Clinical application of circulating tumor cells
-
Nikolas H. Stoecklein
Univ.-Prof. Dr. med. Nikolas H. Stoecklein

 ,
Julia Oles
,
Julia Oles
Julia Oles
Dr. rer. nat. Andre Franken
,
Hans Neubauer
Prof. Dr. rer. nat. Hans Neubauer
,
Leon W.M.M. Terstappen
Prof. Leon W.M.M. Terstappen (MD, PhD)
Dr. rer. nat. Rui P.L. Neves

Abstract
This narrative review aims to provide a comprehensive overview of the current state of circulating tumor cell (CTC) analysis and its clinical significance in patients with epithelial cancers. The review explores the advancements in CTC detection methods, their clinical applications, and the challenges that lie ahead. By examining the important research findings in this field, this review offers the reader a solid foundation to understand the evolving landscape of CTC analysis and its potential implications for clinical practice. The comprehensive analysis of CTCs provides valuable insights into tumor biology, treatment response, minimal residual disease detection, and prognostic evaluation. Furthermore, the review highlights the potential of CTCs as a non-invasive biomarker for personalized medicine and the monitoring of treatment efficacy. Despite the progress made in CTC research, several challenges such as standardization, validation, and integration into routine clinical practice remain. The review concludes by discussing future directions and the potential impact of CTC analysis on improving patient outcomes and guiding therapeutic decision-making in epithelial cancers.
Introduction
Circulating tumor cells (CTCs) have long been recognized as cancer cells originating from solid malignant tumors that have gained access to the bloodstream and can be detected in peripheral blood samples. The first documented description of CTCs is credited to Australian physician Thomas Ashworth, dating back to 1869 [1]. Ashworth made this remarkable observation when he analyzed a venous blood sample taken from a deceased patient with multiple subcutaneous tumors. He noted the presence of cells in the blood that displayed morphological similarities to the cancer cells found within the tumors. Ashworth hypothesized that these cells in the bloodstream might be associated with the spread and multiplication of tumors. He wrote that ‘The fact of cells identical with those of the cancer itself being seen in the blood may tend to throw some light upon the mode of origin of multiple tumors existing in the same person.’ and formulated a concept which was way ahead of its time. However, his findings, unfortunately, faded into obscurity over the years. The systematic investigation of CTCs began between the 1930s to 1960s, coinciding with the establishment of the concept of hematogenous metastasis [2]. During this period, researchers primarily focused on exploring whether CTCs could serve as an indicator of metastatic risk in patients with localized cancers who were undergoing surgical interventions. However, effective methods for enriching CTCs were limited, and their detection relied mostly on conventional cytopathological techniques. Consequently, detecting CTCs posed significant challenges and yielded results that, by today’s standards, were somewhat unreliable. Since then, the field of liquid biopsy analysis has experienced a transformative shift, primarily driven by remarkable advancements in molecular biology and genetics. These advancements have paved the way for exciting possibilities and expanded applications of CTC analysis. From a contemporary perspective, CTCs have garnered significant interest due to their unique ability to provide direct access to systemic cancer at all stages of its development, effectively offering a “real-time liquid biopsy.” This innovative approach can not only enhance our understanding of the biological mechanisms underlying dissemination and metastasis but also holds promise in developing improved biomarkers for the more accurate detection, analysis, and treatment of systemic cancer.
Despite these potential benefits, the detection of CTCs remains a challenging task. Their concentration in the bloodstream is extremely low, and they lack specific markers that are unique to cancer cells, limiting their utility as a diagnostic tool. In response to these challenges, numerous platforms and techniques have been developed to enrich, detect, and isolate CTCs from blood samples, aiming to improve their detection sensitivity and reliability.
The aim of this narrative review is to offer the reader a solid base to understand the current state of CTC analysis and its clinical significance in patients with epithelial cancers. By examining the advancements in CTC detection methods, exploring their clinical applications, and addressing the challenges ahead, we hope to provide a timely overview of the current understanding of CTCs and their potential implications for clinical practice.
Principles and methods for CTC detection and enrichment
Traditionally, two main approaches have been employed to detect epithelial CTCs in blood samples: antibody-based immune-staining and PCR-based molecular detection methods (Figure 1). In immuno-staining, antibodies are utilized to identify epithelial antigens on CTCs. In PCR-based methods, the focus is on detecting cancer-specific DNA mutations, DNA hypermethylation, or cancer-associated mRNA transcripts, which are more commonly used [3–10]. Additionally, fluorescence in situ hybridization (FISH) has emerged as a technique for detecting cancer-specific aneusomy in CTCs [11], and mRNA hybridization with padlock probes has been employed to detect cancer-specific mRNA transcripts [12].
The origins of CTC detection through immuno-staining can be traced back to protocols developed in the late 1980s for detecting disseminated cancer cells in the bone marrow and lymph nodes, which were subsequently adapted for blood samples. Early techniques, such as cytology and flow-cytometry, were able to detect one tumor cell in 100 normal blood cells, while more sensitive immune-cytochemistry methods achieved a detection limit of one tumor cell in 10^5 blood cells [13]. Another variant of CTC immuno-detection evolved the Epispot assay, which represents an in vitro functional assay relying on immunofluorescence detection of secreted proteins markers derived from viable cancer cells in short-term culture [14]. Currently, multi-marker immunofluorescence staining is the most common approach to identifying epithelial tumor cells. This involves the application of antibodies against cytokeratins, which are characteristic intermediate filaments of epithelial cells, or against other epithelial or malignancy-associated markers like EpCAM, ERBB2, MUC-1, EGFR (including phosphorylated states), PSMA, or VAR2 [15–21]. The use of antibodies against CD45 as an exclusion marker to label leukocytes has become standard in most current assays. Additionally, nucleated acid dye such as DAPI is used to identify intact nucleated cells. Such immunostainings are implemented in most semi-automated platforms for CTC detection, including CellSearch [22], Epic Sciences [23], and RareCyte [24]. It should be noted that although the EpCAM+/CK+/CD45-/DAPI+ phenotype for CTC identification used in the CellSearch platform is generally accepted preferably there would be an universally defined CTC phenotype. This however is quite complex as different technologies employ divergent antibody clones with different fluorophores which are detected by different microscope platforms, complicating the comparison and standardization of results across various platforms.
In comparison to immuno-detection, PCR-based molecular CTC detection achieved already in the 1990s a remarkable sensitivity. PCR assays could detect even a single malignant cell among up to 10^7 normal cells [13]. In the context of epithelial cancers, CK mRNA has frequently been utilized for CTC detection [9]. The AdnaTest® is perhaps the most widely used commercial kit for CTC detection through mRNA profiling. It employs a multiplex reverse-transcription (RT-)PCR approach targeting a panel of transcripts as surrogate for the presence of CTCs in a cell suspension obtained from blood after immuno-magnetic enrichment of epithelial cancer cells [25]. A more recent development in detecting CTC-derived nucleic acids is the application of digital PCR, which is commonly 1–2 logs more sensitive than standard PCRs [26, 27]. However, while PCR-based CTC detection may provide clinically valuable information, it does not facilitate the isolation of pure CTCs for subsequent downstream molecular analysis as demonstrated for immuno-detection protocols [28, 29]. Another potential limitation of PCR-based detection assays involves the analysis of mesenchymal antigen expression, as it remains ambiguous whether the detected signal emanates from the tumor cells themselves or originates from the variable background presence of white blood cells.
Given the typically low concentration of CTCs in blood, ranging commonly between 1 and 50 CTCs in a positive sample [2], effective enrichment techniques are essential for their detection and analysis (Figure 1). A standard 10 mL peripheral blood sample contains billions of red blood cells, thrombocytes, and approximately 4.5–6x10^7 leukocytes, making some form of enrichment necessary even for sensitive molecular assays. One of the earliest approaches for enriching epithelial cells from blood samples was density gradient centrifugation, which enriched epithelial cells together with the mononuclear cell fraction due to a similar density of around 1.077 mg/L [30]. Another early biophysical enrichment approach used until today employs filtration techniques exploiting size and deformability differences between blood cells and CTCs [31]. However, it is important to recognize that the lack of specificity in biophysical separation methods can be a drawback to the efficacy of enrichment, as the biophysical characteristics of CTCs and leukocytes often overlap to some extent. For instance, filtration devices with eight μm pore sizes, such as ISET (Isolation by Size of Epithelial Tumor Cells), would inadvertently capture leukocytes while losing smaller CTCs [2].
More specific enrichment methods emerged utilizing immuno-magnetic techniques, either through positive selection targeting epithelial cell-surface antigens or negative selection targeting leukocyte-specific antigens (e. g., CD45). Despite its high specificity, the absence of common cancer-specific antigens and the potential dynamic expression of surface proteins in cancer cells poses a challenge for this approach. This can be exemplified by the EpCAM, the most widely used surface protein for positive selection, which is also utilized in the current “gold standard” for CTC detection, the FDA-cleared CellSearch system. EpCAM is commonly expressed in most carcinomas, providing specificity for epithelial cells, although it is also found in embryonic stem cells and limited subsets of adult stem and progenitor cells [32]. However, EpCAM is not universally expressed in all cancer types. Its expression can be heterogenous, absent, or downregulated in certain cancers, such as squamous cell carcinomas, and especially if cancer cells undergo epithelial to mesenchymal transition (EMT) [33–32]. Consequently, EpCAM-based CTC detection will miss CTCs. However, several studies provided evidence for the important role of EpCAM in metastasis across different cancer types, suggesting that EpCAM identifies relevant CTC populations.
A significant advancement in the field of CTC enrichment was the introduction of microfluidic chips offering versatility and also automation potential. The pioneering publication by Nagrath et al. was a breakthrough for microfluidic CTC enrichment [34]. This microfluidic chip utilized immunoaffinity capture via antibody-coated posts. Since then, various microfluidic platforms have been developed, capitalizing on the physical and biological properties of CTCs in comparison to normal blood cells [35, 36]. These biofluidic technologies, which include immunoaffinity capture, size-based filtration, deformability-based sorting, vortex-sorting, or a combination of these approaches, aim to exploit distinct properties to effectively enrich CTCs while minimizing interference from other blood components. The utilization of microfluidic chips has allowed for precise manipulation and control of fluid flow within small-scale channels, facilitating a more precise capture of CTCs [37]. Immunoaffinity capture involves chip surfaces functionalized with specific antibodies to selectively bind and capture CTCs based on their surface markers (e. g., EpCAM). Size-based filtration relies on the size difference between CTCs and other blood cells to separate and retain CTCs within specific regions of the chip. Deformability-based sorting takes advantage of the varying deformability of CTCs compared to normal blood cells, allowing for their separation based on differences in mechanical properties. Vortex-sorting utilizes hydrodynamic forces and fluid dynamics within microfluidic channels to concentrate and isolate CTCs in specific regions of the chip’s microfluidic sorting channel [35–37]. By harnessing these biofluidic technologies, the efficiency and sensitivity of CTC enrichment can be enhanced, enabling downstream analysis and characterization of these cells. As for conventional biophysical separation, potential drawbacks arise from overlapping characteristics of CTCs and normal blood cells [2]. However, by continuously refining and combing these enrichment methods, future technologic developments aim to overcome the challenges posed by the low abundance and heterogeneity of CTCs in blood samples. For the time being, it is important to acknowledge that currently, no enrichment method achieves 100 % efficiency, and therefore, there is always a degree of cell loss that cannot be precisely quantified for each individual sample.
