Pattern of smartphone use and its influence on psychosocial features among health professional course scholars: a cross-sectional study
-
Kuldeep Deka
 ,
T. N. V. Sai Lakshmi Pranathi
,
T. N. V. Sai Lakshmi Pranathi
 and
Shyam Krishnan
and
Shyam Krishnan

Abstract
Objectives
Patterns of smartphone use vary across ages; however, adolescents and young adults may be at particular risk, with more behavioral addictions and adverse health effects. This study explored the prevalence of smartphone addictions among health adolescent professional students and examined how problematic smartphone usage interferes with their level of physical activity as well as health-related quality of life.
Methods
A cross-sectional Analytical study based on self-perceived outcome measures such as the smartphone addiction scale-short version, the ‘International Physical Activity Questionnaire-short form’, and ‘Patient-Reported Outcomes Measurement Information System 29’-item profile was done with a sample of 400 participants.
Results
A total of 400 individuals (125 Males & 275 females) with mean age being 20.8 + 2.06 years recruited for the study. Smartphone addiction was most prevalent in dentistry students (43 %), followed by medicine (32 %) and allied health science (30.5 %), with no statistically significant differences in the addiction rate among the three programs. Compared with smartphone-addicted individuals, nonaddicted individuals had marginally greater physical function (mean difference =0.670, p<0.001), and those addicted to smartphones had significantly higher. anxiety (mean difference = 2.776, p<0.001), depression (mean difference =2.264, p< 0.001), and fatigue (mean difference =2.264, p<0.001). Physical activity was found to have no statistically significant difference between addicted and non-addicted individuals and except for sleep disturbance, none of the domains of PROMISE-29 showed any statistically significant correlation with physical activity.
Conclusions
The findings highlight the need for recommendation for setting a time limit for the usage of smartphones for formal and informal academic activities, as well as policy measures to promote normal smartphone use.
Introduction
Touchscreen technology and a multitude of applications in smartphones have pushed all human cohorts toward constructive and catastrophic traits. Smartphone usage pattern and the risk of developing an addiction varies across age groups, with some age groups exposed to a heightened risk of addiction than others [1]. There is evidence that adolescents and young adults may be at particular risk [2], [3], [4], [5], with a global prevalence rate of 10–67 % [2], 3], and in developing countries such as India itself, the figures range from 24.6 to 44 % [4], [5], [6], [7].
Behavioral addiction defined as “excessive, compulsive, uncontrolled use of one’s phone, leading to a psychological dependence upon the device (or the content on it)” considered a potential disorder and is commonly associated with smartphone usage [8], 9]. Moreover, recent evidence has revealed that excessive smartphone use is associated with many adverse health effects among adolescents with musculoskeletal disorders [10], 11], ophthalmologic disorders [11], 12], sleep difficulties [11], 13], psychopathologies, and psychiatric disorders [11], 14], 15]. In addition to these potentialities, smartphone use may facilitate learning or interfere with educational and professional lives among students [16], which depends entirely on its usage. On the other hand, evidence shows that many university students consider their smartphones a source of entertainment rather than a working instrument [16], 17].
With the benefit of mobile applications, students undergoing medical education prefer most readings through online textbooks (70 %), medical podcasts (60 %), medical calculators (75 %), online lectures (50 %), and note-taking [18]. Regulated usage of smartphones has definitive advantages in educational activities, as evidenced by the design of flexible M-learning modules implemented by various institutions [19]. Nevertheless, many adolescents develop physical and behavioral issues with their usage [18].
With due consideration to the above concerns, there is a need to understand the pattern of smartphone use and its effects on students of health professions. Understanding their technology usage may help prevent them from negatively impacting their health. Therefore, the purpose of this study was to explore the prevalence of smartphone addiction in this specific group of scholars currently pursuing health professional courses and to methodically examine how problematic smartphone usage interferes with their biopsychosocial factors.
The study primarily aimed to a) determine the prevalence of smartphone addiction among medical, dental, and allied health science university scholars and b) to assess how problematic smartphone usage interferes with their physical activity level and health-related quality of life.
Materials and methods
Ethical considerations
Ethical clearance was obtained from the Institutional Ethics Committee of the Kasturba Medical College, Mangalore, Manipal Academy of Higher Education, India (IEC KMC MLR 08/2024/529). All the procedures were conducted with strict adherence to the Declaration of Helsinki.
Study design and setting
A cross-sectional study was designed to recruit medical, dental, and allied health students who were screened for smartphone addiction, and the empirical association between smartphone addiction and variables like physical activity and health-related quality of life was analyzed. Subjects, 18 years and above of either gender pursuing above mentioned disciplines in an eminent medical education institute from the Dakshina Kannada district of Karnataka state in India were recruited. A non-probability sampling approach with a purposive sampling method using recruitment strategies such as online forums, social media, and physical notices at the college premises to attract participants from the medical, dental, and allied health courses was used. Following this, participant recruitment was carried out over a period spanning 1st September to 31st December 2024. The study was conducted in strict adherence to the STROBE guidelines for conduction and reporting of observational studies.
Sample size and selection criteria
Assuming the prevalence of unhealthy smartphone use among adolescents and young adults as 44 % (as reported by Davey S et al. 2014), the sample size for the current study was estimated to be 379 and approximated to 400 at a 95 % confidence interval using G-Power software. Eligibility criteria for inclusion were individuals aged 18 years and above of either gender with smartphone ownership who were pursuing medical, dental, or allied health science professional courses. Incomplete reporting of the self-reported questionnaire or reluctance to participate were grounds for exclusion.
Outcome measure
Smartphone addiction scale-short version (SAS-SV) [20], 21].
Self-reported measure for the evaluation of smartphone addiction severity. The SAS-SV is a 10-item questionnaire, and each item is scored from 1 (strongly disagree) to 6 (strongly agree), with the total score ranging from 10 to 60, with higher scores indicating more problematic smartphone use. Cut-off scores of 31 & 33 were considered as indicators of maladaptive smartphone use in males and females, respectively.
International Physical Activity Questionnaire-Short form (IPAQ-SF) [22], 23].
