Figure 2.

A classification of the arts into narrative and coordinative categories, as based on Brown (2022). The figure presents a listing of the principal art therapies associated with each category in the classification scheme.
The narrative arts (visual art, oral storytelling, literature, poetry, theatre, and film) function to tell stories about people, objects, and events, often to promote social learning through the modeling of prosocial behaviors. The coordinative arts (dance and music) function to stimulate group participation through collective and synchronized actions, thereby serving as a reinforcer of group affiliation and a promoter of social cooperation. The narrative arts and coordinative arts are in no way mutually exclusive. Art forms that straddle these two categories are seen especially in the performing arts, including narrative forms of dance (such as ballet) and processes of “musical narration” (Brown, 2018) in which music is strategically used to accentuate the emotional meaning of narratives, such as in film (Cohen, 2013; Gorbman, 1987; Tan et al., 2017) and songs with words.
Figure 2 shows that the narrative arts are made up of both static forms – like literature[1] and the visual arts (the latter including both two-dimensional and three-dimensional forms, like painting and sculpture, respectively) – and performance forms like oral storytelling, theatre, and film. The performance forms are themselves divided into narrated forms (like oral storytelling) and acted-out forms in which performers embody characters via portrayal, as seen in theatre, film, opera, and narrative forms of dance. (The static arts are all narrated forms.) This division essentially maps onto that between literature and theatre in the humanities. It follows from Plato’s distinction in The Republic (Plato, 380BC/1968) between diegesis and mimesis, where diegetic forms of narrative are those that are produced from the perspective of the storyteller, and mimetic forms are those that involve the impersonation of the characters of a story by actors, as seen in theatre (Halliwell, 2014). The second general category of the arts, namely the coordinative arts, is made up of the performing arts of dance and music.
Figure 2 lists the principal art therapies associated with each category in the classification scheme. The listing is not meant to be exhaustive, but simply aims to present the major art therapies discussed in comparative texts, such as those of Gladding (2011) and Jones (2021). Briefly, art therapy and expressive writing therapy involve conveying narratives through the generation of static products, such as paintings and written texts, respectively. Drama therapy and certain forms of play therapy employ character portrayal to convey narratives. Dance therapy and music therapy are modalities that take advantage of interpersonal coordination in group formats or that simply employ rhythmic forms of movement or vocalization in individualized formats. While there has been a surge of interest in art applications for educational enhancement (reviewed by Winner et al., 2013), we will restrict our attention to the clinical applications of the arts. Among the latter, our emphasis will be on the treatment of clinical conditions, rather than on the prevention of disease (Fancourt & Finn, 2019; McCrary et al., 2021).
3 Unification Theory: How Art Therapies Work
Having provided a means of classifying the art therapies and relating them to one another, the remainder of this article will focus on how the art therapies work and how their mechanisms of action might be either distinct from one another or shared across the various therapies. The approach that we will take is based on the “unification of the arts” (UA) model developed by the first author (Brown, 2018, 2019, 2022). The principal tenet of this approach is that “a comparative analysis of the arts provides greater insight into each art form than is possible by looking at art forms in isolation” (Brown, 2022, p. 23). Hence, we are able to understand each type of art therapy better if we subject it to a comparative analysis than if we examine it exclusively on its own terms.
3.1 SPI Thinking
The UA approach is predicated on examining the relationships among the arts. It provides a number of conceptual tools for doing so, the first of which – namely classification of the arts – was discussed in the previous section. However, the most central concept is a characterization of three types of relationships among the arts with regard to neurocognitive similarity: sharings, parallels, and interactions (SPI). 1) Sharings. The notion of a sharing implies that the existence of similar features in two art forms is underlain by their use of a common physiological and/or neurocognitive system. For example, phonetic mechanisms for the production of vowels and consonants are shared between speech and song, since the same categories of phonemes are used in both spoken and sung production. 2) Parallels. The notion of a parallel implies that the existence of similar features in two art forms is underlain by analogous but distinct systems between the two art forms. An example of this is the notion of “syntax” as a parallel between music and language (Lerdahl, 2013; Patel, 2008), where such syntactic mechanisms operate on very different types of raw materials, namely words for language and pitches for music. 3) Interactions. Art forms can interact by combining their domain-specific elements in time and/or space to create composite forms. Two examples that will be mentioned in the article are the interaction between music and language to create songs with words, and the interaction between dance and music when dance is choreographed to music.
In developing our theory, we will furnish examples of art applications as they pertain to the clinical uses of the arts in the published literature. These examples will in no way be exhaustive of the ways in which SPI thinking applies to the clinical uses of the arts. More specifically, our discussion of sharings will focus primarily on applications related to dance and music, while our discussion of parallels will cover all of the arts. This is because sharings appear to be most relevant to an understanding of the physical-therapy applications of the arts, and the literature in this area has mainly examined dance and music, rather than the literary and visual arts. By contrast, parallels are more relevant to the psychotherapeutic applications of the arts, and the literature in this area has spanned all of the arts.
3.2 Art Modules
The application of SPI thinking to the art therapies will occupy much of the remainder of the article. However, we will introduce an additional concept from UA theory before doing so. This is the notion of an art module. Art modules refer to newly evolved functions of human cognition and behavior that are specific to, that enable the production of, the arts, and that are not offshoots of other, more-basic cognitive or behavioral functions that evolved for non-art purposes, such as language, memory, or attention. Brown (2022) argues that there are at least four art modules that truly are specific to the arts in the context of human cognition and behavior. 1) Figurative drawing: generating figurative (iconic) re-creations of objects, people, or events, but doing so in two dimensions, rather than three, through a process of flattening. This occurs in the form of pictures and other two-dimensional graphic images. Figurative drawing is specific to the visual arts. 2) Acting: performing a re-creation of a person by pretending to be that person through character portrayal. It occurs predominantly in theatrical works, including theatre, film, and narrative forms of dance (e.g., ballet). 3) Metric entrainment: interpersonal synchronization of movement or vocalizing occurring in a regular, isometric rhythm, as is common in group dancing and chorusing. 4) Tonality: the organization of musical pitch space according to scaled pitches that are used recurrently in the generation of melodies and harmonies. It is specific to music.
What are the implications of art modules for the analysis of the art therapies? First off, they provide an evolutionary foundation for four of the major art therapies: figurative drawing for art therapy, acting for drama therapy, metric entrainment for dance therapy and music therapy, and tonality for music therapy. Art therapies, as compared to non-art therapies, can be seen as capitalizing on evolutionarily-novel, human-specific art functions that are distinct from language and other general functions of human cognition. This suggests that the mechanisms of action of the art therapies involve what we shall call an Added Value Principle: the arts add something novel and art-specific beyond the everyday functions targeted for treatment by the art therapies. They do so through the implementation of two types of factors. The first consists of the art modules that are unique to each art form, whereas the second consists of factors that are shared across all of the arts, such as opportunities for creative expression or the experience of beauty. Later in the article, we shall refer to these factors, respectively, as “specific factors” and “joint factors.” While there is no guarantee that adding value is necessarily going to make an art therapy more efficacious than a non-art therapy, a demonstration of efficacy can be reasonably attributed to the added value that is contributed by the art forms involved, at least in part, since both art modules and joint factors provide additional and unconventional routes for addressing the targeted functions.
3.3 Therapeutic Factors
This raises a critical point about the distinction between the “features” of an art therapy and the therapy’s “active ingredients,” typically referred to as “therapeutic factors” or simply “factors” (de Witte et al., 2021). Little more than armchair thinking is required to make a list of the characteristics of an art therapy, since these characteristics are generally those of the art form itself. For example, it is straightforward to recognize that dance therapy involves rhythmic body movements and social interactions with a partner, whereas art therapy involves the use of different types of physical media and the manipulation of tools to work with them. Saying that a given art therapy has certain desirable characteristics – like offering opportunities for creativity, the experience of beauty, or community building – says nothing at all about whether these features constitute the therapeutic factors that bring about its clinical effects. As it turns out, offering opportunities for creativity, the experience of beauty, and community building have been shown to be therapeutic factors based on quantitative studies (de Witte et al., 2021). However, factors such as these can be found to be effects of all of the art forms, as compared with the art-specificity of the art modules.
Factors such as these that are shared across all of the art therapies are referred to as “joint factors” when they can be shown to be responsible for bringing about clinical effects (de Witte et al., 2021). These factors are distinguished both from “specific factors” that are specific to each art therapy by virtue of their unique characteristics (i.e., the art modules) and from “common factors” that are shared not only among all art therapies but with non-art therapies as well (de Witte et al., 2021). These three categories of therapeutic factors are shown in Figure 3. The fact that each art therapy possesses specific features that are unique to that art form does not rule out the possibility that the art therapies as a whole might bring about their clinical effects through common and/or joint factors, rather than specific factors. In other words, the efficacy of the art therapies may be invariant with respect to differences in the features of the art forms that they employ.