Clinical validation of CTCs
Although over 40 CTC assays based on the principles mentioned above have been published [38] [39], only a handful have been consistently reported as endpoints or pharmacodynamic markers in clinical trials. Among them, the CellSearch system, remains the sole system FDA-cleared for the detection and monitoring of CTCs in patients with metastatic breast, prostate, and colorectal cancers. Due to its significant impact, this section primarily focuses on the data generated using the CellSearch system, which has played a crucial role in establishing reliable clinical evidence that conclusively demonstrates the prognostic impact of CTCs. CellSearch is a system that utilizes ferrofluids and EpCAM-targeting monoclonal antibodies to capture epithelial cells from 7.5 mL of blood [22]. The captured cells are then stained with Phycoerythrin (PE)-conjugated antibodies for cytokeratins (CKs) as well as an Allophycocyanin (APC)-conjugated antibody for CD45. Additionally, the enriched cells are stained with DAPI to ensure the detection of intact nucleated cells. Images of the processed samples are acquired by a computer-controlled fluorescence microscope. Notably, the CellSearch-Magnest device holds magnetically labeled cells (EpCAM+) in place, preventing cell loss during processing. A trained operator screens an image gallery of DAPI+ and CK+ objects generated by a computer algorithm to identify CTCs, which are defined as EpCAM+/CK+/CD45- objects with a cellular shape, size of at least 4x4 µm and a DAPI+ nucleus positioned at least 50 % within the cytoplasm [40]. Several prospective multicenter studies established CTCs according to this definition as prognostically relevant. A count of ≥5 CTCs in metastatic breast and metastatic prostate cancer and ≥3 CTCs in metastatic colorectal cancer (CRC), respectively, has been strongly correlated with poor survival [41–44]. Similar prognostic significance has been observed in non-small cell lung cancer [45], small cell lung cancer [46], gastric cancer [47], pancreatic and peri-ampullary cancer [48], and head and neck cancer [49]. Moreover, in advanced prostate cancer, the combination of elevated serum lactate dehydrogenase (LDH), a biomarker indicating aggressive malignancy, at week 12 of treatment, along with CellSearch CTC counts, fulfills all four Prentice criteria, establishing CTC counts as an individual patient-level surrogate for survival [50]. In patients with ≥5 CTCs in 7.5 mL of blood prior to therapy, a ≥30 % decrease in CTC counts as early as week four has been associated with longer survival [51]. A recent re-analysis, utilizing individual patient data from five prospective randomized phase III trials involving >6,000 patients, identified negative CTC CellSearch test (CTC0) as a readily identifiable and clinically significant endpoint. Since this endpoint can be determined shortly after initiating treatment indicating therapy benefit, the use of CTC0 as a response endpoint has been recommended for early-phase clinical trials [52]. However, the predictive value of CTC enumeration before treatment initiation, i. e., providing information on the probability of response to a specific therapy, has yet to be established in prostate cancer. This limitation currently hinders the routine clinical use of CTC enumeration, despite its well-documented strong prognostic value.
The clinical value of CTC detection in non-metastatic cancer
Most data are available for studies with the CellSearch system, and localized breast cancer is the so far best-investigated cancer for the presence of CTCs. It has been shown to be an independent prognostic factor for disease-free survival and overall survival. CTC counts have also been associated with relapse-free survival and response to radiotherapy. In the neoadjuvant setting, pre-chemotherapy CTC counts have been linked to worse overall survival and distant disease-free survival, with higher CTC counts correlating with increased mortality. Strikingly, CTCs can also be detected in peripheral blood samples in the minimal residual disease (MRD) situation after complete removal of the primary tumor [53–54], after all cycles of neo-/adjuvant therapy were completed [55–56] and even two years after completion of the adjuvant therapy [57]. Apparently, micro-metastatic cancer cells re-enter the bloodstream and become then detectable as rare CTCs. The observation that these MRD-CTCs can predict recurrences suggests that they reflect active MRD. Interestingly, CellSearch detected CTCs in early breast cancer were used for therapeutic decision making in the EORTC 90091–10093 BIG 1–12 Treat CTC trial [58]. This randomized trial aimed to determine whether trastuzumab reduces the detection of ≥1 CTC in high-risk, HER2 nonamplified, early breast cancer. However, the study results showed that trastuzumab did not decrease the detection rate of CTCs in this BC subtype. The trial was terminated early due to futility, as there was no significant difference in CTC detection between the trastuzumab and observation arms. Limitations of this study were the low frequency of CTCs and the fact that HER2 was not assessed on the “treated” CTCs.
As in the metastatic situation, pre-operative CTC detection has been identified as an independent prognostic marker for poor outcomes in localized colorectal cancer [59]. Limited data are available for other cancer types, such as pancreatic cancer including adenocarcinoma of pancreas (PDAC), where pre-operative detection has shown to be an independent prognostic factor for overall survival [48]. The presence of CTCs has been associated with a higher risk of relapse in non-metastatic non-small cell lung cancer patients and several other cancer types. However, studies on localized prostate cancer have yielded conflicting results [60].
The low detection rates of the CellSearch system in localized cancers suggest that this system has no role in screening and early cancer detection. Other systems, such as the filtration system known as ISET, have reported higher detection frequencies, particularly in lung cancer [61]. In a prospective multicenter cohort study, the potential of ISET CTCs as a biomarker for lung cancer screening was evaluated [61]. The study enrolled 614 participants eligible for lung cancer screening and with chronic obstructive pulmonary disease. Participants underwent three screening rounds over one-year intervals, including low-dose chest CT and blood tests for CTC detection. However, the results showed that CTC detection using ISET was not suitable for lung cancer screening, with a sensitivity of only 26 % and an inability to predict lung cancer or extrapulmonary cancer development. These findings indicated that CTC detection using ISET may not be a viable option for lung cancer screening. A plausible explanation for this inconclusive study result may reside in the dedifferentiated character of NSCLC (Non-Small Cell Lung Cancer) CTCs, coupled with the issue of overlapping cell sizes between CTCs and normal white blood cells [62].
The clinical utility of CTC enumeration in metastatic cancer
While the clinical validity of CellSearch-CTCs has been remarkably established and response to therapy can be clearly monitored via CTCs, this biomarker could not be translated into clinical routine yet. Obviously, the design of studies demonstrating clinical utility, thus a survival benefit from the CTC analysis, can be complex, especially in the context of constantly evolving and changing standards of care. This might be one reason why relatively few prospective randomized clinical trials have been conducted so far. The first published clinical trial investigating the predictive potential of CellSearch-CTCs was the SWOG-S0500 trial carried out in MBC [63]. The study included 595 patients with metastatic breast cancer and tested whether a CTC-driven change of therapy can improve overall or progression-free survival. The trial was negative and found no survival benefit but confirmed the strong prognostic significance of CTC enumeration by CellSearch. Challenges discussed included the timing of CTC enumeration and the need for additional markers to predict response to alternative therapies [2]. The CirCe01 trial was also carried out in MBC and aimed to evaluate the clinical utility of CTC-based treatment decisions beyond the third line of therapy [64]. The trial enrolled MBC patients after two lines of chemotherapy, and those with ≥5 CTCs per 7.5 mL were randomized between the CTC-driven and standard arms. In the CTC arm, changes in CTC count were assessed during each line of chemotherapy, and patients with CTC levels indicating early tumor progression had to switch to the next line of chemotherapy. However, due to limited accrual and compliance, the trial could not demonstrate the clinical utility of CTC monitoring. Overall survival (OS) was not different between the CTC-driven and standard arms, but subgroup analysis showed that patients who switched chemotherapy based on CTC response experienced longer survival compared to those who did not.
The recently published STIC CTC trial, a randomized clinical trial involving 755 women with hormone receptor-positive, Her2-negative MBC, could demonstrate the clinical utility of CTC enumeration [65]. Here, the efficacy of the CTC-driven treatment choice was compared to a clinician-driven choice for first-line treatment. The trial demonstrated that CTC counts can guide the selection between chemotherapy and endocrine therapy. The CTC arm, where treatment was based on CTC count (≥5 CTCs/7.5 mL for chemotherapy; <5 CTCs/7.5 mL for endocrine therapy), showed a median progression-free survival of 15.5 months compared to 13.9 months in the standard arm. However, despite its promising results, as the authors noticed, a significant limitation of the STIC trial was that it was designed before CDK4/6 inhibitors became the standard of care [65]. As a result, the study did not specifically address the conundrum between endocrine therapy and chemotherapy in patients who progress on a CDK4/6 inhibitor used as first-line or adjuvant therapy. This decision-making challenge remains unresolved in clinical practice, emphasizing the need for further research and integration of biomarkers like CTC count to guide treatment choices in this context [60].
In metastatic colorectal cancer, a randomized phase III multicenter study (VISNÚ-1) aimed to investigate the role of CTC counts to select patients for a more intense therapy with FOLFOXIRI-bevacizumab in metastatic colorectal cancer versus FOLFOX-bevacizumab [66]. The study included 349 previously untreated patients with unresectable metastatic colorectal carcinoma and ≥ 3 CTCs per 7.5 mL blood. The results showed that FOLFOXIRI-bevacizumab significantly improved progression-free survival (PFS) compared to FOLFOX-bevacizumab in this patient population, with a median PFS of 12.4 months versus 9.3 months, respectively. Grade ≥3 adverse events were more common with FOLFOXIRI-bevacizumab. The findings suggest that CTC count may be a valuable non-invasive biomarker for selecting patients who could benefit from intensive first-line therapy. As the authors discussed, subsequent studies would be of interest to investigate the escalation or de-escalation of therapy according to CTC counts after therapy initiation. One critique of this study centered around its focus on the primary endpoint of PFS while comparing a triplet chemotherapy backbone to a doublet backbone [67]. It was acknowledged that a more significant endpoint would have been OS or the duration of time until the occurrence of a second progression following the administration of a second doublet treatment for those individuals who initially received a doublet treatment in the first line.
The clinical utility of CTC profiling in metastatic cancer
The level of information provided by CTC numbers is apparently limited, especially in the context of targeted therapies or immunotherapies. To augment the depth of information garnered, the CellSearch system introduces a fourth fluorescence channel, permitting additional antibody staining – such as evaluating the expression of a therapeutic target on CTCs. This methodology was employed in the phase 3 DETECT III study, which proactively addressed intra-patient heterogeneity and sought to pinpoint initially HER2-negative MBC (metastatic breast cancer) patients who exhibited HER2-expressing CTCs, positing them as potential beneficiaries of anti-HER2 treatment [68]. A foundational study by Georgoulias et al. underscored the significance of HER2 expression on CTCs in HER2-negative MBC [69]. Through employing CellSearch in the DETECT III study, 105 patients manifesting positive HER2 CTCs were identified and subsequently randomized to assess the efficacy of the HER2-targeted therapy lapatinib in comparison to standard therapy. Notably, while CTC clearance at the first follow-up visit was not significantly disparate between the treatment arms at any point, it was significantly correlated with enhanced OS, presenting 42.4 versus 14.1 months (p=0.002). Besides, this study demonstrated that lapatinib had a positive impact on OS in this patient population. Patients in the lapatinib arm showed a significantly improved OS compared to those in the standard therapy arm (20.5 versus 9.1 months, p=0.009), as evidenced by hazard ratios of 0.54 (95 % CI 0.34–0.86; p = 0.008) and 0.53 (95 % CI, 0.33–0.86; p = 0.010). Although the primary endpoint of CTC clearance rate did not differ significantly between the two arms, the improved OS observed in the lapatinib arm highlights the potential clinical relevance of HER2-positive CTCs as a biomarker for predicting treatment response and clinical benefit in patients with initially HER2-negative MBC [68]. Despite the intriguing data, this study revealed an important drawback of CellSearch CTC-based diagnostics in HER2-negative breast cancer and pointed to an important aspect in general: to randomize the 105 CTC HER2-positive patients 1933 MBC patients were screened, and only 1217 out of them (63.0 %) had ≥1 CTC per 7.5 ml blood and ≥5 CTCs were detected in 735 patients (38.0 %; median 8 CTCs) [70]. This renders a large patient group as not informative at all or providing only limited, potentially unreliable diagnostic information. The full data of this landmark study are expected to be published later in 2023. The DETECT III has been, so far, the only large study in which molecular phenotyping of CTCs using the CellSearch system guided a therapeutic decision.
