Integrating osteopathic manipulative treatment into prenatal care visits in a family medicine resident clinic
-
 ,
,

Abstract
Literature describing the integration of osteopathic manipulative treatment (OMT) during prenatal care visits in a resident clinic setting are scarce. Concise and readily accessible resources reviewing OMT in pregnancy are limited. We sought to integrate OMT into routine prenatal care appointments in a family medicine resident clinic setting and create a concise resource for those performing OMT in pregnancy. Musculoskeletal (MSK) pain in pregnancy is common. Specifically, low back pain (LBP) often accompanies pregnancy and may negatively impact sleep, the ability to work, and the ability to complete daily tasks. Treatment options for LBP in pregnancy are limited due to the concern for fetal or maternal harm associated with pharmacologic options or invasive procedures. OMT is a low-risk intervention that has been demonstrated to improve back pain and reduce deterioration of back-specific function in pregnancy. Over a 12-month period, one resident physician offered OMT during routine prenatal care visits in a family medicine resident clinic. During the study period, we identified barriers to integrating OMT along with solutions. Barriers to integrating OMT were noted in three areas: clinic setup and logistics, attending physician awareness of OMT in pregnancy, and treating physician knowledge of OMT in pregnancy. OMT provides pregnant patients with additional treatment options and relief from MSK pain. This may reduce the number of patients with untreated MSK pain and benefit those who are unable to attend additional appointments outside of prenatal care due to financial or logistic barriers. OMT can be integrated into routine prenatal care visits in a training setting by providing complaint-specific OMT and determining how treatments can be performed for each unique examination room and table. Reviewing OMT in pregnancy with the attending physician prior to treatment, contraindications to OMT in pregnancy, and visualizing how treatments will be altered in pregnancy allows for smooth integration.
Offering OMT during prenatal care appointments provides pregnant patients with another treatment option for MSK pain. Up to 80.0 % of women report musculoskeletal (MSK) pain in pregnancy [1]. Low back pain (LBP) specifically is endorsed by 58.0 % of pregnant individuals, with over half reporting LBP impairing activities of daily living [2]. Unfortunately, only 32.0 % of patients disclose LBP to their physician during prenatal care visits; among those who mention LBP, as few as 25.0 % are given treatment options [2]. Pain during pregnancy negatively impacts sleep and the ability to perform routine activities [2], [3], [4], [5]. Treatment options for LBP in pregnancy are limited due to the potential adverse impact of medication on the fetus or maternal-fetal risk associated with procedures. OMT has been shown to alleviate LBP, lumbopelvic pain, and to reduce deterioration of back-specific functions in pregnancy [6], [7], [8], [9].
The safety of OMT in pregnancy is well established. However, it is important to review nuances of this low-risk intervention in pregnancy [6], [7], [8], [9]. Contraindications to OMT in pregnancy are listed in Table 1. These conditions include hypertensive disorders of pregnancy, preterm labor, premature rupture of membranes, fetal distress, vaginal bleeding, and incompetent cervix [10]. In general, any antenatal condition that would require urgent evaluation in the emergency department or obstetrics triage is a contraindication to OMT in pregnancy.
The OMT modalities to avoid in pregnancy are listed in Table 2. CV-4 is contraindicated due to a pilot study that reported the induction of contractions in postdate women [11]. This finding has not been noted in subsequent studies [11, 12]. Cervical high-velocity low-amplitude (HVLA) is avoided in pregnancy due to increased ligamentous laxity in late pregnancy and a single case report of cervical vertebrae fracture [13, 14].
Studies describing the effectiveness and safety of OMT in pregnancy typically provide treatments at OMT-only appointments where treatment may not be performed by the physician providing the prenatal care [7, 8, 15, 16]. Studies that describe integrating OMT into routine clinic visits in both resident and nonresident clinic settings are limited. Moreover, the literature describing strategies to integrate OMT into routine prenatal care visits in a resident clinic setting is scarce. The purpose of this study is to provide a real-world example of integrating OMT into routine prenatal care in a family medicine resident clinic setting. This will be done by identifying barriers and developing solutions that allow for successful integration of OMT.
Clinical summary
Over the course of an academic year, one family medicine resident provided prenatal care in a family medicine resident clinic. During the review of systems portion of the encounter, patients were asked about new or worsening pain. If patients reported pain, that was deemed MSK, then treatment options such as OMT, physical therapy, massage, chiropractic, acetaminophen, exercise, or pool therapy were offered. If patients expressed interest in OMT, then complaint-specific OMT was performed immediately after routine prenatal care was completed. Verbal consent was obtained prior to performing OMT. Treatment occurred in the same examination room that the patient had prenatal care completed on that day. The duration of OMT typically lasted 5–15 min and was dependent on MSK complaints, the modalities utilized, and time available after completing prenatal care.