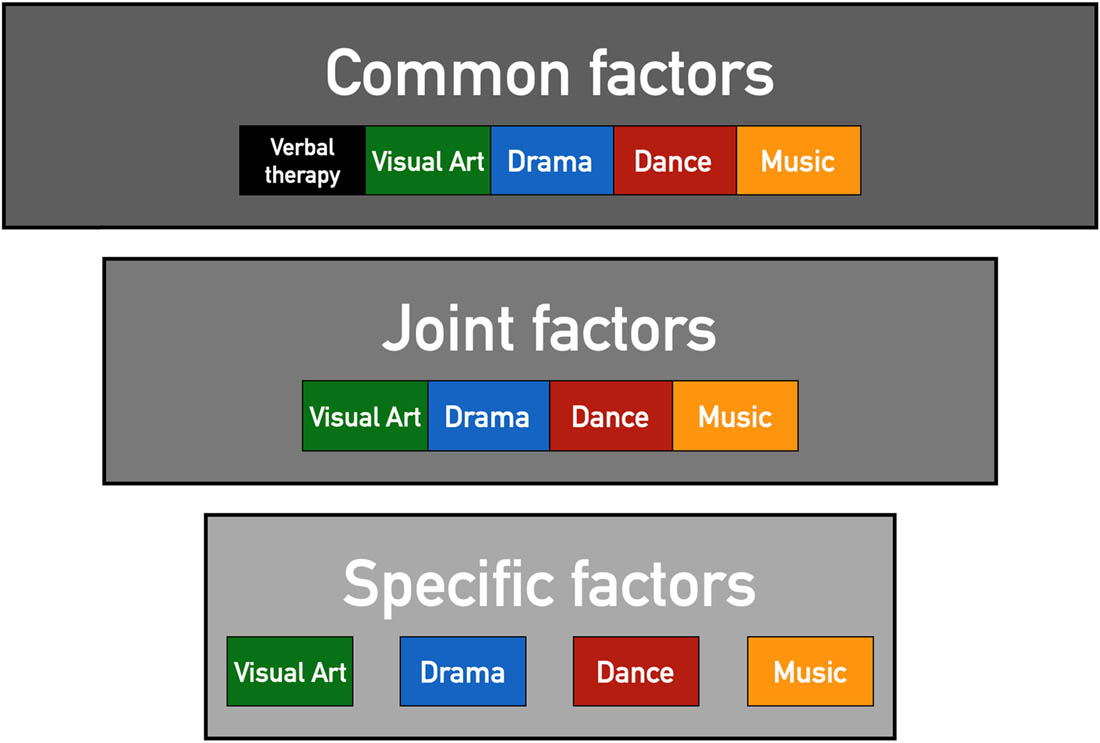
Art psychotherapies achieve therapeutic outcomes by means of a significant number of “common factors” that are shared across all forms of psychotherapy, whether arts or non-arts. They also contain “joint factors” that are shared among themselves, but that differ from therapeutic factors in verbal psychotherapy. Finally, they contain “specific factors” that are specific to each art therapy on its own by virtue of its unique characteristics (e.g., character portrayal in drama therapy and the use of musical scales in music therapy).
De Witte et al. (2021) carried out a detailed scoping review of the creative art psychotherapies with regard to change processes (as opposed to outcomes per se) in 67 studies of psychological well-being (but not physical therapy). They identified 19 domains of therapeutic factors for creative art therapies. Of these, only three were comprised solely of joint and specific factors that are exclusively applicable to the art psychotherapies, while the rest included at least one common factor applicable to all psychotherapies, whether art-based or not. The bottom line for our purposes is that caution must be exercised in claiming that the specific factors associated with any one art form or the joint factors associated with the art psychotherapies as a whole necessarily constitute the basis for their effects. Common factors may be more important in many cases, as will be discussed in greater detail below. Tables S5 and S6 provides a detailed analysis of common, joint, and specific factors.
4 Interactions: Combinations of Art Forms
As a first step in applying SPI thinking to art-based therapies, we will examine interactions. As mentioned earlier, art forms can interact by combining their domain-specific elements in time and/or space to create composite forms, such as when dance is choreographed to music or when poetry is set to music to create a song with words. While there is no guarantee that “more is better” when it comes to clinical efficacy, it might be the case that a combination provides an enhancement of the effects of the contributing art forms on their own, as has been suggested in the educational literature on multi-art combinations (Winner et al., 2013). Empirical and theoretical approaches to the clinical uses of the arts have had little to say about combinations. To the best of our knowledge, there has been no research comparing the efficacy of combined art therapies against that of single art therapies.
While the science of combinations does not currently exist in the applied arts, we can lay the groundwork for it by using UA theory. Brown (2018, 2022) provides a detailed discussion about art combinations, describing the coupling mechanisms for art forms in terms of their relative timing, strength, and directionality. Figure 4 serves as a guide for the current discussion. Combinations of art forms can be simultaneous, sequential (interleaved), or mixed. Among the simultaneous combinations, the coupling can be either blended or non-blended. Examples of blended combinations have already been mentioned, such as the choreographing of dance movements to music or the setting of a poem to music, where blending typically results from processes of phrase alignment that capitalize on rhythmic similarities (i.e., common stress patterns) across domains. However, there are also non-blended means of creating simultaneous combinations. For example, music can be played in the background during a session of drama therapy or during the creation of a visual artwork. Next, combinations can occur in a sequential or interleaved fashion, rather than in a simultaneous fashion. For example, a session of drama can be followed by a session of painting. Finally, we can imagine mixed formats in which a simultaneous format is interleaved with another art form in a sequential manner, such as when the singing of a song with words is interleaved with a session of painting.

Types of art combinations. The figure presents three manners of creating art combinations in applied uses of the arts: simultaneous, sequential (interleaved), and mixed. Examples of each type are shown.
Combinations, whether simultaneous or sequential, relate to parallels among art forms. For example, a given narrative idea can be conveyed using language, pantomimic gesture, or graphic images/objects. Similarly, a musical melody can be generated by means of vocalization at the larynx, by using the vocal tract to whistle or to blow air into a flute, or by using the hands and/or upper body to strike piano keys or to bow strings, among many other instrumental mechanisms. Likewise, the dramatic character of Juliet can be portrayed by a theatre actor who speaks or by a ballet dancer who is silent. Parallel production mechanisms can be used to generate the same or similar outcomes, both within an art form and between art forms, permitting a certain degree of interchangeability and complementarity among these mechanisms.
We would like to propose a Principle of Amplification that postulates that art combinations have the potential to be more efficacious than single art forms on their own. Another way of stating this is that multimodal mechanisms might be more efficacious than unimodal mechanisms. There is currently no empirical work validating the Principle of Amplification that “more is better,” and so there is a great need to carry out research in this area. Combinations offer a large but untapped clinical potential that merits exploration, as shown by analogous work on multi-art programs in education research (Winner et al., 2013).
5 Transfer Effects in Relation to Sharings and Parallels
We used the SPI concept of “interactions” in the previous section to talk about art form combinations and the potential amplification that such combinations might produce. In the current section, we will discuss the concepts of sharings and parallels in order to explain how art therapies might bring out their effects. Art therapies across theoretical orientations are predicated on what learning theorists refer to as transfer effects (Perkins & Salomon, 1992; Zelinski, 2009). Perkins and Salomon (1992) define them as follows: “Transfer of learning occurs when learning in one context enhances (positive transfer) or undermines (negative transfer) a related performance in another context. Transfer includes near transfer (to closely related contexts and performances) and far transfer (to rather different contexts and performances)” (p. 2, emphases added). Given that therapy involves instructing clients to overcome functional deficits, it would seem that any kind of therapy must rely on the transfer of what is learned within the therapy session to contexts beyond it. In addition to this “contextual” transfer, there is a “functional” or “featural” transfer by which features of the art activity are able to transfer to a dysfunctional system to either reactivate a dormant system or substitute for a deficient system. It is important to note that we are using “near” and “far” as relative terms, rather than as categorically distinct mechanisms of action. We think of the near/far distinction as more of a spectrum than a dichotomy, with many clinical applications having either intermediate or joint features of near and far transfer.