An interesting development for CTC-based therapy decisions emerged in metastatic castration-resistant prostate cancer (mCRPC). Here, the androgen receptor splice variant-7 (AR-V7) has garnered significant attention as a biomarker for therapeutic decision-making since elevated AR-V7 expression has been associated with resistance to androgen receptor signaling inhibitors (ARSi). Initially, using the Adna-Test, it was established that AR-V7 in CTCs is associated with resistance to ARSi [71–72]. More recently, the automated image-based Epic Sciences “no cell left behind” CTC detection platform provided a test enabling the immune-detection of nuclear AR-V7 in individual CTCs. After two studies indicated the clinical utility of the Epic Sciences assay in mCRPC patients undergoing treatment change to select patients for therapy with taxanes instead of ARSi [73–74] local health-insurance plans covered AR-V7 protein assay, commercialized as Oncotype DX AR-V7 Nucleus Detect test, for mCRCP patients in the U.S. [75] despite the lack to establish the predictive value for selection of taxanes vs. ARSi. Additional corroborating data came from the PROPHECY study that demonstrated for both mRNA- and protein-based CTC AR-V7 assays, similar value for selecting mCRCP patients to ARSi or taxane treatment in the context of other clinical parameters [76]. The authors stressed that the CTC AR-V7 status could explain some of the resistance to AR therapy, but AR-V7 heterogeneity within patients and over time suggests that additional strategies are needed to overcome resistance in such mCRCP patients.
In the context of clinical relevant CTC profiling, it is of interest that Angle’s Parsortix PC1 system received just recently (May 2022) FDA clearance as an in vitro diagnostic device intended to enrich CTCs from the peripheral blood of MBC patients [77]. The system employs a microfluidic chip for size- and deformability-based CTC capture. Interestingly, FDA clearance did not cover CTC-identification or analysis, but the end user will be responsible for the validation of any further downstream assay. Supporting data for the FDA clearance came from the HOMING Study, a multicenter, prospective, blinded study in healthy volunteers and MBC patients that successfully yielded CTCs for downstream evaluation [78]. CTCs were analyzed by qRT-PCR, RNA sequencing, or cytogenetic analysis of HER2 amplification by FISH. Notably, when the investigators used cytopathology to determine CTCs, they detected 49 % of MBC patients (n=194) CTC-positive, but also 10 % of the healthy volunteers (n=192). This is, however, not a surprising result and relates to the more subjective cytopathology without any immuno-phenotyping. Unfortunately, the study did not compare to a CTC-detection standard, such as the CellSearch system, which is a clear limitation. However, this investigation and this particular FDA clearance pave the way for clinically useful and comprehensive CTC-profiling. In principle, as reviewed elsewhere [79–81], technically exciting possibilities exist to precisely isolate individual CTCs and perform diagnostic tests on the genomic, transcriptomic, epigenomic, and proteomic level (Figure 1).
Overview on studies investigating CSF for tumor cells with CTC-detection methods
|
Author |
Year |
CTC-assay |
molecular CTC analysis |
Cancer type |
patients with LM (n) |
Main findings |
Reference |
|
Patel et al. |
2011 |
CellSearch |
no |
MBC |
5 |
first application of CS on CSF, monitoring of response to therapy |
[104] |
|
Le Rhun et al. |
2012 |
CellSearch |
no |
MBC |
8 |
range 1–10,500/5mL CSF |
[105] |
|
Le Rhun et al. |
2013 |
CellSearch CMC |
no |
Melanoma |
2 |
range 5–1,090 CMC/5mL CSF |
[106] |
|
Magbanua et al. |
2013 |
IE/FACS (developed for CTCs in blood) |
yes, aCGH |
MBC |
15 |
genome profiling in 13/15 patients, typical MBC profiles with subcloncal changes compared to biopsy tissue |
[107] |
|
Nayak et al. |
2013 |
CellSearch |
no |
MBC, lung, others |
16 |
Median CSF CTC/mL: 19.3; sensitivity of 100 % as compared with 66.7 % for conventional cytology and 73.3 % for MRI, one patient false positive |
[108] |
|
Tu et al. |
2015 |
CellSearch |
no |
lung |
18 |
Median CSF CTCs/5 mL: 785; sensitivity of 77.8 %, compared with 44.4 % for conventional cytology |
[109] |
|
Jiang et al. |
2017 |
CellSearch |
yes, NGS pane of 416 genes |
Lung (NSCLC) |
21 |
Sensitivity of 95.2 % versus 57.1 % cytology, and versus cytology + MRI (90.5 %), Genetic profiles of CSF CTCs highly concordant with molecular mutations identified in the primary tumor (17/19, 89.5 %); EGFR T790M detected in 7/9 patients with extracranial lesions, but only in 1/14 CSF CTC samples. |
[110] |
|
Lin et al. |
2017 |
CellSearch |
no |
MBC, Lung, others |
30 |
Sensitivity of 93 %, specificity of 95 %, positive predictive value 90 %, and negative predictive value 97 % |
[111] |
|
Torre et al. |
2020 |
CellSearch |
no |
MBC, Lung, others |
20 |
Sensitivity of 88.9 % and specificity of 100 % for detecting LM – threshold of 1 CTC/mL of CSF |
[112] |
|
Malani et al. |
2020 |
CellSearch |
no |
Her2+ MBC |
15 |
Median CSF CTC/3mL: 22; cytology in 40 % and CSF CTCs identified in 87 %. HER2-expression of CTCs assessed, under therapy; 75 % with of HER2 positivity in CSF |
[113] |
|
Darlix et al. |
2022 |
CellSearch |
yes, HER2 phenotyping |
MBC |
40 |
Median CSF CTC: 5824; sensitivity of100 % and specificity of 77 % for LM diagnosis. HER2+ CSF CTCs detected 41 % of patients with HER2-BC |
[114] |
|
Wooster et al. |
2022 |
CNinside |
yes, HER2 & ER phenotyping |
MBC |
10 |
sensitivity OF 100 % and specificity of 83 % for LM; concordance of ER and HER2 status between CSF-TCs and metastatic biopsy: 60 % and 75 %, respectively |
[115] |
MBC: metastatic breast cancer; CS: CellSearch; CSF: cerebrospinal fluid; aCGH: array comparative genomic hybridization; NGS: next generation sequencing; MRI: magnetic resonance imaging; ER: estrogen receptor
Application of CTC-technologies to cerebrospinal fluid
Finally, an intriguing advancement in the CTC field is the application of highly sensitive CTC-detection platforms to investigate the presence and relevance of tumor cells within cerebrospinal fluid (CSF). Leptomeningeal metastasis (LM) occurs in approximately two to eight percent of patients with solid tumors. The current diagnostic methods for LM rely on clinical symptoms and the presence of contrast enhancement in the leptomeninges on brain and/or spine magnetic resonance imaging (MRI). However, MRI has limited sensitivity (around 76 %) and specificity (around 77 %) for accurately diagnosing LM. In cases where MRI scans are inconclusive, a lumbar puncture (LP) is performed to obtain CSF. The sensitivity of CSF cytology, which is used to detect cancer cells in the CSF, is also relatively low. It ranges from 44 to 67 % upon the first LP and increases to 84 to 91 % upon repeated sampling [82]. The enrichment and identification of epithelial CSF CTCs offer a new avenue to improve LM diagnostics o the central nervous system (CNS) and assessing the effectiveness of therapies targeting CNS metastasis. Moreover, this approach offers significant prospects for unraveling underlying mechanisms of CNS metastasis. Several studies have provided evidence of CTCs’ existence in the CSF of patients with diverse malignancies, including breast, lung, and melanoma (Table 1). When compared, CSF CTC analysis outperforms not only cytology and MRI but also CSF ctDNA analysis in terms of specificity and sensitivity. This has been corroborated in a recent meta-analysis [83]. Besides more precise clinical diagnostics for presence of LM, the analysis of CSF-derived CTCs can provide valuable information on tumor heterogeneity, genomic alterations, and treatment response specific to the CNS compartment. Furthermore, the monitoring of CTCs in CSF may offer insights into the early detection of CNS metastases and the development of targeted therapeutic strategies. Although the field is still evolving, the exploration of CTCs in spinal fluid presents an exciting development for advancing our understanding of CNS involvement in cancer and holds promise for improving patient management in the future.
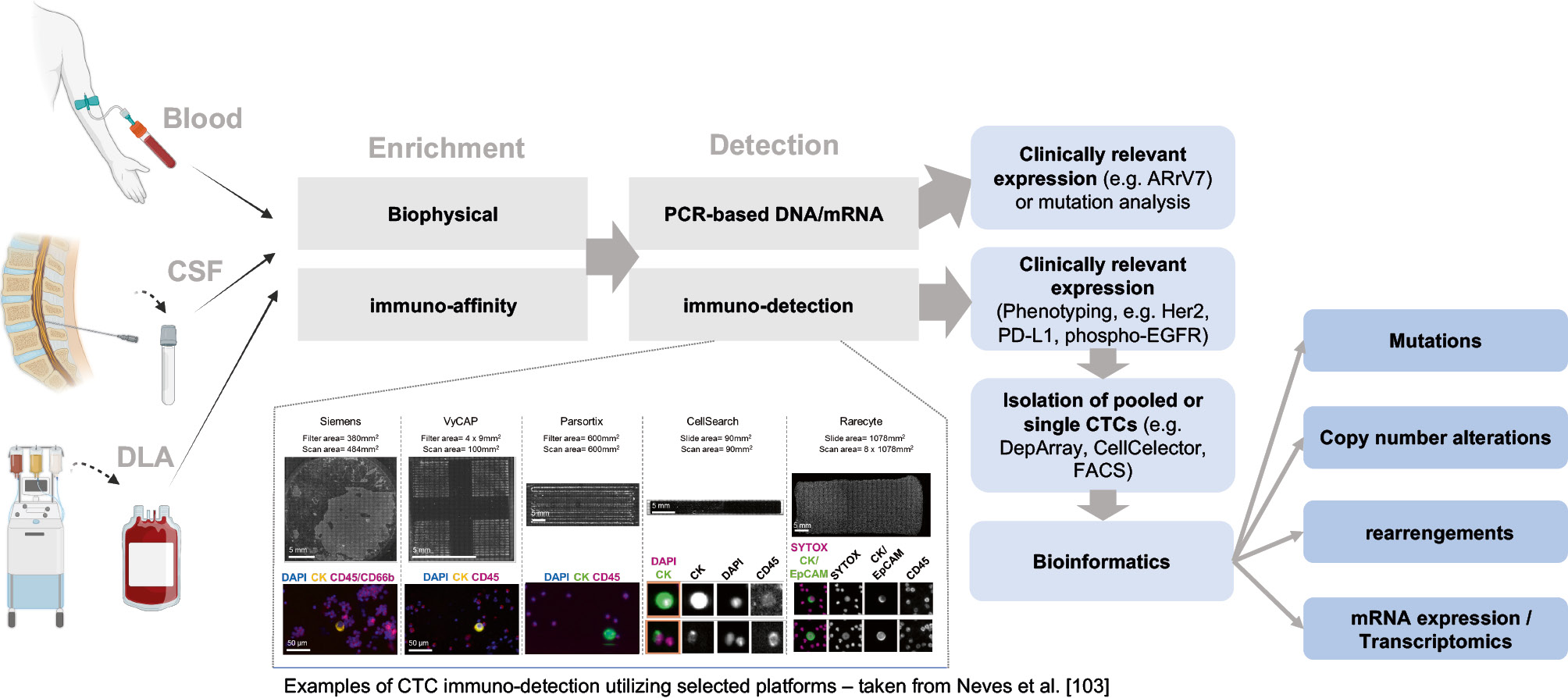
Overview of sample types processed wit CTC technologies and possibilities for subsequent analysis (designed with BioRender).