This clinic was staffed by first-year family medicine residents one-half day per week for prenatal care and postpartum visits only. The supervising physicians for the clinic were family medicine physicians with obstetrics as part of their individual practice. The appointment duration was 30 min. The supervising physicians for the clinic were MDs without OMT-specific training. The family medicine residency in the study does not have osteopathic recognition. The clinic did not have permanent or portable OMT or massage tables available throughout the course of the year.
The data were recorded by the treating physician prior to the clinic visits, during the clinic visits, and upon reflection on the clinic visits throughout the study period. These qualitative data were obtained by reviewing clinic layout, treating patients, and interacting with colleagues. Most data were collected by reviewing what made integrating OMT challenging after clinic encounters. This process continued with each prenatal visit in which OMT was performed. As barriers to integrating OMT were identified, strategies to allow OMT to be performed were developed and noted. This occurred both in real time during patient encounters, by mentally working through mock scenarios before appointments, and by reflecting on encounters after they had occurred. Because this was a qualitative clinical practice study, no statistical analysis was performed.
In one academic year, one resident provided prenatal care for 16 patients. The age range of patients at first visit in which OMT was performed was 29–36 years of age, with the median age of 33 years old (Table 3). Of 16 unique patients seen, 10 patients reported MSK pain during at least one visit. Five of the 10 patients who reported MSK pain expressed interest in OMT and received treatments. All patients who expressed interest in OMT were able to receive treatment during their prenatal appointment that day.
The MSK complaints reported requiring OMT included LBP, leg pain, hip pain, neck pain, and pain of the chest wall, listed in descending frequency. The techniques utilized included myofascial release, counterstrain, muscle energy, and the indirect technique, listed in descending frequency. The patient’s MSK complaint, the OMT performed, and the treatment response were all included in the clinic progress note for that day. A standardized pain scale was not utilized; rather, we made note in the patient report of if or how OMT impacted pain along with an objective assessment of somatic dysfunction before and after treatment. These data were included in the progress note instead of an outside database to avoid creating a barrier to accessing information for clinicians. Documentation of OMT in the progress notes also served as a resource for future visits to see what treatments, if any, impacted MSK pain.
We identified three global areas in which barriers to integrating OMT were present clinic setup and logistics, supervising physician awareness of OMT in pregnancy, and treating physician knowledge of OMT in pregnancy.
Barriers: clinic environment and logistics
All prenatal appointments were 30 min in duration. The length of the appointment was a prominent barrier to integrating OMT due to the required aspects of prenatal care visits and the characteristics of a resident clinic. The amount of time available for OMT was most dependent on patient comorbidities, specific complaints on that clinic day, and if an interpreter was utilized during the clinic visit. For instance, visits where additional lab work, imaging, or medication management took place left less time for OMT. Examples include managing gestational diabetes, chronic or gestational hypertension, and incongruence between fundal height and gestational age that required imaging. Chronic conditions or pregnancy-related maladies were always of higher priority than MSK pain.
A challenge unique to resident clinics was being mindful of the time required to present each patient to the supervising physician before each visit was complete. This typically took 2–5 min per patient. Another resident-specific barrier was experience providing prenatal care. Prenatal care visits in the resident clinic were longer to allow more time with patients and for resident education.
The setup of the examination rooms, the type of examination table, and the lack of OMT tables in the clinic served as barriers to integrating OMT (Figure 1). Like many clinics, none of the examination rooms in our clinic had OMT, massage, or portable OMT tables. Our examination tables did not have a height adjustment, and the head of each table was in the corner of the room preventing the clinician from being able to stand at the head of the bed or behind the patient. Unfortunately, the examination tables were not able to be moved due to size and weight. Examination table type and location made it difficult to screen and treat the cervical and thoracic spine.