This self-reported measure assesses the intensity of physical activity and sitting time with open-ended questions surrounding individuals’ last 7-day recall of physical activity, with the item “During the last 7 days, on how many days did you perform vigorous physical activities such as heavy lifting, digging, aerobics, or fast bicycling?”. Final score is expressed as MET minutes for each activity which considers the Metabolic equivalent for each activity based on intensitry, duration each activity was performed and the number of times the activity was performed in a week. The MET minutes achieved in each category (walking, moderate, and vigorous activity) are summed to obtain the total MET minutes of physical activity a week.
Patient-Reported Outcomes Measurement Information System 29-item profile (PROMIS-29 v2.0) [24], 25].
A multi-dimensional outcome measure recording patient-reported severity of symptoms across multiple domains, like pain, pain interference, and fatigue.
Statistical analysis
Data analyses were performed via Jamovi version 2.3.24. Exploratory and descriptive statistics were derived from variables such as age, sex, smartphone addiction, level of physical activity, and domains of the PROMIS scale. A chi-square test was conducted to compare smartphone addiction among various academic programs and between males and females. A Mann‒Whitney U test was used to compare the domains of the PROMIS-29 scale and physical activities between addicted and non-addicted individuals. Associations between each PROMIS-29 scale domain and the IPAQ, Smartphone Addiction Scale-SV, and IPAQ were estimated via Spearman’s correlation coefficient. A p-value < 0.05 was considered statistically significant.
Results
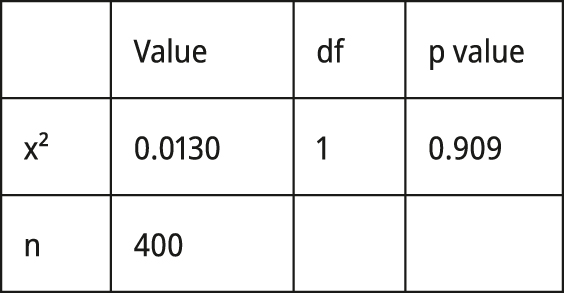
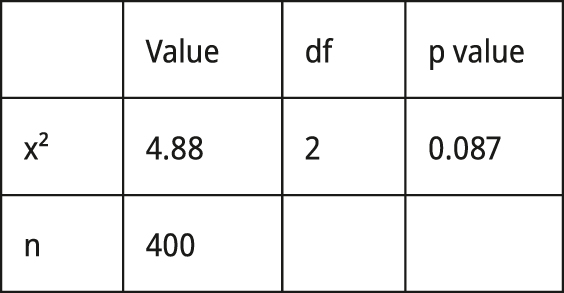
A total of 400 participants were recruited for the study through purposive sampling, of which 125 (31.25 %) were males and 275 (68.75 %) were females. The average age of the participants was 20.8±2.06 years. Among the total population recruited, 136 (34.0 %) were found to be addicted to smartphone usage. Among the categories of students based on their academic programs, the mean value of the smartphone addiction scale was 29.1±10.4, and addiction to smartphones was most prevalent among dentistry students (43 %), followed by medicine (32 %) and allied health science (30.5 %), as depicted in Table 1. Figure 1 illustrates the comparison of smartphone addiction and non-addiction between the medical, dental, and allied health students. Table 2 shows that there were no statistically significant differences in the addiction rates among the students in the three programs. The comparison of smartphone addiction revealed that it was marginally greater in females (34.2 %) than in males (33.6 %); however, these differences were not statistically significant. Figure 2 depicted the Differences in smartphone addiction among gender and course-wise.
Baseline characteristics of the studied participants.
| Variable | n, % | Mean±SD | Range | |
|---|---|---|---|---|
| Age | – | 20.8 ± 2.06 | 18–29 | |
| Gender | Male | 125 (31.25 %) | – | – |
| Female | 275 (68.75 %) | – | – | |
| Academic course | Medicine | 100 (25 %) | – | – |
| Dentistry | 100 (25 %) | – | – | |
| AHS | 200 (50 %) | – | – | |
| SAS-SV | – | 29.1 ± 10.4 | 10–60 | |
| IPAQ-SF | – | 3,956 ± 6,213 | 0.00–100985 |
-
n, number; %, percentage; Mean ± SD, Mean±standard deviation; Range, minimum–maximum value; AHS, Allied Health Science; SAS-SV, smartphone addiction-short version; IPAQ-SF, International Physical Activity Questionnaire-short form.
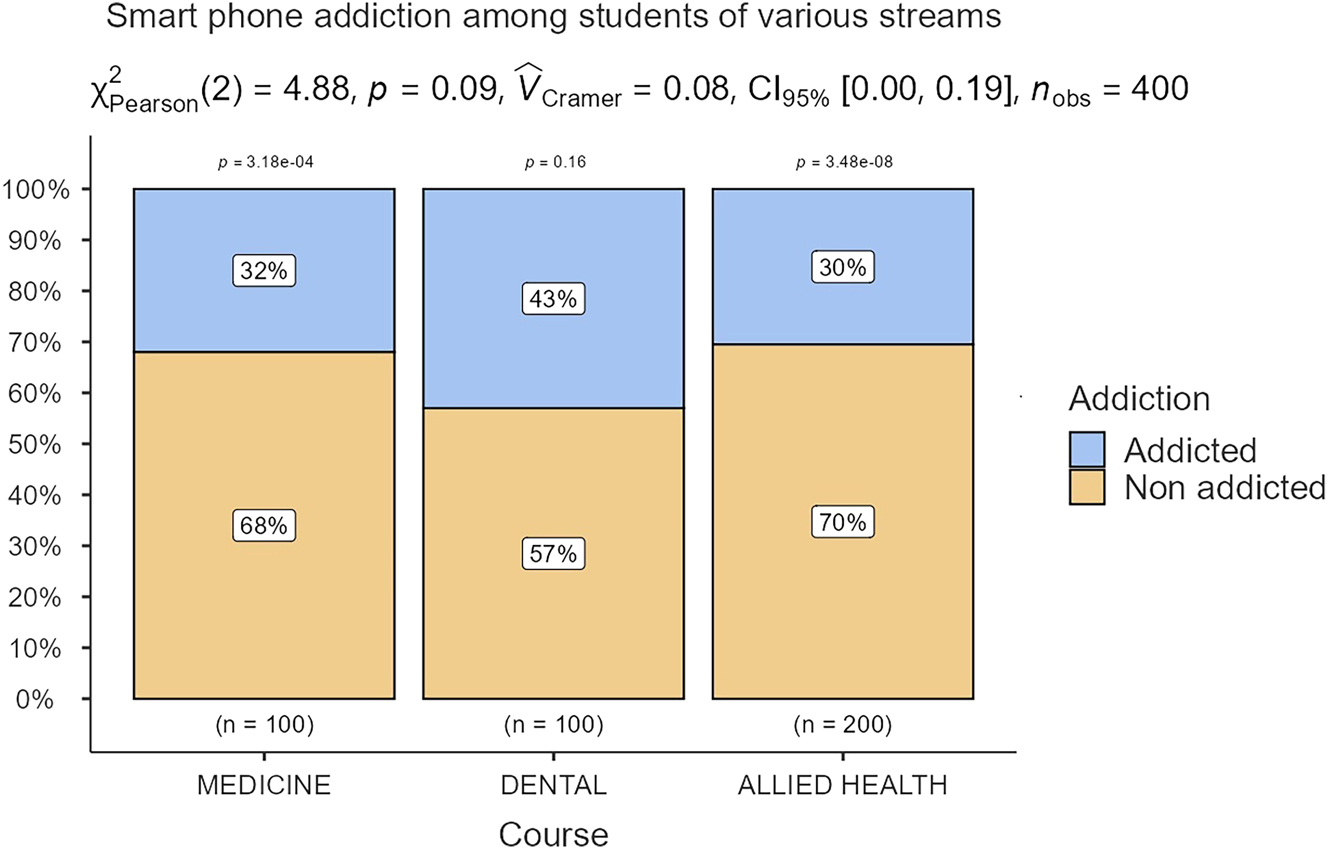
Comparison of smartphone addiction between medical, dental and allied health students.