A straightforward example of transfer can be found in the use of dance as a physical therapy for Parkinson’s patients, one of the clearest success stories of the art therapies (Carapellotti et al., 2020; Dhami et al., 2015; Hackney & Earhart, 2009, 2010). Dance is anything but a regular everyday behavior for most people. However, dance shares many features with everyday movement patterns, since many dances are based on translational movements that resemble walking patterns. But dance contributes “added value” beyond basic locomotion, as per the Added Value Principle discussed earlier. It tends to be more structured, elaborate, and metrically timed than regular locomotor movements. For example, many dances incorporate movements in which the person walks backward or side-to-side or pivots their body (Hackney & Earhart, 2009). Many dances involve not just a single person moving on their own, but movement with one or more dance partners. In some cases, this may involve direct body contact, such as holding hands with people during a circle dance or forming a ballroom embrace with someone during a couple dance. When dance is done to music, the music provides an external timing signal that a person can entrain to in order to help stabilize movement timing. In addition, dances often contain many more moving parts in the body than just the lower limbs, for example, the upper limbs as well, resulting in complex synergies across the body. The bottom line is that these and other features of dance operate by transferring functionality onto the deficient motor system in the person with Parkinson’s disease. Dance therapy is not merely a means of practicing walking, but of supplementing walking with whole-body choreographic patterns, rhythmic timing signals, partnered interactions, emotive features of the music, and much more (Carapellotti et al., 2020; Dhami et al., 2015; McKee & Hackney, 2013). In this way, locomotor functioning is enhanced through the support of dance-specific features.
The example just presented provides a means of distinguishing near and far transfer. In near transfer, treatment efficacy is based on closely matching the qualities of a therapeutic intervention to the function(s) being targeted for enhancement or remediation. Near transfer is nicely exemplified by the case of dance therapy for Parkinson’s disease, where the treatment is highly matched to key domain-specific features of the affected condition. Dance, as an intervention, is well matched – and thus has the potential to transfer a desired effect – to the locomotor and balance disturbances being treated by the intervention.
Another example of a therapeutic approach that is based on near transfer is the use of singing-based therapies for speech and voice disorders. Two well-described examples are Melodic Intonation Therapy (MIT) for motor aphasia (Popescu et al., 2022; Sparks et al., 1974; Zumbansen & Tremblay, 2019) and Lee Silverman Voice Treatment (LSVT) for Parkinsonian dysphonia (Atkinson-Clement et al., 2015; Fox et al., 2006; Ramig et al., 2001; Yuan et al., 2020). Based on the logic of near transfer, you would not, for example, refer a patient with a gait disturbance to a singing-based therapy, nor would you refer a patient with motor aphasia to a dance-based therapy. Near transfer is based on strategically matching the domain-specific features of the intervention to the affected condition, hence dance therapy for gait and singing therapy for voice.
We are not aware of any literature looking at the inverse coupling (i.e., singing-based therapies to improve gait or dance-based therapies to improve speech). While music is certainly a key element in the treatment of movement-based disorders – such as in rhythmic auditory stimulation, patterned sensory enhancement, and therapeutic instrumental music performance (Bukowska et al., 2016; Koshimori & Thaut, 2018; Pereira et al., 2019; Sotomayor et al., 2021) – the music does not typically involve overt singing by the patient, but instead the use of exogenous musical rhythms that are then internalized mentally to aid in movement timing. Even in the exceptional cases where patients do sing overtly, such as that described by Harrison et al. (2019), singing still works by providing a metrical structure to help entrain the walking and does not improve walking on its own. Therefore, as a general principle, art-based physical therapies tend to rely on near transfer effects for their therapeutic efficacy and improve the functions they are targeting by adding value to the training of those functions beyond the ways that they are performed in daily life.
We would like to argue that SPI thinking provides critical insights into the contrast between near and far transfer for the art therapies. In particular, we propose that near transfer is based principally (although not exclusively) on sharings, whereas far transfer is based principally (although not exclusively) on parallels (Figure 5). For example, dance therapy for Parkinson’s disease is based on a sharing of locomotor mechanisms between dance and everyday walking, including features related to movement, balance, spatial cognition, motor timing, and so on (Hackney & Earhart, 2009, 2010).

The logic of sharings and parallels from unification theory accounts for the distinction between near transfer and far transfer, respectively, in the art therapies.
This contention is supported by neuroimaging studies. For example, Brown et al. (2006b) demonstrated that similar brain regions were activated between dancing and walking. This study also showed that the production of dance movements activated the basal ganglia, which is the part of the brain that undergoes damage in Parkinson’s disease. Finally, the study identified brain areas that are important for dancing but not walking, including those involved in metric entrainment to a musical beat, in support of the Added Value Principle. In like form, singing-based therapies for aphasia and dysphonia are based on a sharing of vocal processes between singing and speaking with regard to respiration, phonation, articulation, and prosody (Fox et al., 2006; Popescu et al., 2022; Zumbansen & Tremblay, 2019). The clinical effects of singing-based therapies are partly a result of the ways in which art modules add value. For example, neuroimaging studies comparing singing and speaking show a shift toward greater right-hemisphere brain activation for singing (Brown et al., 2006a) and the recruitment of brain areas for monitoring tonality in song perception (Callan et al., 2006). These findings might account for some of the beneficial effects of singing-based therapies on vocal functioning in Parkinson’s patients, as seen in neuroimaging studies of LSVT (Narayana et al., 2010). Both of these types of art therapies are predicated on strong domain-specific, intra-modal matching between the intervention and the affected condition, leading to near transfer.
5.1 Psychotherapy
Art-based psychotherapies, as compared to art-based physical therapies, present a more remote connection between the art form and what it treats, implying mechanisms of far transfer. We would argue that there are multiple parallel routes for achieving the kinds of self-expression and emotional communication that psychotherapy relies on, although they are manifested differentially across the art domains. As Figure 6 demonstrates, emotions can be expressed and communicated via 1) the creation of graphic images, 2) emotional language, 3) vocal prosody (with or without language), 4) tonality’s language of emotion through the use of musical scales, and 5) kinetic expression via the body and face. These diverse mechanisms can work independently, or they can be combined into composite forms of expression, such as combining emotional language with musical scales or combining expressive movement with music. We contend that emotion regulation is a “common factor” that operates across all of the psychotherapeutic modalities. As such, the art psychotherapies offer parallel means of working with emotion, using parallel channels of expression through image, language, voice, body, and face (Figure 6). This creates a situation whereby the art psychotherapies are relatively interchangeable, rather than being specific to a condition in the way that dance therapy shows specificity for gait disturbances in Parkinson’s disease or that singing therapies show specificity for speech and voice disturbances. This does not imply that the mechanisms of action of the arts in psychotherapy are fundamentally different from those in physical therapy, only that their application is more domain-linked in physical therapy and more domain-general in psychotherapy.

Parallel routes for self-expression and emotional communication, with a listing of the art psychotherapies that employ each route of expression.
In Figure 7, we attempt to present an integrative analysis of the psychotherapeutic applications of the arts with regard to two dimensions of their mechanism of action: the route of emotional expression and the narrative perspective. The check-marks in the figure indicate places where individual art psychotherapies intersect along these two dimensions. With respect to the routes of emotional expression (along the top of the figure), we divide them into two broad categories. The first consists of symbolic routes that employ visual media. These include the non-linguistic route for visual art (both two- and three-dimensional formats) and the linguistic route for expressive writing which employs emotional language, although without the voice and its prosodic mechanisms. The remaining expression routes are based on embodied performance. These include vocal prosody, the use of music’s tonal language of emotion, and kinetic expression of the body and face. Vocal prosody and musical expression use the acoustic route for expression – either through the voice or through instrumental surrogates for it – while facial expression and kinetic expression use the body route. We would argue that the performative routes for emotional expression are more “direct” than the symbolic routes of drawing and writing. As a point of reference, standard forms of verbal psychotherapy are restricted to the use of emotional language, as conveyed performatively through speech prosody. The art psychotherapies produce either a replacement of verbal language (e.g., drawing and dance movement) or a supplementing of it using art-specific mechanisms (e.g., singing words and speaking as a fictional character). In other words, they employ the art form as a complementary medium of exchange between the therapist and the client, which substitutes for verbal language during part or all of the session.

An analysis of the psychotherapeutic applications of the arts with regard to two salient dimensions: the modalities of emotional expression (either symbolic or performative) and the narrative perspective. The check-marks refer to the employment of these features by the art psychotherapies listed along the right side of the figure. The brackets for expressive speech in the top row indicate that some forms of music therapy combine lyrics with vocal music, hence creating a musicalized version of expressive speech. The downward arrow along the left side of the figure indicates that there is a progressive psychological distancing from the self as one proceeds from 1P to 3P to Fic1P. Abbreviations: expr., expression; psych., psychological.