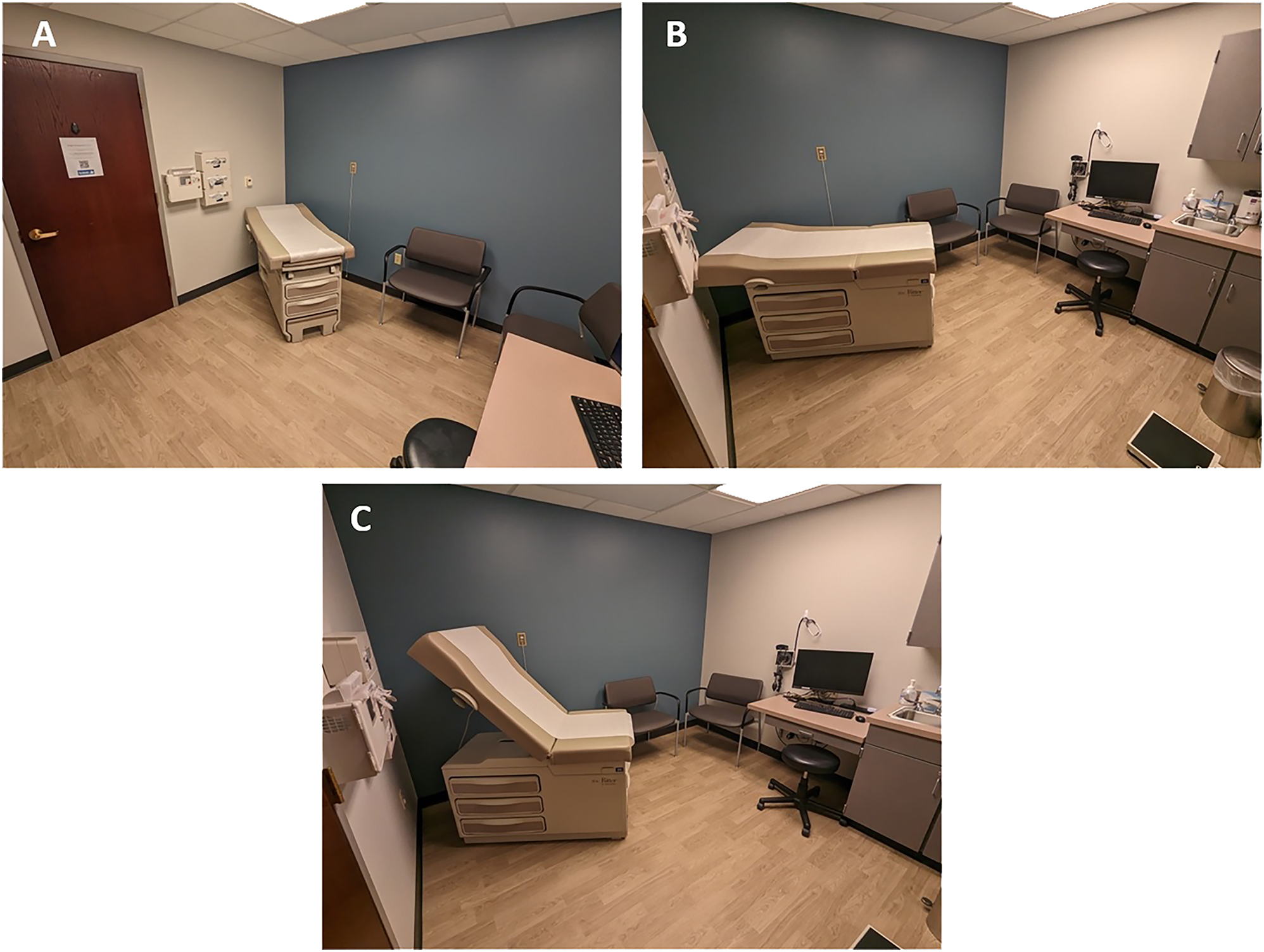
(A–C) images of the examination table and room layout taken from different angles.
The last clinic environment barrier was suboptimal awareness of OMT by patients, nursing staff, and support staff. The overall awareness of OMT and osteopathic medicine by patients and clinic medical staff seemed less in comparison to previous states in which the resident performing OMT had trained (Missouri, Michigan). This was not quantified during clinic visits; rather, it was noted throughout the course of 1 year when offering and discussing OMT with patients and clinic staff. Notably, all other first-year residents and supervising physicians in the clinic were aware of OMT and its utility in pregnancy.
Barriers: supervising physician awareness of OMT in pregnancy
Because OMT is a procedure, resident physicians must have an attending physician present or readily available in clinic when performing OMT. Attending physician knowledge and comfort with OMT may impact the ability of residents to offer OMT. Our clinic attendings did not perform OMT in pregnancy but were aware of OMT and its benefits. Prior to utilizing OMT, it was necessary to review with the supervising physician the evidence describing the efficacy of OMT, its safety, modalities to avoid, and the contraindications of OMT in pregnancy. These discussions also included which modalities would be utilized and avoided when treating patients. If OMT was performed, the MSK complaint, the OMT modalities utilized, and the treatment response were included in the patient presentation to the attending physician.