Outlook and current challenges and
CTCs have undergone extensive examination over the last two decades, consistently nearing, but not fully integrating into, clinical use despite numerous studies. To date, the translational impact of CTCs into meaningful clinical applications has been restricted. It is anticipated that CTC assays may find a place in the routine clinical management of certain cancers that exhibit more robust CTC detection frequencies and counts, such as mCRPC or small-cell lung cancer. Applications that identify the expression of therapeutic targets on CTCs highlight the utility of this liquid biopsy analyte. Specific instances, such as the application of the ARv7 CTC assays for mCRPC in selected U.S. states (as discussed above), serve as demonstrations of gradual integration, with potential for broader adoption in the future. Looking ahead, developments seem to be tentatively exploring the combination of different liquid biomarkers. For instance, the commercially available defineMBC assay, which combines phenotypic and genomic data derived from CTCs with ctDNA analysis, exemplifies this developmental trajectory. It will be crucial to observe how these and similar applications evolve in a clinical setting, ensuring that they undergo rigorous testing and validation in diverse patient cohorts.
However, major challenges must be addressed for the more widespread clinical use of CTC applications. A significant limitation is their extremely low concentration in the entirety of a patient’s blood volume, resulting in low CTC detection frequency and number. Given the Poisson distribution and the estimated quantity of cancer cells ranging from five to 250,000 in the total five-liter blood volume [2], the probability of capturing them in a 10 mL blood sample is low. To overcome this challenge, the concept of high-blood volume analysis has emerged, particularly when molecular profiling of CTCs is desired. High-blood volume analysis can be enabled by diagnostic leukapheresis (DLA) [84], a clinically safe method allowing to screen around 2.5-liter blood for CTCs. Leukapheresis is a clinical routine procedure that collects mononuclear cells (MNCs) from the blood by continuous density-based cell separation. Since epithelial cells have similar densities as the targeted MNCs (1.055–1.08 g/mL), CTCs become co-collected during the process and increase the CTC-detection frequency and yield, which has been convincingly shown by several groups across different cancer types [85–92]. The quality of the harvested cancer cells is high, as demonstrated by the expansion and cultivation of viable DLA-derived CTCs [86, 88–90, 92]. However, a technical challenge remains in the processing of whole DLA products containing around 2 billion leukocytes. Notably, several technical solutions are under development to tackle this problem in DLA [93, 94] but also develop alternative strategies, such as indwelling functionalized catheters to catch CTCs [95] and even wearable devices [96]. Likely, in the not-so-distant future, integrated high-blood volume solutions will become available to not only allow CTC-based profiling in almost every metastatic cancer patient but also to significantly increase CTC-detection sensitivity in organ-confined cancer patients.
The challenges of observer-based CTC detection subjectivity and the complexity of subsequent molecular CTC analysis (from “simple” phenotypic to single cell omics) call for innovative solutions. Machine learning and AI-based imaging analysis offer promising advancements in this context [97–99]. These technologies utilize pattern recognition algorithms and deep learning models to enhance the accuracy and efficiency of CTC detection and analysis. The Epic Sciences platform [100], along with similar new approaches for other platforms such as CellSearch [97, 99], exemplifies the application of machine learning in CTC analysis. By training machine learning algorithms to identify distinctive morphological and molecular features of CTCs, these technologies enable improved detection and classification with high sensitivity. This automated and standardized approach has the potential to revolutionize CTC analysis, particularly in predicting therapeutic outcomes, and facilitate their clinical implementation.
In fact, standardizing CTC technologies and the subsequent molecular analysis poses another significant challenge, and it is imperative to ensure quality control throughout the entire process of CTC analysis, from pre-analytic steps to data analysis. This urgency arises from the growing incorporation of CTC analysis in clinical trials and the potential integration of CTC analysis into routine clinical practice [101]. However, standardization efforts face obstacles due to the diverse detection platforms that employ varying detection methods and even definitions of CTCs. Additionally, there is a lack of standardized systemic external quality assurance programs specifically designed for CTC detection, which poses a significant challenge. Therefore, the European CANCER-ID consortium has undertaken crucial steps to develop guidelines and define minimal performance qualification requirements [102, 103] prior to the clinical validation and integration of CTC assays in clinical trials. These efforts aim to ensure rigorous quality control and enhance the accuracy, reproducibility, and robust implementation of CTC analysis in routine clinical practice. Building upon these initiatives, the European Liquid Biopsy Society (ELBS) is actively engaged in advancing the field further by promoting scientific collaborations, facilitating knowledge exchange, and fostering the development of standardized protocols and methodologies for CTC analysis. Through these collective endeavors, the goal is to elevate the scientific rigor and reliability of CTC-based diagnostics, ultimately translating into improved patient care, treatment selection, and clinical outcomes.
Affiliations
1General, Visceral and Pediatric Surgery University Hospital and Medical Faculty of the Heinrich-Heine University Düsseldorf, Düsseldorf; Liquid Biopsy Center Düsseldorf, University Hospital and Medical Faculty of the Heinrich-Heine University Düsseldorf, Life Science Center, Düsseldorf, Germany
2Department of Obstetrics and Gynecology, University Hospital and Medical Faculty of the Heinrich-Heine University Düsseldorf, Düsseldorf; Liquid Biopsy Center Düsseldorf, University Hospital and Medical Faculty of the Heinrich-Heine University Düsseldorf, Life Science Center, Düsseldorf, Germany
3Center for Integrated Oncology Aachen Bonn Köln Düsseldorf (CIOABCD), University Hospital Düsseldorf, Düsseldorf, Germany
About the authors

Univ.-Prof. Dr. med. Nikolas H. Stoecklein

Julia Oles

Dr. rer. nat. Andre Franken

Prof. Dr. rer. nat. Hans Neubauer
Prof. Leon W.M.M. Terstappen (MD, PhD)

Dr. rer. nat. Rui P.L. Neves
Acknowledgments: (If applicable).
Research funding: None declared.
Author contributions: The author has accepted responsibility for the entire content of this manuscript and approved its submission.
Competing interests: The author receives research funding from Menarini Silicon Biosystems. The authors received compensation for a talk at a conference from Illumina, Inc.
Informed consent: Not applicable.
Ethical approval: Not applicable.
References
[1] Ashworth TR: A Case of Cancer in Which Cells Similar to Those in the Tumors Were Seen in the Blood after Death. Medical Journal of Australia 1869, 14:146–149.Search in Google Scholar
[2] Stoecklein NH, Fischer JC, Niederacher D, Terstappen LW: Challenges for CTC-based liquid biopsies: low CTC frequency and diagnostic leukapheresis as a potential solution. Expert Rev Mol Diagn 2016, 16:147–164.10.1586/14737159.2016.1123095Search in Google Scholar
[3] Sieuwerts AM, Kraan J, Bolt-de Vries J, van der Spoel P, Mostert B, Martens JW, Gratama JW, Sleijfer S, Foekens JA: Molecular characterization of circulating tumor cells in large quantities of contaminating leukocytes by a multiplex real-time PCR. Breast Cancer Res Treat 2009, 118:455–468.10.1007/s10549-008-0290-0Search in Google Scholar
[4] Lianidou ES, Markou A: Circulating tumor cells in breast cancer: detection systems, molecular characterization, and future challenges. Clin Chem 2011, 57:1242–1255.10.1373/clinchem.2011.165068Search in Google Scholar
[5] Helo P, Cronin AM, Danila DC, Wenske S, Gonzalez-Espinoza R, Anand A, Koscuiszka M, Vaananen RM, Pettersson K, Chun FK, et al: Circulating prostate tumor cells detected by reverse transcription-PCR in men with localized or castration-refractory prostate cancer: concordance with CellSearch assay and association with bone metastases and with survival. Clin Chem 2009, 55:765–773.10.1373/clinchem.2008.117952Search in Google Scholar
[6] Smirnov DA, Zweitzig DR, Foulk BW, Miller MC, Doyle GV, Pienta KJ, Meropol NJ, Weiner LM, Cohen SJ, Moreno JG, et al: Global gene expression profiling of circulating tumor cells. Cancer Res 2005, 65:4993–4997.10.1158/0008-5472.CAN-04-4330Search in Google Scholar
[7] Muller V, Riethdorf S, Rack B, Janni W, Fasching PA, Solomayer E, Aktas B, Kasimir-Bauer S, Pantel K, Fehm T, group Ds: Prognostic impact of circulating tumor cells assessed with the CellSearch System and AdnaTest Breast in metastatic breast cancer patients: the DETECT study. Breast Cancer Res 2012, 14:R118.10.1186/bcr3243Search in Google Scholar
[8] Hardingham JE, Hewett PJ, Sage RE, Finch JL, Nuttall JD, Kotasek D, Dobrovic A: Molecular detection of blood-borne epithelial cells in colorectal cancer patients and in patients with benign bowel disease. Int J Cancer 2000, 89:8–13.10.1002/(SICI)1097-0215(20000120)89:1<8::AID-IJC2>3.0.CO;2-KSearch in Google Scholar