The second dimension of the scheme (along the left side of the figure) consists of the narrative perspective engaged by the application. For this, we consider the standard literary perspectives of first-person (1P) and third-person (3P). We also list the perspective of an actor portraying a character, which is referred to as the “fictional first-person” (Fic1P) perspective. Regarding the 1P perspective, we distinguish the narrative form of it that is used in personal storytelling – and that dominates verbal psychotherapy – from a non-narrative self that engages in social activities like dance and music. The downward arrow along the left side of the figure indicates that there is a progressive psychological distancing from the self as one proceeds from 1P to 3P to Fic1P. Playing the role of a fictional character is the most distant condition from being oneself, although a non-literary means of achieving distance is through the use of visual media to create a non-embodied representation of the self through graphic media, such as images and objects.
6 Comparing the Art Psychotherapies to One Another and to Verbal Psychotherapies
The majority of art therapies are used for psychotherapeutic applications, rather than for physical rehabilitation (Gladding, 2011; Jones, 2021). The central issue about their therapeutic efficacy is not simply how the various art-based psychotherapies compare to one another, but how they compare with well-established verbal language psychotherapies (Figure 1), such as those based on 1) learning theory (e.g., cognitive, behavioral, or cognitive-behavioral therapies), 2) stimulating client insight (e.g., the various psychodynamic psychotherapies), and 3) humanistic psychology (e.g., gestalt therapy, existential therapy or logotherapy, and client-centered approaches to therapy across disciplines). The art psychotherapies may in fact adopt any of the theoretical orientations of the verbal language psychotherapies. They tend to differ from them only insofar as art forms are introduced as additional media of exchange between the therapist and client, substituting for some of the roles of the verbal discourse. For a summary of the art psychotherapies organized according to the art form and the expressive route that each one employs, refer to Figure 6.
In thinking about the mechanisms of action of the various art psychotherapies from a comparative perspective, we would like to propose another null hypothesis that can be addressed by future research in this field, what we shall call the Principle of Equivalence. The principle postulates that, when evaluating the efficacy of any psychotherapy at the level of large subject samples and the use of comparable control conditions, 1) the various art psychotherapies are equivalent to one another, and 2) the various art psychotherapies are equivalent to verbal language psychotherapies. Such equivalence is proposed to be attributed to the action of common factors that are shared by most if not all psychotherapies.
This suggestion of the equivalence or interchangeability of the art psychotherapies reflects a similar discussion about the equivalence of the various verbal-language psychotherapies, a well-established concept known in the literature by the unusual name of “the dodo bird verdict” (Budd & Hughes, 2009; Luborsky et al., 2002). This name is an allusion to the verdict given by a dodo bird when he is asked to judge the outcome of a race in Lewis Carroll’s Alice in Wonderland. The dodo bird affirms that “everybody has won, and all must have prizes,” a metaphor that was adopted by Rosenzweig (1936) to indicate that all forms of psychotherapy have comparable therapeutic benefits, despite methodological differences among them.
The major implication of the dodo bird verdict is that common factors across all of the psychotherapies are stronger agents of change than are factors specific to any one psychotherapy. For the art psychotherapies, this would render the art forms themselves as substitute media for the exchange of ideas that takes place via verbal language alone in traditional psychotherapies. Art psychotherapies introduce an art form as an additional medium of exchange between the therapist and client beyond verbal language, but this performs a similar function to verbal language in allowing a client to externalize their representation of the world for adaptive modification. If one consults texts about the various art psychotherapies (e.g., Gladding, 2011; Johnson, 1998; Jones, 2021), it becomes quite clear that much of the justification for using each of the art forms is quite similar across therapies, suggesting that common factors and joint factors are the predominant therapeutic mechanisms.
Common factors include the following: the structure of the session and its regularity and predictability; the capacity that psychotherapy provides for clients to learn and practice new skills; the responsibility that both the client and therapist have to the session, what has traditionally been called the “therapeutic alliance”; overcoming resistances and sacrificing the need for complete control; structuring or promoting positive emotions such as hope, providing a distraction from illness; social factors related to group therapy, such as creating opportunities for feelings of connectedness or acceptance; the opportunity for safe self-expression and emotional catharsis; the feeling of compatibility with or stimulation by the personality of the therapist; and a value for regular adherence to a single coherent model or theory that a client can learn from and use to contain their experiences (de Witte et al., 2021; Rosenzweig, 1936). Tables S5 and S6 provides a complete list of the therapeutic factors derived from the work of Rosenzweig (1936) and de Witte et al. (2021).
The Principle of Equivalence – the notion that common and joint factors are responsible for the bulk of the clinical effects of art psychotherapies – follows from our contention in the previous section that the various art psychotherapies employ parallel expressive routes for achieving the same general outcome, namely the expressive representation of the self. While expressive routes vary between the art psychotherapies (Figure 6), they may, in fact, be intrinsically comparable with regard to their efficacy in conveying therapeutically relevant information, in which case the major determinants of clinical efficacy would revolve around individual differences in affinity for the expressive route(s) employed by each therapy. Such affinities may be due to a client’s intrinsic preference for one expressive route over another. For example, clients who prefer to express themselves artistically may show an affinity for art psychotherapies over verbal therapies. Likewise, a client with an impairment in a particular route of expression might prefer therapies that do not employ it. For example, non-verbal clients, for whom verbal language is inaccessible as a route of expression, may show an affinity for psychotherapies that employ non-verbal expressive routes, such as dance movement therapy or visual art therapy.
Such preference-based factors will unquestionably have a significant impact on a client’s adherence to an art psychotherapy program. This might suggest a Principle of Affinity by which clients are more likely to benefit from certain art interventions than others, as based on a combination of individual differences in preferences for art forms and individual differences in skill at producing a given art form as an expressive activity. While theorists of the art psychotherapies are quick to point out that clients in no way need to have prior expertise in a given art form in order for that modality to be useful and effective (Jones, 2021), it may be the case that some people are so uncomfortable with activities like singing, dancing, or improvising that art psychotherapies that incorporate these activities will lead to resistance, attrition, and poor treatment outcomes.
6.1 Meta-analytic Approaches to Treatment Effects
The Principle of Equivalence requires validation from empirical analyses. The quantitative literature on the efficacy of art psychotherapies is relatively new, and the literature that does exist – and in particular, the meta-analytic literature – has focused principally on evaluating the efficacy of art psychotherapies for regulating mood and anxiety, perhaps because such disorders have become increasingly prevalent in society (Baxter et al., 2013; Lambert, 2006). We have not been able to find any other psychological disorders for which a sufficient number of meta-analyses are available to evaluate treatment efficacy across art domains.
Tables S1–S4 provides a complete summary of the 45 meta-analyses that we have reviewed of the art psychotherapies used for the treatment of mood and anxiety disorders (among other conditions), including descriptions of core findings and effect sizes. Examples from this literature include meta-analyses of interventions involving expressive writing for depression (Reinhold et al., 2018) and anxiety (Qian et al., 2020), visual art for depression and anxiety (Newland & Bettencourt, 2020), drama in the form of play for anxiety (Bratton et al., 2005) (but with no meta-analyses to our knowledge assessing drama or play for depression), music for depression (Zhao et al., 2016) and anxiety (Panteleeva et al., 2018), and dance for depression (Karkou et al., 2019) (but with no meta-analyses to our knowledge assessing dance for anxiety), among other similar meta-analyses. The supplementary table reveals that effect sizes tend to be small to medium, with very few studies showing large effect sizes.
Also common in the meta-analytic literature on the art psychotherapies are “pooled outcome variable” meta-analyses in which the treatment outcomes of a given art psychotherapy for a variety of conditions are viewed together as part of an “overall” assessment of the efficacy of such art psychotherapies for treating mental illness broadly. This has been the case with newer literatures for which insufficient studies exist to formulate meta-analyses examining the efficacy of an art psychotherapy in treating a single disorder or symptom complex [e.g., the meta-analysis by Leblanc & Ritchie (2001) on play therapy]. These meta-analyses are presented here out of convenience as a way of illustrating a pattern. They are by no means exhaustive.
Let us consider the treatment of a condition like depression. Can the same logic of near transfer that was used to justify the choice of dance therapy for the motoric symptoms of Parkinson’s disease be used to justify the choice between art therapy, drama therapy, dance therapy, and music therapy for depression? We would contend that it cannot. Because a client’s mood, cognition, and behavior are higher-order domains of functioning, they are conveyable and thus modifiable via multiple parallel routes of expression. These domains of functioning can be approached equivalently using many different art forms and, by extension, can be treated by various types of psychotherapies, whether art-based or not. If this can reliably be shown to be the case through a rich outcome-based literature demonstrating equivalent effects when comparing art psychotherapies in treating any given psychological disturbance, then it would suggest that the arts are overall interchangeable when it comes to psychotherapy applications, in contrast to the specificity that we argued for in the case of physical therapy applications.