Gender and course-wise observed values – smartphone usage.
|
Smartphone Usage
|
|
||||
|
Gender
|
|
Not addicted
|
Addicted
|
||
| Male | Observed | 83 | 42 | ||
| % within row | 66.4 % | 33.6 % | |||
| Female | Observed | 181 | 94 | ||
| % within row | 65.8 % | 34.2 % | |||
| Total | Observed | 264 | 136 | ||
|
|
% within row |
66.0 % |
34.0 % |
|
|
|
Course
|
|
||||
| Medicine | Observed | 68 | 32 |
|
|
| % within row | 68.0 % | 32.0 % | |||
| Dentistry | Observed | 57 | 43 | ||
| % within row | 57.0 % | 43.0 % | |||
| AHS | Observed | 139 | 61 | ||
| % within row | 69.5 % | 30.5 % | |||
| Total | Observed | 264 | 136 | ||
| % within row | 66.0 % | 34.0 % | |||
-
n, number; %, percentage; AHS, Allied Health Science; p-Value<0.05.
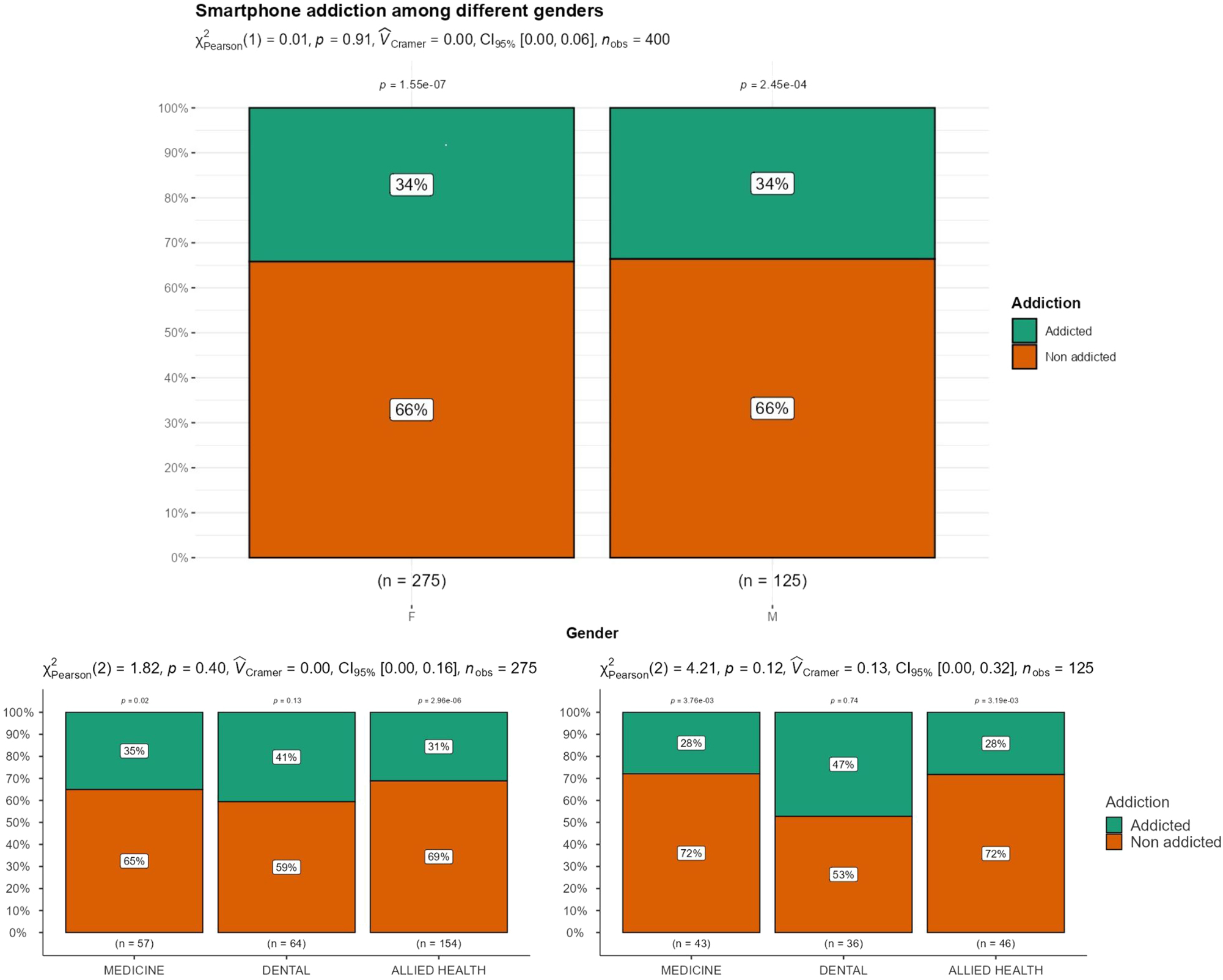
Difference in smartphone addiction among gender and course-wise.