[9] Hardingham JE, Kotasek D, Sage RE, Eaton MC, Pascoe VH, Dobrovic A: Detection of circulating tumor cells in colorectal cancer by immunobead-PCR is a sensitive prognostic marker for relapse of disease. Mol Med 1995, 1:789–794.10.1007/BF03401893Search in Google Scholar
[10] Zieglschmid V, Hollmann C, Mannel J, Albert W, Jaeschke-Melli S, Eckstein B, Hillemann T, Greten TF, Gross E, Bocher O: Tumor-associated gene expression in disseminated tumor cells correlates with disease progression and tumor stage in colorectal cancer. Anticancer Res 2007, 27:1823–1832.Search in Google Scholar
[11] Li Y, Zhang X, Liu D, Gong J, Wang DD, Li S, Peng Z, Li Y, Wang X, Lin PP, et al: Evolutionary Expression of HER2 Conferred by Chromosome Aneuploidy on Circulating Gastric Cancer Cells Contributes to Developing Targeted and Chemotherapeutic Resistance. Clin Cancer Res 2018, 24:5261–5271.10.1158/1078-0432.CCR-18-1205Search in Google Scholar
[12] El-Heliebi A, Hille C, Laxman N, Svedlund J, Haudum C, Ercan E, Kroneis T, Chen S, Smolle M, Rossmann C, et al: In Situ Detection and Quantification of AR-V7, AR-FL, PSA, and KRAS Point Mutations in Circulating Tumor Cells. Clin Chem 2018, 64:536–546.10.1373/clinchem.2017.281295Search in Google Scholar
[13] Johnson PW, Burchill SA, Selby PJ: The molecular detection of circulating tumour cells. Br J Cancer 1995, 72:268–276.10.1038/bjc.1995.324Search in Google Scholar PubMed PubMed Central
[14] Alix-Panabieres C: EPISPOT assay: detection of viable DTCs/CTCs in solid tumor patients. Recent Results Cancer Res 2012, 195:69–76.10.1007/978-3-642-28160-0_6Search in Google Scholar PubMed
[15] Thege FI, Gruber CN, Cardle, II, Cong SH, Lannin TB, Kirby BJ: anti-EGFR capture mitigates EMT- and chemoresistance-associated heterogeneity in a resistance-profiling CTC platform. Anal Biochem 2019, 577:26–33.10.1016/j.ab.2019.02.003Search in Google Scholar PubMed
[16] Franken A, Kraemer A, Sicking A, Watolla M, Rivandi M, Yang L, Warfsmann J, Polzer BM, Friedl TWP, Meier-Stiegen F, et al: Comparative analysis of EpCAM high-expressing and low-expressing circulating tumour cells with regard to their clonal relationship and clinical value. Br J Cancer 2023, 128:1742–1752.10.1038/s41416-023-02179-0Search in Google Scholar PubMed PubMed Central
[17] Gorges TM, Riethdorf S, von Ahsen O, Nastal YP, Rock K, Boede M, Peine S, Kuske A, Schmid E, Kneip C, et al: Heterogeneous PSMA expression on circulating tumor cells: a potential basis for stratification and monitoring of PSMA-directed therapies in prostate cancer. Oncotarget 2016, 7:34930–34941.10.18632/oncotarget.9004Search in Google Scholar PubMed PubMed Central
[18] Beije N, Onstenk W, Kraan J, Sieuwerts AM, Hamberg P, Dirix LY, Brouwer A, de Jongh FE, Jager A, Seynaeve CM, et al: Prognostic Impact of HER2 and ER Status of Circulating Tumor Cells in Metastatic Breast Cancer Patients with a HER2-Negative Primary Tumor. Neoplasia 2016, 18:647–653.10.1016/j.neo.2016.08.007Search in Google Scholar PubMed PubMed Central
[19] Agerbaek MO, Bang-Christensen SR, Yang MH, Clausen TM, Pereira MA, Sharma S, Ditlev SB, Nielsen MA, Choudhary S, Gustavsson T, et al: Author Correction: The VAR2CSA malaria protein efficiently retrieves circulating tumor cells in an EpCAM-independent manner. Nat Commun 2022, 13:3285.10.1038/s41467-022-29351-zSearch in Google Scholar PubMed PubMed Central
[20] Gupta S, Halabi S, Yang Q, Roy A, Tubbs A, Gore Y, George DJ, Nanus DM, Antonarakis ES, Danila DC, et al: PSMA-positive Circulating Tumor Cell Detection and Outcomes with Abiraterone or Enzalutamide Treatment in Men with Metastatic Castrate-resistant Prostate Cancer. Clin Cancer Res 2023, 29:1929–1937.10.1158/1078-0432.CCR-22-3233Search in Google Scholar PubMed PubMed Central
[21] Katsarou SD, Messaritakis I, Voumvouraki A, Kakavogiannis S, Kappaotsakis A, Alkahtani S, Stournaras C, Martin SS, Georgoulias V, Kallergi G: Detyrosinated alpha-Tubulin, Vimentin and PD-L1 in Circulating Tumor Cells (CTCs) Isolated from Non-Small Cell Lung Cancer (NSCLC) Patients. J Pers Med 2022, 12.10.3390/jpm12020154Search in Google Scholar PubMed PubMed Central
[22] Andree KC, van Dalum G, Terstappen LW: Challenges in circulating tumor cell detection by the CellSearch system. Mol Oncol 2016, 10:395–407.10.1016/j.molonc.2015.12.002Search in Google Scholar PubMed PubMed Central
[23] Dago AE, Stepansky A, Carlsson A, Luttgen M, Kendall J, Baslan T, Kolatkar A, Wigler M, Bethel K, Gross ME, et al: Rapid phenotypic and genomic change in response to therapeutic pressure in prostate cancer inferred by high content analysis of single circulating tumor cells. PLoS One 2014, 9:e101777.10.1371/journal.pone.0101777Search in Google Scholar PubMed PubMed Central
[24] Campton DE, Ramirez AB, Nordberg JJ, Drovetto N, Clein AC, Varshavskaya P, Friemel BH, Quarre S, Breman A, Dorschner M, et al: High-recovery visual identification and single-cell retrieval of circulating tumor cells for genomic analysis using a dual-technology platform integrated with automated immunofluorescence staining. BMC Cancer 2015, 15:360.10.1186/s12885-015-1383-xSearch in Google Scholar PubMed PubMed Central
[25] Hauch S, Zimmermann S, Lankiewicz S, Zieglschmid V, Bocher O, Albert WH: The clinical significance of circulating tumour cells in breast cancer and colorectal cancer patients. Anticancer Res 2007, 27:1337–1341.Search in Google Scholar
[26] Ntzifa A, Kotsakis A, Georgoulias V, Lianidou E: Detection of EGFR Mutations in Plasma cfDNA and Paired CTCs of NSCLC Patients before and after Osimertinib Therapy Using Crystal Digital PCR. Cancers (Basel) 2021, 13.10.3390/cancers13112736Search in Google Scholar PubMed PubMed Central
[27] Denis JA, Patroni A, Guillerm E, Pepin D, Benali-Furet N, Wechsler J, Manceau G, Bernard M, Coulet F, Larsen AK, et al: Droplet digital PCR of circulating tumor cells from colorectal cancer patients can predict KRAS mutations before surgery. Mol Oncol 2016, 10:1221–1231.10.1016/j.molonc.2016.05.009Search in Google Scholar PubMed PubMed Central
[28] Neves RP, Raba K, Schmidt O, Honisch E, Meier-Stiegen F, Behrens B, Mohlendick B, Fehm T, Neubauer H, Klein CA, et al: Genomic high-resolution profiling of single CKpos/CD45neg flow-sorting purified circulating tumor cells from patients with metastatic breast cancer. Clin Chem 2014, 60:1290–1297.10.1373/clinchem.2014.222331Search in Google Scholar PubMed
[29] Polzer B, Medoro G, Pasch S, Fontana F, Zorzino L, Pestka A, Andergassen U, Meier-Stiegen F, Czyz ZT, Alberter B, et al: Molecular profiling of single circulating tumor cells with diagnostic intention. EMBO Mol Med 2014, 6:1371–1386.10.15252/emmm.201404033Search in Google Scholar PubMed PubMed Central
[30] Jung R, Petersen K, Kruger W, Wolf M, Wagener C, Zander A, Neumaier M: Detection of micrometastasis by cytokeratin 20 RT-PCR is limited due to stable background transcription in granulocytes. Br J Cancer 1999, 81:870–873.10.1038/sj.bjc.6690778Search in Google Scholar PubMed PubMed Central
[31] Vona G, Sabile A, Louha M, Sitruk V, Romana S, Schutze K, Capron F, Franco D, Pazzagli M, Vekemans M, et al: Isolation by size of epithelial tumor cells: a new method for the immunomorphological and molecular characterization of circulatingtumor cells. Am J Pathol 2000, 156:57–63.10.1016/S0002-9440(10)64706-2Search in Google Scholar PubMed PubMed Central
[32] Gires O, Stoecklein NH: Dynamic EpCAM expression on circulating and disseminating tumor cells: causes and consequences. Cell Mol Life Sci 2014, 71:4393–4402.10.1007/s00018-014-1693-1Search in Google Scholar PubMed PubMed Central
[33] Lim SH, Becker TM, Chua W, Ng WL, de Souza P, Spring KJ: Circulating tumour cells and the epithelial mesenchymal transition in colorectal cancer. J Clin Pathol 2014, 67:848–853.10.1136/jclinpath-2014-202499Search in Google Scholar PubMed
[34] Nagrath S, Sequist LV, Maheswaran S, Bell DW, Irimia D, Ulkus L, Smith MR, Kwak EL, Digumarthy S, Muzikansky A, et al: Isolation of rare circulating tumour cells in cancer patients by microchip technology. Nature 2007, 450:1235–1239.10.1038/nature06385Search in Google Scholar PubMed PubMed Central
[35] Descamps L, Le Roy D, Deman AL: Microfluidic-Based Technologies for CTC Isolation: A Review of 10 Years of Intense Efforts towards Liquid Biopsy. Int J Mol Sci 2022, 23.10.3390/ijms23041981Search in Google Scholar PubMed PubMed Central
[36] Macaraniag C, Luan Q, Zhou J, Papautsky I: Microfluidic techniques for isolation, formation, and characterization of circulating tumor cells and clusters. APL Bioeng 2022, 6:031501.10.1063/5.0093806Search in Google Scholar PubMed PubMed Central
[37] Pei H, Li L, Han Z, Wang Y, Tang B: Recent advances in microfluidic technologies for circulating tumor cells: enrichment, single-cell analysis, and liquid biopsy for clinical applications. Lab Chip 2020, 20:3854–3875.10.1039/D0LC00577KSearch in Google Scholar
[38] Rushton AJ, Nteliopoulos G, Shaw JA, Coombes RC: A Review of Circulating Tumour Cell Enrichment Technologies. Cancers (Basel) 2021, 13.10.3390/cancers13050970Search in Google Scholar PubMed PubMed Central
[39] Ferreira MM, Ramani VC, Jeffrey SS: Circulating tumor cell technologies. Mol Oncol 2016, 10:374–394.10.1016/j.molonc.2016.01.007Search in Google Scholar PubMed PubMed Central
[40] Allard WJ, Matera J, Miller MC, Repollet M, Connelly MC, Rao C, Tibbe AG, Uhr JW, Terstappen LW: Tumor cells circulate in the peripheral blood of all major carcinomas but not in healthy subjects or patients with nonmalignant diseases. Clin Cancer Res 2004, 10:6897–6904.10.1158/1078-0432.CCR-04-0378Search in Google Scholar PubMed