Barriers: treating physician knowledge of OMT in pregnancy
Another barrier we identified was the treating physicians’ clinical experience performing OMT in pregnancy and the recall of OMT in pregnancy. This included having less experience modifying treatment based on equipment in the room (i.e., immovable examination table, poorly placed table for OMT). The treating resident had far more experience treating nonpregnant compared to pregnant adults due to clinical training and makeup of traditional family medicine practice.
Second, the treating resident had a general sense of evidence supporting OMT in pregnancy, the modalities contraindicated, and the techniques to alter OMT in pregnancy. However, a review of each of these areas was needed prior to performing OMT in pregnancy and discussing it with the attending physician. We were not able to identify a succinct resource that contained contraindications to OMT in pregnancy, modalities to avoid, patient positions to avoid, and examples of altering treatments in pregnancy. We searched for literature describing integrating OMT into routine clinic visits or prenatal care visits, although the data were limited. The lack of a succinct resource for OMT in pregnancy, specifically one that can be readily accessible via smartphone or laptop, served as a barrier, especially early on in the study period.
Discussion
This study sought to determine how to successfully integrate OMT into routine prenatal care visits in a family medicine resident, nonspecialty clinic. Integrating OMT into routine prenatal care visits can provide patients with both additional treatment options and potential relief from MSK pain. Many geographic regions may lack OMT specialty clinics. Moreover, OMT-only appointments may introduce financial and logistic challenges that disproportionately impact pregnant patients in marginalized communities [17], [18], [19], [20]. In addition, the resident clinic setting poses additional barriers.
Integrating OMT during prenatal care visits can be challenging if physicians have not seen this modeled by colleagues or are not in a clinic setting in which OMT is commonly performed. Even if the clinicians at your practice do not perform OMT, osteopathic residents can find confidence by reflecting on our medical school training. Osteopathic medical students receive 200 h of learning and application of osteopathic manipulative medicine (OMM) during years one and two of medical school [21]. This is in comparison to many continuing medical education courses that are a few days in duration.
Barriers to integrating OMT and strategies to overcome said barriers were grouped in the following framework: clinic environment and logistics, attending awareness of OMT, and treating physician knowledge of OMT in pregnancy.
Solutions: clinic environment and logistics
Clinic appointment duration was the most notable barrier to integrating OMT in pregnancy. A previous study regarding the use of OMT in the resident clinic setting also noted time as the most significant reason that residents were not able to perform OMT [22]. Routine prenatal care always took precedence over MSK complaints along with any conditions we were managing. In addition, integrating OMT was difficult if an interpreter was required. These barriers simply left less time to perform OMT if MSK complaints were present. The variability in time allotted for OMT prevented us from implementing a protocolized treatment approach such as screening all body areas of each patient with MSK complaints and treating noted somatic dysfunctions. Appointment duration barriers were overcome by performing complaint-specific OMT, thinking through how treatments would need to be altered in the clinic space, and for pregnancy prior to clinic visits.
The next notable barrier was the exam room layout and equipment. This challenge by familiarizing self with clinic space prior to patients being present. We thought through which treatments would need to be altered based on our space, and such treatments included diagnosis and treatment of the cranium, cervical spine, thoracic inlet, and upper thoracic spine (Table 4). We were unable to assess cranial motion in our space. We had patients hang their legs off the side of the table while sitting upright to screen the axial spine. For diagnosis and treatment of the cervical spine, thoracic spine, and thoracic inlet, we either elevated the head of examination table or had the patient sit in a chair. We did not have a portable OMT table available in the clinic; however, a portable table could eliminate many of the challenges associated with standard examination tables and those that are poorly placed.
Barriers posed by the clinic room layout, equipment, and appointment duration were best remedied by reviewing the clinic space before patient arrival, visualizing how techniques would be altered in given space, and performing complaint-specific OMT.
The last barrier noted from a clinic environment standpoint was the limited awareness of OMT by patients and clinic staff. This was likely due to the resident clinic being located in South Dakota. There are no osteopathic medical schools in South Dakota, and only one of the six states bordering South Dakota has an osteopathic medical school [23]. The 2022 Osteopathic Medical Profession report includes total DOs in practice by state. Only 0.2 % of all DOs in America practice in South Dakota [24]. The number of osteopathic physicians in South Dakota likely impacts the awareness of OMT.