While the dodo bird verdict was proposed for the verbal language psychotherapies, it has not been examined with regard to the art psychotherapies, to the best of our knowledge. This is in part due to the fact that the art psychotherapies have not thus far been rigorously and reliably studied quantitatively. The quantitative literature is simply too new and too heterogeneous in methodology to allow for meta-analyses that would allow for direct cross-arts comparisons of the art psychotherapies among themselves or to verbal language psychotherapies for that matter. However, it is our contention that the dodo bird verdict will likely be shown to apply to the art psychotherapies.
One can glean some important information from an indirect analysis of this issue. More specifically, when different domain-specific meta-analyses are used to assess the efficacy of different art psychotherapies against the same types of control conditions, the general observation is that similar effect sizes are found across them. For example, the meta-analyses of Karkou et al. (2019) and Gold et al. (2004) demonstrated medium effect sizes for dance psychotherapy and music psychotherapy, respectively, in treating depression when each one was compared against treatment-as-usual controls. Similarly, art psychotherapies and verbal psychotherapies show similar effect sizes when each category is compared against similar controls. For example, the meta-analyses of Arnberg and Öst (2014) and Karkou et al. (2019) revealed that cognitive-behavioral therapy and dance psychotherapies, respectively, produced medium effect sizes in treating depression when each one was compared against activity-matched or treatment-as-usual controls. This suggests not only sample-level interchangeability of the art psychotherapies with one another but with verbal psychotherapies as well. While this indirect method of comparing the psychotherapies is far from conclusive, it does suggest that there is a certain degree of equivalence among the psychotherapies.
A possible argument against our proposal of the equivalence of the art psychotherapies is that, while meta-analyses of the different art psychotherapies generally produce similar effect sizes when similar control conditions are used in the contributing studies, meta-analyses for some art psychotherapies consistently report smaller effect sizes than others. One methodological feature that could weaken the above argument relates to the rather significant differences in the types of studies that contribute to the meta-analyses. Among the 45 meta-analyses that we have sampled to form our theory (Tables S1–S4), we have observed a trend in which studies of the art psychotherapies tend to show larger effect sizes when 1) clinical samples are used (i.e., where participants with a clinically relevant condition such as depression are given the experimental treatment, rather than healthy participants from the general population), 2) multiple sessions (i.e., at least two, usually over the span of multiple weeks) and longer sessions (i.e., at least one hour) are carried out, and 3) some kind of therapeutic activity (usually some number of sessions of actual therapy) is used that employs the common factors that are known to facilitate healing (Tables S5 and S6 lists these factors). Such therapeutic activities usually involve sessions of the art psychotherapies under study, but can more broadly include any relationship with a mental health professional who gives feedback to participants as they undergo the experimental treatment. Domains of the art psychotherapies whose studies lack these features tend to show smaller effect sizes than those that do. In other words, methodological biases associated with the research studies on the different art psychotherapies may do more to explain apparent differences in clinical outcomes than any intrinsic differences in the clinical efficacy of the art psychotherapies themselves.
This critique applies most especially to the meta-analytic literature on expressive writing. For example, Mogk et al. (2006) examined expressive writing in the treatment of “stressful or traumatic experiences,” and Reinhold et al. (2018) did the same for the treatment of depressive symptoms. Both meta-analyses showed negligible effect sizes. Almost all of the included studies in these meta-analyses involved short expressive-writing episodes spanning 1–5 days and an absence of an interaction with a therapist. What this suggests is that the methodological paradigm that is used in expressive-writing studies tends to exclude the kinds of common factors that are known to produce clinical transformation, for example, a suitable duration of treatment and an interaction with a benevolent and invested other. Individual expressive-writing studies that overcome these limitations tend to show larger effect sizes (Mogk et al., 2006; Reinhold et al., 2018; Sloan & Marx, 2004).
7 An Overall View
In order to provide a synthesis of the major points raised in this article, Figure 8 presents a comparative analysis of the art therapies with regard to their application to either physical therapy (e.g., gait disturbances in Parkinson’s disease) or psychotherapy (e.g., depression). While the picture presented in the figure might be seen as overly dichotomous, it attempts to highlight the contrastive findings that are observed between physical therapies and psychotherapies when it comes to art applications. It is worth pointing out that most approaches to the clinical uses of the arts focus exclusively on either physical therapy applications or psychotherapy applications, but not both. This leads to disciplinary distinctions such as that between dance therapy (mainly physical therapy) and dance movement therapy (mainly psychotherapy). Likewise, the excellent monographs of Gladding (2011) and Jones (2021) only discuss the psychotherapeutic uses of the arts and not the physical therapy applications. We are not aware of any literature that attempts to combine these two types of uses under a single umbrella of the clinical uses of the arts. An important unification is needed in this area.

A comparison of the art therapies for either physical therapy or psychotherapy with regard to their respective reliance on either near or far transfer.
The figure makes the point that physical therapy relies on therapeutic applications associated with intramodal near transfer (sharings) having high specificity for the art application and that tend to produce medium to large effect sizes in meta-analyses and randomized control trials. This applies to the aforementioned treatments such as dance therapy for Parkinson’s disease (Carapellotti et al., 2020), as well as MIT (Popescu et al., 2022; Sparks et al., 1974; Zumbansen & Tremblay, 2019) and LSVT (Atkinson-Clement et al., 2015; Fox et al., 2006) for speech/voice disorders. Evidence from meta-analyses suggests that these therapies tend to produce clinical outcomes that are comparable to conventional non-art therapies. The situation for the psychotherapeutic applications of the arts tends to present a different picture. Psychotherapeutic applications are associated with far transfer based on parallel routes for self-expression and emotional communication that show relatively low specificity for the art application and thus interchangeability. The meta-analysis data tend to suggest that these applications produce small to medium effect sizes (Tables S1–S4).
We can consolidate these observations into a Principle of Proximity that postulates that therapies based on near transfer (i.e., sharings) tend to produce larger clinical effects than therapies based on far transfer (i.e., parallels). What this implies is that intramodal sharings are more efficacious than cross-modal parallels. Near transfer not only produces larger effects than far transfer among the art therapies themselves, but art therapies based on near transfer tend to produce effects that are comparable to non-art physical therapies. The opposite is true for therapies based on far transfer and parallels. This disparity may be due to the amount of effort that is required for the learning that is involved in far versus near transfer (Perkins & Salomon, 1992). Because near transfer in physical therapy involves direct training of a bodily function, the transfer is essentially automatic. By contrast, far transfer in psychotherapy requires additional effort at abstracting what is learned in the therapy session in order to apply it in everyday life.
One benefit of the therapies that are based on far transfer is that they offer multiple manners for achieving comparable clinical outcomes through the various parallel routes that they afford. This offers more routes for achieving a given clinical outcome than is possible for an approach that is constrained by domain-specific mechanisms. This is well exemplified by the psychotherapeutic approaches. Hence, there may be a trade-off between clinical efficacy and flexibility.
While we have discussed the physical therapies and psychotherapies separately in this article, there are clearly conditions that produce both physical and psychological symptoms. In such situations, a modular view of treatment would call for each type of symptom to be treated independently. To take but one example, Parkinson’s disease is highly comorbid with depression (Poewe & Luginger, 1999). As a result, dance-based approaches for targeting movement disturbances in Parkinson’s disease may not be adequate for treating mood disturbances in depression, despite the well-known emotional benefits of dance for many people. Instead, programs for the treatment of Parkinsonian depression need to be applied that are similar to those for other varieties of depression (Veazey et al., 2005). A Principle of Modularity would suggest that, for diseases having both physical and psychological symptoms, treatment should be approached in a modular manner: use physical therapies (and/or pharmacotherapies) to target the physical symptoms, and use psychotherapies (and/or pharmacotherapies) to target the psychological symptoms.
8 Limitations
While this work offers a unified view of the art therapies – attempting to relate the various therapies to one another mechanistically – it suffers from a number of limitations. First off, the work has presented a qualitative picture of the literature as a whole in the form of a narrative review, rather than using statistical methods. We relied on the published meta-analyses to provide measurements of effect sizes, rather than surveying a large number of individual experimental studies. Second, our contention of a “dodo bird verdict” for the psychotherapy applications may be perceived as denigrating the individual art therapies, which is of course not our intention. While we would be happy for future research to compellingly demonstrate that specific factors outweigh common and joint factors in certain forms of art-based psychotherapy, the literature in its current form does not make a strong case for this idea and instead points to common factors as being clear agents of change in psychotherapeutic applications of the arts. Third, the dichotomy that we have presented between physical therapy and psychotherapy is almost certainly an oversimplification. While it is indeed the case that physical rehabilitation and mental health applications tend to be studied in distinct literatures, physical and psychological symptoms are comorbid in many clinical situations. Finally, the meta-analysis literature that we sampled mainly covered studies of individual therapy, and so our conclusions have not been tested against the art-based group therapy literature, for which there are few quantitative meta-analyses. This is particularly problematic for the coordinative arts of dance and music that often achieve their impact on human cognition and behavior by means of group performance. However, meta-analyses of non-art therapies have shown that group sessions are as effective as individual sessions on the scale of large subject samples (Smith & Glass, 1977), and so we would expect that our contentions about the individual therapies would extend to group therapies as well.