Table 3 lists the descriptive statistics with the median and mean ± SD values of each domain of the PROMIS-29. When the domains of the PROMIS scale were compared among subjects with and without smartphone addiction, a statistically significant difference was found in all domains between addicted and non-addicted individuals. The scores for physical function were marginally higher in non-smartphone-addicted individuals than in smartphone-addicted individuals (mean difference=0.670, p<0.001). Subjects addicted to smartphones had significantly greater levels of anxiety (mean difference=2.776, p<0.001), depression (mean difference=2.264, p<0.001), and fatigue (mean difference=2.264, p<0.001). The ability to participate in social roles and activities was better among people with no smartphone addiction (mean difference=2.943, p<0.001) than among those who were addicted to smartphones. Pain interference was also found to be greater in people with smartphone addiction (mean difference=1.485, p<0.001) than in non-addicted individuals. The pain intensity was also significantly greater (mean difference=1.014, p<0.001), as depicted in Table 4.
Descriptive values of the PROMIS-29 domain.
| n | Mean ± SD | Median | SE | ||
|---|---|---|---|---|---|
| Physical function | Not addicted | 264 | 19.28 ± 1.54 | 20.00 | 0.0950 |
| Addicted | 136 | 18.61 ± 5.99 | 19.00 | 0.513 | |
| Anxiety | Not addicted | 264 | 7.88 ± 3.80 | 7.00 | 0.2341 |
| Addicted | 136 | 10.65 ± 4.14 | 11.00 | 0.355 | |
| Depression | Not addicted | 264 | 6.77 ± 3.86 | 5.00 | 0.2377 |
| Addicted | 136 | 9.39 ± 4.78 | 9.00 | 0.410 | |
| Fatigue | Not addicted | 264 | 8.52 ± 3.60 | 8.00 | 0.2215 |
| Addicted | 136 | 10.79 ± 3.74 | 10.00 | 0.321 | |
| Sleep disturbance | Not addicted | 264 | 9.03 ± 3.58 | 9.00 | 0.2205 |
| Addicted | 136 | 10.68 ± 3.57 | 11.00 | 0.306 | |
| Ability to participate in social roles and activities | Not addicted | 264 | 17.69 ± 2.78 | 19.00 | 0.1710 |
| Addicted | 136 | 14.75 ± 3.90 | 15.00 | 0.334 | |
| Pain interference | Not addicted | 264 | 6.13 ± 2.92 | 5.00 | 0.1797 |
| Addicted | 136 | 7.61 ± 3.86 | 6.00 | 0.331 | |
| Pain intensity | Not addicted | 264 | 1.76 ± 2.08 | 1.00 | 0.1279 |
| Addicted | 136 | 2.77 ± 2.46 | 2.00 | 0.211 |
-
n, number; Mean ± SD, Mean ± standard deviation; SE, Standard error; PROMIS-29, Patient-reported outcomes measurement information system-29.
Comparison of PROMIS-29 domains between smartphone-addicted and non-addicted subjects.
| Statistics | df | p-Value | Mean difference | SE difference | ||
|---|---|---|---|---|---|---|
| Physical function | STUDENT’S t | 1.71 | 398 | – | 0.670 | 0.391 |
| Mann‒Whitney U | 12,651 | <0.001 | – | – | ||
| Anxiety | STUDENT’S t | −6.70 | 398 | – | −2.776 | 0.414 |
| Mann‒Whitney U | 11,109 | <0.001 | – | – | ||
| Depression | STUDENT’S t | −5.93 | 398 | – | −2.625 | 0.443 |
| Mann‒Whitney U | 12,231 | <0.001 | – | – | ||
| Fatigue | STUDENT’S t | −5.88 | 398 | – | −2.624 | 0.385 |
| Mann‒Whitney U | 11,592 | <0.001 | – | – | ||
| Sleep disturbance | STUDENT’S t | −4.37 | 398 | – | −1.650 | 0.378 |
| Mann‒Whitney U | 13,039 | <0.001 | – | – | ||
| Ability to participate in social roles and activities | STUDENT’S t | 8.71 | 398 | – | 2.943 | 0.338 |
| Mann‒Whitney U | 9,841 | <0.001 | – | – | ||
| Pain interference | STUDENT’S t | −4.31 | 398 | – | −1.485 | 0.345 |
| Mann‒Whitney U | 14,384 | <0.001 | – | – | ||
| Pain intensity | STUDENT’S t | −4.34 | 398 | – | −1.014 | 0.234 |
| Mann‒Whitney U | 13,590 | <0.001 | – |
-
p-Value<0.05
A correlation analysis showed that there was no statistically significant association between Physical activity and any of the domains of PROMIS-29 (Table 5), except sleep disturbance, which showed a weak positive correlation (r=0.144, p<0.05). Physical function domain of PROMIS-29 was found to be significantly different amongst subjects addicted and not addicted to smartphones. A non-significant association was observed between the SAS-SV score and physical activity level. The relationship between smartphone addiction and physical activity is depicted in Figure 3.
Correlation analysis between physical activity level and PROMIS-29 domains and smartphone usage.
| IPAQ-SF | ||
|---|---|---|
| Physical function | Spearman’s rho | 0.052 |
| df | 398 | |
| p-Value | 0.298 | |
| Anxiety | Spearman’s rho | 0.066 |
| df | 398 | |
| p-Value | 0.187 | |
| Depression | Spearman’s rho | 0.084 |
| Df | 398 | |
| p-Value | 0.093 | |
| Fatigue | Spearman’s rho | 0.009 |
| df | 398 | |
| p-Value | 0.862 | |
| Sleep disturbances | Spearman’s rho | 0.144a |
| df | 398 | |
| p-Value | 0.004 | |
| Ability to participate in social roles and activities | Spearman’s rho | −0.069 |
| df | 398 | |
| p-Value | 0.171 | |
| Pain interference | Spearman’s rho | 0.035 |
| df | 398 | |
| p-Value | 0.489 | |
| Pain intensity | Spearman’s rho | 0.046 |
| Df | 398 | |
| p-Value | 0.357 | |
| SAS scale | Spearman’s rho | −0.019 |
| df | 398 | |
| p-Value | 0.709 |
-
p-Value<0.05; IPAQ-SF, International Physical Activity Questionnaire-Short Form.