Improving awareness of OMT for patients and clinic staff was done during and between appointment times, often by answering questions posed by patients or staff. Patient and clinic staff knowledge of OMT may be further improved by having materials available in the waiting room and examination rooms as well as the clinic staff work areas describing osteopathic medicine. These resources could include purchasing brochures created by AOA that describe OMT and what a DO is. A free option includes printing resources from osteopathic.org (findado.osteopathic.org/faqs). This site has individual webpages with brief lay-person descriptions of: what is a DO, what is osteopathic medicine, and OMT. Finally, resident-or faculty-led lectures to the clinicians and clinic stuff would improve awareness of OMT. We were not able to include printed-out resources or lectures to clinic staff during the study period.
Solutions: supervising physician awareness of OMT in pregnancy
Supervising physician familiarity with OMT may impact integration of OMT in prenatal care. Prior to utilizing OMT, resident physicians must ensure that attending physicians are aware of what OMT is, its proven safety, evidence for treatment of MSK pain in pregnancy, and which modalities we intend to utilize. This sounds like a challenging task; however, most osteopathic physicians will merely need to review OMT resources. From a safety and efficacy standpoint, numerous studies have demonstrated both the safety and benefit of OMT in pregnancy such as King et al. [25] with 321 participants, Licciardone et al. [8] with 144 women, and the PROMOTE study with 400 pregnant women [26].
Finding resources to review for OMT in pregnancy was challenging, especially in the clinic environment where textbooks or notes from medical school were not readily available. Overall, it was difficult to find literature, PowerPoint slides, or online textbooks that were succinct and readily available while having these discussions in the clinic.
We had conversations about OMT with attending physicians prior to patients being in a room and ready to be seen. This allowed time for supervising physicians to ask questions, clarify, and have a good understanding of what OMT in prenatal care looks like. Tables 1 –4 review contraindications, modalities to avoid, and strategies to integrate OMT. These tables were created to serve as a concise tool to review OMT in pregnancy. We viewed questions or uncertainty about OMT by colleagues as opportunities to develop rapport and educate. We improved supervising physician awareness of OMT in pregnancy and developed a rapport by discussing literature regarding OMT in pregnancy and reviewing OMT resources from medical school.
Contraindications to OMT in pregnancy.
|
-
OMT, osteopathic manipulative treatment; DVT, deep vein thrombosis.
OMT modalities contraindicated in pregnancy.
|
-
CV4, compression of the fourth ventricle; HVLA, high-velocity low-amplitude; OMT, osteopathic manipulative treatment.
Overview of the patient population, somatic complaint, and OMT modality utilized.
| Patient identifier | Age, yearsa | No. of prenatal visits with OMT performed | MSK complaint | Modality utilized | Patient report of pain after OMT |
|---|---|---|---|---|---|
| 1 | 36 | 3 | Headache, LBP | MR, C | Improvement in headache and back pain at each visit |
| 2 | 32 | 2 | LBP, buttock, calf | MR, C, ME | Improvement in pain, all areas for both visits |
| 3 | 29 | 2 | LBP, left leg, right rib | MR, C, Ind | Improvement rib pain visit one, improved leg pain with no change in back pain visit two |
| 4 | 33 | 1 | Right leg, right hip | C, Ind | Improvement in pain in both regions |
| 5 | 35 | 1 | LBP | MR, C | Improvement in pain |
-
C, counterstrain; Ind, indirect; LBP, low back pain; ME, muscle energy; MR, myofascial release; MSK, musculoskeletal; OMT, osteopathic manipulative treatment; SD, somatic dysfunction. aPatient age at first OMT visit.
Challenges and solutions to integrating OMT during prenatal care visits.
| Clinic setup | |
|
|
|
| Duration of prenatal appointments | Perform complaint-focused OMT vs. standardized OMT protocol |
| Examination table not movable or poorly located in room | Familiarize self with room setup and examination tables, and identify ways to modify techniques |
|
|
|
| Supervising physician knowledge of OMT in pregnancy | |
|
|
|
| Attending experience with OMT | Review evidence for OMT in pregnancy, contraindications, and techniques intended to utilize |
|
|
|
| Treating physician knowledge of OMT in pregnancy | |
|
|
|
| Contraindicated modalities | CV-4, HVLA (see Table 1) |
| Contraindications to OMT in pregnancy | Typically, maladies that pregnant patients need to be sent to OB triage or hospitalized for (preterm labor, hypertensive disorder of pregnancy) |
| Altering techniques in pregnancy | Visualize performing OMT for low back, pelvic pain in examination rooms that will be utilized Avoid treating patients in the supine position during third trimester |
-
CV-4, compression of fourth ventricle; HVLA, high velocity low amplitude; OB, obstetrician; OMT, osteopathic manipulative treatment.