9 Conclusions: Toward a New Science of the Applied Arts
We have attempted in this article to lay the groundwork for a new science of the clinical uses of the arts. We have presented concepts from a unified model of the arts in order to enlighten the clinical uses of the arts in both physical therapy and psychotherapy. We capitalized on key concepts from Brown’s (2022) “unification of the arts” model in doing so. The basic ingredients of this new science include the following. 1) A classification scheme for the arts that is able to categorize the art therapies and characterize the relationships among them. 2) A consideration of novel, human-specific art modules, and how these functions contribute added value to the everyday functions being targeted by the application, doing so in a domain-specific fashion. 3) A consideration of art interactions, and how art forms are able to combine with one another to create hybrid multi-art therapies. This occurs through parallel production mechanisms, leading to the hitherto-unexplored potential for amplification of the clinical effects of these combinations. 4) SPI (sharing/parallel/interaction) thinking contributes to a new understanding of the mechanisms of action of the art therapies via near transfer (domain-specific sharings) and far transfer (domain-general parallels) effects. This leads to a general approach to the distinction between art specificity and interchangeability in the art therapies.
We examined the clinical effects of the arts in both physical therapy and psychotherapy. A review of the meta-analysis literature indicates that physical-therapy applications based on near transfer through shared physiological mechanisms produce larger clinical effects than psychotherapy applications based on parallel routes for self-expression and emotional communication through far transfer. As a result, physical-therapy applications can show comparable efficacy to traditional non-art treatments, whereas psychotherapy applications have relatively smaller effect sizes and are equivalent to or worse than standard verbal psychotherapy. We described the therapeutic advantage of near-transfer effects as a Principle of Proximity. For far transfer, especially with respect to the parallel routes of emotional expression in psychotherapy applications, we invoked a Principle of Equivalence – which is an extension of the dodo bird verdict from psychotherapy – in which a Principle of Affinity might influence an individual’s receptivity and responsiveness to one psychotherapy over another, but where the psychotherapies, including the art psychotherapies, are equivalently effective on the scale of large subject samples in research studies.
This article has presented a general framework that can guide future research and practice on the clinical applications of the arts. We see two important roads that require the most immediate attention. The first is about art combinations and the clinical potential of amplification in multi-art therapies. As mentioned earlier, there has been virtually no research exploring the relative efficacy of combinations compared to single art forms. There might be much potential to be gained in this area, just as there is in the arts education literature. The second is about refining our ideas regarding near and far transfer via sharings and parallels, respectively. We have presented preliminary ideas about these concepts in our discussion of dance therapy for Parkinson’s disease versus movement therapy for depression. Ultimately, just as “a comparative analysis of the arts provides greater insight into each art form than is possible by looking at art forms in isolation,” the same is true of the art therapies themselves. Much can be gleaned by taking a comparative approach to the art therapies and moving beyond a “restaurant menu” model that sees the art forms as a toolkit of alternative modalities.
A unified model of the art therapies offers much promise in providing a rational understanding of their therapeutic mechanisms. While we are not currently proposing a “system” or protocol for selecting among the art therapies to best suit their applications, we do believe that the concepts presented in this article could serve as the foundation for a unified art therapy that optimizes the selection, combination, and sequencing of the arts and that offers practical guidance for clients interested in optimizing their treatment outcomes in an individualized manner.
People interested in physical therapies should consider art-based physical therapies over traditional exercise-based therapies because of the ways in which art-based activities add value to the therapy and because they demonstrate greater clinical efficacy than traditional therapeutic exercises. People interested in psychotherapy should consider an art therapy as a potential alternative to verbal therapy, although verbal therapies can be quite effective. They should choose the art modality that they are most interested in committing to based on their preferences. But they should also consider sampling among several different modalities in order to explore the various complementary routes to self-expression and emotional communication that are afforded by the arts, as is promoted in EXAT. Finally, and following from the Principle of Modularity, people seeking to address both physical and psychological symptoms should select different treatments to target each of their symptoms, rather than attempting to find one treatment for all of their symptoms.
Acknowledgments
We are grateful to Madeleine Hackney (Emory University) and the members of the NeuroArts Lab for their critical reading of the manuscript and their comments for improvement. We thank Martina de Witte (University of Amsterdam) and Hod Orkibi (University of Haifa) for their permission to reprint a slightly modified version of Table 4 from the study by de Witte et al. (2021) as Tables S5 and S6 in the present article.
-
Funding information: This work was supported by grants to SB from the Natural Sciences and Engineering Research Council (NSERC) of Canada (grant number RGPIN-2020-05718) and the Social Sciences and Humanities Research Council (SSHRC) of Canada (grant number 435-2017-0491).
-
Conflict of interest: The authors state no conflict of interest.
-
Ethical approval: The conducted research is not related to either human or animals use.
-
Data availability statement: Data sharing is not applicable to this article as no datasets were generated or analyzed during the current study.
References
Aristotle. (335BC/1996). Poetics. London: Penguin Books.Search in Google Scholar
Arnberg, A., & Öst, L. G. (2014). CBT for children with depressive symptoms: A meta-analysis. Cognitive Behaviour Therapy, 43(4), 275–288. doi: 10.1080/16506073.2014.947316.Search in Google Scholar
Atkinson-Clement, C., Sadat, J., & Pinto, S. (2015). Behavioral treatments for speech in Parkinson’s disease: Meta-analyses and review of the literature. Neurodegenerative Disease Management, 5(3), 233–248. doi: 10.2217/nmt.15.16.Search in Google Scholar
Batteux, C. (1746/2015). The fine arts reduced to a single principle. J. O. Young (Trans.) Oxford: Oxford University Press.10.1093/oseo/instance.00184601Search in Google Scholar
Baxter, A. J., Scott, K. M., Vos, T., & Whiteford, H. A. (2013). Global prevalence of anxiety disorders: A systematic review and meta-regression. Psychological Medicine, 43(5), 897–910. doi: 10.1017/S003329171200147X.Search in Google Scholar
Bratton, S. C., Ray, D., Rhine, T., & Jones, L. (2005). The efficacy of play therapy with children: A meta-analytic review of treatment outcomes. Professional Psychology: Research and Practice, 36(4), 376–390. doi: 10.1037/0735-7028.36.4.376.Search in Google Scholar
Brown, S. (2018). Toward a unification of the arts. Frontiers in Psychology, 9, 1938. doi: 10.3389/fpsyg.2018.01938.Search in Google Scholar
Brown, S. (2019). A unifying model of the arts: The narration/coordination model. Empirical Studies of the Arts, 37, 172–196. doi: 10.1177/0276237419828213.Search in Google Scholar
Brown, S. (2022). The unification of the arts: A framework for understanding what the arts share and why. Oxford: Oxford University Press.10.1093/oso/9780198864875.001.0001Search in Google Scholar
