Development of the low-cost, smartphone-based cardiac auscultation training manikin
-
Dominik Karch

 ,
Krzysztofa Kopyt
,
Krzysztofa Kopyt

Abstract
Objectives
Cardiac auscultation remains a crucial part of physical examination. In preclinical training, there are multiple approaches for teaching that skill. Our goal was to find a compromise between expensive and complicated high-fidelity simulators and simple devices with a lack of realism.
Methods
Our project is made up of three main parts: a manikin’s torso, a specially prepared stethoscope, and a smartphone application. The position of the stethoscope’s head is recognized by Hall effect sensors inside of a manikin, and the information is sent via Bluetooth to the smartphone. Data are interpreted by the application, and proper recording is selected from sounds’ base. The user can easily adjust additional settings (e.g., main volume, playback speed, background noises). Then, the processed sound is played via a Bluetooth headset that is a part of the stethoscope.
Results
The solution that we suggest is easy to use with minimal adversely affecting the quality of learning. Handling of our device is intuitive, and minimal prior training is required. The low cost of the device itself and the widespread use of smartphones make it easy to implement.
Conclusions
We believe that this solution could be a complement for the currently used methods for teaching cardiac auscultation in preclinical training.
Introduction
Knowledgeable cardiac auscultation remains one of the most important skills for the detection of heart diseases [1]. Teaching at the bedside remains a really effective method of teaching clinical skills; however, it has few limitations. The most frequently reported limitations are the following: the lack of patients with a variety of symptoms, a large student-to-patient ratio during classes, and inconvenience for the patient because of repeated examinations [2].
The solution to the aforementioned problem seemed to be simulation devices. Although high-fidelity and expensive clinical simulators are popular among procedure-related specialties such as emergency medicine or anesthesiology, there is still place for low-fidelity simulators such as heart sound simulators [3], [4].
Our goal was to create the cost-effective device that combines advantages of learning auscultation sounds from sound databases or from the Internet with an increased level of fidelity, which is offered by advanced simulators. We decided to create a project that uses as a central element computing capabilities and other possibilities offered by today’s smartphones.
Methods and results
The designed system consists of three main parts: a manikin’s torso, a specially prepared stethoscope, and a smartphone application. The position of the magnet in the stethoscope head is recognized by sensors inside of the manikin. Then, the information about which valve is currently auscultated is sent via Bluetooth to the smartphone, and the proper sound is played via Bluetooth headphones, which are a part of the stethoscope.
The complexity of the manikin itself is reduced to a minimum, it is only an input device that informs the smartphone about which valve is currently auscultated. The torso shell is based on a simple shop manikin but could be replaced by any other housing. Inside, in four typical points of heart valve auscultation, there are Hall effect switches. We decided to use Hall effect sensors instead of reed switches because of their ability to recognize which magnet pole is currently facing the manikin [5]. Owing to this Hall switches’ property, there is a possibility of potential for differentiating bell and diaphragm sounds. In addition, if we want to place other sensors on the back of the manikin (e.g. for lungs sounds), we can also exclude them from unintentional activation. The switches are responsible for locating the current position of the stethoscope head. Arduino Nano board based on the ATmega328 microcontroller and the HC-06 Bluetooth module are responsible for processing and sending data to the smartphone. All components were connected according to the schema (Figure 1).