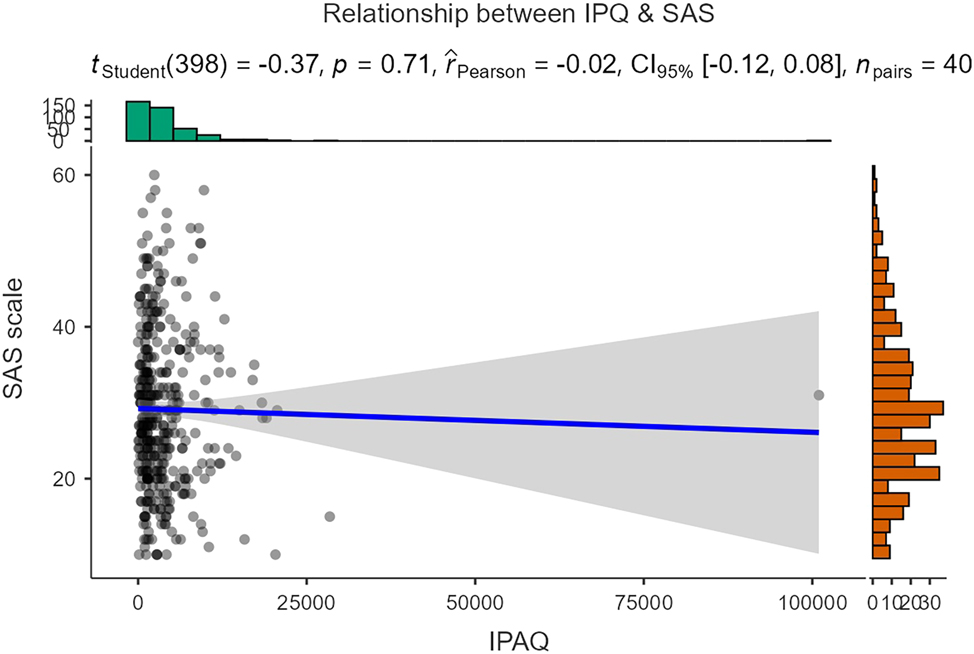
Relationship between smartphone addiction and physical activity.
Discussion
Adolescence is a vital period for physical and intellectual development [26], and in this population, technology-based m-learning encroaches on educational and academic conduct. Moreover, the effect of smartphone use on health varies depending on the basis of the nature and duration of its use. Therefore, the present study explored the prevalence of addiction to smartphone usage among university students in medical, dentistry, and allied health professional courses for whom the use of this technology is necessary for academic purposes. In addition, the study also tried to explore the association between problematic smartphone usage and physical activity levels as well as psychosocial functions of individuals.
The current study revealed that 34 % of the studied population (health professional course students) are addicted to smartphone usage, which is higher than the global prevalence (26.99 %) [27], and the same findings are in line with the range of university students’ problematic smartphone use in countries such as Malaysia (46.9 %) [28], Turkey (39.8 %) [29], China (29.8 %) [30] and Brazil (33.1 %) [31]. Moreover, recent studies where SAS-SV was used to determine the prevalence, addiction rate among adolescent medical students were found to be 39.7 % among Chinese students [32], 21.7 % in Serbia [33], 36 % in Saudi Arabia [34], and 30.2 % in Tunisia [35]. These facts and figures show no such wide variation in the prevalence rate when compared with our study’s addiction prevalence rate, but it’s quite alarming. This highlights that problematic smartphone usage is more of a behavioral addiction, and in the current scenario, smartphone addiction issues are turning more towards a global health concern.
In the present study, which categorized the academic programs of health professional courses, problematic smartphone use was more common among dentistry scholars (43 %), followed by medicine (32 %) and allied health science (30.5 %). Most importantly, higher education institutions have effectively supplemented traditional classroom teaching with emerging social media tools both within and outside the classroom, and more specifically in health professional courses; and their utilization for networking, clinical practice, and educational tasks is more need-based [36], [37], [38]. However, there are no set or standardized guidelines for the timeline or limits on its usage from academic or educational directions. Therefore, the period permissible for its usage as an academic conduit is not specified.
The data collected in our study revealed no significant sex differences in the prevalence of smartphone use. The addiction rate was marginally higher in females (34.2 %) than in males (33.6 %); however, these differences were not statistically significant. This aligns with the results of previous studies conducted in Iran [39], China [40], and Malaysia [41].
It is evident from the present study that the smartphone addiction of the studied population acts as a distraction and creates divergence in their attention from that of the primary tasks. These factors are well reflected in the statistical analysis of the PROMIS scale domains, where it was very clearly shown that students with addiction have greater anxiety, depression, fatigue, and pain interference and intensity. Additionally, a statistically significant difference was found in all the domains of the PROMIS-29 between the subjects with addiction and those without addiction to smartphones. Research has reported similar findings that addiction to smartphones among university students affects their physical and mental health, leading to sleep disorders, reduced academic performance, stress, depression, and weary social relationships [42], [43], [44], [45].
Smartphone addiction may negatively affect physical health by reducing the amount of physical activity [46]. In contrast, in our study, there was no significant statistical association between physical activity levels and domains of PROMIS-29 in the studied population. Except for the sleep disturbance domain (r=0.144, p=0.004), none of the other domains of PROMIS-29 showed any significant relationship with physical activity measured by IPAQ-SF. Similar findings were reported for physical activity and mobile phone addiction among adolescents and young adults aged 18–24 years in another study [47], 48]. Smartphone addiction and participation in physical activity are distinct behaviors, and associating them may be inappropriate without considering other influencing factors. However, studies showed that this behavioral phone addiction has a negative predictive effect on physical activity and a positive impact on social motivation [49]. Additionally, physical activity stimulates the pituitary gland to release endorphins and build up the ability of human dopamine signal transduction to promote positive emotions and replenish self-control [50], 51], which could be the most likely reason behind the lack of a statistical relationship between physical activity level and the Promis-29 domain in our study participants. Furthermore, theoretical frameworks such as the Bio-Psycho-Social model and the Use and Gratifications Theory offer insight into this phenomenon, and the Person-Affect-Cognition-Execution (I-PACE) model signals that smartphone addiction arises from the interplay of individual characteristics, cognitive-emotional processes, and executive function deficits [51].