[41] Cristofanilli M, Budd GT, Ellis MJ, Stopeck A, Matera J, Miller MC, Reuben JM, Doyle GV, Allard WJ, Terstappen LW, Hayes DF: Circulating tumor cells, disease progression, and survival in metastatic breast cancer. N Engl J Med 2004, 351:781–791.10.1056/NEJMoa040766Search in Google Scholar PubMed
[42] Riethdorf S, Fritsche H, Muller V, Rau T, Schindlbeck C, Rack B, Janni W, Coith C, Beck K, Janicke F, et al: Detection of circulating tumor cells in peripheral blood of patients with metastatic breast cancer: a validation study of the CellSearch system. Clin Cancer Res 2007, 13:920–928.10.1158/1078-0432.CCR-06-1695Search in Google Scholar PubMed
[43] de Bono JS, Scher HI, Montgomery RB, Parker C, Miller MC, Tissing H, Doyle GV, Terstappen LW, Pienta KJ, Raghavan D: Circulating tumor cells predict survival benefit from treatment in metastatic castration-resistant prostate cancer. Clin Cancer Res 2008, 14:6302–6309.10.1158/1078-0432.CCR-08-0872Search in Google Scholar PubMed
[44] Cohen SJ, Punt CJ, Iannotti N, Saidman BH, Sabbath KD, Gabrail NY, Picus J, Morse M, Mitchell E, Miller MC, et al: Relationship of circulating tumor cells to tumor response, progression-free survival, and overall survival in patients with metastatic colorectal cancer. J Clin Oncol 2008, 26:3213–3221.10.1200/JCO.2007.15.8923Search in Google Scholar PubMed
[45] Lindsay CR, Blackhall FH, Carmel A, Fernandez-Gutierrez F, Gazzaniga P, Groen HJM, Hiltermann TJN, Krebs MG, Loges S, Lopez-Lopez R, et al: EPAC-lung: pooled analysis of circulating tumour cells in advanced non-small cell lung cancer. Eur J Cancer 2019, 117:60–68.10.1016/j.ejca.2019.04.019Search in Google Scholar PubMed
[46] Foy V, Lindsay CR, Carmel A, Fernandez-Gutierrez F, Krebs MG, Priest L, Carter M, Groen HJM, Hiltermann TJN, de Luca A, et al: EPAC-lung: European pooled analysis of the prognostic value of circulating tumour cells in small cell lung cancer. Transl Lung Cancer Res 2021, 10:1653–1665.10.21037/tlcr-20-1061Search in Google Scholar PubMed PubMed Central
[47] Hiraiwa K, Takeuchi H, Hasegawa H, Saikawa Y, Suda K, Ando T, Kumagai K, Irino T, Yoshikawa T, Matsuda S, et al: Clinical significance of circulating tumor cells in blood from patients with gastrointestinal cancers. Ann Surg Oncol 2008, 15:3092–3100.10.1245/s10434-008-0122-9Search in Google Scholar PubMed
[48] Hugenschmidt H, Labori KJ, Brunborg C, Verbeke CS, Seeberg LT, Schirmer CB, Renolen A, Borgen EF, Naume B, Wiedswang G: Circulating Tumor Cells are an Independent Predictor of Shorter Survival in Patients Undergoing Resection for Pancreatic and Periampullary Adenocarcinoma. Ann Surg 2020, 271:549–558.10.1097/SLA.0000000000003035Search in Google Scholar PubMed
[49] Grobe A, Blessmann M, Hanken H, Friedrich RE, Schon G, Wikner J, Effenberger KE, Kluwe L, Heiland M, Pantel K, Riethdorf S: Prognostic relevance of circulating tumor cells in blood and disseminated tumor cells in bone marrow of patients with squamous cell carcinoma of the oral cavity. Clin Cancer Res 2014, 20:425–433.10.1158/1078-0432.CCR-13-1101Search in Google Scholar PubMed
[50] Scher HI, Heller G, Molina A, Attard G, Danila DC, Jia X, Peng W, Sandhu SK, Olmos D, Riisnaes R, et al: Circulating tumor cell biomarker panel as an individual-level surrogate for survival in metastatic castration-resistant prostate cancer. J Clin Oncol 2015, 33:1348–1355.10.1200/JCO.2014.55.3487Search in Google Scholar PubMed PubMed Central
[51] Lorente D, Olmos D, Mateo J, Bianchini D, Seed G, Fleisher M, Danila DC, Flohr P, Crespo M, Figueiredo I, et al: Decline in Circulating Tumor Cell Count and Treatment Outcome in Advanced Prostate Cancer. Eur Urol 2016, 70:985–992.10.1016/j.eururo.2016.05.023Search in Google Scholar PubMed PubMed Central
[52] Heller G, McCormack R, Kheoh T, Molina A, Smith MR, Dreicer R, Saad F, de Wit R, Aftab DT, Hirmand M, et al: Circulating Tumor Cell Number as a Response Measure of Prolonged Survival for Metastatic Castration-Resistant Prostate Cancer: A Comparison With Prostate-Specific Antigen Across Five Randomized Phase III Clinical Trials. J Clin Oncol 2018, 36:572–580.10.1200/JCO.2017.75.2998Search in Google Scholar PubMed PubMed Central
[53] van Dalum G, van der Stam GJ, Tibbe AG, Franken B, Mastboom WJ, Vermes I, de Groot MR, Terstappen LW: Circulating tumor cells before and during follow-up after breast cancer surgery. Int J Oncol 2015, 46:407–413.10.3892/ijo.2014.2694Search in Google Scholar PubMed
[54] Janni WJ, Rack B, Terstappen LW, Pierga JY, Taran FA, Fehm T, Hall C, de Groot MR, Bidard FC, Friedl TW, et al: Pooled Analysis of the Prognostic Relevance of Circulating Tumor Cells in Primary Breast Cancer. Clin Cancer Res 2016, 22:2583–2593.10.1158/1078-0432.CCR-15-1603Search in Google Scholar PubMed
[55] Rack B, Schindlbeck C, Juckstock J, Andergassen U, Hepp P, Zwingers T, Friedl TW, Lorenz R, Tesch H, Fasching PA, et al: Circulating tumor cells predict survival in early average-to-high risk breast cancer patients. J Natl Cancer Inst 2014, 106.10.1093/jnci/dju066Search in Google Scholar PubMed PubMed Central
[56] Bidard FC, Michiels S, Riethdorf S, Mueller V, Esserman LJ, Lucci A, Naume B, Horiguchi J, Gisbert-Criado R, Sleijfer S, et al: Circulating Tumor Cells in Breast Cancer Patients Treated by Neoadjuvant Chemotherapy: A Meta-analysis. J Natl Cancer Inst 2018, 110:560–567.10.1093/jnci/djy018Search in Google Scholar PubMed
[57] Trapp E, Janni W, Schindlbeck C, Juckstock J, Andergassen U, deGregorio A, Alunni-Fabbroni M, Tzschaschel M, Polasik A, Koch JG, et al: Response to Di Cosimo, Torri, and Porcu. J Natl Cancer Inst 2019, 111:1234–1235.10.1093/jnci/djz095Search in Google Scholar PubMed PubMed Central
[58] Ignatiadis M, Litiere S, Rothe F, Riethdorf S, Proudhon C, Fehm T, Aalders K, Forstbauer H, Fasching PA, Brain E, et al: Trastuzumab versus observation for HER2 nonamplified early breast cancer with circulating tumor cells (EORTC 90091–10093, BIG 1–12, Treat CTC): a randomized phase II trial. Ann Oncol 2018, 29:1777–1783.10.1093/annonc/mdy211Search in Google Scholar PubMed
[59] van Dalum G, Stam GJ, Scholten LF, Mastboom WJ, Vermes I, Tibbe AG, De Groot MR, Terstappen LW: Importance of circulating tumor cells in newly diagnosed colorectal cancer. Int J Oncol 2015, 46:1361–1368.10.3892/ijo.2015.2824Search in Google Scholar PubMed
[60] Vasseur A, Kiavue N, Bidard FC, Pierga JY, Cabel L: Clinical utility of circulating tumor cells: an update. Mol Oncol 2021, 15:1647–1666.10.1002/1878-0261.12869Search in Google Scholar PubMed PubMed Central
[61] Marquette CH, Boutros J, Benzaquen J, Ferreira M, Pastre J, Pison C, Padovani B, Bettayeb F, Fallet V, Guibert N, et al: Circulating tumour cells as a potential biomarker for lung cancer screening: a prospective cohort study. Lancet Respir Med 2020, 8:709–716.10.2139/ssrn.3496941Search in Google Scholar
[62] Pantel K: Blood tests for early detection of lung cancer: challenges and promises. Lancet Respir Med 2020, 8:654–656.10.1016/S2213-2600(20)30115-6Search in Google Scholar PubMed
[63] Smerage JB, Barlow WE, Hortobagyi GN, Winer EP, Leyland-Jones B, Srkalovic G, Tejwani S, Schott AF, O’Rourke MA, Lew DL, et al: Circulating tumor cells and response to chemotherapy in metastatic breast cancer: SWOG S0500. J Clin Oncol 2014, 32:3483–3489.10.1200/JCO.2014.56.2561Search in Google Scholar PubMed PubMed Central
[64] Cabel L, Berger F, Cottu P, Loirat D, Rampanou A, Brain E, Cyrille S, Bourgeois H, Kiavue N, Deluche E, et al: Clinical utility of circulating tumour cell-based monitoring of late-line chemotherapy for metastatic breast cancer: the randomised CirCe01 trial. Br J Cancer 2021, 124:1207–1213.10.1038/s41416-020-01227-3Search in Google Scholar PubMed PubMed Central
[65] Bidard FC, Jacot W, Kiavue N, Dureau S, Kadi A, Brain E, Bachelot T, Bourgeois H, Goncalves A, Ladoire S, et al: Efficacy of Circulating Tumor Cell Count-Driven vs Clinician-Driven First-line Therapy Choice in Hormone Receptor-Positive, ERBB2-Negative Metastatic Breast Cancer: The STIC CTC Randomized Clinical Trial. JAMA Oncol 2021, 7:34–41.10.1001/jamaoncol.2020.5660Search in Google Scholar PubMed PubMed Central
[66] Aranda E, Vieitez JM, Gomez-Espana A, Gil Calle S, Salud-Salvia A, Grana B, Garcia-Alfonso P, Rivera F, Quintero-Aldana GA, Reina-Zoilo JJ, et al: FOLFOXIRI plus bevacizumab versus FOLFOX plus bevacizumab for patients with metastatic colorectal cancer and >/=3 circulating tumour cells: the randomised phase III VISNU-1 trial. ESMO Open 2020, 5:e000944.10.1136/esmoopen-2020-000944Search in Google Scholar PubMed PubMed Central
[67] Kurniali PC, Storandt MH, Jin Z: Utilization of Circulating Tumor Cells in the Management of Solid Tumors. J Pers Med 2023, 13.10.3390/jpm13040694Search in Google Scholar PubMed PubMed Central
[68] Fehm T, Müller V, Banys-Paluchowski M, Fasching P, Friedl T, Hartkopf A, Huober J, Loehberg C, Rack B, Riethdorf S, et al: Abstract PD3-12: Efficacy of the tyrosine kinase inhibitor lapatinib in the treatment of patients with HER2-negative metastatic breast cancer and HER2-positive circulating tumor cells – results from the randomized phase III DETECT III trial.2021.10.1158/1538-7445.SABCS20-PD3-12Search in Google Scholar
[69] Georgoulias V, Bozionelou V, Agelaki S, Perraki M, Apostolaki S, Kallergi G, Kalbakis K, Xyrafas A, Mavroudis D: Trastuzumab decreases the incidence of clinical relapses in patients with early breast cancer presenting chemotherapy-resistant CK-19mRNA-positive circulating tumor cells: results of a randomized phase II study. Ann Oncol 2012, 23:1744–1750.10.1093/annonc/mds020Search in Google Scholar PubMed