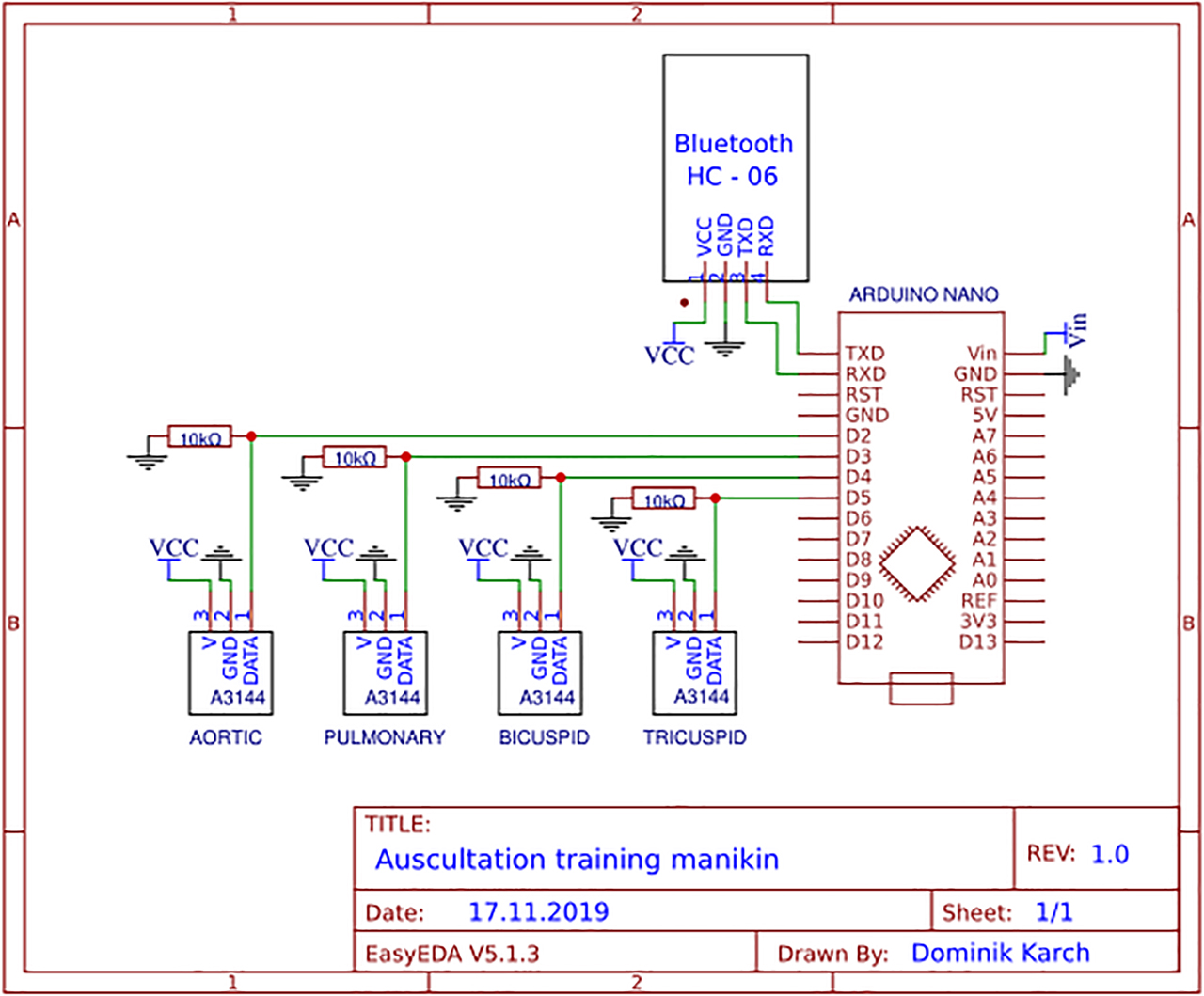
Circuit design.
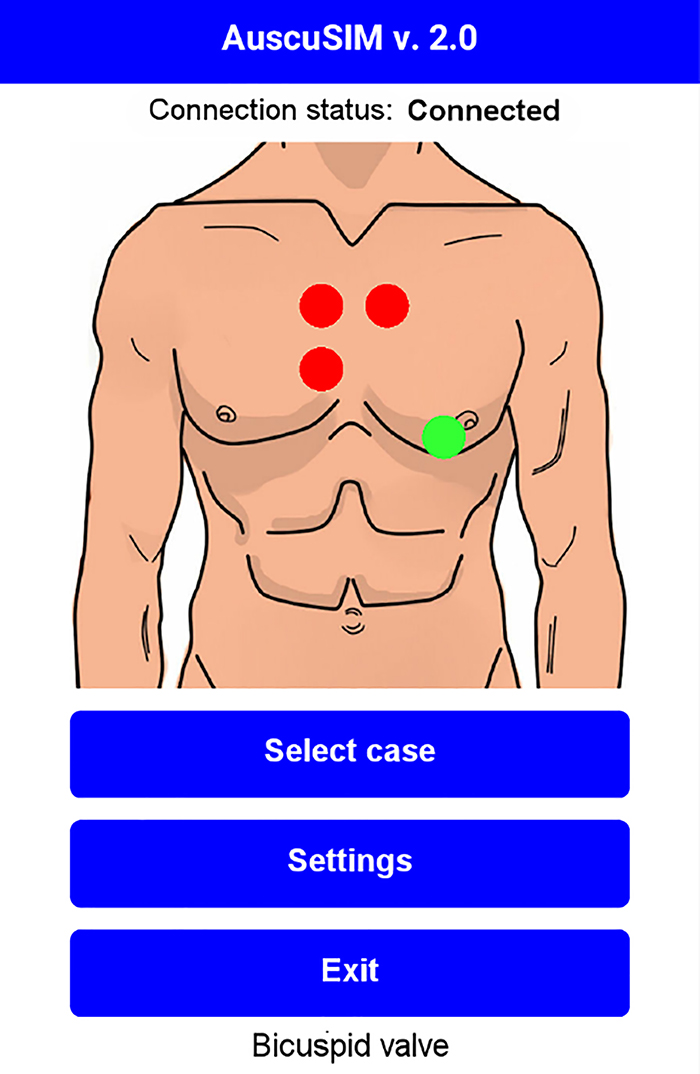
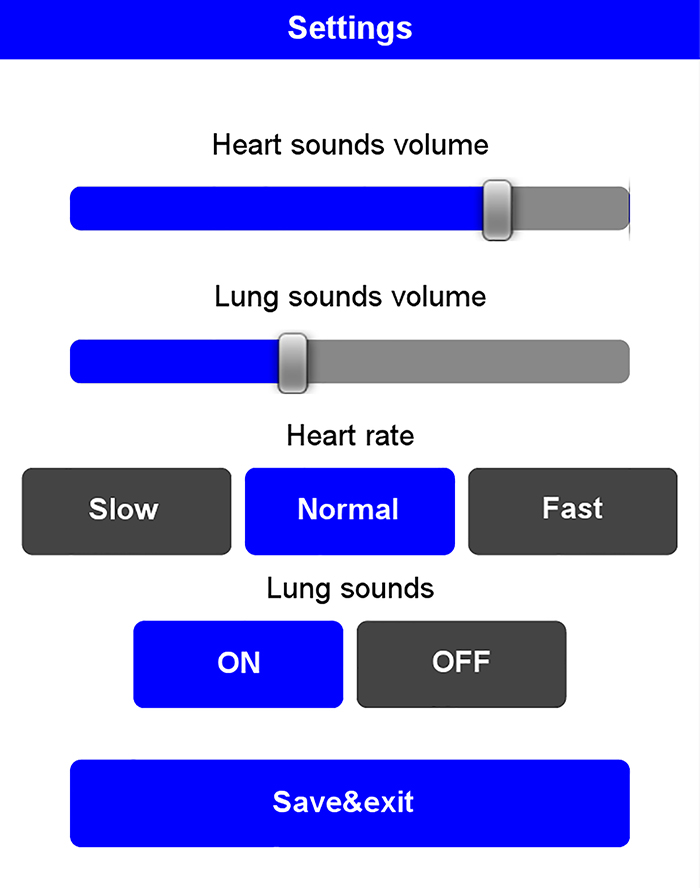
The smartphone application was created using drag and drop software called MIT App Inventor 2. We decided to simplify the application interface as much as possible to avoid difficulties in learning how to use the system. In the application, the user can choose a set of sounds that correspond to the given disorder. In addition, the user can turn on, turn off, or change the volume of background breathing sounds that are played to increase the difficulty and provide more realism. The student can also choose one of three levels of playback speed, depending on their experience (Figure 2A). During auscultation, a graphical representation of the currently auscultated valve is displayed on the smartphone screen (Figure 2B).
Application settings.
Main interface.
The stethoscope is the simplest element of the system. It consists of only two parts: a round neodymium magnet located in its head, which activates the proper sensors in the manikin’s body, and wireless Bluetooth headphones, through which the smartphone plays the appropriate sounds.
One of the main advantages of the system is the open base of auscultation sounds. In the application, there is an option to import own sound sets. Supported file formats are the following: .wav and .mp3. During our first tests, we have been using 3M™ Littmann® Electronic Stethoscope Model 3200 as a recording device.
Summary
In our project, we strove to make the whole system and the usage of application as simple as it is possibly without adversely affecting the quality of learning. Handling of our device is intuitive, and no prior training is required. It is important because the most commonly reported barrier in other research works in implementation of modern learning methods was the lack of time to learn how to use them [6]. The simplification of the system also allowed significant reduction in manufacturing and implementation costs. The cost of the parts needed to make a single simulator is less than 50 euros (without smartphones and wireless headphones).