The present study provides an in-depth view of the characterization of problematic smartphone users among health professional course scholars, for whom the application of smartphones mandates most of their academic activities. Additionally, this study’s analysis provides preparatory evidence for future studies and can be used for public health evaluation and policy-making purposes. Thus, there is an urgent demand for screening for behavioral addiction toward smartphones, evaluating the usage time of smartphones among adolescents and young adults across various academic courses, and most importantly, setting guidelines/recommendations concerning the time limit of their usage for scholarly activities.
However, the present study has several limitations. First, the study participants were exclusively from health professional courses, and the study area was a single center, which may have affected the generalizability of the findings. Incorporating adolescent participants from different and diverse geographical regions could have improved the external validity of the findings. Second, the application of self-reported outcome measures is subject to more subjective perceptions and biases. Third, the study did not address the influence of confounding factors such as the nature of smartphone use, academic performance, socioeconomic state, and other biopsychosocial factors that could impact the relationships observed in this study. Future studies should stress these variables and factors to obtain a clearer picture of the effects of problematic smartphone use on health behavior and quality of life.
Conclusions
The present study revealed a high prevalence of smartphone addiction among health professional adolescent students, with no statistically significant differences in the addiction rates among students in the three programs – medicine, dentistry, and allied health science. Those who are addicted to smartphones show high levels of anxiety, depression, fatigue, and pain interference. However, the current study failed to identify any statistically significant association between smartphone addiction and physical activity. These findings underscore the need for a set recommendation for setting a time limit for the usage of smartphones for both formal and informal academic activities, and to promote awareness of healthy digital habits. Longitudinal studies are required to understand problematic smartphone usage and its detrimental effects based on a biopsychosocial model of disability.
Acknowledgement
The authors would like to thank all our participants for their active support and contribution to the study.
-
Research ethics: The protocol was evaluated and approved by the Institutional Ethics Committee of Kasturba Medical College, Mangalore, India (IEC KMC MLR 08/2024/529).
-
Informed consent: Informed consent was obtained from all individuals included in this study, or their legal guardians or wards.
-
Author contributions: K.D., T.P.: Study conception and design; M.N., T.P., and S.K.: Methodology, data collection, data analysis, and interpretation; T.P., K.D., and S.K.: Writing, reviewing, and editing; M.N.,: Draft manuscript. All authors reviewed the results and approved the final version of the manuscript.
-
Use of Large Language Models, AI and Machine Learning Tools: None declared.
-
Conflict of interest: The author states no conflict of interest.
-
Research funding: None declared.
-
Data availability: Data is available on request from the authors.
References
1. Csibi, S, Griffiths, MD, Demetrovics, Z, Szabo, A. Analysis of problematic smartphone use across different age groups within the components model of addiction. Int J Ment Health Addiction 2021;19:616–31. https://doi.org/10.1007/s11469-019-00095-0.Search in Google Scholar
2. Sohn, SY, Rees, P, Wildridge, B, Kalk, NJ, Carter, B. Prevalence of problematic smartphone us-age and associated mental health outcomes amongst children and young people: a systematic review, meta-analysis and GRADE of the evidence. BMC Psychiatry 2019;19:356. https://doi.org/10.1186/s12888-019-2350-x.Search in Google Scholar PubMed PubMed Central
3. Candussi, CJ, Kabir, R, Sivasubramanian, M. Problematic smartphone usage, prevalence and patterns among university students: a systematic review. J Affect Disord 2023;14:100643. https://doi.org/10.1016/j.jadr.2023.100643.Search in Google Scholar
4. Gangadharan, N, Borle, AL, Basu, S. Mobile phone addiction as an emerging behavioral form of addiction among adolescents in India. Cureus 2022;14:e23798. https://doi.org/10.7759/cureus.2379.Search in Google Scholar PubMed PubMed Central
5. Das, P, Saraswathy, KN, Chaudhary, V. Prevalence of smartphone addiction and its relationship with obesity among young adults: a cross-sectional study from Delhi, India. Indian J Community Med 2024;49:544–8. https://doi.org/10.4103/ijcm.ijcm-288-23.Search in Google Scholar
6. Davey, S, Davey, A. Assessment of smartphone addiction in Indian adolescents: a mixed method study by systematic-review and meta-analysis approach. Int J Prev Med 2014;5:1500–11.Search in Google Scholar
7. Jain, P, Gedam, SR, Patil, PS. Study of smartphone addiction: prevalence, pattern of use, and personality dimensions among medical students from rural region of central India. Open J Psy-chiatry Allied Sci 2019;10:132–8. https://doi.org/10.5958/2394-2061.2019.00029.6.Search in Google Scholar
8. James, RJE, Dixon, G, Dragomir, MG, Thirlwell, E, Hitcham, L. Understanding the construction of ‘behavior’ in smartphone addiction: a scoping review. Addict Behav 2023;137:107503. https://doi.org/10.1016/j.addbeh.2022.107503.Search in Google Scholar PubMed
9. Kwon, M, Lee, JY, Won, WY, Park, JW, Min, JA, Hahn, C, et al.. Develop-ment and validation of a smartphone addiction scale (SAS). PLoS One 2013;8:e56936. https://doi.org/10.1371/journal.pone.0056936.10.Search in Google Scholar