Brown, S., Martinez, M. J., & Parsons, L. M. (2006a). Music and language side by side in the brain: A PET study of the generation of melodies and sentences. European Journal of Neuroscience, 23(10), 2791–2803. doi: 10.1111/j.1460-9568.2006.04785.x.Search in Google Scholar
Brown, S., Martinez, M. J., & Parsons, L. M. (2006b). The neural basis of human dance. Cerebral Cortex, 16, 1157–1167. doi: 10.1093/cercor/bhj057.Search in Google Scholar
Budd, R., & Hughes, I. (2009). The Dodo Bird Verdict: Controversial, inevitable and important. A commentary on 30 years of meta-analyses. Clinical Psychology & Psychotherapy, 16(6), 510–522. doi: 10.1002/cpp.648.Search in Google Scholar
Bukowska, A. A., Krężałek, P., Mirek, E., Bujas, P., & Marchewka, A. (2016). Neurologic music therapy training for mobility and stability rehabilitation with Parkinson’s disease: A pilot study. Frontiers in Human Neuroscience, 9, 710. doi: 10.3389/fnhum.2015.00710.Search in Google Scholar
Callan, D. E., Tsytsarev, V., Hanakawa, T., Callan, A. M., Katsuhara, M., Fukuyama, H., & Turner, R. (2006). Song and speech: Brain regions involved with perception and covert production. Neuroimage, 31, 1327–1342. doi: 10.1016/j.neuroimage.2006.01.036.Search in Google Scholar
Carapellotti, A. M., Stevenson, R., & Doumas, M. (2020). The efficacy of dance for improving motor impairments, non-motor symptoms, and quality of life in Parkinson’s disease: A systematic review and meta-analysis. PLoS ONE, 15(8), e0236820. doi: 10.1371/journal.pone.0236820.Search in Google Scholar
Cohen, A. J. (2013). Film music. In S.-L Tan & A. J. Cohen (Eds.), The psychology of music in multimedia (pp. 17–47). Oxford: Oxford University Press.10.1093/acprof:oso/9780199608157.003.0002Search in Google Scholar
de Witte, M., Orkibi, H., Zarate, R., Karkou, V., Sajnani, N., Malhotra, B., Tin Hung Ho, R., Kaimal, G., Baker, F. A., & Koch, S. C. (2021). From therapeutic factors to mechanisms of change in the creative arts therapies: A scoping review. Frontiers in Psychology, 12, 678397. doi: 10.3389/fpsyg.2021.678397.Search in Google Scholar
Dhami, P., Moreno, S., & DeSouza, J. F. X. (2015). New framework for rehabilitation - Fusion of cognitive and physical rehabilitation: The hope for dancing. Frontiers in Psychology, 5, 1478. doi: 10.3389/fpsyg.2014.01478.Search in Google Scholar
Fancourt, D., & Finn, S. (2019). What is the evidence on the role of the arts in improving health and well-being? A scoping review. Copenhagen: World Health Organization. Regional Office for Europe.Search in Google Scholar
Fox, C. M., Ramig, L. O., Ciucci, M. R., Sapir, S., McFarland, D. H., & Farley, B. G. (2006). The science and practice of LSVT/LOUD: Neural plasticity-principled approach to treating individuals with Parkinson disease and other neurological disorders. Seminars in Speech and Language, 27(4), 283–299.10.1055/s-2006-955118Search in Google Scholar
Gladding, S. T. (2011). The creative arts in counseling (4th ed). Alexandria, VA: American Counseling Association.Search in Google Scholar
Gold, C., Voracek, M., & Wigram, T. (2004). Effects of music therapy for children and adolescents with psychopathology: A meta-analysis. Journal of Child Psychology and Psychiatry, 45(6), 1054–1063. doi: 10.1111/j.1469-7610.2004.t01-1-00298.x.Search in Google Scholar
Gorbman, C. (1987). Unheard melodies: Narrative film music. Bloomington, IN: Indiana University Press.Search in Google Scholar
Hackney, M. E., & Earhart, G. M. (2009). Effects of dance on movement control in Parkinson’s disease: A comparison of Argentine tango and American ballroom. Journal of Rehabilitation Medicine, 41(6), 475–481. doi: 10.2340/16501977-0362.Search in Google Scholar
Hackney, M. E., & Earhart, G. M. (2010). Effects of dance on gait and balance in Parkinson’s disease: A comparison of partnered and nonpartnered dance movement. Neurorehabilitation and Neural Repair, 24(4), 384–392. doi: 10.1177/1545968309353329.Search in Google Scholar
Halliwell, S. (2014). Diegesis - mimesis. In P. Huehn (Ed.), The living handbook of narratology (pp. 129–137). Berlin: de Gruyter.10.1515/9783110316469.129Search in Google Scholar
Harrison, E. C., Horin, A. P., & Earhart, G. M. (2019). Mental singing reduces gait variability more than music listening for healthy older adults and people with Parkinson disease. Journal of Neurologic Physical Therapy, 43, 204–211. doi: 10.1097/NPT.0000000000000288.Search in Google Scholar
Johnson, D. R. (1998). On the therapeutic action of the creative arts therapies: The psychodynamic model. The Arts in Psychotherapy, 25(2), 85–99. doi: 10.1016/S0197-4556(97)00099-3.Search in Google Scholar
Jones, P. (2021). The arts therapies: A revolution in healthcare. (2nd ed.). London: Routledge.10.4324/9781315536989-2Search in Google Scholar
Karkou, V., Aithal, S., Zubala, A., & Meekums, B. (2019). Effectiveness of dance movement therapy in the treatment of adults with depression: A systematic review with meta-analyses. Frontiers in Psychology, 10, 936. doi: 10.3389/fpsyg.2019.00936.Search in Google Scholar
Knill, P. J., Barba, H. N., & Fuchs, M. N. (2004). Minstrels of the soul: Intermodal expressive therapy. (2nd ed.). Toronto: EGS Press.Search in Google Scholar
Koshimori, Y., & Thaut, M. H. (2018). Future perspectives on neural mechanisms underlying rhythm and music based neurorehabilitation in Parkinson’s disease. Ageing Research Reviews, 47, 133–139. doi: 10.1016/j.arr.2018.07.001.Search in Google Scholar
Kristeller, P. O. (1952). The modern system of the arts: A study in the history of aesthetics (II). Journal of the History of Ideas, 13, 17–46. doi: 10.1017/CBO9781107415324.004.Search in Google Scholar
Lambert, K. G. (2006). Rising rates of depression in today’s society: Consideration of the roles of effort-based rewards and enhanced resilience in day-to-day functioning. Neuroscience & Biobehavioral Reviews, 30(4), 497–510. doi: 10.1016/j.neubiorev.2005.09.002.Search in Google Scholar
Leblanc, M., & Ritchie, M. (2001). A meta-analysis of play therapy outcomes. Counselling Psychology Quarterly, 14(2), 149–163. doi: 10.1080/09515070110059142.Search in Google Scholar
Lerdahl, F. (2013). Musical syntax and its relation to linguistic syntax. In M. A. Arbib (Ed.), Language, music, and the brain (pp. 257–272). Cambridge, MA: MIT Press.10.7551/mitpress/9780262018104.003.0010Search in Google Scholar
Luborsky, L., Rosenthal, R., Diguer, L., Andrusyna, T. P., Berman, J. S., Levitt, J. T., Seligman, D. A., & Krause, E. D. (2002). The dodo bird verdict is alive and well--mostly. Clinical Psychology: Science and Practice, 9(1), 2–12. doi: 10.1093/clipsy.9.1.2.Search in Google Scholar
Malek, J. M. (1974). The arts compared: An aspect of eighteenth-century British aesthetics. Detroit: Wayne State University Press.Search in Google Scholar
McCrary, J. M., Redding, E., & Altenmüller, E. (2021). Performing arts as a health resource? An umbrella review of the health impacts of music and dance participation. PLoS ONE, 16, e0252956. doi: 10.1371/journal.pone.0252956.Search in Google Scholar
McKee, K. E., & Hackney, M. E. (2013). The effects of adapted tango on spatial cognition and disease severity in Parkinson’s disease. Journal of Motor Behavior, 45(6), 519–529. doi: 10.1080/00222895.2013.834288.Search in Google Scholar
Mogk, C., Otte, S., Reinhold-Hurley, B., & Kröner-Herwig, B. (2006). Health effects of expressive writing on stressful or traumatic experiences: A meta-analysis. Psycho-Social Medicine, 3, 1–9. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2736499/.Search in Google Scholar
Narayana, S., Fox, P. T., Zhang, W., Franklin, C., Robin, D. A., Vogel, D., & Ramig, L. O. (2010). Neural correlates of efficacy of voice therapy in Parkinson’s disease identified by performance-correlation analysis. Human Brain Mapping, 31(2), 222–236. doi: 10.1002/hbm.20859.Search in Google Scholar
Newland, P., & Bettencourt, B. A. (2020). Effectiveness of mindfulness-based art therapy for symptoms of anxiety, depression, and fatigue: A systematic review and meta-analysis. Complementary Therapies in Clinical Practice, 41, 101246. doi: 10.1016/j.ctcp.2020.101246.Search in Google Scholar