Great opportunities for further development are connected with the fact that electronics do not have to be placed in the manikin’s torso shell. Electronics could be placed, for example, in specially prepared T-shirts for standardized patients. Friederichs et al. (2014) showed that the use of hybrid models was a superior teaching method than the use of auscultation manikins [7].
A key message from this project is that, in the technology world, it is worth looking for the most high-end solutions. The created prototype has of course its own limitations, such as requirement of precise placement of the stethoscope head on the manikin or the number of auscultatory points limited by the number of sensors. Despite this, we believe that our solution could be a valuable complement for the currently used methods for teaching the auscultation art, especially in preclinical training. Because the whole system is based on the smartphone application, the final result that we would like to achieve would be the community gathered around this project, which could share its own recordings that would be synchronized in real time with the application.
Research funding: None declared.
Author contributions: All the authors have accepted the responsibility for the entire content of this submitted manuscript and approved submission.
Competing interests: The funding organization(s) played no role in the study design; in the collection, analysis, and interpretation of data; in the writing of the report; or in the decision to submit the report for publication.
Informed consent: Informed consent was obtained from all individuals included in this study.
Ethical Approval: The conducted research is not related to either human or animal use.
References
1. Barrett, MJ, Mackie, AS, Finley, JP. Cardiac auscultation in the modern era: premature requiem or phoenix rising?. Cardiol Rev 2017;25:205–10. https://doi.org/10.1097/crd.0000000000000145.Search in Google Scholar
2. Ewy, GA, Felner, JM, Juul, D, Mayer, JW, Sajid, AW, Waugh, RA. Test of a cardiology patient simulator with students in fourth-year electives. J Med Educ 1987;62:738–43. https://doi.org/10.1097/00001888-198709000-00005.Search in Google Scholar
3. Akins, R, Ho, H. Outcomes of using heart sound simulator in teaching cardiac auscultation. Can Med Educ J 2010;1:46–50. https://doi.org/10.36834/cmej.36528.Search in Google Scholar
4. de Giovanni, D, Roberts, T, Norman, G. Relative effectiveness of high- versus low-fidelity simulation in learning heart sounds. Med Educ 2009;43:661–8. https://doi.org/10.1111/j.1365-2923.2009.03398.x.Search in Google Scholar
5. Chien, C. The Hall effect and its applications. New York: Springer Science & Business Media; 2013. 550 p.Search in Google Scholar
6. Hudder, A, Tackett, S, Moscatello, K. First-Year experience implementing an adaptive learning platform for first- and second-year medical students at the lake erie College of osteopathic medicine. J Am Osteopath Assoc 2019;119:51–8. https://doi.org/10.7556/jaoa.2019.008.Search in Google Scholar
7. Friederichs, H, Weissenstein, A, Ligges, S, Möller, D, Becker, JC, Marschall, B. Combining simulated patients and simulators: pilot study of hybrid simulation in teaching cardiac auscultation. Adv Physiol Educ 2014;38:343–7. https://doi.org/10.1152/advan.00039.2013.Search in Google Scholar
© 2020 Dominik Karch et al., published by De Gruyter, Berlin/Boston
This work is licensed under the Creative Commons Attribution 4.0 International License.
Articles in the same Issue
- Research Articles
- Overview of the holographic-guided cardiovascular interventions and training – a perspective
- Development of the low-cost, smartphone-based cardiac auscultation training manikin
- Cooperation of CUDA and Intel multi-core architecture in the independent component analysis algorithm for EEG data
- A distributed cognitive approach in cybernetic modelling of human vision in a robotic swarm
- Thingspeak-based respiratory rate streaming system for essential monitoring purposes
- Recognition of multifont English electronic prescribing based on convolution neural network algorithm
- Short Communication
- BatchDeconvolution: a Fiji plugin for increasing deconvolution workflow
Articles in the same Issue
- Research Articles
- Overview of the holographic-guided cardiovascular interventions and training – a perspective
- Development of the low-cost, smartphone-based cardiac auscultation training manikin
- Cooperation of CUDA and Intel multi-core architecture in the independent component analysis algorithm for EEG data
- A distributed cognitive approach in cybernetic modelling of human vision in a robotic swarm
- Thingspeak-based respiratory rate streaming system for essential monitoring purposes
- Recognition of multifont English electronic prescribing based on convolution neural network algorithm
- Short Communication
- BatchDeconvolution: a Fiji plugin for increasing deconvolution workflow