[70] Muller V, Banys-Paluchowski M, Friedl TWP, Fasching PA, Schneeweiss A, Hartkopf A, Wallwiener D, Rack B, Meier-Stiegen F, Huober J, et al: Prognostic relevance of the HER2 status of circulating tumor cells in metastatic breast cancer patients screened for participation in the DETECT study program. ESMO Open 2021, 6:100299.10.1016/j.esmoop.2021.100299Search in Google Scholar PubMed PubMed Central
[71] Antonarakis ES, Lu C, Wang H, Luber B, Nakazawa M, Roeser JC, Chen Y, Mohammad TA, Chen Y, Fedor HL, et al: AR-V7 and resistance to enzalutamide and abiraterone in prostate cancer. N Engl J Med 2014, 371:1028–1038.10.1056/NEJMoa1315815Search in Google Scholar PubMed PubMed Central
[72] Antonarakis ES, Lu C, Luber B, Wang H, Chen Y, Zhu Y, Silberstein JL, Taylor MN, Maughan BL, Denmeade SR, et al: Clinical Significance of Androgen Receptor Splice Variant-7 mRNA Detection in Circulating Tumor Cells of Men With Metastatic Castration-Resistant Prostate Cancer Treated With First- and Second-Line Abiraterone and Enzalutamide. J Clin Oncol 2017, 35:2149–2156.10.1200/JCO.2016.70.1961Search in Google Scholar PubMed PubMed Central
[73] Scher HI, Lu D, Schreiber NA, Louw J, Graf RP, Vargas HA, Johnson A, Jendrisak A, Bambury R, Danila D, et al: Association of AR-V7 on Circulating Tumor Cells as a Treatment-Specific Biomarker With Outcomes and Survival in Castration-Resistant Prostate Cancer. JAMA Oncol 2016, 2:1441–1449.10.1001/jamaoncol.2016.1828Search in Google Scholar PubMed PubMed Central
[74] Scher HI, Graf RP, Schreiber NA, Jayaram A, Winquist E, McLaughlin B, Lu D, Fleisher M, Orr S, Lowes L, et al: Assessment of the Validity of Nuclear-Localized Androgen Receptor Splice Variant 7 in Circulating Tumor Cells as a Predictive Biomarker for Castration-Resistant Prostate Cancer. JAMA Oncol 2018, 4:1179–1186.10.1001/jamaoncol.2018.1621Search in Google Scholar PubMed PubMed Central
[75] Response to Comments: MolDX: Oncotype DX AR-V7 Nucleus Detect for Men with Metastatic Castrate Resistant Prostate Cancer (MCRPC) (DL37915) [https://www.cms.gov/medicare-coverage-database/view/article.aspx?articleId=56234&ver=3]Search in Google Scholar
[76] Armstrong AJ, Halabi S, Luo J, Nanus DM, Giannakakou P, Szmulewitz RZ, Danila DC, Healy P, Anand M, Rothwell CJ, et al: Prospective Multicenter Validation of Androgen Receptor Splice Variant 7 and Hormone Therapy Resistance in High-Risk Castration-Resistant Prostate Cancer: The PROPHECY Study. J Clin Oncol 2019, 37:1120–1129.10.1200/JCO.18.01731Search in Google Scholar PubMed PubMed Central
[77] FDA: DEN200062. 2022.Search in Google Scholar
[78] Cohen EN, Jayachandran G, Moore RG, Cristofanilli M, Lang JE, Khoury JD, Press MF, Kim KK, Khazan N, Zhang Q, et al: A Multi-Center Clinical Study to Harvest and Characterize Circulating Tumor Cells from Patients with Metastatic Breast Cancer Using the Parsortix((R)) PC1 System. Cancers (Basel) 2022, 14.10.3390/cancers14215238Search in Google Scholar PubMed PubMed Central
[79] Visal TH, den Hollander P, Cristofanilli M, Mani SA: Circulating tumour cells in the -omics era: how far are we from achieving the ‘singularity’? British Journal of Cancer 2022, 127:173–184.10.1038/s41416-022-01768-9Search in Google Scholar PubMed PubMed Central
[80] Deng Z, Wu S, Wang Y, Shi D: Circulating tumor cell isolation for cancer diagnosis and prognosis. EBioMedicine 2022, 83:104237.10.1016/j.ebiom.2022.104237Search in Google Scholar PubMed PubMed Central
[81] Kolinsky MP, Stoecklein N, Lambros M, Gil V, Rodrigues DN, Carreira S, Zafeiriou Z, de Bono JS: Genetic Analysis of Circulating Tumour Cells. Recent Results Cancer Res 2020, 215:57–76.10.1007/978-3-030-26439-0_3Search in Google Scholar PubMed
[82] van Bussel MTJ, Pluim D, Bol M, Beijnen JH, Schellens JHM, Brandsma D: EpCAM-based assays for epithelial tumor cell detection in cerebrospinal fluid. J Neurooncol 2018, 137:1–10.10.1007/s11060-017-2691-6Search in Google Scholar PubMed
[83] Nakasu Y, Deguchi S, Nakasu S, Yamazaki M, Notsu A, Mitsuya K, Hayashi N: Diagnostic accuracy of cerebrospinal fluid liquid biopsy and MRI for leptomeningeal metastases in solid cancers: A systematic review and meta-analysis. Neurooncol Adv 2023, 5:vdad002.10.1093/noajnl/vdad002Search in Google Scholar PubMed PubMed Central
[84] Fischer JC, Niederacher D, Topp SA, Honisch E, Schumacher S, Schmitz N, Zacarias Fohrding L, Vay C, Hoffmann I, Kasprowicz NS, et al: Diagnostic leukapheresis enables reliable detection of circulating tumor cells of nonmetastatic cancer patients. Proc Natl Acad Sci U S A 2013, 110:16580–16585.10.1073/pnas.1313594110Search in Google Scholar PubMed PubMed Central
[85] Andree KC, Mentink A, Zeune LL, Terstappen L, Stoecklein NH, Neves RP, Driemel C, Lampignano R, Yang L, Neubauer H, et al: Toward a real liquid biopsy in metastatic breast and prostate cancer: Diagnostic LeukApheresis increases CTC yields in a European prospective multicenter study (CTCTrap). Int J Cancer 2018, 143:2584–2591.10.1002/ijc.31752Search in Google Scholar PubMed PubMed Central
[86] Faugeroux V, Pailler E, Oulhen M, Deas O, Brulle-Soumare L, Hervieu C, Marty V, Alexandrova K, Andree KC, Stoecklein NH, et al: Genetic characterization of a unique neuroendocrine transdifferentiation prostate circulating tumor cell-derived eXplant model. Nat Commun 2020, 11:1884.10.1038/s41467-020-15426-2Search in Google Scholar PubMed PubMed Central
[87] Fehm TN, Meier-Stiegen F, Driemel C, Jager B, Reinhardt F, Naskou J, Franken A, Neubauer H, Neves RPL, van Dalum G, et al: Diagnostic leukapheresis for CTC analysis in breast cancer patients: CTC frequency, clinical experiences and recommendations for standardized reporting. Cytometry A 2018, 93:1213–1219.10.1002/cyto.a.23669Search in Google Scholar PubMed
[88] Franken A, Driemel C, Behrens B, Meier-Stiegen F, Endris V, Stenzinger A, Niederacher D, Fischer JC, Stoecklein NH, Ruckhaeberle E, et al: Label-Free Enrichment and Molecular Characterization of Viable Circulating Tumor Cells from Diagnostic Leukapheresis Products. Clin Chem 2019, 65:549–558.10.1373/clinchem.2018.296814Search in Google Scholar PubMed
[89] Lambros MB, Seed G, Sumanasuriya S, Gil V, Crespo M, Fontes M, Chandler R, Mehra N, Fowler G, Ebbs B, et al: Single-Cell Analyses of Prostate Cancer Liquid Biopsies Acquired by Apheresis. Clin Cancer Res 2018, 24:5635–5644.10.1158/1078-0432.CCR-18-0862Search in Google Scholar PubMed
[90] Mout L, van Dessel LF, Kraan J, de Jong AC, Neves RPL, Erkens-Schulze S, Beaufort CM, Sieuwerts AM, van Riet J, Woo TLC, et al: Generating human prostate cancer organoids from leukapheresis enriched circulating tumour cells. Eur J Cancer 2021, 150:179–189.10.1016/j.ejca.2021.03.023Search in Google Scholar PubMed
[91] Tamminga M, Andree KC, van den Bos H, Hiltermann TJN, Mentink A, Spierings DCJ, Lansdorp P, Timens W, Schuuring E, Terstappen L, Groen HJM: Leukapheresis increases circulating tumour cell yield in non-small cell lung cancer, counts related to tumour response and survival. Br J Cancer 2022, 126:409–418.10.1038/s41416-021-01634-0Search in Google Scholar PubMed PubMed Central
[92] Dong L, Du X, Lu C, Zhang Z, Huang CY, Yang L, Warren S, Kuczler MD, Reyes DK, Luo J, et al: RNA profiling of circulating tumor cells systemically captured from diagnostic leukapheresis products in prostate cancer patients. Mater Today Bio 2022, 17:100474.10.1016/j.mtbio.2022.100474Search in Google Scholar PubMed PubMed Central
[93] Mishra A, Dubash TD, Edd JF, Jewett MK, Garre SG, Karabacak NM, Rabe DC, Mutlu BR, Walsh JR, Kapur R, et al: Ultrahigh-throughput magnetic sorting of large blood volumes for epitope-agnostic isolation of circulating tumor cells. Proc Natl Acad Sci U S A 2020, 117:16839–16847.10.1073/pnas.2006388117Search in Google Scholar PubMed PubMed Central
[94] Stevens M, Liu P, Niessink T, Mentink A, Abelmann L, Terstappen L: Optimal Halbach Configuration for Flow-through Immunomagnetic CTC Enrichment. Diagnostics (Basel) 2021, 11.10.3390/diagnostics11061020Search in Google Scholar PubMed PubMed Central
[95] Cieslikowski WA, Milecki P, Swierczewska M, Ida A, Kasperczak M, Jankowiak A, Nowicki M, Pantel K, Alix-Panabieres C, Zabel M, et al: Baseline CTC Count as a Predictor of Long-Term Outcomes in High-Risk Prostate Cancer. J Pers Med 2023, 13.10.3390/jpm13040608Search in Google Scholar PubMed PubMed Central
[96] Kim TH, Wang Y, Oliver CR, Thamm DH, Cooling L, Paoletti C, Smith KJ, Nagrath S, Hayes DF: A temporary indwelling intravascular aphaeretic system for in vivo enrichment of circulating tumor cells. Nat Commun 2019, 10:1478.10.1038/s41467-019-09439-9Search in Google Scholar PubMed PubMed Central
[97] Stevens M, Nanou A, Terstappen L, Driemel C, Stoecklein NH, Coumans FAW: StarDist Image Segmentation Improves Circulating Tumor Cell Detection. Cancers (Basel) 2022, 14.10.3390/cancers14122916Search in Google Scholar PubMed PubMed Central
[98] Shen C, Rawal S, Brown R, Zhou H, Agarwal A, Watson MA, Cote RJ, Yang C: Automatic detection of circulating tumor cells and cancer associated fibroblasts using deep learning. Sci Rep 2023, 13:5708.10.1038/s41598-023-32955-0Search in Google Scholar PubMed PubMed Central
[99] Zeune LL, Boink YE, van Dalum G, Nanou A, de Wit S, Andree KC, Swennenhuis JF, van Gils SA, Terstappen LWMM, Brune C: Deep learning of circulating tumour cells. Nature Machine Intelligence 2020, 2:124–133.10.1038/s42256-020-0153-xSearch in Google Scholar