10. Yang, SY, Chen, MD, Huang, YC, Lin, CY, Chang, JH. Association between smartphone use and musculoskeletal discomfort in adolescent students. J Community Health 2017;42:423–30. https://doi.org/10.1007/s10900-016-0271-x.Search in Google Scholar PubMed
11. Cha, JH, Choi, Y-J, Ryu, S, Moon, J-H. Association between smartphone usage and health out-comes of adolescents: a propensity analysis using the Korea youth risk behavior survey. PLoS One 2023;18:e0294553. https://doi.org/10.1371/journal.pone.0294553.Search in Google Scholar PubMed PubMed Central
12. Wang, J, Li, M, Zhu, D, Cao, Y. Smartphone overuse and visual impairment in children and young adults: systematic review and meta-analysis. J Med Internet Res 2020;22:e21923. https://doi.org/10.2196/21923.Search in Google Scholar PubMed PubMed Central
13. Baiden, P, Tadeo, SK, Peters, KE. The association between excessive screen-time behaviors and insufficient sleep among adolescents: findings from the 2017 youth risk behavior surveil-lance system. Psychiatry Res 2019;281:112586. https://doi.org/10.1016/j.psychres.2019.112586.Search in Google Scholar PubMed
14. Wang, C, Li, K, Kim, M, Lee, S, Seo, D-C. Association between psychological distress and el-evated use of electronic devices among US adolescents: results from the youth risk behavior surveillance 2009–2017. Addict Behav 2019;90:112–8. https://doi.org/10.1016/j.addbeh.2018.10.037.Search in Google Scholar PubMed
15. Yang, J, Fu, X, Liao, X, Li, Y. Association of problematic smartphone use with poor sleep quality, depression, and anxiety: a systematic review and meta-analysis. Psychiatry Res 2020;284:112686. https://doi.org/10.1016/j.psychres.2019.112686.Search in Google Scholar PubMed
16. Amez, S, Baert, S. Smartphone use and academic performance: a literature review. Int J Educ Res 2020;103:101618. https://doi.org/10.1016/j.ijer.2020.101618.Search in Google Scholar
17. Lepp, A, Barkley, JE, Sanders, GJ, Rebold, M, Gates, P. The relationship between cell phone use, physical and sedentary activity, and cardiorespiratory fitness in a sample of U.S. college students. Int J Behav Nutr Phys Activ 2013;10:79. https://doi.org/10.1186/1479-5868-10-79.Search in Google Scholar PubMed PubMed Central
18. Wallace, S, Clark, M, White, J. ‘It’s on my iPhone’: attitudes to the use of mobile computing devices in medical education, a mixed-methods study. BMJ Open 2012;2:e001099. https://doi.org/10.1136/bmjopen-2012-001099. [Internet].Search in Google Scholar PubMed PubMed Central
19. Singh, K, Sarkar, S, Gaur, U, Gupta, S, Adams, OP, Sa, B, et al.. Smartphones and educational apps use among medical students of a smart university campus. Front. Commun. 2021:649102. https://doi.org/10.3389/fcomm.2021.649102.Search in Google Scholar
20. Kwon, M, Kim, DJ, Cho, H, Yang, S. The smartphone addiction scale: development and validation of a short version for adolescents. PLoS One 2013;8:e83558. https://doi.org/10.1371/journal.pone.0083558.Search in Google Scholar PubMed PubMed Central
21. Yue, H, Yue, X, Liu, B, Li, X, Dong, Y, Bao, H. Short version of the smartphone addiction scale: measurement invariance across gender. PLoS One 2023;18:e0283256. https://doi.org/10.1371/journal.pone.0283256.Search in Google Scholar PubMed PubMed Central
22. Craig, CL, Marshall, AL, Sjöström, M, Bauman, AE, Booth, ML, Ainsworth, BE, et al.. International physical activity questionnaire: 12-country reliability and validity. Med Sci Sports Exerc 2003;35:1381–95. https://doi.org/10.1249/01.MSS.0000078924.61453.FB.Search in Google Scholar PubMed
23. Lee, PH, Macfarlane, DJ, Lam, TH, Stewart, SM. Validity of the international physical activi-ty questionnaire short form (IPAQ-SF): a systematic review. Int J Behav Nutr Phys Activ 2011;8:115. https://doi.org/10.1186/1479-5868-8-115.Search in Google Scholar PubMed PubMed Central
24. Hays, RD, Spritzer, KL, Schalet, BD, Cella, D. PROMIS®-29 v2.0 profile physical and mental health summary scores. Qual Life Res 2018;27:1885–91. https://doi.org/10.1007/s11136-018-1842-3.Search in Google Scholar PubMed PubMed Central
25. Cella, D, Gershon, R, Bass, M, Rothrock, N. Assessment center scoring ser-vice SM user manual v1 4. 2017. https://www.assessmentcenter.net/ac_scoringservice/templates/UserManual.pdf [Accessed August 2018].Search in Google Scholar
26. Yoon, M, Yun, H. Relationships between adolescent smartphone usage patterns, achievement goals, and academic achievement. Asia Pac Educ Rev 2023;24:13–23. https://doi.org/10.1007/s12564-021-09718-5.Search in Google Scholar
27. Meng, S-Q, Cheng, J-L, Li, Y-Y, Yang, X-Q, Zheng, J-W, Chang, X-W, et al.. Global prevalence of digital addiction in general population: a systematic review and meta-analysis. Clin Psychol Rev 2022;92:102128. https://doi.org/10.1016/j.cpr.2022.102128.Search in Google Scholar PubMed
28. Ching, SM, Yee, A, Ramachandran, V, Sazlly Lim, SM, Wan Sulaiman, WA, Foo, YL, et al.. Validation of a malay version of the smartphone addiction scale among medical students in Malaysia. PLoS One 2015;10:e0139337. https://doi.org/10.1371/journal.pone.0139337.Search in Google Scholar PubMed PubMed Central
29. Demirci, K, Akgonul, M, Akpinar, A. Relationship of smartphone use severity with sleep quality, depression, and anxiety in university students. J Behav Addict 2015;4:85–92. https://doi.org/10.1556/2006.4.2015.010.Search in Google Scholar PubMed PubMed Central
30. Chen, B, Liu, F, Ding, S, Ying, X, Wang, L, Wen, Y, et al.. Gender differences in factors associated with smartphone addiction: a cross-sectional study among medical college students. BMC Psychiatry 2017;17:341. https://doi.org/10.1186/s12888-017-1503-z.Search in Google Scholar PubMed PubMed Central
31. Mescollotto, FF, Castro, EM, Pelai, EB, Pertille, A, Bigaton, DR. Translation of the short ver-sion of the smartphone addiction scale into Brazilian Portuguese: cross-cultural adaptation and testing of measurement properties. Braz J Phys Ther 2019;23:250–6. https://doi.org/10.1016/j.bjpt.2018.08.013.Search in Google Scholar PubMed PubMed Central