Panteleeva, Y., Ceschi, G., Glowinski, D., Courvoisier, D. S., & Grandjean, D. (2018). Music for anxiety? Meta-analysis of anxiety reduction in non-clinical samples. Psychology of Music, 46(4), 473–487. doi: 10.1177/0305735617712424.Search in Google Scholar
Patel, A. D. (2008). Music, language, and the brain. Oxford: Oxford University Press.Search in Google Scholar
Pereira, A. P. S., Marinho, V., Gupta, D., Magalhaes, F., Ayres, C., & Teixeira, S. (2019). Music therapy and dance as gait rehabilitation in patients with Parkinson disease: A review of evidence. Journal of Geriatric Psychiatry and Neurology, 32(1), 49–56. doi: 10.1177/0891988718819858.Search in Google Scholar
Perkins, D., & Salomon, G. (1992). Transfer of learning. International Encyclopedia of Education, 2, 6452–6457.Search in Google Scholar
Perrot, S. (2016). The apotropaic function of music inside the sanctuaries of Asklepios: Ritual soundscape and votive offerings. Greek and Roman Musical Studies, 4(2), 209–230.10.1163/22129758-12341276Search in Google Scholar
Plato. (380BC/1968). The republic. New York: Basic Books.Search in Google Scholar
Poewe, W., & Luginger, E. (1999). Depression in Parkinson’s disease: Impediments to recognition and treatment options. Neurology, 52(7), S2-6.Search in Google Scholar
Popescu, T., Stahl, B., Wiernik, B. M., Helm, H., Zemanek, M., Haiduk, F., Matzinger, T., Beisteiner, R., & Fitch, T. W. (2022). Melodic Intonation Therapy for aphasia: A multi-level meta-analysis. MedRxiv. doi: 10.1101/2021.08.28.21262764.Search in Google Scholar
Porter, J. I. (2009). Is art modern? Kristeller’s “Modern System of the Arts” reconsidered. British Journal of Aesthetics, 49, 1–24. doi: 10.1093/aesthj/ayn054.Search in Google Scholar
Qian, J., Zhou, X., Sun, X., Wu, M., Sun, S., & Yu, X. (2020). Effects of expressive writing intervention for women’s PTSD, depression, anxiety and stress related to pregnancy: A meta-analysis of randomized controlled trials. Psychiatry Research, 288, 112933. doi: 10.1016/j.psychres.2020.112933.Search in Google Scholar
Ramig, L. O., Sapir, S., Countryman, S., Pawlas, A. A., O’Brien, C., Hoehn, M., & Thompson, L. L. (2001). Intensive voice treatment (LSVT) for patients with Parkinson’s disease: A 2 year follow up. Journal of Neurology, Neurosurgery & Psychiatry, 71(4), 493–498. doi: 10.1136/jnnp.71.4.493.Search in Google Scholar
Reinhold, M., Bürkner, P.-C., & Holling, H. (2018). Effects of expressive writing on depressive symptoms: A meta-analysis. Clinical Psychology: Science and Practice, 25(1), e12224. doi: 10.1111/cpsp.12224.Search in Google Scholar
Robbins, A. (Ed.). (1997). Therapeutic presence: Bridging expression and form. London: Jessica Kingsley Publishers.Search in Google Scholar
Rosenzweig, S. (1936). Some implicit common factors in diverse methods of psychotherapy. American Journal of Orthopsychiatry, 6(3), 412–415. doi: 10.1037/1053-0479.12.1.5.Search in Google Scholar
Shiner, L. (2001). The invention of art: A cultural history. Chicago: University of Chicago Press.10.7208/chicago/9780226753416.001.0001Search in Google Scholar
Shiner, L. (2009). Continuity and discontiuity in the concept of art. British Journal of Aesthetics, 49, 159–169. doi: 10.1093/aesthj/ayp006.Search in Google Scholar
Sloan, D. M., & Marx, B. P. (2004). A closer examination of the structured written disclosure procedure. Journal of Consulting and Clinical Psychology, 72(2), 165–175. doi: 10.1037/0022-006X.72.2.165.Search in Google Scholar
Smith, M. L., & Glass, G. V. (1977). Meta-analysis of psychotherapy outcome studies. American Psychologist, 32, 752–760.10.1037/0003-066X.32.9.752Search in Google Scholar
Sotomayor, M. J. M., Arufe-Giráldez, V., Ruíz-Rico, G., & Navarro-Patón, R. (2021). Music therapy and Parkinson’s disease: A systematic review from 2015–2020. International Journal of Environmental Research and Public Health, 18, 11618.10.3390/ijerph182111618Search in Google Scholar
Sparks, R., Helm, N., & Albert, M. (1974). Aphasia rehabilitation resulting from Melodic Intonation Therapy. Cortex, 10(4), 303–316. doi: 10.1016/S0010-9452(74)80024-9.Search in Google Scholar
Tan, S-L., Spackman, M. P., & Wakefield, E. M. (2017). The effects of diegetic and nondiegetic music on viewers’ interpretations of a film scene. Music Perception, 34(5), 605–623. doi: 10.1525/mp.2017.34.5.605.Search in Google Scholar
Utigaard, N. (2022). The new virtual world of expressive arts therapy: What does it look like? How can it help? IEATA 14th Annual International Conference. Online.Search in Google Scholar
van Westrhenen, N., & Fritz, E. (2014). Creative Arts Therapy as treatment for child trauma: An overview. The Arts in Psychotherapy, 41, 527–534.10.1016/j.aip.2014.10.004Search in Google Scholar
Veazey, C., Ozlem Erden Aki, S., Cook, K. F., Lai, E. C., & Kunik, M. E. (2005). Prevalence and treatment of depression in Parkinson’s disease. Journal of Neuropsychiatry and Clinical Neurosciences, 17(3), 310–323. doi: 10.1176/jnp.17.3.310.Search in Google Scholar
Wile, I. S. (1926). The worship of Asklepios: With special reference to the tholos and the theatre. Annals of Medical History, 8(4), 419–434.Search in Google Scholar
Winkleman, M. (2010). Shamanism and the origins of spirituality and ritual healing. Journal for the Study of Religion, Nature and Culture, 3(4), 458–489. doi: 10.1558/jsrnc.v3i4.458.Search in Google Scholar
Winner, E., Goldstein, T. R., & Vincent-Lacrin, S. (2013). Art for art’s sake: The impact of arts education. OECD Publishing.10.1787/9789264180789-enSearch in Google Scholar
Young, J. O. (2015). The ancient and modern system of the arts. British Journal of Aesthetics, 55, 1–17. doi: 10.1093/aesthj/ayu097.Search in Google Scholar
Yuan, F., Guo, X., Wei, X., Xie, F., Zheng, J., Huang, Y., Huang, Z., Chang, Z., Li, H., Guo, Y., & Wang, Q. (2020). Lee Silverman Voice Treatment for dysarthria in patients with Parkinson’s disease: A systematic review and meta‐analysis. European Journal of Neurology, 27(10), 1957–1970. doi: 10.1111/ene.14399.Search in Google Scholar
Zelinski, E. M. (2009). Far transfer in cognitive training of older adults. Restorative Neurology and Neuroscience, 27(5), 455–471. doi: 10.3233/RNN-2009-0495.Search in Google Scholar
Zhao, K., Bai, Z. G., Bo, A., & Chi, I. (2016). A systematic review and meta-analysis of music therapy for the older adults with depression. International Journal of Geriatric Psychiatry, 31(11), 1188–1198. doi: 10.1002/gps.4494.Search in Google Scholar
Zumbansen, A., & Tremblay, P. (2019). Music-based interventions for aphasia could act through a motor-speech mechanism: A systematic review and case–control analysis of published individual participant data. Aphasiology, 33(4), 466–497. doi: 10.1080/02687038.2018.1506089.Search in Google Scholar
© 2023 the author(s), published by De Gruyter
This work is licensed under the Creative Commons Attribution 4.0 International License.
Articles in the same Issue
- Research Articles
- Contextual Specificity of (Un)Healthy Food/Drink Intake in Everyday Life: A Study Based on Episodic Memories
- Influences of Music Reading on Auditory Chord Discrimination: A Novel Test Bed for Nonconscious Processing of Irrelevant Prime Meaning
- Toward a New Science of the Clinical Uses of the Arts
- No Effect of Forest Representations on State Anxiety, Actual and Perceived Noise
- “The Authors” Make Me Think Equally of Women and Men: Exploring Mixed-Gender Representations in a Visual Categorisation Task
- Revisiting the Watching Eyes Effect: How Emotional Expressions, Sex, and Age of Watching Eyes Influence Stereotypical Statement Endorsement
Articles in the same Issue
- Research Articles
- Contextual Specificity of (Un)Healthy Food/Drink Intake in Everyday Life: A Study Based on Episodic Memories
- Influences of Music Reading on Auditory Chord Discrimination: A Novel Test Bed for Nonconscious Processing of Irrelevant Prime Meaning
- Toward a New Science of the Clinical Uses of the Arts
- No Effect of Forest Representations on State Anxiety, Actual and Perceived Noise
- “The Authors” Make Me Think Equally of Women and Men: Exploring Mixed-Gender Representations in a Visual Categorisation Task
- Revisiting the Watching Eyes Effect: How Emotional Expressions, Sex, and Age of Watching Eyes Influence Stereotypical Statement Endorsement