Solutions: treating physician knowledge of OMT in pregnancy
Resident physicians and medical students may have fewer total encounters treating pregnant patients due to the makeup of the family medicine panel, medical school training, or clinical rotation site. Luckily, the palpatory skills, screening techniques, and knowledge of various OMT modalities do not suddenly become useless if a patient is pregnant. Just like performing OMT on patients in hospital beds, pregnancy presents itself as a similar and equally doable challenge.
The resident performing OMT initially noted challenges with immediate recall of OMT in pregnancy. Before the first day in the obstetric clinic, the treating physician reviewed contraindications to OMT in pregnancy, modalities to avoid, and studies of OMT in pregnancy. We also thought through ways in which OMT would need to be altered to reflect the patient’s MSK complaint, examination room setup, and pregnancy (i.e., avoiding supine techniques in the third trimester). The vast majority of OMT in pregnancy content review occurred within the first month of beginning the resident obstetric clinic. Not having certainty of which modalities and positions to avoid, along with how techniques should be altered, can reduce resident physician confidence or create anxiety surrounding OMT in pregnancy. The treating resident utilized lectures and personal notes from medical school, the Foundations of Osteopathic Medicine textbook, and PowerPoint slides available online by osteopathic physicians. Tables 1 and 2 were created to allow for concise review of contraindications to OMT in pregnancy and what modalities to avoid [10, 13, 14]. Technical treatment tips include avoiding the supine posture during the third trimester, the use of a wedge or raising the head of the table during the third trimester, and utilizing the lateral recumbent position.
Next, we reviewed our clinic space to determine if any treatments would need to be altered or would not be feasible. Once our clinic space was reviewed, we visualized how OMT would be performed in our given space. Our confidence performing OMT in pregnancy was improved after reviewing evidence for contraindications and modalities to avoid. Our first few treatments were likely smoother because we reviewed our clinic space and visualized how we would perform OMT.
We recommend developing a succinct explanation of OMT for patients who have not heard of OMT previously. Finally, if patients have what seems like MSK pain, we recommend considering alternative diagnoses to avoid missing more serious maladies of pregnancy such as venous thromboembolism or symptoms of preeclampsia.
Limitations
Our study limitations relate to having one location and one resident physician providing OMT during prenatal care. Each clinic and residency training setting will have different examination room setups, clinic staff, and attendings with differing knowledge of OMT. The total number of patients seen was also limited by having one resident physician offering OMT.
Conclusions
We provide a real-world example of integrating OMT into routine prenatal care visits in a family medicine resident clinic setting. Challenges to integrating OMT were overcome by reviewing examination room equipment and layout, providing complaint-specific OMT and discussing OMT with the supervising physician. The remainder of the preparation included refreshing our memory of OMT in pregnancy from both an academic and a practical standpoint. We reviewed the current literature, contraindications to, and modalities to avoid regarding OMT in pregnancy. We also mentally worked through how treatments would be altered for pregnant patients in our clinic space.
Factors influencing integrating OMT in pregnancy that are unique to resident clinics include developing a rapport with the supervising physician before performing procedures, the ability to succinctly review OMT in pregnancy with the attending physician, and being able to perform prenatal care visits in an efficient manner to allow time for OMT if indicated. Creating a resident clinic environment in which OMT in pregnancy is accepted benefits residents as they develop their craft. More importantly, being able to integrate OMT into routine visits will benefit patients seen both during residency and throughout a physician’s career.
This study identified an opportunity for the AOA to support family medicine residents and residency programs who are trying to integrate OMT in clinical practice, especially those in training programs without osteopathic recognition. This support could include free online clinical resources and contact with DOs interested in mentoring residents who have questions about integrating OMT in clinical practice.
-
Research ethics: Deemed non-human research by Sanford IRB.
-
Author contributions: All authors provided substantial contribution to conception and design, acquisition of data, or analysis and interpretation of data; all authors drafted the article or revised it critically for important intellectual content; all authors contributed to review of data; all authors gave final approval of version of article to be published; all authors agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy and integrity of any part of the work are appropriately investigated and resolved.
-
Competing interests: None reported.
-
Research funding: None reported.