32. Liu, H, Zhou, Z, Zhu, E, Huang, L, Zhang, M. Smartphone addiction and its associated factors among freshmen medical students in China: a cross-sectional study. BMC Psychiatry 2022;22:308. https://doi.org/10.1186/s12888-022-03957-5.Search in Google Scholar PubMed PubMed Central
33. Nikolic, A, Bukurov, B, Kocic, I, Vukovic, M, Ladjevic, N, Vrhovac, M, et al.. Smartphone addiction, sleep quality, depression, anxiety, and stress among medical students. Front Public Health 2023;11:1252371. https://doi.org/10.3389/fpubh.2023.1252371.Search in Google Scholar PubMed PubMed Central
34. Aftab, T, Khyzer, E. Smartphone addiction and its association with hypertension and quality of sleep among medical students of northern border university, arar, Saudi Arabia. Saudi Med J 2023;44:1013–19. https://doi.org/10.15537/smj.2023.44.10.20230402.Search in Google Scholar PubMed PubMed Central
35. Zemni, I, Bennasrallah, C, Kacem, M, Garrach, B, Dhouib, W, Ben Fredj, M, et al.. Smartphone addiction among medical students in the university of Monastir, Tunisia. Eur J Publ Health 2024;34. https://doi.org/10.1093/eurpub/ckae144.2266. ckae144.2266.Search in Google Scholar
36. Dzvapatsva, GP, Mitrovic, Z, Dietrich, AD. Use of social media platforms for improving academ-ic performance at further education and training colleges. SA J Inf Manag [Internet] 2010;16:1–7. https://doi.org/10.4102/sajim.v16i1.604. Available from: http://sajim.co.za/index.php/SAJIM/article/view/604.Search in Google Scholar
37. Blaschke, LM. Using social media to engage and develop the online learner in self-determined learning res learn. Tech 2014;22:21635. https://doi.org/10.3402/rlt.v22.21635.Search in Google Scholar
38. Latif, MZ, Hussain, I, Saeed, R, Qureshi, MA, Maqsood, U. Use of smart phones and social media in medical education: trends, advantages, challenges and barriers. Acta Inf Med 2019;27:133–8. https://doi.org/10.5455/aim.2019.27.133-138.Search in Google Scholar PubMed PubMed Central
39. Mokhtarinia, HR, Torkamani, MH, Farmani, O, Biglarian, A, Gabel, CP. Smartphone addiction in children: patterns of use and musculoskeletal discomfort during the COVID-19 pandemic in Iran. BMC Pediatr 2022;22:681. https://doi.org/10.1186/s12887-022-03748-7.Search in Google Scholar PubMed PubMed Central
40. Arora, A, Wong, WW, Yee, NS, Lee, RY, Soe, HHK. Smartphone usage and addiction among un-dergraduate dental students in Malaysia: a cross-sectional study. J Educ Health Promot 2022;11:110. https://doi.org/10.4103/jehp.jehp-858-21.Search in Google Scholar
41. Awasthi, S, Kaur, A, Solanki, HK, Pamei, G, Bhatt, M. Smartphone use and the quality of life of medical students in the kumaun region, Uttarakhand. J Fam Med Prim Care 2020;9:4252–8. https://doi.org/10.4103/jfmpc.jfmpc-805-20.Search in Google Scholar
42. Demirkan, AK. Exploring the relationship between smartphone addiction, quality of life, and personality traits in university students. Iran J Psychiatry 2024;19:210–20. https://doi.org/10.18502/ijps.v19i2.15107.Search in Google Scholar PubMed PubMed Central
43. Kim, SG, Park, J, Kim, HT, Pan, Z, Lee, Y, McIntyre, RS. The relationship between smartphone ad-diction and symptoms of depression, anxiety, and attention-deficit/hyperactivity in south Kore-an adolescents. Ann Gen Psychiatr 2019;18:1. https://doi.org/10.1186/s12991-019-0224-8.Search in Google Scholar PubMed PubMed Central
44. Seo, DG, Park, Y, Kim, MK, Park, J. Mobile phone dependency and its impacts on adolescents’ social and academic behaviors. Comput Hum Behav 2016;63:282–92. https://doi.org/10.1016/j.chb.2016.05.026.Search in Google Scholar
45. Kim, SE, Kim, JW, Jee, YS. Relationship between smartphone addiction and physical activity in Chinese international students in Korea. J Behav Addict 2015;4:200–5. https://doi.org/10.1556/2006.4.2015.028.Search in Google Scholar PubMed PubMed Central
46. Abbasi, GA, Jagaveeran, M, Goh, Y, Tariq, B. The impact of type of content use on smartphone addiction and academic performance: physical activity as moderator. Technol Soc 2021;64:101521. https://doi.org/10.1016/j.techsoc.2020.101521.Search in Google Scholar
47. Xiao, W, Wu, J, Yip, J, Shi, Q, Peng, L, Lei, QE, et al.. The relationship between physical activi-ty and mobile phone addiction among adolescents and young adults: systematic review and meta-analysis of observational studies. JMIR Public Health Surveill 2022;8:e41606. https://doi.org/10.2196/41606.Search in Google Scholar PubMed PubMed Central
48. Lin, B, Teo, EW, Yan, T. The impact of smartphone addiction on Chinese university students’ physical activity: exploring the role of motivation and self-efficacy. Psychol Res Behav Manag 2022;15:2273–90. https://doi.org/10.2147/PRBM.S375395.Search in Google Scholar PubMed PubMed Central
49. Zhang, Y. Study on the feasibility of sports prescription to treatment of young internet addiction. In: Advanced Technology in Teaching-Proceedings of the 2009 3rd International Conference on Teaching and Computational Science (WTCS 2009) Volume 1: Intelligent Ubiq-uitous Computing and Education. Berlin Heidelberg: Springer; 2012. p. 877–84.10.1007/978-3-642-11276-8_118Search in Google Scholar
50. Song, Y, Zhang, G, Liu, N, Zhang, Y, Zhai, J, Niu, X, et al.. Influence of physical activity on prob-lematic smartphone use in medical students: mediating effects of social anxiety and the moder-ating role of gender. Front Psychol 2024;15:1445847. https://doi.org/10.3389/fpsyg.2024.1445847.Search in Google Scholar PubMed PubMed Central
51. Chang, K, Li, X, Zhang, L, Zhang, H. A double-edged impact of social smartphone use on smartphone addiction: a parallel mediation model. Front Psychol 2022;13:808192. https://doi.org/10.3389/fpsyg.2022.808192.Search in Google Scholar PubMed PubMed Central
© 2025 the author(s), published by De Gruyter, Berlin/Boston
This work is licensed under the Creative Commons Attribution 4.0 International License.