[100] Schonhoft JD, Zhao JL, Jendrisak A, Carbone EA, Barnett ES, Hullings MA, Gill A, Sutton R, Lee J, Dago AE, et al: Morphology-Predicted Large-Scale Transition Number in Circulating Tumor Cells Identifies a Chromosomal Instability Biomarker Associated with Poor Outcome in Castration-Resistant Prostate Cancer. Cancer Res 2020, 80:4892–4903.10.1158/0008-5472.CAN-20-1216Search in Google Scholar PubMed PubMed Central
[101] Strati A, Markou A, Kyriakopoulou E, Lianidou E: Detection and Molecular Characterization of Circulating Tumour Cells: Challenges for the Clinical Setting. Cancers (Basel) 2023, 15.10.3390/cancers15072185Search in Google Scholar PubMed PubMed Central
[102] Pantel K, Terstappen LW, Baggiani B, Krahn T, Panabières C, Lianidou E, Naume B, Farace F, Schlange T: Abstract 1579: IMI’s CANCER-ID: Implications of liquid biopsy technology standardization for its clinical use. Cancer Research 2018, 78:1579–1579.10.1158/1538-7445.AM2018-1579Search in Google Scholar
[103] Neves RPL, Ammerlaan W, Andree KC, Bender S, Cayrefourcq L, Driemel C, Koch C, Luetke-Eversloh MV, Oulhen M, Rossi E, et al: Proficiency Testing to Assess Technical Performance for CTC-Processing and Detection Methods in CANCER-ID. Clin Chem 2021, 67:631–641.10.1093/clinchem/hvaa322Search in Google Scholar PubMed
[104] Patel AS, Allen JE, Dicker DT, Peters KL, Sheehan JM, Glantz MJ, El-Deiry WS: Identification and enumeration of circulating tumor cells in the cerebrospinal fluid of breast cancer patients with central nervous system metastases. Oncotarget 2011, 2:752–760.10.18632/oncotarget.336Search in Google Scholar PubMed PubMed Central
[105] Le Rhun E, Massin F, Tu Q, Bonneterre J, Bittencourt Mde C, Faure GC: Development of a new method for identification and quantification in cerebrospinal fluid of malignant cells from breast carcinoma leptomeningeal metastasis. BMC Clin Pathol 2012, 12:21.10.1186/1472-6890-12-21Search in Google Scholar PubMed PubMed Central
[106] Le Rhun E, Tu Q, De Carvalho Bittencourt M, Farre I, Mortier L, Cai H, Kohler C, Faure GC: Detection and quantification of CSF malignant cells by the CellSearch technology in patients with melanoma leptomeningeal metastasis. Med Oncol 2013, 30:538.10.1007/s12032-013-0538-3Search in Google Scholar PubMed
[107] Magbanua MJ, Melisko M, Roy R, Sosa EV, Hauranieh L, Kablanian A, Eisenbud LE, Ryazantsev A, Au A, Scott JH, Park JW: Molecular profiling of tumor cells in cerebrospinal fluid and matched primary tumors from metastatic breast cancer patients with leptomeningeal carcinomatosis. Cancer Res 2013, 73:7134–7143.10.1158/0008-5472.CAN-13-2051Search in Google Scholar PubMed
[108] Nayak L, Fleisher M, Gonzalez-Espinoza R, Lin O, Panageas K, Reiner A, Liu CM, Deangelis LM, Omuro A: Rare cell capture technology for the diagnosis of leptomeningeal metastasis in solid tumors. Neurology 2013, 80:1598–1605; discussion 1603.10.1212/WNL.0b013e31828f183fSearch in Google Scholar PubMed PubMed Central
[109] Tu Q, Wu X, Le Rhun E, Blonski M, Wittwer B, Taillandier L, De Carvalho Bittencourt M, Faure GC: CellSearch technology applied to the detection and quantification of tumor cells in CSF of patients with lung cancer leptomeningeal metastasis. Lung Cancer 2015, 90:352–357.10.1016/j.lungcan.2015.09.008Search in Google Scholar PubMed
[110] Jiang BY, Li YS, Guo WB, Zhang XC, Chen ZH, Su J, Zhong WZ, Yang XN, Yang JJ, Shao Y, et al: Detection of Driver and Resistance Mutations in Leptomeningeal Metastases of NSCLC by Next-Generation Sequencing of Cerebrospinal Fluid Circulating Tumor Cells. Clin Cancer Res 2017, 23:5480–5488.10.1158/1078-0432.CCR-17-0047Search in Google Scholar PubMed
[111] Lin X, Fleisher M, Rosenblum M, Lin O, Boire A, Briggs S, Bensman Y, Hurtado B, Shagabayeva L, DeAngelis LM, et al: Cerebrospinal fluid circulating tumor cells: a novel tool to diagnose leptomeningeal metastases from epithelial tumors. Neuro Oncol 2017, 19:1248–1254.10.1093/neuonc/nox066Search in Google Scholar PubMed PubMed Central
[112] Torre M, Lee EQ, Chukwueke UN, Nayak L, Cibas ES, Lowe AC: Integration of rare cell capture technology into cytologic evaluation of cerebrospinal fluid specimens from patients with solid tumors and suspected leptomeningeal metastasis. J Am Soc Cytopathol 2020, 9:45–54.10.1016/j.jasc.2019.09.001Search in Google Scholar PubMed
[113] Malani R, Fleisher M, Kumthekar P, Lin X, Omuro A, Groves MD, Lin NU, Melisko M, Lassman AB, Jeyapalan S, et al: Cerebrospinal fluid circulating tumor cells as a quantifiable measurement of leptomeningeal metastases in patients with HER2 positive cancer. J Neurooncol 2020, 148:599–606.10.1007/s11060-020-03555-zSearch in Google Scholar PubMed PubMed Central
[114] Darlix A, Cayrefourcq L, Pouderoux S, Menjot de Champfleur N, Bievelez A, Jacot W, Leaha C, Thezenas S, Alix-Panabieres C: Detection of Circulating Tumor Cells in Cerebrospinal Fluid of Patients with Suspected Breast Cancer Leptomeningeal Metastases: A Prospective Study. Clin Chem 2022, 68:1311–1322.10.1093/clinchem/hvac127Search in Google Scholar PubMed
[115] Wooster M, McGuinness JE, Fenn KM, Singh VM, Franks LE, Lee S, Cieremans D, Lassman AB, Hershman DL, Crew KD, et al: Diagnosis of Leptomeningeal Metastasis in Women With Breast Cancer Through Identification of Tumor Cells in Cerebrospinal Fluid Using the CNSide Assay. Clin Breast Cancer 2022, 22:e457-e462.10.1016/j.clbc.2021.11.002Search in Google Scholar PubMed PubMed Central
© 2023 bei den Autoren, publiziert von De Gruyter.
Dieses Werk ist lizensiert unter einer Creative Commons Namensnennung 4.0 International Lizenz.
Articles in the same Issue
- Frontmatter
- MAIN TOPIC Liquid Biopsies
- Liquid Biopsy: minimal-invasive analysis of somatic alterations
- The changing face of circulating tumor DNA (ctDNA) profiling: Factors that shape the landscape of methodologies, technologies, and commercialization
- Clinical application of circulating tumor cells
- Clinical applications and challenges in the field of extracellular vesicles
- Liquid biopsy-based early tumor and minimal residual disease detection: New perspectives for cancer predisposition syndromes
- Liquid biopsies and those three little words: finding the perfect match for the MTB
- The utility of liquid biopsy in clinical genetic diagnosis of cancer and monogenic mosaic disorders
- Non-invasive prenatal testing: when results suggests maternal cancer
- BERICHTE AUS DER HUMANGENETIK
- Personalia
- Nachruf Prof. Dr. med. Michael Speicher
- Nachruf Prof. Dr. rer. nat. Jeanette Erdmann
- Nachruf Prof. Dr. med. Wilko Weichert
- Ein Geburtstagsgruß für Hans-Hilger Ropers
- Stellungnahmen und Leitlinien
- Deutsche Gesellschaft für Humangenetik e.V. (GfH)
- Deutsche Gesellschaft für Humangenetik e.V. (GfH)
- GfH-Verbandsmitteilungen
- Syndromtag 2023 in Aachen vom 22.–23. September
- Frank-Majewski-Preisträgerin 2023
- Die GfH-Juniorakademie 2023 – #GfHJAK23 @schlossbuchenau
- Tagungsbericht SSIEM Jahrestagung vom 29.08.2023 bis 01.09.2023 in Jerusalem
- Tagungsbericht Kongress für Kinder- und Jugendmedizin 20. bis 23. September 2023 in Hamburg
- Ausschreibung Humangenetik-Promotionspreis 2024
- 36. Tumorgenetische Arbeitstagung
- Wie ist die Weiterbildungssituation der NaturwissenschaftlerInnen in der Humangenetik in Deutschland, und wie erreichen wir eine staatliche Anerkennung der Weiterbildung zur/zum FachhumangenetikerIn?
- BVDH-Verbandsmitteilungen
- Die staatliche Anerkennung der/des „Fachhumangenetiker/in (GfH)“ ist überfällig
- Die humangenetische Beratung ist mit den aktuellen Vergütungsstrukturen nicht mehr zu erbringen: KollegInnen, die nur humangenetische Beratung anbieten, müssen ihre Praxen schließen!
- Aktuelle Nachrichten
- Akademie Humangenetik
Articles in the same Issue
- Frontmatter
- MAIN TOPIC Liquid Biopsies
- Liquid Biopsy: minimal-invasive analysis of somatic alterations
- The changing face of circulating tumor DNA (ctDNA) profiling: Factors that shape the landscape of methodologies, technologies, and commercialization
- Clinical application of circulating tumor cells
- Clinical applications and challenges in the field of extracellular vesicles
- Liquid biopsy-based early tumor and minimal residual disease detection: New perspectives for cancer predisposition syndromes
- Liquid biopsies and those three little words: finding the perfect match for the MTB
- The utility of liquid biopsy in clinical genetic diagnosis of cancer and monogenic mosaic disorders
- Non-invasive prenatal testing: when results suggests maternal cancer
- BERICHTE AUS DER HUMANGENETIK
- Personalia
- Nachruf Prof. Dr. med. Michael Speicher
- Nachruf Prof. Dr. rer. nat. Jeanette Erdmann
- Nachruf Prof. Dr. med. Wilko Weichert
- Ein Geburtstagsgruß für Hans-Hilger Ropers
- Stellungnahmen und Leitlinien
- Deutsche Gesellschaft für Humangenetik e.V. (GfH)
- Deutsche Gesellschaft für Humangenetik e.V. (GfH)
- GfH-Verbandsmitteilungen
- Syndromtag 2023 in Aachen vom 22.–23. September
- Frank-Majewski-Preisträgerin 2023
- Die GfH-Juniorakademie 2023 – #GfHJAK23 @schlossbuchenau
- Tagungsbericht SSIEM Jahrestagung vom 29.08.2023 bis 01.09.2023 in Jerusalem
- Tagungsbericht Kongress für Kinder- und Jugendmedizin 20. bis 23. September 2023 in Hamburg
- Ausschreibung Humangenetik-Promotionspreis 2024
- 36. Tumorgenetische Arbeitstagung
- Wie ist die Weiterbildungssituation der NaturwissenschaftlerInnen in der Humangenetik in Deutschland, und wie erreichen wir eine staatliche Anerkennung der Weiterbildung zur/zum FachhumangenetikerIn?
- BVDH-Verbandsmitteilungen
- Die staatliche Anerkennung der/des „Fachhumangenetiker/in (GfH)“ ist überfällig
- Die humangenetische Beratung ist mit den aktuellen Vergütungsstrukturen nicht mehr zu erbringen: KollegInnen, die nur humangenetische Beratung anbieten, müssen ihre Praxen schließen!
- Aktuelle Nachrichten
- Akademie Humangenetik