References
1. Sabino, J, Grauer, JN. Pregnancy and low back pain. Curr Rev Musculoskelet Med 2008;1:137–41. https://doi.org/10.1007/s12178-008-9021-8.Suche in Google Scholar PubMed PubMed Central
2. Wang, SM, Dezinno, P, Maranets, I, Berman, MR, Caldwell-Andrews, AA, Kain, ZN. Low back pain during pregnancy: prevalence, risk factors, and outcomes. Obstet Gynecol 2004;104:65–70. https://doi.org/10.1097/01.AOG.0000129403.54061.0e.Suche in Google Scholar PubMed
3. Pennick, V, Liddle, SD. Interventions for preventing and treating pelvic and back pain in pregnancy. Cochrane Database Syst Rev 2013;8:10. https://doi.org/10.1002/14651858.CD001139.PUB3.Suche in Google Scholar
4. Katonis, P, Kampouroglou, A, Aggelopoulos, A, Kakavelakis, K, Lykoudis, S, Makrigiannakis, A, et al.. Pregnancy-related low back pain. Hippokratia 2011;15:205–10.Suche in Google Scholar
5. Lavelle, JM. Osteopathic manipulative treatment in pregnant women. J Am Osteopath Assoc 2012;112:343–6. https://doi.org/10.7556/jaoa.2012.112.6.343.Suche in Google Scholar PubMed
6. Licciardone, JC, Aryal, S. Prevention of progressive back-specific dysfunction during pregnancy: an assessment of osteopathic manual treatment based on cochrane back review group criteria. J Osteopath Med 2013;113:728–36. https://doi.org/10.7556/jaoa.2013.043.Suche in Google Scholar PubMed
7. McIntyre, IN, Broadhurst, NA. Effective treatment of low back pain in pregnancy. Aust Fam Physician 1996;25:S65–7.Suche in Google Scholar
8. Licciardone, JC, Buchanan, S, Hensel, KL, King, HH, Fulda, KG, Stoll, ST. Osteopathic manipulative treatment of back pain and related symptoms during pregnancy: a randomized controlled trial. Am J Obstet Gynecol 2010;202:43.e1–8. https://doi.org/10.1016/j.ajog.2009.07.057.Suche in Google Scholar PubMed PubMed Central
9. Daly, J, Frame, P, Rapoza, P. Sacroiliac subluxation: a common, treatable cause of low-back pain in pregnancy. Fam Pract Res J 1991;11:149–59.Suche in Google Scholar
10. Tettambel, M. Foundations of osteopathic medicine, 3rd ed. Chila, A, editor. Philadelphia: Lippincott & WIlkins; 2018.Suche in Google Scholar
11. Gitlin, RWD, Wolf, DL. Uterine contractions following osteopathic cranial manipulation-a pilot study. J Am Osteopath Assoc 1992;92:1183.Suche in Google Scholar
12. Hensel, KL, Roane, BM. Does compression of the fourth ventricle cause preterm labor? Analysis of data from the PROMOTE study. J Am Osteopath Assoc 2019;119:668–72. https://doi.org/10.7556/JAOA.2019.114/MACHINEREADABLECITATION/RIS.Suche in Google Scholar
13. Kristiansson, P, Svärdsudd, K, von Schoultz, B. Serum relaxin, symphyseal pain, and back pain during pregnancy. Am J Obstet Gynecol 1996;175:1342–7. https://doi.org/10.1016/s0002-9378(96)70052-2.Suche in Google Scholar PubMed
14. Schmitz, A, Lutterbey, G, Von Engelhardt, L, Von Falkenhausen, M, Stoffel, M. Pathological cervical fracture after spinal manipulation in a pregnant patient. J Manip Physiol Ther 2005;28:633–6. https://doi.org/10.1016/j.jmpt.2005.08.017.Suche in Google Scholar PubMed
15. Lavelle, JM. Osteopathic manipulative treatment in pregnant women. J Am Osteopath Assoc 2012;112:343–6. https://doi.org/10.7556/JAOA.2012.112.6.343/MACHINEREADABLECITATION/RIS.Suche in Google Scholar
16. Hensel, KL, Roane, BM, Chaphekar, AV, Smith-Barbaro, P. PROMOTE study: safety of osteopathic manipulative treatment during the third trimester by labor and delivery outcomes. J Am Osteopath Assoc 2016;116:698–703. https://doi.org/10.7556/JAOA.2016.140/MACHINEREADABLECITATION/RIS.Suche in Google Scholar
17. Heaman, MI, Gupton, AL, Moffatt, MEK. Prevalence and predictors of inadequate prenatal care: a comparison of aboriginal and non-aboriginal women in manitoba. J Obstet Gynaecol Can 2005;27:237–48. https://doi.org/10.1016/S1701-2163(16)30516-3.Suche in Google Scholar PubMed
18. Heaman, MI, Sword, W, Elliott, L, Moffatt, M, Helewa, ME, Morris, H, et al.. Barriers and facilitators related to use of prenatal care by inner-city women: perceptions of health care providers. BMC Pregnancy Childbirth 2015;15:2. https://doi.org/10.1186/s12884-015-0431-5.Suche in Google Scholar PubMed PubMed Central
19. Fair, F, Raben, L, Watson, H, Vivilaki, V, van den Muijsenbergh, M, Soltani, H. Migrant women’s experiences of pregnancy, childbirth and maternity care in European countries: a systematic review. PLoS One 2020;15:e0228378. https://doi.org/10.1371/JOURNAL.PONE.0228378.Suche in Google Scholar
20. Phillippi, JC. Women’s perceptions of access to prenatal care in the United States: a literature review. J Midwifery Wom Health 2009;54:219–25. https://doi.org/10.1016/J.JMWH.2009.01.002.Suche in Google Scholar
21. Gevitz, N. The DOs: osteopathic medicine in America, 2nd ed. London: Johns Hopkins University Press; 2004.Suche in Google Scholar
22. Caldwell, G, Zeng, L, Kaufman, J, Bates, J. Osteopathic manipulative treatment use among family medicine residents in a teaching clinic. J Osteopath Med 2022;122:517–20. https://doi.org/10.1515/JOM-2022-0040.Suche in Google Scholar PubMed
23. Ruffini, N, D’Alessandro, G, Pimpinella, A, Galli, M, Galeotti, T, Cerritelli, F, et al.. The role of osteopathic care in gynaecology and obstetrics: an updated systematic review. Healthcare 2022;10:1566. https://doi.org/10.3390/healthcare10081566.Suche in Google Scholar PubMed PubMed Central
24. American Osteopathic Association. Osteopathic medical profession (OMP) report; 2022. https://osteopathic.org/wp-content/uploads/2022-AOA-OMP-Report.pdf [Accessed 1 Jun 2023].Suche in Google Scholar
25. King, HH, Tettambel, MA, Lockwood, MD, Johnson, KH, Arsenault, DA, Quist, R. Osteopathic manipulative treatment in prenatal care: a retrospective case control design study. J Am Osteopath Assoc 2003;103:577–82.Suche in Google Scholar
26. Hensel, KL, Roane, BM, Chaphekar, AV, Smith-Barbaro, P. PROMOTE study: safety of osteopathic manipulative treatment during the third trimester by labor and delivery outcomes background: few quality data exist on the safety of osteopathic manipulative. J Am Osteopath Assoc 2016;116:698–703.https://doi.org/10.7556/jaoa.2016.140.Suche in Google Scholar PubMed
© 2023 the author(s), published by De Gruyter, Berlin/Boston
This work is licensed under the Creative Commons Attribution 4.0 International License.
Artikel in diesem Heft
- Frontmatter
- Innovations
- Original Article
- Analysis of alternate material Onyx™ for total knee arthroplasty instrumentation sets
- Medical Education
- Original Article
- Impact of the USMLE Step 1 and COMLEX Level 1 transition to Pass/Fail on osteopathic medical student stress levels and board preparation
- Musculoskeletal Medicine and Pain
- Original Article
- Ultrasound-guided injection through the rotator cuff interval: a clinical perspective of one institution’s results and description of technique
- Neuromusculoskeletal Medicine (OMT)
- Clinical Practice
- Integrating osteopathic manipulative treatment into prenatal care visits in a family medicine resident clinic
- Public Health and Primary Care
- Original Article
- The effectiveness of disinfection protocols in osteopathic family medicine offices
- Clinical Image
- Lichen planus pigmentosus inversus: a rare clinical variant
- Abstracts
- 2023 AOA Research Abstracts and Student Poster Competition
Artikel in diesem Heft
- Frontmatter
- Innovations
- Original Article
- Analysis of alternate material Onyx™ for total knee arthroplasty instrumentation sets
- Medical Education
- Original Article
- Impact of the USMLE Step 1 and COMLEX Level 1 transition to Pass/Fail on osteopathic medical student stress levels and board preparation
- Musculoskeletal Medicine and Pain
- Original Article
- Ultrasound-guided injection through the rotator cuff interval: a clinical perspective of one institution’s results and description of technique
- Neuromusculoskeletal Medicine (OMT)
- Clinical Practice
- Integrating osteopathic manipulative treatment into prenatal care visits in a family medicine resident clinic
- Public Health and Primary Care
- Original Article
- The effectiveness of disinfection protocols in osteopathic family medicine offices
- Clinical Image
- Lichen planus pigmentosus inversus: a rare clinical variant
- Abstracts
- 2023 AOA Research Abstracts and Student Poster Competition